Back to Journals » Patient Preference and Adherence » Volume 17
Factors Influencing Medication Adherence in Elderly Patients with Hypertension: A Single Center Study in Western China
Authors Pan Q ![]() , Zhang C, Yao L, Mai C, Zhang J, Zhang Z, Hu J
, Zhang C, Yao L, Mai C, Zhang J, Zhang Z, Hu J
Received 21 April 2023
Accepted for publication 8 July 2023
Published 17 July 2023 Volume 2023:17 Pages 1679—1688
DOI https://doi.org/10.2147/PPA.S418246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Qiuyu Pan,1,2 Cheng Zhang,3 Lansicheng Yao,4 Chenyao Mai,1 Jinpeng Zhang,5 Zhitong Zhang,6 Jun Hu7
1Medical College, Tibet University, Lhasa, Tibet, 850000, People’s Republic of China; 2School of Public Health, North Sichuan Medical College, Nanchong, Sichuan, 637100, People’s Republic of China; 3Policy Research Room 2, Sichuan Health Development Research Center, Chengdu, Sichuan, 610042, People’s Republic of China; 4Foreign Affairs Office, North Sichuan Medical College, Nanchong, Sichuan, 637100, People’s Republic of China; 5School of Public Health, Weifang Medical University, Weifang, Shandong, 261053, People’s Republic of China; 6Dalla Lana School of Public Health, University of Toronto, Toronto, ON, M5T 3M7, Canada; 7School of Management, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250355, People’s Republic of China
Correspondence: Jun Hu, School of Management, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, 250355, People’s Republic of China, Email [email protected]
Purpose: To develop and empirically test a conceptual model that explains the factors influencing antihypertensive medication adherence behavior in elderly patients in a city in western China.
Patients and Methods: The conceptual model was based on the Theory of Planned Behavior and the Health Belief Model and was empirically tested using cross-sectional survey data from Nanchong City, a city in western China, collected between October and December 2020. Data were analyzed using structural equation modeling.
Results: Behavioral intentions were the main predictor of medication adherence behavior (path coefficient of 0.353). Perceived benefits and perceived barriers directly (path coefficient = 0.201 and − 0.150, respectively), and indirectly (path coefficient = 0.118 and − 0.060) through behavioral intentions, influenced medication adherence behavior. Perceived susceptibility (path coefficient = 0.390) and perceived severity (path coefficient = 0.408) influenced behavioral attitudes, which influenced behavioral intentions (path coefficient = 0.298).
Conclusion: The conceptual model demonstrates a robust ability to predict and explain medication adherence behavior among elderly patients with hypertension, facilitating the adoption and maintenance of changes in adherence behavior and the potential for preventing disease progression and improving quality of life.
Keywords: compliance, theory of planned behavior, health belief model, elderly patients, China
Introduction
As the global burden of disease shifts from infectious to non-communicable diseases, and with the extension of life expectancy and changes in lifestyle, the prevalence of hypertension in China continues to rise, posing a major health challenge.1,2 In China, as many as 245 million people suffer from hypertension, which accounts for 24% of all deaths and 14% of disability-adjusted life years.3 The prevalence of hypertension among Chinese adults has reached 29.6%.4
Hypertension is a concern in China due to poor patient awareness and adherence to treatment, leading to low rates of hypertension treatment and control. Treatment and control rates significantly increased from 12.1% and 2.8% in 1991 to 40.7% and 15.3% in 2012–2015,5,6 and decreased to 34.6% and 12.0% in 2018, although changes in monitoring methods and an expanding treatment population may have resulted in biased estimations.7 Non-adherence to medication is a widespread problem, with rates ranging from 30% to 50%,8,9 and is closely linked to poor clinical outcomes and escalating healthcare costs.10 Hypertension is preventable and controllable,11 and the efficacy of antihypertensive medication depends on a patient’s adherence; therefore, improving antihypertensive medication adherence has become a priority in China.
