Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Factors Influencing Poor Drug Compliance Among Patients with Diabetes Mellitus: An Experience from Rural Indonesia
Authors Pasambo Y ![]() , Murti FAK
, Murti FAK ![]() , Efendi F
, Efendi F ![]() , Widyawati IY, Pradipta RO
, Widyawati IY, Pradipta RO ![]() , Chong MC
, Chong MC ![]()
Received 29 August 2025
Accepted for publication 8 January 2026
Published 28 January 2026 Volume 2026:19 563957
DOI https://doi.org/10.2147/JMDH.S563957
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Yourisna Pasambo,1,2 Fadhaa Aditya Kautsar Murti,3 Ferry Efendi,1,4,5 Ika Yuni Widyawati,1 Rifky Octavia Pradipta,1,4 Mei-Chan Chong6
1Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia; 2Nursing Department, Politeknik Kesehatan Kementerian Kesehatan Manado, Manado, Indonesia; 3Department of Biostatistics and Population Studies, Faculty of Public Health, Universitas Indonesia, Depok, Indonesia; 4Research Centre of Advancing Community Healthcare (REACH), Surabaya, Indonesia; 5School of Nursing & Midwifery, La Trobe University, Melbourne, Australia; 6Department of Nursing Science, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Malaysia
Correspondence: Ferry Efendi, Faculty of Nursing, Universitas Airlangga, Surabaya, East Java, 60115, Indonesia, Tel/Fax +6231 5913257, Email [email protected]
Background: Low medication compliance is one of the main challenges in managing Type 2 Diabetes Mellitus (T2DM) in rural areas, increasing the risk of complications. Identifying factors that influence compliance is essential for improving disease management.
Methods: This cross-sectional study used data from the 2023 Indonesian Health Survey, including 292 rural T2DM patients who met the inclusion criteria. Variables examined were demographic factors and health-related factors. Odds ratios (OR) were calculated to assess associations with medication compliance.
Results: Men and individuals with lower educational levels had a higher likelihood of non-compliance men (OR 1.41; p = 0.302), elementary education or below (OR 1.29; p = 0.618), whereas older age tended to be associated with better compliance (OR 0.98; p = 0.305); however, none of these associations were statistically significant. Unemployed patients had lower odds of non-compliance compared with those who were employed (aOR 0.39; p = 0.002), whereas individuals who only occasionally or never attended follow-up visits had much higher odds of non-compliance than those who did so regularly (p < 0.001 and p < 0.001), and both associations were statistically significant. Medication-related knowledge was significant in the unadjusted model (OR 3.78; p < 0.001), but not after adjustment. Perceived accessibility of health facilities was not significantly associated with non-compliance (p = 0.375).
Conclusion: Medication non-compliance among patients with T2DM in rural areas shows an inverse association with being unemployed and older age, and a direct association with lower frequency of follow-up visits, male gender, lower educational level, poorer medication-related knowledge, and perceived poor accessibility of health facilities. Interventions should strengthen rural primary care via flexible service hours, active outreach, and family-involved education, particularly for working-age men.
Keywords: diabetes mellitus, poor drug compliance, risk factor, rural areas, Indonesia
Introduction
Type 2 diabetes mellitus (T2DM) continues to increase, both globally and in Indonesia, and remains a major challenge for the healthcare system. The 2023 Indonesian Health Survey (SKI) showed an increase in the prevalence of diabetes compared to the 2018 Basic Health Research (Riskesdas) results, from 2% to 2.2% in the ≥15 age group.1,2
This disease requires appropriate management to prevent serious complications, such as microvascular complications (retinopathy, nephropathy, and neuropathy) and macrovascular complications (coronary heart disease, cerebrovascular disease, and peripheral artery disease),3,4 as well as cardiovascular complications, which are the leading cause of morbidity and mortality in diabetes mellitus patients and account for up to 85% of deaths.5
A qualitative study in rural communities in Indonesia demonstrated that medication adherence is part of a complex self-care burden influenced by limited access, low health literacy, and sociocultural factors.6 Another study in the Manis Mata Community Health Center in Ketapang reported that 94.3% of T2DM patients were non-compliant with their medication, with a common pattern of only taking medication when feeling unwell and stopping when feeling better, as well as not attending regular check-ups.7
Non-compliance with medication is associated with poor glycemic control, leading to increased fasting blood glucose (FBG) and postprandial blood glucose (PPBG) levels,8 and may increase the risk of diabetes-related complications, higher hospitalisation rates, and higher mortality rates.9–11
Patients with T2DM in rural areas face different challenges than those living in urban areas. In Indonesia, secondary and tertiary services are more concentrated in cities, while rural communities rely more on community health centres (Puskesmas) and primary healthcare facilities with more limited staff and infrastructure, creating a gap in service utilization between urban and rural areas.12 Long distances, long travel and waiting times, and the costs of transportation, medication, and supporting examinations are additional barriers that can reduce service utilization and treatment adherence in rural T2DM patients.13
Traditional healing beliefs and practices also shape the treatment behavior of diabetes patients in rural Indonesia. Studies of patients with chronic diseases show that approximately one-third of respondents use traditional medicine (jamu/herbs), and traditional medicine users tend to have lower or more complex adherence patterns to medication.14 Research on T2DM patients in Aceh also reported that many patients choose herbal medicines because they are cheaper, readily available, and believed to have fewer side effects than synthetic drugs. These cultural and belief-related factors may influence patients’ decisions to initiate, continue, or discontinue prescribed treatments.15
Previous studies have identified various factors influencing medication compliance, including socioeconomic status, health literacy, comorbidities, and access to healthcare services.11,16–20 However, these studies have not specifically examined these factors in the context of rural T2DM patients, who face unique challenges related to limited access to healthcare facilities, knowledge about the disease, and limited resources. Studies on medication compliance in T2DM in Indonesia are still dominated by research conducted in urban areas, so evidence on the factors influencing compliance among T2DM patients in rural areas remains very limited.21–23 Therefore, it is important to explore further how these factors interact in the rural context and affect medication adherence among T2DM patients.
