Back to Journals » Cancer Management and Research » Volume 18

Factors Associated with Standardized Diagnosis and Treatment of Breast Cancer: A Real-World Multicenter Study
Authors Liu J, Li L, Zhao X, Hou J
Received 2 January 2026
Accepted for publication 23 February 2026
Published 4 March 2026 Volume 2026:18 588686
DOI https://doi.org/10.2147/CMAR.S588686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bilikere Dwarakanath
Jiaxin Liu,1,2 Lin Li,1,2 Xinchun Zhao,1 Jixue Hou1
1Department of Breast and Thyroid Surgery, First Affiliated Hospital of Shihezi University, Shihezi, Xinjiang, 832000, People’s Republic of China; 2Clinical Medical College, Shihezi University, Shihezi, Xinjiang, 832000, People’s Republic of China
Correspondence: Jixue Hou, Email [email protected]
Objective: Breast cancer remains one of the leading causes of cancer-related death among women, and its incidence in Xinjiang is significantly higher than the national average. However, the extent to which breast cancer diagnosis and treatment are standardized in this region remains unclear, particularly with respect to key clinical decision-making processes such as surgical approach, pathological confirmation, and systemic treatment selection. This study aimed to identify factors associated with standardized breast cancer care within the Xinjiang Production and Construction Corps (XPCC).
Methods: A total of 670 patients who received their first breast cancer diagnosis at 11 XPCC hospitals between January 1, 2021, and January 1, 2022, were retrospectively included. Clinical and pathological variables were collected. According to the Chinese Anti-Cancer Association Guidelines for Breast Cancer (2021 Edition) and the AJCC Cancer Staging Manual (8th Edition), patients were classified into standardized and non-standardized care groups. Univariate and multivariate logistic regression analyses were performed to identify independent factors associated with standardized diagnosis and treatment.
Results: The median age at diagnosis was 53.27 years. The rate of standardized diagnosis was 76.12%. Multivariate analysis indicated that hospital location, ethnicity, and method of detection were independent predictors of standardized diagnosis (P < 0.05). Notably, low rates of preoperative core-needle biopsy and regional disparities in diagnostic capacity were observed. The rate of standardized treatment was 46.71%. Standardized diagnosis, hospital location, pathological type, and tumor stage were independently associated with standardized treatment (P < 0.05), with substantial variations in surgical modality selection, axillary management, neoadjuvant therapy use, and access to radiotherapy across hospitals.
Conclusion: The median age of breast cancer onset in the XPCC region is slightly younger than the national average. Significant disparities in standardized diagnosis and treatment exist between southern and northern Xinjiang, reflecting differences in healthcare infrastructure, availability of pathological testing, radiotherapy resources, and multidisciplinary decision-making capacity. Minority patients exhibited lower levels of disease awareness. These findings underscore the need to strengthen medical resources, optimize guideline-concordant clinical decision-making, and improve breast cancer management in this region.
Keywords: breast cancer, multicenter study, real-world study
Introduction
Breast cancer has become the most commonly diagnosed malignancy among women worldwide and remains the leading cause of cancer-related mortality, according to the latest GLOBOCAN estimates released by the International Agency for Research on Cancer (IARC).1 Considerable geographic disparities in breast cancer incidence, stage at diagnosis, and survival outcomes have been reported, particularly between regions with differing levels of healthcare resources.2–6 These differences are often attributed to variations in screening accessibility, health awareness, socioeconomic development, and the availability of standardized diagnostic and treatment services.7,8
In China, the incidence of breast cancer has shown a continuous upward trend, with the highest incidence observed among women aged 45–49 years9. Lifestyle changes associated with rapid socioeconomic development, including reduced physical activity, increased obesity rates, and shortened breastfeeding duration, have further contributed to the rising disease burden.10–12 Notably, the Xinjiang region exhibits a significantly higher incidence of breast cancer than the national average.13 Previous studies have demonstrated that ethnic minority women in Xinjiang present distinct clinicopathological characteristics and poorer survival outcomes compared with Han women, underscoring potential disparities in healthcare access and treatment quality.14,15
Surgical management remains a cornerstone of breast cancer treatment. In Western countries, more than half of patients with early-stage breast cancer undergo breast-conserving surgery (BCS), whereas the rate of breast conservation in China has historically been much lower.16 Previous studies have reported that nearly 90% of early-stage breast cancer patients in China underwent mastectomy rather than BCS, although this proportion decreased to approximately 50% by 2015 and fluctuated between 51.1% and 54.5% until 2017.17 This discrepancy may be partly attributable to the limited availability of radiotherapy resources and a shortage of adequately trained radiation oncologists and technical staff. In addition, insufficient patient awareness of breast-conserving options, concerns regarding cosmetic outcomes, and fear of disease recurrence may further influence surgical decision-making.18–21 Compared with BCS, mastectomy may result in greater body image disturbance and psychological distress, thereby adversely affecting patients’ quality of life.
In recent years, advances in multidisciplinary breast cancer management have led to the increasing use of neoadjuvant therapy.22 Neoadjuvant treatment can facilitate tumor downstaging, increase surgical resectability and breast conservation rates, and provide valuable information for subsequent therapeutic decision-making, thereby potentially improving patient prognosis.23 However, challenges remain in accurately assessing treatment response, optimizing treatment selection and timing, and managing treatment-related adverse effects, highlighting the need for further investigation into the real-world implementation of standardized treatment strategies.24
Despite these developments, limited evidence is available regarding the extent to which breast cancer diagnosis and treatment within the Xinjiang Production and Construction Corps (XPCC) adhere to established clinical guidelines. Given the unique multi-ethnic composition and variability in healthcare resources across XPCC hospitals, a comprehensive evaluation of standardized diagnostic and therapeutic practices is warranted.25 Therefore, this multicenter, real-world study aimed to assess the current status of breast cancer diagnosis and treatment in XPCC hospitals and to identify key factors associated with standardized care, thereby providing evidence to inform targeted interventions and improve the overall quality of breast cancer management in this region.
Materials and Methods
Study Population
This multicenter, real-world retrospective study included breast cancer patients who received their first diagnosis between January 1, 2021, and January 1, 2022, at 11 hospitals within the Xinjiang Production and Construction Corps (XPCC). Hospitals in southern Xinjiang included the First, Second, and Third Division Hospitals, whereas hospitals in northern Xinjiang included the Fifth, Sixth, Seventh, Eighth, Ninth, Tenth, and Thirteenth Division Hospitals, as well as the First Affiliated Hospital of Shihezi University. A total of 670 patients met the inclusion criteria and were included in the final analysis. Across the 11 participating hospitals, the number of included patients per center ranged from 9 to 206.
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) female patients; (2) age ≥ 18 years; and (3) pathologically confirmed primary breast cancer.
The exclusion criteria included: (1) bilateral breast cancer; (2) a history of other malignant tumors; (3) non-primary breast cancer; and (4) insufficient clinical information that prevented assessment of standardized diagnosis and treatment.
Data Collection
Data were collected across three domains. General clinical characteristics included hospital location, age at diagnosis, marital status, ethnicity, medical history, smoking and alcohol consumption history, family history of breast cancer, and menopausal status. Tumor-related clinicopathological features included tumor laterality and quadrant, BI-RADS category at first detection, presence of symptoms, method of detection, tumor size, lymph node status, pathological type, clinical stage, Ki-67 expression, and immunohistochemical markers including estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2). Treatment-related variables included whether a core-needle biopsy was performed before surgery, type of breast surgery and axillary lymph node surgery, use of neoadjuvant therapy, and receipt of postoperative chemotherapy, endocrine therapy, targeted therapy, radiotherapy, or other treatments. Detailed variable definitions and coding schemes are summarized in Table 1.