A comprehensive understanding of the factors that impact medication adherence in patients with hypertension in China represents an important first step to improving blood pressure control. Currently, medication adherence in patients with hypertension in China has been evaluated in observational studies that considered patients’ demographic and clinical characteristics, type of drug and frequency of hospital visits.12,13 The objective of the present study was to extend these findings and develop and empirically test an innovative conceptual model to explain the factors influencing antihypertensive medication adherence in elderly patients from an urban environment in western China. The conceptual model was based on assumptions derived from the Theory of Planned Behavior (TPB)14 and the Health Belief Model (HBM).15 The TPB and HBM are conventional tools used to predict behavior. The TPB states that social norms, behavioral attitudes and perceived behavioral control predict intentions. The HBM explains and predicts health-related behavior. The HBM states that the implementation of a health-related behavior is influenced by an individual’s perceived threat from a disease, and whether adopting a health-related behavior will be effective in mitigating that threat. The HBM includes six components: perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues-to-action, and self-efficacy.16 The TPB and HBM were developed to characterize the factors that underlie behavior and do not account for other variables that factor into behavior, such as fear, mood, or past experience. Both the TPB and HBM were developed to characterize the factors that underlie behavior. The objective of the present study was to extend these findings and develop and empirically test an innovative conceptual model to explain the factors influencing antihypertensive medication adherence in representative of elderly patients from a highly urban environment in western China.
Materials and Methods
Innovative Conceptual Model
The TPB and HBM are limited as their main components have a weak effect size and the theories have low predictive capability.17 The TPB assumes that the primary determinant of behavioral intentions is an individual’s attitudes about the likelihood that a behavior will have the expected outcome. When considering medication adherence behavior, behavioral attitudes to medication adherence are influenced by perceived outcomes, and behavioral control is influenced by how confident an individual is that s/he can execute a given behavior. According to TPB, behavioral attitudes to medication adherence are influenced by perceived outcomes, and behavioral control is influenced by how confident an individual is that s/he can execute a given behavior. The HBM assumes that behavioral intentions depend on an individual’s own beliefs.18 When considering medication adherence behavior, perceived susceptibility and perceived severity describe an individual’s subjective perception of the risk and potential threat of a disease and influence the individual’s attitudes and intentions to adopt medication adherence behavior. Perceived benefits and perceived barriers describe the benefits that an individual obtains or barriers that may be encountered, reflecting an individual’s willingness and likelihood to adopt medication adherence behavior. Cues-to-action and self-efficacy refer to an individual’s subjective judgment of whether s/he will be able to successfully adopt medication adherence behavior.19 This study combined the strongest components from each theory to create a complete integrated model to elicit change in health-related behavior (Figure 1).
 |
Figure 1 Theoretical model of factors influencing medication adherence behavior. The conceptual model combined the strongest components of the Theory of Planned Behavior (TPB) and the Health Belief Model (HBM). |
Participants
This study was approved by the ethics committee of North Sichuan Medical College (#NSMC lunlishencha 202201). Data were analyzed using structural equation modeling (SEM). Sample size was calculated as n=400, assuming a confidence interval of 1.96, a margin of error of 5%, a population proportion of 0.5, and that an SEM requires 10–15 observations per estimated parameter.20
A convenience sample of patients aged >60 years with confirmed hypertension attending various community health service centers in Nanchong City, China, between October and December 2020 were eligible for his study. Inclusion criteria were 1) history of hypertension; 2) aged > 60 years; 3) currently or previously prescribed antihypertensive medication; 4) attending a community health service center in Nanchong, China; 5) provided written informed consent to participate in the study; and 6) ability to communicate and willing to work with the researchers. Exclusion criteria were patients with 1) severe complications including cancer, severe cardiopathy, and liver and kidney diseases; 2) secondary hypertension; 3) cognitive impairment; or 4) psychiatric abnormalities.
