Back to Journals » Patient Preference and Adherence » Volume 17
Factors Influencing Participation in Shared Decision-Making Among Patients with Glaucoma in China: A Cross-Sectional Study
Authors Sun Y ![]() , Zhou W, Zuo S, Chen C, Zhang Q, Chen Y
, Zhou W, Zuo S, Chen C, Zhang Q, Chen Y ![]()
Received 6 March 2023
Accepted for publication 3 May 2023
Published 16 May 2023 Volume 2023:17 Pages 1261—1270
DOI https://doi.org/10.2147/PPA.S411274
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Yiwen Sun,1 Wenzhe Zhou,2 Shushu Zuo,1 Chen Chen,1 Qiqi Zhang,1 Yanyan Chen3
1School of Ophthalmology and Optometry, Biomedical Engineering, Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China; 2Glaucoma Clinical Center, the Eye Hospital of Wenzhou Medical University, National Clinical Research Center for Ocular Diseases, Wenzhou, Zhejiang, People’s Republic of China; 3Nursing Department, the Eye Hospital of Wenzhou Medical University, National Clinical Research Center for Ocular Diseases, Wenzhou, Zhejiang, People’s Republic of China
Correspondence: Yanyan Chen, The Eye Hospital of Wenzhou Medical University, National Clinical Research Center for Ocular Diseases, No. 270, West College Road, Wenzhou City, Zhejiang Province, People’s Republic of China, Tel +86 13858855689, Email [email protected]
Purpose: To explore the level of participation in shared decision-making by patients with glaucoma and identify influencing factors, to subsequently provide references to promote shared decision-making in ophthalmology, and achieve patient-centered care.
Patients and Methods: A questionnaire was completed by 148 patients with glaucoma who had been admitted to a specialized ophthalmic hospital in China, between October 2021 and January 2022. The participants’ responses to the nine-item Shared Decision-Making Questionnaire (SDM-Q-9) and a general information survey were analyzed to determine their level of participation in shared decision-making and influencing factors. Multiple linear regression was used to identify factors that influence shared decision-making at the time of clinical practice.
Results: The mean score of SDM-Q-9 was 71.73± 21.27 (n=140). Multiple linear regression analysis showed that patients with negative attitudes towards participation in decision-making (P=0.023) and those who had rural insurance (P=0.017) had significantly lower SDM-Q-9 scores than those with positive attitudes and those with medical insurance. Patients who were more satisfied with their medical service had higher SDM-Q-9 scores (P< 0.05).
Conclusion: Patients with glaucoma presented a high level of shared decision-making. Patients’ attitudes towards participating in decision-making, the payment method of medical expenses, and the level of satisfaction with medical services are factors that influence their level of participation in shared decision-making.
Keywords: glaucoma, shared decision-making, patient participation, influencing factor
Introduction
As society and medicine have continued to undergo extensive development over the years, patients’ rights of autonomy and participation in medical decision-making have improved. In China, patient centered care and shared decision-making (SDM) now align with the nation’s practical needs. SDM refers to the process whereby clinicians inform patients of the advantages and disadvantages of medical treatments as determined by evidence-based research, thus enabling patients to make reasonable and personalized medical decisions that complement their personal values and preferences.1,2 Researches have indicated that SDM can enhance patients’ medical cognitive level,3,4 relieve decisional conflict, and minimize anxiety and depression.5,6 Clinicians also benefit, as the explicit communication and collaboration with their patients facilitate the establishment of a trusting relationship, which can promote treatment adherence and satisfaction with medical decisions.7 The China Hospital Association encourages patients for patient safety.8 Medical staff can help patients build health awareness, improve health literacy and participation in medical decision-making by providing relevant education and training and various ways to participate in the medical care process.
Glaucoma is the leading causes of irreversible blindness in the world.9 The damage it causes to the optic nerve results in serious degeneration of visual health, and as a chronic eye disease with a low cure rate and high blindness rate, it requires lifelong treatment. As diagnostic and treatment technologies have advanced, a more diversified range of treatment options have become available to patients with glaucoma.10 However, issues such as the uncertainty of disease occurrence, development, and prognosis, as well as the risk and benefit analysis of various treatments, and the diversity of patient values culminate in a complicated and challenging process of decision-making for patients with glaucoma.11 When patients are faced with two or more equally effective options, with the advantages and disadvantages of such options related to their values and personal preferences, SDM becomes especially important.
Most previous studies on SDM have focused on cancer, cardiovascular disease, and advanced kidney disease.12–14 Very few studies have targeted the development of decision aids in glaucoma,15 and there is a distinct lack of research covering the status of SDM in glaucoma management. In addition, factors that influence the clinical application of SDM in glaucoma have not yet been studied. Therefore, the main purpose of this study is to understand the current implementation status and deficiencies in the implementation process of SDM in glaucoma, before investigating appropriate ways to apply SDM to clinical practice by determining influencing factors.
Patients and Methods
Participant
This study was conducted in accordance with the Declaration of Helsinki. After obtaining ethical approval from the ethics committee of the Eye Hospital of Wenzhou Medical University (Ethical approval number: 2020-180-K-163-01), data were collected from the glaucoma outpatient and inpatient departments of the hospital between October 2021 and January 2022.
