")
Back to Journals » Patient Preference and Adherence » Volume 11
Factors associated with preoperative anxiety levels of Turkish surgical patients: from a single center in Ankara
Authors Erkilic E, Kesimci E , Soykut C, Doger C, Gumus T, Kanbak O
Received 11 November 2016
Accepted for publication 25 January 2017
Published 28 February 2017 Volume 2017:11 Pages 291—296
DOI https://doi.org/10.2147/PPA.S127342
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ezgi Erkilic, Elvin Kesimci, Cem Soykut, Cihan Doger, Tülin Gumus, Orhan Kanbak
Department of Anesthesiology and Reanimation, Atatürk Training and Research Hospital, Ankara, Turkey
Background: Preoperative anxiety and stress are undoubtedly a difficult experience in patients undergoing elective surgery. These unpleasant sensations depend on several factors. The objective of this study was to evaluate the preoperative anxiety levels in a sample of Turkish population, as well as the underlying causes using the Spielberger State-Trait Anxiety Inventory (STAI anxiety) scale.
Methods: The study was conducted according to the Declaration of Helsinki and was approved by the local ethical committee. All participants gave written informed consent upon having received detailed information on the study. Upon entry in the study, state and trait anxiety questionnaires were completed by 186 patients scheduled for elective surgery. The influencing factors in regard to age, sex, educational status and others were also reported.
Results: There was a statistically significant positive correlation between state and trait anxiety scores in this Turkish population. While the most important predictive factors that affected state-STAI scores were age, sex and duration of sleep the night before surgery; educational status and age were the best predictors for determining the variation in trait-STAI scores.
Conclusion: The factors affecting anxiety levels in different populations might vary among different countries. Interestingly, in this sample of Turkish population, the trait anxiety levels were found to be higher from state-anxiety levels, especially in women and less educated people. Thus, doubts about operation and anesthesia are overlooked. This could be attributed to the low to intermediate life standards of people admitted to our hospital.
Keywords: state and trait anxiety, preoperative
Introduction
In studies on patients undergoing elective surgery, anxiety, depression, somatoform disorders and fear of pain are reported to be frequently observed.1–3 Among these, preoperative anxiety, with a prevalence ranging from 11% to 80% among adults, is of particular importance as a factor in increasing perioperative morbidity.4–6 It is an emotional response associated with several pathophysiological responses accompanied by activation of the autonomous nervous system.7,8 The level of preoperative anxiety may adversely affect different aspects of anesthesiological approach, surgical recovery and outcome.9–12
There are different factors playing a role in the development of preoperative anxiety. Generally, patients are ignorant about anesthesia and the anesthesiologist’s role in their care. Moreover, going under general anesthetic for a surgery is associated highly with a fear of death. Patients are curious about anesthesia options, experiences of postoperative pain and nausea.13,14 Due to these factors, preanesthetic assessment has several objectives.15 However, lack of education, the physical structure and the intensity of an anesthesia clinic as well as economical issues in different countries may sometimes cause limitations in reducing patient compliance with treatment.
The main objective of this paper was to determine the preoperative anxiety levels of patients in a sample of Turkish population admitted to our hospital for any kind of surgery. We evaluated the impact of underlying causes on the level of anxiety status using the Spielberger State-Trait Anxiety Inventory (STAI) scale in this population.
Methods
This study was conducted according to the Declaration of Helsinki and was approved by the local ethical committee of Ataturk Training and Research Hospital, Ankara, Turkey. All participants provided written informed consent upon having received detailed information on the study. At Ankara Atatürk Training and Research Hospital, patients admit to the anesthesia clinic after referral to surgical clinics with decision of surgical team prior to their scheduled surgery. For those who were unable to attend an anesthesia clinic, an anesthesia resident visited the patient and returned the information of the patient to the consultant anesthesiologist. A standard interview format was delivered during the preanesthetic interview. The patients medical history, including previous surgical and anesthesia experiences, was taken. A physical examination was performed, and preoperative laboratory tests and necessary consultations from other specialties were obtained. Anesthesia methods and patient-specific conditions were then explained to the patients.