Instruments
In this study, a total of five trained investigators administered a structured self-administered questionnaire to the patients enrolled in the study. Most patients were able to complete the questionnaire independently. For patients with dyslexia, investigators could directly communicate with these patients, but were unable to provide responses to the questions. In these circumstances, a specifically trained investigator completed the questionnaire based on patient response.
The questionnaire consisted of three parts. Part 1 described the concepts of medication adherence behavior. Part 2 collected demographic data, including patient gender, age, education level, marital status, occupation, per capita monthly income, and health insurance. Part 3 comprised components derived from the TPB and HBM, included as seven subscales with 3 items each: behavioral intentions, behavioral attitudes, perceived susceptibility, perceived severity, perceived benefits, perceived barriers, and medication adherence behavior. Behavioral intentions referred to the motivating factors that influenced the patient to perform a health-related behavior. Behavioral attitudes referred to the degree to which the patient had a positive or negative evaluation of a health-related behavior, following consideration of the outcomes of the behavior. Perceived susceptibility referred to the patient’s subjective perception of the risk of acquiring a disease or health problem. Perceived severity referred to the patient’s subjective perception of the consequences of a disease. Perceived benefits/barriers referred to the patient’s subjective perception of the benefits and barriers related to a health-related behavior. Medication adherence behavior referred to the extent to which a patient correctly followed medical advice (Table 1).
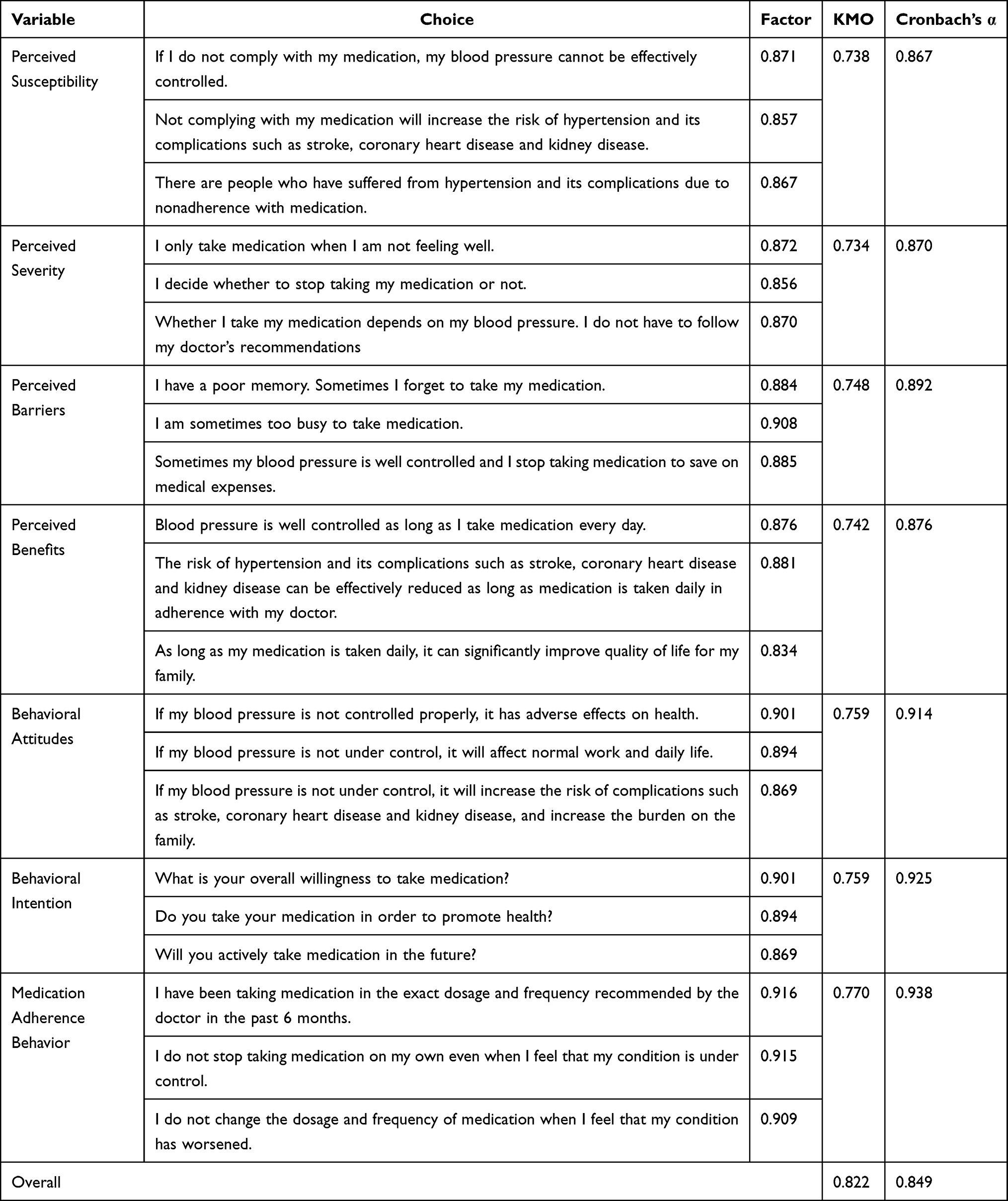 |
Table 1 Psychometric Assessment of Part 3 of the Questionnaire (N=400) |
Items were developed based on a literature review, expert consultation and factor analysis. Items were scored on a 5-point Likert scale. Psychometric assessment of Part 3 of the questionnaire showed the Cronbach’s α of the total questionnaire and each subscale were > 0.8, which indicates good internal consistency. Kaiser-Meyer-Olkin (KMO) testing confirmed that the variables were suitable for a factor analysis (Table 1).
Statistical Methods
Data were collected in Excel. Exploratory factor analysis was conducted using SPSS software to assess the reliability and validity of Part 3 of the questionnaire. Confirmatory factor analysis and SEM were conducted using AMOS software, including calculating factor loadings and standardized path coefficients, and fitting the SEM. P < 0.05 was considered a statistically significant difference.
