")
Back to Journals » Patient Preference and Adherence » Volume 17
Factors Associated with Prevention of Metabolic Syndrome Among Middle-Aged Postmenopausal Korean Women: A Study Based on the Information, Motivation, Behavioral Skills (IMB) Model
Received 4 July 2023
Accepted for publication 8 September 2023
Published 14 September 2023 Volume 2023:17 Pages 2279—2288
DOI https://doi.org/10.2147/PPA.S426248
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Yoonjung Kim, Sooyeon Park
College of Nursing, Konyang University, Daejeon, Republic of Korea
Correspondence: Sooyeon Park, College of Nursing, Konyang University, 158 Gwanjeodong-ro, Seo-gu, Daejeon, 35365, Republic of Korea, Tel +82 42 600 8584, Fax +82 42 600 2850, Email [email protected]
Purpose: Metabolic syndrome (MetS) is a significant risk factor for cardiovascular disease. Middle-aged women, in particular, have been reported to have significantly increased cardiovascular disease rates after menopause; however, their adherence to health behaviors is lower than that of other populations. This study examined the factors associated with health behaviors for MetS prevention based on the Information–Motivation–Behavior skills model and described the relationships between the components of the model in middle-aged women.
Patients and Methods: This investigative study used an online self-report questionnaire survey that included 241 middle-aged postmenopausal women aged 45– 64 years. The collected data were analyzed using descriptive statistics with SPSS 28.0, independent t-tests, one-way ANOVA, and Pearson’s correlation coefficient. Multiple regression analysis was used to examine the relationships among the variables.
Results: After controlling for age, time since menopause, and comorbidities, knowledge of MetS, social support, self-efficacy, and attitudes explained 42% of the variance in health behaviors for MetS prevention (F=18.38, p< 0.001). Among these variables, self-efficacy (β=0.33, p< 0.001), attitudes toward health behaviors (β=0.26, p< 0.001), and knowledge of MetS (β=0.13, p=0.005) had a significant impact on health behaviors for MetS prevention.
Conclusion: Significant associations were found between knowledge, self-efficacy, and attitudes toward health behaviors for MetS prevention among middle-aged women. The results of this study suggest that it is essential for healthcare provider to consider the components of the Information–Motivation–Behavior skills model when developing interventions aimed at improving health behaviors for MetS prevention among middle-aged postmenopausal women.
Keywords: women, menopause, metabolic syndrome, health behavior, lifestyle behavior
Introduction
Cardiovascular disease is the main cause of death worldwide,1 with metabolic syndrome (MetS) forming a major risk factor for cardiovascular disease.2–5 MetS is a growing epidemic that affects approximately 20% of adults in Western countries,6 and its prevalence among adults in the United States increased by more than 35% between 1998–1994 and 2007–2012.7 Roughly 1 in 4 adults in Korea report MetS, and according to the Korea National Health and Nutrition Examination Survey, 27.7% of Korean adults aged ≥ 30 years had MetS between 2016 and 2018, with its prevalence in Korea steadily increasing since 2015.8
MetS, which includes abdominal obesity, elevated blood pressure, low high-density lipoprotein cholesterol, elevated triglycerides, and elevated fasting blood sugar levels, refers to a set of interconnected risk factors for cardiovascular disease morbidity and mortality.9,10 Previous studies have reported age and sex differences in metabolic syndrome,11,12 with women exhibiting a higher prevalence of MetS and an increased risk of cardiovascular disease than men, with increasing age.13 Particularly, middle-aged women experience a significant increase in cardiovascular disease as they enter menopause,14,15 and menopause itself is a risk factor for cardiovascular disease.16
The Third US Cholesterol Management Guidelines recommended therapeutic lifestyle modifications based on physical activity, diet, and education as the primary intervention for managing MetS.17 Lifestyle factors influence the components of MetS and lifestyle interventions can slow or prevent the development of MetS.18,19 However, few efforts to adopt health behaviors for MetS prevention have been reported.20,21 Particularly, adherence to health behaviors has been reported to be lower in middle-aged women than in other populations.22
The factors that influence the target behaviors of middle-aged women should be considered to prevent and manage the incidence of MetS among them. A systematic review of lifestyle modifications for MetS reported that patient motivation to improve lifestyle adherence is a key factor in reducing MetS components23 and that the influencing factors such as knowledge, skills, and social cues and norms, and motivation should be considered.24 The Information-Motivation-Behavioral skills (IMB) model has gained attention because it accounts for the limitations of existing health behavior theories by suggesting the importance of factors such as information, motivation, and behavioral skills that individuals need to successfully perform complex health behaviors.25,26 The concept of the IMB model has been applied to a variety of studies aimed at positive behavior change.27,28 A systematic review of intervention studies based on the IMB model reported that it has been widely applied to desirable behavior change interventions for health promotion, such as smoking cessation, physical activity, and cancer self-examination.29 Furthermore, Information, motivation, and behavioral skills related to MetS management and complication prevention directly influence health behaviors, and that behavioral skills mediate the effects of information and motivation on health behaviors in various populations.30,31
However, studies identifying the factors that influence health behaviors for preventing MetS in middle-aged women are lacking. Existing research on middle-aged women and health behaviors for MetS prevention has focused on demographic characteristics,32 or single health behaviors, such as physical activity33 and, depression,34 leaving a gap in understanding the motivations and behavioral skills for integrated health behaviors for MetS prevention. There is a need for theory-based empirical studies that comprehensively assess the complex health behaviors associated with metabolic syndrome, to prevent and manage MetS among middle-aged postmenopausal women.
