Back to Journals » Open Access Emergency Medicine » Volume 14
Factors Associated with Willingness to Call Emergency Medical Services for Worsening Symptoms of COVID-19 in Addis Ababa, Ethiopia
Authors Olani A ![]() , Beza Demisse L
, Beza Demisse L ![]() , Alemayehu M
, Alemayehu M ![]() , Sultan M
, Sultan M
Received 30 June 2022
Accepted for publication 30 September 2022
Published 19 October 2022 Volume 2022:14 Pages 563—572
DOI https://doi.org/10.2147/OAEM.S380566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Ararso Olani,1 Lemlem Beza Demisse,2 Michael Alemayehu,3 Menbeu Sultan4
1College of Medicine and Health Science, Arba Minch University, Arbaminch, Ethiopia; 2Department of Emergency Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Tirunesh Beijing Hospital, Addis Ababa, Ethiopia; 4Department of Emergency Medicine and Critical Care, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Correspondence: Lemlem Beza Demisse, Department of Emergency Medicine, College of Health Sciences, Addis Ababa University, Po Box 2021, Bole Road, Addis Ababa, Ethiopia, Tel +251 923-092533, Email [email protected]
Background: In response to the COVID-19 pandemic, the Ethiopian Ministry of Health has established ambulances and dispatch centers specifically designed to transport COVID-19 patients to city medical centers. Due to a lack of evidence in this area, it is critical to assess the factors that influence the willingness to call for emergency medical services.
Methods: A community-based cross-sectional study was conducted from June to July 2021 in Addis Ababa. The data were gathered through use of a pretested questionnaire and analyzed using SPSS 25. Logistic regression was used to calculate odds ratios with and without confounding variable controls, and significant associations were declared at (0.05). For the variables that show significant associations in bivariate and multivariate analyses, a 95% confidence interval is provided.
Results: Three-quarters of those surveyed said they would call ambulance if they experienced worsening COVID-19 symptoms. The individual’s language was associated with the willingness to call EMS for worsening COVID-19 symptoms [AOR 0.51(95% CI: 0.28– 0.92)].; awareness of the availability of toll-free ambulance services [AOR 3.4(95% CI: 1.92– 5.95)]; recalling an EMS number [AOR 4.3(95% CI: 1.71– 10.67)]; ambulance crew quality of care perception [AOR 3.6(95% CI: 2.09– 6.10)]; ambulance service adequacy and accessibility perception [AOR 0.25(95% CI: 0.11– 0.55)].
Conclusion: The study showed significant portion of the Addis Ababa community recognized the need to call EMS due to worsening COVID-19 symptoms. The individual’s language, awareness of toll-free ambulance; ability to recall an ambulance number, perception of the ambulance crew’s quality of care and adequacy and accessibility of service in the city influence the decision to call an ambulance. The finding highlights the significance of addressing problems through various media outlet, for advocacy and public awareness. More research, including qualitative studies, is needed to investigate the factors that encourage people to seek EMS.
Keywords: the need to call emergency medical services, prehospital care, worsening COVID-19, Addis Ababa, Ethiopia
Background
Prehospital care is the emergency medical care provided to a person in need to outside a dedicated medical care or hospital.1 It has been proven to lower morbidity and mortality from emergency medical illness or injuries requiring emergency medical care.2–5 It is possible to prevent up to 45% of fatalities and 35% of disability-adjusted life years in low- and middle-income countries (LMIC)6 solely by creating effective emergency medical services (EMS). However, a sizeable fraction of the population in LMIC reside in regions with poor access to formal EMS.7,8 Despite growing government concerns and encouraging advances in Ethiopia about out-of-hospital emergency services over the past 10 years9 Although there are increasing government concerns and encouraging developments in Ethiopia over the last decade on out-of-hospital emergency services,10 Emerging works of literature have revealed that the proportion of patients obtaining prehospital care in the country is still quite low,11–14 Pressures on EMS are widely acknowledged since the first case report of COVID-19 in the world.15–17 To face the COVID-19 outbreak in Ethiopia, major adaptive and transformative changes were made to health care sectors including the establishment of emergency task forces, improvement in health communication flow, activation of toll-free numbers to report suspected cases, and redistribution of resources including manpower and material resources such as ambulances.18 In addition to the aforementioned interventions, Federal Ministry of Health in collaboration with Addis Ababa Health Bureau has established ambulances and dispatch centers dedicated to transporting COVID-19 patients to specialized treatment centers located in the city. However, prior research suggests that increasing access to ambulance service alone may not increase the overall demand for ambulance service utilization.19 Lack of awareness, the availability of the service, misconceptions, education level, and confidence in the safety and care provided by the service were all found to have an impact on the need to call EMS.20–22 Studies also showed that seeking of emergency medical service could be affected by the fear related to COVID-19.23,24 Therefore, understanding the factors that hinder or enhance the willingness to call for EMS for worsening symptoms of COVID-19 could be important. Despite inadequate public awareness, there is little to no research in Ethiopia on the willingness to call EMS for emergency illness and COVID 19 or worsening COVID −19 symptoms. One study conducted in Northern Ethiopia independent of COVID-19 reported that 88.1% of the respondents did not know emergency medical service (EMS) calling number and only 42.2% showed a preference for ambulance transport over other transportations during the emergency.21 Therefore, this study was aimed at assessing the factors associated with willingness to call emergency medical services for worsening symptoms of COVID-19 in Addis Ababa Ethiopia.