Results
Characteristics of the Study Subjects
A total of 400 patients with hypertension were enrolled in this study. Table 2 summarizes the baseline characteristics of these patients. Mean (SD) age was 64.81±12.05 years, and 49.0% of the patients were male. 13.2% of patients had higher education, and approximately 50% of patients were educated below high school. 54.5% of patients were farmers. Most patients had experienced hypertension for more than 5 years, with 36.7% of patients experiencing hypertension for more than 10 years.
 |
Table 2 Patient Demographic Characteristics (N=400) |
Main Results
AMOS software was used to estimate the SEM. Fit indices (χ2=265.959, χ2/DF = 1.469 [< 2], root mean square error of approximation [RMSEA] = 0.034 [<0.05], and Comparative Fit Index [CFI]; Normed Fit Index [NFI], Tucker Lewis index [TLI] and Incremental Fit Index [IFI], all ≥ 0.9), implied good fit between the conceptual model and the survey data in this study.
Final path coefficients representing the strength of connections between the variables are shown in Figure 2. Behavioral intentions had a direct positive effect on antihypertensive medication adherence behavior at the 0.001 level (path coefficient =0.353; p<0.001), and was the main predictor of antihypertensive medication adherence behavior. Behavioral attitudes had a direct positive effect on behavioral intentions (path coefficient =0.298; p<0.001) and an indirect positive effect on antihypertensive medication adherence behavior (path coefficient =0.105; p<0.001). Perceived benefits had a direct positive effect on behavioral intentions (path coefficient = 0.335; p<0.001) and antihypertensive medication adherence behavior (path coefficient = 0.201; p<0.001), and an indirect positive effect on antihypertensive medication adherence behavior (path coefficient = 0.118; p<0.001). Perceived barriers had a direct negative effect on behavioral intentions (path coefficient =−0.169; p<0.001) and antihypertensive medication adherence behavior (path coefficient =−0.150, p<0.01), and an indirect negative effect on antihypertensive medication adherence behavior (path coefficient =−0.060; p<0.001). Perceived susceptibility and perceived severity were predictors of behavioral attitudes. Perceived susceptibility (path coefficient =0.390, p<0.001, and perceived severity (path coefficient =0.408; p<0.001) had direct positive effects on behavioral attitudes.
