")
Back to Journals » Patient Preference and Adherence » Volume 17
Factors Associated with Self-Regulatory Fatigue in Chinese Older Patients with Coronary Heart Disease: A Cross-Sectional Survey
Received 10 December 2022
Accepted for publication 10 February 2023
Published 1 April 2023 Volume 2023:17 Pages 941—949
DOI https://doi.org/10.2147/PPA.S400996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Xiaofu Ji, Hongyu Yu
School of Nursing, Jinzhou Medical University, Jinzhou, Liaoning, People’s Republic of China
Correspondence: Hongyu Yu, School of Nursing, Jinzhou Medical University, Jinzhou, Liaoning, People’s Republic of China, Tel +86 15941628522, Email [email protected]
Purpose: To identify important determinants of self-regulatory fatigue in older adults with coronary heart disease based on demographics, health literacy, and health empowerment factors.
Patients and Methods: A total of 201 older patients with coronary heart disease (CHD) from First Affiliated Hospital of Jinzhou Medical University by cluster sampling method. Demographic Questionnaire, the Health Literacy Management Scale (HLSCP), the Patient Perception Empowerment Scale (PPES), and the Self-Regulatory Fatigue Scale (SRF-S) were used to collect the data.
Results: The coronary heart disease elderly scored 44.20± 6.98 points in self-regulatory fatigue. The results showed that residence, monthly household income, hospitalized times of CHD since illness, health literacy and health empowerment were significant determinants of self-regulatory fatigue (p< 0.001). Self-regulatory fatigue was negatively correlated with health literacy (r=− 0.639, P< 0.01) and health empowerment (r=− 0.580, P< 0.01).
Conclusion: Residence, monthly household income, hospitalized times of CHD since illness influence self-regulatory fatigue among coronary heart disease patients. Health literacy and health empowerment were independent predictors of self-regulatory among coronary heart disease patients.
Keywords: coronary heart disease, older adults, health literacy, health empowerment, self-regulatory fatigue
Introduction
Coronary heart disease (CHD) is one of the highest non-communicable chronic diseases in morbidity and mortality worldwide.1 Worldwide, approximately 17 million people die from cardiovascular disease each year, with coronary heart disease accounting for 67.1% of all cardiovascular deaths.2 Due to the accelerated aging of the Chinese population and changes in people’s lifestyles, such as frequent smoking, heavy alcohol consumption, unhealthy eating habits,3 the incidence and mortality of coronary heart disease have increased since the early 1970s, posing a severe threat to national health. The mortality rate of coronary heart disease in China exceeded 120/100,000 in 2018, and the prevalence of coronary heart disease among people over 60 years old was as high as 27.8%.4 Coronary heart disease is also the leading cause of death among the elderly in China.5
Self-regulatory fatigue refers to the physical and psychological stress of patients, enduring the discomfort of the disease and rapidly depleting the patient’s self-control resources.6 The long duration of the disease and susceptibility to recurrence are characteristics of coronary artery disease that predispose patients to physical and psychological challenges.7 In addition, health-promoting behaviors are the basis of clinical treatment and secondary preventive care for coronary heart disease and will directly influence treatment outcomes. Patients with coronary heart disease need to adhere to health promotion behaviors, including strict control of diet, exercise, lipid monitoring, and medication.8 These behaviors overuse self-control resources, which may lead to a significant reduction of their self-control resources in a short period of time, and even be depleted.9 This is the most critical factor that leads to the failure of self-control tasks.10 Facing such difficulties may decrease self-control and make patients experience self-regulatory fatigue.11
Some studies have shown that self-regulation fatigue can lead to decreased life quality and self-management in patients.12 Therefore, it is important to pay attention to the patient’s self-regulatory fatigue and take effective measures to improve it. The finite resource model13 argues that people’s psychological resources are limited but also temporary and can be replenished through some channels.
In previous studies, people had mainly used external interventions to reduce patients’ self-regulatory fatigue.14,15 Health literacy is the ability to make sound health decisions for themselves to maintain and promote their health.16 According to WHO, health literacy is a more accurate predictor of population health status than patients’ race, education level, socio-economic factors, etc.17 According to previous studies, low health literacy can lead to poor outcomes, such as a lack of understanding of disease and low adherence.18 Health empowerment refers to a positive partnership and patient self-care strategies developed to improve health outcomes and quality of life in chronic disease and is a prerequisite for wellness.19 Literature illustrated that health literacy and perceived empowerment play a dominant role in health behaviors.20 The purpose of this study, therefore, were to explore the impact of health literacy and perceived empowerment on the self-regulatory fatigue of older patients with coronary heart disease. We hypothesized that 1) Demographic and illness characteristics were important determinants of self-regulatory fatigue among older patients with CHD. 2) highly health literacy and perceived empowerment would predict lower self-regulatory fatigue, after controlling for the effects of background variables.