In this study, once informed consent was given, any Turkish patient aged >18 years who was to undergo various procedures with either general/regional anesthesia which were less than 3 hrs were included in the study. The patients with significant cognitive impairment or an existing psychiatric disorder were not involved. The STAI questionnaire was administered to the patient. STAI is a self-administered questionnaire in Turkish,16–18 and consists of 40 items which are grouped into 2 scales that measure baseline (trait; t-STAI) and situational (state; s-STAI) anxiety.
On the day of surgery, once the patient had arrived at the operating theatre, the responsible anesthesiologist reviewed the anesthetic information. The patients were prepared for anesthesia and surgery. No premedication was given. A 20 G intravenous cannula was inserted into a large antecubital vein, and Ringer’s lactate solution 5–7 mL/kg−1 was administered. Heart rate (3-channel electrocardiography), blood pressure, peripheral oxygen saturation and end-tidal CO2 (Datex-Ohmeda S/5TM Compact Critical Care Monitor) were monitored. By this point, the study was finished.
A total sample size of 164 cases was required to detect at least 0.25 correlation between STAI scores and any of clinical characteristics with a power of 95% at the 5% significance level. The correlation coefficient of 0.25 was taken from both the pilot study and our clinical experiments. Sample size estimation was performed by using G*Power (version 3.0.10; Kiel, Germany) software.
Statistical analysis
Data analysis was performed by using SPSS for Windows, version 11.5 (SPSS Inc., Chicago, IL, USA). Whether the distributions of continuous variables were normal or not was determined by Kolmogorov-Smirnov test. Levene’s test was used for the evaluation of homogeneity of variances. Data were shown as mean ± standard deviation or number of cases and (%) where applicable.
While the mean differences between groups were compared by Student’s t-test, one-way analysis of variance (ANOVA) was applied for determining the differences among more than 2 independent groups. When the P-value from one-way ANOVA was statistically significant, post hoc Tukey HSD test was used to know which group differs from which others. Degrees of association between variables were evaluated by Spearman’s rank correlation analyses.
Determining the best predictor(s) that affected both state and trait anxiety levels were evaluated by multiple linear regression analyses after adjustment for all possible confounding factors. Any variable whose univariate test had a P-value <0.10 was accepted as a candidate for the multivariable model along with all variables of known clinical importance. Coefficient of regression and 95% confidence interval (CI) for each independent variable were also calculated.
A P-value <0.05 was considered statistically significant.
Results
During the 6 month study period, 250 adult patients were screened, with data completed by 186 patients (due to missing information [n=50] and patient refusal to partake [n=14]). Patient mean age was 44.4±16.1 years. Out of the total respondents, 104 (55.9%) were males and 21% aged >60 years. Ten (5.4%) participants were illiterate, and 45.7% of the participants were employed. One hundred and eight patients (58.1%) were classified as American Society of Anesthesiologist (ASA) I, while only 2 patients (1.1%) belonged to ASA IV. More than half of the patients (57.5%) had had at least 1 previous operation. In regard to sleeping hours, 12 patients (6.5%) had 0–2 hours of sleep the night before surgery. In the study population, the mean preoperative trait anxiety score was 40.6±8.5, while state anxiety score was 38.0±9.9 (Table 1).