To provide scientific evidence for promoting health behaviors to prevent MetS, this study examined the factors associated with health behaviors for MetS prevention based on the Information–Motivation–Behavior skills model and described the relationships between the components of the model in middle-aged postmenopausal women.
Materials and Methods
Study Design
This cross-sectional study used a descriptive correlational approach to identify the associations between the components (knowledge about metabolic syndrome, social support, self-efficacy, and attitudes) of the IMB model and health behaviors for MetS prevention among postmenopausal women.
Participants
The participants of this study were middle-aged women who had experienced menopause, and the specific inclusion criteria were as follows: 1) women aged 50–64 years, 2) who had experienced their last menstrual period one year ago, 3) had not induced menopause, 4) were able to communicate in Korean, 5) comprehended the objectives of study, and 6) agreed to participate in the research were included in this study. Participants who had been diagnosed with MetS or mental illness, including cognitive issues, were excluded from the study.
The sample size for multiple regression analysis was determined using the G*Power 3.1.9.7 program. Existing research35 was used as reference for the power calculation, with an effect size of 0.15, power of 0.95, and a significance level of 0.05. The minimum required sample size was 189 participants; considering a dropout rate of 30% for online surveys, a total of 245 middle-aged women were recruited for the study. Excluding the four who withdrew participation midway, a total of 241 middle-aged women are the final participants.
Data Collection
The survey was conducted online, and data were collected in December 2022. Recruitment advertisements, which included a website link, were posted on a social network. Participants could check the online documents for the study details, including the objectives, significance, and content. If they wished to participate, they provided informed consent by clicking the consent button, and were able to access the questionnaire. In other words, the study participants expressed their willingness to participate voluntarily before the survey began. Participation was optional, and withdrawal was permitted. And before starting the survey, we set up questions to check if the participants met the inclusion and exclusion criteria, going through a procedure to ensure they were suitable candidates for the study. The survey that followed was conducted online, and it took approximately 10 minutes.
Measurement
The survey comprised questions on demographics, knowledge of MetS, social support, self-efficacy, attitudes toward health behaviors, and health behaviors for MetS prevention. We considered knowledge of MetS and social support as motivators, and self-efficacy and attitudes toward health behaviors as skills. The demographic questions included age, education, marital status, occupation, and household income. Questions related to menopausal status, smoking status, and alcohol consumption were also included.
Knowledge of MetS
Knowledge of MetS was measured using an instrument developed by Oh et al.36 The instrument consists of 20 items, including diagnostic criteria, causes, management methods, and complications related to MetS, with responses provided as “yes”, “no”, or “don’t know”. A higher percentage of correct responses indicated a higher level of knowledge about MetS. The original study did not calculate the Cronbach’s ⍺, which was 0.76 in this study.
Social Support
Social support was assessed using the Multidimensional Scale of Perceived Social Support developed by Zimet, Dahlem.37 The instrument consists of 12 items that assesses perceived support from family, friends, and significant others, rated on a 5-point scale. Higher scores indicate greater perceived support for healthy behaviors from the family. Cronbach’s ⍺ was 0.92 at the time of development, and 0.96 in this study.
Self-Efficacy
Self-efficacy was measured using a 13-item instrument developed by Sherer, Maddux38 to measure general self-efficacy, which was supplemented by Jung39 and consisted of a responses provided on a scale ranging from 10 to 100-point. Higher scores indicate greater self-efficacy. Cronbach’s ⍺ was 0.92 in the original study, and 0.97 in this study.
Attitude Toward Health Behaviors
Attitudes toward physical activity were measured using an instrument developed by Boudreau and Godin40 and adapted by Jang and Song.41 The instrument consists of eight items rated on a 7-point Likert scale. Higher scores indicate a more positive attitude toward health behaviors. The original study reported a Cronbach’s ⍺ of 0.91,40 while Jang and Song41 reported a Cronbach’s ⍺ of 0.86. In this study, Cronbach’s ⍺ was 0.93.
Health Behaviors for MetS Prevention
Health behaviors were measured using the Lifestyle Habits Assessment instrument targeted at individuals with a high risk of metabolic syndrome, developed by Kang.42 This instrument comprises 36 items divided into six subscales, namely physical activity and weight control, dietary habits, alcohol and smoking habits, stress, sleep and rest, and medication and health screening, rated on a 4-point scale. Higher scores indicate healthier lifestyle habits. Cronbach’s ⍺ was 0.92 in the original study42 and 0.91 in the present study.
Data Analysis
Statistical analyses were conducted using SPSS 28, and the significance level was set at p < 0.05. Descriptive statistics summarized the participants’ demographic characteristics and knowledge of MetS, social support, attitudes, self-efficacy, and health behaviors. Subsequently, we analyzed the differences in demographic characteristics based on the variables using an independent t-test, one-way ANOVA, Scheffe’s test for post hoc analysis, and, and Pearson’s correlation coefficient. Finally, multiple linear regression was used to determine the associations between demographic characteristics and health behaviors among middle-aged postmenopausal women.
Results
Demographic Characteristics
As shown in Table 1, the average age of the participants was 55.9 years (SD=3.6). The majority of participants (81.7%) were aged between 50 and 59 years. The self-perceived health status of the participants was generally good or moderate, with 40.7% reporting good health and 41.5% reporting moderate health. Approximately one-third of the participants (36.9%) reported comorbidities. Additionally, 41.5% of the participants did not drink alcohol, while 98.8% were non-smokers.
