Back to Journals » Patient Preference and Adherence » Volume 17
Factors Influencing Patient and Caregiver Preferences for Antipsychotic Treatment of Schizophrenia in China: A Discrete Choice Experiment
Authors Zhang W, He S, Wilson L, Foix-Colonier A ![]() , Pacou M, Zhu Y, Zhu Y, Xue L, Wang Y, Li J, Liu Y
, Pacou M, Zhu Y, Zhu Y, Xue L, Wang Y, Li J, Liu Y ![]() , Cai J
, Cai J ![]()
Received 14 February 2023
Accepted for publication 17 May 2023
Published 13 June 2023 Volume 2023:17 Pages 1421—1430
DOI https://doi.org/10.2147/PPA.S403252
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Weibo Zhang,1,2,* Siyuan He,1,* Liam Wilson,3 Astrid Foix-Colonier,4 Maud Pacou,4 Youwei Zhu,1 Yi Zhu,1 Lili Xue,1 Yanfeng Wang,1 Junmei Li,1 Yanli Liu,1 Jun Cai1,2
1Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Mental Health Branch, China Hospital Development Institute, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 3Amaris Consulting, Shanghai, People’s Republic of China; 4Amaris Consulting, Paris, France
*These authors contributed equally to this work
Correspondence: Jun Cai, Shanghai Mental Health Center, Shanghai Jiao Tong University School of Medicine, 600 Wan Ping Nan Road, Shanghai, 200030, People’s Republic of China, Email [email protected]
Purpose: This study aimed to quantify the preferences of Chinese patients with schizophrenia and their caregivers for antipsychotic treatment.
Patients and Methods: Patients with schizophrenia (aged 18– 35) and their caregivers were recruited via six outpatient mental health clinics in Shanghai, People’s Republic of China. In a discrete choice experiment (DCE), participants chose between two hypothetical treatment scenarios that varied regarding the type of treatment, rate of hospitalization, severity of positive symptoms, treatment cost and rates of improvement in daily and social functioning. Data for each group were analyzed using the modelling approach that yielded the lower deviance information criterion. The relative importance score (RIS) for each treatment attribute was also determined.
Results: A total of 162 patients and 167 caregivers participated. Frequency of hospital admission was the most important treatment attribute for patients (average scaled RIS=27%), followed by mode and frequency of treatment administration (24%). Improvement in ability to carry out daily activities (8%) and improvement in social functioning (8%) were least important. Patients in full-time employment placed more importance on the frequency of hospital admission than unemployed patients (p< 0.01). Frequency of hospital admission was also the most important attribute for caregivers (RIS=33%), followed by improvement in positive symptoms (20%), while improvement in daily activities (7%) was the least important.
Conclusion: Patients with Schizophrenia in China prefer treatments that help reduce the number of times they are admitted to hospital, as do their caregivers. These results may bring insight for physicians and health authorities in China regarding the treatment characteristics that patients value the most.
Keywords: conjoint analysis, discrete choice experiment, schizophrenia, preference study, patients, caregivers
Introduction
Schizophrenia is a chronic, progressive behavioral and cognitive psychiatric disorder and a leading cause of disability worldwide.1 Symptoms are heterogenous and variable over time.2 Hallucinations, delusions, and poor social functioning have a detrimental impact on personal, vocational, and familial activities, while cognitive deficits affect all aspects of decision-making.1,3
Schizophrenia poses considerable clinical and economic burden to patients, caregivers, and society. The World Health Organization (WHO) estimates the direct costs of schizophrenia in Western countries to account for 1.6% to 2.6% of total healthcare expenditure; European studies estimate the cost of relapse over a 6–12-month period to range between $8665 to $18,676 (2015 USD).1 Estimates of global prevalence vary between 0.3 to 0.7%, while prevalence is 0.83% in China.1,4
The goal of long-term antipsychotic medication includes a reduction in psychotic and functional symptoms while minimizing treatment-induced adverse events (AEs).5 Side-effects contribute to the overall burden of illness despite improvements in treatment tolerability profiles. Current treatments have high rates of discontinuation, and several factors, including patient expectations, treatment benefit, and side-effects influence adherence.6 Poor adherence may increase hospitalization rates; in a large multicenter, observational study across China, relapse rates for non-adherent patients were 2.5 times higher than those of adherent patients.7
Long-acting injectable (LAI) medications aim to simplify dosing regimens and improve outcomes as an alternative to daily oral therapy.2 Administration varies from monthly to three-monthly.1 A study evaluating real-world effectiveness of oral and LAI treatments for schizophrenia in China demonstrated that patients treated with LAIs experienced a reduced rate of hospital readmissions in the year following discharge compared to patients treated with oral medication (60% and 64.6% respectively).8 Such reductions in hospitalization rates among patients treated with LAIs versus oral medication have also been demonstrated in other Asian and European studies.9–11
Although traditionally based on the physician’s perspective, there is increasing recognition that patient input into decision making has the potential to improve the effectiveness of healthcare interventions through better adoption, satisfaction and adherence.5,12 Conjoint analysis, or Discrete Choice Experiments (DCE), provides a systematic method to elicit trade-offs and quantify the relative importance of treatment attributes when patients select a therapy.1,5,6 In DCE, respondents choose between competing hypothetical scenarios, characterized by differences in (for example) symptom improvement, side effects and formulation.2 DCE can be a powerful tool for quantifying decision makers’ preferences for healthcare and its application has increased rapidly over the past decade.12
Different studies have demonstrated that patients with schizophrenia can complete conjoint analysis tasks in a meaningful way, base decisions on their own preferences and make trade-offs between treatment attributes.1,2,5,13 Although cognitive deficits can affect decision making, patients appeared capable of judging their own health status, performance, and treatment preferences.3 Previous research, conducted in Australia, Europe, and North America, has investigated the treatment preferences of patients with schizophrenia.1,2,5,13 However, to the authors knowledge, no conjoint analysis on the treatment preferences of patients with schizophrenia had been completed in China.
