")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Factors Contributing to Loss to Follow-Up from HIV Care Among Men Living with HIV/AIDS in Kibaha District, Tanzania
Authors Mandawa MB , Mahiti GR
Received 10 July 2022
Accepted for publication 18 October 2022
Published 9 November 2022 Volume 2022:14 Pages 503—516
DOI https://doi.org/10.2147/HIV.S381204
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Mathew Bernard Mandawa, Gladys Reuben Mahiti
School of Public Health and Social Sciences, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania
Correspondence: Mathew Bernard Mandawa, School of Public Health and Social Sciences, Muhimbili University of Health and Allied Sciences, P.O Box 65001, Da-es-Salaam, Tanzania, Tel +255 654 452 445, Email [email protected]
Purpose: Human immunodeficiency virus/acquired immune deficiency syndrome (HIV/AIDS) remains a global public health challenge and epidemic disease in sub-Saharan African (SSA) countries. Retention in HIV care should be emphasized to reach”, 95-95-95” the Joint United Nations Program on HIV/AIDS (UNAIDS) target by 2030. In Tanzania, in spite of existing strategies to ensure retention, loss to follow-up (LTFU) among HIV-infected men is still a common challenge. With limited studies focusing on men’s population, little is known on their perspectives on factors contributing to LTFU. This study aimed to explore factors contributing to LTFU among men living with HIV/AIDS in the Kibaha district and to try to formulate strategies that work for men.
Methods: The qualitative study using a phenomenological approach was conducted among 16 men with experience in LTFU from three HIV care and treatment clinics located in the Kibaha district. Purposive sampling was used to select informants for semi-structured in-depth interviews from August to December, 2021. The collected data was analyzed thematically.
Results: The findings were grouped into three themes which highlightedthe contribution of individual factors, socio-economic factors and health system factors. These factors include anticipated HIV-related stigma, lack of disclosure of their HIV status to their partners, poor knowledge on HIV care, unbearable antiretroviral (ART) medication side effects, sharing of ART medications with their partners, perceived good health status, financial difficulties, work-related travels, demanding employment schedules, spiritual belief in faith healing, poor conduct among healthcare workers and loss of Care and Treatment Clinic (CTC) cards hindered their use of ART services at clinics.
Conclusion: The findings from this study revealed linked multi-level factors that influence LTFU from HIV care among HIV-infected men. In order to retain men in HIV care, tailored intervention approaches should be formulated.
Keywords: human immunodeficiency virus, HIV care, loss to follow-up, LTFU, contributing factors, HIV
Introduction
AIDS is still a major untreated disease of global public health importance, which contributes to high morbidity and mortality worldwide.1 The Joint United Nations Program on HIV/AIDS (UNAIDS) reports global estimate of 38.4 million people are infected with HIV by 2021 and about two-thirds of them reside in the African region, particularly in sub-Saharan Africa (SSA).2 About 1.5 million new infections occurred in 2021, mostly reported in SSA.2 Therefore HIV/AIDS is considered an epidemic in SSA countries.
Tanzania is one among several developing countries that have a high HIV burden, with a prevalence of 4.7% among adults aged above 15 years, which corresponds to an estimate of 1.7 million people with HIV.3 The HIV prevalence among men (3.6%) is lower compared to that of women (6.0%).4 Despite having lower disease burden, the mortality due to HIV/AIDS among men is higher compared to women.5 Data show that more men died due to AIDS-related illness and this was attributed to poor health-seeking behavior, low treatment coverage, poor adherence, poor retention and high rates of loss to follow-up (LTFU).6,7 In 2019, it was estimated that 81% of men living with HIV knew their HIV status, 78% were on antiretroviral treatment (ART) and 92% had achieved suppression of the HIV virus with no infectious risk, compared to 83–90–92% of the general population.4 This is below the UNAIDS target of “95-95-95” of people knowing their HIV status, receiving ART and achieving suppression by 2030, respectively. The Tanzanian Ministry of Health established approaches in addressing the HIV/AIDS pandemic aimed at reaching the UNAIDS target by increasing accessibility to early HIV diagnosis, post-exposure prophylaxis, treatment, care and prevention that would result in improved welfare and health status of PLHIV.
Although there are known benefits of ART to PLHIV, LTFU has remained a fundamental problem facing HIV care programs in most of the developing countries.8 In 2012, it was declared that LTFU will be one of the key challenges in HIV programs and a leading cause of attrition from ART care in this era.9 In 2019, a study in Tanzania found LTFU among PLHIV to be 35.6% at 33 months since the initiation of ART care.10 Men are more likely to be lost and less likely to be retained in care and achieve virological suppression than women.11–15 This likelihood may be partly influenced by social norms which make them unable to express their feelings towards their health needs.11,16–18 Retention in HIV care minimizes transmission of infections, ART resistance and ultimately reduces AIDS-related mortality.19,20
The government also implements strategies such as increased accessibility to ART, free ART services to reduce the magnitude of LTFU from HIV care however, high level retention of men in HIV care is still not realized.21 As a result of LTFU, the health status of an individual deteriorates and becomes highly infectious to the community due to the decreased CD4 counts and increased viral load. The LTFU is thought to increase following a new HIV care approach of “test and treat” that has been implemented since 2018.22 The findings from studies in developing countries identified multiple-level factors contributing to LTFU that include perceived good health, stigmatization, failure to disclose their HIV status, lack of transport fare to care and treatment clinics (CTC), receiving care at lower-level health facilities, harsh health care workers at their clinics, long waiting times for service at their clinics, spiritual beliefs, use of traditional medicines and employment schedules.20–23 However these factors vary by regions, regional level factors may not be similar to the district level factors hence for developing tailored interventions that reduce LTFU, it is important to concentrate on smaller scales such as district-level factors.24
Most of these factors were studied on the perspectives of women, children and adolescents regarding LTFU from HIV care. However, the perspectives of men who had experienced LTFU and retention challenges have not been studied. Hence little is known on the factors contributing to LTFU among men. This gap necessitated a need for a qualitative study in Kibaha district. Therefore, the purpose of this study was to explore in-depth why men living with HIV stop receiving HIV care. Our study also provide a better understanding of factors and ultimately helps to identify opportunities to formulate strategies that improve men's engagement in HIV care.
Materials and Methods
Study Design and Setting
In order to achieve the purpose of exploring factors that contribute to LTFU from HIV care among men living with HIV, a qualitative study following a phenomenological approach was conducted to study the lived experiences and perspectives of men regarding factors that contributed to LTFU from HIV care.