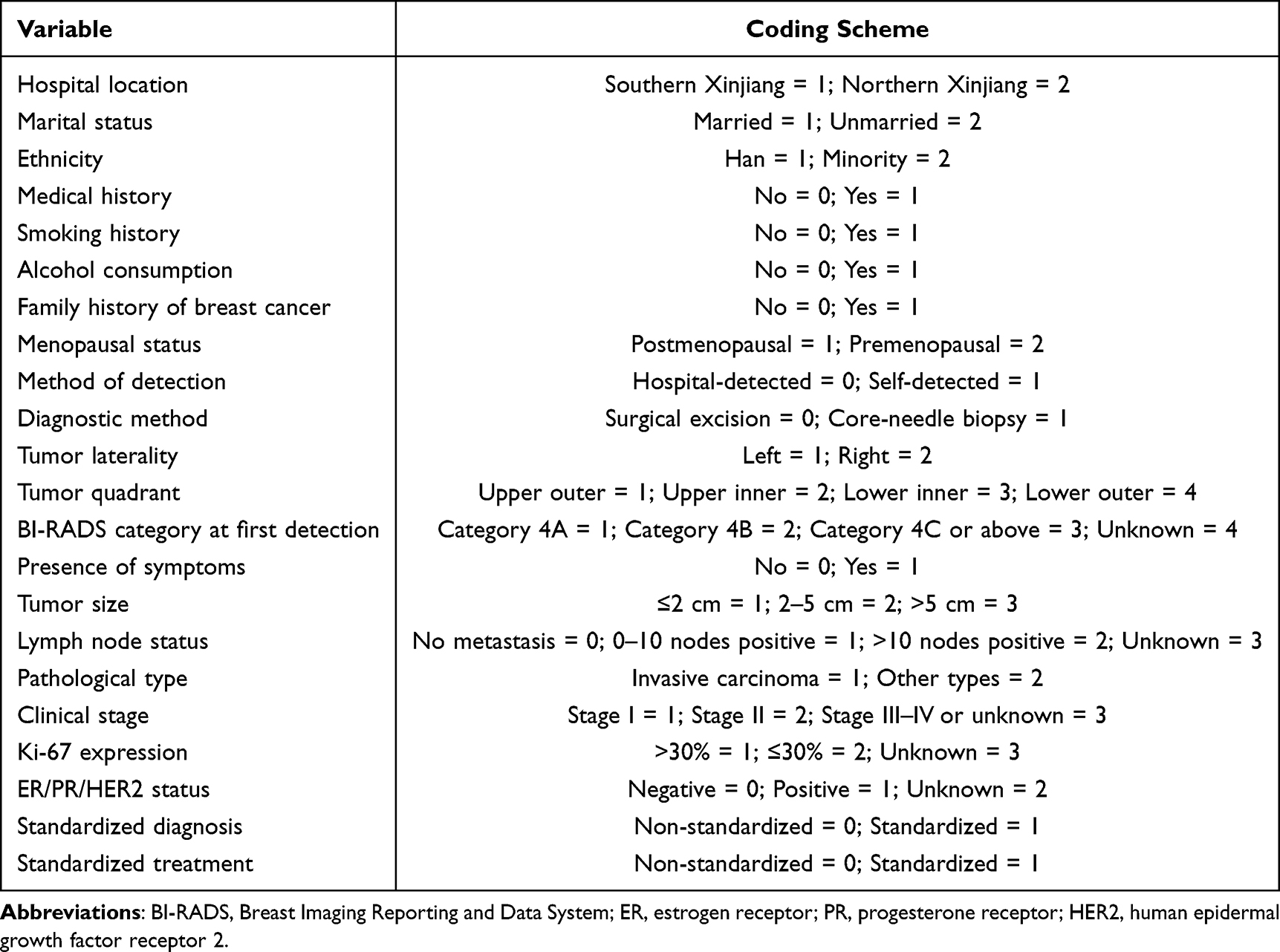 |
Table 1 Variable Assignment Notes |
Definition of Standardized Diagnosis and Treatment
Standardized diagnosis was defined based on adherence to the AJCC Cancer Staging Manual (8th Edition), including complete clinical staging and documentation of molecular subtype classification. Cases lacking appropriate staging or molecular profiling were considered non-standardized. Reasons for non-standardized diagnosis were recorded.
Standardized treatment was defined according to the recommendations of the Chinese Anti-Cancer Association Guidelines for Breast Cancer (2021 Edition) and the NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Treatment plans were evaluated based on molecular subtype, pathological stage, and the presence of high-risk factors. Patients who received guideline-concordant therapy were classified into the standardized treatment group, whereas those who were undertreated or overtreated relative to guideline recommendations were assigned to the non-standardized group. Reasons for non-standardized treatment were also documented.
Statistical Analysis
Statistical analyses were performed using SPSS version 27.0. Categorical variables were presented as frequencies and percentages and compared using the chi-square test. Continuous variables following a normal distribution were expressed as mean ± standard deviation and compared using the independent-samples t-test. Skewed continuous variables were reported as median (interquartile range, IQR) and compared using the Wilcoxon rank-sum test. Univariate analysis and binary logistic regression models were used to identify factors associated with standardized diagnosis and treatment. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. A two-tailed P < 0.05 was considered statistically significant.
Results
General Clinical Characteristics
A total of 670 patients aged 28–87 years were included, with a peak age distribution between 48 and 52 years. The mean age at diagnosis was 53.27 years (Figure 1). Most patients were from northern Xinjiang (n = 558, 83.28%). Individuals aged 43–62 years accounted for more than 70% of the study population. The majority were married (n = 629, 93.88%) and of Han ethnicity (n = 602, 89.85%). More than half of the patients had no prior medical history (n = 376, 56.12%), and only 5 patients (0.75%) reported a family history of breast cancer. Smoking and alcohol consumption were uncommon, reported by 9 (1.34%) and 13 patients (1.94%), respectively. Additionally, 396 patients (59.10%) were postmenopausal (Table 2).
