Back to Journals » International Journal of Women's Health » Volume 17
Factors Influencing Knowledge, Attitudes, and Practices (KAP) Regarding Dental Diagnosis and Treatment During Pregnancy Among Pregnant Women in Harbin, China: A Cross-Sectional Study
Authors Wang X ![]() , Xu B, Fan J, Wang Y
, Xu B, Fan J, Wang Y ![]()
Received 14 August 2025
Accepted for publication 17 November 2025
Published 13 December 2025 Volume 2025:17 Pages 5399—5410
DOI https://doi.org/10.2147/IJWH.S560628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Xiaonan Wang, Baiqiang Xu, Jiayu Fan, Yanming Wang
Department of Stomatology, the Forth Affiliated Hospital of Harbin Medical University, Harbin, Heilongjiang, 150001, People’s Republic of China
Correspondence: Yanming Wang, Department of Stomatology, the Forth Affiliated Hospital of Harbin Medical University, 37 Yiyuan Street, Harbin, Heilongjiang, 150000, People’s Republic of China, Tel +8615846576709, Email [email protected]
Purpose: This study primarily aimed to identify factors influencing the knowledge, attitudes, and practices (KAP) of pregnant women regarding dental diagnosis and treatment during pregnancy in Harbin, China.
Patients and Methods: A cross-sectional study was conducted from May to July 2025, during which 383 pregnant women attending the Obstetrics Department of the Fourth Affiliated Hospital of Harbin Medical University were successfully recruited via convenience sampling. A self-designed, validated questionnaire based on the KAP model and the standardized Modified Dental Anxiety Scale (MDAS) was used for data collection. Data were analyzed using descriptive statistics, Pearson correlation, univariate analysis, and multiple linear regression.
Results: The mean KAP scores (standardized to a 100-point scale) were suboptimal: knowledge, 59.36 ± 14.10; attitude, 59.92 ± 13.60; practice, 64.66 ± 16.74; and total KAP, 60.33 ± 12.28. Knowledge gaps were most evident regarding oral medications and radiographic examinations. Dental anxiety was prevalent in 72.0% of participants. The primary barrier to seeking care was safety concerns (74.93%). Medical professionals and online new media were the most frequently reported sources of oral health information. Multiple linear regression identified medical background, pregnancy intention, educational attainment, and dental anxiety as significant predictors of total KAP score (p < 0.05).
Conclusion: Pregnant women’s KAP toward dental diagnosis and treatment were influenced by educational attainment, Medical professional background, pregnancy intention, and dental anxiety. Developing national guidelines, enhancing multidisciplinary collaboration, and providing targeted education and psychological support may improve oral health outcomes.
Keywords: pregnant women, dental diagnosis and treatment, knowledge–attitude–practice, KAP, cross-sectional study, dental anxiety, influencing factors
Introduction
Pregnancy is a unique physiological and psychological state during which women experience profound systemic changes that may increase their susceptibility to oral diseases such as pregnancy gingivitis, periodontitis, and dental caries. Poor oral health during pregnancy has been associated with adverse pregnancy outcomes, including preterm birth and low birth weight,1,2 underscoring the importance of maintaining oral health as part of comprehensive maternal care.
Although clinical guidelines have established that dental treatment are safe and necessary during all trimesters, many women remain inadequately informed or hold misconceptions regarding dental care. According to the Knowledge–Attitude–Practice (KAP) model, knowledge serves as the foundation for attitudes, which subsequently influence health practices.3 Consequently, inadequate knowledge may lead to negative attitudes and poor health practices. Numerous studies have demonstrated that the utilization of dental services during pregnancy remains low worldwide.4 This persistent gap represents a global public health concern shaped by sociodemographic, economic,5 and healthcare system factors,6 as well as individual psychological characteristics.
However, psychological and emotional determinants have received comparatively limited attention. Pregnancy is characterized by substantial emotional fluctuation and increased vulnerability to anxiety and fear. Dental anxiety and treatment-related fear may act as important psychological barriers influencing pregnant women’s knowledge, attitudes, and practices concerning dental care.
Given this context, the present study primarily aimed to identify factors influencing the knowledge, attitudes, and practices (KAP) of pregnant women regarding dental diagnosis and treatment during pregnancy in Harbin, China, with particular emphasis on the role of dental anxiety as a potential determinant. The findings are expected to provide evidence for developing targeted health education initiatives and integrated prenatal oral health programs to promote better maternal and fetal outcomes.
Materials and Methods
Participants and Sampling
This cross-sectional survey was conducted from May to July 2025, during which a total of 383 pregnant women attending the Obstetrics Department of the Fourth Affiliated Hospital of Harbin Medical University were successfully recruited via convenience sampling. Inclusion criteria were: (1) age ≥18 years; (2) ability to read and write; (3) absence of serious medical or mental disorders; and (4) provision of informed consent.
Sample size estimation followed conventional rules of thumb used in multivariable regression, requiring at least 10–20 observations per predictor variable, as suggested in clinical research guidelines.7 Based on 16 independent variables, the estimated range was 160–320, with an additional 20% to account for potential invalid responses, yielding a target of 192–384. A total of 400 questionnaires were distributed, and 383 valid responses were obtained (response rate: 95.8%). While practical in the hospital setting, convenience sampling may introduce selection bias and limit generalizability.
Research Instrument
Self-Designed Questionnaire
Survey Questionnaire on Knowledge, Attitudes, and Practices Regarding Dental Diagnosis and Treatment Among Pregnant Women, which contains three sections: 1) General Information: demographic and pregnancy-related data; 2) KAP Section: 33 items across three domains—knowledge (18 items), attitudes (10 items), and practices (5 items). Items were rated on a 5-point Likert scale ranging from 1 (“completely unaware/disagree”) to 5 (“completely aware/agree”), with higher scores reflecting better KAP levels. 3) Knowledge Dissemination Channels and Treatment Concerns: two multiple-choice items. Since all data were self-reported, the findings may be affected by participants’ memory errors or their tendency to respond in a socially acceptable manner.