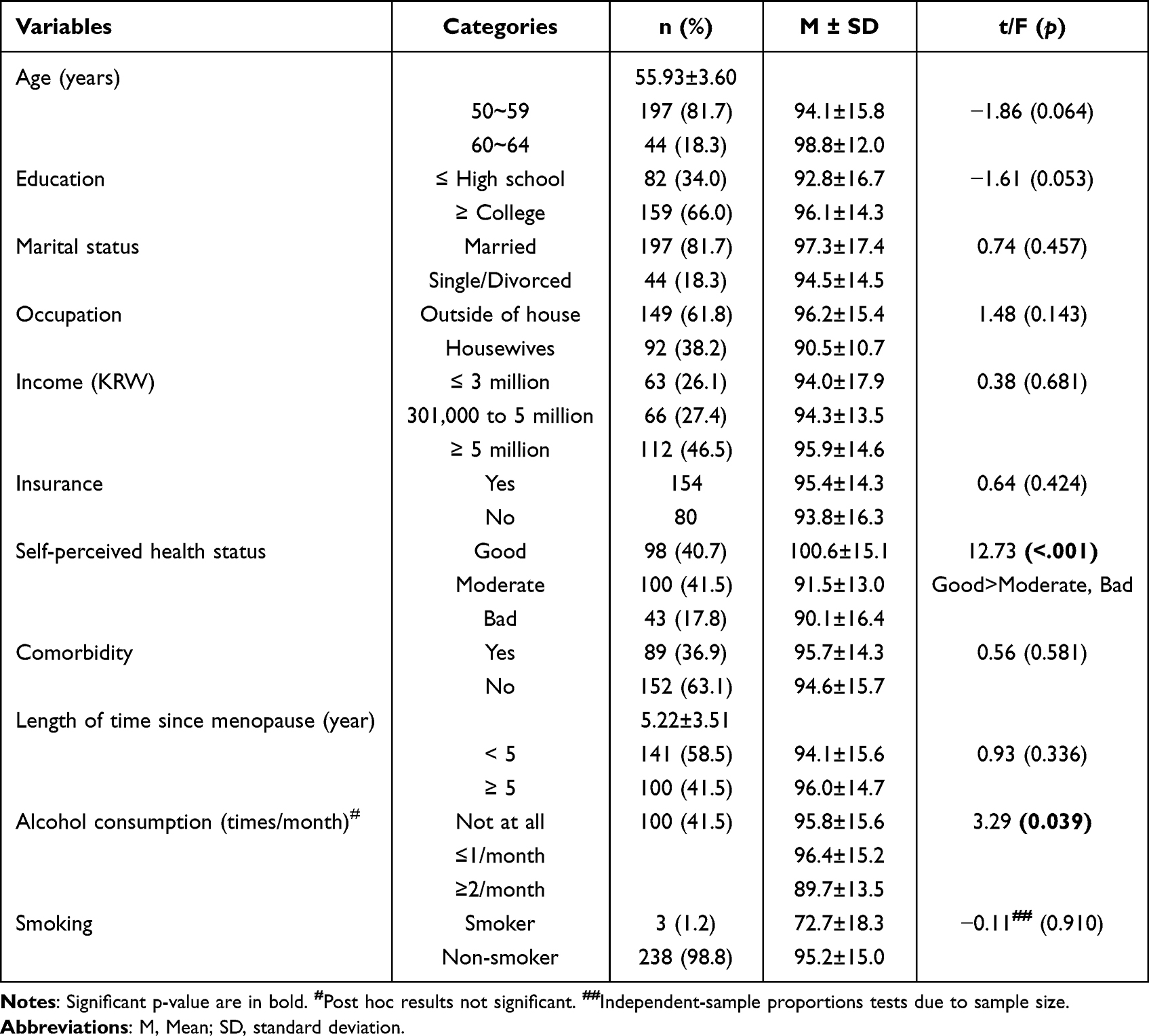 |
Table 1 Differences in Demographic Characteristics Based on Health Behaviors for Metabolic Syndrome Prevention (N = 241) |
Average Scores for the Variables
The average score for participants’ knowledge of metabolic syndrome was 12.24 (SD=2.29) points. The scores for social support, self-efficacy, and attitude toward health behavior were 46.80 (SD=9.99) points, 932.02 (SD=203.41) points, and 9.14 (SD=9.72) points, respectively. The score for health behaviors for metabolic syndrome prevention was 94.96 (SD=15.22) points (Table 2).
