Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Factors Associated with Viral Suppression Among Adolescents on Antiretroviral Therapy in Homa Bay County, Kenya: A Retrospective Cross-Sectional Study
Received 30 October 2021
Accepted for publication 1 December 2021
Published 24 December 2021 Volume 2021:13 Pages 1111—1118
DOI https://doi.org/10.2147/HIV.S345731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Anne Mwangi, Brian van Wyk
School of Public Health, University of the Western Cape, Bellville, Western Cape Province, South Africa
Correspondence: Brian van Wyk Tel +27 82 8049055
Email [email protected]
Background: Despite the success in initiating adolescents living with HIV on antiretroviral therapy (ART), questions remain about factors affecting viral suppression. In Kenya, only 63% of adolescents (aged 10– 19 years) on ART had achieved viral suppression in 2016. We investigated factors associated with viral suppression among adolescents initiated on ART before November 30, 2017 in Homa Bay County, Kenya.
Methods: A retrospective cross-sectional analysis of 908 adolescents registered on ART for at least 6 months and with at least one documented viral load in the last 12 months, in six health facilities in Homa Bay County was conducted. Data were extracted from the electronic medical records and exported into an excel spreadsheet. Bivariate and multivariate logistic regression analyses were conducted to identify factors associated with viral suppression and adjust for confounding, using Stata 12.0.
Results: Out of all participants, 80% (726) had achieved viral suppression (< 1,000 copies of viral RNA/mL of blood at latest viral load count). After adjusting for other covariates, adolescents with good adherence to ART (AOR=2.3, 95% CI=1.38– 3.84) and a most recent CD4 count of above 500 cells/mm3 (AOR=1.87, 95% CI=1.13– 3.08), were more likely to be virally suppressed. Adolescents on second line ART treatment (AOR=0.45, 95% CI=0.28– 0.73) and having inadequate adherence to ART (AOR=0.26, 95% CI=0.11– 63) were less likely to be virally suppressed.
Conclusion: Viral suppression for adolescents on ART in this study is significantly higher than the national prevalence in 2016 (80% vs 63%), but it is still below the WHO target of 90%. Enhanced adherence support for adolescents on ART should be implemented to improve long-term adherence. Specific interventions are needed to “rescue” adolescents on second-line ART regimens who may have a history of poor adherence.
Keywords: adolescents, HIV, antiretroviral therapy, viral suppression, adherence, Kenya
Background
Globally, it is estimated that about 1.8 million adolescents aged 10–19 years were living with HIV in 2015.1 According to the 2015 Kenya HIV estimates, about 133,455 adolescents are living with HIV in Kenya.2 In the last decade Kenya’s HIV program has experienced a rapid scale-up of HIV testing and initiating infants, children, and adults on antiretroviral therapy (ART). This has necessitated a stringent monitoring system to track the effectiveness of the programme for those in HIV care and treatment.