This study aimed to identify factors associated with medication non-compliance in T2DM patients in rural areas, focusing on sociodemographic and health-related factors. By understanding these factors more specifically in the rural context, this study was expected to provide a basis for developing more effective and targeted intervention strategies to improve medication compliance and health outcomes in T2DM patients in rural areas.
This study provides a comprehensive analysis by integrating various variables, including treatment type, health factors (perceived health facility accessibility and well-informed medication), and sociodemographic factors. This holistic approach can provide a more complete picture of the influence of various factors on medication compliance, which may not have been extensively studied in previous research. Investigating patients’ perceptions regarding access to healthcare facilities and possession of medication information is an important yet often overlooked aspect. This study can provide new insights into how these perceptions influence patients’ decisions regarding medication compliance.
This study uses the latest data from the 2023 national-scale Indonesian Health Survey to ensure that the findings reflect current trends and challenges in diabetes management. This is important for developing timely and relevant interventions.8,24
Methods
Study Design and Population
The research employed a cross-sectional design to analyze the 2023 Indonesian Health Survey (SKI) data and was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.25 SKI 2023 was conducted to assess the achievement of health development results in the last five years in Indonesia and to determine the nutritional status of toddlers in 2019–2024.2 Survey data is managed by the Indonesian Ministry of Health.
The survey was conducted nationwide, down to the district/city level, through face-to-face interviews using standardized individual and household questionnaires, administered by trained local enumerators under technical and administrative supervision to ensure uniform procedures. The classification of areas as urban or rural in this study follows the guidelines established by the Central Statistics Agency (BPS) regarding urban and rural classification in Indonesia. Determining an area as urban or rural is done by considering the following criteria: (1) population density, (2) percentage of households classified as agricultural, and (3) access to urban facilities (education, health, trade, energy, and other public service infrastructure). If a village or sub-district meets certain thresholds in these criteria, it is categorized as an urban area; conversely, if it does not meet these criteria, it is categorized as a rural area.2,26 To minimize measurement and respondent bias, validated instruments and standard procedures were used.
Data were collected from May to July 2023 with a response rate of 91.49%. The sampling technique was stratified and multilevel random sampling. The number of SKI 2023 samples obtained was 315,646 ordinary households representing districts and cities in Indonesia, with details of 877,531 household members interviewed, and 1,191,692 respondents interviewed. SKI also carried out data weighting to accurately represent the data, correct bias, and improve data quality.2
The population in this study was individuals with Diabetes Mellitus (DM). The sample was determined based on inclusion criteria, namely T2DM status obtained from a doctor’s diagnosis and living in a rural area. A total of 292 T2DM patients met the criteria and became the study sample, with 253 patients in the compliant group and 39 in the non-compliant group.
Measurement
The independent variables in this study were divided into sociodemographic factors and health-related factors. Sociodemographic factors consisted of age, gender, education, employment status, and follow-up visit frequency. Education level was adapted from UNESCO’s International Standard Classification of Education (ISCED), which was adjusted to the education system in Indonesia, and was classified into: elementary school and below, high school, and college. Employment status was classified into working and not working. The frequency of follow-up visits/DM disease control to healthcare facilities was measured using the question, “Do you routinely visit a doctor to control your diabetes?”, with three choices: 1) yes, routinely; 2) yes, sometimes; and 3) no.
Health-related factors included patient perceptions of the accessibility of health facilities and of being well-informed about medication. Perceptions regarding the accessibility of health facilities were measured through household assessments of the health services provided by healthcare facilities with easy access to affordable care. The answer “yes” was categorized as easy access to affordable health services, and “no” as unaffordable access to health services.
Well-informed about medication was measured using the question “Have you ever received information/explanation that DM medication must be taken continuously/for life? The answer “yes” was categorized as having complete treatment information, and the answer “no” as not having complete treatment information.
The dependent variable was the patient’s level of medication compliance. This variable was measured by the question “Do you take/inject anti-diabetes medication according to the doctor’s instructions? If the patient answered “Yes”, according to the doctor’s instructions, the patient was categorized as compliant; if the patient answered “No”, the patient was categorized as non-compliant.
Data Analysis
We describe the prevalence of DM for the entire study population and also for population groups defined in terms of age, gender, educational level, follow-up visit frequency, perceived accessibility of health facilities, and well-informed of medication. DM prevalence was calculated as the number of cases per 100 people, and the figure was adjusted for other variables using the direct method, with the survey population as the standard population.
Based on the data obtained, differences and ratios were calculated to compare age, gender, educational level, follow-up visit frequency, perceived accessibility of healthcare facilities, and well-informed of medication. Odds ratios were determined by dividing the odds in the highest group by the odds in the lowest group.