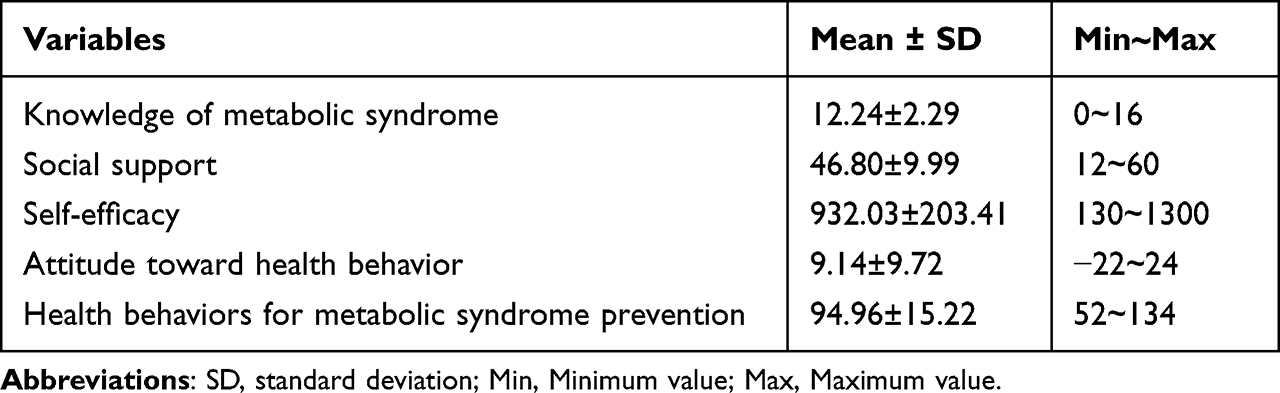 |
Table 2 The Average Scores of Knowledge, Social Support, Self-Efficacy, Attitude, and Health Behaviors for Metabolic Syndrome Prevention (N = 241) |
Health Behaviors for MetS Prevention According to General Characteristics
The results indicated significant group differences in perceived health status (F=12.7, p<0.001). Those who reported “good” health status had higher health behavior scores for MetS prevention than those who reported “moderate” or “bad” health status (Table 1).
Correlations of Health Behaviors for MetS Prevention
The examined correlation coefficients included knowledge of MetS, social support, self-efficacy, attitudes, and health behaviors for MetS prevention (Table 3). Health behaviors for MetS prevention displayed positive correlations with all other coefficients, with self-efficacy (r = 0.54, p < 0.01) and attitude toward health behavior (r = 0.45, p < 0.01) displaying moderate correlations, and knowledge about metabolic syndrome (r = 0.24, p < 0.01) and social support (r = 0.31, p < 0.01) displaying weak correlations.
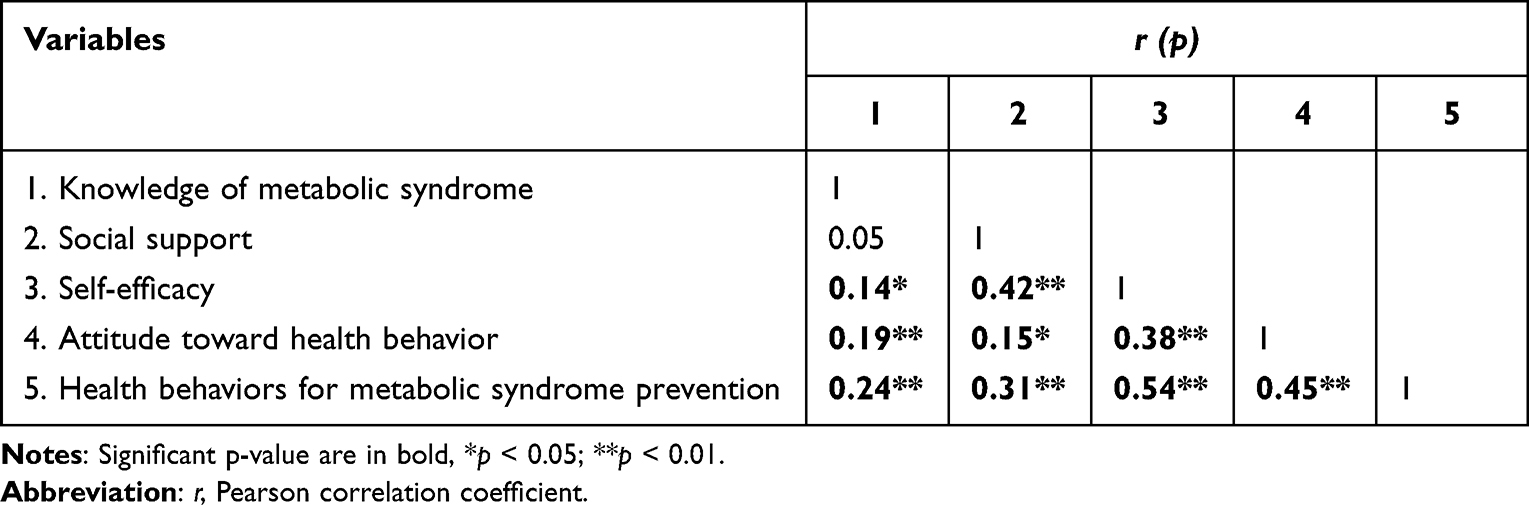 |
Table 3 Correlations Among Knowledge, Social Support, Self-Efficacy, Attitude, and Health Behaviors for Metabolic Syndrome Prevention (N = 241) |
Regression Analysis of Health Behaviors for MetS Prevention
Table 4 presents the results of the regression analysis of health behaviors for MetS prevention. Self-perceived health status was a significant predictor of health behaviors for MetS prevention, with participants who reported good perceived health displaying a significantly higher level of health behaviors for MetS prevention than those who reported bad perceived health (β = 0.24, t = 2.85, p = 0.005). Knowledge of MetS was also a significant predictor of health behaviors for MetS prevention, with higher levels of knowledge being associated with higher levels of health behaviors (β = 0.13, t = 2.58, p = 0.011). Self-efficacy and attitude were significant predictors of health behaviors for MetS prevention (β =0.09, t = 1.53, p =0.127), whereas social support was not. Higher levels of self-efficacy were associated with higher levels of health behaviors for MetS prevention (β = 0.33, t = 5.29, p < 0.001), as were higher levels of attitude toward health behavior (β = 0.26, t = 4.66, p < 0.001). The overall model was significant (R2=0.42, ΔR2=0.40, F=18.38, p <0.001), explaining 42% of the variance in health behaviors for MetS prevention. The findings indicated that self-perceived health status, knowledge of MetS, self-efficacy, and attitudes were significantly associated with the prediction of health behaviors for MetS prevention among middle-aged postmenopausal women.