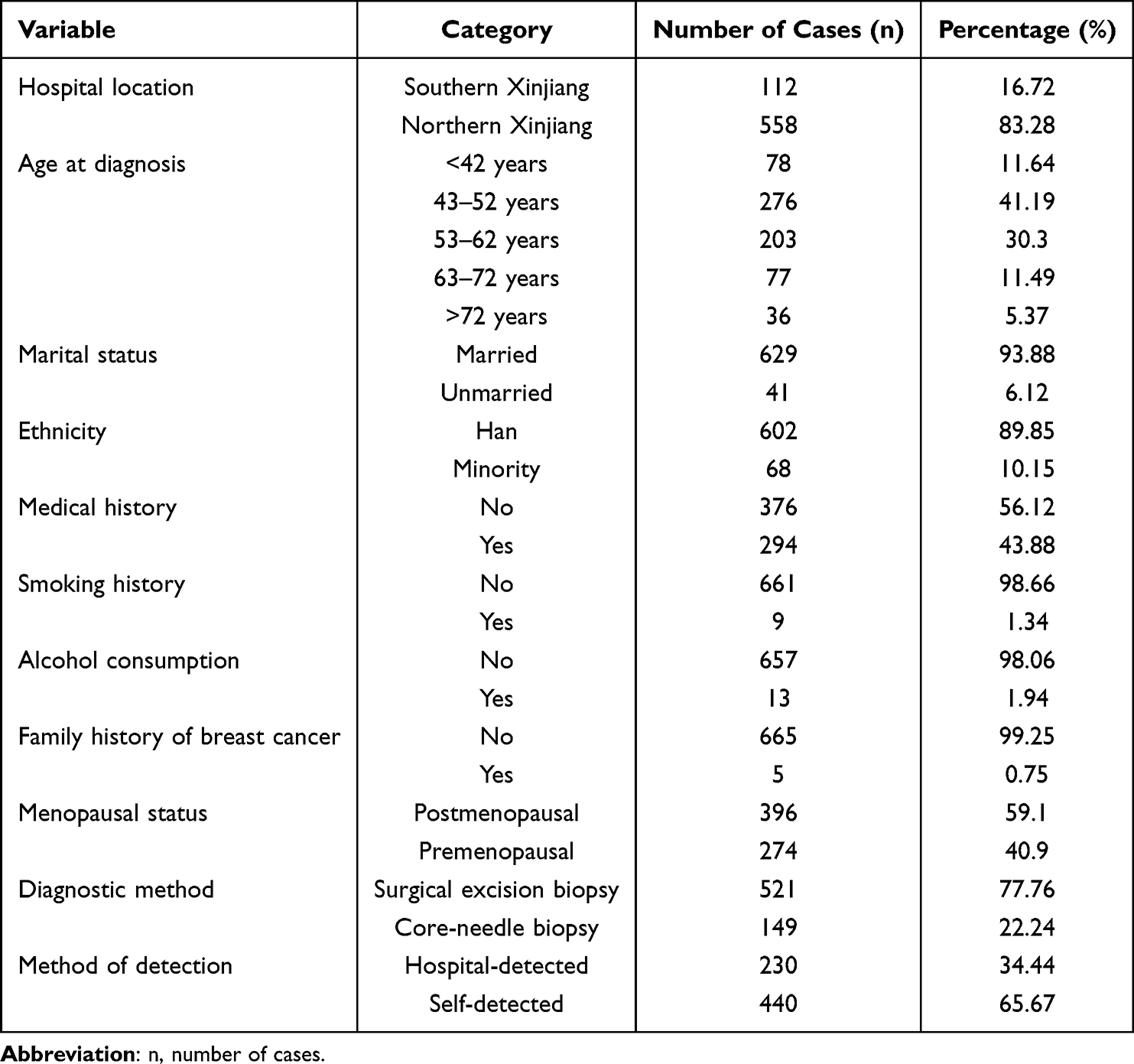 |
Table 2 Baseline Data on Breast Cancer in Hospitals of Some Divisions and Cities of Xinjiang Production and Construction Corps (2021–2022) |
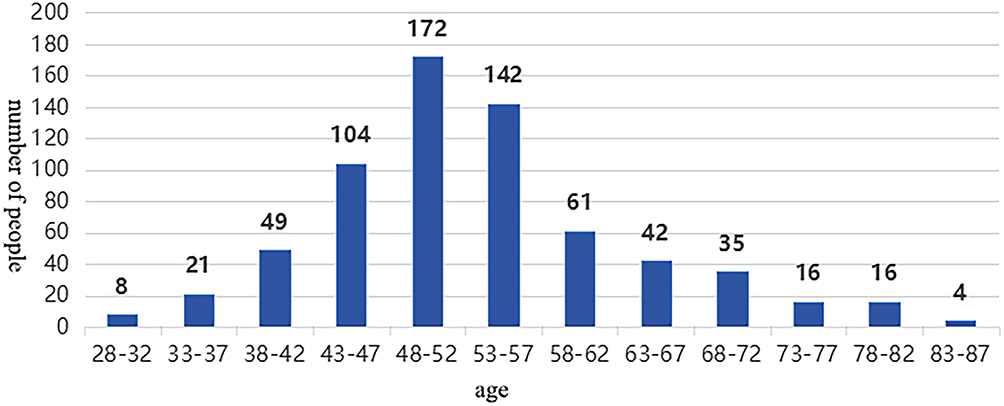 |
Figure 1 Distribution of breast cancer patients by age group in hospitals of some divisions and cities of Xinjiang Production and Construction Corps (2021–2022). |
Tumor Clinicopathological Characteristics
Tumor laterality was almost evenly distributed, with 334 (49.85%) tumors located in the left breast and 336 (50.15%) in the right breast. The upper outer quadrant was the most common tumor location (n = 200, 29.85%). At first detection, 342 patients (51.04%) were classified as BI-RADS 4B, and 121 (18.06%) as BI-RADS 4C or higher. More than half of the patients (n = 349, 52.09%) presented with symptoms at the time of diagnosis. Tumor size ranged from ≤2 cm in 267 patients (39.85%) to 2–5 cm in 344 patients (51.34%), whereas 59 patients (8.81%) had tumors >5 cm. Most patients had no lymph node metastasis (n = 460, 68.66%), while 188 (28.06%) had 1–10 positive lymph nodes and 22 (3.28%) had >10 positive nodes. The predominant pathological type was invasive carcinoma (n = 614, 91.64%). Stage II disease accounted for 370 cases (55.22%), followed by stage I (n = 197, 29.40%) and stage III–IV (n = 56, 8.36%); staging information was unknown in 47 patients (7.01%). Regarding proliferation and receptor status, 321 patients (47.91%) had a Ki-67 index ≤30%. ER, PR, and HER2 positivity were observed in 433 (64.63%), 343 (51.19%), and 162 (24.18%) patients, respectively (Table 3).
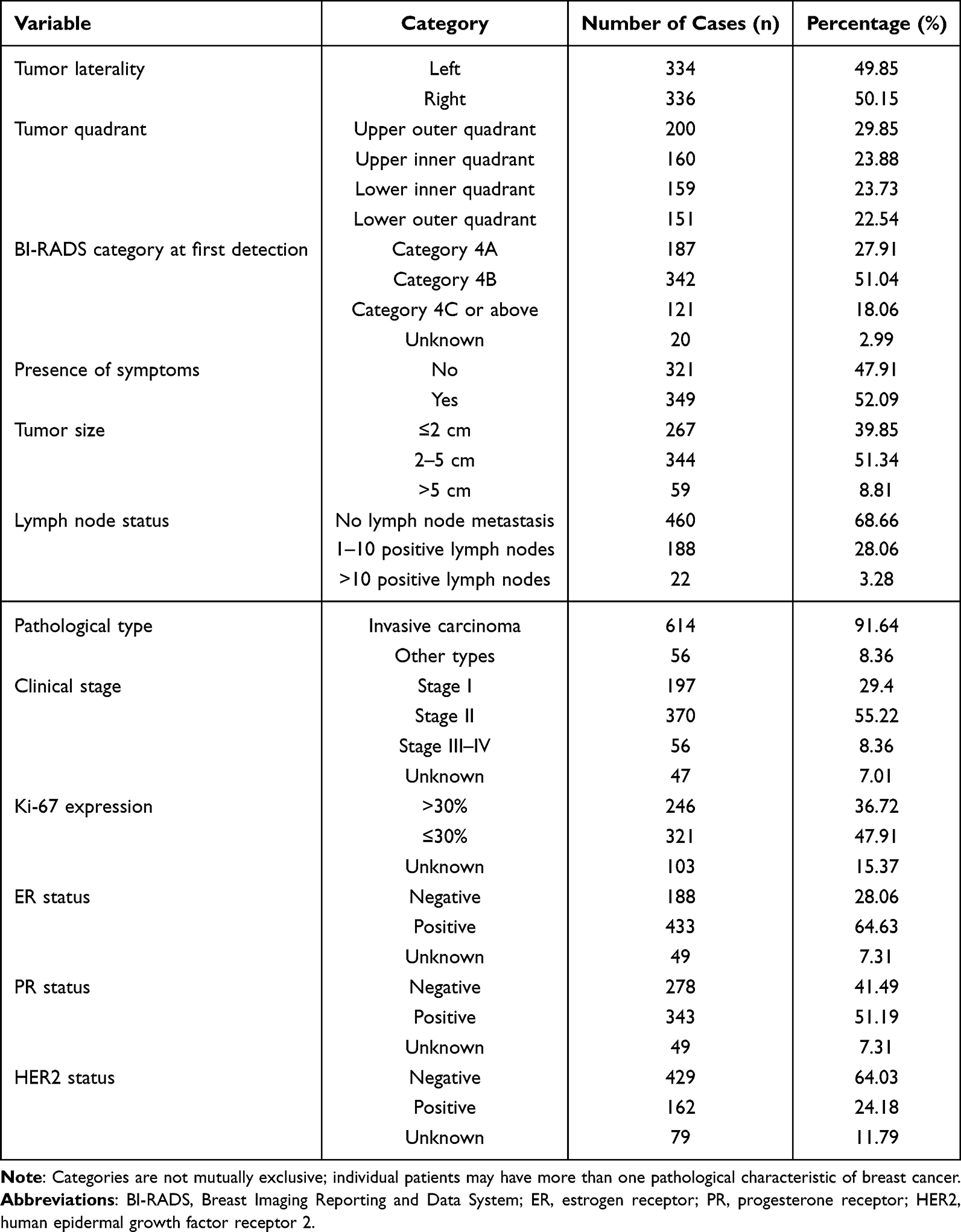 |
Table 3 Pathological Characteristics of Breast Cancer in Hospitals of Some Divisions and Cities of Xinjiang Production and Construction Corps from 2021 to 2022 |
Treatment Patterns
Among the 670 patients, 582 (86.87%) underwent mastectomy, while 88 (13.13%) received breast-conserving surgery. For axillary management, 298 patients (44.48%) underwent sentinel lymph node biopsy alone, 178 (26.57%) received sentinel lymph node biopsy combined with axillary lymph node dissection, and 149 (22.24%) underwent axillary lymph node dissection alone; surgical details were unknown in 45 cases (6.72%). Preoperative core-needle biopsy was performed in 149 patients (22.24%), and 101 patients (15.07%) received neoadjuvant therapy. Postoperative chemotherapy and endocrine therapy were administered in 438 (65.37%) and 401 (59.85%) patients, respectively. In contrast, the proportions of patients receiving targeted therapy and radiotherapy were relatively low, at 143 (21.34%) and 140 (20.90%), respectively. A small number of patients (n = 14, 2.09%) received Uygur medicine, traditional Chinese medicine, or other alternative treatments (Table 4).