Overall, 148 patients were enrolled in this study. Inclusion criteria included Chinese-speaking patients, aged 18 and older, able to provide informed consent, conforming to the diagnostic criteria of glaucoma in the Chinese Glaucoma Guidelines (2020),16 and voluntary participation. Exclusion criteria included altered mental status or suffering from other serious physical diseases or cognitive, hearing, or language disorders.
Measurements
After providing informed consent to participate in the study, all participants completed a general information questionnaire and SDM-Q-9. The general information questionnaire included demographic characteristics such as gender, age, marital status, educational level, place of residence, payment method of medical expenses, and economic burden; in addition, information regarding the clinical characteristics was obtained, including diagnosis type, visual acuity, intraocular pressure, course of disease, and treatment experience. Participants were also asked about their willingness and attitude towards participating in decision-making and their level of satisfaction with previous medical services.
The SDM-Q-9 was used to determine the involvement of patients in SDM during diagnosis and treatment of glaucoma. The questionnaire was revised by Kriston et al17 in 2010 based on the SDM-Q18 and was later sinicized by Luo et al19 in 2019. The questionnaire is a single dimension that comprises nine specific items, each of which is scored from 0 (“completely disagree”) to 5 (“completely agree”) on a 6-point Likert-scale. Following completion of the questionnaire by participants, the scores of each item were added together to attain a total score between 0 and 45. This total score was multiplied by 20/9 to obtain a standardized score of 0 to 100. A higher score indicates a higher level of SDM participation during disease diagnosis and treatment. Cronbach’s alpha coefficient of the Chinese questionnaire revised by Luo et al is 0.945,19 and the correlation coefficient between each item and the total score of the questionnaire is 0.790~0.879, showing a high degree of internal consistency.
Data Collection
The questionnaires were completed on a one-to-one basis with the researcher, who used a standard and unified language to explain the purpose of the survey and the contents of the questionnaire to the participants and their families. Before the questionnaire, the researcher identified herself to the patients as a third party, not involved in specific treatment and care, and informed them that participation in the survey would not affect their subsequent treatment. In the case of a participant having poor vision or dyslexia, the researcher would verbally state each question and complete the corresponding answers based on the oral responses given by the participant. All questionnaires were collected immediately after completion to be checked for missing values. Questionnaires with contradictory answers to the items were excluded. The questionnaire data were then input by two other researchers and a consistency test was conducted to ensure the accuracy of the data.
Statistical Analysis
All statistical analyses were performed with IBM SPSS Statistics, version 26.0. Continuous variables of normal distribution were presented as the mean and standard deviation, while categorical variables were presented as frequencies and percentages. To compare the differences in patient agreement with each item of SDM-Q-9, the items were ranked based on the mean of the raw scores. Independent 2-samples t-test and one-way analysis of variance (ANOVA) were performed to compare differences in the participation levels in SDM among participants with varying characteristics. Multiple linear regression analysis was conducted to identify the factors influencing patients’ participation in SDM, using the statistically significant variables in the univariate analysis (P<0.05) as the independent variables and the SDM-Q-9 standard scores as the dependent variables. The independent variables were input into the multiple linear regression model by way of “enter”. The variance inflation factor (VIF) of less than 5 for each independent variable was considered acceptable. The level of significance was set at 0.05.
Results
Participant Characteristics
Whilst 148 patients completed the questionnaire, eight questionnaires were deemed invalid due to contradictory answers, and therefore, were excluded. A total of 140 valid questionnaires were subsequently analyzed, resulting in a recovery efficiency of 94.59%. The demographic and clinical disease characteristics of the 140 subjects are displayed in Table 1.
