Back to Journals » Cancer Management and Research » Volume 13
Factors Associated with Pre- and Post-Educational Intervention Knowledge Levels of HPV and Cervical Cancer Among the Male and Female University Students, Northwest Ethiopia
Authors Indracanti M ![]() , Berhane N
, Berhane N ![]() , Minyamer T
, Minyamer T
Received 2 July 2021
Accepted for publication 30 August 2021
Published 14 September 2021 Volume 2021:13 Pages 7149—7163
DOI https://doi.org/10.2147/CMAR.S326544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Meera Indracanti, Nega Berhane, Tigist Minyamer
Institute of Biotechnology, University of Gondar, Gondar, Ethiopia
Correspondence: Meera Indracanti Email [email protected]; [email protected]
Background: Human papillomavirus (HPV) infections are sexually transmitted and most frequently associated with cervical cancer in women, but they are also a public health concern in men. There is rising evidence that HPV’s role in other cancers, such as anal, vulva, vaginal, penis, head, and neck cancers. The present study aimed to understand the factors associated with HPV and cervical cancer knowledge levels of university students before and after an educational intervention.
Methods: An Institutional-based cross-sectional study was conducted from October to November 2018. A total of 638 study participants were selected using a simple random multistage sampling technique. A pretested questionnaire was used, consolidated the data, and analyzed with SPSS version 23. Bivariate and multivariate logistic regression analyses were performed to identify which variables were associated with the knowledge levels.
Results: Six hundred thirty-eight study participants with a 100% response rate, and the mean age was 21.07 years (±SD, 1.96). Initial awareness of various broad categories was 4.09, and after the intervention, it increased to 23.4, with an average increase of 19.31 at 99% CI, p≤ 0.001 significance level. Before the educational intervention, students with < 21 years of age [6.16, 95% CI: (2.21– 17.18)] and ≤ 2.5 CGPA [3.44, 95% CI: (1.51– 7.81)] were less knowledgeable over other counterparts. After educational intervention, the year of study was significantly associated with increased knowledge of overall and different broad categories of cervical cancer and HPV. Year of study, 1st-year students [AOR: 0.27, 95% CI: (0.14– 0.51)] over third years and above are less knowledgeable. First-year students and CGPA ≤ 2.5 were less improved awareness over others.
Conclusion: The educational intervention improved more than fourfold increase knowledge on cervical cancer and HPV, and the year of study was a key factor associated with overall improvement. This study suggests that educational intervention effectively strengthens our understanding of the spread of HPV and cervical cancer disease burden.
Keywords: Amhara, cancer, pre and posttest
Introduction
The human papillomavirus (HPV) infection is the most commonly sexually transmitted1,2 and coupled with an increased risk of cancer.3,4 HPV infection occurs soon after sexual debut, and about 80–90% of HPV infections are transitory and clear by early life.5 If HPV persists, it can lead to a range of benign and malignant lesions in both sexes,6 including genital warts,7 oropharyngeal, anal, penile,8,9 cervix, vulva, and vaginal cancers.10,11 70–80% of sexually active women will become infected with HPV at some point in their lives.8,12 Young women in their 20s have the highest prevalence of HPV infections,12,13 although men are at continual risk of contracting new infections throughout their lives.14
Cervical cancer is the sixth most commonly occurring cancer in women, accounting for 1.7% of all cancers.15 Cervical cancer has claimed the lives of over 90% of people in low- and middle-income nations.16 Cervical cancer is the second most common cancer in Ethiopian women aged 15 to 44 years old. According to ET (2019), HPV infections lead to 26.4% of cervical cancer, while 1.2% of anogenital cancer.17 It is projected that 6294 women are diagnosed with cervical cancer each year, with 4884 dying of the disease.