Modified Dental Anxiety Scale (MDAS)
The MDAS includes five items rated on a 5-point Likert scale (score range: 5–25). A score ≥12 indicates dental anxiety, while scores >19 reflect high anxiety levels.8
Questionnaire Development and Validation
The Survey Questionnaire on Knowledge, Attitudes, and Practices Regarding Dental Diagnosis and Treatment Among Pregnant Women was self-developed based on the Knowledge-Attitude-Practice (KAP) framework and relevant literature.9–14
To establish content validity, we conducted a two-round Delphi expert consultation process. Fifteen experts, specializing in eight fields including maternal oral health, obstetrics, and dental care, were invited to participate (Table S1). During this process, experts evaluated the relevance and importance of each item, providing valuable feedback for revision. The final version achieved full expert consensus (Table S2).
Prior to the main study, a pilot study was performed on a sample of 260 participants to assess the questionnaire’s feasibility and refine its items. Item analysis was performed to assess discriminatory power and internal consistency, leading to the removal of statistically suboptimal items (Table S3).
The questionnaire’s reliability and validity were subsequently evaluated using the pilot study data. Reliability (Table S4): The internal consistency was measured using Cronbach’s alpha coefficient. The results indicated that the coefficients for the overall questionnaire and its three dimensions (knowledge, attitude, and practice) were all above the standard threshold of 0.7, suggesting high internal consistency. Validity (Table S5–S7): Exploratory Factor Analysis (EFA) was performed separately on the knowledge, attitude, and practice dimensions to assess their construct validity, consistent with the questionnaire’s theoretical structure. Kaiser-Meyer-Olkin (KMO) values for the knowledge (0.933), attitude (0.811), and practice (0.805) dimensions were all above 0.7, and Bartlett’s test of sphericity was significant for all three (p < 0.001), confirming their suitability for factor analysis. EFA identified three factors for knowledge (explaining 68.35% of variance), two for attitude (63.13%), and one for practice (58.45%), all consistent with the theoretical framework.
These results indicate that the questionnaire demonstrated satisfactory reliability and validity, supporting its suitability for assessing KAP regarding dental diagnosis and treatment among pregnant women.
Data Collection
With departmental approval, eligible participants were given standardized instructions regarding the study’s purpose and significance. After providing informed consent, they completed anonymous questionnaires on site, which were immediately reviewed by the research team to correct omissions or errors.
Data Processing and Analysis
Data were entered into Microsoft Excel 2021 and analyzed using IBM SPSS Statistics for Windows, Version 27.0.1.
Descriptive statistics summarized demographic characteristics, dental anxiety levels, KAP scores, information sources, and treatment concerns. Categorical variables were presented as frequencies and percentages, and continuous variables as means ± standard deviations.
For univariate analysis, Pearson correlation examined relationships between KAP dimensions and dental anxiety. Independent-samples t tests and one-way ANOVA assessed associations between demographic variables and KAP scores. When variance homogeneity was violated, Welch’s t test or Welch’s ANOVA was applied, with post hoc comparisons using LSD-t or Tamhane’s T2 tests as appropriate.
For multivariate analysis, multiple linear regression was performed with total KAP score as the dependent variable. Independent variables were those significant in univariate analyses. Education level and family income, as ordinal categorical variables with unequal intervals, were converted into dummy variables (ordinal categorical variables with unequal intervals) before analysis.
Results
General Information About Pregnant Women
A total of 383 pregnant women were included, with a mean age of 30.64 ± 3.96 years and a mean gestational age of 25.61 ± 10.38 weeks. Most were primiparous (84.6%), urban residents (92.69%), and had college or higher education (71.02%). Over 75% had planned pregnancies, 93.47% conceived naturally, and 83.55% reported no adverse pregnancy outcomes. Only 10.44% were employed in medical-related fields, and the majority had a monthly household income above 4,000 yuan (Table 1).
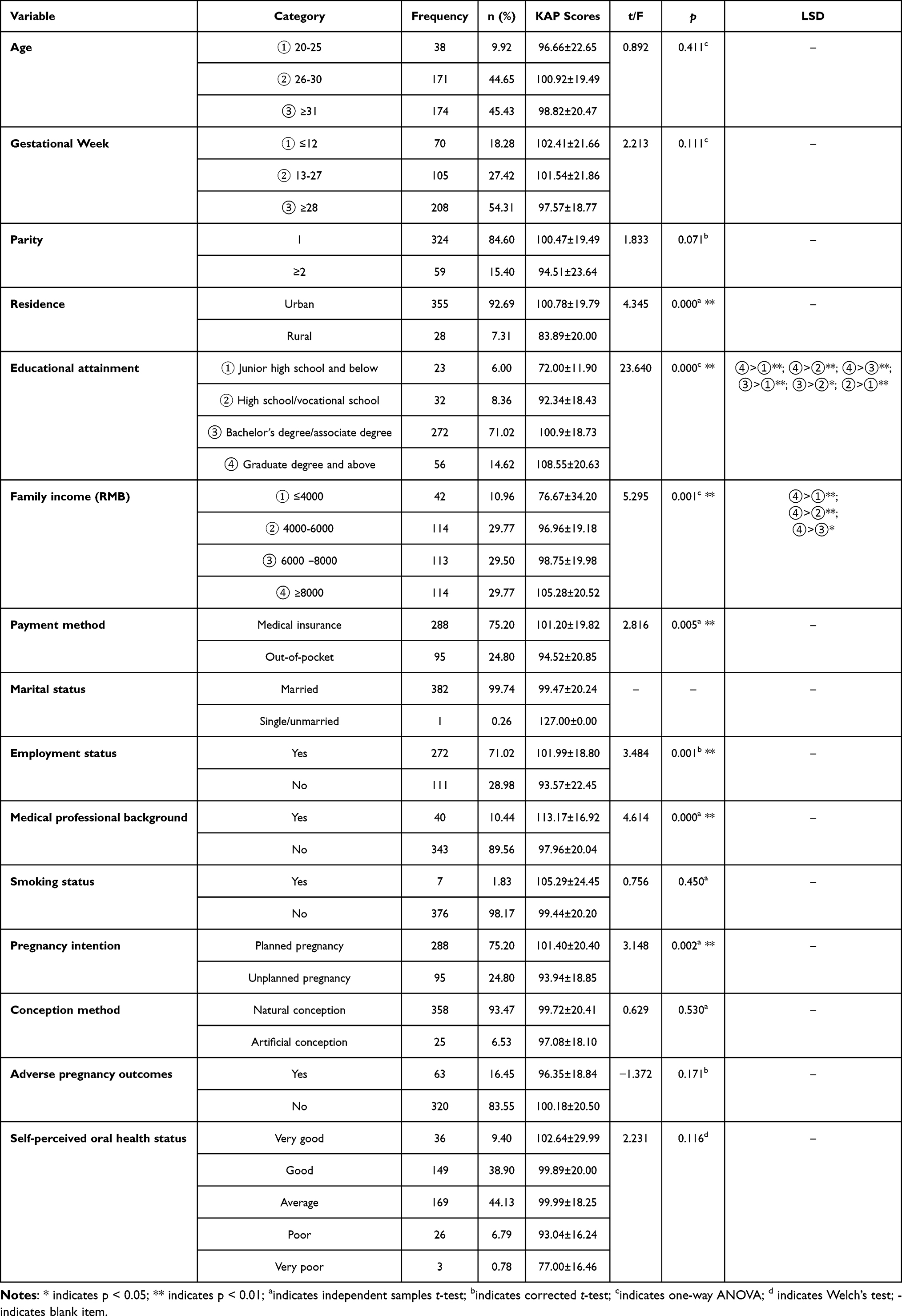 |
Table 1 Results of Univariate Analysis |
Nearly half of the pregnant women reported average oral health status (44.13%). A majority of the participants experienced oral health issues during pregnancy, with gingival bleeding (39.69%) being the most prevalent oral symptom (Figure 1).