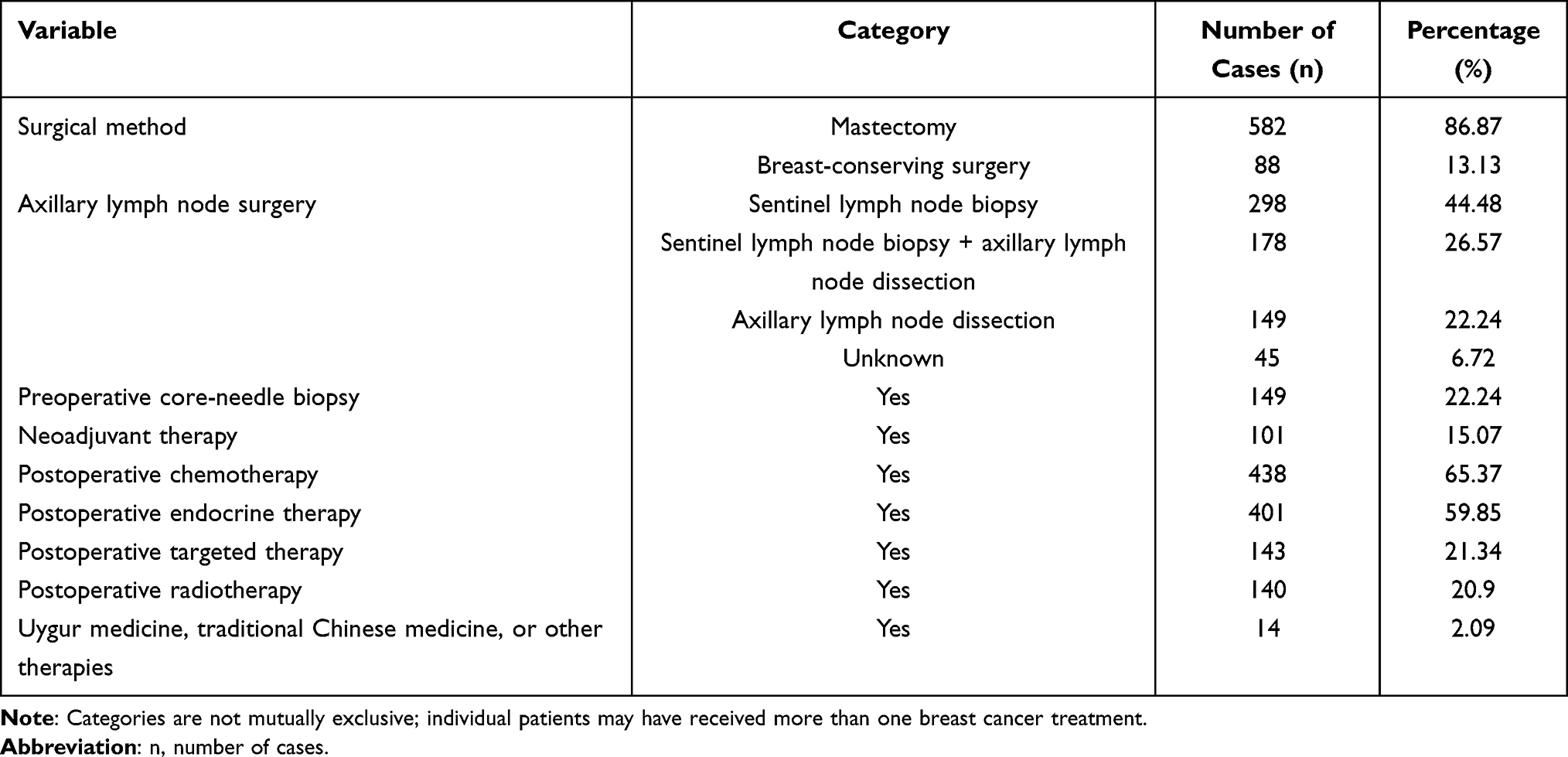 |
Table 4 Breast Cancer Treatment in Hospitals of Some Divisions and Cities of Xinjiang Production and Construction Corps from 2021 to 2022 |
Factors Associated with Standardized Diagnosis
Univariate Analysis of Factors Associated with Standardized Diagnosis
In the univariate analysis, hospital location, ethnicity, menopausal status, and method of detection were significantly associated with standardized diagnosis (P < 0.05), whereas marital status, medical history, smoking, alcohol consumption, family history, presence of symptoms, and diagnostic method showed no significant association (P > 0.05) (Table 5).