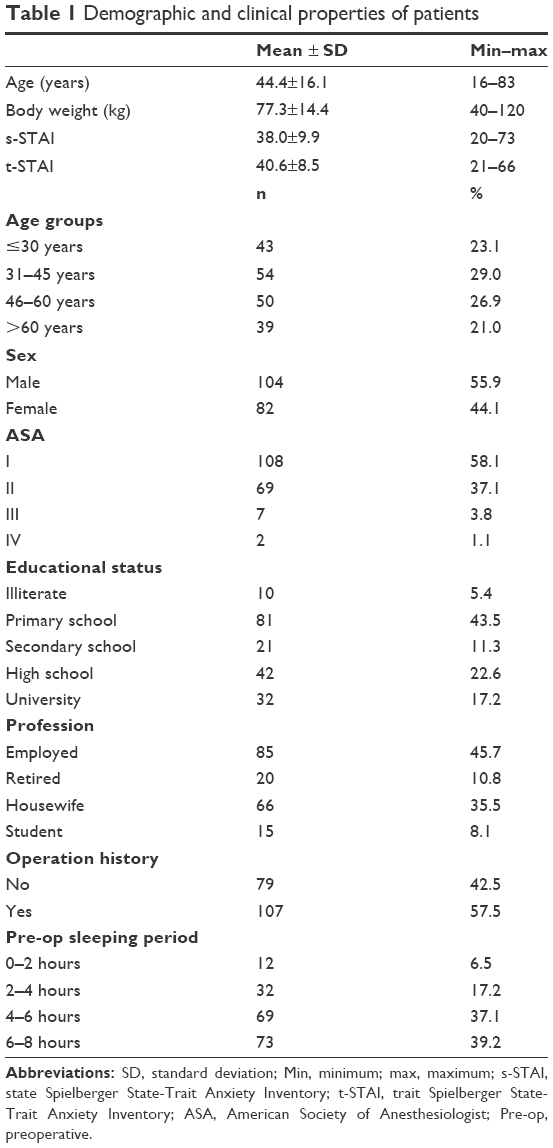 | Table 1 Demographic and clinical properties of patients |
Age was found to be significantly correlated with preoperative state anxiety score. Being younger (≤30 years) caused a significantly higher preoperative state anxiety score in comparison to patients >45 years of age (P<0.001), while patients aged between 31–45 years had a significantly higher preoperative trait anxiety score with respect to aging (>60 years). Female sex (B=7.988 [95% CI: 2.917–13.060], P=0.002) and less sleeping periods (B=−2.069 [95% CI: −3.552–0.586], P=0.006) were found to increase preoperative state anxiety scores. As educational level increased, preoperative trait score decreased (r=−0.261 and P<0.001). Female patients had both higher preoperative trait and state anxiety scores (P<0.001). Housewives had significantly higher preoperative trait scores than employees and retired people (P<0.001). The patients who were primary school graduates were more anxious than high school graduates (preoperative trait anxiety score; 42.6±8.2 vs 38.0±8.0, P=0.030). With regard to type of surgery planned, preoperative state anxiety scores of patients undergoing cardiovascular surgery were significantly lower in comparison to gynecologic and aesthetic surgery (P=0.014 vs P=0.036) (Tables 2 and 3). On the other hand, preoperative trait anxiety scores were significantly higher in the gynecologic surgery group compared to cardiovascular and urologic surgery group (P=0.026 vs P=0.023) (Table 4).
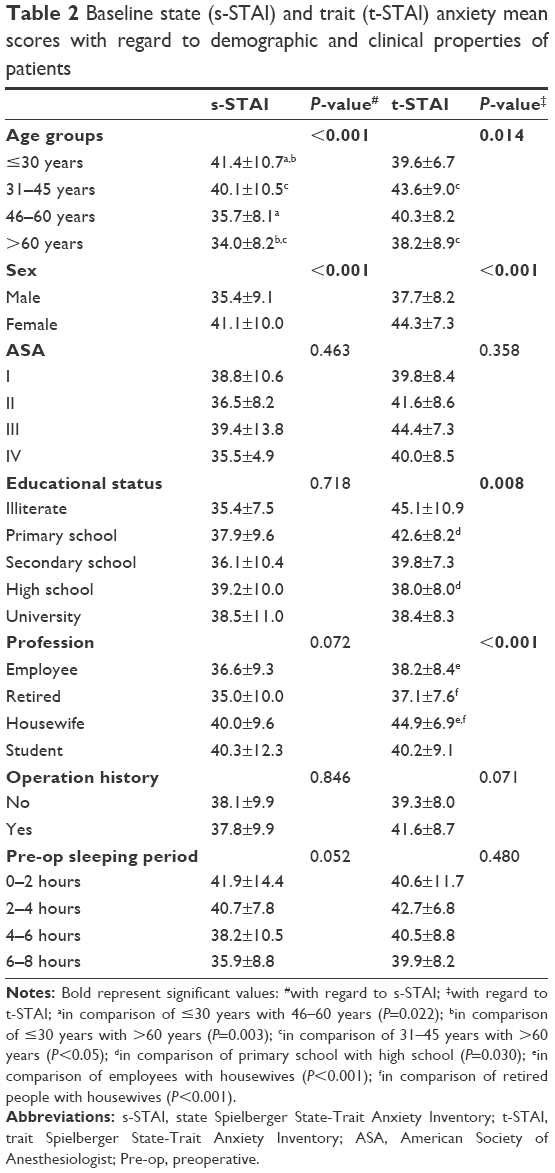 | Table 2 Baseline state (s-STAI) and trait (t-STAI) anxiety mean scores with regard to demographic and clinical properties of patients |