The magnitude of differences in medication compliance among T2DM patients in rural areas was estimated using odds ratios (OR). Odds ratios were used to evaluate the relationship between factors influencing medication compliance and measured health outcomes. A higher OR value indicates a greater likelihood of medication non-compliance, as seen in the variables of follow-up visit frequency and well-informed of medication. In this study, we also controlled for other variables to gain a better understanding of the factors influencing medication compliance among diabetes patients in rural areas.
Results
In this study, there was no significant difference in mean age between diabetes mellitus patients who complied with medication and those who did not (Mean: 55 in both groups). In both groups, females outnumbered males. Additionally, a higher proportion of participants were employed compared to those who were not. Regarding education, the majority had completed high school, while the rest had only attained an elementary-level education. Only a small number had obtained a diploma or university degree.
In terms of health-related factors, a clear gradient was observed between the two groups. The number of individuals who attended follow-up visits increased in the compliance group, whereas the opposite trend was seen in the non-compliance group. In addition, non-compliance was slightly higher among those who perceived health facilities as inaccessible. Interestingly, individuals who were well-informed about their medication had higher non-compliance rates (28%) than those who were not (9%). More details are presented in Table 1.
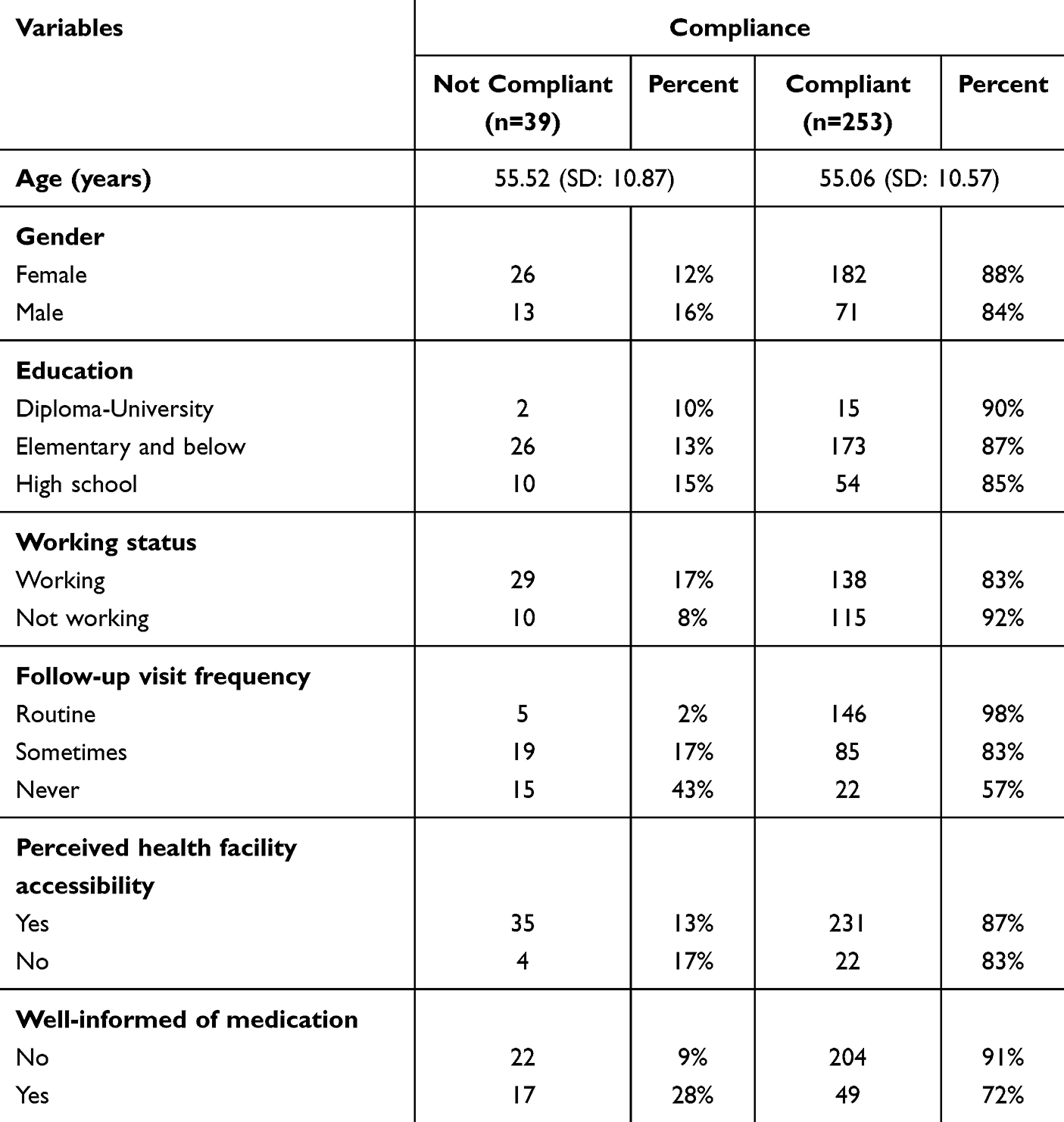 |
Table 1 Sociodemographic Distribution of the Research Population |
Medication Type
Among non-compliance, OAD (Oral Antidiabetic Drugs) showed the highest non-compliance rate compared to others (65%). The proportion of people who did not consume medication was also notably high (32%). Insulin showed the lowest non-compliance proportion among all, with 2.3%.