In 2014, the Joint United Nations Programme on HIV/AIDS (UNAIDS) set new targets towards the elimination of HIV, including diagnosis of 90% of people living with HIV (PLWH), access to treatment for 90% of PLWH, and 90% viral suppression among those initiated on treatment.3 In 2015, Kenya adopted the UNAIDS targets, and also rolled out routine viral load testing as the gold standard to monitor treatment outcomes of ART.4 Monitoring viral suppression among PLWH enrolled on ART is important for timely detection of treatment failures, and identification of patients who need enhanced adherence counseling and support.5 HIV drug resistance testing is not routinely done in Kenya, but previous studies show an increasing prevalence of transmitted antiretroviral drug resistance in ART-naïve patients.6,7
Viral suppression is defined as viral load below 1,000 copies/mL3 after at least 6 months of using ART.8 Effective ART leads to viral suppression, which in turn restores immune function, reduces HIV-related morbidity, prolongs survival, and improves quality-of-life of PLWH, and also prevents transmission of HIV to their uninfected sexual partners.8,9
Virologic failure occurs when ART fails to suppress and sustain a person’s viral load to less than 1,000 copies/mL3.8 According to the Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV infection in Kenya a viral load test should be carried out at 6 and 12 months after initiation of ART and annually thereafter if the viral load is less than 1,000 copies/mL3.8
High levels of adherence to ART are needed to ensure viral suppression and prevention of the emergence of HIV drug resistance.10 It is widely reported that adolescents find consistent, long-term adherence to any medication regimen difficult, and ART is no exception.11 Compared to adults, adolescents on ART are more likely to have an unsuppressed viral load and more likely to fail virologically, as reported by two South African studies.12,13 Similarly a study in Uganda found that children (0–18 years) are almost twice as likely to have virological failure compared to adults.14
According to the Kenya national viral load dashboard, the proportion of adolescents achieving viral suppression country-wide is 63%; which is much lower than the UNAIDS recommended target of 90%.8 It is therefore essential to identify the risk and protective factors that influence viral suppression among adolescents on ART, so as to assess the success of the ART program and identify factors for possible intervention. The aim of the study was to determine factors associated with viral suppression among adolescents on ART in Homa Bay County, Kenya. Homa Bay County bears the largest burden of HIV in the country with an adult prevalence of 26% in 2014, compared to the national average of 6%.15 The county has an estimated 15,323 adolescents living with HIV, with 2,945 new HIV infections and 238 HIV-related deaths annually.2
Methods
Study Setting, Design, and Population
We conducted a retrospective descriptive cross-sectional study, using routinely collected program data extracted from the electronic medical records (EMR) in one county referral hospital and five sub-county hospitals. The six hospitals were selected for the study because they had a high volume of patients and hence a higher number of adolescents on ART, and were using EMR for patient management.
The study population constituted all adolescents, aged 10–19 years, on ART for at least 6 months with at least one documented viral load in the last 12 months.
Participants’ Selection
We included in the study sample all adolescents on antiretroviral therapy for at least 6 months who had at least one documented viral load in the last 12 months. Adolescents who had been transferred in from another health facility within the last 6 months and those who had transferred out to another facility more than 12 months prior to the start of the study were excluded from the study.
Variables
We created the outcome variable of suppression status by categorizing the viral load results into two groups. All results <1,000 copies/mL of blood were categorized as virally suppressed while ≥1,000 copies/mL of blood were categorized as not suppressed. Viral suppression proportion was defined as the percentage of the number of total suppressed among the total number tested. We also collected information on adolescents’ characteristics, including age, gender, age at ART initiation, initial WHO clinical stage, CD4 count at ART initiation, and current CD4 count, TB history, ART regimen, reported adherence, and disclosure of HIV status.
Data Abstraction and Management
The EMR was reviewed and a list of all adolescents on ART for at least 6 months generated. Of these, only adolescents with recorded viral loads in the last 12 months were included in the study. Before extracting data from the EMR, a query was run for the specific variables of interest in the EMR. The data from the EMR was then downloaded into an excel file or a Comma-Separated Values (CSV) file. Once downloaded in the Excel or CSV file, cross-checking was done to identify anomalies, and these were corrected by drawing the particular patient’s paper files.
Statistical Analyses
Data from the EMR was downloaded into an excel spreadsheet and cleaned. Since the EMR is a secondary data source; pharmacy records, laboratory, and the patient’s clinic records were used to complete any missing data in the EMR. Values that were missed completely were dropped automatically from each variable and analysis conducted based on the totals with complete records. To explore associations of viral suppression, we conducted bivariate and multivariate logistic regression analyses using Stata 12.0 (Stata Corporation, College Station, TX).
We analyzed a total of 908 patient records who had a viral load done in the last 12 months to estimate the proportion of patients with viral suppression, and to identify factors associated with viral suppression. We used univariate analyses to describe the socio-demographic and clinical characteristics of the study population. We used bivariate analyses to determine the strengths of association between the independent variables and the outcome variable (viral suppression status). Crude odds ratios (OR) and 95% confidence intervals were calculated. Variables that were statistically significant in the bivariate analysis were included in the multivariate analyses. We used multivariate logistic regression to identify factors independently associated with viral suppression. Adjusted odds ratios (AOR) and 95% confidence intervals were calculated. Cut-off for statistical significance was set at a p-value less than 0.05.