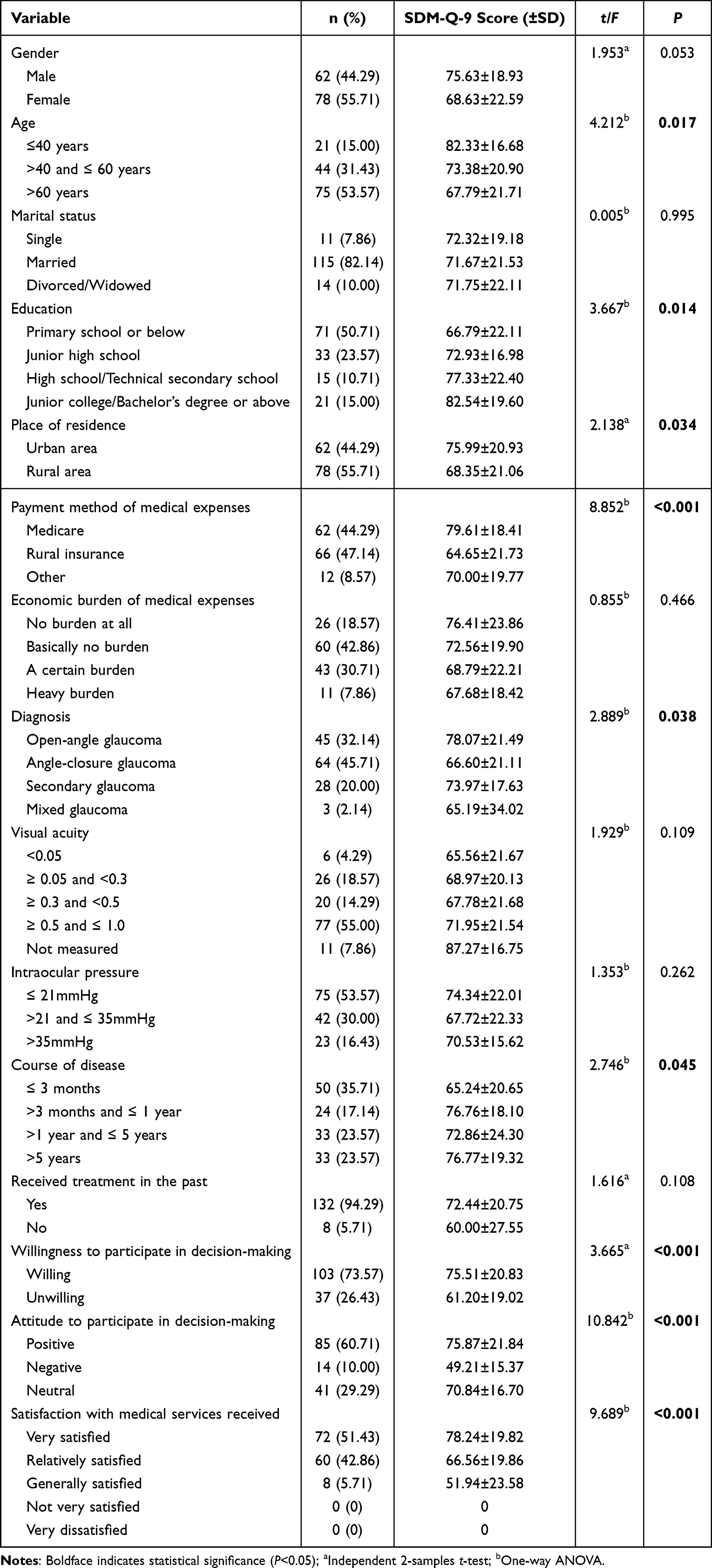 |
Table 1 General Data and Univariate Analysis of the Level of Participation in Shared Decision-Making of Patients with Glaucoma (n=140) |
SDM-Q-9 Scores
The mean (±SD) score of the SDM-Q-9 responses was (71.73±21.27) (standardized total score ranged from 0 to 100). Among the questionnaire items, the ninth item “My doctor and I reached an agreement on how to proceed” (4.18±0.74) (item score ranged from 0 to 5), the first item “My doctor made clear that a decision needs to be made” (4.16±0.96), and the fifth item “My doctor helped me understand all the information” (4.12±0.84) were the top three scoring items. The lower scoring items were the second item “My doctor wanted to know exactly how I want to be involved in making the decision” (2.52±1.47) and the sixth item “My doctor asked me which treatment option I prefer” (3.07±1.74). These findings are presented in Table 2.
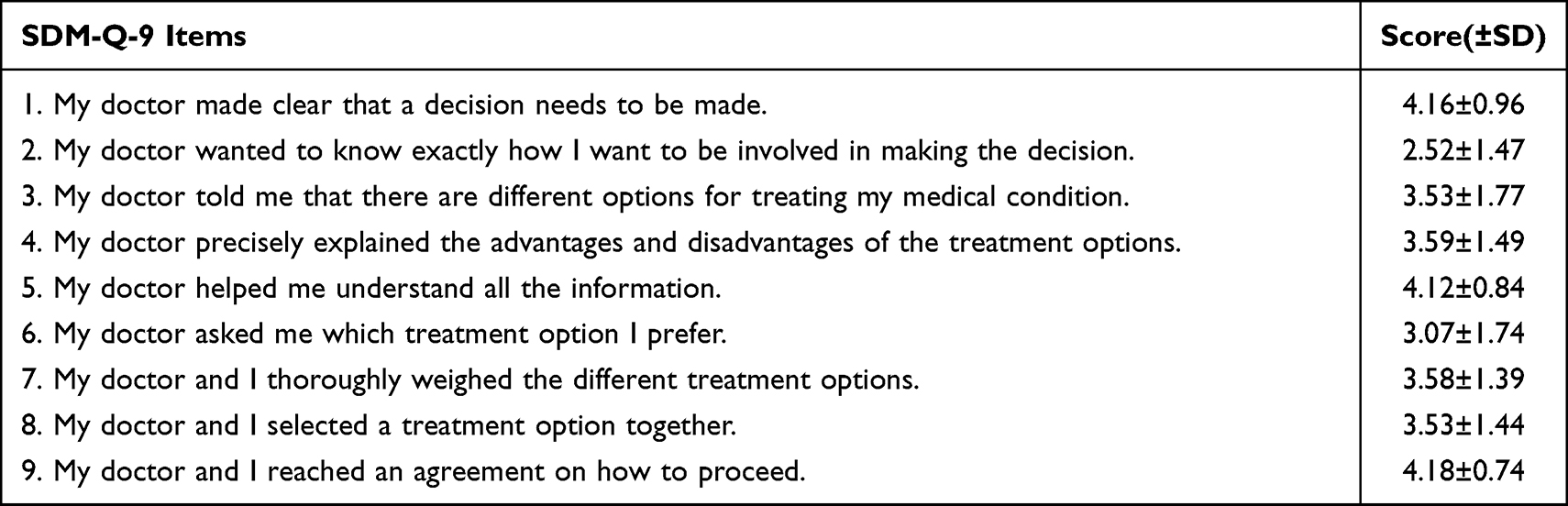 |
Table 2 Score of Each Item in Nine-Item Shared Decision-Making Questionnaire |
Factors Influencing the Level of Participation in Shared Decision-Making
Univariate analysis found that there were differences in SDM-Q-9 scores among patients with different age groups (P=0.017), educational level (P=0.014), residence (P=0.034), payment method of medical expenses (P<0.001), disease diagnosis (P=0.038), course of disease (P=0.045), willingness to participate in decision-making (P<0.001), attitude to participate in decision-making (P<0.001), and satisfaction of medical services (P<0.001) (Table 1). The multiple linear regression with the above factors as independent variables showed that participants’ attitude towards participating in decision-making, their payment method of medical expenses, and their level of satisfaction with the medical services received were influencing factors of their extent of participation in SDM (P<0.05) (Table 3). In particular, participants with a negative attitude towards participation had a lower level of participation in SDM than those with a positive attitude (P=0.023). Meanwhile, participants with rural insurance had lower participation than participants with medical insurance (P=0.017). In addition, it was found that participants who were relatively (P=0.007) or generally (P=0.020) satisfied with their medical services reported a lower level of SDM than those who were very satisfied. The final model significantly accounted for 22.5% of the variance of the SDM-Q-9 score (F=3.122, P<0.001).
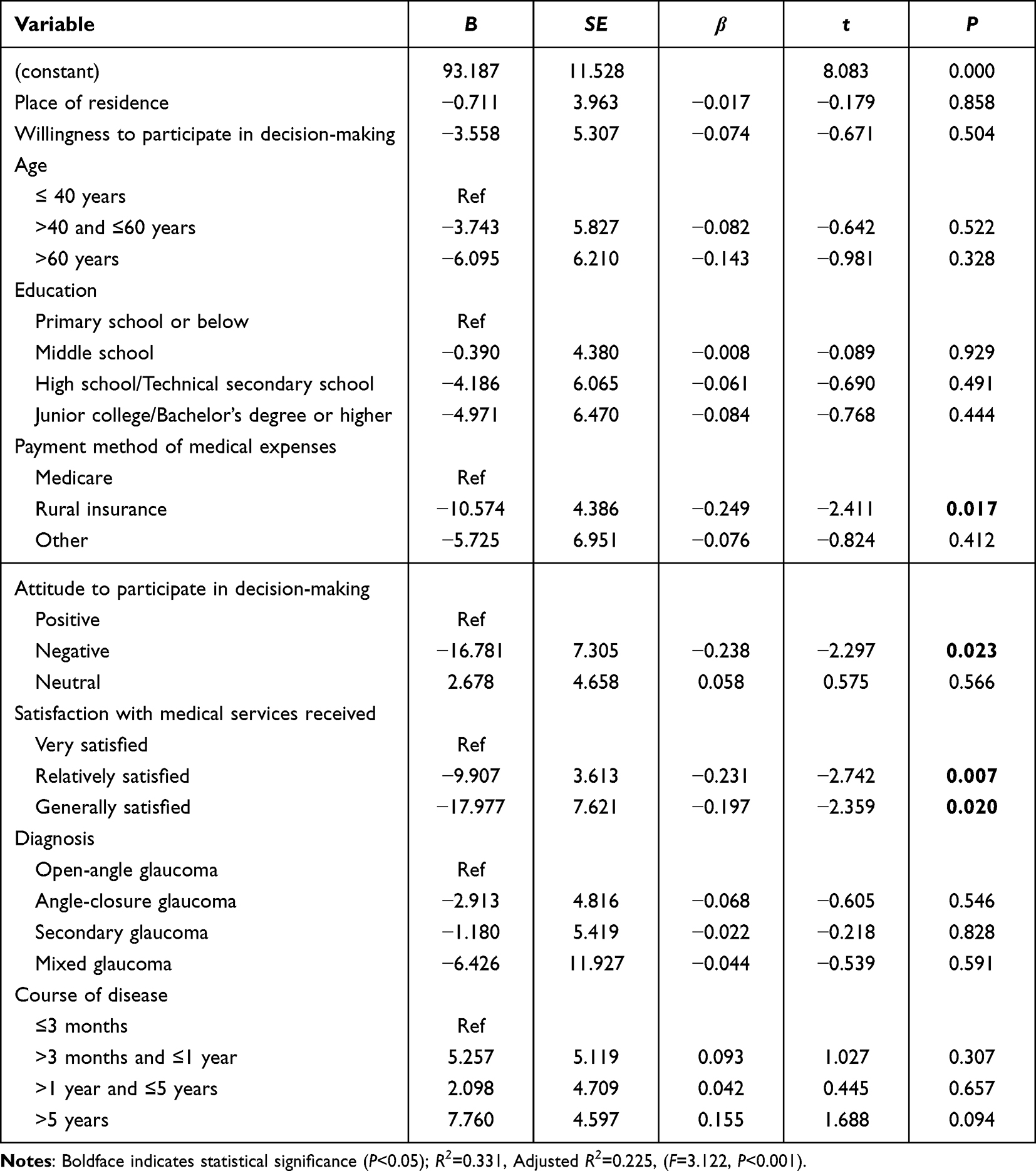 |
Table 3 Multiple Linear Regression Analysis of Factors That Influence the Level of Participation in Shared Decision-Making of Patients with Glaucoma (n=140) |
Discussion
SDM involves collaborative efforts between medical staff and patients, whereby the clinical experiences of the medical staff are combined with the patients’ preferences to decide on a treatment option that is agreeable for both parties. In this study, the patients with glaucoma self-reported high levels of SDM (71.73±21.27). Recent studies investigating the participation of other patient populations in decision-making found similar results.20–22 For example, a study involving 372 urological patients also used the SDM-Q-9 and produced a mean score of 77.8±20.6, with 72.84% of the participants showing a high level of involvement in the SDM process (total score of SDM-Q-9>66). However, other studies have generated conflicting results as the participation level of patients in SDM was established as low;14,23 these contrasting outcomes could be due to differences in the decisional capacity of the selected subjects or due to varying decision topics.