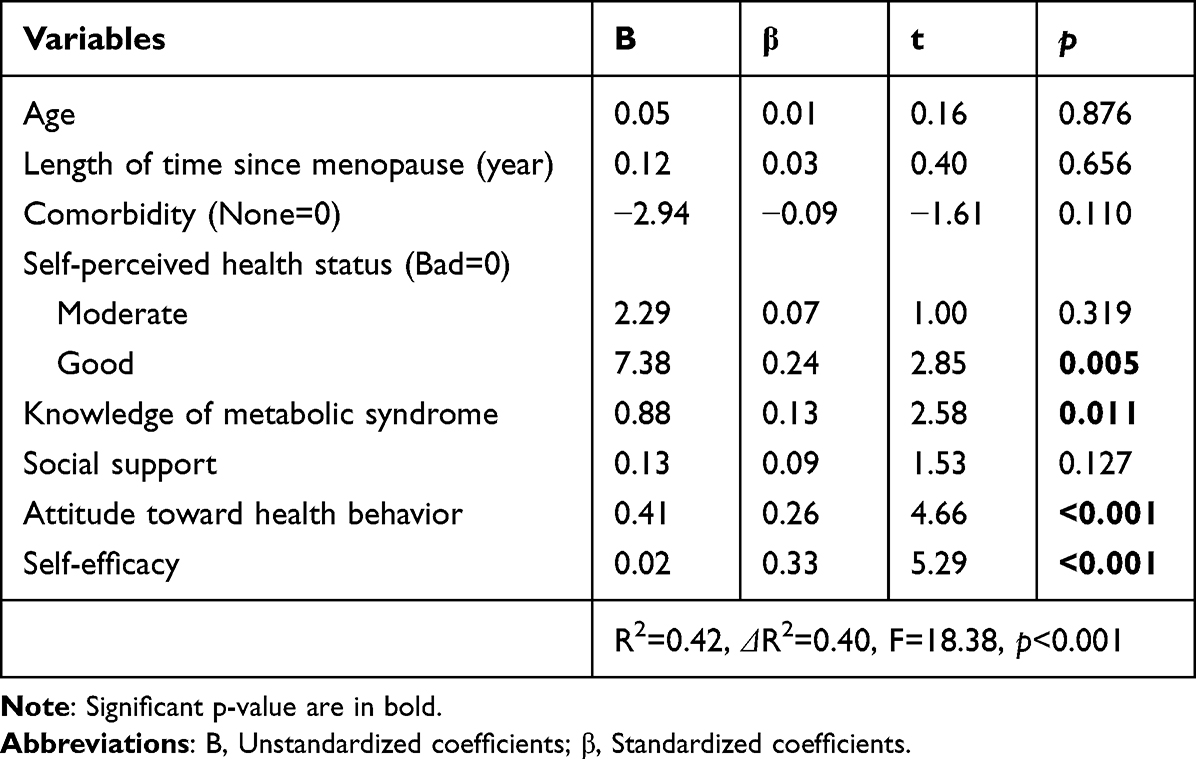 |
Table 4 Influencing Factors on Health Behaviors for Metabolic Syndrome Prevention (N = 241) |
Discussion
This study investigated the factors affecting health behaviors for MetS prevention among middle-aged postmenopausal women based on the IMB model. Among middle-aged women, hormonal fluctuations increase vulnerability to cardiovascular disease, and the presence of MetS further exacerbates this risk.16 Consequently, prevention of MetS is crucial for reducing mortality rates and enhancing overall health in middle-aged postmenopausal women. To prevent and treat MetS, it is important to maintain healthy behaviors,43 including exercise and a healthy diet;44 therefore, this study aimed to examine the factors that influence health behaviors that can prevent MetS. To our knowledge, this is the first study to examine health behaviors for MetS prevention based on the components of the IMB model among postmenopausal women at risk of MetS in Korea.
No significant differences were found in health behaviors for MetS prevention based on general characteristics, such as education, occupation, and income. Previous research has indicated that socioeconomic factors, including education, occupation, and income, result in significant differences in the incidence of MetS, with higher levels associated with a lower risk of MetS.45,46 However, the lack of significant differences in this study may be due to the fact that the study measured health behaviors rather than the occurrence of MetS. It is also possible that the study missed socioeconomically disadvantaged people who did not have access to the online questionnaire.
Middle-aged postmenopausal women who reported good perceived health were found to have a significantly higher level of health behaviors than those who reported bad perceived health. Previous studies have also shown that better perceived health is associated with greater engagement in health behaviors for MetS prevention.47 Additionally, a previous study reporting the association between MetS and subjective health status among Pakistani immigrant women found that the poorer the subjective health status, the higher the prevalence of MetS.48 Therefore, these findings emphasize the need to consider both objective and subjective health measures when promoting health behaviors.
Furthermore, knowledge of MetS helps predict health behaviors for MetS prevention. According to a previous study, inadequate knowledge about MetS negatively affects an individual’s adherence to lifestyle changes.21 Additionally, inadequate knowledge may negatively affect an individual’s motivation to change their behavior.49 Previous studies have shown47 that higher levels of knowledge about MetS are associated with higher levels of health behaviors for MetS prevention. Previous studies have also reported that improving awareness of cardiovascular disease not only increases the related preventive behaviors but also significantly reduces mortality from cardiovascular disease in women.20 Therefore, improving awareness of MetS prevention behaviors is expected to reduce the prevalence of MetS. However, awareness of MetS among women remains low, and there is a lack of research on this topic. In this context, we propose increasing education for middle-aged women at the government and community levels to raise awareness about MetS prevention. The results of this study suggest that providing individualized education is important for promoting health behaviors.