Methods and Materials
Design and Participants
A cross-sectional study was conducted. A total of 211 patients with CHD were sampled by cluster sampling method at the First Hospital of Jinzhou Medical University (Liaoning Province, China) from September 2021 to January 2022. The patient inclusion criteria were as follows: (a) confirmed diagnosis of coronary heart disease; (b) aged 60 years or older; (c) had some language skills; (d) voluntarily participated in this study. The exclusion criteria were as follows: (a) unstable vital signs in the acute phase or with symptoms such as severe liver and kidney insufficiency; (b) unconscious and serious psychological disorders. But 10 dropped out in the questionnaire survey. Finally, 201 eligible participants were included in the analysis.
Measurements
Demographic Characteristics
A self-designed questionnaire that consisted of age, sex, education, marital status, family residence, medical payment methods and monthly household income was used to collect demographic characteristics of patients. Family history of CHD, the number of combined chronic diseases, duration of CHD and hospitalized times for CHD since illness captured disease-related conditions of patients.
Self-Regulatory Fatigue Scale(SRF-S)
The Self-Regulatory Fatigue Scale (SRF-S) was developed by Nes et al21, in Australia. It has frequently been used as a measurement of individual self-regulatory fatigue status. In the Chinese version developed by Wang et al22, the overall Cronbach alpha coefficient for this study scale was 0.772. The SRF-S contains 3 dimensions, cognitive (6 items), emotional (5 items), and behavioral (5 items), with a total of 16 items. A 5-point Likert scale was used with range of scores from 1–5, representing strongly disagree (1) to strongly agree (5), respectively, with higher scores indicating more severe self-loss.
Health Literacy Management Scale (HLSCP)
The Health Literacy Management Scale (HLSCP) was developed by Professor Jordan23 of the University of Melbourne, Australia, in 2010. It Described the level of individual health-related knowledge and skills. This study used the Chinese version of HLSCP translated by Sun et al24, Cronbach’s alpha was 0.980 in this study. The scale had 24 items and contains four dimensions: Information acquisition ability (9 items), Communicative interaction ability (9 items), Health improvement willingness (4 items), and Economic support willingness (2 items). The scale used a 5- point Likert scale, with scores ranging from 0–5. A score of 96 or above is considered greater health literacy, while a score of 95 and below represented less health letter literacy.
Patient Perception Empowerment Scale (PPES)
The Patient Perception Empowerment Scale (PPES) was developed by Lewin et al.25 To measure patients with coronary heart disease about their health empowerment and decision-making. Ye et al26 translated it into Chinese. The Cronbach’s alpha for this study was 0.935. It included of 4 dimensions, namely, information (3 items), decision (3 items), individual (2 items) and self-management (3 items). Each item was rated on a 5-point scale from 1 (“strongly disagree”) to 5 (“strongly agree”), with the total range of scores from 0–30. Higher scores indicated the better perception of empowerment.
Data Collection
The questionnaire consisted of demographic characteristics, HLSCP, PPES, and SRF-S. We explained the purpose and method of this study to the nursing directors of the hospital and asked for their cooperation in data collection. After obtaining permission, Three graduate nursing students receiving instruction of coronary heart disease and unified training served as research assistants and visited the clinical departments to distribute and collect the questionnaires. Each participant was fully informed of the aim of the survey. Since the survey subjects were all elderly, the questionnaire was filled out by the investigator after asking the patients about the contents. Secondary check when exporting data.
Statistical Analysis
All statistical analyses were performed using IBM SPSS 26.0 (IBM Corp, Armonk, NY, USA). Categorical variables were expressed as frequency (percentages), whereas continuous data were expressed as mean ±SD. The t-test and the ANOVA test were applied to compare statistical differences in self-regulatory fatigue scores between groups. Pearson correlation analysis was used to examine the relationship between health literacy, health empowerment, self-regulatory fatigue, cognitive, emotional and behavioral. Factors with P<0.05 in univariate analysis were input into the hierarchical multiple regression analysis was conducted to find independent factors associated with self-regulating fatigue. The variance inflation factor (VIF) for each covariate was below 5, a result considered acceptable. In this study, differences were indicated as statistically significant when P<0.05.
Results
Demographic Characteristics
Most of those eligible participants were from city areas (58.2%), married (74.1%) and had an educational background of Junior High School (47.8%). Regarding the monthly household income, 52.7% of them had a monthly salary of 1000–3000 yuan ($141.90 - $425.70). In addition, most of this population had no family history of CHD (73.6%) and duration of disease less than 1 year (43.8%). The results of the t-test and the ANOVA test showed significant differences in self-regulatory fatigue among CHD patients in terms of age, education, marital status, residence,monthly household income, the number of combined chronic diseases, and hospitalized times of CHD since illness. Overall characteristics of the sample can be found in Table 1.