Differences were found between the scores of each item in the questionnaire, each of which relates to a different aspect of the SDM process. The first, fifth, and ninth items presented high scores, indicating that the participants considered the medical staff to be relatively adequate in providing them information, helping them to understand the information, and reaching a consensus with them to form the final decision. This is promising, as previous studies have shown that effective communication between doctors and patients, as well as clear information sharing, can improve the level of SDM.14,24 To build on this, it may be necessary for medical staff to actively explore patients’ individual needs for medical information and focus on the effectiveness of information delivery to enhance the patient experience of SDM participation. In contrast, the second, sixth, and eighth items had low scores, which related to the level of patient involvement and the preferences involved in decision-making. These are critical to the success of SDM. The low scores imply that the participants felt that not all medical staff had fully considered and identified their preferences for involvement in decision-making, nor had they actively invited patients to share their opinions. For many of the participants, their level of involvement in decision-making did not align with their personal preferences. This is consistent with the findings of Fu et al and Hahlweg et al.25,26 Clarifying patients’ decision-making preferences can help medical staff support patients in the way they want.14 A one-way information exchange can occur when there is an imbalance between the content of the information provided by doctors and the information obtained from patients. However, consensus also can be reached in decision-making when patients have more confidence in the knowledge, experience, and advice given by their doctors.7,27 Additionally, previous studies have shown that doctors do not necessarily acknowledge or recognize the specific needs of patients. Doctors tend to focus on the pros and cons of disease treatments, while patients focus more on their own social role, economic status, and other personal factors.28 Therefore, identifying each patient’s decision-making preferences and actively seeking their personal opinions on potential medical plans is important to the implementation of SDM. These approaches may facilitate the development of personalized diagnosis and treatment plans that are consistent with patient values, and achieve a transformation from passive informed consent by patients to equal and collaborative patient-centred SDM.20
In this study, multiple linear regression analysis found that patients’ attitudes towards participating in decision-making, their payment method of medical expenses, and satisfaction with medical services were factors that influenced patients’ level of SDM participation. Patients’ attitudes may affect their behavior to participate in decision-making. The majority of the participants in this study (73.57%) wanted to discuss their condition and treatment options with clinicians, and 60.71% of the participants stated they were positively involved in decision-making. Similarly, a study by Cheng et al found that 71.93% of patients with a