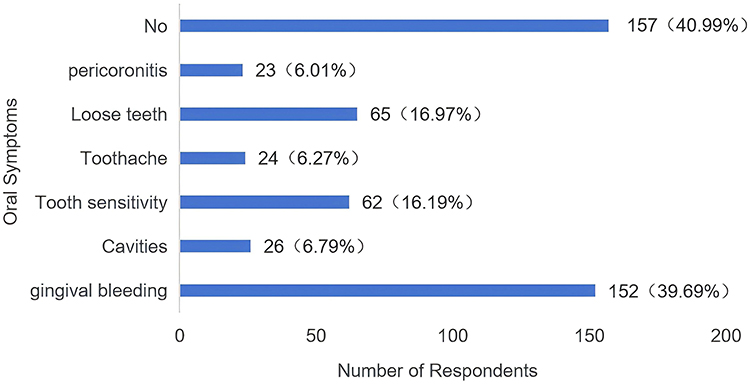 |
Figure 1 Self-Assessment of Oral Symptoms in Pregnant Women. |
Dental Anxiety in Pregnant Women
In this study, pregnant women scored relatively high on items 3 and 5. The total scale scores ranged from 5 to 25, with an average score of 13.52 ± 3.92. Among the participants, 64.2% scored between 12 and 19, indicating the presence of dental anxiety, while 7.8% scored above 19, categorizing them as high dental anxiety (Table 2).
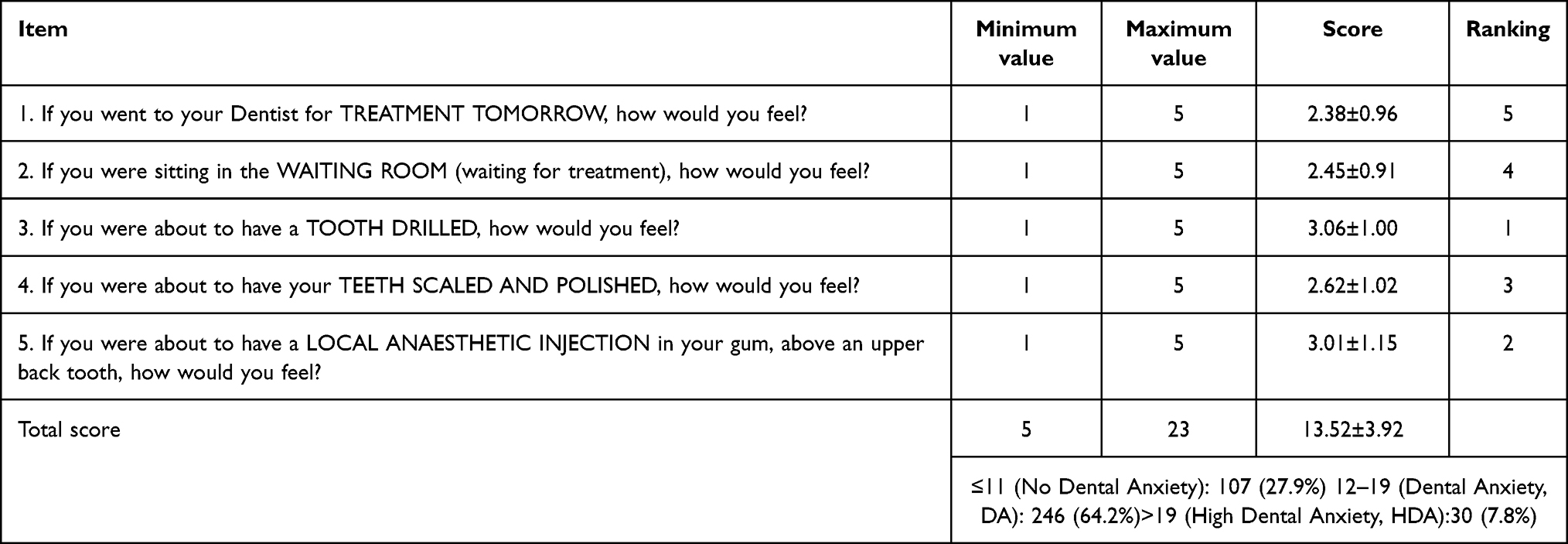 |
Table 2 Dental Anxiety Scores in Pregnant Women |
Pregnant Women’s KAP Score Distribution
The mean total KAP score was 99.55 ± 20.26, with knowledge, attitude, and practice scores of 53.42 ± 12.69, 29.96 ± 6.80, and 16.16 ± 4.19, respectively. Standard scores were calculated using the formula: Standard score = (Actual score / Total possible score) × 100. After conversion, the total, knowledge, attitude, and practice scores were 60.33 ± 12.28, 59.36 ± 14.10, 59.92 ± 13.60, and 64.66 ± 16.74, respectively (Table 3). The lowest subdimension scores were for oral medications and radiographic examinations in knowledge (54.93 ± 16.01) and acceptance of dental procedures during pregnancy in attitude (53.10 ± 15.88), both below the passing threshold (Table 4). To further explore this aspect, Table 5 provides a detailed breakdown of the items assessing acceptance of dental diagnosis and treatment during pregnancy.