This study found that self-efficacy and attitudes toward health behaviors were significant predictors of health behaviors for MetS prevention, which suggests that intrapersonal factors, such as self-efficacy and attitude, may be more influential in promoting health behaviors. Previous studies have shown negative health attitudes in populations at high risk for MetS. Attitudes toward health, in turn, influence health behaviors.21,45 This finding emphasizes the importance of addressing individual beliefs and attitudes when promoting health behaviors.
Social support was not a significant predictor of health behaviors for MetS prevention. Although social support has been considered as helpful in improving health behaviors in previous studies,50,51 our results are inconsistent with this finding. This may be related to the sociocultural phenomenon that middle-aged Korean women tend to prioritize their families’ health over their own and adopt a family centered approach in their daily lives.52 However, spousal and family support is often needed to manage the symptoms of MetS,51 and social support may be an important factor in the implementation of other interventions; therefore, further research should be conducted.
A literature review showed that lifestyle interventions effectively reduce MetS risk factors and their prevalence.46 While both individual and structural approaches are needed,51 the findings of this study show the importance of an individualized approach to treat MetS. This study suggests that intrapersonal approaches are more effective than interpersonal strategies for middle-aged women. Therefore, in addition to objective physical health assessments and counseling, it is important to include subjective health status assessments, individualized knowledge education, and interventions that can positively impact self-efficacy and attitudes toward health behaviors. These findings can aid health promotion strategies aimed at improving health behaviors among middle-aged women.
As prevention is important in the case of MetS, this study focused on undiagnosed middle-aged postmenopausal women at high risk of MetS to prevent the incidence of MetS among them. However, not including individuals diagnosed with MetS may be a limitation of this study. Thus, it is recommended that this study be expanded to include individuals who have been diagnosed with MetS, as health behaviors are important for the treatment of MetS.
Conclusion
In conclusion, this study found that middle-aged postmenopausal Korean women’s cognitive, motivation and behavioral skills of health behaviors significantly influenced health behaviors for MetS prevention, which provides theoretical evidence for designing targeted programs to promote health behaviors for MetS prevention. The finding of this study suggest that intrapersonal factors such as knowledge, self-efficacy and attitude were found to be more influential in promoting health behaviors for MetS prevention. Therefore, healthcare providers should emphasize the importance of addressing individuals’ cognition, motivation and behavioral skills in the sociocultural context, provide individualized education to promote health behaviors for MetS prevention in middle-aged women during menopause.
Abbreviations
MetS, metabolic syndrome; IMB, Information, Motivation, Behavioral skills.
Data Sharing Statement
The participants of this study did not provide written consent for their data to be shared publicly; therefore, owing to the sensitive nature of the research, the data is not available.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Review Board of Konyang University (IRB NO. KYU 2022-11-022-001). The study complied with the Declaration of Helsinki on the ethical principles for human medical research. Participation in this study was completely voluntary. Participants could check the online documents for the study details, including the objectives, significance, and content. If they wished to participate, they provided informed consent by clicking the consent button, and were able to access the questionnaire. In other words, the participants in the research expressed their intention to voluntarily participate prior to starting the research survey. The IRB accepted a paper consent form waiver owing to the inherent difficulty of acquiring paper consent forms from online surveys. The researcher subsequently posted the study description online, which the participant reviewed, with the consent form presented on the next page. If the participant agreed to participate in the study, they were asked to sign the consent form by pressing the button labelled “I agree to participate in the study”.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Fuster V. The global burden of cardiovascular diseases and risks: a compass for global action. J Am Coll Cardiol. 2020;76(25):2980–2981. doi:10.1016/j.jacc.2020.11.021
2. Eckel RH, Alberti KG, Grundy SM, Zimmet PZ. The metabolic syndrome. Lancet. 2010;375(9710):181–183. doi:10.1016/S0140-6736(09)61794-3
3. Sperling LS, Mechanick JI, Neeland IJ, et al. The cardiometabolic health alliance: working toward a new care model for the metabolic syndrome. J Am Coll Cardiol. 2015;66(9):1050–1067. doi:10.1016/j.jacc.2015.06.1328
4. Stepanova M, Rafiq N, Younossi ZM. Components of metabolic syndrome are independent predictors of mortality in patients with chronic liver disease: a population-based study. Gut. 2010;59(10):1410–1415. doi:10.1136/gut.2010.213553
5. O’Neill S, O’Driscoll L. Metabolic syndrome: a closer look at the growing epidemic and its associated pathologies. Obes Rev. 2015;16(1):1–12. doi:10.1111/obr.12229
6. Tune JD, Goodwill AG, Sassoon DJ, Mather KJ. Cardiovascular consequences of metabolic syndrome. Transl Res. 2017;183:57–70. doi:10.1016/j.trsl.2017.01.001
7. Moore JX, Chaudhary N, Akinyemiju T. Metabolic syndrome prevalence by race/ethnicity and sex in the United States, National Health and Nutrition Examination Survey, 1988–2012. Prev Chronic Dis. 2017;14:E24. doi:10.5888/pcd14.160287
8. Huh JH, Kang DR, Kim JY, Koh KK. Metabolic syndrome fact sheet 2021: executive report. Cardiometab Syndr J. 2021;1(2):125–134. doi:10.51789/cmsj.2021.1.e15
9. Cornier MA, Dabelea D, Hernandez TL, et al. The metabolic syndrome. Endocr Rev. 2008;29(7):777–822. doi:10.1210/er.2008-0024
10. Isomaa B, Almgren P, Tuomi T, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001;24(4):683–689. doi:10.2337/diacare.24.4.683
11. Ford ES, Giles WH, Dietz WH. Prevalence of the metabolic syndrome among US adults: findings from the third National Health and Nutrition Examination Survey. JAMA. 2002;287(3):356–359. doi:10.1001/jama.287.3.356
12. Ervin RB. Prevalence of metabolic syndrome among adults 20 years of age and over, by sex, age, race and ethnicity, and body mass index: United States, 2003–2006. Natl Health Stat Report. 2009;13(13):1–7.