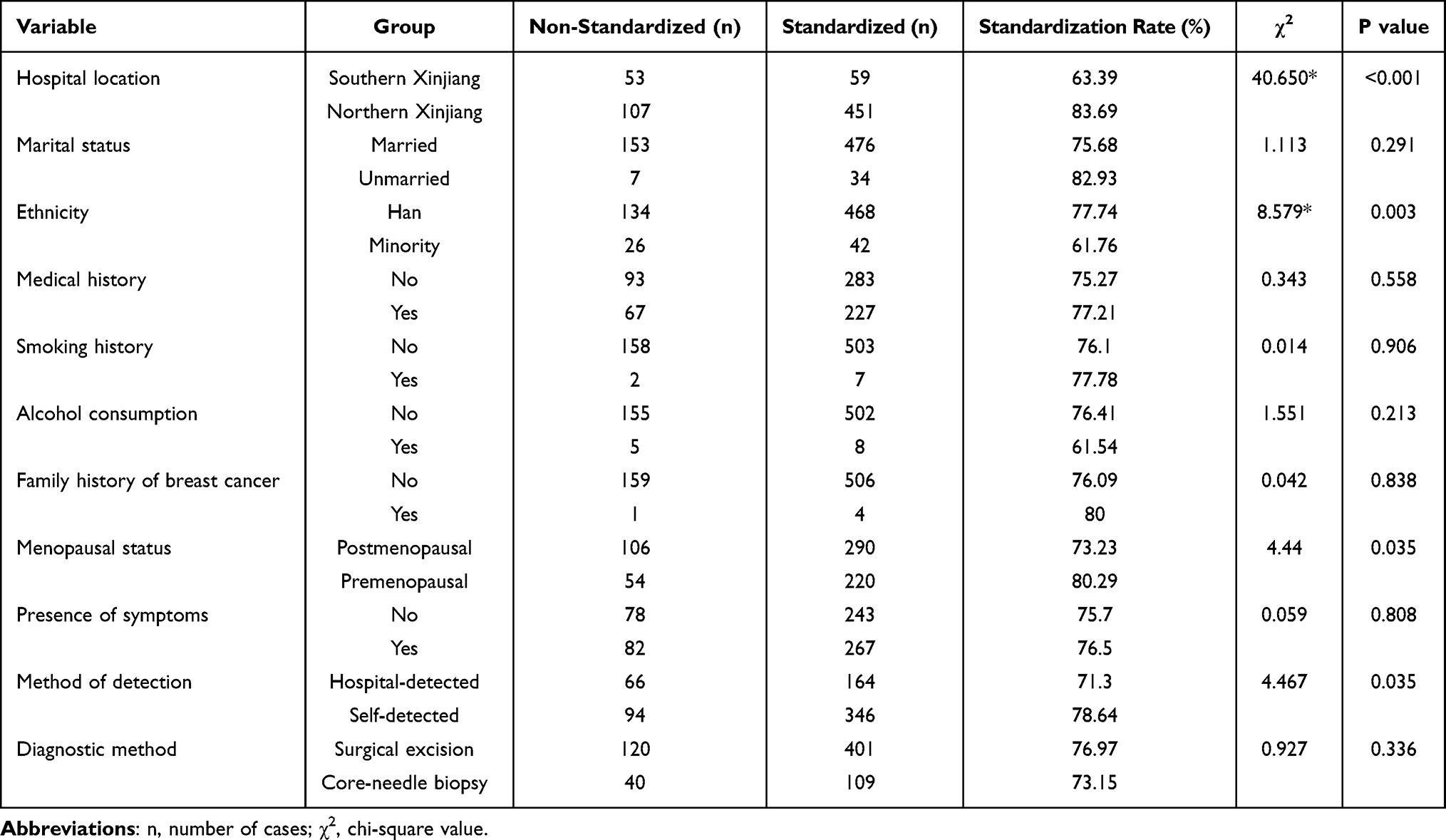 |
Table 5 Single-Factor Analysis of the Diagnostic Specification Rate for Breast Cancer in Hospitals of Some Divisions and Cities of Xinjiang Production and Construction Corps from 2021 to 2022 |
Multivariate Analysis of Factors Associated with Standardized Diagnosis
Variables with P < 0.05 in the univariate analysis were included in the multivariate logistic regression model. The results showed that hospital location, ethnicity, and method of detection were independent predictors of standardized diagnosis, while menopausal status was not (P > 0.05). Patients treated in southern Xinjiang had significantly lower odds of receiving standardized diagnosis compared with those in northern Xinjiang (OR = 0.290, 95% CI: 0.187–0.449). Han patients were more likely to receive standardized diagnosis than ethnic minority patients (OR = 1.771, 95% CI: 1.014–3.094). In addition, patients whose tumors were self-detected had higher odds of standardized diagnosis than those whose tumors were detected through hospital examination (hospital-detected vs self-detected: OR = 0.644, 95% CI: 0.440–0.942) (Table 6).
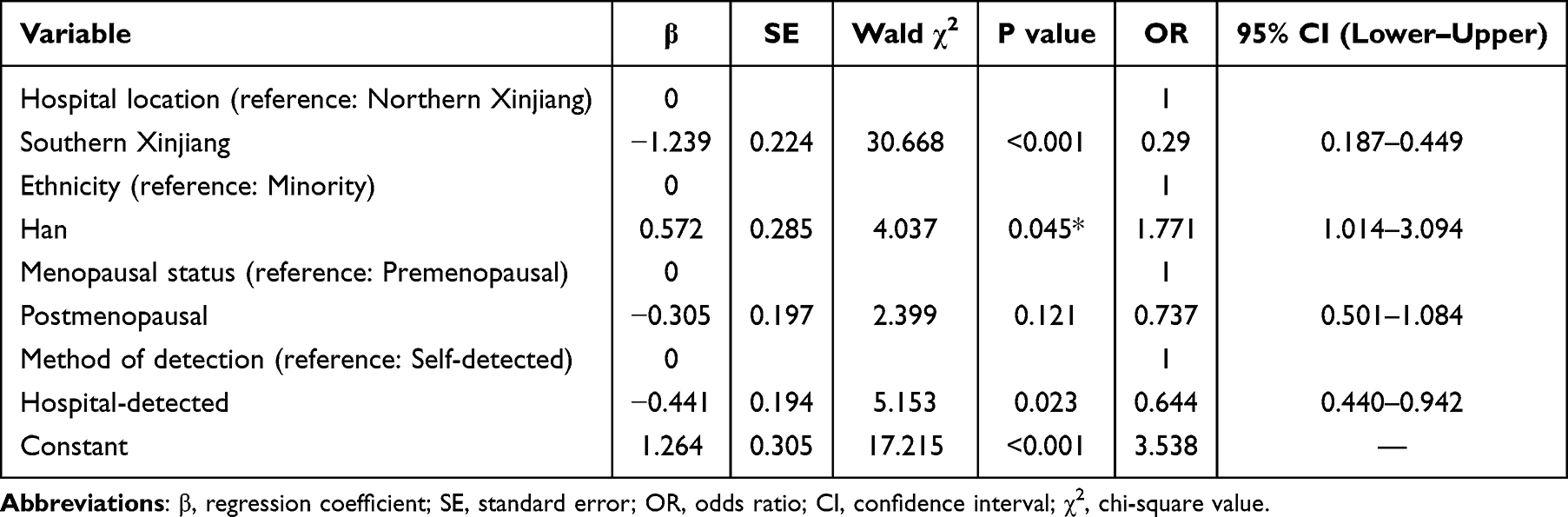 |
Table 6 Multivariate Analysis of the Diagnostic Specification Rate of Breast Cancer in Some Divisional Hospitals of Xinjiang Production and Construction Corps from 2021 to 2022 |
Factors Associated with Standardized Treatment
Univariate Analysis of Factors Associated with Standardized Treatment
Univariate analysis revealed that hospital location, ethnicity, menopausal status, diagnostic method, pathological type, clinical stage, ER status, PR status, HER2 status, HR+HER2− subtype, unknown subtype, and standardized diagnosis were significantly associated with standardized treatment (P < 0.05). In contrast, marital status, medical history, smoking, alcohol consumption, family history, method of detection, tumor laterality, tumor quadrant, BI-RADS category, tumor size, lymph node status, Ki-67 expression, and other molecular subtypes were not significantly associated with standardized treatment (P > 0.05) (Table 7).