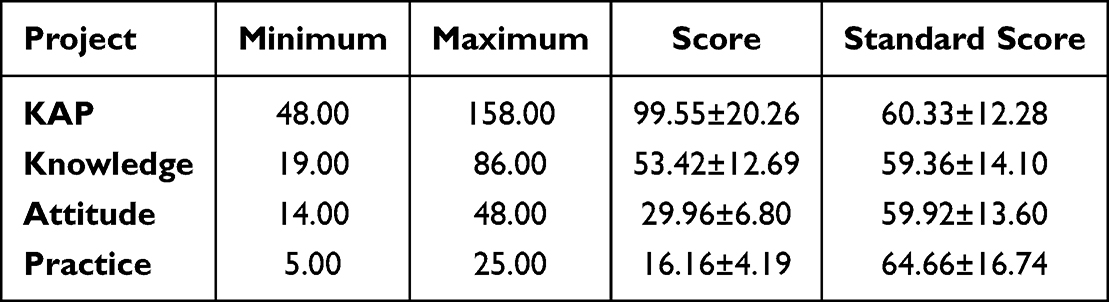 |
Table 3 Scores of Dimensions in Pregnant Women |
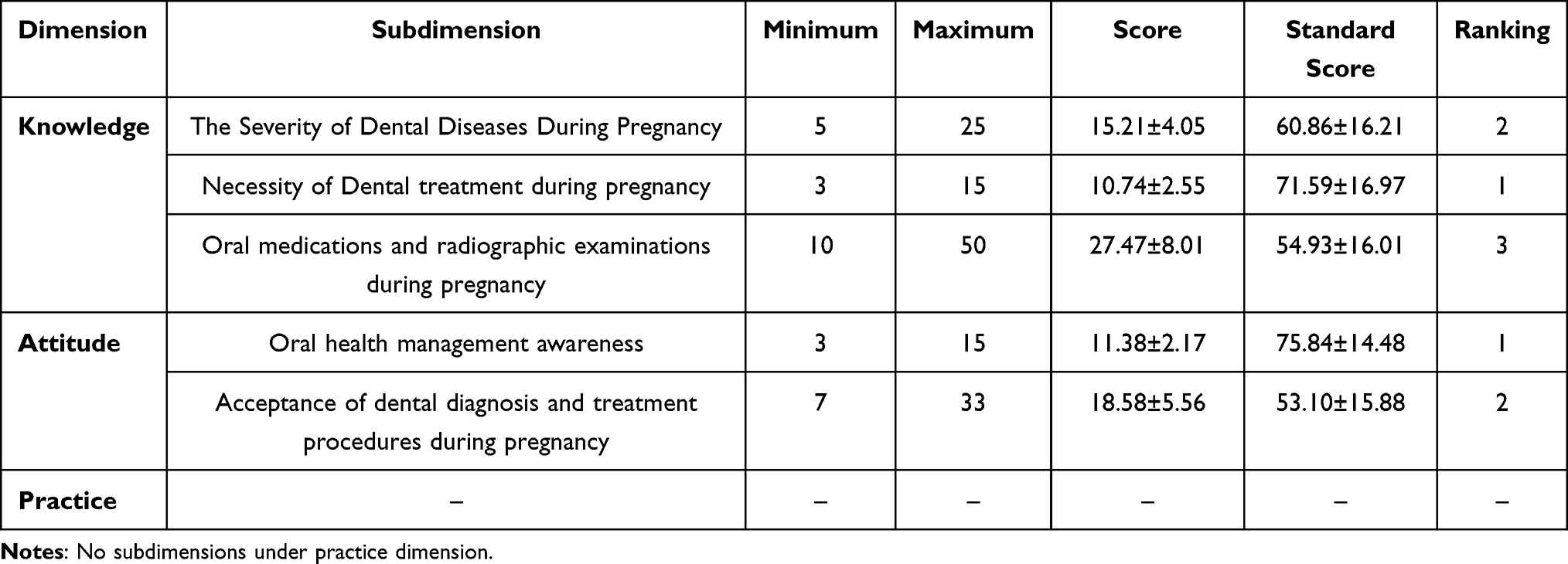 |
Table 4 Scores of Subdimensions in Pregnant Women |
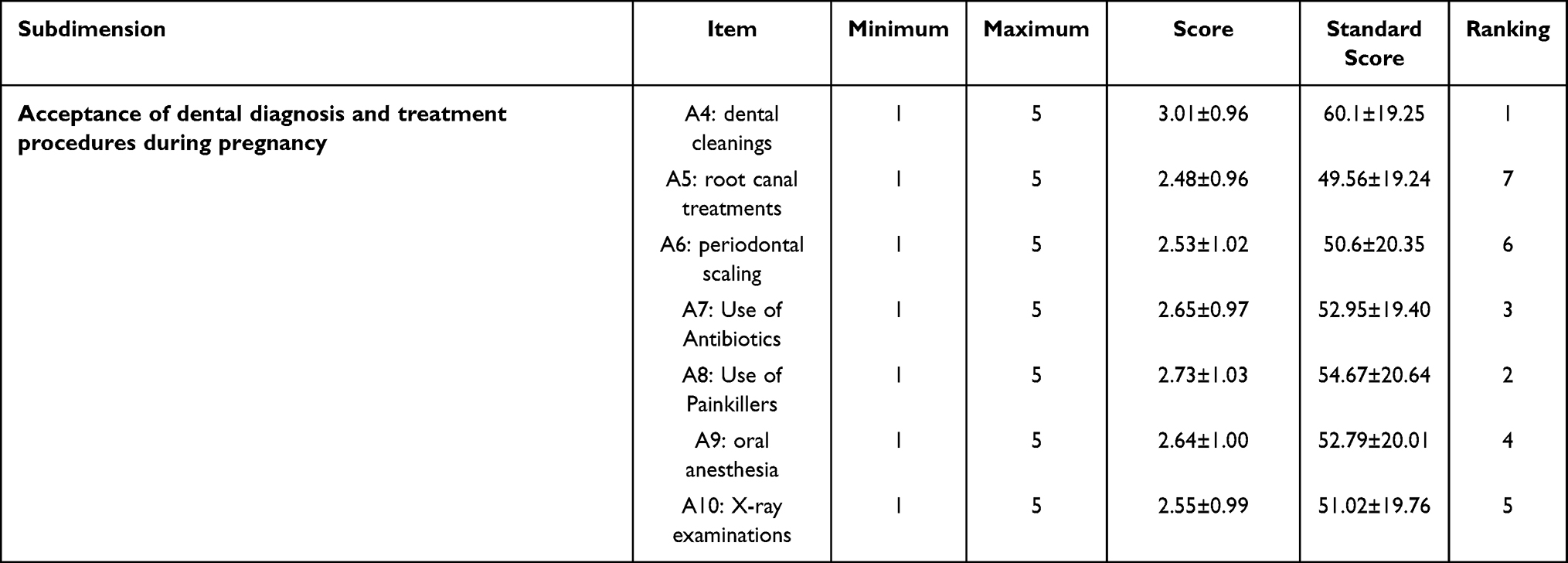 |
Table 5 Item Scores on Acceptance of Dental Diagnosis and Treatment During Pregnancy |
Knowledge Dissemination Channels and Treatment Concerns
Medical professionals and online new media were the most preferred channels for pregnant women to access oral health information (Figure 2). However, many participants expressed concerns about dental treatment during pregnancy: 74.93% were worried about safety, 40.73% cited inconvenience, and 39.95% reported fear. Smaller proportions mentioned time constraints (19.58%) or believed symptoms would resolve after childbirth (16.45%) (Figure 3).