 |
Figure 2 Path analysis medication adherence behavior. In structural equation modeling, the p-value is used to determine the significance of the assumed path. Model output results indicate that the independent variable is significantly correlated with the dependent variable at the 0.01 or 0.001 level. Notes: **P value <0.01; ***P value <0.001. |
Discussion
Adaptability of the Model
The most important contribution of this study is that a conceptual model based on TPB and HBM is innovatively developed and empirically tested using survey data from Nanchong city in western China. Empirical study has proved that the model has a high explanatory and predictive ability for the antihypertensive drug compliance behavior of elderly patients in western China.
This new conceptual model integrates the influence of behavioral intentions, behavioral attitudes, perceived benefits, perceived barriers, perceived susceptibility, and perceived severity on antihypertensive medication adherence.
Fully consider that the patient is a social being, and his/her behavior will be affected by various sources. These complicated factors will affect whether the patient will comply with the medication. Only by clarifying these factors can we better help the patient.
The Effect of Behavioral Intentions
In the present study, behavioral intentions (path coefficient =0.353; p<0.001) were the main predictor of antihypertensive medication adherence behavior. These findings are consistent with previous research, which has demonstrated the close association between behavioral intentions and medication adherence.21,22
Within the context of medication adherence behavior, behavioral intentions determine whether patients take their medication in accordance with medical advice. Treatment for hypertension requires chronic therapy and maintenance of certain lifestyle habits and dietary restrictions, such as taking medication on time and avoiding foods or beverages that interact with medications. Only patients with strong behavioral intentions can adhere to medication and change their lifestyle, increasing treatment efficacy. These findings imply that enhancing behavioral intentions may improve medication adherence and treatment outcomes in patients with hypertension.23–25
The Effect of Behavioral Attitudes
In this study, behavioral attitudes indirectly influenced medication adherence behavior through behavioral intentions (path coefficient = 0.105). Previous research shows a close correlation between behavioral attitudes, behavioral intentions, medication adherence, and blood pressure control.26–28 Patients with a positive attitude towards medication and the intention to adhere to the prescribed medication regimen are more likely to exhibit positive medication adherence behavior, which should improve clinical outcomes. To the authors’ knowledge, previous reports have examined the effects of behavioral attitudes and behavioral intentions on medication adherence behavior. The present study verified the accuracy of these previous studies and further explored the mediating role of behavioral intentions in medication adherence behavior in patients with hypertension.
The Effect of Perceived Benefits and Perceived Barriers
Perceived benefits (direct: path coefficient = 0.201; indirect: path coefficient = 0.118) and perceived barriers (direct: path coefficient = −0.150; indirect: path coefficient = −0.060) directly, and indirectly through behavioral intentions, influenced antihypertensive medication adherence behavior. When patients perceive the benefits of medication, such as reducing blood pressure and complications, they are more likely to adhere to the prescribed medication.29 Perceived barriers, such as lack of efficacy, side effects, and costs may reduce patients’ confidence in treatment and decrease their adherence behavior.30,31 Consistent with this, other studies have demonstrated the direct impact of perceived benefits and barriers on patients’ decisions to manage hypertension.32
Perceived benefits and perceived barriers have an indirect influence on medication adherence through behavioral intentions. When patients perceive the benefits of medication, such as reducing blood pressure and complications, lowering medical costs, and improving health outcomes, their willingness to continue using medication increases.33 Conversely, perceived barriers can diminish individuals’ recognition of the effectiveness and importance of medication therapy, creating doubts and resistance to medication adherence,33 highlighting the importance of reducing perceived barriers to medication adherence.34
The Effect of Perceived Susceptibility and Perceived Severity
Perceived susceptibility and perceived severity were predictors of behavioral attitudes, with standardized path coefficients of 0.390 and 0.408, respectively (p<0.001). Patients’ perception of the severity and susceptibility of their condition can motivate them to adhere to antihypertensive medication.35 When patients perceive hypertension as a more severe condition (perceived high severity) and themselves as more susceptible to hypertension (perceived high susceptibility), they are more likely to exhibit improved medication adherence behavior.36
Perceived severity and susceptibility can indirectly affect patients’ medication adherence behavior by influencing their behavioral attitudes and behavioral intentions towards hypertension. When individuals have a high perception of severity and susceptibility, they tend to pay more attention to their illness and personal feelings, take their condition seriously, and are more likely to adopt positive attitudes and behaviors to control hypertension. Conversely, if they have a low perception of severity and susceptibility, they may not take their illness seriously and may not adhere to medication as prescribed.