There is insufficient evidence regarding young people’s knowledge and understanding of cervical cancer, risk factors, screening, and HPV vaccine in the developing world.18 Despite its high incidence, HPV awareness is often low in most nations, including young adults.19
In underdeveloped countries, the sources of information through which people learn about cervical cancer remain restricted. Cervical cancer and HPV awareness and knowledge are persistently poor in developing countries.18 In Africa, unsafe sexual behavior and a lack of understanding of health issues are prevalent among youth aged 15 to 24.20 Men should indeed play a critical role in lowering the burden of cervical cancer.16 Men can also help reduce the burden of cervical cancer by safeguarding their partners from HPV infections, inspiring them to get screened, and empowering them to protect themselves.21,22 WHO has made recommendations and urged men to be integrated into cervical cancer prevention efforts in the middle- and low-income countries.23 Men’s roles in prevention are direct and indirect, including avoiding cancer-causing chemicals, quitting smoking, restricting sexual partners, and safe coitus.24 Men’s involvement in cervical cancer prevention is critical, and men’s health behavior and attitudes are expected to be influenced by their disease awareness.25
Men have limited awareness of cervical cancer and are unconcerned about cervical cancer prevention.26 There is little research on male awareness of cervical cancer in women and why men are excluded from prevention initiatives worldwide.25 However, little is known about male participation in cervical cancer screening and treatment.16 However, there is little study on men’s awareness of cervical cancer.25 Only a few research looked at HPV-related knowledge in young male and female adults, and the results were mixed.27 According to several studies, most men are unaware of cervical cancer, and some men believe they are not accountable for cervical cancer in women.22,28 Men’s lack of knowledge about cervical cancer is risky because women are typically passive to males.29 Cervical cancer and human papillomavirus (HPV) awareness and knowledge are extremely low in Ethiopia.30 Health education initiatives are crucial for enhancing women’s knowledge and perspectives regarding cervical cancer, screening, and self-efficacy.31 Additionally, studies indicate that educational intervention has increased HPV knowledge.32
Furthermore, no study has been conducted in Ethiopia to assess men’s knowledge levels and educational interventions’ effectiveness among university students. This study aimed to explore educational intervention and the overall knowledge levels changes on HPV and cervical cancer awareness in male and female students from two campuses of the University of Gondar (UoG).
Methods
Study Design, Area, Source, and Study Participants
Institutional-based cross-sectional pre- and post-test comparative studies were conducted to understand the factors associated with HPV and cervical cancer awareness levels among male and female students from Tewodros and Maraki campuses of UoG.
Inclusion and Exclusion Criteria
All students enrolled in the regular programs aged 18 to 30 were included in the study.
Students enrolled in extension programs and aged below 18 and above 30 were excluded from the study.
Sample Size and Questionnaire
Sample Size Determination
The sample size was determined using the online tool of UCSF,33, to calculate the sample size required for before and after study, a two-tailed, 5% precision, 80% power, and effect size=0.5 and SDΔ=4.5, the sample size for the study was 638. G*Power ver3.1.9.7, for the McNemer test,34 a two-tailed, 1.5 effect size, α 0.05, 80% power, and 33% (based on pilot study) of the population changes due to the intervention, 604 participants needed to detect the effect and a finite population formula35 to determine the number of males and females required. The assumption was that 50% of the university students had sufficient knowledge of cervical cancer, 95% confidence interval, and 4% reliability. The sample size was determined as follows:

Where: n=the desired sample size
p=0.5 (expected minimum variability) and so, q=0.5
Zα1/2=critical value at 95% confidence level of certainty is=(1.96)
=[(1.96)2 (0.5)(0.5)]/(0.04)2=600.25=601,
Adding 5% non-response rate=31
The final sample size was N=601+31=632
(Applying finite population, N=11500 male (N=6900) female (N=4600) students enrolled into different programs at University of Gondar.)
The sample number of females:
=NTxA/N; =4600×631/11,500=252
The sample number of males:
=6900×630/11,500=378
The final sample size for the study was 638.
Questionnaire Development
The questionnaire was designed and developed based on study objectives, literature review (CDC, WHO), and pilot study. An initial pilot study was carried out at the college level, UoG, before the study was conducted in October–November 2018. The study was carried out using questionnaires consisting of six sections, including 53 items, both open- and close-ended questions in English and Amharic languages. The questionnaire was initially written in English and translated to Amharic and back to English to keep the questions’ consistent. Most students prefer to use the questionnaire in Amharic. The questionnaire was coded and had the same items and provided two different time intervals, before and after the interventions.
Study Variables
Socio-Demographic Variables
Age, sex, religion, year of study, the branch of study, CGPA, place of residence, father’s and mother’s educational qualifications and occupation, family size, family income.
Dependent Variables
Cervical cancer symptoms, risk factors, HPV, screening, vaccine.
Educational Intervention
The educational intervention was one time for a brief one-hour audio-visual-based presentation on cervical cancer symptoms, risk factors, HPV epidemiology, screening, and vaccination highlighting the STD nature of HPV transmission to the students, followed by 10-minute open discussion. Then, the post-test questionnaire was provided to the study participants to answer.