This study was conducted in the Kibaha district, which is an urban district, among six districts found in the Pwani region, Tanzania. This district is bordered by a highly populated and commercial city, Dar-es-salaam. Administratively, Kibaha district has two councils which are Kibaha town council and Kibaha rural council. In the district, the study involved three-level health facilities which are; Tumbi Regional Referral hospital, Mkoani Health Centre and Kongowe dispensary that serve a big population and have the CTCs with high patient volume within the district. According to the 2017 Tanzania HIV impact survey, the prevalence of HIV in the Pwani region was 5.3% which was higher compared to the national prevalence of 4.8%.25 Town areas, including the Kibaha district in this region, recorded higher prevalence compared to their rural counterparts.
Study Population and Inclusion Criteria
The study population comprised of men living with HIV/AIDS aged above 15 years, who were enrolled in HIV care and who had experienced LTFU from HIV care at the selected CTCs in the Kibaha district since June, 2018. The study participants were referred as LTFU if they had not attended the clinic for at least 90 days after their last appointment date for drug refill, yet were not recorded as dead or transferred-out.26,27
Sampling, Sample Size and Recruitment of the Study Participants
The study used a non-probability, purposive sampling technique to get a heterogeneous sample with information richness from three CTCs within the district. At the CTC of each selected health facility the sorting of clients was carried out by facility data managers and a list of potential informants with a history of LTFU was created by the principal investigator (first author) including those who returned to care and those who were out of care. The list included only men living in the Kibaha district who enrolled between July 2018 and June 2021 This is due to fact that from June 2018, the country initiated a test and treat approach which required people to test and all those infected to be started on treatment regardless of their CD4 counts or viral load, hence this approach resulted in a high volume of clients at the CTC.7
From the list, informants were purposively selected so that to get informants of different experiences, ages, occupations and education levels. The selected informants were tracked by principal investigator and facility trackers, approached, thoroughly informed about the research (topic, objectives and purpose) and requested to participate in the study. Only those men who agreed to participate were scheduled for interviews. A total of 16 informants were interviewed and this final number was determined by the principle of information saturation.28
Data Collection Methods and Tools
The study employed semi-structured in-depth interviews to collect information. This method was useful in exploring detailed information about individual thoughts, behaviors and experience on sensitive issues such as HIV/AIDS.29 Unlike focus group discussions, in-depth interviews offer more comprehensive information and provide a more comfortable atmosphere for conversation.30,31 Data collection using in-depth interview guide was conducted from August to December 2021. The interview guide comprised of four sections (demographic data, individual, socio-economic and health system factors) with open ended questions which were translated from English to Swahili for easier understanding among informants.
The pre-testing of the interview guide was done before actual data collection and involved a lost to follow-up man from Mlandizi Health Centre. Prior to an in-depth interview, each informant signed a written informed consent, then interviewed in a private and quiet place where an informant selected. The interviews lasted between 25 and 55 minutes and all interviews were conducted during the daytime as per the informant’s preference. During interviews, all conversations were audio-recorded and field notes were taken.
Data Processing and Analysis
The collected data were transcribed verbatim within three days after interviews, translated from Swahili to English, and verified by researchers to ensure the essence of the transcription was captured. Correction of discrepancy was done between researchers without changing the meaning of the original information. All transcripts were read to identify and remove all personal details to ensure confidentiality, and were later saved into a password-protected laptop.
Data analysis was done using thematic analysis approach based on pre-conceived themes using computerized qualitative software NVivo 12. The analysis was done by a stepwise process in which a researcher read and re-read all transcripts line-by-line to familiarize with the data. Initial notes were taken and used to generate initial codes. The codes with similar patterns were combined to generate 13 sub-themes. These sub-themes were further combined to form 3 themes which were later reviewed, defined and named to match the pre-conceived themes used as the headings in the results section.32 Example of thematic analysis is shown in Table 1.
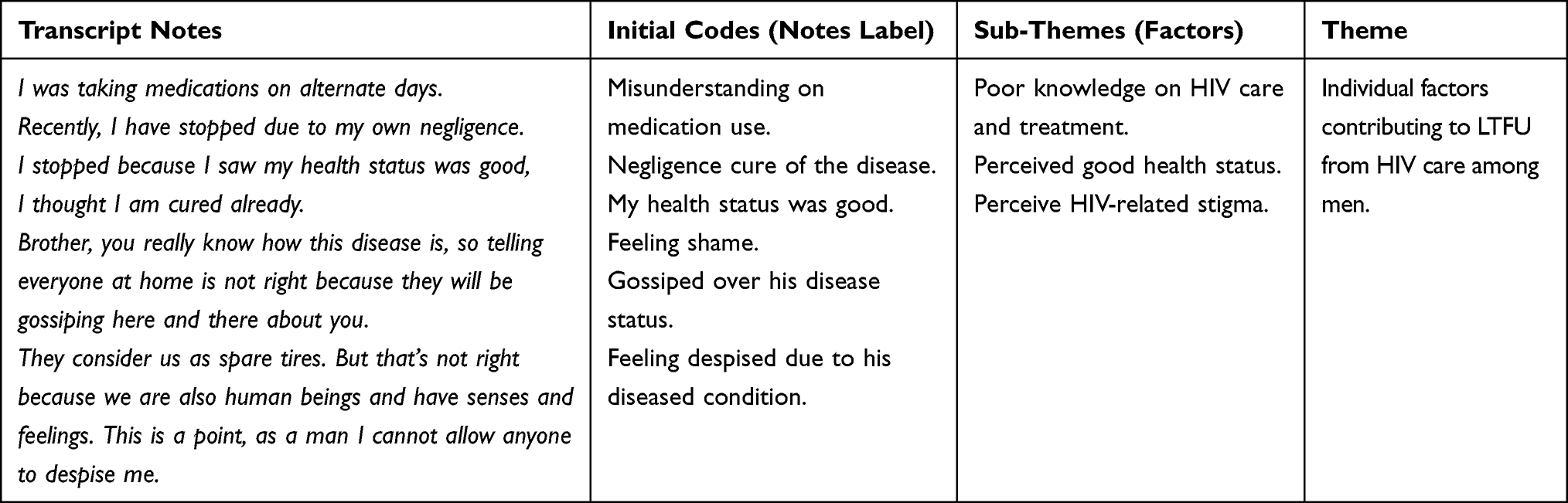 |
Table 1 Thematic Analysis Framework of the Factors Contributing to LTFU from HIV Care |
Ethical Consideration
In line with ethical considerations in research, the study complies with the declaration of Helsinki. Ethical approval for this study was obtained from Muhimbili University of Health And Allied Sciences Institutional Ethical Review Board (IRB) with reference MUHAS-REC-08-2021-820. Permission to access the CTC 2 data at selected CTCs was sought from the Regional Administrative Secretary for Regional Referral Hospital and District Administrative Secretary for Health Centre and dispensary. Local administrative permission was sought from the in-charges of the respective health facilities for data collection. No risk, harm or threat was imposed on study participants and their privacy, autonomy and confidentiality were ensured. The IRB approved participants under 18 years of age to provide consent on their own behalf as emancipated minors. Participation was voluntary and written informed consents were obtained from all informants including those aged below 18 years because they were living independently as married and heads of their families. Informants were assured that their written informed consents included publication of anonymized responses. All written informed consents forms were stored and locked in a cabinet to ensure confidentiality. Permission for audio-recording was obtained prior to interviews. After interviews, participants were given between $2 and $5 as a compensation for transport fare depending on the distance and actual cost used for transport.