Factors Associated with Medication Non-Compliance
In this study, we found that the older the patient was, the less likely they were to be non-compliant (cOR: 0.98, 95% CI: 0.95–1.01), although the effect was not significant at the 95% confidence level. Similarly, the effect differences of gender and education were not significant (p-value > 0.05). However, males had higher odds of non-compliance compared to females (cOR: 1.41, 95% CI: 0.73–2.71). Additionally, individuals with lower education levels were more likely to be non-compliant compared to those with a diploma or university degree (cOR: 1.29, 95% CI: 0.46–3.60 for elementary education and cOR: 1.69, 95% CI: 0.57–5.01 for high school education). Moreover, perceived accessibility of healthcare facilities was not significantly associated. People who perceived healthcare as not accessible had higher odds of being non-compliant (cOR: 1.36, 95% CI: 0.68–2.72).
Statistical associations were found among working status, follow-up visit frequency, and well-informed medication. Interestingly, people who were informed that diabetic medication should be consumed during their lifetime showed higher odds to be non-compliant (cOR: 3.78, 95% CI: 1.88–7.59). However, this association was not significant after being adjusted with other variables. In contrast, people who were not working showed lower odds of being non-compliant (cOR: 0.45, 95% CI: 0.25–0.81), and this association remained significant after being controlled by other variables (aOR: 0.39, 95% CI: 0.21–0.70).
We also observed a gradient in the odds ratio concerning follow-up visit frequency. The less frequently individuals attended follow-up visits, the more likely they were to be non-compliant. Individuals who only occasionally attended follow-up visits had higher odds of non-compliance than those who did so routinely (cOR: 11.40, 95% CI: 4.09–31.77). Likewise, those who never attended follow-up visits for their diabetes care had even higher odds of non-compliance (cOR: 44.4, 95% CI: 17.20–114.61). These associations remained significant even after adjusting for other variables (aOR: 9.61 and 42.59). More details are presented in Table 2.
 |
Table 2 Factors Associated with Medication Non-Compliance |
Discussion
Employment Status and Frequency of Visits as the Main Determinants of Non-Compliance
The study showed a significant relationship between employment status and the frequency of follow-up visits with medication non-compliance among patients with T2DM in rural areas, with non-compliance lower among unemployed patients and higher among those who rarely or never attended follow-up visits. These findings highlight that patients’ ability to make time and maintain regular contact with healthcare services is a greater determinant for compliance than sociodemographic characteristics such as gender or education. This is in line with various studies showing that continuous follow-up visits and working conditions significantly influence compliance and clinical outcomes in diabetes mellitus patients.16,27,28
In the rural Indonesian context, individuals work primarily in the informal sector, such as farming or daily labor—often with long, inflexible working hours, making it difficult for them to leave work to visit the Puskesmas or follow regular medication schedules.6 In contrast, unemployed patients generally spend more time at home, making them easier to reach by community health cadres and healthcare workers and more able to participate in Chronic Disease Management Program (Prolanis) and Integrated Post for Noncommunicable Disease Control (Posbindu PTM) activities in the village. This more frequent contact provides repeated reinforcement about the importance of treatment and helps maintain a regular medication supply, thereby reducing the risk of treatment interruption and making compliance easier to maintain.29
In Indonesia, the status of “unemployed” in rural areas does not necessarily mean a lack of financial capacity to obtain medicines, because antidiabetic drugs for National Health Insurance (JKN) participants can be obtained free of charge at Puskesmas.30 Economic barriers are more often related to indirect costs, such as transportation, loss of income, and time, rather than the cost of medication itself.13 Thus, unemployed status more accurately reflects the availability of time and proximity to health services than the ability to pay. Many in this group are also elderly or individuals with declining health who have already experienced the impact of the disease, making them more motivated to adhere to treatment.31 Stronger family support, such as accompanying them to follow-up visits and reminding them to take medication, is also more likely in this group.32
A low frequency of follow-up visits indicates that patients have only occasional contact with health services. Many patients in rural areas come to the Puskesmas only when symptoms become severe or when their medication has entirely run out, which may be influenced by distance, transportation costs, loss of work opportunities, and the perception that “as long as there are no symptoms, they are healthy”.33,34 As a result, patients who rarely or never attend follow-up have a much higher likelihood of not adhering to their medication regimen, as reflected in the high odds ratios. From this perspective, infrequent follow-up visits and medication non-compliance are two manifestations of the same structural barriers, particularly those related to physical access, economic constraints, and limited time.35,36
These findings emphasize the need to strengthen not only general education but also the role of primary care in rural areas. Puskesmas and Prolanis should be optimized as centers for chronic disease management by implementing more structured visit scheduling, active follow-up of patients who miss appointments, and home visits for those who rarely attend. Support measures such as proper record-keeping, coordination with village health cadres, more flexible service hours for workers, and clear referral pathways would be more realistic strategies to reduce non-compliance in rural settings.