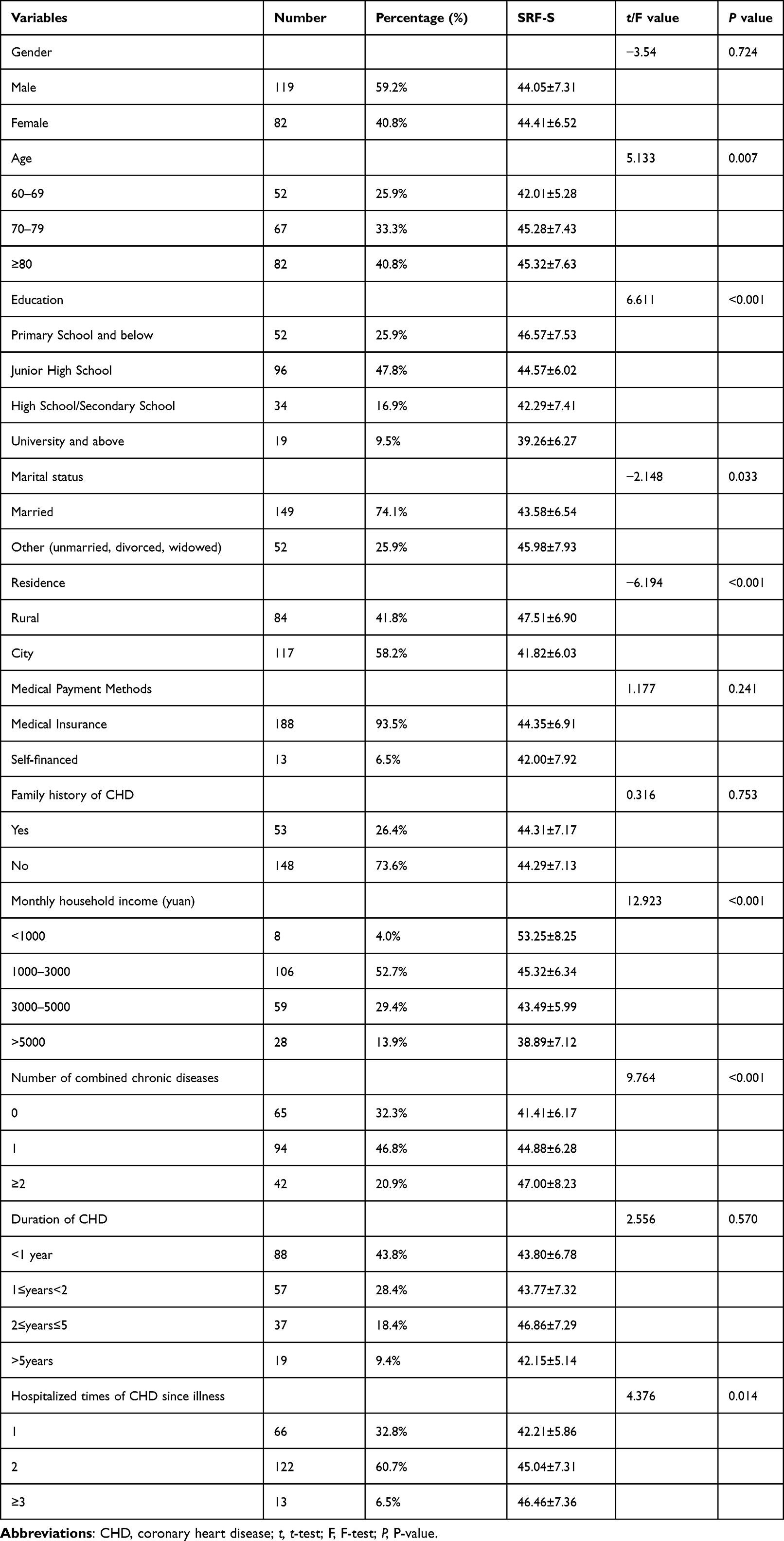 |
Table 1 Distribution of Demographic and Illness Characteristics and the Associations with Self-Regulatory Fatigue (n=201) |
Score of HLSCP, PPES and SRF-S of the CHD Patient
The mean (SD) scores for SRF-S were (44.20±6.98), with (15.31±3.10), (14.67±2.91) and (14.21±2.57) in cognitive, emotional, and behavioral, respectively. Besides, 89.6% had better health literacy and 10.4% lacked health literacy. The mean (SD) scores for HLSCP were (69.74±19.95).AS shown in Table 2.