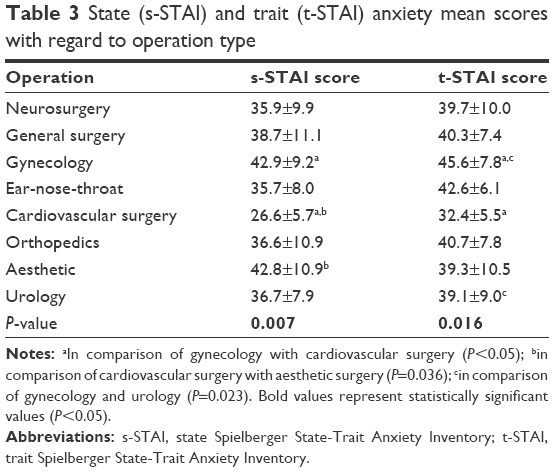 | Table 3 State (s-STAI) and trait (t-STAI) anxiety mean scores with regard to operation type |
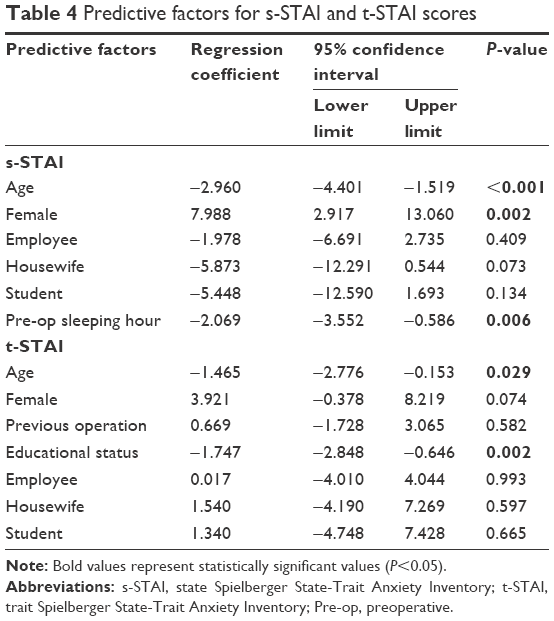 | Table 4 Predictive factors for s-STAI and t-STAI scores |
Discussion
The primary endpoint of this study was to assess the anxiety levels of Turkish patients in a teaching hospital. Our results are similar with those reported in other studies. On the other hand, we recognized that surgery and hospitalization did not add extra stress to the patients’ baseline anxiety status.
There have been several studies performed to evaluate anxiety levels of Turkish people. In one of these, Kara and Açikel reported that Turkish people had similar characteristic properties with people from Europe and Middle East.19 As far as surgical patients are concerned, moderate to severe anxiety observed in this study is similar to the data reported from previous studies.20,23
In one study, it was emphasized that stress and coping strategy of Turks was mainly emotion focused.24 This was confirmed by 2 other studies reporting the importance of preoperative visits and social support on the level of anxiety in hospitalized patients.21,22 However, as far as we know, there has not been a study performed by anesthesiologists from Turkey in determining the anxiety levels of preoperative patients. In Turkey, mainly anesthesiologists, not the surgeons, play a vital role in informing patients and avoiding stress before, during and after operation.25 This brings the necessity of sparing enough time preoperatively, which is a serious problem in developing countries such as Turkey, with impossibilities related to time and unequal opportunities.