Recommendations
The findings from the present study may inform the implementation of public health programs to improve blood pressure control, education and medication adherence in patients with hypertension in western China. Based on the factors influencing medication adherence behavior identified in this study and in conjunction with the development of targeted interventions led by primary healthcare providers, appropriate measures can be taken to improve medication adherence behavior in patients with hypertension.
Collaborative decision-making between clinicians and patients may enhance disease awareness, promote a high level of awareness of the severity and susceptibility of the disease, assist elderly patients and their families in managing chronic diseases, and induce changes in attitudes and behaviors. Emphasis should be placed on the burden of chronic disease and the provision of community resources, and family members should be provided health education so they can offer appropriate support to elderly patients.
Limitations
This study was limited by its cross-sectional design. Data were collected from patients with hypertension in Nanchong City, Sichuan Province, China; therefore, the sample size was small and may not be generalizable to other regions. Also, our study based on the data from a single center, which may have some selection bias and thus distort the conclusions.
Conclusion
A novel conceptual model integrating key components from TPB and HBM was developed and empirically tested using survey data collected in Nanchong city, western China. The model’s high explanatory and predictive power for antihypertensive drug compliance behavior among elderly patients was demonstrated by empirical studies.
The model suggested the development of interventions that improve medication adherence behavior in elderly patients with hypertension in western China. Managing elderly patients with chronic diseases may facilitate the adoption and maintenance of long-term changes in medication adherence behavior, with potential to prevent progression of disease and improve quality of life.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki, and approved by the the ethics committee of North Sichuan Medical College (#NSMC lunlishencha 202201). Informed consent was obtained from all study subjects.
Funding
This work was supported by the Nanchong City Social Science Research “13th Five Year Plan” 2020 Project [NC2020C076], 2020 Sichuan Research Center for Applied Psychology Project [CSXL-202A06], and “High-level Talents Training Program” for postgraduates of Tibet University [2020-GSP-B020].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mills KT, Stefanescu A, He J. The global epidemiology of hypertension. Nat Rev Nephrol. 2020;16(4):223–237. doi:10.1038/s41581-019-0244-2
2. Zhou C, Chen J, Tan F, et al. Relationship between self-care compliance, trust, and satisfaction among hypertensive patients in China. Front Public Health. 2023;10:1085047. doi:10.3389/fpubh.2022.1085047
3. Fan W, Xie F, Wan Y, Campbell NRC, Su H. The impact of changes in population blood pressure on hypertension prevalence and control in China. J Clin Hypertens. 2020;22(2):150–156. doi:10.1111/jch.13820
4. Zhang M, Shi Y, Zhou B, et al. Prevalence, awareness, treatment, and control of hypertension in China, 2004-18: findings from six rounds of a national survey. BMJ. 2023;380:e071952. doi:10.1136/bmj-2022-071952
5. Tao S, Wu X, Duan X, et al. Hypertension prevalence and status of awareness, treatment and control in China. Chin Med J. 1995;108(7):483–489.