Ethics Considerations
The study was conducted upon approval from the University of the Western Cape Biomedical Research Ethics Committee (BMREC) (Ref: BM17/9/9) and the AMREF Kenya Ethics and Scientific Review Committee (Ref: P418/2017). Administrative approval was sought from the Ministry of Health Homa Bay County Health Department. Informed consent was not sought because the data was collected retrospectively and there was no contact with patients. Further, no patient identifiers were collected to protect the anonymity and confidentiality of information of all participants. The study was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments.
Results
A total of 908 records of adolescents on antiretroviral therapy for at least 6 months who had a viral load done in the last 12 months were analyzed. The median age of adolescents in the study was 14.0 years (Interquartile Range [IQR]=12.0–16.0). Table 1 describes the sociodemographic and clinical characteristics of adolescent participants. The majority of the adolescents in this study were aged 10–14 years (59%) and female (57.5%). The median age at ART initiation was 7.0 years (IQR=3.0–10.0); with 302 (33%) initiating ART before 4 years of age, 343 (38%) between 5–9 years, 204 (23%) between 10–14 years, and 59 (6.5%) between 15–19 years.
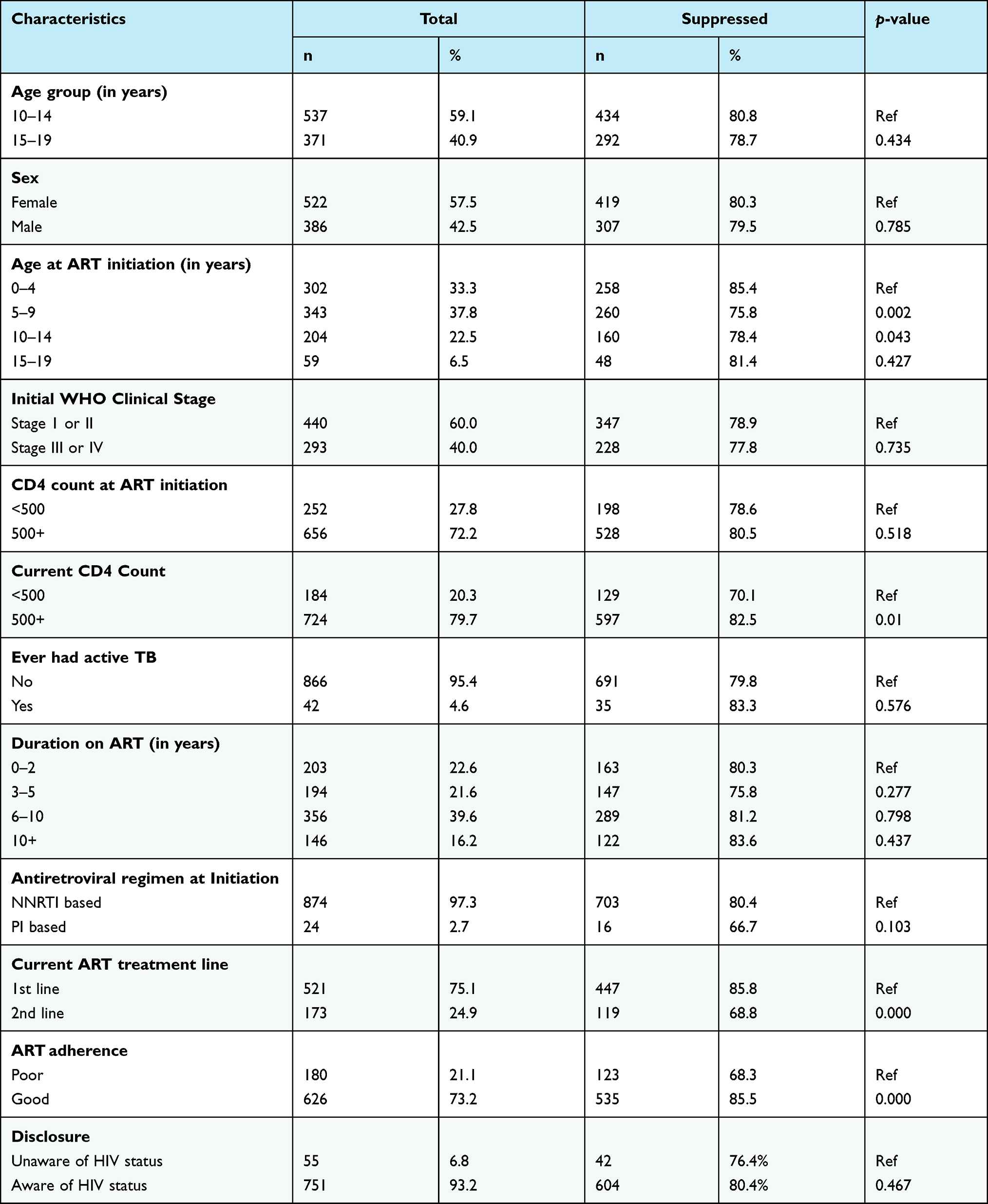 |
Table 1 Demographic and Clinical Characteristics of the Adolescent Patients on ART, and Who are Virally Suppressed in Homa Bay County, Kenya 2017 (N=908) |
Of those participants who had documented WHO staging done at ART initiation, 440 (60%) were classified as WHO stage I or II, and 293 (40%) were WHO stage III or IV. Most participants (656, 72.2%) had a CD4 count above 500 cells/mm3 at ART initiation. Only 42 (4.6%) participants had a history of active TB.