Well-Informed Medication
Being well-informed about medication was significantly associated with non-compliance in the unadjusted analysis, but this association was no longer significant after adjustment for other variables. Interestingly, individuals who were well-informed about their medications had higher levels of non-compliance than those who were less informed. This finding indicates that medication knowledge is not an independent determinant but is influenced by other factors, such as more frequent contact with health services.37 This finding aligns with studies showing that medication and disease knowledge are indeed related to compliance, but are often mediated by the intensity of interaction with healthcare providers and structured educational programs.38,39
In rural settings with various social and economic constraints, knowledge alone is not sufficient to ensure compliance. Patients who feel they “already know” sometimes feel more free to adjust doses or stop taking their medication when they feel well, while adherence decisions are also influenced by side effects, indirect costs, family support, and trust in the medication itself.40 This illustrates that adherence behaviour is complex and shaped by multiple factors, as reflected in qualitative studies on barriers to DM self-care and chronic disease management in primary care.6,36,40
These findings highlight that education alone is not sufficient; it needs to be combined with social support, simplified medication regimens, and empathetic two-way communication between healthcare providers and patients. In rural areas, education should be embedded within structured follow-up, such as regular Prolanis meetings and home visits, and should actively involve family members as treatment companions.41,42 Various studies also show that a combination of intensive counselling, simple reminders (such as SMS), and ongoing follow-up is more effective in improving adherence than brief, stand-alone educational sessions.43,44
Age, Gender, Education, and Perceived Accessibility
Age, gender, education, and perceived accessibility of health facilities did not show a statistically significant association with medication non-compliance, although certain patterns were still observable. Older age tended to be associated with lower non-compliance. This may reflect the fact that older adults have lived longer with diabetes, have more frequent contact with healthcare providers, and may already have experienced complications, thus increasing motivation to adhere to treatment.45,46 In rural areas, elderly patients also often receive strong family support, for example, being driven to Puskesmas and reminded to take the medication, which indirectly improves compliance, as reported in several studies on factors related to DM treatment compliance.47,48
Men were more likely than women to be non-compliant, although the difference was not significant. This pattern may be linked to gender norms, whereby men often minimize health risks, are reluctant to seek help, and focus more on their role as breadwinners.49,50 Meanwhile, women tend to have more frequent contact with health services, greater involvement in village community activities, and stronger social support networks.51
The lack of a significant effect of education on non-compliance may be related to the characteristics of rural areas, where most respondents have relatively homogeneous and generally low levels of education.52 In addition, the existence of the JKN scheme and relatively standardized services at Puskesmas, including Prolanis group education delivered in simple language, may reduce information gaps between education levels.53
Perceived accessibility of health facilities also showed no significant association, although non-compliance was slightly higher among patients who perceived facilities as difficult to reach. In rural settings, the network of Puskesmas and auxiliary health posts (Pustu) is relatively widespread, but the barriers perceived by patients are not limited to physical distance; they also include transport costs, the need for a companion, waiting time, and lost work opportunities. When these barriers are perceived as substantial, patients tend to delay visits and are less motivated to adhere to treatment, even when health facilities are objectively available.54,55
The tendency toward better compliance in older age groups suggests that they are relatively protected by their longer illness experience, so efforts to improve compliance should be more focused on younger groups, who may not yet have felt the full impact of the disease and are less accustomed to routine follow-up.46,47 The trend toward higher non-compliance among men also indicates the need for more targeted education for men through channels that are close to their daily activities, such as workplaces, farmer groups, or religious forums in rural communities.56,57 On the other hand, the absence of clear differences by education level supports an educational approach that prioritizes simple, repeated, and easy-to-understand information delivery to all patients, rather than focusing only on those with low education.52,53 Meanwhile, the tendency toward higher non-compliance among patients who find access difficult highlights the need to improve practical aspects such as transport costs, waiting time, and flexibility of service hours, so that the existing network of Puskesmas and Pustu is truly perceived as accessible by rural patients.54,55
These findings indicate the need to strengthen primary care services so that they are more worker-friendly, structured, and family–community based. Primary health centers (Puskesmas) can adjust service hours, strengthen active tracing of patients who rarely attend (through reminders, home visits, and the role of community health cadres), and optimize Prolanis and Posbindu as centers for monitoring adherence and continuity of medication. Treatment education should be embedded within routine visits, involve family members, and be delivered using simple, easy-to-understand language. Young adults and male workers can be reached through workplaces, farmer groups, or religious forums, while practical barriers such as costs, waiting times, and loss of income need to be reduced through outreach services, health posts closer to the village, or combining multiple services in a single visit.
We acknowledge several limitations of this study. The use of secondary data from the Indonesian health survey may affect the accuracy and relevance of some variables. In addition, the relatively simple categorization of variables may not fully capture the complexity of factors influencing adherence, and the focus on the local context may limit the generalizability of the findings. The restriction to rural areas also limits generalization to the broader population, as determinants of adherence may differ between urban and rural settings. Although data weighting was applied to improve representativeness, the results should be generalized with caution, especially to regions outside rural settings.
Conclusion
This study shows that medication non-compliance among patients with T2DM in rural areas is mainly associated with employment status and the follow-up visit frequency. Unemployed patients tend to be more adherent because they have more time, more frequent contact with health services, and stronger family support, whereas patients who rarely or never attend follow-up visit have a much higher risk of non-compliance. Medication knowledge plays a role, but is not a single determining factor; its influence is largely mediated by the intensity of contact with healthcare providers and the socioeconomic context of rural communities.