Methods and Materials
Study Design and Setting
A community-based cross-sectional study was carried out in Addis Ababa, the capital and largest city of Ethiopia, to determine the variables that influence people’s willingness to call emergency medical services for COVID-19 symptoms that are getting worse. There are 11 sub-cities in the city, but for this study, only four were chosen at random: Gulelle, Yeka, Kolfe-Keranio, and Nifas-Silk-Lafto. The selected sub cities are place of residence to between 200,000 and 300,000 people. These sub-cities provide support for the majority of the primary COVID-19 treatment facilities in Addis Ababa’s town. These sub-cities also have an emergency operations center, dispatch centers, and ambulances. The study was conducted between June 8 and July 30, 2021.
Eligibility Criteria
The eligibility requirements included being an Addis Ababa permanent resident (having resided in the city for at least 6 months) and being 18 years of age or older. However, those who declined to take part, were mentally incompetent, or were not in their usual residence during data collection were not included in the study.
Sample Size Determination and Sampling Procedure
The sample size was estimated using single population proportion formula with the following assumptions: taking 53.4% proportion of the people who can name at least one ambulance number in Addis Ababa,25 setting the level of confidence (α) at 0.05 (Z (1-α) = 1.96), and assuming 5% margin of error to the study. Considering 10% for non-response rate, 420 sample size was estimated for the study. Regarding the sampling process, four of the city’s 11 sub-cities were selected by simple random sampling technique (SRS). One woreda (the district equivalent) was randomly selected from each of the sub-cities. Then, three Ketena—the woreda’s smallest geographic subdivision—were selected from each selected woreda using SRS. Lastly, the first home in each Ketena was selected at random, and the others were chosen depending on their proximity to the first household. From each family, only one individual was interviewed (Figure 1.)
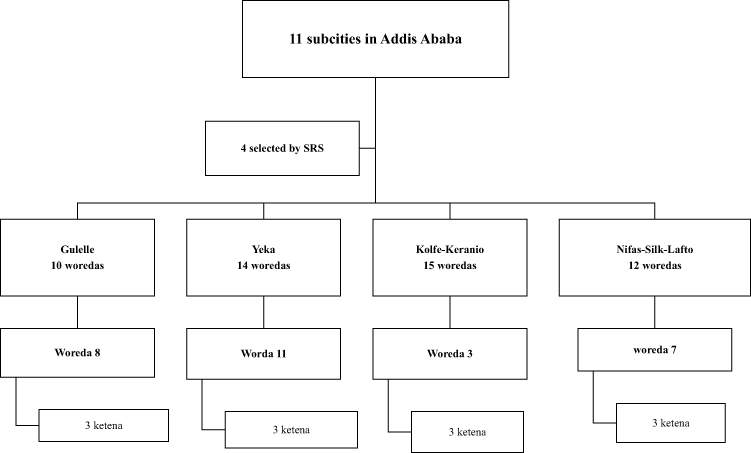 |
Figure 1 Flow diagram of sampling procedure. |
Data Collection and Quality Assurance
Structured questionnaire was given to the study participant by the interviewer in order to obtain the required data. The survey questionnaire has both open-ended and closed-ended questions. The information gather was socio-demographic data, knowledge, attitudes, and practices relating to prehospital EMS. The data collection tool was previously validated and adopted from a similar study. The data collectors are proficient in at least one additional local language in addition to Amharic, have a bachelor’s degree, and prior data collection experience. Training was provided to ensure that each data collector had a common understanding of the tool. Prior to the start of the actual data collection, a pilot study involving 21 participants from the same city was conducted. After the pilot study, the questionnaires were edited for their readability and clarity as per the local context. Furthermore, after each questionnaire was filled out, the completeness of the data was checked to ensure data quality.
Measurements
Respondents were asked a hypothetical question such as “would you call EMS if you experienced worsening clinical manifestations of COVID-19 such as cough, shortness of breath, chest pain, confusion, and tiredness?” The participants’ responsiveness to calling EMS for worsening clinical manifestations of suspected or confirmed COVID-19 was the outcome of interest. The desired response was for the participant to call EMS if the above-mentioned clinical manifestations worsened.
Data Entry, Processing, and Analysis
The collected data were checked for completeness, entered into Epi Data software version 4.2,26 and analyzed using SPSS version 25.27 Descriptive statistics such as frequency, percentages, mean and standard deviations were used to summarize the findings while tables were used to present the data. Logistic regression was used to estimate the degree of association between a dependent variable and its associated factors. Wald test of logistic regression for purposive selection of the variable with a cut-off p-value of <0.25 on bivariable analysis was considered for logistic regression to control the effect of potential confounders. Statistically, a significant association was declared at a 5% level.
Operational Definitions
Knowledge of the Work of Ambulance Crew
The respondent was labeled as having adequate knowledge on the work of the ambulance crew if responded to the following roles: (a) transporting the patients in emergency condition to a health care facility as quickly as possible (b) administration of life-saving medications, (c) and provision of life-saving procedures. Otherwise, if the respondent missed any of the aforementioned roles, we labeled them as having inadequate knowledge of the work of the ambulance crew.
Ethical Approval and Consent to Participate
The Yeka Kotbe hospital Ethical Review Board with reference number-EKGH/150/5/85 granted ethical approval. The purpose, general content, and nature of the study were explained to the respondents in the language preferred by each respondent. Verbal consent was obtained from each participant, and the protocol was approved by IRB. The respondents were informed that they had the right to be involved or refuse to participate in the study and the right to withdraw from the study at any time during the interview. The participants were assured that the data would be handled exclusively by the investigators for the intended purpose only. The information obtained from each participant was kept confidential and their identity was kept anonymous. All procedures involved in this study have adhered to the principles of the Helsinki Declaration.