The median duration on treatment (ART) was 6.5 years (IQR=3.2–9.0); and 39.6% of the adolescents had been on ART for 6–10 years, 22.6% less than 2 years, 21.6% 3–5 years, and 16.2% more than 10 years.
The majority of the patients had started ART with a non-nucleoside reverse transcriptase inhibitor (NNRTI) based regimen (97.3%), while 24 (2.7%) had started on a protease inhibitor (PI) based regimen. Most participants (75.1%) in the study were currently on the first line ART regimen and the majority of the patients (93.2%) were aware of their HIV status, while 73.2% were documented to have good adherence to ART at the last visit.
Overall, 726 (80%) of the adolescents had a suppressed viral load. From Table 1, viral suppression was significantly associated with age at ART initiation, current CD4 count, current ART treatment line, and ART adherence. The study population did not differ by age group, gender, WHO stage, CD4 count at ART initiation, TB history, duration on treatment (ART), antiretroviral regimen at initiation, and documented disclosure of HIV status by viral suppression status.
Table 2 shows factors associated with viral suppression in a multivariate logistic regression model. In bivariate analysis, those who initiated ART between the ages of 5–9 years (crude OR=0.53, 95% CI=0.36–0.80) and 10–14 years (crude OR=0.62, 95% CI=0.39–0.98) were significantly less likely to be virally suppressed compared to those who initiated at ages 0–4 years. However, after controlling for other covariates, age at ART initiation was not statistically significantly associated with viral suppression. In multivariate analysis, viral suppression was significantly higher for those adolescents with current CD4 count >500 cells/mm3 (AOR=1.87, 95% CI=1.13–3.08) and documented good adherence to ART (AOR=2.3, 95% CI=1.38–3.84). The likelihood for viral suppression was significantly lower for those adolescents who were on an second line ART regimen (AOR=0.45, 95% CI=0.28–0.73).