Trustworthiness
The validity of our study was ensured by the trustworthiness of the data and findings.28 It is assessed by ensuring credibility, dependability, conformability and transferability.33 In this study, credibility was attained by triangulation of information sources (use of two informants’ groups with experience of LTFU; lost and returned in care and others who did not return in care) and selection of a maximum variation sample to capture the range of the reasons of LTFU informants. Dependability was attained by allowing independent researcher to review and examine research process and data analysis process. Conformability was guaranteed by researchers deriving the interpretations and highlighted every step of data analysis. Transferability was attained by providing clear descriptions of all aspects of the study that make a reader judge the applicability of the findings in other contexts.
Results
Socio-Demographic Characteristics of the Study Informants
A total of 16 men living with HIV/AIDS who experienced LTFU participated in the study. Among them, 6 men were out of care and 10 men returned to care. Their ages ranged between 17 to 56 years with an average age of 36 years. With regard to education level, the majority had primary education, followed by secondary education and above. Only one informant had not attended formal education. The majority of the informants were self-employed, few had formal employment working at private institutions and only one had no formal employment. With regard to marital status, half of the informants were single, one third were married and 2 were divorce and only 1 was a widower. The socio-demographic characteristics of the 16 informants are summarized in Table 2.
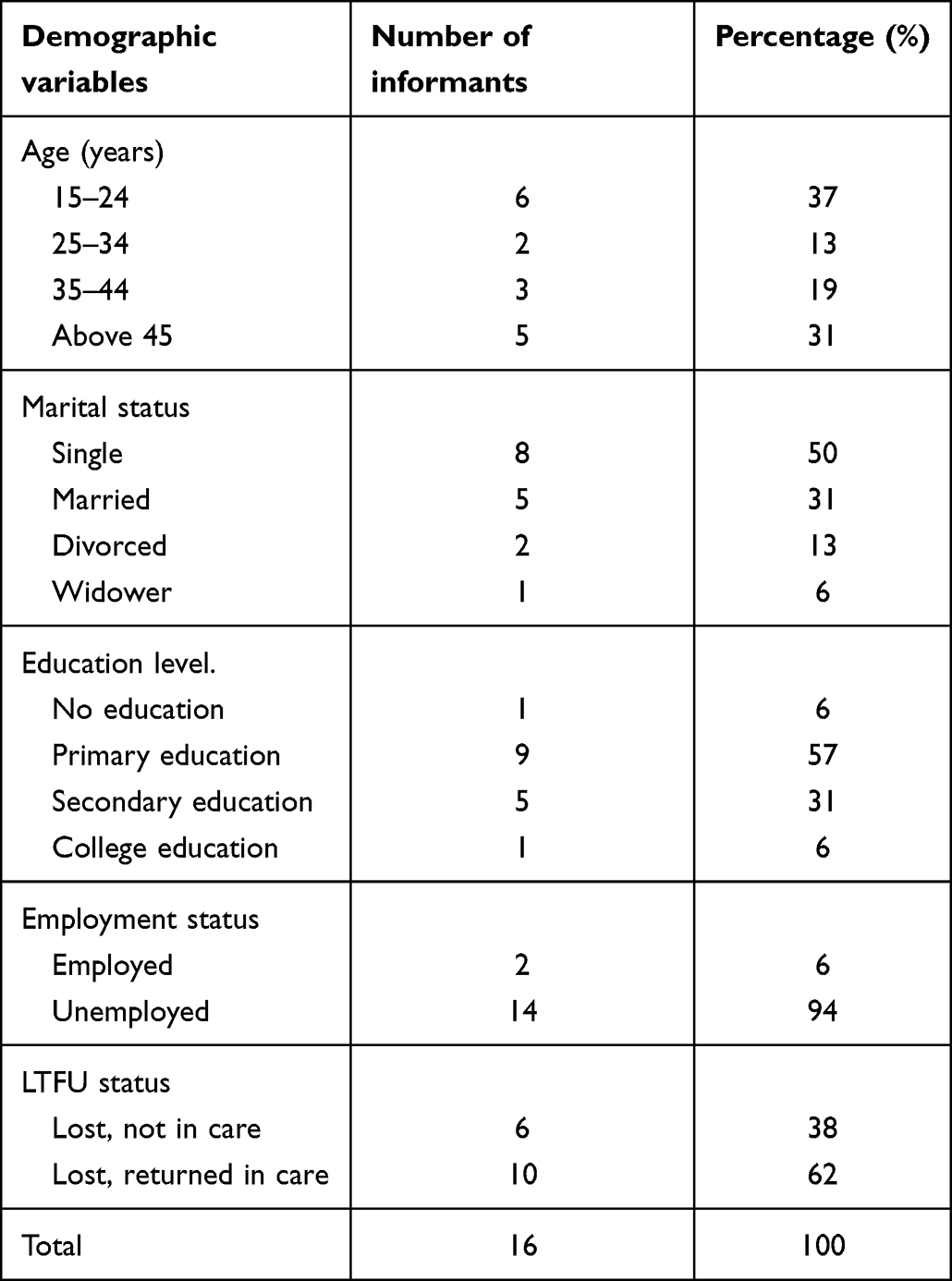 |
Table 2 Socio-Demographic Characteristics of the Study Participants |
Factors Contributing to LTFU from HIV Care
This study explored factors contributing to LTFU from HIV care among men that have been grouped into three themes; individual factors, socio-economic factors and organizational health system factors, as shown in Table 3.