Results
Socio-Demographic Characteristics
The study included 414 participants in the analysis, giving a response rate of 98.6%. Their mean age was 35.2 years with a standard deviation (SD) of 11.2. Of the total participants, 34.3% were within the age group of 25–34 years and 62.6% were men. Two-hundred-forty (58.0%) of the respondents were married and more than half (54.6%) of the study participants hold at least a university degree. More than three-fourth (76.6%) of the study participants speak Amharic (the working language of EMS in Addis Ababa) and nearly half (46.1%) of the respondents lived in Addis Ababa for more than 10 years (Table 1).
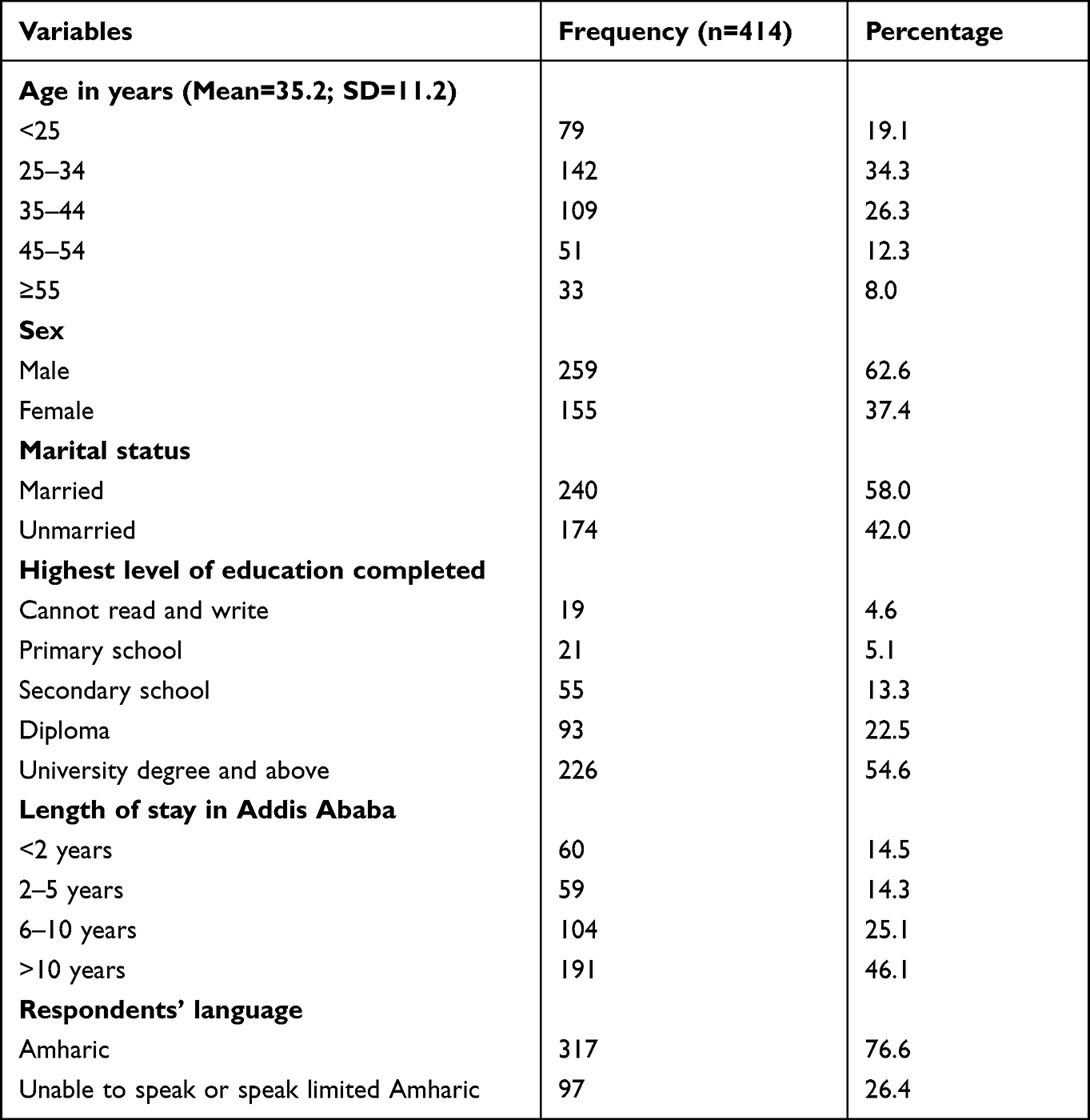 |
Table 1 Socio-Demographic Characteristics of the Study Participants, Addis Ababa, Ethiopia, June to July 2021 |
Respondent’s Awareness of Local EMS
The majority of respondents (76.6%) were aware that prehospital emergency medical services were available for any type of emergency illness or injury. Likewise, over three-fourths (73.4%) of the participants knew that prehospital care was available specifically for COVID-19 patients. The availability of toll-free ambulances to transfer COVID-19 patients to medical facilities was known to 290 of the respondents (70.5%). The majority of research participants (90.3%) had sufficient knowledge of the tasks of the ambulance crew, with (55.1%) of them being able to identify at least one EMS calling number (Table 2).