Efforts to improve compliance should therefore focus on strengthening primary care, particularly Puskesmas, Prolanis activities, and Posbindu, through more flexible service hours for workers, active tracing of patients who rarely attend, home visits, and education integrated into routine follow-up and involving family members. Young adults and male workers should be specifically targeted for interventions. Further research, mainly qualitative studies and community-based intervention trials, is needed to identify and test the most effective strategies for improving medication compliance among patients with diabetes mellitus in rural areas.
Ethics and Informed Consent Statements
This study utilized secondary data from the 2023 Indonesian Health Survey, conducted by the Health Policy Agency, Ministry of Health, Indonesia. All data were fully anonymized prior to being accessed by the researchers. This study involved no direct intervention or interaction with participants. All data collection procedures conducted by the survey organizer adhered to ethical standards and received approval from the Ministry of Health Research and Development health survey ethics protocol (approval No. LB.02.01/I/KE/L/287/2023) on May 10, 2023. Informed consent was obtained from all participants during the original data collection process.
Based on the Guidelines and Ethical Standards for National Health Research and Development published by the Indonesian Ministry of Health,58 in the section “Types/Levels of Ethical Review” that are exempted, point ii (page 55), it is stated that research that has obtained ethical approval from an accredited ethics committee does not need to obtain ethical approval from other ethics committees. Therefore, the use of data from the 2023 Indonesian Health Survey did not require further ethical approval.
Acknowledgments
There are no acknowledgments to declare.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Riskesdas. Hasil Utama Riskesdas 2018. 2018.
2. Kemenkes. Survei Kesehatan Indonesia (SKI) Tahun 2023 [Internet]. Jakarta; 2023. Available from: https://www.slideshare.net/slideshow/survei-kesehatan-indonesia-ski-tahun-2023/269424965.
3. Shah T, Farooq Z, Cohen-Addad D, DeAlwis D. A multisystemic pictorial review of diabetes mellitus. Contemp Diagn Radiol. 2021;44(2):1–11. doi:10.1097/01.CDR.0000725624.70337.47
4. Johnson L, Weinstock R. Medical complications of diabetes mellitus. In: Diabetes Mellitus and Oral Health: An Interprofessional Approach. 2014:45–68.
5. Price J, Verma S, Li RK. Diabetic heart dysfunction: is cell transplantation a potential therapy? Heart Fail Rev. 2003;8(3):213–219. doi:10.1023/A:1024701113383
6. Kurnia A, Said FM, Panduragan SL. Experience of burden in self-care of type 2 diabetes mellitus: a qualitative study in indonesian context. Malaysian J Nurs. 2025;16(4):33–44. doi:10.31674/mjn.2025.v16i04.004
7. Deomedes AR, Pradika J, Pradika J. Kepatuhan minum obat pada penderita DM tipe 2. Jurnal Riset Keperawatan Dan Kesehatan. 2025;2:191–199. doi:10.71203/jrkk.v2i5.66
8. Kaaffah S, Soewondo P, Riyadina W, Renaldi FS, Sauriasari R. Adherence to treatment and glycemic control in patients with type 2 diabetes mellitus: a 4-year follow-up PTM bogor cohort study, Indonesia. Patient Prefer Adherence. 2021;15:2467–2477. doi:10.2147/PPA.S318790
9. Polonsky WH, Henry RR. Poor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributors. Patient Prefer Adherence. 2016;10:1299–1306. doi:10.2147/PPA.S106821
10. Blackburn DF, Swidrovich, J, Lemstra, M. Nonadherence in type 2 diabetes: practical considerations for interpreting the literature. Patient Prefer Adherence. 2013; 7:183–189. doi:10.2147/PPA.S30613
11. Ho PM, Rumsfeld JS, Masoudi FA, et al. Effect of medication nonadherence in diabetes mellitus. Cardiol Rev. 2007, 4. 24;4: doi:.
12. Wulandari RD, Laksono AD. Urban-rural disparity: the utilization of primary healthcare centers among elderly in East Java, Indonesia. Indonesian J Health Adm. 2019;7(2):147–154.