heart valve replacement wanted to actively contribute to their treatment decisions.29 Patients who are actively involved in decision-making will communicate with medical staff, obtain relevant information and express their opinions, thus helping them be more involved in their treatment decisions.21 However, some of the participants in this study had a negative attitude towards participating in decision-making. These participants had a low level of participation in SDM. During the conversations, some of them volunteered that because they were unable to understand complex medical information accurately, they worried that participating in decision-making would affect the quality of treatment or that they would be held responsible for treatment failure. There was a belief that the doctor’s decision was absolutely correct, therefore, these patients wanted their doctor to make the decisions pertaining to their medical care, rather than making these choices themselves. In addition, patients also mentioned the difficulty of requesting help to fully understand medical information due to the short duration of the clinical consultation. Similar findings to the above have been found in other study.30 Decision aids may be able to improve patients’ medical knowledge, help weigh the pros and cons of different treatment options and improve the quality of decision making.4 Therefore, medical staff could consider using simple language or providing decision aids to help patients better understand complex medical information, while increasing the time or frequency of communication with patients whenever possible to enhance their enthusiasm for participating in SDM.31
The method of medical expenses payment is an influencing factor of the level of participation in SDM. Glaucoma is an eye disease that requires lifelong treatment, and the medical costs it incurs and what the patient can afford need to be taken into account when making a treatment plan. Patients with rural insurance are reimbursed at a lower rate than those with medicare. Therefore, these patients with rural insurance may have a greater financial burden. Although financial burden is not associated with SDM in this study, other study has shown that the burden may influence patients’ treatment options, as most patients in this circumstance will firstly consider their ability to afford the medical costs before considering the effectiveness and safety of the treatment options.32 Resultantly, these patients are more likely to choose more conservative and lower-cost treatments, and have mostly passive roles in decision-making.32 In addition, heavy financial burdens due to medical expenses make patients more prone to feelings of anxiety and helplessness, which further hinders their effective participation in SDM.33 In contrast, patients with a higher insurance reimbursement ratio experience less financial pressure due to medical expenses and experience greater access to medical services.34 These patients will focus on their quality of life when considering treatment options, and will actively express their demands as part of the decision-making process.34 Therefore, It is hoped that medical staff could pay attention to the method of medical expenses payment of patients during SDM and provide them with the most suitable medical plan for their situation. It is notable that this finding was derived in the context of China’s socio-economic system and therefore its extrapolation may be limited.