6. Wang Z, Chen Z, Zhang L, et al. Status of Hypertension in China: results From the China Hypertension Survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
7. Wang JG, Zhang W, Li Y, Liu L. Hypertension in China: epidemiology and treatment initiatives. Nat Rev Cardiol. 2023. doi:10.1038/s41569-022-00829-z
8. Hameed MA, Dasgupta I. Medication adherence and treatment-resistant hypertension: a review. DIC. 2019;8:1–11. doi:10.7573/dic.212560
9. Lawson AJ, Hameed MA, Brown R, et al. Nonadherence to antihypertensive medications is related to pill burden in apparent treatment-resistant hypertensive individuals. J Hypertens. 2020;38(6):1165–1173. doi:10.1097/HJH.0000000000002398
10. Sohn IS, Kim CJ, Yoo BS, et al. Clinical impact of guideline-based practice and patients’ adherence in uncontrolled hypertension. Clin Hypertens. 2021;27(1):26. doi:10.1186/s40885-021-00183-1
11. The National Essential Public Health Service Program Office. National Committee on Hypertension Management in Primary Health Care. National Clinical Practice Guidelines on the Management of Hypertension in Primary Health Care in China (2020). Chinese Circulation J. 2021;36(03):209–220. doi:10.3969/j.issn.1000-3614.2021.03.001
12. Li T, Shuai P, Wang J, Wang L. Prevalence, awareness, treatment and control of hypertension among Ngawa Tibetans in China: a cross-sectional study. BMJ Open. 2021;11(9):e052207. doi:10.1136/bmjopen-2021-052207
13. Yu P, Ning Y, Gao Y, et al. Hypertension among Mongolian adults in China: a cross-sectional study of prevalence, awareness, treatment, control, and related factors: hypertension among Mongolian adults in China. J Clin Hypertens. 2021;23(9):1786–1801. doi:10.1111/jch.14348
14. Ajzen I. From Intentions to Actions: a Theory of Planned Behavior. In: Kuhl J, Beckmann J, editors. Action Control. Berlin Heidelberg: Springer; 1985:11–39. doi:10.1007/978-3-642-69746-3_2
15. Janz NK, Becker MH. The Health Belief Model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
16. Matlabi M, Esmaeili R, Moshki M, Ranaei A, Haji A, Mehrabi R. The status and predictors of hypertension preventive nutritional behaviors in adolescents based on the constructs of the Theory of Planned Behavior. Electron Phys. 2018;10(1):6223–6230. doi:10.19082/6223
17. Wang X, Chen D, Xie T, Zhang W. Predicting women’s intentions to screen for breast cancer based on the health belief model and the theory of planned behavior. J Obstet Gynaecol Res. 2019;45(12):2440–2451. doi:10.1111/jog.14109
18. Lee YH, Wu J. The indirect effects of online social entertainment and information seeking activities on reading literacy. Comput Educ. 2013;67:168–177. doi:10.1016/j.compedu.2013.03.001
19. Khorsandi M, Fekrizadeh Z, Roozbahani N. Investigation of the effect of education based on the health belief model on the adoption of hypertension-controlling behaviors in the elderly. Clin Interv Aging. 2017;12:233–240. doi:10.2147/CIA.S117142
20. Wolf EJ, Harrington KM, Clark SL, Miller MW. Sample Size Requirements for Structural Equation Models: an Evaluation of Power, Bias, and Solution Propriety. Educ Psychol Meas. 2013;76(6):913–934. doi:10.1177/0013164413495237
21. Tan FCJH, Oka P, Dambha-Miller H, Tan NC. The association between self-efficacy and self-care in essential hypertension: a systematic review. BMC Fam Pract. 2021;22:44. doi:10.1186/s12875-021-01391-2
22. Shen Z, Shi S, Ding S, Zhong Z. Mediating Effect of Self-Efficacy on the Relationship Between Medication Literacy and Medication Adherence Among Patients With Hypertension. Front Pharmacol. 2020;11:569092. doi:10.3389/fphar.2020.569092