As such, we sought to conduct a DCE in China to quantify the preferences of patients with schizophrenia and their caregivers for antipsychotic therapy. The main study objective was to determine the antipsychotic parameters preferred by Chinese patients and caregivers, as well as the importance of the different treatment attributes.
Methods
Participants
Participants included patients diagnosed with schizophrenia and currently undergoing outpatient treatment, as well as people who care for patients with schizophrenia. The patients and caregivers were recruited from six mental health centers in Shanghai, PR China. Ethical approval for this study was granted by the Shanghai Mental Health Center Ethics Committee (2020–89). In line with the declaration of Helsinki, all participants in the study provided written informed consent to participate. Where possible, patients and caregivers were recruited in pairs, to allow an assessment of the concordance in their preferences for treatment. Patients were eligible for inclusion if they were aged 18 to 35, currently living in China, and had been receiving a stable dose of medication for at least the previous two months. Caregivers were required to be over 18 years old, currently caring for a person with schizophrenia, and living in China for inclusion in the study.
Using the sample size formula from de Bekker-Grobb et al, the minimum sample size required was 77 patients and 77 caregivers. However, based on the sample size of previously published DCEs and in order to produce robust results, we aimed to recruit 150 respondents for each of the patient and caregiver groups.14
Survey Design
The non-interventional cross-sectional pen and paper questionnaire was distributed by trained healthcare professionals at six mental health centers in Shanghai in January 2021. Included in the survey were a consent form, the DCE questionnaire, and demographic and clinical questions. The DCE evaluated the most critical qualities of schizophrenia antipsychotic treatment for Chinese patients and caregivers. In line with the ISPOR recommendations for conjoint analyses, a DCE questionnaire consisting of 13 choice sets was developed.15 Each choice set contained two hypothetical and unlabeled treatment options, defined by a select number of attributes, each with corresponding levels. A targeted literature review and expert opinion allowed the determination of the included treatment attributes and their levels that were appropriate to the local cultural and clinical context. Six attributes were included in the final DCE questionnaire: mode and frequency of treatment administration, frequency of hospital admission, improvement in positive symptoms, treatment cost, improvement in daily activities, and improvement in social activities (Table 1). All attributes consisted of three levels, except for treatment cost, which had four levels. Additional to the 13 choices sets, a “dominant” choice set was included to ensure the quality of participants’ responses. This choice set comprised intentionally imbalanced treatment qualities, with one treatment designated the “correct” answer. Based on participants’ preferences, the DCE quantified the utility of a given treatment element.
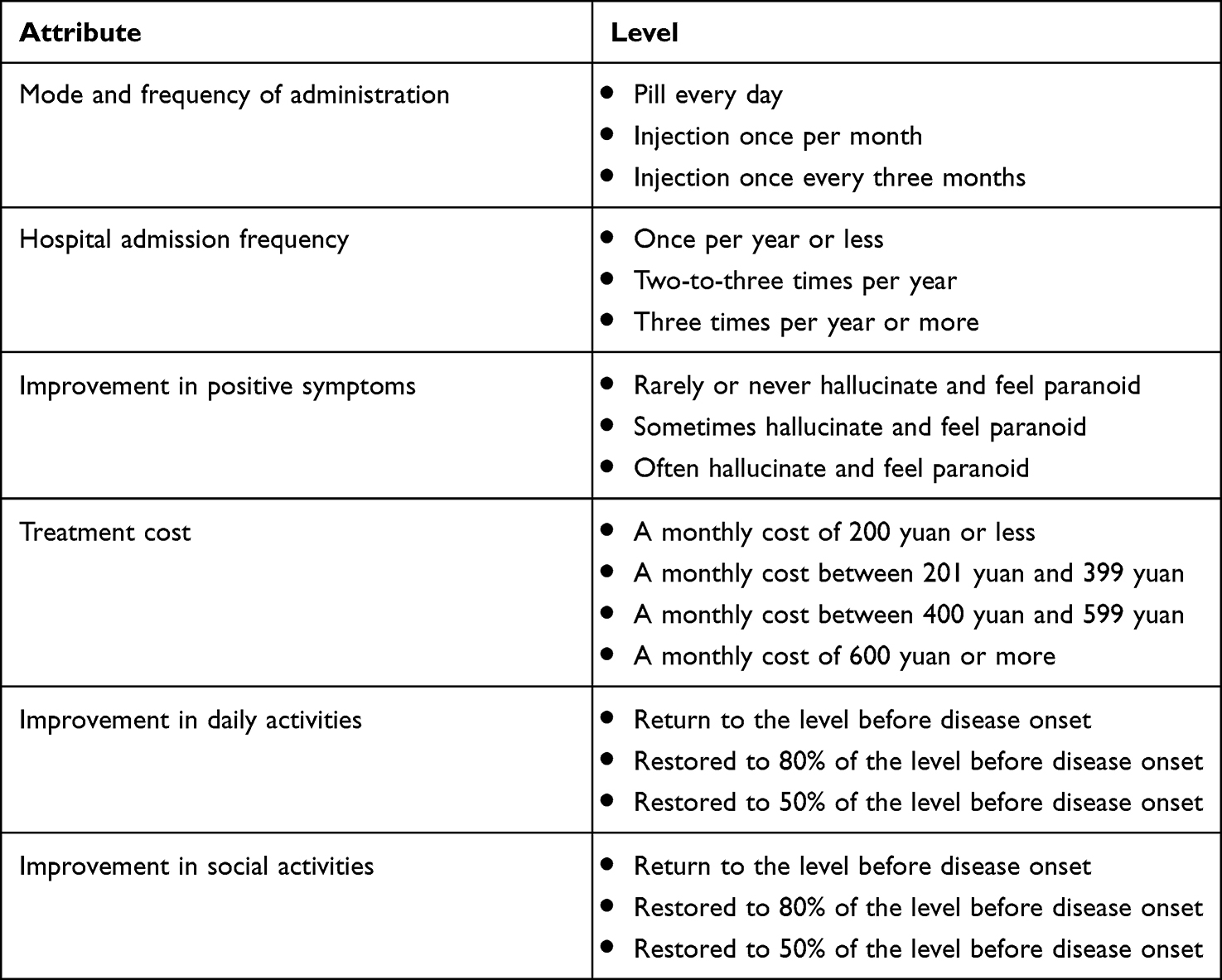 |
Table 1 Attributes and Levels Associated with Schizophrenia Treatment Included in DCE Choice Sets |