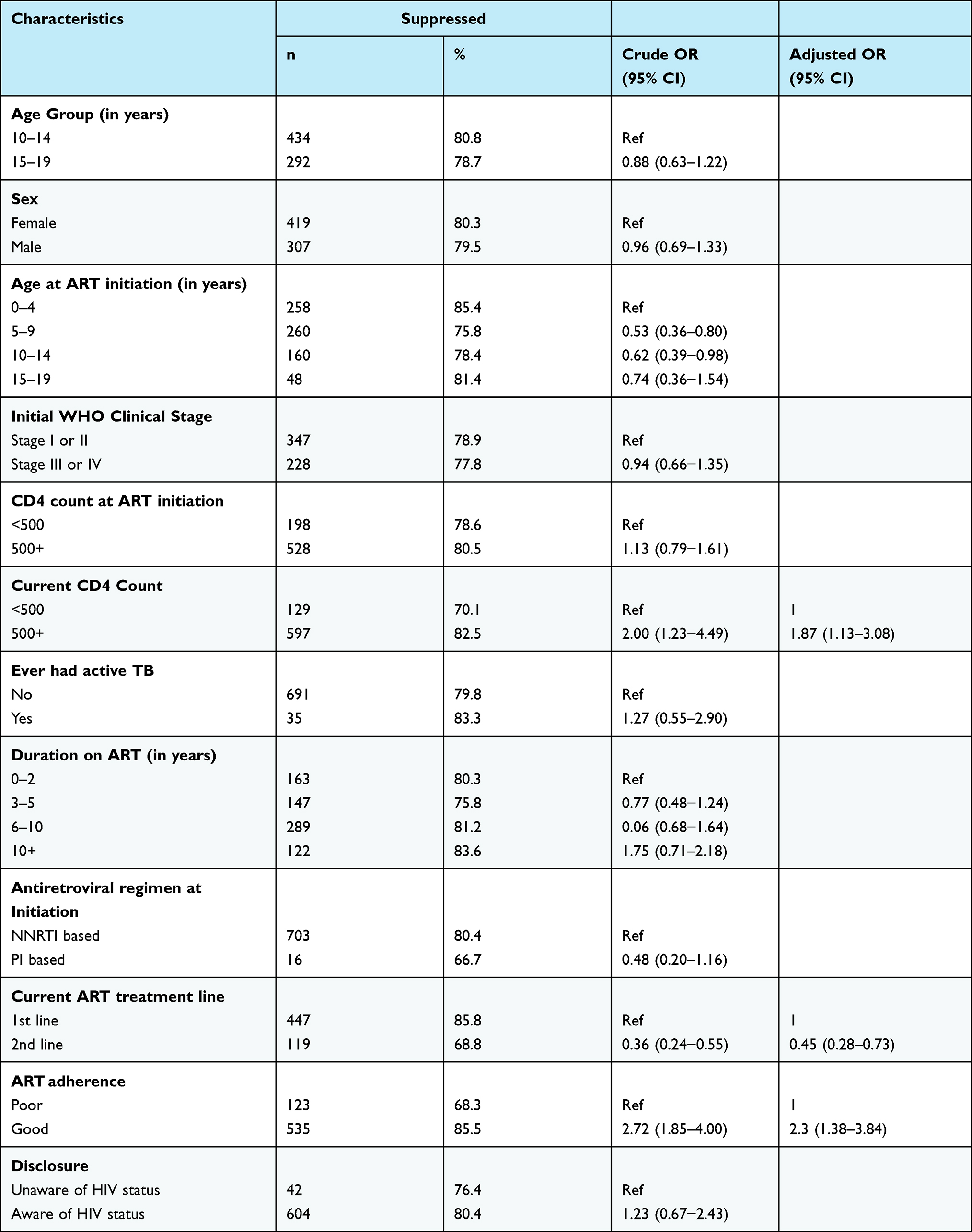 |
Table 2 Factors Associated with Viral Suppression Amongst Adolescents on ART in Homa Bay County, Kenya, 2017 (n=726) |
Discussion
After a median duration of 6.5 years on ART, the rate of viral suppression among adolescents in this study was 80%, which was higher than the national prevalence of 63% reported in 2016.6 This rate is comparable with studies in Eswatini and South Africa, at 84% and 85%, respectively.19,24 However, this observed level of viral suppression falls short of the UNAIDS’ 90-90-90 target.3 The improved viral suppression may be related to the launch of the “test and treat” guidelines in 2016 in Kenya, which placed emphasis on enhanced adherence counseling (EAC) and support for patients with high viral loads.6 Patients with high viral loads receive three sessions of EAC after which a repeat viral load test was performed. Our findings suggest that the WHO target of 90% viral suppression is possible for adolescents in Kenya.