In our study, 51.43% of the participants were very satisfaction with the medical services they had received. Multiple linear regression analysis suggest that patients who were more satisfied with medical services had higher levels of SDM. Given the nature of this cross-sectional analysis, this study did not specifically explore the causal relationship between the level of participation in SDM and medical service satisfaction. However, previous study has also found that higher medical care satisfaction is significantly associated with higher levels of SDM.14 The possible explanation is that the technical level and service attitude of the medical staff affect the patients’ satisfaction with medical services;35 patients will have greater trust in the medical staff when they are highly professional and experienced, present a capable level of technical ability, convey a positive attitude, and communicate well;36 from this, patients will be more enthusiastic and comfortable to discuss their condition and will be more willing to express their needs and concerns with medical staff.37,38 It may suggest that solid technical skills and good communication skills of medical staff can improve patients’ satisfaction with medical services, thus promote the implementation of SDM. Further research is needed to determine what increases patients’ satisfaction with medical services and how medical services satisfaction relates to SDM.
This study demonstrates the level of involvement of glaucoma patients in SDM and explores the factors that influence SDM, which has implications for the application of SDM to clinical practice. Although the findings of this study are of great interest, certain limitations have been acknowledged. Firstly, this work is based on the application of SDM from the perspective of patients. Yet, to complete a more comprehensive evaluation of SDM in ophthalmology, the other parties need to be considered; this could be achieved in future studies through the use of the SDM-Q-Doc scale39 aimed at physicians, as well as the OPTION scale40 and RPAD scale41 for third parties. Secondly, the level of SDM changes in accordance with changes in the clinical practice environment, but as this was a single-centre study, the conclusions drawn may not be directly generalisable to other clinical settings. Therefore, a multicentre, large-sample survey study should be followed up in future to determine whether these findings are applicable to other contexts.
Conclusion
This study found that patients with glaucoma experienced a high level of SDM. Patients’ attitudes towards participating in decision-making, the payment method of medical expenses, and the level of satisfaction with medical services may be factors that influence the level of participation in SDM. These need to be brought to the attention of medical staff to promote the application of SDM in clinical practice.
Abbreviations
SDM-Q-9, the nine-item Shared Decision-Making Questionnaire; SDM, Shared Decision-Making.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We are grateful to the hospital and patients for their support and cooperation in this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Basic Scientific Research Projects of Wenzhou [grant number Y20220155].
Disclosure
None of the authors declared a conflict of interest.
References
1. Charles C, Gafni A, Whelan T. Shared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango). Soc Sci Med. 1997;44(5):681–692. doi:10.1016/s0277-9536(96)00221-3
2. Spatz ES, Krumholz HM, Moulton BW. Prime Time for Shared Decision Making. JAMA. 2017;317(13):1309–1310. doi:10.1001/jama.2017.0616
3. Austin C, Mohottige D, Sudore R, Smith A, Hanson L. Tools to promote shared decision making in serious illness: a systematic review. JAMA Intern Med. 2015;175(7):1213–1221. doi:10.1001/jamainternmed.2015.1679
4. Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017. doi:10.1002/14651858.CD001431.pub5
5. Schott SL, Berkowitz J, Dodge SE, et al. Personalized, electronic health record-integrated decision aid for stroke prevention in atrial fibrillation: a small cluster randomized trial and qualitative analysis of efficacy and acceptability. Circ Cardiovasc Qual Outcomes. 2021;14(6):e007329. doi:10.1161/CIRCOUTCOMES.120.007329
6. Korteland NM, Ahmed Y, Koolbergen DR, et al. Does the use of a decision aid improve decision making in prosthetic heart valve selection? A multicenter randomized trial. Circ Cardiovasc Qual Outcomes. 2017;10(2):e003178. doi:10.1161/circoutcomes.116.003178
7. Paduca A, Arnaut O, Beschieru E, Lundmark PO, Bruenech JR. Shared decision making and patients satisfaction with strabismus care-a pilot study. BMC Med Inform Decis Mak. 2021;21(1):109. doi:10.1186/s12911-021-01469-y
8. Chinese Hospital Association. 中国医院协会患者安全目标(2019版) [Patient Safety Objectives of the Chinese Hospital Association (2019)]. Chin Health. 2019;2019:57–58. Chinese.