Immediately after completing the choice sets, participants completed a demographic survey. Patients were asked for their age, gender, height and weight, living situation, medical insurance status, employment situation, education level, time of and age at schizophrenia diagnosis, family income, and antipsychotic treatment experience. Caregivers were asked the same questions about both the patient they care for and themselves, and were also asked about their relationship with the patient in their care.
Statistical Analysis
Three approaches to modelling utility were used. To analyze the DCE results for the patients and caregivers, the model that yielded the lowest deviance information criterion (DIC) for each group was used. This resulted in the selection of a random parameter logit model and a hierarchical Bayes model for patients and caregivers, respectively. Additionally, the relative importance score (RIS), which expresses the overall weight of an attribute in the choices made by responders, was calculated for both groups. For each patient, the RIS of each attribute was calculated as the difference between the parameter estimate associated with the level of highest preference and the parameter estimate associated with the level of lowest preference. The RIS were then scaled to be expressed as a percentage between 0 and 100%.
The impact of clinical and demographic characteristics on the importance placed on each attribute by participants was explored through modeling the RIS for each attribute as a function of patient and caregiver traits. A univariate regression was conducted to select the covariates that had a greater statistically significant impact on the RIS. Specifically, covariates with a p-value lower than 0.2 were selected. Subsequently, a multivariate stepwise regression was performed using the selected covariates. The multivariate model selected for each attribute was based on whether the covariate significantly impacted the RIS, with a p-value threshold of 0.10. A positive coefficient indicates an increase in the RIS while a negative coefficient indicates a decrease. For variables with more than 20% missing values (ie family income), an imputation of missing values was performed by using the value of the corresponding participant from the patient-caregiver pair before using the variable in the RIS modelling.
Results
Patient and Caregiver Characteristics
From the mental health centers surveyed, a total of 162 patients and 167 caregivers provided informed consent to participate in the study. Among these participants, there were 155 patient-caregiver pairs. Most participants (99%) answered the dominant choice set correctly, indicating that patients and caregivers understood the task well and were attentive while completing the survey. Table 2 outlines the demographic and clinical details of the final sample. For the patients, the mean age was 30.6 years while the mean age at diagnosis of schizophrenia was 21.7 years. There was a relatively even gender distribution amongst patients with 49.4% identifying as female. Regarding treatment experience, 98.8% had previously been treated with an oral antipsychotic regimen while 8.6% had previously received LAIs. For the caregivers, the mean age was 58 years, with 51.5% identifying as female. All caregivers were related to the person in their care, and 96.4% were living with the person in their care. Within patient and caregiver pairs, the rate of concordance in responses to the DCE choice sets was 70% on average.