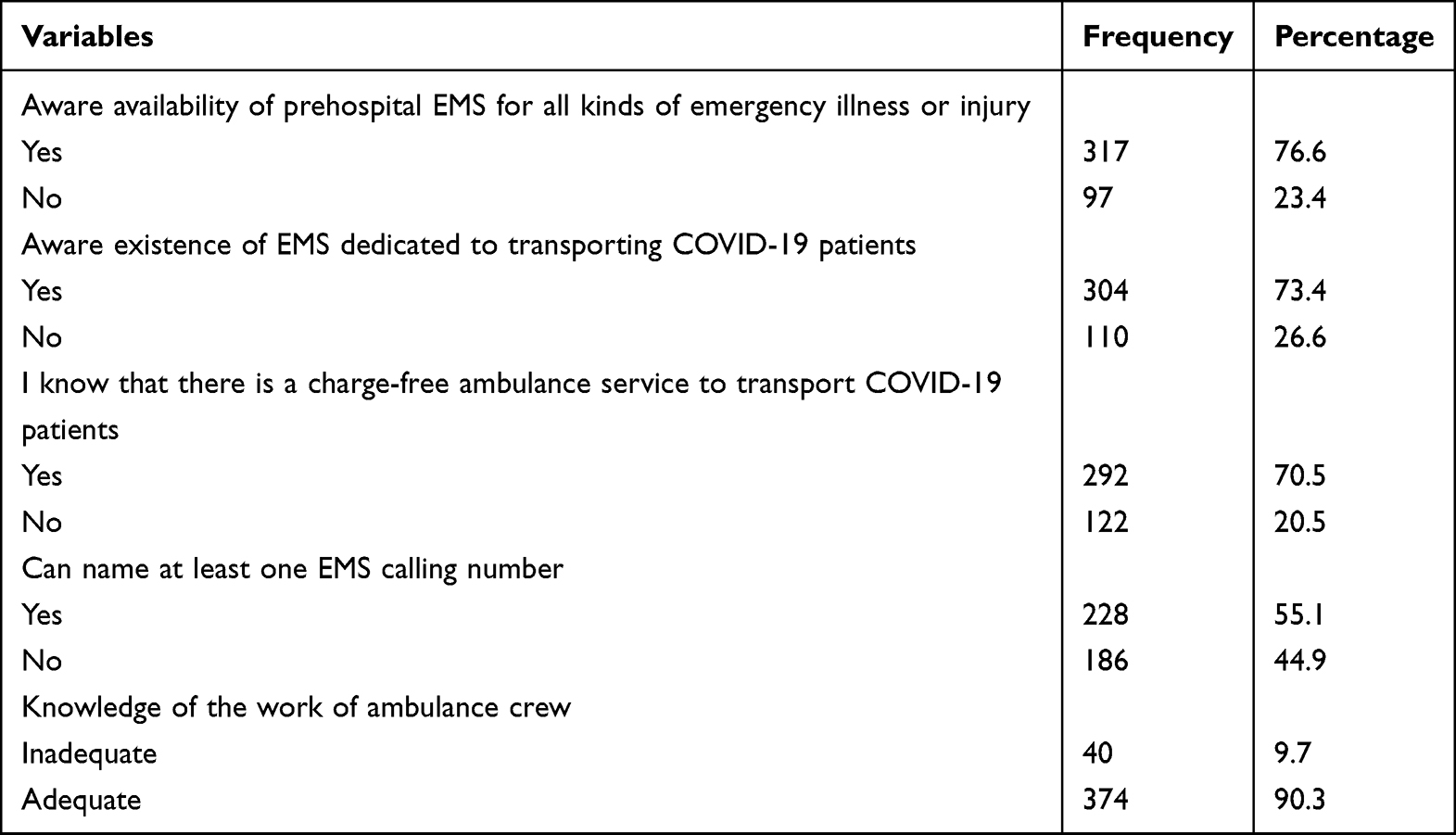 |
Table 2 Description of the Respondents’ Awareness of EMS in Addis Ababa, Ethiopia, June to July 2021 |
Perceptions of the Study Participants on Ambulance Services and the Need to Call EMS
Regardless of whether the virus suspected or confirmed, 74.6% of the study participants said they would call EMS if they experienced symptoms of worsening COVID-19. Participants were polarized 62.8% support ambulance crews providing high-quality care, while 27.1% support taxis as a safer way to get to the hospital after an emergency. Twenty-four percent of the respondents came to believe taxis would arrive faster than ambulances. Almost three-fourths (73.9%) of those surveyed believe Addis Ababa’s ambulance service is insufficient and difficult to access (Table 3).