Sampling and Data Collection Procedure
The study was conducted on 638 undergraduate and postgraduate male (60%) and female (40%) students aged between 18 and 30 years. The study's aims and scope were posted on different official noticeboards and asked for voluntary participation. The study participants were chosen to use a simple random sampling technique and were enrolled using a multistage sampling technique. Information sheets and written informed consent were distributed randomly with a fixed number of questionnaires at a given time and venue. The sampling was repeated in different locations of the two campuses until the desired sample size, and ratio of male to female was achieved. Data were collected using a pretested questionnaire. Data collectors were trained laboratory technical staff to employ questionnaires on the selected study participants and collected the data.
Statistical Analysis
In the sample population, all variables of interest were summarized using descriptive statistics. For continuous variable age, means and standard deviations were generated. Knowledge levels of respondents regarding symptoms, risk factors, HPV and its relationship with cervical cancer, screening, and vaccination were measured using a 38-item instrument. A score of 1 was allotted for a good/correct answer and 0 for a wrong answer or “Do not know.” The maximum possible score was 38. The total score was divided into those scored above 19 or more were categorized as having good (“sufficient”) knowledge; the others were categorized as poor knowledge.
Proportions were compared by using the McNemar Chi2 test to determine the changes between pre- and post-intervention knowledge levels at 99% CI, p≤0.001 significance. The impact of socio-demographic characteristics on knowledge levels of cervical cancer was investigated using binary logistic regression. Finally, explanatory variables with a p-value less than 0.2 in the bivariate analysis were included in multivariate regression analyses to investigate factors that predict the correlation between baseline cervical cancer knowledge scores and changes in scores after the educational intervention. The odds ratio and 95% CI interval were used to assess the association’s existence and strength. All tests of significance were two-tailed at a 5% level. The reference category was the most common category of an independent variable (IV).
Ethical Considerations
Ethical clearance was obtained from the Institute of Biotechnology (EC No.: IoB/28/12/2018), University of Gondar, Gondar, Ethiopia. Enrolled students of eligible ages volunteered to participate, and a signed written consent form was included in the study. The study’s purpose and importance were explained to the participants before obtaining written informed consent, and the confidentiality of their identities was ensured. Data collectors were given one day of training on purpose, the study’s scope, and the study’s ethical aspects, such as maintaining the research’s confidentiality. The data from the questionnaire were processed anonymously by assigning random codes. During data collection, the confidentiality of the information was protected by omitting names or I.D. numbers from the questionnaire.
Results
Socio-Demographic Characteristics of the Study Participants
A total of 638 student participants attended pre- and post-intervention, with a 100% response rate. Of the total respondents, 384 (60.18%) were male (Table 1). The study participants ranged from 18 to 30 with a mean age of 21.07 (±SD, 1.96) years. More than 50% of study participants were from the Amhara region. The majority of the study's participants were Orthodox Christians (77.1%), undergraduates (95%), and never married. Nearly 50% (332) of participants’ CGPA was <2.5. More than 30% of the study participants’ father’s educational levels (215) and mother’s educational levels (212) were up to the primary level. Forty-two percent of students belonged to biological sciences. More than 90% of the respondent’s fathers had some occupation, while 54.7% of the participants were homemakers. Most of the participants’ 519 (81.3%) family income were <5000 birr.
 |
Table 1 Socio-Demographics of Male and Female University Students, N=638 |
Knowledge Levels of Study Participants About HPV and Cervical Cancer and McNemar’s Test of the Significance of Knowledge Levels Before and After Intervention
Responses to questions on selected domains before and after educational intervention are presented in Table 2. McNemar test determined a statistically significant difference in the proportion of HPV and cervical cancer awareness pre- and post-intervention at 99% CI, P≤0.001 significance level.
 |
Table 2 Awareness About Cervical Cancer and McNemar Test Before and After Educational Intervention at P≤0.001 Significance Level, N=638 |
Knowledge About the Symptoms of Cervical Cancer
Nine questions were asked about the symptoms (Table 2). Before, 174 (27.3%) students, and after the educational intervention, 581 (91.1%) reported that they had heard about cervical cancer. Vaginal bleeding after menopause could be a sign of cervical cancer? Before the intervention, only 47 (7.4%) students and 410 (64.3%) responded correctly after the educational intervention. However, more than sixty percent of the respondents, 392 (61.4%), did not know any symptoms associated with cervical cancer before the intervention. After the intervention, 3.4% of study respondents could not correctly respond to any cervical cancer symptoms.