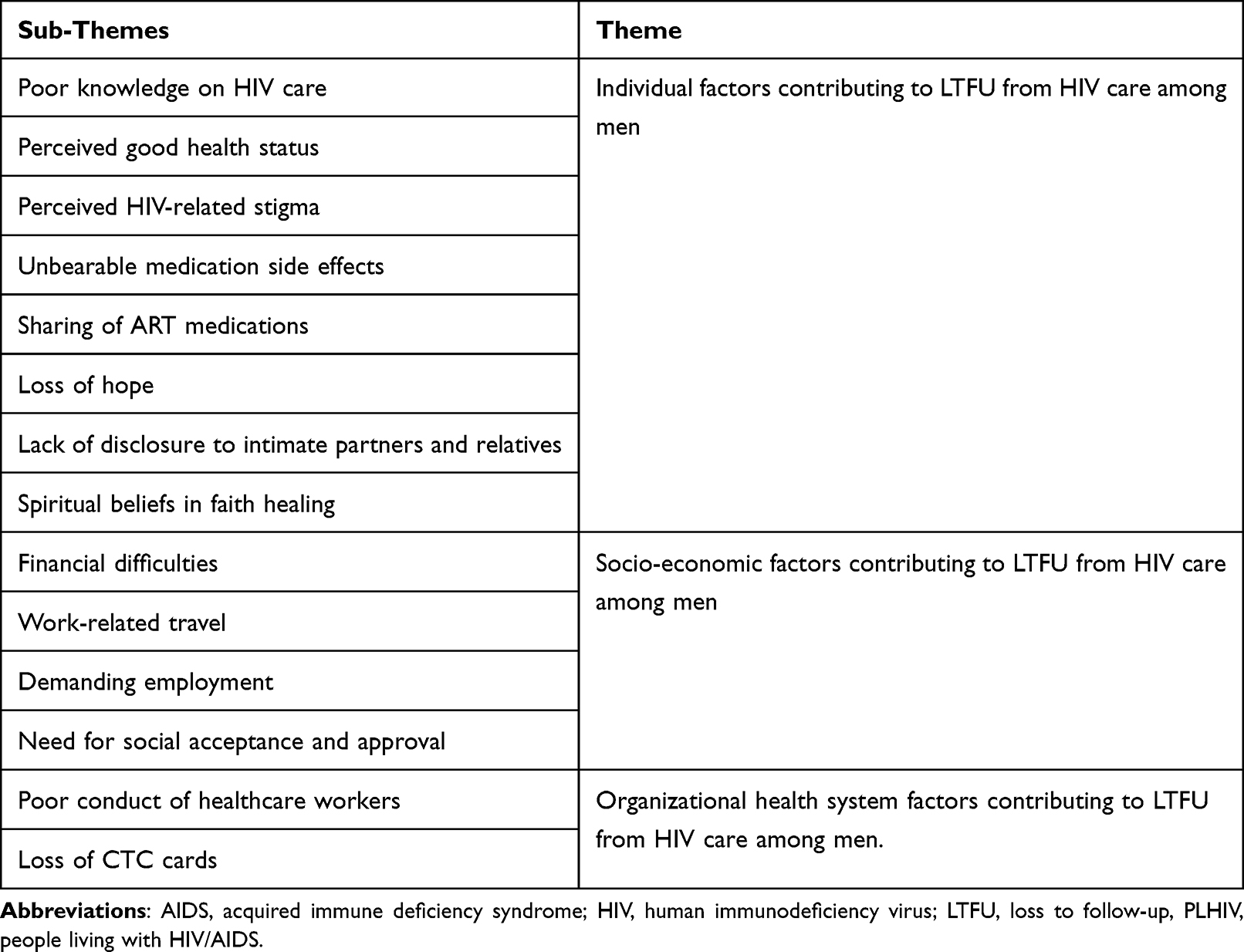 |
Table 3 Themes and Sub-Themes Created from the Study on Factors Contributing to LTFU |
Theme 1: Individual Factors Contributing to LTFU from HIV Care
Informants from this study explained various factors that contributed to stopping attending HIV care at their respective clinics. These factors included: poor knowledge on HIV care and treatment, perceived good health status, HIV-related stigma, unbearable medication side-effects, sharing of medications with their partners, spiritual beliefs in faith healing and lack of disclosure to intimate partners.
Poor Knowledge on HIV Care and Treatment
Most of the informants could not explain proper use of medications or good adherence during interviews. Poor general knowledge on HIV/AIDS made them stop attending their HIV care clinics because they thought use of ART medication was for a limited time. Other informants compared their initial health status to their current status and considered their improvement as a sign of a cure and decided to stop medications. One of the informant, who was LTFU and not returned to HIV care did not know importance of having good adherence to ARVs and decided to take last refill medications on alternate days before he ceased his CTC visits.