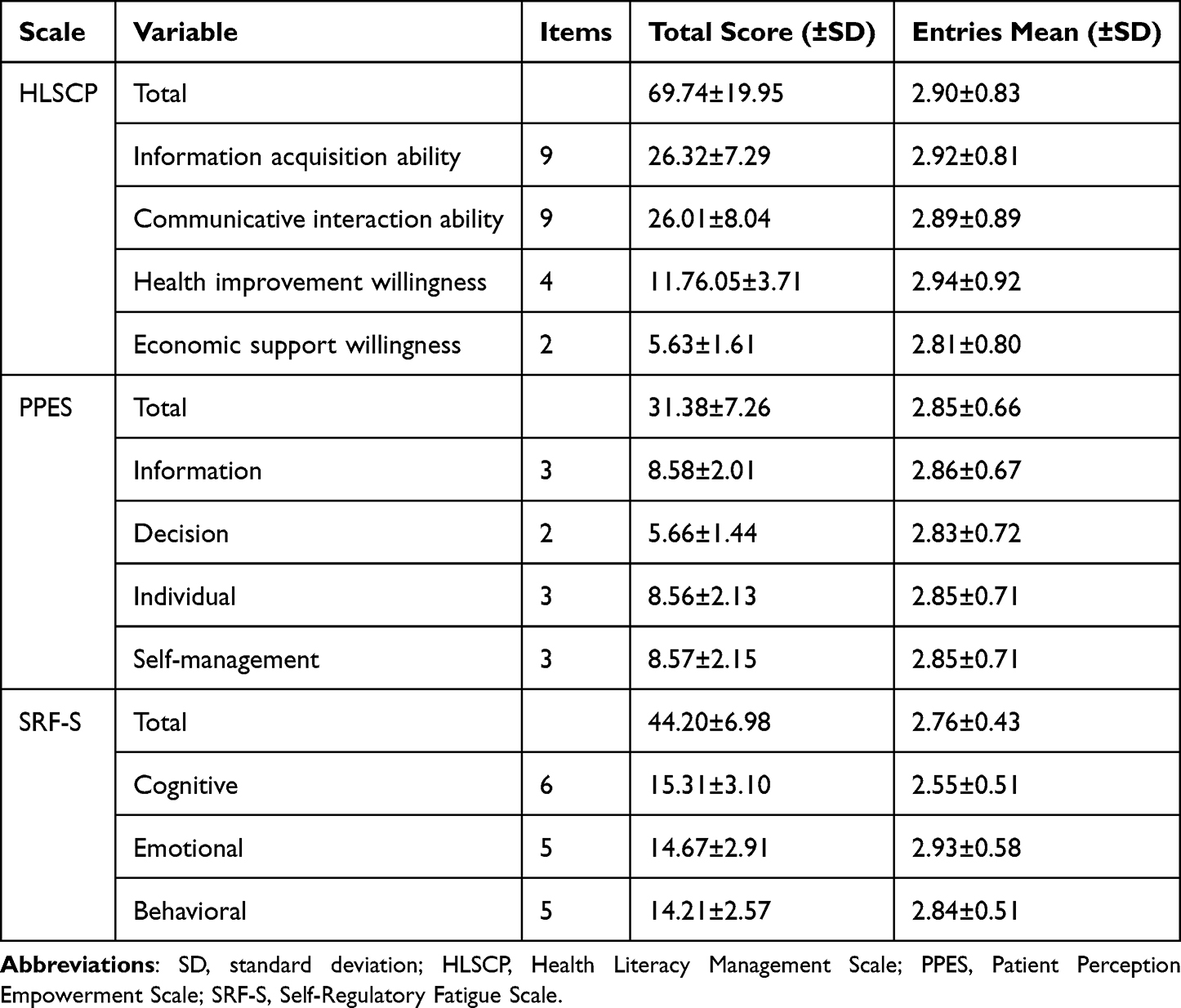 |
Table 2 Score of HLSCP, PPES, and SRF-S Among the CHD Patients (n=201) |
Association Between Health Literacy, Health Empowerment and Self-Regulatory Fatigue.
As presented in Table 3, Self-regulating fatigue was negatively correlated with health literacy (r=−0.639, P<0.01) and health empowerment (r=−0.580, P<0.01). Moreover, there was a positive association between health literacy and empowerment (r=0.600, P<0.01).