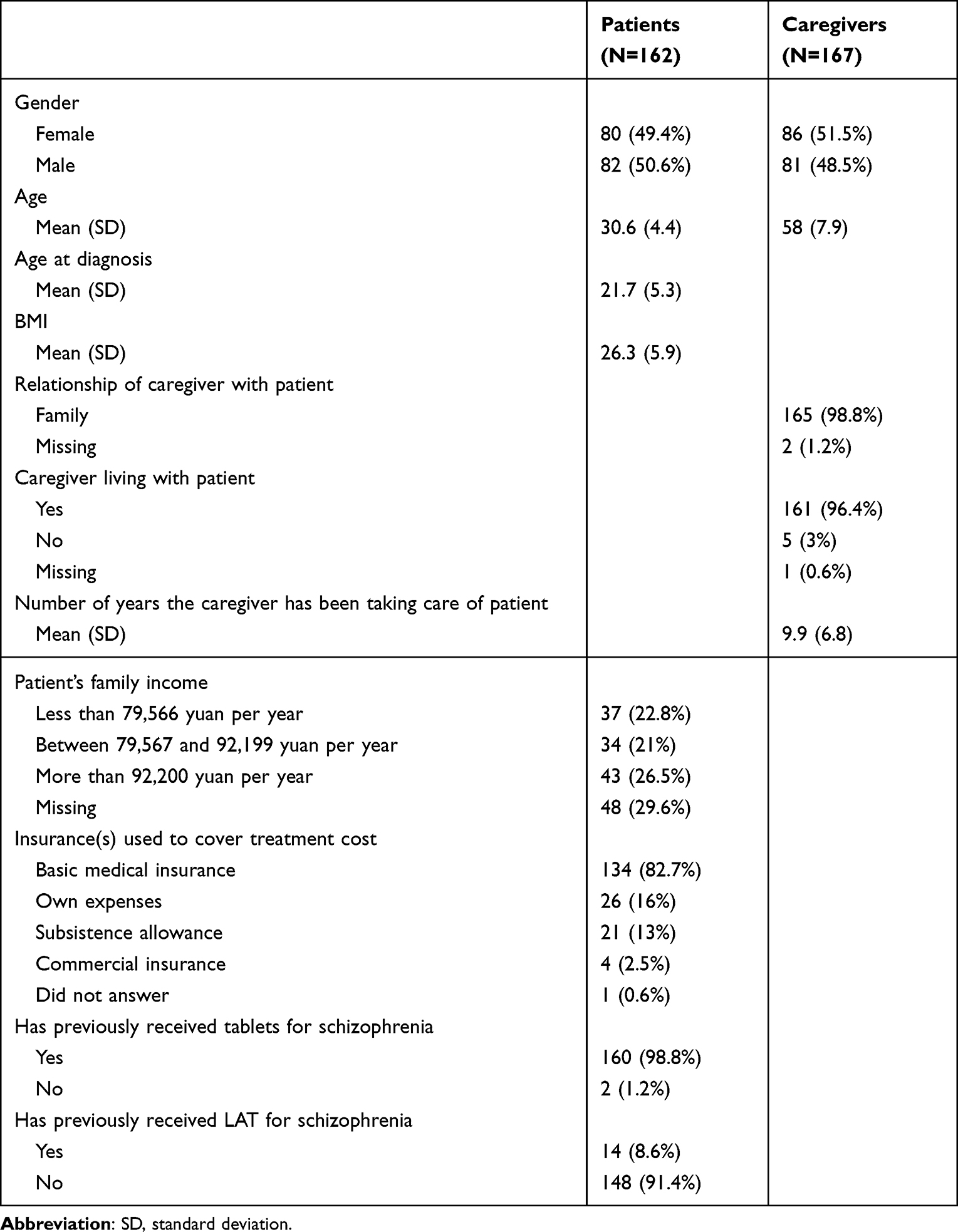 |
Table 2 Demographic Characteristics of Patients and Caregivers |
Relative Importance of Treatment Attributes
Statistical analyses of the 13 choice sets revealed that when selecting a treatment, frequency of hospital admission was the most important attribute for both patients and caregivers (Figure 1). That is, compared to all other attributes, participants valued frequency of hospital admission the most when deciding between treatment options in each choice set. Both groups preferred hospitalization once per year or less to more frequent hospitalization (Figure 2), with this attribute receiving a RIS of 27% and 33% for patients and caregivers, respectively. The average scaled RIS across patients and across caregivers are presented in Figure 1. The preference weights for patients and for caregivers are presented in Figure 2 and detailed in Table 3.