23. Patton DE, Hughes CM, Cadogan CA, Ryan CA. Theory-Based Interventions to Improve Medication Adherence in Older Adults Prescribed Polypharmacy: a Systematic Review. Drugs Aging. 2017;34(2):97–113. doi:10.1007/s40266-016-0426-6
24. Lehane E, McCarthy G. Intentional and unintentional medication non-adherence: a comprehensive framework for clinical research and practice? A discussion paper. Int J Nurs Stud. 2007;44(8):1468–1477. doi:10.1016/j.ijnurstu.2006.07.010
25. Heshmati R, Alizadeh M, Javadpour S, Alizada N. Psychosocial determinants of self-care behavior in outpatients with heart failure: a test of Pender’s health promotion model. Iran Red Crescent Med J. 2020;22(12). doi:10.32592/ircmj.2020.22.12.141
26. Choi HY, Oh IJ, Lee JA, et al. Factors Affecting Adherence to Antihypertensive Medication. Korean J Fam Med. 2018;39(6):325–332. doi:10.4082/kjfm.17.0041
27. Alsofyani MA, Aloufi AO, Al-Qhtani NS, Bamansour SO, Almathkori RS. Factors related to treatment adherence among hypertensive patients: a cross-sectional study in primary healthcare centers in Taif city. J Family Community Med. 2022;29(3):181–188. doi:10.4103/jfcm.jfcm_153_22
28. Eslamimehr F, Hosseini Z, Aghamolaei T, Nikparvar M, Ghanbarnezhad A. Self-Care Behaviors in Patients with Hypertension to Prevent Hypertensive Emergencies: a Qualitative Study Based on the Theory of Planned Behavior. J Cardiovascular Em. 2022;8(4):75–85. doi:10.2478/jce-2022-0016
29. Rimando M. Perceived Barriers to and Facilitators of Hypertension Management among Underserved African American Older Adults. Ethn Dis. 2015;25(3):329–336. doi:10.18865/ed.25.3.329
30. Hsu YH, Mao CL, Wey M. Antihypertensive medication adherence among elderly Chinese Americans. J Transcult Nurs. 2010;21(4):297–305. doi:10.1177/1043659609360707
31. Woode E, Boakye‐Gyasi E, Obirikorang Y, et al. Predictors of medication nonadherence among hypertensive clients in a Ghanaian population: application of the Hill‐Bone and Perceived Barriers to Treatment Compliance Scale. Health Sci Rep. 2022;5(3):e584. doi:10.1002/hsr2.584
32. Goudarzi H, Barati M, Bashirian S, Moeini B. Determinants of medication adherence among hypertensive patients using the Pender’s health promotion model. J Educ Health Promot. 2020;9:89. doi:10.4103/jehp.jehp_687_19
33. Sadeghi R, Masoudi MR, Patelarou A, Khanjani N. Predictive Factors for the Care and Control of Hypertension Based on the Health Belief Model Among Hypertensive Patients During the COVID-19 Epidemic in Sirjan, Iran. Curr Hypertens Rev. 2022;18(1):78–84. doi:10.2174/1573402117666210603115309
34. Yue Z, Li C, Weilin Q, Bin W. Application of the health belief model to improve the understanding of antihypertensive medication adherence among Chinese patients. Patient Educ Couns. 2015;98(5):669–673. doi:10.1016/j.pec.2015.02.007
35. Obirikorang Y, Obirikorang C, Acheampong E, et al. Predictors of Noncompliance to Antihypertensive Therapy among Hypertensive Patients Ghana: application of Health Belief Model. Int J Hypertens. 2018;2018:4701097. doi:10.1155/2018/4701097
36. Kamran A, Sadeghieh Ahari S, Biria M, Malepour A, Heydari H. Determinants of Patient’s Adherence to Hypertension Medications: application of Health Belief Model Among Rural Patients. Ann Med Health Sci Res. 2014;4(6):922–927. doi:10.4103/2141-9248.144914
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.