9. Tham YC, Li X, Wong TY, Quigley HA, Aung T, Cheng CY. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
10. Stein JD, Khawaja AP, Weizer JS. Glaucoma in adults-screening, diagnosis, and management: a review. JAMA. 2021;325(2):164–174. doi:10.1001/jama.2020.21899
11. Bhartiya S. Patient centricity and the ethics of glaucoma care. J Curr Glaucoma Pract. 2020;14(2):68–71. doi:10.5005/jp-journals-10078-1281
12. Kunneman M, Branda ME, Hargraves IG, et al. Assessment of shared decision-making for stroke prevention in patients with atrial fibrillation: a randomized clinical trial. JAMA Intern Med. 2020;180(9):1215–1224. doi:10.1001/jamainternmed.2020.2908
13. Nishi S, Lowenstein LM, Mendoza TR, et al. Shared decision-making for lung cancer screening: how well are we “sharing”? Chest. 2021;160(1):330–340. doi:10.1016/j.chest.2021.01.041
14. Frazier R, Levine S, Porteny T, et al. Shared decision making among older adults with advanced CKD. Am J Kidney Dis. 2022;80(5):599–609. doi:10.1053/j.ajkd.2022.02.017
15. Shum J, Lam W, Choy B, Chan J, Ho W, Lai J. Development and pilot-testing of patient decision aid for use among Chinese patients with primary open-angle glaucoma. BMJ Open Ophthalmol. 2017;2(1):e000100. doi:10.1136/bmjophth-2017-000100
16. Glaucoma group of ophthalmologist branch of Chinese Medical Association, glaucoma group of ophthalmologist branch of Chinese Medical Association. 中国青光眼指南(2020年)[China glaucoma guidelines (2020)]. Chin J Ophthalmol. 2020;56:573–586. Chinese. doi:10.3760/cma.j.cn112142-20200313-00182
17. Kriston L, Scholl I, Holzel L, Simon D, Loh A, Harter M. The 9-item Shared Decision Making Questionnaire (SDM-Q-9). Development and psychometric properties in a primary care sample. Patient Educ Couns. 2010;80(1):94–99. doi:10.1016/j.pec.2009.09.034
18. Simon D, Schorr G, Wirtz M, et al. Development and first validation of the shared decision-making questionnaire (SDM-Q). Patient Educ Couns. 2006;63(3):319–327. doi:10.1016/j.pec.2006.04.012
19. Luo BH, Xiao SY. 中文版医患共同决策问卷患者版的信效度 [Reliability and validity for Chinese version of the 9-item Shared Decision Making Questionnaire]. J Cent South Univ. 2019;44:823–829. Chinese. doi:10.11817/j.issn.1672-7347.2019.180316
20. Grune B, Kother AK, Budenbender B, Michel MS, Kriegmair MC, Alpers GW. Patients’ perspective on shared decision-making in urology: a prospective study at a university hospital. World J Urol. 2021;39(12):4491–4498. doi:10.1007/s00345-021-03794-3
21. Chang HL, Li FS, Lin CF. Factors influencing implementation of shared medical decision making in patients with cancer. Patient Prefer Adherence. 2019;13:1995–2005. doi:10.2147/PPA.S217561
22. Feiten S, Scholl I, Dunnebacke J, et al. Shared decision-making in routine breast cancer care in Germany-A cross-sectional study. Psychooncology. 2022;31(7):1120–1126. doi:10.1002/pon.5898
23. De Las Cuevas C, Penate W. To what extent psychiatric patients feel involved in decision making about their mental health care? Relationships with socio-demographic, clinical, and psychological variables. Acta Neuropsychiatr. 2014;26(6):372–381. doi:10.1017/neu.2014.21
24. Schoenfeld EM, Probst MA, Quigley DD, et al. Does shared decision making actually occur in the emergency department? Looking at it from the patients’ perspective. Acad Emerg Med. 2019;26(12):1369–1378. doi:10.1111/acem.13850
25. Hahlweg P, Kriston L, Scholl I, et al. Cancer patients’ preferred and perceived level of involvement in treatment decision-making: an epidemiological study. Acta Oncol. 2020;59(8):967–974. doi:10.1080/0284186X.2020.1762926
26. Fu WJ, Dai Y, Li XL. 126例门诊慢性伤口患者参与治疗决策的现状调查[Participation in treatment decision-making of patients with chronic wounds in outpatient: a 126-case study]. J Nurs China. 2017;24:44–47. Chinese. doi:10.16460/j.issn1008-9969.2017.18.044
27. Cao YY, Liu HR, Peng YJ, Yang Q, Yang SR, Tao YL. 肾移植受者手术决策参与满意度的调查研究[Current status and influencing factors of participating satisfaction with surgical treatment decision-making in patients with renal transplantation]. Chin J Nurs. 2021;56:1340–1346. Chinese. doi:10.3761/j.issn.0254-1769.2021.09.010
28. Zhao GG. 医患共同决策的研究现状及展望[Research situation and expectation of doctor-patient shared decision making]. Chin Nurs Manag. 2020;40:59–62. Chinese.