13. Bratanegara A, Pitoyo A, vWidayani P, Hizbaron D. Geospatial disparities in elderly health: a gis-based study of functional independence in Tasikmalaya Regency, Indonesia. International Journal of Geoinformatics. 2025;21(9): 17–36 doi:10.52939/ijg.v21i9.4439
14. Pradipta RO, Efendi F, Alruwaili AS, Diansya MR, Kurniati A. The journey of Indonesian nurse migration: a scoping review. Healthc Low Resour Settings. 2023;11(2). doi:10.4081/hls.2023.11278
15. Husna F, Marisa M, Suryawati S, et al. Traditional remedies from Aceh for diabetes mellitus treatment: patterns of use in rural-urban areas in Aceh. Clin Epidemiol Glob Health. 2025;34:102079. doi:10.1016/j.cegh.2025.102079
16. Kassaw AT, Tarekegn TB, Derbie A, Ashagrie G, Girmaw F, Mengesha A. Non-adherence to antidiabetic medications and associated factors among adult type 2 diabetes mellitus patients in Northeast Ethiopia: institutional based cross-sectional study. BMJ Open. 2025;15(4):e093413. doi:10.1136/bmjopen-2024-093413
17. Jackson IL, Adibe MO, Okonta MJ, Ukwe CV. Medication adherence in type 2 diabetes patients in Nigeria. Diabetes Technol Ther. 2015;17(6):398–404. doi:10.1089/dia.2014.0279
18. Azharuddin M, Adil M, Sharma M, Gyawali B. A systematic review and meta-analysis of non-adherence to anti-diabetic medication: evidence from low- and middle-income countries. Int J Clin Pract. 2021;75(11). doi:10.1111/ijcp.14717
19. Waari G, Mutai J, Gikunju J. Medication adherence and factors associated with poor adherence among type 2 diabetes mellitus patients on follow-up at Kenyatta National Hospital, Kenya. Pan Afr Med J. 2018;29. doi:10.11604/pamj.2018.29.82.12639
20. Jeyalakshmi K, Rao M, Shashidhara YN, et al. Determinants of medication non-adherence among the elderly with co-existing hypertension and type 2 diabetes mellitus in rural areas of Udupi District in Karnataka, India. Patient Prefer Adherence. 2023;17:1641–1656. doi:10.2147/PPA.S380784
21. Alfian R, Ariani N, Nita Y, Athiyah U. Assessment to barriers of medication adherence among patients with type 2 diabetes mellitus. J Res Pharm. 2025;29(3):918–927. doi:10.12991/jrespharm.1693752
22. Suprapti B, Izzah Z, Anjani AG, Andarsari MR, Nilamsari WP, Nugroho CW. Prevalence of medication adherence and glycemic control among patients with type 2 diabetes and influencing factors: a cross-sectional study. Glob Epidemiol. 2023;5:100113. doi:10.1016/j.gloepi.2023.100113
23. Zairina E, Nugraheni G, Sulistyarini A, Setiawan CD, Kripalani S, Lestari SI. Factors related to barriers and medication adherence in patients with type 2 diabetes mellitus: a cross-sectional study. J Diabetes Metab Disord. 2022;21(1):219–228. doi:10.1007/s40200-021-00961-6
24. Kurniawan F, Sigit FS, Trompet S, et al. Lifestyle and clinical risk factors in relation with the prevalence of diabetes in the Indonesian urban and rural populations: the 2018 Indonesian basic health survey. Prev Med Rep. 2024;38:102629. doi:10.1016/j.pmedr.2024.102629
25. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
26. BPS. Peraturan Kepala Badan Pusat Statistik Nomor 37 Tahun 2010 Tentang Klasifikasi Perkotaan Dan Perdesaan Di Indonesia. Jakarta: Badan Pusat Statistik; 2010.
27. Monju IH, Ahmed T, Abrar M, et al. Prevalence and factors associated with medication adherence among diabetes patients in rural sub-district health facilities in Bangladesh. Discover Public Health. 2025;22(1). doi:10.1186/s12982-025-00504-x
28. Owolabi EO, Ajayi AI. Adherence to medication, dietary and physical activity recommendations: findings from a multicenter cross-sectional study among adults with diabetes in rural South Africa. J Eval Clin Pract. 2024;30(7):1261–1271. doi:10.1111/jep.14035
29. Maarif S, Setiaji B, Noviansyah N, Pratiwi DU. The factors that are related to visiting participants of the chronic disease management program to the prolanis aerobic club in lampung central regency, 2020. J Qual Public Health. 2021;4(2):38–48. doi:10.30994/jqph.v4i2.192
30. Firori FA, Wisana IDGK. The effect of participation in JKN on unmet needs for healthcare services. Indonesian J Health Adm. 2023;11(2):186–195.
31. Afkhami S, Asadi F, Emami H, Sabahi A. The morisky method for measuring medication adherence in older adults with chronic diseases: a cross-sectional study. Health Sci Rep. 2025;8(5). doi:10.1002/hsr2.70681
32. Alcântara L, Figueiredo T, Costa E. Exploring the perceptions and self-perceptions of therapeutic adherence in older adults with chronic conditions: a scoping review. Patient Prefer Adherence. 2025;19:503–526. doi:10.2147/PPA.S496707
33. Asril NM, Tabuchi K, Tsunematsu M, Kobayashi T, Kakehashi M. Predicting healthy lifestyle behaviours among patients with type 2 diabetes in Rural Bali, Indonesia. Clin Med Insights Endocrinol Diabetes. 2020;13:1179551420915856.
34. Hilmi IL, Alfian SD, Abdulah R, Puspitasari IM. Factors associated with health-seeking behavior in Indonesia: evidence from the indonesian family life survey 2014. Medicina. 2024;60(10):1607. doi:10.3390/medicina60101607
35. Kulhawy-Wibe S, King-Shier KM, Barnabe C, Manns BJ, Hemmelgarn BR, Campbell DJT. Exploring structural barriers to diabetes self-management in Alberta First Nations communities. Diabetol Metab Syndr. 2018;10(1). doi:10.1186/s13098-018-0385-7
36. Pi L, Shi X, Wang Z, Zhou Z. Predictors of and barriers to follow-up uptake: analysis of factors and perceived barriers among high-risk individuals with diabetes after screening in China. Public Health. 2024;232:128–131. doi:10.1016/j.puhe.2024.04.026
37. Kardas P. From non-adherence to adherence: can innovative solutions resolve a longstanding problem? Eur J Intern Med. 2024;119:6–12. doi:10.1016/j.ejim.2023.10.012
38. AlShayban DM, Naqvi AA, Alhumaid O, et al. Association of disease knowledge and medication adherence among out-patients with type 2 diabetes mellitus in Khobar, Saudi Arabia. Front Pharmacol. 2020,2;11:60 doi:10.3389/fphar.2020.00060.