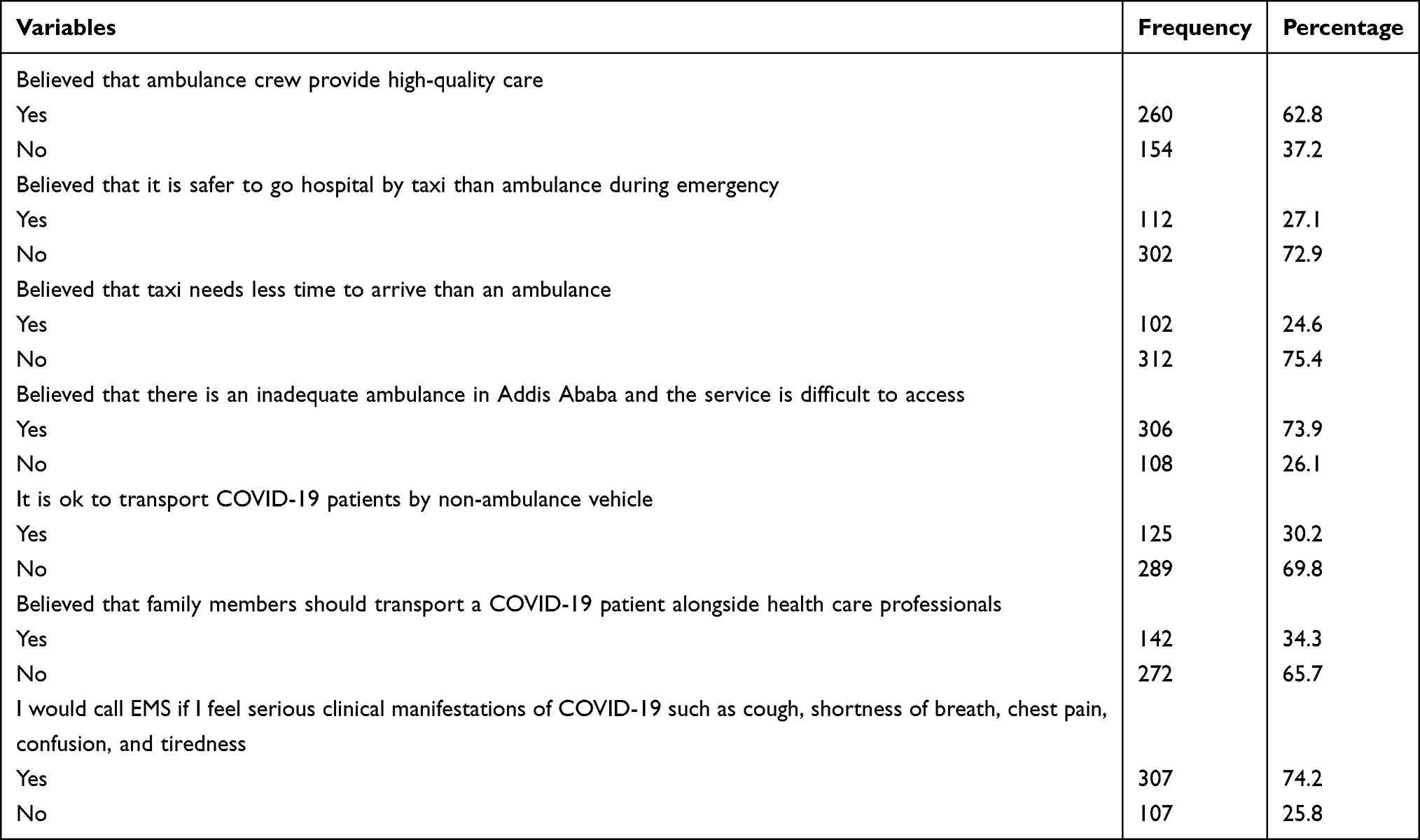 |
Table 3 Description of Respondents’ Perception of Ambulance Services and the Need to Call EMS in Addis Ababa, June to July 2021 |
Factors Associated with the Need to Call EMS for Worsening Symptoms of COVID-19
The factors associated with the willingness to call EMS for worsening symptoms of COVID-19 are shown in Table 4. The respondents who speak limited Amharic or were unable to speak Amharic were 49% less likely to report the willingness to call EMS for worsening symptoms of COVID-19 [AOR 0.51(95% CI: 0.28–0.92)]. The respondent’s awareness of the availability of toll-free ambulances to transport critically ill COVID-19 patients was another factor associated with the need to call EMS [AOR 3.4(95% CI: 1.92–5.95)]. Accordingly, respondents who were aware that toll-free ambulance service was available to transport seriously ill COVID-19 patients were 3.4 times more likely than their counterparts to report the need to call EMS for COVID-19 symptoms that were getting worse. The respondents’ knowledge of EMS calling numbers was also independently associated with the need to call EMS for worsening symptoms of COVID-19 [AOR 4.3(95% CI: 1.71–10.67)]. After adjusting for all potential confounders, the respondents who were able to name at least one EMS calling number were 4.3 times more likely to report the need to call EMS compared to those unable to mention at least one EMS calling number. On multivariate analysis, the respondents who believed that ambulance crew provides high-quality care had 3.6 times more likely reported the need to call EMS for worsening symptoms of COVID-19 compared to their counterparts [AOR 3.6(95% CI: 2.09–6.10)]. In addition, the respondents who thought the number of ambulances in Addis Ababa is inadequate and the service is difficult to access were 75% less likely to report the need to call EMS for worsening COVID-19 symptoms [AOR 0.25(95% CI: 0.11–0.55)].