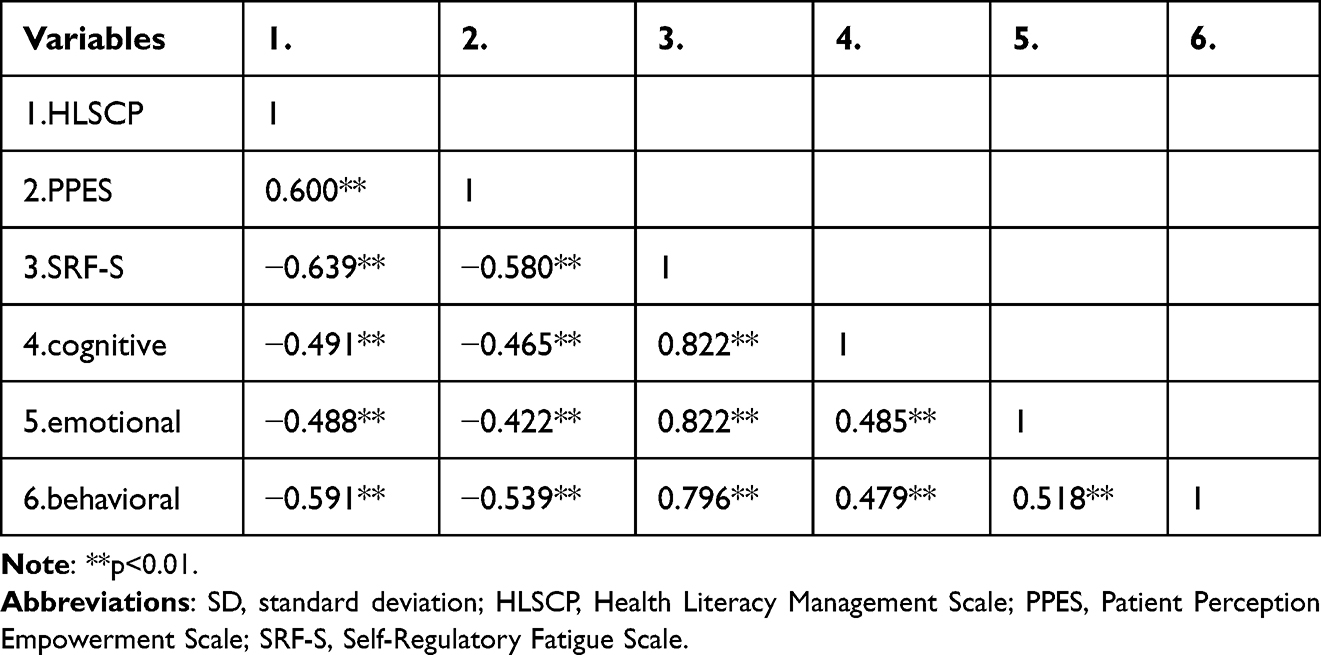 |
Table 3 Correlation Among Health Literacy, Health Empowerment, and Self-Regulatory Fatigue (n=201) |
Effect Of Demographic Statistical Data On SRF-S.
The SRF-S evaluation score of CHD patients was used as the dependent variable, and the first layer using factors with statistical significance in the ANOVA test was used as the independent variable. The second layer put HLSCP and PPES scores as independent variables for linear regression analysis. The regression equation demonstrates that the residence, monthly household income, hospitalized times of CHD since illness, health literacy, and empowerment were significant for self-regulatory fatigue (in Table 4).
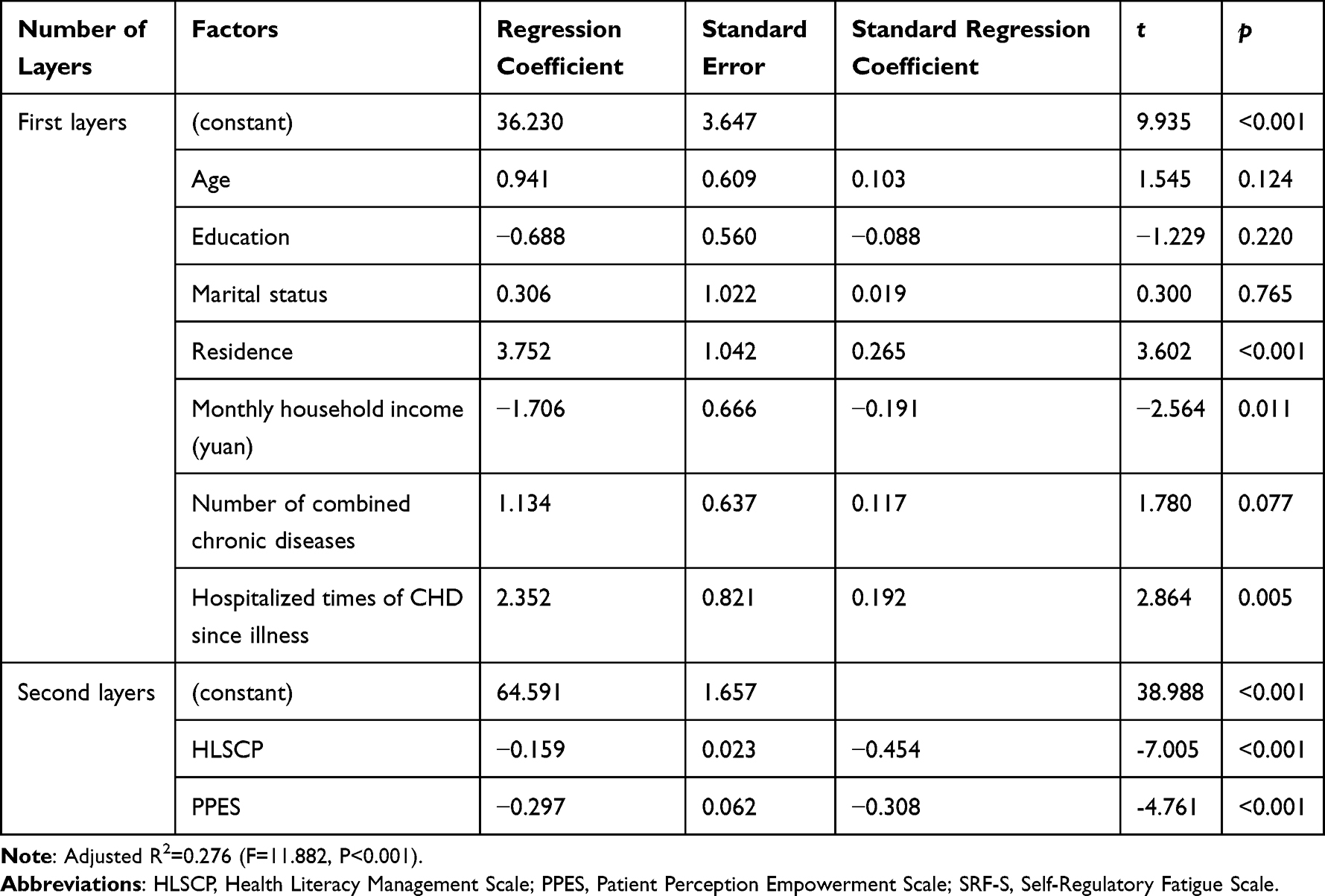 |
Table 4 Multiple Linear Regression for Self-Regulatory Fatigue (n=201) |
Discussion
This study found that health literacy and health empowerment were important determinants of self-regulatory fatigue in older patients with CHD. The results of this study may help healthcare professionals to provide specific interventions for CHD patients.
This study showed that older patients with CHD had high self-regulatory fatigue scores. Higher than previous scores in peritoneal dialysis patients.27 The findings suggest that patients with coronary heart disease have more severe self-loss in their self-management process. Coronary heart disease is characterized by the difficulty of complete recovery and requires long recovery times, with patients taking long-term medications and changing their lifestyle choices. This requires strong self-control, which also depletes patient resources. Individuals have limited self-regulatory resources and will experience attrition.28 Meanwhile, emotional control had the most significant influence on patients’ self-regulatory fatigue. This finding was consistent with a previous study focused on cancer survivors.29 Patients with coronary artery disease primarily type A and D personalities,30 characterized by quick temper and irritability, quickly triggering adverse emotional problems. Therefore, health care professionals and caregivers of coronary heart disease should focus on the patients’ self-regulatory fatigue.
The results showed that residence, monthly household income, and hospitalized times of CHD since illness for CHD were the influencing factors for self-regulatory fatigue in older adult patients with CHD. Patients living in city areas have lower self-regulatory fatigue than those living in rural areas. The reasons might be that the city has more medical resources, and patients can get timely solutions to their health problems. The lower monthly family income, the heavier patient’s self-regulatory fatigue. CHD is a chronic disease, and long-term medication will increase the patient’s family economic