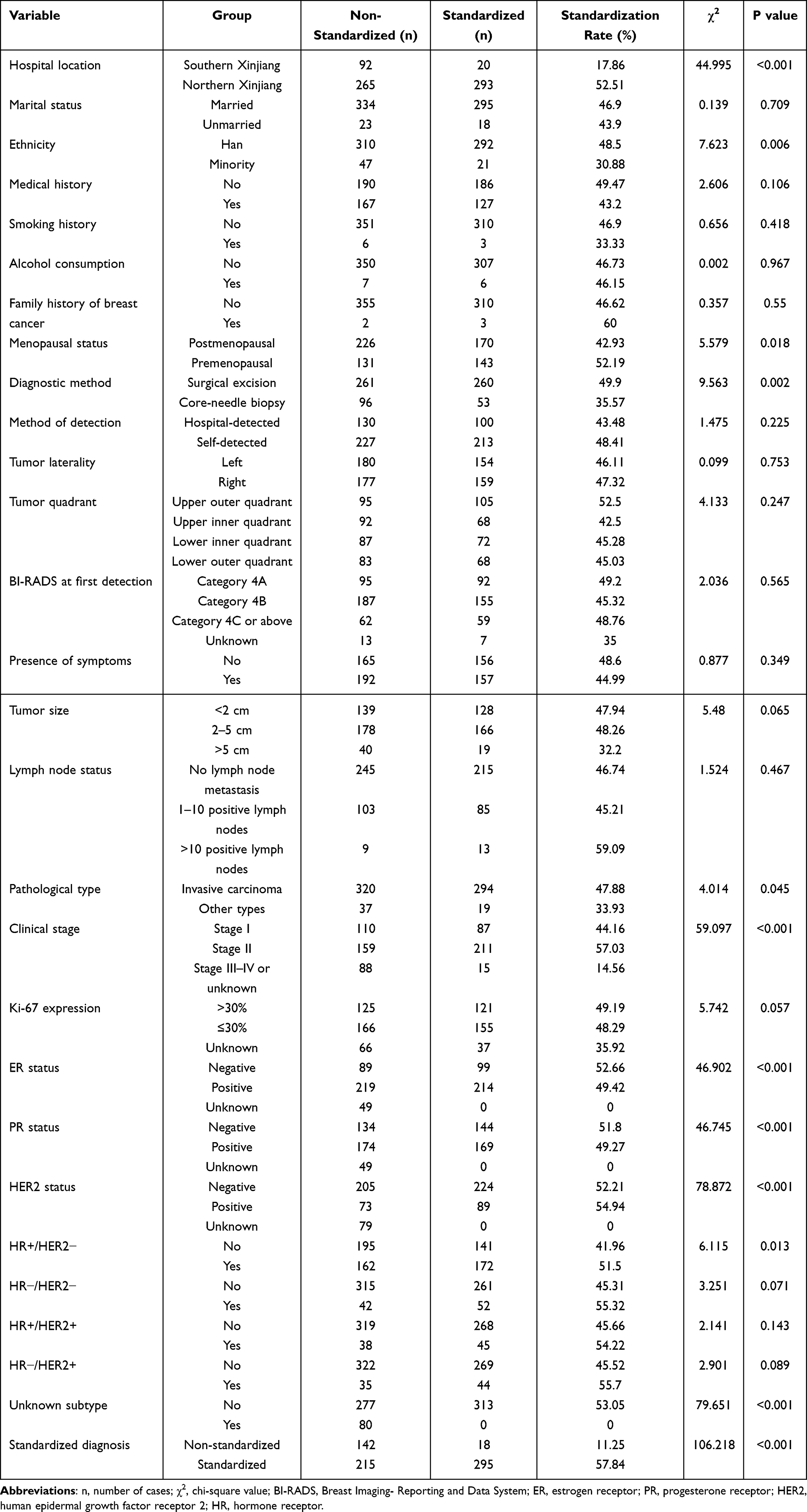 |
Table 7 Univariate Analysis of the Treatment Compliance Rate for Breast Cancer in Hospitals of Some Divisions and Cities of Xinjiang Production and Construction Corps from 2021 to 2022 |
Multivariate Analysis of Factors Associated with Standardized Treatment
Variables with P < 0.05 in the univariate analysis were entered into a multivariate logistic regression model. Due to collinearity between ER, PR, and HER2 status and standardized diagnosis, only standardized diagnosis was included in the multivariable model. The results showed that standardized diagnosis, hospital location, pathological type, and clinical stage were independent factors associated with standardized treatment, whereas ethnicity and diagnostic method were not (P > 0.05). Patients with non-standardized diagnosis had markedly lower odds of receiving standardized treatment compared with those with standardized diagnosis (OR = 0.126, 95% CI: 0.073–0.218). Treatment standardization was higher in northern Xinjiang than in southern Xinjiang (southern vs northern: OR = 0.276, 95% CI: 0.155–0.491). Compared with patients with stage III–IV or unknown stage, those with stage II and stage I disease were more likely to receive standardized treatment (OR = 2.089, 95% CI: 1.056–4.136; OR = 4.272, 95% CI: 2.234–8.169, respectively). In addition, patients with invasive carcinoma were more likely to receive standardized treatment than those with other pathological types (OR = 2.207, 95% CI: 1.168–4.170) (Table 8).
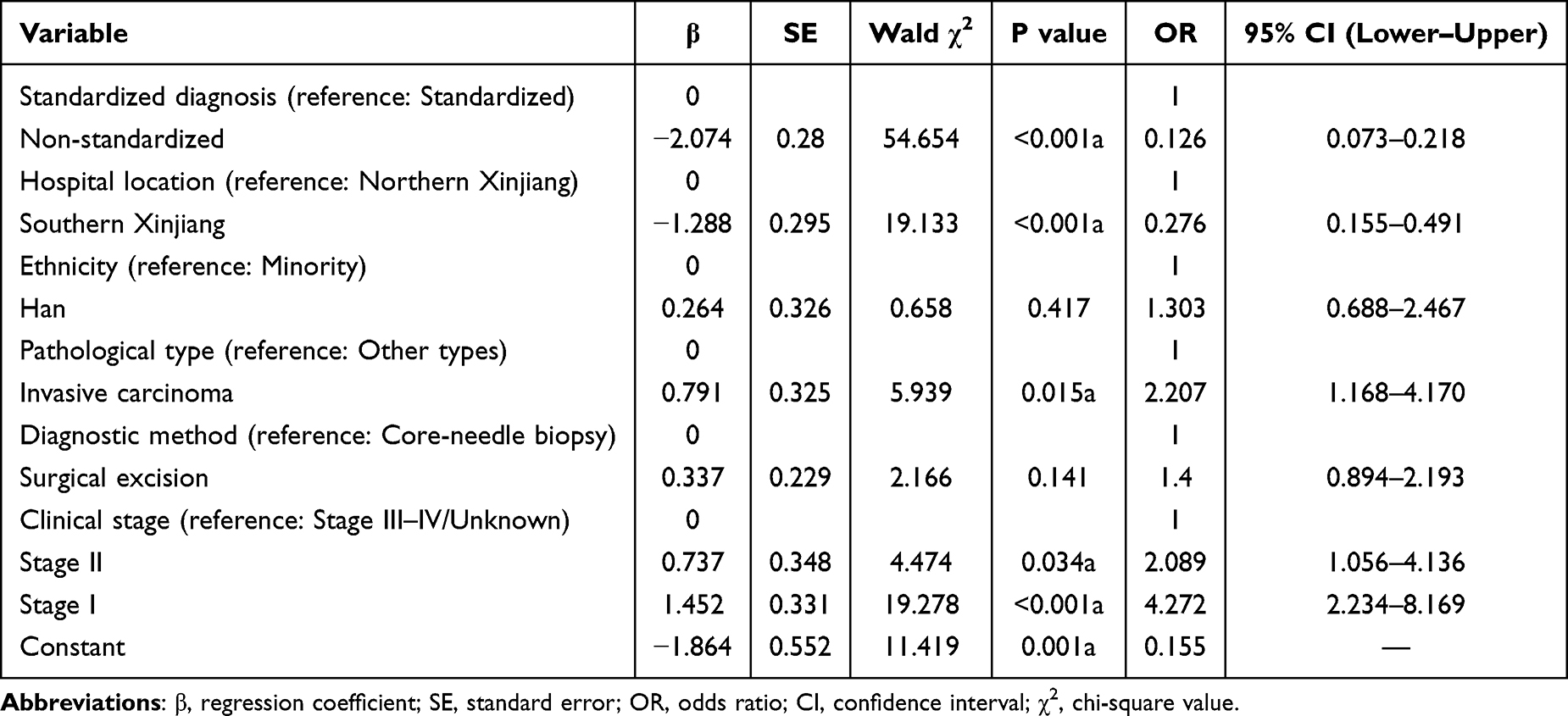 |
Table 8 Multivariate Analysis of the Rate of Breast Cancer Treatment Compliance in Hospitals of Some Divisions and Cities of Xinjiang Production and Construction Corps from 2021 to 2022 |
Discussion
Breast cancer incidence in China has continued to rise over recent decades, accompanied by a trend toward younger age at onset. National epidemiological data indicate that the median age at diagnosis is approximately 55 years, with the majority of cases occurring between 45 and 65 years.10 In the present study, patients from the Xinjiang Production and Construction Corps (XPCC) exhibited a slightly younger median age of 53.27 years. This finding suggests a potential earlier onset pattern among women in the XPCC compared with the national average, underscoring the need for region-specific prevention strategies and age-appropriate screening programs. Although breast-conserving surgery (BCS) has been increasingly adopted in China, the BCS rate in the XPCC remained low at 13.13% in this study. Notably, none of the participating hospitals had established breast oncoplastic or reconstructive surgery programs, which may substantially limit surgical options for patients. Compared with more developed mainland regions, this gap highlights considerable room for improvement in surgical capacity and the promotion of standardized breast-conserving approaches. In addition to institutional factors, patient-related considerations—including limited awareness of BCS, concerns regarding postoperative radiotherapy, and fear of recurrence—may also influence surgical decision-making.26 Given that mastectomy may be associated with greater body image disturbance and psychological stress, the low uptake of BCS may have important implications for patients’ quality of life. Similarly, the utilization rate of neoadjuvant therapy was relatively low (15.07%) in the XPCC cohort. Multiple factors may contribute to this pattern, including misconceptions regarding the safety or effectiveness of neoadjuvant treatment, concerns about delaying surgery, and limited access to timely medical information—particularly among ethnic minority populations. Cultural and language barriers may further influence treatment preferences, with some patients favoring immediate surgical intervention over systemic therapy. At the institutional level, the absence of well-established multidisciplinary team (MDT) frameworks in many hospitals may hinder standardized evaluation and implementation of neoadjuvant treatment. In addition, insurance coverage limitations and financial constraints may reduce patients’ willingness or ability to receive recommended therapies.
Decisions regarding axillary surgery also reflect variability in real-world clinical practice. The choice between sentinel lymph node dissection (SLND) and axillary lymph node dissection (ALND) is often influenced by preoperative imaging findings, surgeon experience, institutional protocols, and resource availability. In settings where standardized diagnostic workup or multidisciplinary discussion is limited, such variability may contribute to deviations from guideline-recommended axillary management. Notably, the standardization rate of breast cancer diagnosis in southern Xinjiang was significantly lower than that observed in northern Xinjiang. This disparity likely reflects differences in medical resources and diagnostic capacity. Missing immunohistochemistry results and incomplete staging documentation were more frequently observed in southern Xinjiang. Furthermore, some hospitals lacked fluorescence in situ hybridization (FISH) testing capabilities or relied on external tertiary centers for pathological review, leading to delays or incomplete molecular subtyping. As accurate and standardized diagnosis forms the foundation for appropriate treatment planning, these diagnostic deficiencies may result in downstream deviations from guideline-concordant therapy.