39. Hassan M, ElHelaly M, Badawi N, Nader M, Shamma R. Impact of tailored diabetes education on adherence and glycemic control in children and adolescents on continuous subcutaneous insulin infusion, prospective interventional study in a tertiary center. BMC Pediatr. 2025;25(1). doi:10.1186/s12887-025-06018-4
40. Tu P, Smith D, Clark R, Bayzle L, Tu R, Lin C. Patients’ characterization of medication, emotions, and incongruent perceptions around adherence. J Pers Med. 2021;11(10):975. doi:10.3390/jpm11100975
41. Coulter KJ. Standardized follow-ups lower HbA1c in adults with type 2 diabetes living in a rural community: a pilot study. J Dr Nurs Pract. 2018;11(1):16–24. doi:10.1891/2380-9418.11.1.16
42. Pamungkas RA, Chamroonsawasdi K. Family functional-based coaching program on healthy behavior for glycemic control among Indonesian communities: a quasi-experimental study. Oman Med J. 2020;35(5):1–11. doi:10.5001/omj.2020.115
43. Bashir MB, Ijaz S, Farooq U, Kahar A, Quan WZ. Diabetes educator-led education intervention to improve the medication adherence and quality of life in type 2 diabetes patients: a pre-and post-analysis. Rom J Diabetes Nutr Metab Dis. 2025;32(2):119–127.
44. Evensen E, Emaus N, Furberg AS, et al. Adolescent body composition and associations with body size and growth from birth to late adolescence. The Tromsø study: fit Futures—A Norwegian longitudinal cohort study. Pediatr Obes. 2019;14(5). doi:10.1111/ijpo.12492
45. Barba EL, de Miguel MR, Hernández-Mijares A, et al. Medication adherence and persistence in type 2 diabetes mellitus: perspectives of patients, physicians and pharmacists on the Spanish health care system. Patient Prefer Adherence. 2017;11:707–718. doi:10.2147/PPA.S122556
46. Mohammed AG, Yaseen NT, AlWaeli DK. Analyzing medication adherence patterns among type 2 diabetes patients in Thi-Qar, Iraq: a cross-sectional study. J Diabetes Res. 2025;2025(1). doi:10.1155/jdr/6659722
47. Nurjanah S, Sufyanti Y, Soleha U, Hatmanti NM, Purwanti N, Karlina S. The relationship between the role of the family and the use of control card with the level of compliance with medication in elderly patients at UPTD Puskesmas Wonokromo. Bali Med J. 2023;12(3):2808–2811. doi:10.15562/bmj.v12i3.4354
48. Olagbemide OJ, Omosanya OE, Ayodapo AO, Agboola SM, Adeagbo AO, Olukokun TA. Family support and medication adherence among adult type 2 diabetes: any meeting point? Ann Afr Med. 2021;20(4):282–287. doi:10.4103/aam.aam_62_20
49. Heredia-Pi IB, Orozco-Núñez E, Guerrero-López CM, et al. Gendered experience of people living with type 2 diabetes in rural and urban Mexico: an ethnographic study. Int J Equity Health. 2025;24(1). doi:10.1186/s12939-025-02523-1
50. Kausar R, Awan B, Khan N. Gender differences in risk perception and emotional distress in patients with type 2 diabetes. Indian Acad Appl Psychol. 2013;39:222–7.
51. Li H, Min H, Zhang L, Li Y, Wang J, Jia X. The relationships between social support, medication adherence, and glycemic control among inpatients with type 2 diabetes: a cross-sectional survey in Xi’an, China. Front Pharmacol. 2025 ;16(6):1634768. doi:10.3389/fphar.2025.1634768
52. Dangaura NR, Khanal P, Kuikel BS, et al. Impact of national health insurance on medication adherence among hypertensive patients: a hospital-based cross-sectional study from Kailali, Nepal. PLoS One. 2025;20(9):e0332602. doi:10.1371/journal.pone.0332602
53. Sari CWM, Witdiawati W, Purnama D, Kurniawan T. Evaluation of diabetes patients about chronic disease management program in Bandung. Malaysian J Med Health Sci. 2022;18.
54. Asalde CAB, de Bonilla ORL, Lozada ICR, et al. Barriers to accessing quality health coverage and their association with medication adherence in patients with type 2 diabetes mellitus at a hospital in Peru. Pak J Med Health Sci. 2020;14(2):853–859.
55. Liu Y, Zupan NJ, Shiyanbola OO, et al. Factors influencing patient adherence with diabetic eye screening in rural communities: a qualitative study. PLoS One. 2018;13(11):1–14. doi:10.1371/journal.pone.0206742
56. Nopitasari A, Ghozali MT. Exploration of Self-management strategies for type 2 diabetes mellitus among patients in rural community health centers: a descriptive study. Res J Pharm Technol. 2024;17(12):5974–5980. doi:10.52711/0974-360X.2024.00906
57. Thylefors J, Annersten Gershater M, Mangrio E, Zdravkovic S. Intervention strategies for type 2 diabetes prevention in high-income countries targeting low socioeconomic groups: a scoping review. Front Public Health. 2025;13.
58. Kemenkes R. Pedoman dan Standar Etik Penelitian dan Pengembangan Kesehatan Nasional. Lembaga Penerbit Badan Penelitian dan Pengembangan Kesehatan Indonesia; 2021.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.