High levels of anxiety experienced by most patients scheduled for surgery are mainly due to the magnitude of operation, anesthesia and postoperative pain. Actually, preoperative preparation is very important.26–28 We should effectively inform the patients, especially those who were illiterate, in the preoperative visit. However, Lebanese patients failed to show such favorable effects of preoperative information.29,30 Although we have no idea about the educational status of this study population, we believe in the importance of basal levels of patient’s cultural status. On the other hand, we observed that high school graduates were significantly less anxious in comparison to primary school graduates. This was parallel to other studies findings.31,32 There are contradictory results concerning the educational status. Caumo et al reported that as educational status increased, anxiety level also increased as observed in other investigators’ studies.4,33,34 This could be attributed to the awareness that educated people have about the risks involved in an operation. Educated people could express their anxiety level more precisely.35 Probably, sometimes inadequate information obtained by literate people from different sources, like television, internet, or neighbors, could lead to misinterpretation and misunderstanding of medical information. This could harm patients by increasing their anxiety. However, according to our results, we believe that education helps in preparing the patient and reducing anxiety preoperatively. Interestingly, Wells et al reported that education could not be the predictor of preoperative anxiety.35
We are not surprised with the findings from other studies, supporting the relationship of high ASA classification status with higher levels of anxiety, but we could not show such a correlation in our patients.25 Nevertheless, our patients who had high body mass indexes had lower preoperative anxiety levels. This was hard to explain for us.
In these subjects, age and sex are two of the most talked about parameters. Mainly, it is evident that older age and male sex decrease preoperative anxiety.4,31,32–37 Our results confirm these findings. Housewives were found to be more anxious than employed and even retired people. However, some authors stated that in older adults, anxiety disorders and depression were more prevalent, so that older people were more anxious than younger ones preoperatively.38 The explanation of aging and the basal social and cultural status of old people studied in these investigations may have caused such inconsistent results. We did not divide patients >60 years into further decades. The oldest patient in our study was 83 years, which could be an intermediate old age in other western populations. Even so, patients >45 years old were less anxious in our study.
In correlation with female sex and high anxiety levels, gynecologic operations were also related to more anxiety states in our population in parallel with findings in Pakistani surgical patients determined by Jafar and Khan.25 As expected, there are contradictory results about this parameter. Some authors did not take surgery type into consideration for anxiety, while others suggested thoracic or ear-nose-throat surgery as leading causes of preoperative anxiety.31,39,40
Although many authors agree that previous surgeries decrease the preoperative anxiety status, they do not play a role in either reduction or increase of anxiety levels in our study.4,31,33,35,38,41
Unlike other studies, we tried to investigate the effectiveness of preoperative sleeping period in preoperative anxiety levels. Less sleeping hours caused increased levels of anxiety. This confirms the importance of preanesthetic visit and premedication, as expected.
In this study, we conducted the STAI questionnaire at the preanesthetic visit. This allowed the patients to meet their anesthesiologists and be informed about their health status. The patients could also have been asked about their anxiety levels again after the first meeting in order to evaluate the effectiveness of preoperative education, but our facilities did not allow us to visit them for a second time before their operation.
Another limitation in our study was that we could not interpret the social family support in our study population. This has been reported to be an important factor in our population. The results of this study should be evaluated with those underlying factors. Mostly, what we had observed was that surgery and hospitalization did not augment anxiety levels of this population. This could be attributed to either strong family relationships or rather high levels of anxiety due to life standards of this country.
Conclusion
Patients might have different frequencies of anxiety before surgery. The factors affecting anxiety levels in different populations might vary among different countries. This is an important study since it reflects the clinical characteristics and personality traits of a sample of Turkish people. As far as our population is concerned, we believe that difficult life standards have already prepared the Turkish population to unfavorable events. Moreover, people give importance to preoperative counseling. We believe that detailed preoperative anesthesia visits and strong family ties are important to reduce anxiety and increase patients’ coping strategies in this population.
Acknowledgments
All the authors contributed to the research. The manuscript was read and approved by all the authors. This study was presented as a pilot study and as an oral presentation in European Society of Anaesthesiology Congress 31 May–03 June 2014/Stockholm, Sweden.