Multivariate analysis further identified hospital location, pathological type, and clinical stage as independent factors influencing treatment standardization. Patients with invasive carcinoma were more likely to receive guideline-based treatment than those with other pathological types, potentially because treatment pathways for invasive disease are more clearly defined and supported by stronger clinical evidence. In addition, patients diagnosed at earlier stages were more likely to receive standardized treatment, which may reflect both greater feasibility of guideline adherence and fewer treatment-related constraints. Conversely, reduced adherence among patients with advanced-stage disease may be attributable to physical frailty, increased financial burden, or heightened psychological stress. Several limitations of this study should be acknowledged. As a retrospective, multicenter analysis conducted within selected XPCC hospitals, the findings may not fully represent all institutions in the region. Socioeconomic factors—including income level, educational attainment, and insurance coverage—were not collected, although these variables are known to influence access to care and treatment adherence.27–29 In addition, the relatively short observation period precluded the evaluation of long-term oncological outcomes, such as disease-free survival and overall survival. These limitations should be considered when interpreting the results, and future prospective studies incorporating longer follow-up and broader socioeconomic data are warranted to further elucidate determinants of standardized breast cancer care In conclusion, substantial regional disparities persist in the standardization of breast cancer diagnosis and treatment within the XPCC, particularly between northern and southern Xinjiang. Strengthening pathology services, expanding access to molecular diagnostic technologies, improving multidisciplinary collaboration, and enhancing patient education—especially among ethnic minority populations—are critical steps toward improving guideline-concordant care.30,31 Tailoring management strategies according to pathological subtype and disease stage, while providing additional support for patients with advanced disease, may further contribute to improving the overall quality of breast cancer management in this region.32
Conclusion
This study demonstrates pronounced regional disparities in the standardization of breast cancer diagnosis and treatment within the Xinjiang Production and Construction Corps, with substantially lower adherence observed in southern Xinjiang. Standardized diagnosis emerged as the most important determinant of guideline-concordant treatment, while hospital location, pathological type, and clinical stage were also independently associated with treatment adherence. These findings highlight the critical role of diagnostic capacity in shaping downstream treatment decisions. Strengthening pathology services, expanding multidisciplinary collaboration, and improving patient education—particularly among ethnic minority populations—are essential steps toward enhancing the consistency and quality of breast cancer care across the region.
Study Limitations
Several limitations of this study should be acknowledged. Although data were collected from multiple hospitals within the Xinjiang Production and Construction Corps, the participating institutions may not fully represent all healthcare settings in the region. As a retrospective analysis, the study depended on the completeness and accuracy of medical records, and incomplete pathological or molecular information may have affected the evaluation of diagnostic standardization. In addition, socioeconomic variables, such as income level, educational attainment, and insurance coverage, were not available for analysis, despite their potential influence on treatment decision-making and adherence. Finally, the absence of long-term follow-up data precluded assessment of oncological outcomes, limiting conclusions regarding the clinical impact of non-standardized diagnosis and treatment. Future prospective studies with extended follow-up and more comprehensive data collection are warranted to further clarify determinants of standardized breast cancer care in this region.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Research Ethics Committee of the First Affiliated Hospital of Shihezi University (Approval No.: KJ2023-546-01). Written informed consent was obtained from all participants prior to study commencement. We state that our study complies with the Declaration of Helsinki.
Funding
Key Technology Research Project in Key Areas (2024AB065).