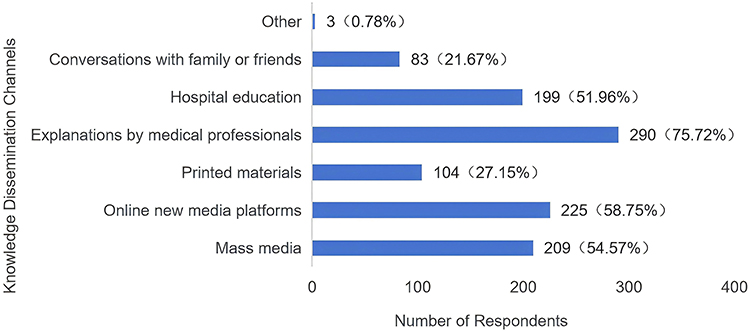 |
Figure 2 Knowledge Dissemination Channels Among Pregnant Women. |
 |
Figure 3 Treatment Concerns in Pregnant Women. |
Correlation Analysis of Knowledge, Attitude, Practices, and Dental Anxiety
A statistically significant positive correlation was observed between knowledge, attitude, and practices (P < 0.01). In contrast, a significant negative correlation was found between dental anxiety and the Knowledge, Attitudes, and Practices (KAP) (P < 0.01) (Table 6).
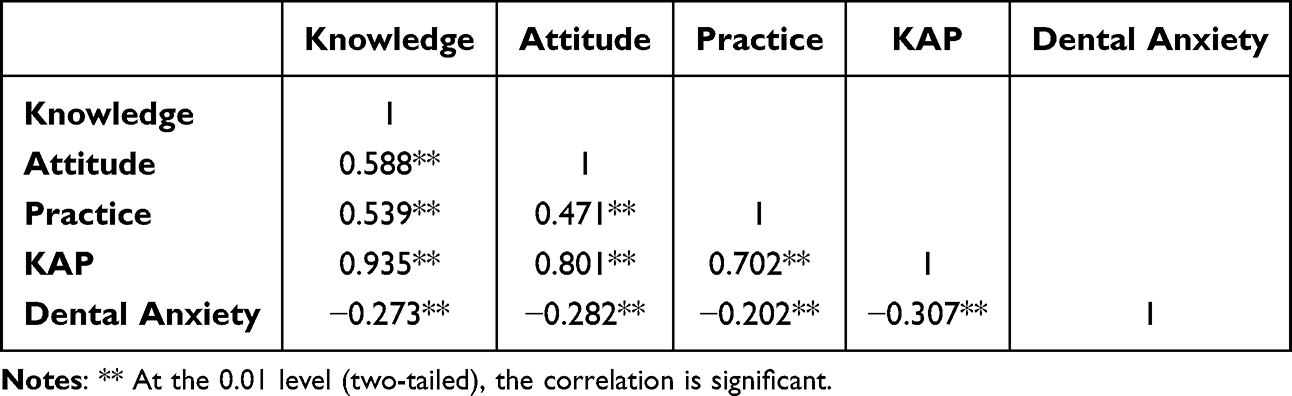 |
Table 6 Correlation Analysis of Knowledge, Attitude, Practices, and Dental Anxiety |
Univariate Analysis
The results revealed that seven factors—residence, educational attainment, family income, payment method, employment status, medical professional background, and pregnancy intention—significantly influenced pregnant women’s knowledge, attitude, and practices (KAP) regarding dental diagnosis and treatment (P < 0.05) (Table 1).
Multivariate Analysis
Multiple linear regression analysis (Table 7) showed that a medical professional background (β = 10.410, p = 0.001) and planned pregnancy (β = 5.612, p = 0.008) were positively associated with higher KAP scores, whereas dental anxiety was negatively associated (β = –1.235, p < 0.001). Compared with women holding a postgraduate degree or above, those with a high school/vocational education and junior high school or below had KAP scores lower by 10.366 (p = 0.013) and 28.505 (p < 0.001), respectively.