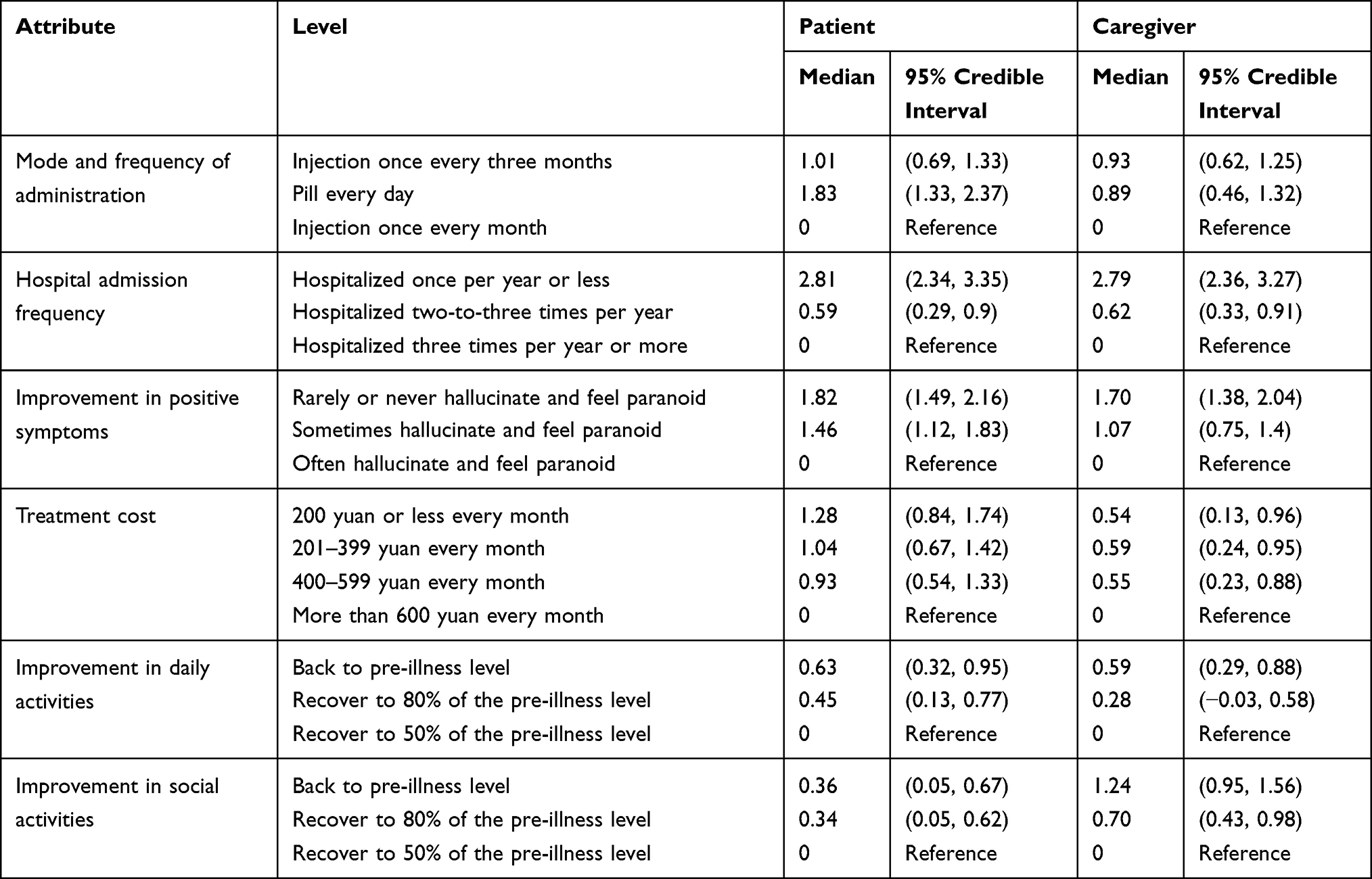 |
Table 3 Preference Weights for Patients and Caregivers |
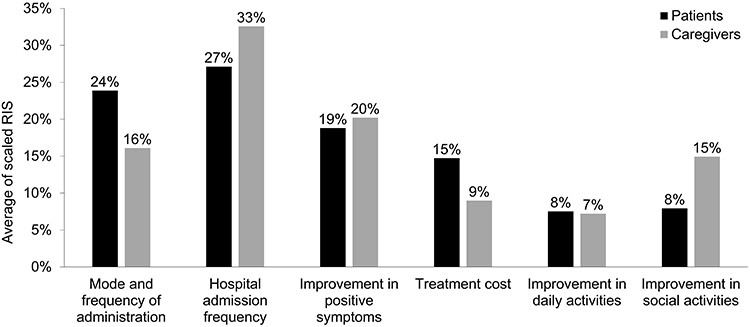 |
Figure 1 The average scaled Relative Importance Score (RIS) attributed to each treatment attribute by patients and caregivers. |
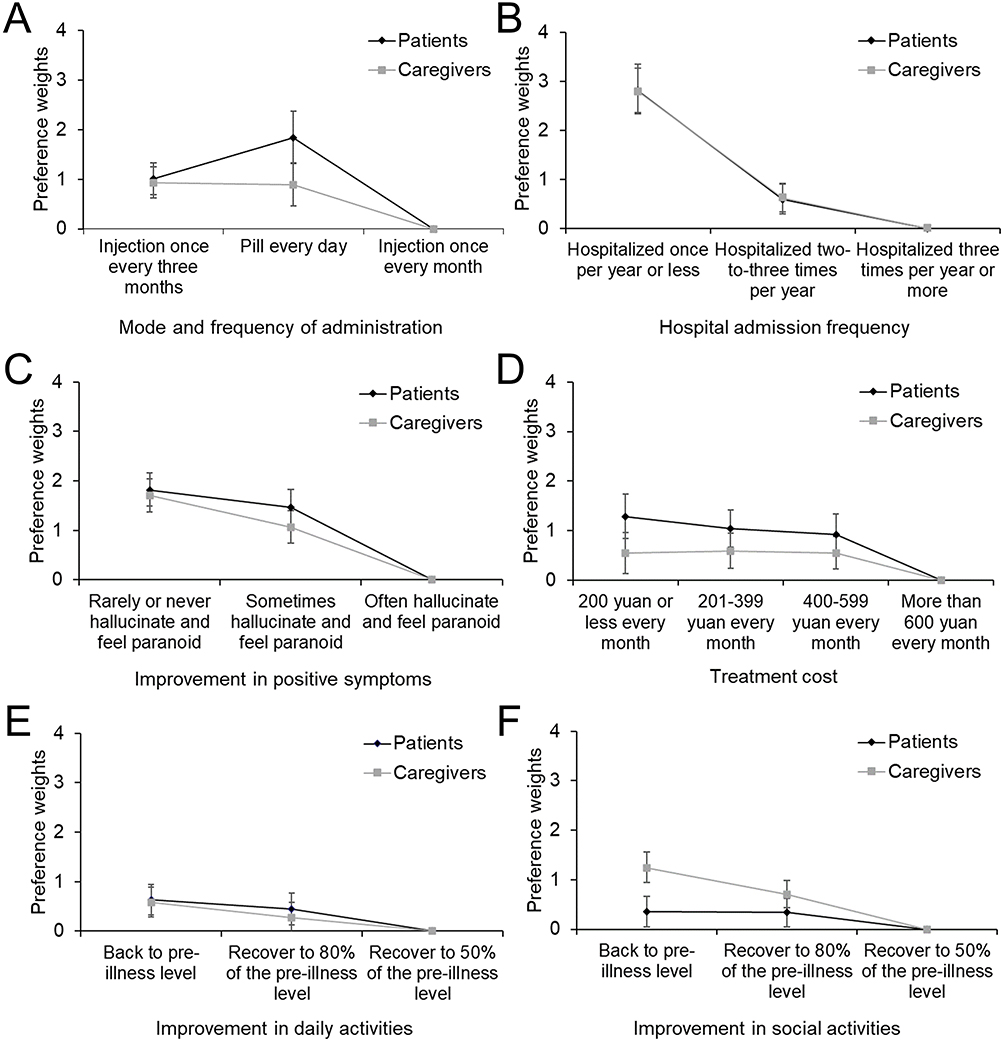 |
Figure 2 The preference weights for each of the six attributes and their corresponding levels. Each graph reflects the median preference weight and 95% credibility interval for the patient and caregivers with regard to each attribute: (A) Mode and frequency of administration; (B) Hospital admission frequency; (C) Improvement in positive symptoms; (D) Treatment cost; (E) Improvement in daily activities; (F) Improvement in social activities. |
Mode and frequency of treatment administration was the second most important attribute for patients (RIS=24%) and the third most important for caregivers (RIS=16%). Between levels, patients preferred a daily pill to injection, while trimonthly injections were preferred over monthly injections. For caregivers, there was no difference between preference for a daily pill or a trimonthly injection, but both were preferred over a monthly injection. For caregivers, the second most important attribute was improvement in positive symptoms (RIS=20%). While this was ranked third for patients (RIS=19%), they still placed nearly equal importance on this attribute when compared to caregivers. Across the board, both groups preferred less frequent experience of positive symptoms.
Between the groups, patients placed more importance on treatment costs (RIS=15%) than caregivers (RIS=9%). However, both groups preferred treatments that cost less than RMB 600 per month. Caregivers placed relatively greater importance on improvement in social activities (RIS=15%) compared to patients (RIS=8%). In this regard, caregivers most valued a return to the level of social activity that patients experienced before the onset of schizophrenia and preferred this compared to recovery to 80% of the pre-illness level of social activity. For patients, there was no difference between making a full recovery in social activities and recovering just 80% of their previous social functioning. Improvement in daily activities was the least important attribute for both caregivers (RIS=7%) and patients (RIS=8%).
RIS Modelling Results
The relative importance of frequency of hospital admission was impacted by patient employment status, with patients in full-time employment placing significantly more importance on this attribute compared to unemployed patients (p<0.01). Method of payment for medication also affected the importance of this attribute for both patients and caregivers. Patients who were self-financing their medication valued this attribute less than those using insurance (p=0.06). For caregivers, if the patient in their care was covered by basic medical insurance, regardless of whether they used it to cover treatment costs, less importance was placed on frequency of hospital admission (p=0.08, p=0.03). More importance was placed on this attribute if the patient did not use subsistence allowance to cover the cost of medication (p=0.01).
None of the recorded patient characteristics significantly impacted the importance that patients place on improvement in positive symptoms. However, among caregivers, there were traits that affected relative importance. Caregivers who did not live with the person in their care placed more importance on improvement in positive symptoms compared to those who did (p<0.01). The full modelling results can be found in Tables S1 to S12.