He explained:
“I still had some medications that I took when I went to the clinic. I was taking them on alternate days. Sometimes I did not take them because I felt well.” (41 years, primary education)
Another informant with 20-years who returned to care reported that his ignorance contributed to LTFU. He thought only using medications for a specific period would have cured him completely. He said:
“As I told you earlier, it was just ignorance, I took all the medications that I was given until I completed them however, it was just difficult to get back to taking other medications. It was not possible again.” (20 years, secondary education)
Perceived Good Health Status
Some informants expressed an absence of emerging recurrent illnesses, symptoms and perception of having good health after using ARVs for certain period of time as a contributing factor to LFTU, particularly those who started medication when they were critically ill or having recurrent illnesses. Improved health status made them see no benefits offered with CTC visits. As one informant who had multiple episodes of LTFU and is currently in care explained:
“Recently, I have stopped due to my own negligence. I stopped because I saw my health status was good. I thought I was cured already, so I was asking myself why I should continue taking medications.” (44 years, college education)
Another informant with experience of LTFU and returned to care also said:
“You know what, when I went back home from workplace I used to forget to take my medications because I was tired of them. I felt like I was cured though I knew I was supposed to take them all the time.” (55 years, primary education)
HIV-Related Stigma
Most of the informants reported anticipated self-stigma that prohibited them from disclosing their HIV status, hence they failed to get social support from their sexual partners and family members. In order for them to feel normal as did other family members, they decided to stop attending clinic visits for medication pick-up and ceased taking their medications as prescribed. As one of the informants who never returned to care explained:
“Brother, you really know how stigmatizing the HIV disease is, so telling everyone at home is not right because some relatives will be talking here and there about your disease status.” (20 years, primary education)
Another informant reported fear of being a topic of discussion in social groups, pointed fingers at the streets and being gossiped about because of their health status had really compromised their visits to CTC. Fear of being discriminated against in various social activities had also contributed to the discontinuation of clinic visits, as one of the participants who was a long-distance truck driver described:
“When you tell your neighbors or relatives about your HIV status, you know we differ; some of them will pray for you to get on bed with serious disease so that they get to gossip over you. And you never know your relative’s weakness, so you may tell him/her then he/she becomes a person of gossip.” (54 years, primary education)
Unbearable Side Effects of the ART Medications
Informants reported to have experienced side effects of ART medications and their fear towards developing more serious adverse effects contributed to cessation of medications. They reported excessive weight gain that accompanied a loss of libido and erectile dysfunction, reduced self-confidence, affected their sexual relationship. One informant who experienced LTFU and returned to care explained:
“I started these medications with 44kg body weight but now my weight is 90kg. This is too much for me and when I sit in my vehicle, people claim that I am having diabetes mellitus.” (54 years, primary education)
A young man who was LTFU and returned to care decided to stop medications due to enlargement of the breast (gynaecomastia) explained how medications affected him psychologically and was not able to have social interactions with fellow men. He narrated:
“Those medications enlarged my breasts and this was a reason that made me stop taking them and drop out of school. It started when I was taking my medications from another CTC and shifted with it to this clinic, but I did not get any help for this problem and I lost hope to continue using these medications, so I decided to stop.” (23 years, secondary education)
Lack of Disclosure of HIV Status to Intimate Partners and Close Relatives
The majority of informants hide their HIV status from their sexual partners and wives due to fear of being rejected and divorced. Their fear of being stigmatized pushed them away from HIV care because they did not want to inform any close family member and hide their HIV status. To keep their status a secret, they decided to stop attending a CTC for HIV care. One of the informants could not disclose his status to his wife, thus, he hid his ART medication at his brother’s house, but later his wife suspected. For him to keep his status hidden, he decided to stop taking medications at all. He explained:
“My wife once saw the ART pills but she did not know if I picked them up from CTC clinic. I stored my medications to my brother’s house for some time since April but later I was busy with work and I stopped taking medications.” (41 years, primary education)
Loss of Hope for Definitive Cure of the HIV Disease
Some informants lost hope of living with a life-long disease that requires lifetime treatment, so they decided to quit attending their clinics for drug refills. Long-term medication use had affected some men psychologically and led to depression and suicidal thoughts. As one young informant who was LTFU and returned to care explained:
“I found myself losing hope of taking medications and decided to stop taking them. On my side it was a hard situation; sometimes I was thinking of killing myself and I did a self-killing trial but God did not want me to die at that moment.” (23 years, secondary education)
Another informant said:
“Sometimes it is due to improper thinking, you just agree to die of a disease, we lose hope and it discourages taking ART medications when we see our fellow client whom we take medications together has died.” (55 years, primary education)
Another informant who was divorced (lack of partner support) by his wife after being diagnosed with HIV explained:
“It was depressing thoughts, only thoughts that brought me in depression, I was thinking my wife was the one who gave me this disease, and then she ran away from home suddenly.” (56 years, primary education)
Sharing of ART Medications with Intimate Partners
Use of partner’s ARTs was also explained by a client as a contributing factor to stop accessing ART services at the designated CTC. Since his partner knew his HIV status and was given a 3-month-package of medications, she decides to share them with her husband. An informant, who was LTFU and never returned to care was using his wife’s medications that are regularly offered by the clinic she attends, explained:
“Since she has the same disease and attends at CTC regularly, we use her medications together on alternate days.” (33 years, primary education)
Spiritual Beliefs in Faith Healing
One informant reported spiritual beliefs that aligned with spiritual teachings (believers would live free of diseases) contributed to loss-to-follow-up among believers. On informant said he was convinced with such a belief when his medications were completed and had serial sessions of spiritual teachings that assured him of disease-free-life in faith. He reported that:
“There were religious teachings that I would believe in being healthy even if I stopped taking medications. There were two religious leaders who taught me to believe in God that i will be fine. I am a son of God, I do not use medications. If I die or get healed, God will save me.” (17 years, primary education)
Another informant also said:
“I put my faith in these medications because I am responsible for taking them but I believe there is a day that I will be healed.” (44 years, college education)
Theme 2: Socio-Economic Factors Contributing to LTFU from HIV Care
The study found that financial difficulties, demanding employment, work-related travel for longer time, spiritual belief in faith healing and need for social acceptance were the socio-economic factors which contributed to LTFU from HIV care.
Influence of Financial difficulties
Majority of informants reported that financial constraints hindered them from attending ART clinics for medication refills. Since men are the ones responsible for the family's financial matters, they could not ask for financial help, including transport cost or for family needs from their partners, hence they decided to stop visiting CTCs and alternatively spend the time in earning activities. As explained by one informant who experienced LTFU and never returned to care:
“It hurts missing a clinic appointment, but I need money so I comforted myself that missing medications only for two or three days had no problem and I decided to go for work. Poverty costs poor people.” (41 years, primary education)
Another informant of 17 years of age reported that a lack of transport cost to his CTC contributed to his decision to stop attending clinic to take medication. He explained:
“Nowadays it is too hard to get money, poverty contributed to stop going to my clinic for medications refill.” (17 years, primary education)
Work-Related Travel Hindering Clinic Visits
Informants working as long-distance truck drivers experienced difficulties in attending their clinics for medication collections because of being out of their residential areas. They found it challenging to access medications at their destinations, where it was not possible to have medications for the time that matched the duration of their stay in that particular country, hence they stopped using medication and were lost by their respective clinics. One informant who was traveling to nearby countries explained:
“I traveled to Uganda for work and I stayed there for like 4 months, but all the clinics there were stigmatizing me. When I arrived at the CTC, I was only asked a lot of questions but not given medications. I really went through challenges in Kapeka.”(54 years, primary education)
Similar narrations were given by a man who was LTFU and not returned to care:
“For me to stop medications, was due to my employment. I stopped taking my medications for real. I was called through phone to report at a work station at a far place from the clinic and a day that I was supposed to start working coincides with the clinic date. So I did not look back and I traveled.” (41 years, primary education)
Demanding Employment
Overlapping of clinic appointment dates and work schedules was reported to be a contributing factor. Competing priorities between work and ART clinics made clients choose work over clinic visits, thus contributing to LTFU from HIV care. A-17-year-old client who was working at a local music library narrated how his work limited him from attending CTC for medication refill. He said:
“This work also prohibits me from visiting my clinic. I do not get time to attend clinics. There were days where I was supposed to stay at the clinic up to 01.00pm and failed to be in my workplace.” (17 years, primary education)
Another informant who was not currently in care also explained:
“Sometimes I wish to visit my clinic, but my work is so demanding. You may find when I am required to attend at CTC on the same day I am also supposed to go for a work so I choose to go for work so that I can get a bread for my family.” (41 years, primary education)
The Need for Social Acceptance
Some informants reported to secure social approval to their company at work and streets that they were also physically fit without taking medications, hence they decided to stop their clinic visits. Social influence from friends and social pressure from their peers were reported as contributing factors to LTFU from their clinics for HIV care. One informant who had a history of LTFU and returned to care reported peer pressure from his young colleagues at school:
“After school, I did not go back home where I was attending my clinic, I went to reside in the street as other peers do, their influence brought me to the street escaping from home where I was taking medications.” (17 years, primary education)
Theme 3: Organizational Health System Factors Contributing to LTFU from HIV Care
This study explored two organizational health system factors that contributed to LTFU from HIV care that were poor conduct among health care workers and misplacement or loss of CTC cards.