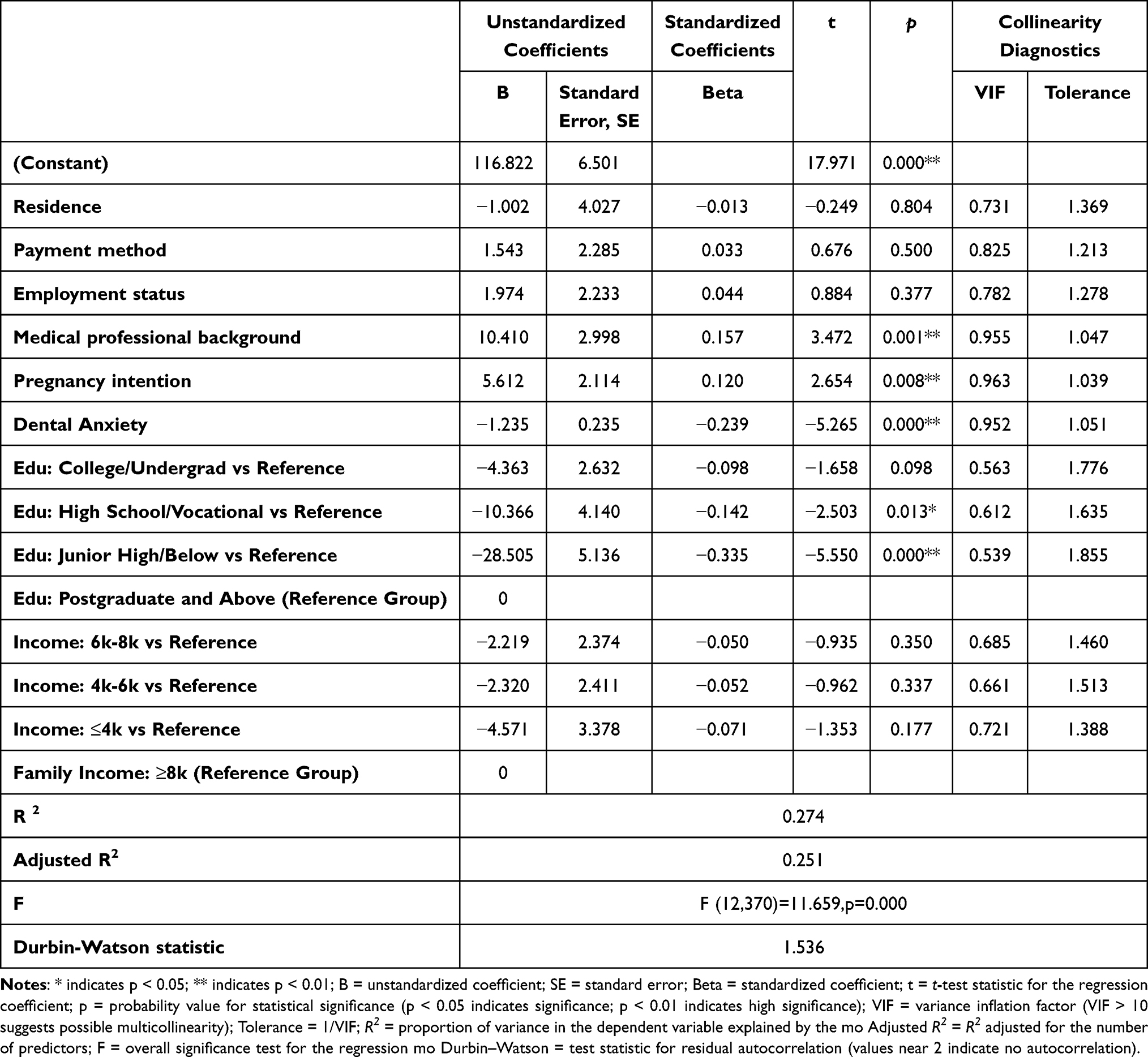 |
Table 7 Results of Multivariate Analysis |
Discussion
Current Status of KAP Regarding Dental Diagnosis and Treatment for Pregnant Women
This survey revealed an average knowledge score of 59.36 ± 14.10 (Table 3), which falls below the threshold for adequate knowledge, indicating a limited understanding of dental diagnosis and treatment during pregnancy. Moreover, further analysis showed that the lowest levels of knowledge pertained to the use of oral medications and radiographic examinations (Table 4), consistent with findings reported in clinical practice. Misconceptions or limited awareness concerning the use of local anesthetics, anti-inflammatory analgesics, and radiographic procedures may be key factors contributing to the reluctance of pregnant women to seek necessary dental care.
The average attitude score was 59.92 ± 13.60 (Table 3), just below the passing threshold, indicating that pregnant women’s proactive attitudes toward dental diagnosis and treatment during pregnancy require further improvement. A study by Li Xiaorui et al15 similarly found that pregnant women tend to adopt a conservative approach to dental treatment. Further examination revealed the highest acceptance for dental cleanings during pregnancy. However, acceptance of more invasive procedures, such as oral anesthesia, X-ray examinations, root canal treatments, and periodontal scaling, was relatively low, with standard scores all below 60 (Table 5). These findings suggest that pregnant women are generally more willing to accept conservative procedures, like dental cleanings, which are perceived as less invasive and safer. In contrast, they exhibit greater resistance to procedures they are less familiar with, such as oral anesthesia, X-ray examinations, and intraoral treatments. This is consistent with the knowledge dimension results, highlighting the significant knowledge gaps pregnant women have regarding dental care, particularly about anesthesia and X-rays.
The score for the practice dimension was 64.66 ± 16.74 (Table 3), meeting the passing level, but with room for improvement. Globally, pregnant women have poor oral health care-seeking behavior, with utilization rates of oral health services during pregnancy ranging from 27% to 53%,4 Studies in the United States16,17 show that 23–49% of pregnant women visit dental clinics during pregnancy, with significant state-level variation. Even in countries such as the United Kingdom,18–20 where free dental treatment is available for pregnant women, the utilization of oral health services during pregnancy remains low, ranging from 33% to 61%.
The results of this survey reveal that pregnant women perceive their oral health status as average, with nearly 60% of respondents reporting at least one oral health issue during pregnancy. The most commonly self-reported symptom was gingival bleeding (39.69%) (Figure 1). This finding aligns with previous studies, as clinical research and epidemiological surveys have shown that pregnancy gingivitis is the most prevalent oral condition during pregnancy, with global prevalence rates ranging from 30% to 100%.21
Regarding knowledge acquisition channels (Figure 2), pregnant women are most receptive to promotional methods such as explanations from medical professionals and the use of new media platforms. Future health education initiatives could combine these two approaches by, for example, having medical personnel create engaging, vivid, and intuitive educational videos or skits, which could then be distributed via short video platforms to enhance the effectiveness of oral health education.