We found no statistically significant difference in viral suppression between younger and older adolescents (10–14 years vs 15–19 years). However, those who initiated ART at 5–9 years and 10–14 years were less likely to be virally suppressed. In Thailand, virological failure was higher among adolescents aged 10–16 years at ART initiation.16 Other studies conducted in Tanzania and Zimbabwe associated older age at ART initiation with viral suppression.17,18 We found no significant association in viral suppression by gender, which is similar to findings in Swaziland.19 However, the study in Tanzania associated virological failure with the female gender,17 whereas two studies in Uganda associated female gender with viral suppression.20,21
In our study CD4 count at ART initiation was not significantly associated with viral suppression, but adolescents who had a current CD4 count above 500 cells/mm3 were more likely to be suppressed. In Tanzania, among children and adolescents, having a high CD4 cell count at ART initiation was associated with better viral suppression.17 In Kenya, changes in national guidelines favored viral load testing over CD4 count tests.6 However, CD4 count reflects a recovering immune system as a result of better viral suppression. Although most patients had initiated ART with a WHO stage of 1 or 2, WHO stage was not significantly associated with viral suppression in our study. This contradicts findings of a study in Vietnam where advanced clinical disease or WHO clinical stage 4 condition at the time of ART initiation was associated with virological failure among adult patients.22
Though some patients had missing data on past infection with tuberculosis (TB), history of TB infection was not found to be significantly associated with viral suppression. A study in South Africa showed that ongoing HIV replication and high viral load was an important risk factor for active TB.23 Similarly, in Uganda, having an active opportunistic infection like TB was associated with low viral suppression across all age categories.20 In South Africa, significantly more patients on TB treatment had unsuppressed viral loads.24 The difference in our findings could be explained by the fact that we collected data on past history of TB and not active (current) TB or being on TB treatment.
The majority of our adolescents were initiated on non-nucleoside reverse transcriptase inhibitor (NNRTI based regimen nevirapine (NVP) or efavirenz (EFV)). However, this did not seem to affect viral suppression. This finding can be explained by the fact that a very small proportion of adolescents were on a protease inhibitor (PI) based regimen at ART initiation.
The majority of the adolescents in our study were still on their first-line ART regimen and had achieved viral suppression. Those on a second-line were less likely to be suppressed. This finding is confirmed by studies that adherence to first-line ART is an important predictor of adherence to second-line ART.25
In our study being aware of one’s HIV status (disclosure) was not significantly associated with viral suppression, because the majority of the adolescents in the study were aware of their HIV status. Delayed disclosure affects adherence and viral suppression in pre-adolescent and adolescent patients.26 In a qualitative study conducted in Uganda, delay in disclosing HIV status to perinatally infected children prior to adolescence was common and led to non-adherence.27 In Zimbabwe, non-disclosure increased the odds of virological failure28 and in Nigeria disclosure of HIV status predicted a better adherence to ART.29 On the contrary, fear of disclosing HIV status to others, especially boy/girlfriends, was an important contributor to suboptimal adherence.30
Conclusions and Recommendations
This was the first study of its kind to examine the factors associated with viral suppression among adolescents living with HIV and on ART in Kenya. Our study found significant improvement in viral suppression rates among adolescents on ART in Homa Bay County when compared to the national average. Our study confirms adherence as the single most important factor associated with achievement of viral suppression. Good adherence was key to viral suppression regardless of current age, age at ART initiation, duration on ART, gender, or ART regimen. Adherence is particularly critical for viral suppression in adolescents who were initiated on ART in pre-adolescence and early adolescence stage. The study echoes the significance of ART on immune recovery and viral suppression, where adolescents with a CD4 count above 500 cells/mm3 had also achieved viral suppression.
The study was not without limitations: due to the retrospective design, we encountered missing records of some of the variables. The missing values were dropped automatically from each variable and analysis conducted based on the totals with complete records; which may have affected the analysis of factors associated with viral suppression.
The study involved retrospective extraction of data from the EMR, which restricted us to routinely collected information. Thus, important variables related to social, cultural, behavioral, and economic factors that are known to affect viral suppression could not be measured.