burden and psychological burden, and the economic basis is the self-health management motivation. Therefore, health care professionals can enhance patients’ confidence in self-management of the disease, reduce patients’ negative emotions and decrease patients’ self-regulation fatigue through relaxation training and psychological guidance. The more hospitalized times of CHD since illness, the higher the level of self-regulatory fatigue. It was consistent with the finding of Li et al.31 Studies10 showed that high levels of self-control sustained over long periods can deplete self-control. Patients admitted to the hospital multiple times for coronary artery disease have undergone long periods of self-control and have a higher depletion of self-control resources, so their self-regulatory fatigue is higher.
The present study showed that health empowerment was negatively associated with self-regulatory fatigue in elderly patients with coronary artery disease, which was consistent with the findings of Zhang et al.32 The possible reason for this is that health empowerment emphasizes patient-centeredness and helps individuals to discover and develop their inner potential and increase their control over the disease, ensuring persistence in treatment.33 Studies34 demonstrated that patients autonomously involved in self-health management experience less impact on self-depletion than those supervised to perform. Thus, it was not difficult to find that empowering patients to increase their autonomy in self-management can reduce the degree of patient self-loss. Therefore, health care providers should help patients to explore their potential to reduce their attrition. In addition, the health literacy of elderly patients with coronary artery disease was negatively associated with self-regulatory fatigue, ie, the higher the patient’s health literacy level, the lower the self-regulatory fatigue. Patients with a higher level of health literacy can obtain, understand, and use health information more accurately, make correct health decisions, promote physical health, and reduce self-regulatory fatigue.
This suggests that health care professionals should use easy-to-understand language to teach patients about the disease and enhance the health literacy of patients with coronary heart disease by improving widespread health knowledge and strengthening communication with patients. Because older people may be less social, patients’ families and patients should strengthen communication among themselves weekly. Health care workers should provide timely help and support, pay attention to patients’ psychological changes, strengthen patients’ internal drive to fight against the disease, enhance the ability to perceive empowerment, and ultimately reduce patients’ self-regulation fatigue.