As for concerns about treatment (Figure 3), the primary worry remains the safety of dental diagnosis and treatment during pregnancy, followed by a fear of undergoing dental procedures. This finding is supported by numerous qualitative studies.22 Safety concerns further highlight the cognitive gaps pregnant women have regarding treatment, while treatment-related fears can significantly hinder their acceptance of necessary dental care during pregnancy.
Dental Anxiety
In this survey, pregnant women generally exhibited anxiety toward dental treatment, with the highest levels of anxiety associated with two specific procedures: drilling and local anesthesia (Table 2). This finding aligns with previous research. A study by Alratroot et al23 reported that over 90% of pregnant women experienced varying degrees of dental anxiety. Similarly, Al Khamis S’s study24 highlighted that concerns about pain during drilling and local anesthesia were the primary factors contributing to anxiety among pregnant women.
Correlation and multiple linear regression analyses in this study revealed a negative relationship between dental anxiety and pregnant women’s knowledge, attitudes, and practices (KAP) regarding dental diagnosis and treatment (Table 6 and Table 7).These results underscore the critical need for psychological intervention when treating this population. Dentists should prioritize thorough pre-treatment communication, emphasizing the safety of procedures and the risks associated with delaying treatment. Encouraging the presence of family members or friends for emotional support can help patients relax and mentally prepare for the procedure. During treatment, effective pain and discomfort management is essential to alleviate anxiety. Post-treatment, Oral Health Instruction (OHI) should be provided, along with personalized oral care plans tailored to the specific needs of pregnant women.
Analysis of Factors Affecting KAP
This study reveals that pregnant women employed in medical-related professions tend to have better knowledge, attitudes, and behaviors regarding dental diagnosis and treatment during pregnancy (Table 7). Women with a medical background are exposed to more information about oral health care during pregnancy and are more likely to comprehend and apply this information effectively. Their medical knowledge helps them avoid common misconceptions about dental diagnosis and treatment, leading to more positive attitudes and appropriate behaviors.
Pregnant women who planned their pregnancies had significantly higher Knowledge, Attitudes, and Practices (KAP) scores than those who became pregnant unexpectedly (Table 7). Women who planned their pregnancies typically took a proactive approach to gather information about prenatal health before conception and were more likely to address existing oral health issues in advance to ensure optimal oral health during pregnancy. In contrast, women who became pregnant unexpectedly often lacked awareness of prenatal oral health, and the unanticipated nature of their pregnancies made it difficult for them to manage and prepare for their oral health before conception. These findings suggest that the optimal timing for perinatal oral health management should be prior to pregnancy. This includes conducting oral health examinations and addressing existing oral health issues before conception, thereby preventing the exacerbation of oral health problems during pregnancy, which could lead to adverse pregnancy outcomes. Incorporating oral health screenings into routine pre-pregnancy checkups can help address the challenges of diagnosing and treating oral diseases during pregnancy from the outset.
The results of both univariate and multivariate analyses indicate that educational attainment significantly influences pregnant women’s KAP regarding dental diagnosis and treatment (Table 1, Table 7). Studies by Lee H,25 Mousa O,26 Thompson TA,27 and others also highlight that educational attainment is a key factor affecting the utilization of dental services. Pregnant women with higher educational attainment typically have better access to health information, a greater understanding of the risks of oral diseases during pregnancy, and the safety of treatment. They are also better equipped to assess the risks of neglecting oral health issues and the benefits of receiving standardized treatment. This heightened risk perception motivates them to adopt a more proactive attitude toward treatment and to seek professional medical assistance promptly. Analysis by Thompson and colleagues27 indicated that higher educational attainment—specifically completion of at least twelve years of schooling—was linked to a substantially greater likelihood that expectant mothers would obtain professional dental cleaning during pregnancy. Educational attainment is often closely correlated with socioeconomic status, which directly influences a pregnant woman’s access to quality medical services and health resources. Therefore, future interventions should focus on: 1) providing targeted oral health education and creating accessible, diverse, and easy-to-understand educational materials for pregnant women with lower educational attainment; and 2) reducing economic barriers to oral health services, such as by including low-risk, high-benefit procedures like pre-pregnancy oral checkups and dental cleanings in basic medical or maternity insurance coverage.
Strengths, Limitations, and Future Perspectives
The KAP questionnaire used in this research was developed through a rigorous Delphi expert consultation process and demonstrated good reliability and validity, ensuring the credibility of the measurement results. Incorporating dental anxiety as an influencing factor allowed for a more comprehensive understanding of the psychological factors shaping pregnant women’s oral health–related knowledge, attitudes, and practices. Moreover, this is the first study conducted among pregnant women in Harbin, China, providing valuable regional data to the existing body of evidence. However, the use of convenience sampling from a single tertiary hospital may limit the generalizability of the findings. Future studies with larger, multicenter, and randomly selected samples are warranted to enhance external validity and to develop targeted strategies for improving oral health awareness and behaviors among pregnant women.
Conclusions
This study identified key factors influencing pregnant women’s knowledge, attitudes, and practices (KAP) regarding dental diagnosis and treatment in Harbin, China. Educational attainment, medical professional background, pregnancy intention, and dental anxiety were significantly associated with KAP levels, highlighting the combined effects of demographic and psychological factors on oral health behaviors during pregnancy. To address these determinants, China should expedite the development of expert consensus guidelines for oral healthcare during pregnancy, strengthen multidisciplinary collaboration between dental, obstetric, and psychological services, and implement targeted health education and psychological interventions for women with lower education levels, non-medical backgrounds, or elevated dental anxiety.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Fourth Affiliated Hospital of Harbin Medical University (Approval No.: 2025-伦理审查-106; ethics approval code in Chinese). Written informed consent was obtained from all participants prior to data collection.