13. Ren J, Kelley RO. Cardiac health in women with metabolic syndrome: clinical aspects and pathophysiology. Obesity. 2009;17(6):1114–1123. doi:10.1038/oby.2009.8
14. Eshtiaghi R, Esteghamati A, Nakhjavani M. Menopause is an independent predictor of metabolic syndrome in Iranian women. Maturitas. 2010;65(3):262–266. doi:10.1016/j.maturitas.2009.11.004
15. Pu D, Tan R, Yu Q, Wu J. Metabolic syndrome in menopause and associated factors: a meta-analysis. Climacteric. 2017;20(6):583–591. doi:10.1080/13697137.2017.1386649
16. Mumusoglu S, Yildiz BO. Metabolic syndrome during menopause. Curr Vasc Pharmacol. 2019;17(6):595–603. doi:10.2174/1570161116666180904094149
17. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment Panel III). JAMA. 2001;285(19):2486–2497. doi:10.1001/jama.285.19.2486
18. Oh EG, Bang SY, Hyun SS, et al. Effects of a 6-month lifestyle modification intervention on the cardiometabolic risk factors and health-related qualities of life in women with metabolic syndrome. Metabolism. 2010;59(7):1035–1043. doi:10.1016/j.metabol.2009.10.027
19. Watanabe M, Yokotsuka M, Yamaoka K, Adachi M, Nemoto A, Tango T. Effects of a lifestyle modification programme to reduce the number of risk factors for metabolic syndrome: a randomised controlled trial. Public Health Nutr. 2017;20(1):142–153. doi:10.1017/S1368980016001920
20. Haidinger T, Zweimüller M, Stütz L, Demir D, Kaider A, Strametz-Juranek J. Effect of gender on awareness of cardiovascular risk factors, preventive action taken, and barriers to cardiovascular health in a group of Austrian subjects. Gend Med. 2012;9(2):94–102. doi:10.1016/j.genm.2012.02.001
21. Alefishat EA, Abu Farha RK, Al-Debei MM. Self-reported adherence among individuals at high risk of metabolic syndrome: effect of knowledge and attitude. Med Princ Pract. 2017;26(2):157–163. doi:10.1159/000453037
22. Im EO, Ko Y, Hwang H, et al. ‘Physical activity as a luxury’: African American women’s attitudes toward physical activity. West J Nurs Res. 2012;34(3):317–339. doi:10.1177/0193945911400637
23. Bassi N, Karagodin I, Wang S, et al. Lifestyle modification for metabolic syndrome: a systematic review. Am J Med. 2014;127(12):1242:e1–1242.10. doi:10.1016/j.amjmed.2014.06.035
24. Chen D, Zhang H, Shao J, et al. Determinants of adherence to diet and exercise behaviours among individuals with metabolic syndrome based on the Capability, Opportunity, Motivation, and Behaviour model: a cross-sectional study. Eur J Cardiovasc Nurs. 2023;22(2):193–200. doi:10.1093/eurjcn/zvac034
25. Deakin T, McShane CE, Cade JE, Williams RD. Group based training for self-management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2005;2005(2):CD003417. doi:10.1002/14651858.CD003417.pub2
26. Fisher JD, Fisher WA, Amico KR, Harman JJ. An information-motivation-behavioral skills model of adherence to antiretroviral therapy. Health Psychol. 2006;25(4):462–473. doi:10.1037/0278-6133.25.4.462
27. Robertson AA, Stein JA, Baird-Thomas C. Gender differences in the prediction of condom use among incarcerated juvenile offenders: testing the information-motivation-behavior skills (imb) model. J Adolesc Health. 2006;38(1):18–25. doi:10.1016/j.jadohealth.2004.08.013
28. Osborn CY, Egede LE. Validation of an Information-Motivation-Behavioral Skills model of diabetes self-care (IMB-DSC). Patient Educ Couns. 2010;79(1):49–54. doi:10.1016/j.pec.2009.07.016
29. Chang SJ, Choi S, Kim S-A, Song M. Intervention strategies based on information-motivation-behavioral skills model for health behavior change: a systematic review. Asian Nurs Res. 2014;8(3):172–181. doi:10.1016/j.anr.2014.08.002
30. Kim CJ, Kang HS, Kim JS, Won YY, Schlenk EA. Predicting physical activity and cardiovascular risk and quality of life in adults with osteoarthritis at risk for metabolic syndrome: a test of the information-motivation-behavioral skills model. Nurs Open. 2020;7(4):1239–1248. doi:10.1002/nop2.500
31. Lee G, Yang SJ, Chee YK. Assessment of healthy behaviors for metabolic syndrome among Korean adults: a modified information-motivation-behavioral skills with psychological distress. BMC Public Health. 2016;16(1):518. doi:10.1186/s12889-016-3185-8
32. Malayala SV, Raza A. Health behavior and perceptions among African American women with metabolic syndrome. J Community Hosp Intern Med Perspect. 2016;6(1):30559. doi:10.3402/jchimp.v6.30559