Disclosure
The authors declare that there is no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–13. doi:10.3322/caac.21834
2. Xiong X, Zheng LW, Ding Y, et al. Breast cancer: pathogenesis and treatments. Signal Transduct Target Ther. 2025;10(1):49. doi:10.1038/s41392-024-02108-4
3. Demirors B, Ahmed SH, Grace K, et al. Geographic variations in demographics, socioeconomic status, and stage at diagnosis among hormone receptor-positive invasive ductal carcinoma: an NCDB analysis (2004–2020). Anticancer Res. 2026;46(2):811–817. doi:10.21873/anticanres.17989
4. Pasokh Z, Mazidimoradi A, Hamidian M, Shahabinia Z, Kiani M, Salehiniya H. National and subnational burden of female breast cancer in Iran from 2010 to 2021. Diseases. 2025;14(1):15. doi:10.3390/diseases14010015
5. Brooks JD, Blackmore KM, Ngo NNM, et al. Canadian women’s attitudes toward receiving personalized breast cancer risk information: insights from the PERSPECTIVE I&I project. Clin Breast Cancer. 2025. doi:10.1016/j.clbc.2025.12.009
6. Rabe M, Robinson NM. Breast cancer survivorship in South Africa: a holistic primary care approach. South Afr Family Pract. 2026;68(1):e1–e6. doi:10.4102/safp.v68i1.6200
7. Nguyen CQ, Gunaratne SD, Clune CG, Sandhu NP, Klassen CL. Management during pregnancy and lactation of patients who are at high risk of breast cancer. Maturitas. 2026;206. doi:10.1016/j.maturitas.2026.108860
8. Sivapalan S, Chuba PJ, Szpunar SM, et al. All-cause mortality by race and socioeconomic status among women treated for breast cancer in metropolitan Detroit. Cancer Epidemiol. 2026;101. doi:10.1016/j.canep.2026.103013
9. Luan HH, Luo LS, Lu ZY. Historical trends in incidence of breast cancer in Shanghai, Hong Kong and Los Angeles, 1973–2012: a joinpoint and age-period-cohort analysis. Int J Public Health. 2021;66:603810. doi:10.3389/ijph.2021.603810
10. Tao X, Li T, Gandomkar Z, Brennan PC, Reed WM. Incidence, mortality, survival, and disease burden of breast cancer in China compared to other developed countries. Asia Pac J Clin Oncol. 2023;19(6):645–654. doi:10.1111/ajco.13958
11. Huang S, Yang Q, Zheng X, Chow KM, Wu J, Zhu J. Predictors of surgery choices in women with early-stage breast cancer in China: a retrospective study. BMC Cancer. 2023;23(1):23. doi:10.1186/s12885-023-10510-4
12. Sun Q, Hu J, Ye Y, et al. The effect of smoking on breast cancer screening results in female population: a study in Wu wei, China. BMC Cancer. 2025;25(1):1225. doi:10.1186/s12885-025-14586-y
13. Shan M, Wang X, Sun G, et al. A retrospective study of the clinical differences of Uygur breast cancer patients compared to Han breast cancer patients in the Xinjiang region of China. Int J Clin Exp Med. 2014;7(10):3482–3490.
14. Abudukeremu M, Ayoufu A, Tuerhong A, Paizula X, Ou JH. Distribution of CYP2D6 and CYP2C19 gene polymorphisms in Han and Uygur populations with breast cancer in Xinjiang, China. Open Life Sci. 2024;19(1):20220728. doi:10.1515/biol-2022-0728
15. Wang CH, Li JZ, Zhang W. Breast cancer molecular subtypes of Uygur and Han in Xinjiang of China. Int J Clin Exp Med. 2014;7(4):1116–1121.
16. Zhu H, Geng C, Xia X, et al. Current practices and trends of breast-conserving surgery in China: a nationwide cross-sectional survey. Chin Med J. 2025:10–97. doi:10.1097/CM9.0000000000003929
17. Yu LX, Shi P, Tian XS, Yu ZG; Chinese Society of Breast Surgery. A multi-center investigation of breast-conserving surgery based on data from the Chinese Society of Breast Surgery (CSBrS-005). Chin Med J. 2020;133(22):2660–2664. doi:10.1097/CM9.0000000000001152
18. Bao X, Sun K, Tian X, et al. Present and changing trends in surgical modalities and neoadjuvant chemotherapy administration for female breast cancer in Beijing, China: a 10-year (2006–2015) retrospective hospitalization summary report-based study. Thorac Cancer. 2018;9(6):707–717. doi:10.1111/1759-7714.12636
19. Roy PG, Mustata L, Hu J, et al. Partial breast reconstruction with lateral chest wall perforator flap to facilitate breast conservation in breast cancer: first 100 cases with cancer outcomes at 8 years follow-up and the lessons learned. Cancer Manag Res. 2021;13:9453–9466. doi:10.2147/CMAR.S321192
20. Li J, Zhong G, Wang K, Kang W, Wei W. Tumor-to-gland volume ratio versus tumor-to-breast ratio as measured on CBBCT: possible predictors of breast-conserving surgery. Cancer Manag Res. 2021;13:4463–4471. doi:10.2147/CMAR.S312288
21. Xiu B, Zhang Q, Meng X, et al. Current practices and challenges of endoscopic-assisted breast surgery in China: a nationwide cross-sectional survey. Eur J Surg Oncol. 2025;51(5):109620. doi:10.1016/j.ejso.2025.109620
22. Chen R, Li S, Li Y, et al. Can axillary surgery be omitted in patients with breast pathologic complete response after neoadjuvant systemic therapy for breast cancer? A real-world retrospective study in. China J Cancer Res Clin Oncol. 2021;147(12):3495–3501. doi:10.1007/s00432-021-03763-8
23. Lee TH, Lee H, Jang JY, et al. Refined risk stratification in residual triple-negative breast cancer after neoadjuvant therapy using residual cancer burden class and lymphovascular invasion. Breast Cancer Res Treat. 2026;215(3):76. doi:10.1007/s10549-026-07906-8
24. O’Meara TA, Tarantino P. Different diseases, different escapes: trastuzumab deruxtecan resistance in HER2-amplified versus HER2-low breast cancer. Cancer Discov. 2026;16(2):195–197. doi:10.1158/2159-8290.CD-25-2102
25. Jiang Y, Du F, Zhang M, et al. Patterns and costs of breast reconstruction in Chinese plastic surgery department: a study from national quality control databases (2022–2023). Gland Surg. 2025;14(11):2131–2141. doi:10.21037/gs-2025-246
26. Yang B, Ren G, Song E, et al. Current status and factors influencing surgical options for breast cancer in china: a nationwide cross-sectional survey of 110 hospitals. Oncologist. 2020;25(10):e1473–re1480. doi:10.1634/theoncologist.2020-0001
27. Duan Q, Sun M, Kong D, Liu J, Liu B, Knowledge LK. Attitude, and practice toward breast reconstruction among breast surgery healthcare professionals in China. J Multidiscip Healthc. 2025;18:5701–5712. doi:10.2147/JMDH.S534905
28. Song P, Liu T, Zhang Y, et al. Traditional Chinese medicine in the treatment of breast Cancer. Mol Cancer. 2025;24(1):209. doi:10.1186/s12943-025-02416-5
29. Tian G, Xu J, Zhang T, et al. Rural residents’ willingness to participate in basic medical insurance and influential factors: a survey of three provinces in China. Front Public Health. 2022;10:1037763. doi:10.3389/fpubh.2022.1037763
30. Xie Y, Valdimarsdóttir UA, Wang C, et al. Public health insurance and cancer-specific mortality risk among patients with breast cancer: a prospective cohort study in China. Int J Cancer. 2021;148(1):28–37. doi:10.1002/ijc.33183
31. Galvis Rojas G, Strang P, Schultz T, Levin LÅ. Healthcare costs and resource use in advanced breast cancer at the end of life: a register study. Acta Oncol. 2026;65:75–82. doi:10.2340/1651-226X.2026.44970
32. Diaz R, Poggio F, Fozza A, Giannubilo I, Cuniolo L, Fregatti P. Editorial: the essential role of multidisciplinary teams in breast cancer surgery: collaboration for superior patient outcomes. Front Oncol. 2026;15:1754900. doi:10.3389/fonc.2025.1754900
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.