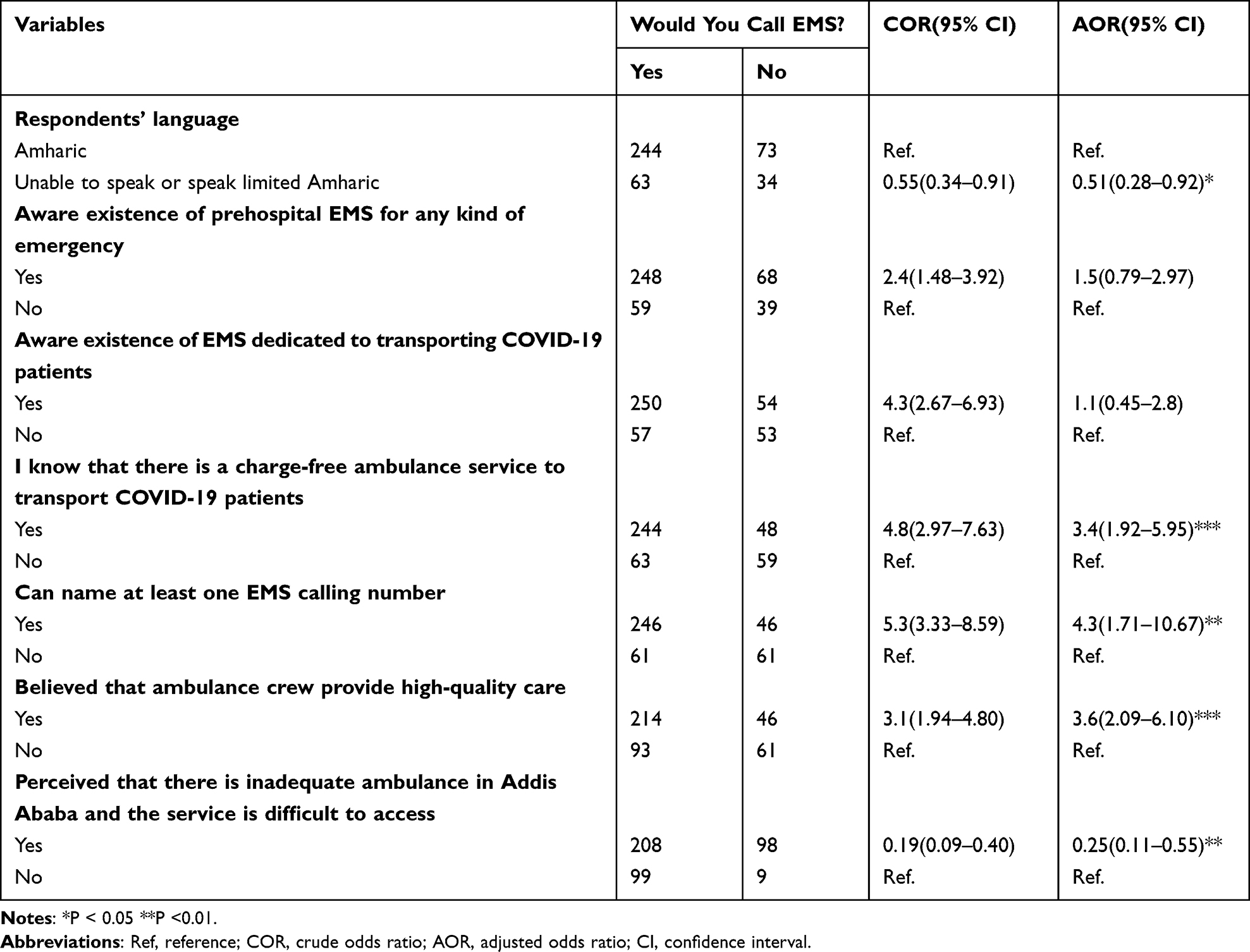 |
Table 4 Bivariate and Multivariate Analyses of the Need to Call EMS for Worsening Suspected or Confirmed COVID-19 in Addis Ababa, June to July 2021 |
Discussion
This study examined the willingness to call EMS and associated factors among residents of Addis Ababa city, Ethiopia. Although over three-fourth of the participants had awareness of the availability of prehospital EMS, only 55.1% were able to name at least one EMS calling number in the present study. Our findings are nearly similar to the report of a previous study conducted in the same city independent of the COVID-19 outbreak, which reported 53.4%.25
The current finding is concerning and highlights the need for additional interventions, such as mass media and social media campaigns, to increase public awareness of EMS calling numbers.
The willingness to call prehospital EMS identified in this study was 74.2%. Although we could not find literature that assessed the need to call EMS for deteriorating COVID-19 patients, our finding is higher than the finding of the hypothetical study conducted on trauma emergency in the capital of Ghana, Accra, which reported 12.4%.20 The disparity could be due to the difference in the level of awareness of the respondents on EMS in the respective countries, as more respondents in the present study had awareness of the availability of prehospital care for emergency events compared to the Ghanaian study. In addition, the difference could be attributable to the hypothetical emergency used in the present study is COVID-19 while the Ghanaian study used trauma. The government has been providing emerging and evolving information to the public about COVID-19 and the threat it could pose to an infected person.18 This could increase the willingness to call EMS in the present study. However, our findings imply that there is still a need to educate the public on when to call EMS for COVID-19 patients and the importance of using the ambulance to increase the demand for the service.
According to this study, respondents who spoke limited Amharic or were unable to speak Amharic were 49% less likely to call EMS in the event of worsening COVID-19 symptoms than Amharic speakers which is the working language. A previous study on trends and barriers to emergency medical services in Addis Ababa found comparable findings.25 Language barriers’ impact on health-care utilization, including access to prehospital care, has previously been well documented in a number of countries.28–31 One unpublished study in Addis Ababa on the impact of language barriers on proper health care utilization was also in agreement with finding from other county.32 Our findings show the need to take innovative interventions such as introducing ambulance service in other additional local languages to overcome disparities in accessing health care attributable to language barriers. Similar to a previous study from Addis Ababa,25 the majority of the respondents in this study thought that there is inadequate ambulance in the city and the service is difficult to access. Such misperception was independently associated with the need to call EMS. Accordingly, those respondents who thought the ambulance is inadequate in the city and the service is difficult to access were less likely to report they would call for EMS in the event of worsening symptoms of COVID-19. The present findings suggest that there is a need to introduce digital tools and technology to increase access to ambulance services.
Although we could not find a significant association in the present study, previous studies reported that individuals who perceived an ambulance as safer than a taxi were more likely to report the need to call ambulance services during emergency events.20,25 However, in the present study, we found that respondents who believed that ambulance crews provide high-quality care were more likely to report the need to call EMS for worsening symptoms of COVID-19. Further investigations are needed to understand and confirm this particular finding.