Discussion
In the present study, we used a DCE questionnaire to determine the qualities of schizophrenia antipsychotic treatment that are most valued by Chinese patients and their caregivers, in addition to how the relative importance of treatment attributes are impacted by patient and caregiver characteristics. To our knowledge, this is the first DCE to quantify preferences for schizophrenia treatment among patients and those who care for them in China. Furthermore, this study adds to the growing body of evidence indicating that patients with schizophrenia can meaningfully participate in DCE, with more than 99% of participants in this study answering the dominant choice set “correctly”.
Our study found that the most important attributes for patients and their caregivers when selecting a treatment were the rate of hospital admission, mode and frequency of treatment administration, and improvement in positive symptoms. These findings are broadly in line with the findings of previous research employing conjoint analysis to study the treatment preferences of patients with schizophrenia in countries other than China.1,2,16
Across the board, patients place great importance on reducing the burden of positive symptoms, while in general less frequent treatment administration is preferred. In the present study however, reduced hospitalizations were the main driver of treatment preferences. The characteristics of hospitalization for patients with schizophrenia in China and what this may represent for both patients and their caregivers should be explored in further research to aid in understanding this result.
Further differences in the approach to schizophrenia care in China compared to other countries may also be relevant in interpreting the results of the present study. For example, the current study highlighted that most patients with schizophrenia receive care from a relative (98.8%) and live with their caregiver (96.4%). This highly family-centric approach to schizophrenia care in China may explain the slight differences in preferences in our study compared to those from studies conducted in western countries and would be an interesting focus of future research.
Although both patients and caregivers most valued frequency of hospitalization when selecting treatment options, their preferences diverged with regard to other treatment characteristics. Patients placed more importance on mode and frequency of administration with a preference for daily oral treatments over monthly or trimonthly LAIs, which is consistent with the results of a study conducted in the UK.1 However, some other studies found that most patients would prefer LAIs over daily pills, with less frequent (trimonthly) injections preferred over monthly injections.2,5,16 Our own results may be explained by lower awareness of LAIs compared to oral drugs among patients (with just 8.6% of patients in our study having previous experience of LAIs), indicating a need for improved understanding of treatment options in China.
In the present study, all other attributes being equal, patients would be willing to trade off a more preferred mode and frequency of treatment administration in favor of the lowest hospital admission frequency. This was particularly the case for patients in full-time employment, who placed relatively more importance on this quality. Given that use of LAIs is directly associated with lower rates of rehospitalization,8,10,11 these results suggest that greater use of LAIs may be a future direction for schizophrenia treatment in China that is acceptable for patients.
The limitations of this study reflect those of many survey-based analyses, including information bias due to the fact participants provided the information, and the potential for varying interpretation of questions among participants. Additionally, many patients and caregivers did not fill in information related to their family income, and no information was collected on the proportion of cost that is borne by patients when they are covering medication costs out-of-pocket. As such, our analysis regarding the impact of financial considerations on treatment preferences is limited to some degree. Plus, although several baseline characteristics have been collected, some confounding factors might not have been included. It should also be noted that the current study focused on patients with a stable dose of antipsychotics, therefore it does not tackle the preferences of caregivers or patients not adherent to antipsychotic medication. Furthermore, this study could be subject to selection bias, as only patients and caregiver who consented to participate were included to the study, and the recruitment was restricted to patients and their caregivers living in Shanghai, a large, wealthy city in China. As such, further research would be required to determine whether the findings of this study can be generalized to patients living in less economically developed regions.
Further qualitative research should investigate the specific reasons that patients prefer oral medication over long-acting injections even though the latter have been associated with improved outcomes in terms of hospitalization.8–11 Such research could provide insight into how patient education or treatment options should be designed and delivered. Furthermore, to the authors’ knowledge, the degree of consistency between the results of DCE models and the actual treatment choices of patients has not been examined and could represent a valuable next step in future research for this field.
Patient preferences are an important component of treatment decisions and should be taken into account where possible by physicians, regulators, and other healthcare decision-makers. This study has demonstrated that patients with schizophrenia and their caregivers living in Shanghai, China, value treatments based on their effectiveness for reducing the rate of hospital admissions. Although patients expressed a strong preference for daily oral regimens, results indicated that this would be traded off for a less preferred mode and frequency of administration in favor of the lowest hospital admission frequency. This study has implications for our understanding of the factors that are important to those affected by schizophrenia when selecting a treatment and may bring valuable insight for physicians and health authorities in China.
Acknowledgments
The authors would like to thank the patients and caregivers who participated in this study for their valuable contribution. We are also very grateful to the following hospitals in Shanghai for their assistance with recruitment: the Mental Health Center of Minghang District, the Mental Health Center of Xuhui District, the Mental Health Center of Jing’an District, the Mental Health Center of Songjiang District and the Mental Health Center of Jiading District. We would additionally like to thank Claire Fischer and Riya Sivakumar for their support on the study. Weibo Zhang and Siyuan He are co-first authors for this study.