Limitation
This study was cross-sectional, lacking dynamic observation of variables, and should be supplemented by future longitudinal studies. The study was conducted only in a tertiary care hospital in Jinzhou city, and the representativeness of the sample size needs to be further improved. A multicenter, large-sample survey study can be conducted in the future.
Conclusion
Our study identifies several factors associated with self-regulatory fatigue in Chinese older patients and elucidated the relationship among them. It provided a basis for future targeted intervention strategies. Medical practitioners should focus on the assessment of self-regulatory fatigue in patients with coronary artery disease and strengthen the psychological construction of patients with coronary artery disease to reduce the level of self-regulatory fatigue.
Ethical Considerations and Consent Statement
This study conformed to the standards of the Declaration of Helsinki. Ethical approval was granted by the Ethics Committee of Jinzhou Medical University (No. JZMULL2022028). Patients signed informed consent in this study.
Funding
This work was supported by the “Liaoning Provincial Social Science Planning Fund Project” No. L22BZZ003.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Naghavi M, Abajobir AA, Abbafati C; GBD 2016 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: a systematic analysis for the global burden of disease study 2016. Lancet. 2017;390(10100):1151–1210. doi:10.1016/S0140-6736(17)32152-9
2. Amrein ML, Lopez-Ayala P, Walter J, Widmer V, Mueller C. Coronary heart disease and TMAO concentrations. J Am Coll Cardiol. 2020;75(24):3102. doi:10.1016/j.jacc.2020.03.079
3. Lv J, Yu C, Guo Y, et al. Adherence to healthy lifestyle and cardiovascular diseases in the Chinese population. J Am Coll Cardiol. 2017;69(9):1116–1125. doi:10.1016/j.jacc.2016.11.076
4. Yearbook. Editorial Committee of the China Health and Health Statistics Yearbook Editorial Committee of the China Health and Health Statistics Yearbook. Zhang Xegao General Editor, China Health and Health Statistics Yearbook. China Union Medical University Press; 2019:4. doi:10.41656/y.cnki.ysife.2020.000001
5. Zhou M, Wang H, Zhu J, et al. Cause-specific mortality for 240 causes in China during 1990–2013: a systematic subnational analysis for the global burden of disease study 2013. Lancet. 2016;387(10015):251–272. doi:10.1016/S0140-6736(15)00551-6
6. Li X, Gao Q, Sun L, Gao W. Effect of self-control on health promotion behavior in patients with coronary heart disease: mediating effect of ego-depletion. Psychol Health Med. 2022;27(6):1268–1276. doi:10.1080/13548506.2020.1867316
7. Nes LS, Ehlers SL, Whipple MO, Vincent A. Self-regulatory fatigue: a missing link in understanding fibromyalgia and other chronic multisymptom illnesses. Pain Pract. 2017;17(4):460–469. doi:10.1111/papr.12480
8. Detweiler-Bedell JB, Friedman MA, Leventhal H, Miller IW, Leventhal EA. Integrating co-morbid depression and chronic physical disease management: identifying and resolving failures in self-regulation. Clin Psychol Rev. 2008;28(8):1426–1446. doi:10.1016/j.cpr.2008.09.002
9. Hagger MS, Wood C, Stiff C, Chatzisarantis NL. Ego depletion and the strength model of self-control: a meta-analysis. Psychol Bull. 2010;136(4):495–525. doi:10.1037/a0019486
10. Shmueli D, Prochaska JJ. Resisting tempting foods and smoking behavior: implications from a self-control theory perspective. Health Psychol. 2009;28(3):300–306. doi:10.1037/a0013826
11. Aaron LA, Burke MM, Buchwald D. Overlapping conditions among patients with chronic fatigue syndrome, fibromyalgia, and temporomandibular disorder. Arch Intern Med. 2000;160(2):221–227. doi:10.1001/archinte.160.2.221
12. Solberg Nes L, Ehlers SL, Patten CA, Gastineau DA. Self-regulatory fatigue, quality of life, health behaviors, and coping in patients with hematologic malignancies. Ann Behav Med. 2014;48(3):411–423. doi:10.1007/s12160-014-9621-z
13. Inzlicht M, Schmeichel BJ, Macrae CN. Why self-control seems (but may not be) limited. Trends Cogn Sci. 2014;18(3):127–133. doi:10.1016/j.tics.2013.12.009
14. Tangney JP, Baumeister RF, Boone AL. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J Pers. 2004;72(2):271–324. doi:10.1111/j.0022-3506.2004.00263.x