The previous study reported that awareness on the availability of toll-free ambulances was associated with an increased need for prehospital EMS use.21 The present study supports the findings of the previous study indicating that the respondents’ awareness of the availability of toll-free ambulance service to transport critically ill COVID-19 patients more likely increases the need to call EMS for worsening COVID-19 symptoms. Availability of toll-free ambulance services or lack of direct out-of-pocket expenses for ambulance services increases the demands for the services.33,34
Limitations
Our study had some limitations. Cross-sectional research design was used. It must be underlined that great care should be taken when drawing conclusions about causality. Moreover, the study presented a hypothetical question to gauge whether it would be necessary to call EMS in the event that COVID-19 worsened so that it might either overstate or underestimate the findings. Furthermore, the study was conducted in Addis Ababa, the capital city, which may not be representative of the community living in rural areas.
Conclusion
In conclusion, the study’s findings indicated that a substantial proportion of Addis Ababa’s population had realized the need to call EMS when COVID-19 symptoms became severe. However, the decision to call an ambulance for worsening COVID-19 symptoms varies based on the respondent’s language, awareness of the existence of toll-free ambulance services, ability to recall the EMS calling number, perception of the level of care provided by the ambulance crew, and perception of the sufficiency of the city’s and its accessibility’s ambulance service. To deal with the challenges mentioned, it is necessary to strengthen ongoing interventions like media campaigns and create innovative interventions. To understand the factors that influence people’s decisions to use an ambulance, additional research, including qualitative research and longitudinal studies, is required.
Data Sharing Statement
All the data generated or analyzed during this study are available with the corresponding author and will be shared upon reasonable request.
Acknowledgment
The authors would like to thank participants of the study.
Author Contributions
All authors contributed significantly to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or in all of these areas; participated in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article was submitted; and agree to be accountable for all aspects of the work.
Funding
This research work data collection was financed by Health Ministry of Ethiopia.
Disclosure
The authors declare no conflict of interest for this work.
References
1. Calvello E, Reynolds T, Hirshon J, Buckle C, Moresky R, O’Neill J. Operative care after the Haiti 2010 earthquake: implications for post-disaster definitive care. Am J Emerg Med. 2013;31(2):429–431. doi:10.1016/j.ajem.2012.10.020
2. Band RA, Gaieski DF, Hylton JH, Shofer FS, Goyal M, Meisel ZF. Arriving by emergency medical services improves time to treatment endpoints for patients with severe sepsis or septic shock. Acad Emerg Med. 2011;18(9):934–940. doi:10.1111/j.1553-2712.2011.01145.x
3. Canto JG, Zalenski RJ, Ornato JP, et al. Use of emergency medical services in acute myocardial infarction and subsequent quality of care: observations from the National Registry of Myocardial Infarction 2. Circulation. 2002;106(24):3018–3023. doi:10.1161/01.CIR.0000041246.20352.03
4. Henry JA, Reingold AL. Prehospital trauma systems reduce mortality in developing countries: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2012;73(1):261–268. doi:10.1097/TA.0b013e31824bde1e
5. Maddock A, Corfield AR, Donald MJ, et al. Prehospital critical care is associated with increased survival in adult trauma patients in Scotland. Emerg Med J. 2020;37(3):141–145. doi:10.1136/emermed-2019-208458
6. Kobusingye OC, Hyder AA, Bishai D, et al. Emergency medical services. In: Jamison DT, Breman JG, Measham AR, editors. Disease Control Priorities in Developing Countries. Washington (DC) New York: The International Bank for Reconstruction and Development/The World Bank Oxford University Press Copyright © 2006, The International Bank for Reconstruction and Development/The World Bank Group; 2006.
7. Mock C. Strengthening prehospital trauma care in the absence of formal emergency medical services. World J Surg. 2009;33(12):2510–2511. doi:10.1007/s00268-009-0239-4
8. Wilson A, Hillman S, Rosato M, et al. A systematic review and thematic synthesis of qualitative studies on maternal emergency transport in low- and middle-income countries. Int J Gynaecol Obstet. 2013;122(3):192–201. doi:10.1016/j.ijgo.2013.03.030
9. Sultan M, Debebe F, Azazh A. The status of emergency medicine in Ethiopia challenges and opportunities. Ethiop Med J. 2018;56(2):119–124.
10. Mohammed MS, Tumebo AA. The status of emergency medicine in Ethiopia, challenges and opportunities. Ethiop Med J. 2018;56:119–124.