29. Cheng ZS, Bai XL, Xie GH, Zhang Z, Lou T. 心脏瓣膜置换患者参与治疗决策现状及影响因素分析[Determinants of participation in treatment decision-making by patients undergoing cardiac valve replacement]. J Nurs Sci. 2020;35:31–34. Chinese. doi:10.3870/j.issn.1001-4152.2020.19.031
30. Wan JL, Bian W, Liu MQ, et al. 湿性年龄相关性黄斑变性患者共同决策影响因素的质性研究[Qualitative study on factors influencing co-decision in patients with wet age-related macular degeneration]. J Clin Pathol Res. 2020;40:417–422. Chinese. doi:10.3978/j.issn.2095-6959.2020.02.026
31. Pieterse AH, Stiggelbout AM, Montori VM. Shared decision making and the importance of time. JAMA. 2019;322(1):25–26. doi:10.1001/jama.2019.3785
32. Xia WF. 医患共同决策临床实效的影响因素分析[Analysis of factors influencing clinical effectiveness of shared decision-making between doctors and patients]. Med Philosophy. 2021;42:11–14. Chinese. doi:10.12014/j.issn.1002-0772.2021.12.03
33. Liu YQ, Guo YL, Xu J, et al. Shared decision-making in hemophilic arthropathy rehabilitation: a qualitative study. Patient Prefer Adherence. 2023;17:249–257. doi:10.2147/PPA.S394095
34. Li Y, Ye ZX, Liu PY, Li L. 原发性肝癌诊断知情患者参与手术决策现状及影响因素研究[Current status of participation in surgery decision-making of informed primary liver cancer patients and its influence factors]. J Nurs China. 2016;23:6–10. Chinese. doi:10.16460/j.issn1008-9969.2016.18.006
35. Jin XF, Wu XY, Tao R. 住院患者满意度影响因素研究进展[Research progress on influencing factors of inpatient satisfaction]. Hosp Admin J Chin People’s Liberation Army. 2020;27:227–229. Chinese. doi:10.16770/J.cnki.1008-9985.2020.03.008
36. Guan WB, Liang D, Huang XY. 宁夏回族自治区县级公立医院住院患者满意度及其影响因素[Satisfaction and influencing factors of inpatients in county-level public hospitals in Ningxia Hui Autonomous Region]. China Health Resources. 2021;24:284–287. Chinese. doi:10.3969/j.issn.1007-953X.2021.03.016
37. Pang JM, Zhang QY, Wang XY, Wang Y. 医护人员实施乳腺癌患者决策辅助障碍及促进因素的质性研究[A qualitative study on the obstacles and promoting factors in the implementation of patient-centered decision-making in medical care]. Chin J Nurs. 2021;56:1516–1521. Chinese. doi:10.3761/j.issn.0254-1769.2021.10.012
38. Zhu YZ, Zhang S, Guan YZ, Meng M, Li LZ. 共享决策在ICU中的应用进展[Application progress of shared decision-making in ICU]. Chin J Nurs. 2021;56:289–294. Chinese. doi:10.3761/j.issn.0254-1769.2021.02.023
39. Scholl I, Kriston L, Dirmaier J, Buchholz A, Harter M. Development and psychometric properties of the Shared Decision Making Questionnaire--physician version (SDM-Q-Doc). Patient Educ Couns. 2012;88(2):284–290. doi:10.1016/j.pec.2012.03.005
40. Elwyn G, Edwards A, Wensing M, Hood K, Atwell C, Grol R. Shared decision making: developing the OPTION scale for measuring patient involvement. Qual Saf Health Care. 2003;12(2):93–99. doi:10.1136/qhc.12.2.93
41. Shields CG, Franks P, Fiscella K, Meldrum S, Epstein RA. Rochester participatory decision-making scale (RPAD): reliability and validity. Ann Fam Med. 2005;3(5):436–442. doi:10.1370/afm.305
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Statistical Analysis of Factors Affecting Surgically Induced Astigmatism Following Trabeculectomy
Shiratori N, Nakamoto K, Nishio Y, Takano Y, Arima T, Kunishige T, Suzuki H, Igarashi T, Takahashi H
Clinical Ophthalmology 2022, 16:3833-3839
Published Date: 21 November 2022
Influencing Factors of Self-Management Behavior in Patients with Glaucoma in West China: A Cross-Sectional Study
Zhang X, Ren J, Tang L, Zeng JH, Tang J
Patient Preference and Adherence 2025, 19:2377-2389
Published Date: 10 August 2025