Disclosure
The authors report no conflicts of interest in this work.
References
Theunissen M, Peters ML, Bruce J, Gramke HF, Marcus MA. Preoperative anxiety and catastrophizing: a systematic review and meta-analysis of the association with chronic postsurgical pain. Clin J Pain. 2012;28(9):819–841. | ||
Rodin G, Voshart K. Depression in the medically ill: an overview. Am J Psychiatry. 1986;143(6):696–705. | ||
Valenzuela Millán J, Barrera Serrano JR, Ornelas Aguirre JM. Anxiety in preoperative anesthetic procedures. Cir Cir. 2010;78(2):147–151. | ||
Caumo W, Schmidt AP, Schneider CN, et al. Risk factors for postoperative anxiety in adults. Anaesthesia. 2001;56(8):720–728. | ||
Jlala HA, French JL, Foxall GL, Hardman JG, Bedforth NM. Effect of preoperative multimedia information on perioperative anxiety in patients undergoing procedures under regional anaesthesia. Br J Anaesth. 2010;104(3):369–374. | ||
Maranets I, Kain ZN. Preoperative anxiety and intraoperative anesthetic requirements. Anesth Analg. 1999;89(6):1346–1351. | ||
Miller AA. Psychological considerations in dentistry. J Am Dent Assoc. 1970;81(4):941–948. | ||
Williams JG, Jones JR. Psychophysiological responses to anesthesia and operation. JAMA. 1968;203(6):415–417. | ||
Gras S, Servin F, Bedairia E, et al. The effect of preoperative heart rate and anxiety on the propofol dose required for loss of consciousness. Anesth Analg. 2010;110(1):89–93. | ||
Kil HK, Kim WO, Chung WY, Kim GH, Seo H, Hong JY. Preoperative anxiety and pain sensitivity are independent predictors of propofol and sevoflurane requirements in general anaesthesia. Br J Anaesth. 2012;108(1):119–125. | ||
Kim WS, Byeon GJ, Song BJ, Lee HJ. Availability of preoperative anxiety scale as a predictive factor for hemodynamic changes during induction of anesthesia. Korean J Anesthesiol. 2010;58(4):328–333. | ||
Munafò MR, Stevenson J. Anxiety and surgical recovery. Reinterpreting the literature. J Psychosom Res. 2001;51(4):589–596. | ||
Klafta JM, Roizen MF. Current understanding of patients’ attitudes toward and preparation for anesthesia: a review. Anesth Analg. 1996;83(6):1314–1321. | ||
Matthey P, Finucane BT, Finegan BA. The attitude of the general public towards preoperative assessment and risks associated with general anesthesia. Can J Anaesth. 2001;48(4):333–339. | ||
Oztas A, Erkilic E, Kesimci E, Keser I, Canatan D. What happens if the patient does not tell the truth to his anesthesiologist? Int J Anesthetic Anesthesiol. 2014;1:2. | ||
Mitchell M. Patient anxiety and modern elective surgery: a literature review. J Clin Nurs. 2003;12(6):806–815. | ||
Panda N, Bajaj A, Pershad D, Yaddanapudi LN, Chari P. Pre-operative anxiety. Effect of early or late position on the operating list. Anaesthesia. 1996;51(4):344–346. | ||
Le Compte A, Oner N. A study related to adaptation and standardization of State-Trait Anxiety Inventory into Turkish. Proceeding of 9th National Congress Psychiatry and Neurologic Sciences. 1975:457–462. | ||
Kara B, Açikel CH. Predictors of coping in a group of Turkish patients with physical disability. J Clin Nurs. 2012;21(7–8):983–993. | ||
Aykent R, Kocamanoğlu IS, Üstün E, Tür A, Şahinoğlu H. The reasons and evaluation of preoperative anxiety: a comparison of APAIS and STAI scores. Turkiye Klinikleri J Anest Reanim. 2007;5(1):7–13. | ||
Yardakci R, Akyolcu N. The effect of the visits made preoperative period on the patients’ anxiety level. J Nursing Res Dev (HEMAR-G). 2004;6:7–14. | ||