Poor Conduct Among Healthcare Workers
Informants reported that healthcare workers addressed them with less courtesy, sometimes communicating harshly and shouting at them when they appeared to miss visits or failed to visit at their scheduled dates. Inappropriate communication seemed to be unwelcoming and disappointed clients. As one informant who lamented on negative attitudes and unfriendly behaviors of healthcare workers explained:
“Leave aside lack of fare, I faced another challenge when healthcare providers started shouting at me loudly saying I missed out on my scheduled dates, they said I was stubborn and lost in care. That is an embarrassment to me, you know I am a man. To avoid all these, if you miss out for a single day, you do not go at all.” (44 years, college education)
Misplacement and Loss of CTC Cards
Some informants reported that CTC cards were required to identify them during clinic visits for drug refills so when they lost or misplaced their cards, they failed to attend their clinic visit. They claimed that it was not possible to get their medications without their cards, and hence they decided to discontinue attending clinics. One informant who has returned to care after getting his card some months later narrated:
“As I told you, I forgot my identity CTC card therefore I had no medications take from the clinic. I did not make any follow-up on how I could be given medications because medication refills work only when you have your CTC card.” (30 year, no formal education)
Another young man who was out of care because he had not found his CTC card explained:
“I went to religious training school where I lost my CTC card, I tried to look after it but I did not find it so I feared visiting CTC for medication refill. When I was at school, my card got lost and I stopped attending clinic to take medications.” (17 years, primary education)
Discussion
The purpose of our study was to explore factors that contributed to LTFU from HIV care among men living in Kibaha district. These factors were individual level, socio-economic and organizational health system factors based on male perspectives.
Individual Factors Contributing to LTFU from HIV Care
The individual factors explored in this study include poor knowledge of HIV care, perceived good health, HIV-related stigma, ART medication side effects, sharing of ART medications, spiritual beliefs in faith healing and lack of disclosure to intimate partners and close relatives. The study findings are consistent with the findings reported from other studies conducted among the general population in developing countries.21,34
Due to poor knowledge on HIV care, lost to follow-up men thought there was a specific duration for using ART medications and their improved health status signified complete cure of the disease. This may be due to limited time that is offered to clients when attending clinic for medication refill, hence they lack thorough counseling sessions that could have improved their knowledge on adherence. Unbearable side-effects of the ART medications such as enlarged breasts and fear of developing more serious side effects, including obesity and diabetes, were explored in our study. This is in agreement with other studies done in other places in SSA.34–37 Sariah et al in their study among women lost in Option B+ also argued that intolerance to side effects of ARTs pushed women out of care. We also found that men stopped attending their clinics because of sharing of ART medications with their intimate partners. This does not only affect treatment regimen but also affects individual health of the partners as no prompt treatment is taken. This finding is consistent with what had been reported by Nyamuhanga et al in his study conducted in the Dar-es-salaam, Tanzania. He argued that men tend to use their wives’ ART medications or buy from other clients who have double registrations at different CTCs while no study conducted among women reported this incidence.16
Lack of disclosure of HIV status due to fear of HIV-related stigma was found to affect medication adherence and resulted to LTFU from HIV care. Interviewed men in our study revealed distrust to their partners and reported fear of relationship break-up and social separation hence led them to miss positive social support from their significant other. The same findings were described in other studies conducted in East African countries and elsewhere.34,37–39 The study on retention challenges among women conducted in Moshi, Tanzania by GAK et al reported that women tend to disclose their HIV status to their partners or father of their babies, unlike men, as found in our study, who fear disclosing their status to their partners or wives.37 Another study conducted among the general population also reported the fear of disclosure of HIV status made clients uncomfortable and contributed to LTFU.38 The masculine character of men that is socially constructed that men should never be weak before women influenced disclosures.16
This study also found that men prefer to attend clinics that are located far away from their residential areas so that they could not be identified by other clients and healthcare workers due to anticipated self-stigma. This increased the transport cost and time to clinics. These findings are contrary to some studies conducted among LTFU women that have indicated long distance access to HIV care contributed to LTFU from HIV care.34,37,38,40 While evidence show that long distance influenced LTFU among women, men find it comfortable to attend to distant CTCs so that they could hide their identities. This inconsistency could be due to a gender-based population that was interviewed in our study compared to women who absolutely depend on their male-partners for financial support.
Socio-Economic Factors Contributing to LTFU from HIV Care
This study explored socio-economic factors including financial difficulties, long-stay work-related travel, demanding employment, spiritual beliefs in faith healing and need for social acceptance.
Financial difficulties to access basic needs for their families and cover transport cost to CTCs made a choice to continue taking medications difficult and resulted in LTFU. This finding is similar to what was explained in other studies and they argued food shortage due to poverty hindered medications adherence among clients.34 Since men are socially constructed to be responsible for financial matters of the family, they need to work continuously and ensure the family gets basic needs. When there are competing interest between clinics and any earning activity then men will choose to earn and leave behind their clinic appointments.