15. Smith TW, Cribbet MR, Nealey-Moore JB, et al. Matters of the variable heart: respiratory sinus arrhythmia response to marital interaction and associations with marital quality. J Pers Soc Psychol. 2011;100(1):103–119. doi:10.1037/a0021136
16. Smith BJ, Tang KC, Nutbeam D. WHO health promotion glossary: new terms. Health Promot Int. 2006;21(4):340–345. doi:10.1093/heapro/dal033
17. Dewalt DA, Berkman ND, Sheridan S, Lohr KN, Pignone MP. Literacy and health outcomes: a systematic review of the literature. J Gen Intern Med. 2004;19(12):1228–1239. doi:10.1111/j.1525-1497.2004.40153.x
18. Andrus MR, Roth MT. Health literacy: a review. Pharmacotherapy. 2002;22(3):282–302. doi:10.1592/phco.22.5.282.33191
19. Neuhauser D. The coming third health care revolution: personal empowerment. Qual Manag Health Care. 2003;12(3):171–186. doi:10.1097/00019514-200307000-00007
20. Lee YJ, Shin SJ, Wang RH, Lin KD, Lee YL, Wang YH. Pathways of empowerment perceptions, health literacy, self-efficacy, and self-care behaviors to glycemic control in patients with type 2 diabetes mellitus. Patient Educ Couns. 2016;99(2):287–294. doi:10.1016/j.pec.2015.08.021
21. Nes LS, Ehlers SL, Whipple MO, Vincent A. Self-regulatory fatigue in chronic multisymptom illnesses: scale development, fatigue, and self-control. J Pain Res. 2013;6:181–188. doi:10.2147/JPR.S40014
22. Ligang W, Jinyi Z, Jia W, et al. Validity and reliability of the Chinese version of the self-regulation fatigue scale to assess young people. Chin Ment Health J. 2015;29(4):290–294.
23. Jordan JE, Buchbinder R, Osborne RH. Conceptualising health literacy from the patient perspective. Patient Educ Couns. 2010;79(1):36–42. doi:10.1016/j.pec.2009.10.001
24. Hao-Lin S. A Study on Health Literacy Scale for Patients with Chronic Diseases and Its Preliminary Application. Fudan University; 2012.
25. Lewin D, Piper S. Patient empowerment within a coronary care unit: insights for health professionals drawn from a patient satisfaction survey. Intensive Crit Care Nurs. 2007;23(2):81–90. doi:10.1016/j.iccn.2006.09.003
26. Yeh MY, Lin SH, Tung TH. Psychometric evaluation of the Chinese version of the patient perceptions of empowerment scale (PPES). Biomed Res Int. 2014;2014:867451. doi:10.1155/2014/867451
27. Gao Y, Shan Y, Jiang T, et al. Dietary adherence, self-regulatory fatigue and trait self-control among chinese patients with peritoneal dialysis: a cross-sectional study. Patient Prefer Adherence. 2021;15:443–451. doi:10.2147/PPA.S298231
28. Baumeister RF, Bratslavsky E, Muraven M, Tice DM. Ego depletion: is the active self a limited resource? J Pers Soc Psychol. 1998;74(5):1252–1265. doi:10.1037//0022-3514.74.5.1252
29. Johns SA, Brown LF, Beck-Coon K, Monahan PO, Tong Y, Kroenke K. Randomized controlled pilot study of mindfulness-based stress reduction for persistently fatigued cancer survivors. Psychooncology. 2015;24(8):885–893. doi:10.1002/pon.3648
30. Pogosova N, Kotseva K, De Bacquer D, et al. Psychosocial risk factors in relation to other cardiovascular risk factors in coronary heart disease: results from the EUROASPIRE IV survey. A registry from the European society of cardiology. Eur J Prev Cardiol. 2017;24(13):1371–1380. doi:10.1177/2047487317711334
31. Jiayi L. A study on the correlation between self-regulation fatigue, self-efficacy and self-management behavior in patients with type 2 diabetes. Master’s thesis, Shandong University; 2021. Available from: http://59.44.216.2:8082/rwt/CNKI/https/NNYHGLUDN3WXTLUPMW4A/KCMS/detail/detail.aspx?dbname=CMFD202102&filename=1021044654.nh.
32. Mengqian Z, Xiaomin LI, Mingming L, et al. Current status of self-loss and its influencing factors in patients with coronary artery disease after percutaneous coronary intervention (PCI). Chin J Health Psychol. 2020;28(06):856–861.
33. Garcimartín P, Comín-Colet J, Pardo-Cladellas Y, et al. Validation of the Spanish version of the questionnaire on Patient Empowerment in Long-Term Conditions. PLoS One. 2020;15(6):e0233338. doi:10.1371/journal.pone.0233338
34. Li J, Ye H, Tang Y, Zhou Z, Hu X. What are the effects of self-regulation phases and strategies for Chinese students? A meta-analysis of two decades research of the association between self-regulation and academic performance. Front Psychol. 2018;9:2434. doi:10.3389/fpsyg.2018.02434
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.