33. Lin CH, Chiang SL, Yates P, et al. Moderate physical activity level as a protective factor against metabolic syndrome in middle-aged and older women. J Clin Nurs. 2015;24(9–10):1234–1245. doi:10.1111/jocn.12683
34. Gurka MJ, Vishnu A, Okereke OI, Musani S, Sims M, DeBoer MD. Depressive symptoms are associated with worsened severity of the metabolic syndrome in African American women independent of lifestyle factors: a consideration of mechanistic links from the Jackson heart study. Psychoneuroendocrinology. 2016;68:82–90. doi:10.1016/j.psyneuen.2016.02.030
35. Jeon HW, Kim J. A study of factors influencing on health 1behavior compliance in metabolic syndrome risk group’s. KAIS. 2022;23(1):236–246. doi:10.5762/KAIS.2022.23.1.236
36. Oh EG, Bang SY, Hyun SS, Chu SH, Jeon JY, Kang MS. Knowledge, perception and health behavior about metabolic syndrome for an at risk group in a rural community area. J Korean Acad Nurs. 2007;37(5):790–800. doi:10.4040/jkan.2007.37.5.790
37. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
38. Sherer M, Maddux JE, Mercandante B, Prentice-Dunn S, Jacobs B, Rogers RW. The self-efficacy scale: construction and validation. Psychol Rep. 1982;51(2):663–671. doi:10.2466/pr0.1982.51.2.663
39. Jung YS. Effects of Phase I Cardiac Rehabilitation Program on Self-Efficacy and Performance of Health Behavior in Acute Myocardial Infarction Patients. Seoul: Seoul National University; 2002.
40. Boudreau F, Godin G. Participation in regular leisure-time physical activity among individuals with type 2 diabetes not meeting Canadian guidelines: the influence of intention, perceived behavioral control, and moral norm. Int J Behav Med. 2014;21(6):918–926. doi:10.1007/s12529-013-9380-4
41. Jang T, Song R. A structural model explaining the health behaviors among adults with metabolic syndrome: theory of planned behavior approach. Korean J Adult Nurs. 2020;32(1):98–108. doi:10.7475/kjan.2020.32.1.98
42. Kang SW. The validity and reliability of a lifestyle evaluation tool for patients with metabolic syndrome. J Korean Acad Fundam Nurs. 2010;17(4):487–497.
43. Park YS, Kang SH, Jang SI, Park EC. Association between lifestyle factors and the risk of metabolic syndrome in the South Korea. Sci Rep. 2022;12(1):13356. doi:10.1038/s41598-022-17361-2
44. Takahara M, Shimomura I. Metabolic syndrome and lifestyle modification. Rev Endocr Metab Disord. 2014;15(4):317–327. doi:10.1007/s11154-014-9294-8
45. Hoveling LA, Liefbroer AC, Bültmann U, Smidt N. Understanding socioeconomic differences in metabolic syndrome remission among adults: what is the mediating role of health behaviors? Int J Behav Nutr Phys Act. 2021;18(1):147. doi:10.1186/s12966-021-01217-5
46. van Namen M, Prendergast L, Peiris C. Supervised lifestyle intervention for people with metabolic syndrome improves outcomes and reduces individual risk factors of metabolic syndrome: a systematic review and meta-analysis. Metabolism. 2019;101:153988. doi:10.1016/j.metabol.2019.153988
47. Lo SF, Lu FT, O Yang AC, et al. Metabolic syndrome-related knowledge, attitudes, and behavior among indigenous communities in Taiwan: a cross-sectional study. Int J Environ Res Public Health. 2023;20(3):2547. doi:10.3390/ijerph20032547
48. Hjellset VT, Ihlebæk CM, Bjørge B, Eriksen HR, Høstmark AT. Health-related quality of life, subjective health complaints, psychological distress and coping in Pakistani immigrant women with and without the metabolic syndrome: the innvadiab-deplan study on Pakistani immigrant women living in Oslo, Norway. J Immigr Minor Health. 2011;13(4):732–741. doi:10.1007/s10903-010-9409-6
49. Lewis SJ, Rodbard HW, Fox KM, Grandy S; SHIELD Study Group. Self-reported prevalence and awareness of metabolic syndrome: findings from SHIELD. Int J Clin Pract. 2008;62(8):1168–1176. doi:10.1111/j.1742-1241.2008.01770.x
50. Park S, Cho S, Lee E, Choi S, Choo J. The association between social support and health behaviors for metabolic syndrome prevention among university students: the mediating effect of perceived stress. J Korean Acad Community Health Nurs. 2021;32(3):404–414. doi:10.12799/jkachn.2021.32.3.404
51. Nilsson PM, Tuomilehto J, Rydén L. The metabolic syndrome–What is it and how should it be managed? Eur J Prev Cardiol. 2019;26(2_suppl):33–46. doi:10.1177/2047487319886404
52. Kang YS, Chung MJ, Park YS, et al. An analysis of articles for health promotion behaviors of Korean middle-aged. Res Community Public Health Nurs. 2009;20(1):75–86.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.