Funding
This research was supported by Shanxi Province Key laboratory of Oral Diseases Prevention and New Materials (No. KF2020-05).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu B, Han YW. Oral bacteria, oral health, and adverse pregnancy outcomes. Periodontol. 2022;89(1):181–189. doi:10.1111/prd.12436
2. Daalderop LA, Wieland BV, Tomsin K, et al. Periodontal disease and pregnancy outcomes: overview of systematic reviews. J Dent Res. 2018;97(1):20–29. doi:10.1177/0022034517731097
3. Ye D. Medical Research Methods and Clinical Epidemiology.
4. Onwuka C, Onwuka CI, Iloghalu EI, et al. Pregnant women utilization of dental services: still a challenge in low resource setting. BMC Oral Health. 2021;21(1):384. doi:10.1186/s12903-021-01746-2
5. Llena C, Nakdali T, Sanz JL, Forner L. Oral health knowledge and related factors among pregnant women attending to a primary care center in Spain. Int J Environ Res Public Health. 2019;16(24):5049. doi:10.3390/ijerph16245049
6. Frey-Furtado L, Fonseca M, Melo P, Listl S, Pereira ML. Oral healthcare access: self-perceived barriers faced during pregnancy - a systematic review. BMC Public Health. 2025;25(1):1394. doi:10.1186/s12889-025-22593-8
7. Green SB. How many subjects does it take to do a regression analysis? Multivariate Behav Res. 1991;26(3):499–510. doi:10.1207/s15327906mbr2603_7
8. Humphris GM, Dyer TA, Robinson PG. The modified dental anxiety scale: UK general public population norms in 2008 with further psychometrics and effects of age. BMC Oral Health. 2009;9:20. doi:10.1186/1472-6831-9-20
9. Wan K. Dental norms and safety assurance for pregnant patients. Chin J Pract Stomatol. 2018. doi:10.19538/j.kq.2018.02.004
10. New York State Department of Health. Oral health care during pregnancy and early childhood: practice guideline [homepage on the Internet]. Albany (NY): New York State Department of Health; 2006. Available from: https://www.health.ny.gov/publications/0824.pdf.
11. California Dental Association Foundation; American College of Obstetricians and Gynecologists, District IX. Oral health during pregnancy and early childhood: evidence-based guidelines for health professionals. J Calif Dent Assoc. 2010;38(6):391–440.
12. Massachusetts Department of Public Health. Massachusetts oral health practice guidelines for pregnancy and early childhood [homepage on the Internet]. Massachusetts: Massachusetts Department of Public Health; 2016. Available from: https://www.mass.gov/service-details/massachusetts-oral-health-practice-guidelines-for-pregnancy-and-early-childhood.
13. American Academy of Pediatric Dentistry. Perinatal and infant oral health care [homepage on the Internet]. Chicago: American Academy of Pediatric Dentistry; 2021. Available from: https://www.aapd.org/globalassets/media/policies_guidelines/bp_perinataloralhealthcare.pdf.
14. European Federation of Periodontology. The relationship between oral health and pregnancy guidelines for oral-health professionals [homepage on the Internet]. European Federation of Periodontology; 2020. Available from: https://www.efp.org/gum-disease-general-health/oral-health-pregnancy/resources/guidelines-for-oral-health-professionals-29041/.
15. Li X, Chen M, Huang Y, et al. Survey on the attitudes of pregnant women in Harbin city towards the diagnosis and treatment of oral diseases during pregnancy. Maternal Child Health Care China. 2020;35(16):3079–3081. doi:10.19829/j.zgfybj.issn.1001-4411.2020.16.046
16. Lee H, Tranby E, Shi L. Dental visits during pregnancy: pregnancy risk assessment monitoring system analysis 2012–2015. JDR Clin Trans Res. 2022;7(4):379–388. doi:10.1177/23800844211028541
17. Dasanayake AP, Gennaro S, Hendricks-Muñoz KD, Chhun N. Maternal periodontal disease, pregnancy, and neonatal outcomes. MCN Am J Matern Child Nurs. 2008;33(1):45–49. doi:10.1097/01.NMC.0000305657.24613.47
18. Moosavi A, Smith B, Chen C, et al. Barriers to accessibility, affordability, and acceptability of oral health services among pregnant women: a global systematic review. BMC Public Health. 2025;25:22593. doi:10.1186/s12889-025-22593-8
19. Hullah E, Turok Y, Nauta M, Yoong W. Self-reported oral hygiene habits, dental attendance and attitudes to dentistry during pregnancy in a sample of immigrant women in North London. Arch Gynecol Obstet. 2008;277(5):405–409. doi:10.1007/s00404-007-0480-8
20. Rogers SN. Dental attendance in a sample of pregnant women in Birmingham, UK. Community Dent Health. 1991;8:361–368.
21. Wu M, Chen SW, Jiang SY. Relationship between gingival inflammation and pregnancy. Mediators Inflamm. 2015;2015:623427. doi:10.1155/2015/623427
22. Rocha JS, Arima L, Chibinski AC, et al. Barriers and facilitators to dental care during pregnancy: a systematic review and meta-synthesis of qualitative studies. Cad Saude Publica. 2018;34(8):e00130817. doi:10.1590/0102-311X00130817
23. Alratroot S, Alotaibi G, Albishi F, et al. Dental anxiety amongst pregnant women: relationship with dental attendance and sociodemographic factors. Int Dent J. 2022;72(2):179–185. doi:10.1016/j.identj.2021.05.007
24. Al Khamis S, Asimakopoulou K, Newton JT, Daly B. Oral health knowledge, attitudes, and perceptions of pregnant Kuwaiti women: a qualitative study. JDR Clin Trans Res. 2016;1(3):211–217. doi:10.1177/2380084416665075
25. Lee H, Marsteller JA, Wenzel J. Dental care utilization during pregnancy by Medicaid dental coverage in 26 states: pregnancy risk assessment monitoring system 2014-2015. J. Public Health Dent. 2022;82(1):61–71. doi:10.1111/jphd.12483
26. Mousa O. The association of knowledge on oral health and utilization of dental services among pregnant women. J Nurs Educ Pract. 2019. doi:10.5430/JNEP.V9N6P1
27. Thompson TA, Cheng D, Strobino D. Dental cleaning before and during pregnancy among Maryland mothers. Matern Child Health J. 2013;17(1):110–118. doi:10.1007/s10995-012-0954-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Multicenter Cross-Sectional Study on Clinical Characteristics and Disease Burden of 1010 Patients with Moderate to Severe Atopic Dermatitis in Chinese Tertiary Hospitals
Sun Y, Ma S, Wang Z, Cao H, Jiang G
Clinical, Cosmetic and Investigational Dermatology 2026, 19:431875
Published Date: 10 March 2026