11. Baru A, Azazh A, Beza L. Injury severity levels and associated factors among road traffic collision victims referred to emergency departments of selected public hospitals in Addis Ababa, Ethiopia: the study based on the Haddon matrix. BMC Emerg Med. 2019;19(1):2. doi:10.1186/s12873-018-0206-1
12. Gebresenbet RF, Aliyu AD. Injury severity level and associated factors among road traffic accident victims attending emergency department of Tirunesh Beijing Hospital, Addis Ababa, Ethiopia: a cross sectional hospital-based study. PLoS One. 2019;14(9):e0222793. doi:10.1371/journal.pone.0222793
13. Laeke T, Tirsit A, Debebe F, et al. Profile of head injuries: prehospital care, diagnosis, and severity in an Ethiopian Tertiary hospital. World Neurosurg. 2019;127:e186–e192. doi:10.1016/j.wneu.2019.03.044
14. Seid M, Azazh A, Enquselassie F, Yisma E. Injury characteristics and outcome of road traffic accident among victims at Adult Emergency Department of Tikur Anbessa specialized hospital, Addis Ababa, Ethiopia: a prospective hospital based study. BMC Emerg Med. 2015;15:10. doi:10.1186/s12873-015-0035-4
15. Al Amiry A, Maguire BJ. Emergency medical services (EMS) calls during covid-19: early lessons learned for systems planning (a narrative review). OAEM. 2021;13:407. doi:10.2147/OAEM.S324568
16. Caviglia M, Buson R, Pini S, et al. The National emergency medical service role during the COVID-19 pandemic in Sierra Leone. Prehosp Disaster Med. 2020;35(6):693–697. doi:10.1017/S1049023X20001211
17. Katayama Y, Kiyohara K, Kitamura T, Hayashida S, Shimazu T. Influence of the COVID-19 pandemic on an emergency medical service system: a population-based, descriptive study in Osaka, Japan. Acute Med Surg. 2020;7(1):e534. doi:10.1002/ams2.534
18. Shigute Z, Mebratie AD, Alemu G, Bedi A. Containing the spread of COVID-19 in Ethiopia. J Glob Health. 2020;10(1). doi:10.7189/jogh.10.010369
19. Tippett VC, Toloo GS, Eeles D, Ting JY, Aitken PJ, Fitzgerald GJ. Universal access to ambulance does not increase overall demand for ambulance services in Queensland, Australia. Aust Health Rev. 2013;37(1):121–126. doi:10.1071/AH12141
20. Mould-Millman NK, Rominski SD, Bogus J, et al. Barriers to accessing emergency medical services in Accra, Ghana: development of a survey instrument and initial application in Ghana. Glob Health Sci Pract. 2015;3(4):577–590. doi:10.9745/GHSP-D-15-00170
21. Takele GM, Ballo TH, Gebrekidan KB, Gebregiorgis BG. Utilization, barriers and determinants of emergency medical services in Mekelle City, Tigray, Ethiopia: a community-based cross-sectional study. Open Access Emerg Med. 2021;13:325–334. doi:10.2147/OAEM.S315459
22. Yonemoto N, Kada A, Yokoyama H, Nonogi H. Public awareness of the need to call emergency medical services following the onset of acute myocardial infarction and associated factors in Japan. J Int Med Res. 2018;46(5):1747–1755. doi:10.1177/0300060518757639
23. Metzler B, Siostrzonek P, Binder RK, Bauer A, Reinstadler SJ. Decline of acute coronary syndrome admissions in Austria since the outbreak of COVID-19: the pandemic response causes cardiac collateral damage. Eur Heart J. 2020;41(19):1852–1853. doi:10.1093/eurheartj/ehaa314
24. Wong LE, Hawkins JE, Langness S, Murrell KL, Iris P, Sammann A. Where are all the patients? Addressing Covid-19 fear to encourage sick patients to seek emergency care. Nejm Catalyst. 2020;1(3):1–12.
25. Sultan M, Abebe Y, Tsadik AW, Ababa A, Yesus AG, Mould-Millman N-K. Trends and barriers of emergency medical service use in Addis Ababa; Ethiopia. BMC Emerg Med. 2019;19(1):1–8. doi:10.1186/s12873-019-0242-5
26. Lauritsen JM, Bruus M; EpiData entry. A Comprehensive Tool for Validated Entry and Documentation of Data. Odense Denmark: The EpiData Association; 2008.
27. George D, Mallery P; Data Files. IBM SPSS Statistics 25 Step by Step. Routledge; 2018:381–384.
28. de Moissac D, Bowen S. Impact of language barriers on access to healthcare for official language minority Francophones in Canada. Healthc Manage Forum. 2017;30(4):207–212. doi:10.1177/0840470417706378
29. Grow RW, Sztajnkrycer MD, Moore BR. Language barriers as a reported cause of prehospital care delay in Minnesota. Prehosp Emerg Care. 2008;12(1):76–79. doi:10.1080/10903120701709878
30. Kohlenberger J, Buber-Ennser I, Rengs B, Leitner S, Landesmann M. Barriers to health care access and service utilization of refugees in Austria: evidence from a cross-sectional survey. Health Policy. 2019;123(9):833–839. doi:10.1016/j.healthpol.2019.01.014
31. Noack EM, Kleinert E, Müller F. Overcoming language barriers in paramedic care: a study protocol of the interventional trial ‘DICTUM rescue’evaluating an app designed to improve communication between paramedics and foreign-language patients. BMC Health Serv Res. 2020;20(1):1–12. doi:10.1186/s12913-020-05098-5
32. Mekuria T, Urgie T, Tolu LB, Abbas F, Gashawbeza B. Overcoming patient-provider language barrier: impact of a tailored language training on health professionals’ language proficiency; 2021.
33. Rucker DW, Edwards RA, Burstin HR, O’Neil AC, Brennan TA. Patient-specific predictors of ambulance use. Ann Emerg Med. 1997;29(4):484–491. doi:10.1016/S0196-0644(97)70221-X
34. Ting JY, Chang AM. Path analysis modeling indicates free transport increases ambulance use for minor indications. Prehosp Emerg Care. 2006;10(4):476–481. doi:10.1080/10903120600885209
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Incidence, Bacterial Profile and Predictors of Surgical Site Infection After Cesarean Section in Ethiopia, A Prospective Cohort Study
Mezemir R, Olayemi O, Dessie Y
International Journal of Women's Health 2023, 15:1547-1560
Published Date: 13 October 2023