Akkaş Gürsoy A. To determine the anxiety levels and the factors which may cause anxiety in preoperative surgical patients. J Nursing Res Dev (HEMAR-G). 2001;1:23–29. | ||
Jerusalem M, Schwarzer R. Anxiety and self-concept as antecedents of stress and coping: a longitudinal study with German and Turkish adolescents. Pers Individ Dif. 1989;10(7):785–792. | ||
Deiner S, Lin HM, Bodansky D, Silverstein J, Sano M. Do stress markers and anesthetic technique predict delirium in the elderly? Dement Geriatr Cogn Disord. 2014;38(5–6):366–374. | ||
Jafar MF, Khan FA. Frequency of preoperative anxiety in Pakistani surgical patients. J Pak Med Assoc. 2009;59(6):359–363. | ||
Fountoulakis KN, Papadopoulou M, Kleanthous S, et al. Reliability and psychometric properties of the Greek translation of the State-Trait Anxiety Inventory form Y: preliminary data. Ann Gen Psychiatry. 2006;5:2. | ||
Lee D, Henderson A, Shum D. The effect of music on preprocedure anxiety in Hong Kong Chinese day patients. J Clin Nurs. 2004;13(3):297–303. | ||
Klopfenstein CE, Forster A, Van Gessel E. Anesthetic assessment in an outpatient consultation clinic reduces preoperative anxiety. Can J Anesth. 2000;47(6):511–515. | ||
Haque SN, Ara A, Imtiaz A, Hamirani M. Validity of visual analogue scale in assessment of anxiety: a comparative study in anesthesia clinic. Ann Abbasi Shaheed Hosp Karachi Med Dent Coll. 2004;9(2):571–574. | ||
Kindler CH, Harms C, Amsler F, Ihde-Scholl T, Scheidegger D. The visual analogue scale allows effective measurement of preoperative anxiety and detection of patient’s anesthetic concerns. Anesth Analg. 2000;90(3):706–712. | ||
Uddin I, Kurkuman AR, Jamil T, Iftikhar R. Pre-operative anxiety in patients admitted for elective surgery in King Saud hospital, Unaizah, Al-Qassim Kingdom of Saudi Arabia. Pak J Med Sci. 2002;18(4):306–310. | ||
Lichtor JL, Johanson CE, Mhoon D, Faure EA, Hassan SZ, Roizen MF. Preoperative anxiety: does anxiety level the afternoon before surgery predict anxiety level just before surgery? Anesthesiology. 1987;67(4):595–599. | ||
Domar AD, Everett LL, Keller MG. Preoperative anxiety: is it a predictable entity? Anesth Analg. 1989;69(6):763–767. | ||
Corman HH, Hornick EJ, Kritchman M, Terestman N. Emotional reactions of surgical patients to hospitalization, anesthesia and surgery. Am J Surg. 1958;96(5):646–653. | ||
Wells JK, Howard GS, Nowlin WF, Vargas MJ. Presurgical anxiety and postsurgical pain and adjustment: effects of a stress inoculation procedure. J Consult Clin Psychol. 1986;54(6):831–835. | ||
Wolters U, Wolf T, Stützer H, Schröder T. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1996;77(2):217–222. | ||
Soskolne V, Bonne O, Denour AK, Shalev AY. Depressive symptoms in hospitalized patients: a cross-sectional survey. Int J Psychiatry Med. 1996;26(3):271–285. | ||
Flint AJ. Epidemiology and comorbidity of anxiety disorders in the elderly. Am J Psychiatry. 1994;151(5):640–649. | ||
Moerman N, van Dam FS, Muller MJ, Oosting H. The Amsterdam preoperative anxiety and information scale (APAIS). Anesth Analg. 1996;82(3):445–451. | ||
Boker A, Brownell L, Donen N. The Amsterdam preoperative anxiety and information scale provides a simple and reliable measure of preoperative anxiety. Can J Anaesth. 2002;49(8):792–798. | ||
Badner NH, Nielsen WR, Munk S, Kwiatkowska C, Gelb AW. Preoperative anxiety: detection and contributing factors. Can J Anaesth. 1990;374(4 Pt 1):444–447. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.