The strength of this study was its fairly large sample size derived from five sub-county hospitals and one major county referral hospital and thus provided a near true reflection of viral suppression among adolescents receiving ART in Homa Bay County.
The study confirms that adherence on ART is imperative for viral suppression and should be assessed at every visit to identify and address possible barriers that adolescents on ART may experience. Barriers to adherence should be identified and addressed for all adolescents before or upon switching to a second-line ART regimen. Adolescents on second-line therapy should receive intensified adherence support in order to achieve and sustain viral suppression. Further studies (qualitative or mixed methods) are recommended to identify other factors associated with viral suppression, especially social, cultural, and economic factors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNAIDS. Ending the AIDS epidemic for adolescents, with adolescents: a practical guide to meaningfully engage adolescents in the AIDS response,2016. Available from: http://www.unaids.org/en/resources/documents/2016/ending-AIDS-epidemic-adolescents.
2. Ministry of Health. Kenya HIV estimates 2015. Nairobi, Kenya, 2016. Available from: https://nacc.or.ke/…/uploads/2016/12/Kenya-HIV-Estimates-2015.pdf.
3. UNAIDS. 90-90-90: an ambitious treatment target to help end the AIDS epidemic. 2017. Available from: http://www.unaids.org/sites/default/files/media_asset/90-90-90_en.pdf.
4. World Health Organization. Consolidated Guidelines on the Use of Antiretroviral Drugs for Treating and Preventing HIV Infection, Recommendations for a Public Health Approach; 2016 [cited January 10, 2016]. Available from: http://www.who.Int/hiv/pub/arv/arv-2016/en/.
5. World Health Organization. Progress report 2016: prevent HIV, test and treat all. WHO support for country impact, 2017. Available from: http://www.who.int/hiv/pub/progressreports/2016-progress-report/en/.
6. Onsongo S, Abidi SH, Khamadi S, et al. Prevalence of transmitted drug resistance mutations in HIV-1-infected drug-naive patients from urban and suburban regions of Kenya. AIDS Res Hum Retroviruses. 2016;32(3):220–225. doi:10.1089/aid.2015.0026
7. Silverman RA, Beck IA, Kiptinness C, et al. Prevalence of pre-antiretroviral-treatment drug resistance by gender, age, and other factors in HIV-infected individuals initiating therapy in Kenya, 2013–2014. J Infect Dis. 2017;216(12):1569–1578. doi:10.1093/infdis/jix544
8. Ministry of Health. Guidelines on the use of antiretroviral drugs for treating and preventing HIV infection, Nairobi, Kenya, 2017. Available from: https://www.nascop.or.ke/?page_id=2411.
9. Cohen MS, Smith MK, Muessig KE, et al. Antiretroviral treatment of HIV-1 prevents transmission of HIV-1: where do we go from here? Lancet. 2013;382(9903):1515–1524. doi:10.1016/S0140-6736(13)61998-4
10. Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
11. Hanghøj S, Boisen KA. Self-reported barriers to medication adherence among chronically ill adolescents: a systematic review. J Adolesc Health. 2014;54(2):121–138. doi:10.1016/j.jadohealth.2013.08.009
12. Evans D, Menezes C, Mahomed K, et al. Treatment outcomes of HIV-infected adolescents attending public-sector HIV clinics across Gauteng and Mpumalanga, South Africa. AIDS Res Hum Retroviruses. 2013;29(6):892–900. doi:10.1089/AID.2012.0215
13. Nglazi MD, Kranzer K, Holele P, et al. Treatment outcomes in HIV-infected adolescents attending a community-based antiretroviral therapy clinic in South Africa. BMC Infect Dis. 2012;12(1):21. doi:10.1186/1471-2334-12-21
14. Kamya MR, Mayanja-Kizza H, Kambugu A, et al. Predictors of long-term viral failure among Ugandan children and adults treated with antiretroviral therapy. J Acquir Immune Defic Syndr. 2007;46(2):187–193. doi:10.1097/QAI.0b013e31814278c0
15. Ministry of Health. The Kenya AIDS indicator survey. Nairobi, Kenya, 2012. Available from: https://nacc.or.ke/kais-2012-final-report/.