Work-related travels for longer time outside of their residence interfered with clinic attendance. This is consistent to what has been described by Makumbang et al in his study on conceptualizing factors affecting retention in Zambia. He reported that long-distance truck drivers defaulted due to long stays on trips to work.34
This study found that religious belief in faith healing after receiving prayers from religious leaders and encouragement that insisted on God’s healing. This finding is supported by a study conducted in Tanzania by Sariah et al who also found that religious faith facilitated women to stop medications in option B+.39 However, other evidence emphasize on the roles of religious beliefs in promoting adherence to medications and retention in care.41 Similarities in these findings could be due to similar social norms and same kind of teachings that are related across the country.
Also our study found that men needed social acceptance and approval to their social groups, their relatives and friends. LTFU men were encouraged to stop taking medication and defaulting on their clinic appointments, as opposed to women who required social support from their partners, close relatives and friends to adhere to ART medications.34 This study found that men were convinced to stop taking medication when they fail to perform their duties normally. Men were also encouraged to stop ART in order to look physically fit and get rid of some medications side-effects such as oversleeping that interfere their work performance.
Organizational Health System Factors Contributing to LTFU from HIV Care
This study found poor conduct among healthcare workers that included negative attitudes and impolite reactions towards men who had either missed their dates or came out of scheduled date for refill made the clients fear to attend clinics when they missed their scheduled dates. This finding is supported by Denis et al in his study on LTFU from care among people living with HIV conducted in Uganda.21 He argued that the manner in which healthcare providers handle clients influenced them stopping attending clinics.21
This study also found that men who had lost or misplaced their CTC cards were afraid to visit their clinic for medication refills because they knew medication could only be provided when they had CTC cards. They presumed that no CTC cards meant no ART services at their clinics, so they decided to stop attending their clinics when they lost or misplaced their CTC cards. This is consistent with findings from a study conducted by Kisigo et al that revealed policy issues with regards to access to ART and transfer of clients to other clinics.37
Other studies in SSA countries based on general population pointed out other health system factors such as lack of confidentiality and privacy among healthcare workers and long waiting times at CTCs contribute to LTFU, however none of these have been reported by men in our study.34,35,37–39 This can be due to significant improvement that the government and implementing partners have correctively done in addressing health-system related factors such as establishing a number of CTCs, training healthcare workers on costumer care and providing quality services.
The strength of our study is that researchers recruited and interviewed men who experienced LTFU who were either out of care or returned to care recently, hence explored views of different data sources. The researchers involved participants from different health care facilities within Kibaha district to maximize data sources. Our findings were drawn from a men’s population which is mostly impacted by the gaps in HIV care. We also involved a sample with real life experience hence minimized a chance of recall bias. Despite these strength, we also encountered limitations. Our study had small sample size and was unable to recruit majority of the men who were LTFU and never returned to care by the period of data collection. Their participation could give more insight to other factors that prohibited them from returning back to HIV care.
Conclusion
While there is a wide expansion of HIV care that has significantly reduced the rate of LTFU among women, men have still lagged behind. The findings have enlightened the existence of complex multi-level factors contributing to LTFU among men which require tailored interventions to reduce incidences of LTFU. Our study enlightened sharing of ART medications with their intimate partners and the need for men to have social approval contributing factors from HIV care. In order to attain 100% retention, which is crucial in prevention of HIV transmission, addressing these factors is inevitable.
In light of our findings from this study, we recommend CTC management to emphasize on tailored counseling educational sessions during clients visits, emphasize and implement community-based ART delivery to tackle stigma, establish on-transit ART centres at our borders for long-distance truck drivers and emphasize healthcare workers to adhere to professionalism and good conduct. There is also a need for further research on the effectiveness of the counseling sessions.
Acknowledgments
The authors would like to thank the Muhimbili University of Health and Allied sciences for reviewing our research proposal and giving ethical approval for this study. We thank Pwani Regional and District Administrations for giving permission to conduct our study in Kibaha district and selected health facilities; Tumbi Regional Referral Hospital, Mkoani Health Centre and Kongowe dispensary. We also thank our study participants for their cooperation during data collection and researcher assistants who helped in tracking lost to follow-up clients who were involved in this study.
Author Contributions
All authors made a significant contribution to the work reported from the conception, study design, execution, acquisition of data, analysis and interpretation, took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no competing interests in this work. No funding was provided by any financial or academic institution for this study.
References
1. Pandey A, Galvani AP. The global burden of HIV and prospects for control. Lancet HIV. 2019;6(12):e809–e811. doi:10.1016/S2352-3018(19)30230-9
2. UNAIDS. Global HIV statistics. Fact Sheet. 2021;2021:1–3.
3. United Nations Programme on HIV/aids. UNAIDS. UNAIDS data 2021; 2021:4–38.
4. UNICEF. AIDS HIV and AIDS; 2020:1–6. Available from: https://www.unicef.org/tanzania/media/2436/file/HIV.Programme.FactSheet.pdf.
5. Nachega JB, Adetokunboh O, Uthman OA, et al. Community-based interventions to improve and sustain antiretroviral therapy adherence, retention in HIV care and clinical outcomes in low- and middle-income countries for achieving the UNAIDS 90- 90-90 Targets. Curr HIV/AIDS Rep. 2016;13(5):241–255. doi:10.1007/s11904-016-0325-9
6. Kusemererwa S, Akena D, Nakanjako D, et al. Strategies for retention of heterosexual men in HIV care in sub-Saharan Africa: a systematic review. PLoS One. 2021;16:1–13. doi:10.1371/journal.pone.0246471
7. Conserve DF, Issango J, Kilale AM, et al. Developing national strategies for reaching men with HIV testing services in Tanzania: results from the male catch-up plan. BMC Health Serv Res. 2019;19(1):1–10. doi:10.1186/s12913-019-4120-3
8. Swartz M. PDF view of the file Chapter 8.pdf. Open books; 2022:194–195. Available from: https://www.rcipress.rcipublisher.org/index.php/rcipress/catalog/view/53/30/149-1%0Ahttps://openbooks.uct.ac.za/uct/catalog/view/29/43/1431-1.