Funding
Data acquisition, research, and preparation of the manuscript were funded by the Health Industry Clinical Research Project of the Shanghai Municipal Health Commission (2020040362); Shanghai “New Star Medical Garden” Young Medical Talents Training Program; the Science and Technology Commission of Shanghai Municipality Research Project (19411950800); Youth Project of Shanghai Philosophy and Social Science Planning (2020ESH001), Shanghai Municipal People’s Government decision-making consultation research special subject of civil affairs (2022-Z-Q02) and Xian Janssen Pharmaceutical Ltd.
Disclosure
Astrid Foix Colonier is an employee of Amaris Consulting Ltd., a paid consultant to Xian Janssen Pharmaceutical Ltd. During the conduct of the study, Liam Wilson and Maud Pacou were paid employees of Amaris Consulting, paid consultants to Xian Janssen Pharmaceutical Ltd. The authors report no other conflicts of interest in this work.
References
1. Bridges JF, Beusterien K, Heres S, et al. Quantifying the treatment goals of people recently diagnosed with schizophrenia using best-worst scaling. Patient Prefer Adherence. 2018;12:63–70. doi:10.2147/PPA.S152870
2. Levitan B, Markowitz M, Mohamed AF, et al. Patients’ preferences related to benefits, risks, and formulations of schizophrenia treatment. Psychiatr Serv. 2015;66(7):719–726. doi:10.1176/appi.ps.201400188
3. Bridges JFP, Kinter ET, Schmeding A, Rudolph I, Mühlbacher A. Can patients diagnosed with schizophrenia complete choice-based conjoint analysis tasks? Patient. 2011;4(4):267–275. doi:10.2165/11589190-000000000-00000
4. Chan KY, Zhao FF, Meng S, et al. Prevalence of schizophrenia in China between 1990 and 2010. J Glob Health. 2015;5(1):10410. doi:10.7189/jogh.05.010410
5. Katz EG, Hauber B, Gopal S, et al. Physician and patient benefit-risk preferences from two randomized long-acting injectable antipsychotic trials. Patient Prefer Adherence. 2016;10:2127–2139. doi:10.2147/PPA.S114172
6. Achtyes E, Simmons A, Skabeev A, et al. Patient preferences concerning the efficacy and side-effect profile of schizophrenia medications: a survey of patients living with schizophrenia. BMC Psychiatry. 2018;18(1):292. doi:10.1186/s12888-018-1856-y
7. Xiao J, Mi W, Li L, Shi Y, Zhang H. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: results from an observational survey in the People’s Republic of China. Neuropsychiatr Dis Treat. 2015;11:1161–1167. doi:10.2147/NDT.S72367
8. Lin CH, Chen FC, Chan HY, Hsu CC. Time to rehospitalization in patients with schizophrenia receiving long-acting injectable antipsychotics or oral antipsychotics. Int J Neuropsychopharmacol. 2019;22(9):541–547. doi:10.1093/ijnp/pyz035
9. Kim HO, Seo GH, Lee BC. Real-world effectiveness of long-acting injections for reducing recurrent hospitalizations in patients with schizophrenia. Ann Gen Psychiatry. 2020;19. doi:10.1186/s12991-019-0254-2
10. Schreiner A, Svensson A, Wapenaar R, et al. Long-acting injectable risperidone and oral antipsychotics in patients with schizophrenia: results from a prospective, 1-year, non-interventional study (InORS). World J Biol Psychiatry. 2014;15(7):534–545. doi:10.3109/15622975.2014.902990
11. Tiihonen J, Haukka J, Taylor M, Haddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168(6):603–609. doi:10.1176/appi.ajp.2011.10081224
12. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health--a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
13. Zipursky RB, Cunningham CE, Stewart B, Rimas H, Cole E, Vaz SM. Characterizing outcome preferences in patients with psychotic disorders: a discrete choice conjoint experiment. Schizophr Res. 2017;185:107–113. doi:10.1016/j.schres.2016.12.018
14. de Bekker-Grob EW, Donkers B, Jonker MF, Stolk EA. Sample size requirements for discrete-choice experiments in healthcare: a practical guide. Patient. 2015;8(5):373–384. doi:10.1007/s40271-015-0118-z
15. Orme BK. Getting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research.
16. Blackwood C, Sanga P, Nuamah I, et al. Patients’ preference for long-acting injectable versus oral antipsychotics in schizophrenia: results from the patient-reported medication preference questionnaire. Patient Prefer Adherence. 2020;14:1093–1102. doi:10.2147/PPA.S251812
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding the Treatment Preferences of People Living with Schizophrenia in Australia; A Patient Value Mapping Study
Fifer S, Keen B, Newton R, Puig A, McGeachie M
Patient Preference and Adherence 2022, 16:1687-1701
Published Date: 19 July 2022
Understanding Treatment Preferences Among People Living with HIV in Australia: A Discrete Choice Experiment
Fifer S, Kularatne T, Tan M, Drummond F, Rule J
Patient Preference and Adherence 2023, 17:1825-1843
Published Date: 26 July 2023