16. Bunupuradah T, Sricharoenchai S, Hansudewechakul R, et al. Risk of first-line antiretroviral therapy failure in HIV-infected Thai children and adolescents. Pediatr Infect Dis J. 2015;34(3):e58–e62. doi:10.1097/INF.0000000000000584
17. Muri L, Gamell A, Ntamatungiro AJ, et al. Development of HIV drug resistance and therapeutic failure in children and adolescents in rural Tanzania: an emerging public health concern. AIDS. 2017;31(1):61–70. doi:10.1097/QAD.0000000000001273
18. Makadzange AT, Higgins-Biddle M, Chimukangara B, et al. Clinical, virologic, immunologic outcomes and emerging HIV drug resistance patterns in children and adolescents in public ART care in Zimbabwe. PLoS One. 2015;10(12):e0144057. doi:10.1371/journal.pone.0144057
19. Jobanputra K, Parker LA, Azih C, et al. Factors associated with virological failure and suppression after enhanced adherence counselling, in children, adolescents and adults on antiretroviral therapy for HIV in Swaziland. PLoS One. 2015;10(2):e0116144. doi:10.1371/journal.pone.0116144
20. Bulage L, Ssewanyana I, Nankabirwa V, et al. Factors associated with virological non-suppression among HIV-positive patients on antiretroviral therapy in Uganda, August 2014-July 2015. BMC Infect Dis. 2017;17(1):326. doi:10.1186/s12879-017-2428-3
21. Kipp W, Alibhai A, Saunders LD, et al. Gender differences in antiretroviral treatment outcomes of HIV patients in rural Uganda. AIDS Care. 2010;22(3):271–278. doi:10.1080/09540120903193625
22. Huong DT, Bannister W, Phong PT, et al. Factors associated with HIV-1 virological failure in an outpatient clinic for HIV-infected people in Haiphong, Vietnam. Int J STD AIDS. 2011;22(11):659–664. doi:10.1258/ijsa.2011.010515
23. Fenner L, Atkinson A, Boulle A, et al. HIV viral load as an independent risk factor for tuberculosis in South Africa: collaborative analysis of cohort studies. J Int AIDS Soc. 2017;20(1):21327. doi:10.7448/IAS.20.1.21327
24. Davey JD, Abrahams Z, Feinberg M, et al. Factors associated with recent unsuppressed viral load in HIV-1-infected patients in care on first-line antiretroviral therapy in South Africa. Int J STD AIDS. 2018;29(6):603–610. doi:10.1177/0956462417748859
25. Ramadhani HO, Bartlett JA, Thielman NM, et al. Association of first-line and second-line antiretroviral therapy adherence. Open Forum Infect Dis. 2014;1(2):ofu079. doi:10.1093/ofid/ofu079
26. Bernheimer JM, Patten G, Makeleni T, et al. Paediatric HIV treatment failure: a silent epidemic. J Int AIDS Soc. 2015;18(1):20090. doi:10.7448/IAS.18.1.20090
27. Inzaule SC, Hamers RL, Kityo C, et al. Long-term antiretroviral treatment adherence in HIV-infected adolescents and adults in Uganda: a qualitative study. PLoS One. 2016;11(11):e0167492. doi:10.1371/journal.pone.0167492
28. Sithole Z, Mbizvo E, Chonzi P, et al. Virological failure among adolescents on ART, Harare City, 2017- A case-control study. BMC Infect Dis. 2018;18(1):469. doi:10.1186/s12879-018-3372-6
29. Ugwu R, Eneh A. Factors influencing adherence to paediatric antiretroviral therapy in Portharcourt, South- South Nigeria. Pan Afr Med J. 2013;16:30. doi:10.11604/pamj.2013.16.30.1877
30. Xu L, Munir K, Kanabkaew C, Le Coeur S, Thorne C. Factors influencing antiretroviral treatment suboptimal adherence among perinatally HIV-infected adolescents in Thailand. PLoS One. 2017;12(2):e0172392. doi:10.1371/journal.pone.0172392
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.