9. Kalinjuma AV, Glass TR, Weisser M, et al. Prospective assessment of loss to follow-up: incidence and associated factors in a cohort of HIV-positive adults in rural Tanzania. J Int AIDS Soc. 2020;23(3):1–10. doi:10.1002/jia2.25460
10. Ndege RC, Okuma J, Kalinjuma AV, et al. Failure to return pillbox is a predictor of being lost to follow-up among people living with HIV on antiretroviral therapy in rural Tanzania. HIV Med. 2022;23(6):661–672. doi:10.1111/hiv.13223
11. Chen M, Dou Z, Wang L, et al. Gender differences in outcomes of antiretroviral treatment among HIV-infected patients in china: a retrospective cohort study, 2010–2015. J Acquir Immune Defic Syndr. 2017;76(3):281–288. doi:10.1097/QAI.0000000000001500
12. Moraes DC, de A Oliveira RC, De Costa SFG. Adherence of men living with HIV/AIDS to antiretroviral treatment. Esc Anna Nery Rev Enferm. 2014;18(4):676–681. doi:10.5935/1414-8145.20140096
13. Mugisha V, Teasdale CA, Wang C, et al. Determinants of mortality and loss to follow-up among adults Enrolled in HIV care services in Rwanda. PLoS One. 2014;9(1):1–9. doi:10.1371/journal.pone.0085774
14. Makunde WH, Francis F, Mmbando BP, et al. Lost to follow up and clinical outcomes of HIV adult patients on antiretroviral therapy in care and treatment centres in Tanga city, North-Eastern Tanzania. Tanzan J Health Res. 2012;14(4):1–10. doi:10.4314/thrb.v14i4.3
15. Somi G, Keogh SC, Todd J, et al. Low mortality risk but high loss to follow-up among patients in the Tanzanian national HIV care and treatment programme. Trop Med Int Heal. 2012;17(4):497–506. doi:10.1111/j.1365-3156.2011.02952.x
16. Nyamhanga TM, Muhondwa EPY, Shayo R. Masculine attitudes of superiority deter men from accessing antiretroviral therapy in Dar es Salaam, Tanzania. Glob Health Action. 2013;6:21812. doi:10.3402/gha.v6i0.21812
17. Ochieng-Ooko V, Ochieng D, Sidle JE, et al. Influence du sexe de la personne sur la perte du suivi dans un vaste programme de traitement du VIH dans l’ouest du Kenya. Bull World Health Organ. 2010;88(9):681–688. doi:10.2471/BLT.09.064329
18. Clark A. Getting to zero: diverse methods for male involvement in HIV care and treatment; 2012:20.
19. Global information and education on HIV and AIDS; 2020. www.avert.org.
20. Salema J. Factors and challenges associated with loss; 2015.
21. Opio D, Semitala FC, Kakeeto A, et al. Loss to follow-up and associated factors among adult people living with HIV at public health facilities in Wakiso district, Uganda: a retrospective cohort study. BMC Health Serv Res. 2019;19(1):1–10. doi:10.1186/s12913-019-4474-6
22. Kiwanuka J, Waila JM, Kahungu MM, Kitonsa J, Kiwanuka N. Determinants of loss to follow-up among HIV positive patients receiving antiretroviral therapy in a test and treat setting: a retrospective cohort study in Masaka, Uganda. PLoS One. 2020;15(4):1–17. doi:10.1371/journal.pone.0217606
23. Baldé A, Lièvre L, Maiga AI, et al. Risk factors for loss to follow-up, transfer or death among people living with HIV on their first antiretroviral therapy regimen in Mali. HIV Med. 2019;20(1):1. doi:10.1111/hiv.12668
24. Kassaw MW, Samuel T; Matula, Ayele Mamo Abebe AMK& BBA. The perceived determinants and recommendations by mothers and healthcare professionals on the loss-to-follow-up in Option B+ program and child mortality in the Amhara region, Ethiopia. MC Infect Dis. 2020;20:876.
25. Zanzibar AI. Tanzania HIV impact survey (THIS) 2016–2017; 2017.
26. Nshimirimana C, Ndayizeye A, Smekens T, Vuylsteke B. Loss to follow-up of patients in HIV care in Burundi: a retrospective cohort study. Trop Med Int Health. 2022;27(6):574–582. doi:10.1111/tmi.13753
27. Hizza, Elizabeth et al March 2016 . Validation of data in the USAID ASSIST Project HIV care improvement activities in Tanzania
28. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
29. Farr BC. Designing qualitative research. Transform Int J Holist Mission Stud. 2008;25(2–3):165–166. doi:10.1177/026537880802500310
30. Showkat N, Parveen H. In-depth interview quadrant-I (e-Text); 2017.
31. Jacobvitz D, Curran M, Moller N. Measurement of adult attachment: the place of self-report and interview methodologies. Attach Hum Dev. 2002;4(2):207–215. doi:10.1080/14616730210154225
32. Nowell LS, Norris JM, White DE, Moules NJ. Thematic analysis: striving to meet the trustworthiness criteria. Int J Qual Methods. 2017;16(1):1–13. doi:10.1177/1609406917733847
33. Efron L, Efron L. Establishing trust. Purp Meets Exec. 2018;69–81. doi:10.4324/9781315169804-6
34. Mukumbang FC, Mwale JC, Van WB. Conceptualising the factors affecting retention in care of patients on antiretroviral treatment in Kabwe District. Zambia: Using the Ecological Framework; 2017.
35. Miller CM, Ketlhapile M. Why are antiretroviral treatment patients lost to follow-up? A qualitative study from South Africa. Trop Med Int Heal. 2010;15(Suppl 1):47–54.
36. Nakigozi G, Atuyambe L, Moses Kamya FE, et al. A qualitative study of barriers to enrollment into free HIV care: perspectives of never-in-care hiv-positive patients and providers in Rakai, Uganda. Biomed Res Int. 2013;2013:1–7. doi:10.1155/2013/470245
37. Id GAK, Ngocho JS, Knettel BA, Oshosen M, Mmbaga BT, Watt MH. “At home, no one knows”: a qualitative study of retention challenges among women living with HIV in Tanzania. PLoS One. 2020;1–15. doi:10.1371/journal.pone.0238232
38. Yakob B, Ncama BP. A socio-ecological perspective of access to and acceptability of HIV/AIDS treatment and care services: a qualitative case study research. BMC Public Health. 2016;16(1):1–15. doi:10.1186/s12889-016-2830-6
39. Sariah A, Rugemalila J, Protas J, et al. Why did I stop? And why did I restart? Perspectives of women lost to follow-up in option B + HIV care in Dar es Salaam, Tanzania. BMC Public Health. 2019;19:1–11. doi:10.1186/s12889-019-7518-2
40. Ziqubu SN. Faculty of community and health sciences supervisor: professor diane cooper; 2019.
41. Kagimu M, Guwatudde D, Rwabukwali C, Kaye S, Walakira Y, Ainomugisha D. Religiosity for promotion of behaviors likely to reduce new HIV infections in Uganda: a study among Muslim youth in Wakiso District. J Relig Health. 2013;52(4):1211–1227. doi:10.1007/s10943-011-9563-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.