Knowledge About Cervical Cancer’s Risk Factors
To study participants, nine questions were asked to assess knowledge about cervical cancer risk factors (Table 2). About 336 (57.4%) of study respondents had no idea about risk factors associated with the disease before the educational intervention, and only 36 (5.6%) students could not identify any of the risk factors even after the intervention. Before the intervention, 57 (8.9%) students responded that high parity could be a risk factor, and after the intervention, 283 (44.4%) could feel high parity could be a risk factor, and the least correctly responded question under the risk factor domain.
Knowledge About the HPV and Its Relationship with Cervical Cancer
Nine different questions like the causative organism, mode of transmission of HPV, and different diseases in males and females were asked to understand the knowledge levels before and after the educational intervention. Before the intervention, 81 (12.7%) of study respondents were aware of the STI nature of HPV, and 448 (70.2%) students responded correctly after intervention (Table 2). Before the intervention, only 23 (3.6%) and 27 (4.4%) were aware of anal and genital cancers before the intervention, respectively. On the other hand, HPV can cause anal cancers was the least correctly answered before (9.5%) and even after (20.8%) educational intervention. About 501 (78.5%) of study respondents had no idea about HPV and its association with the diseases before the educational intervention, and only 56 (8.8%) students could not know about HPV after the intervention.
Knowledge About the Screening of Cervical Cancer
There were four different questions asked about cervical cancer screening methods and their importance. Before the educational intervention, only 13.8% of total respondents were aware of screening, and 74.9% could respond correctly after the intervention (Table 2). About 465 (72.9%) of study respondents had no idea about screening before the educational intervention, and only 57 (8.9%) students could not answer after the intervention. Only 7.4% of respondents identified that the Pap smear test could pick up cell changes before and increased to 60% after the intervention.
Awareness Regarding HPV Vaccination
There were six different questions: availability of HPV vaccine for both girls and boys, vaccination age. Before the educational intervention, 10% of the participants heard about the HPV vaccine, and only 3% were aware of the vaccine available for males (Table 2). Five hundred and seven (79.5%) and 77 (12.1%) were unaware of any question on HPV vaccine before and after educational intervention, respectively.
Study Participants’ Awareness of Broad Categories of Cervical Cancer
McNemar test showed a change in the mean level of awareness on various broad categories of cervical cancer and HPV before and after intervention statistically significant at 99% CI, p≤0.001 (Table 3). After the intervention, there was more than five-fold increase in overall awareness of cervical cancer.
 |
Table 3 Mean Level of Awareness on Various Broad Categories of Cervical Cancer and McNemar Test Score at P≤0.001 Significance Level, N=638 |
Factors Associated with Cervical Cancer Knowledge Among Study Participants
Factors Associated with Pre-Intervention Cervical Cancer Knowledge Among Study Participants
The multivariate analysis showed that seven independent variables were significantly associated with base-level knowledge about different domains of cervical cancer: gender, year of study, age, parent’s educational level, CGPA, and family income (Table 4). However, no factor was statistically significant in the overall knowledge of cervical cancer. Base-level knowledge on symptoms, females nearly three times [AOR:2.57, 95% CI: (1.37–4.82)], third year and above [AOR:3.13, 95% CI: (1.3–7.43)], and family income 5000 and above [AOR:3.25, 95% CI: (1.04–10.16)] were more knowledgeable over other counterparts. Similarly, baseline awareness on cervical cancer risk factors, females [AOR:2.09, 95% CI: (1.37–3.19)], family income 5000 and above [AOR:4.33, 95% CI: (2.08–9.01)] were more knowledgeable over others and study participants mother’s education level: primary and below [AOR:2.43, 95% CI: (1.24–4.76)] were less knowledgeable over others. Knowledge level about HPV, age <21 years six times less knowledgeable [AOR:6.16, 95% CI: (2.21–17.18)] over higher age groups, and CGPA <2.5 were three times less knowledgeable [AOR:3.44, 95% CI: (1.515–7.81)] over higher CGPA. Similarly, the study participant’s father’s education level, primary and below, was nearly five times less [AOR:4.89, 95% CI: (1.79–13.37)] knowledgeable over higher education on screening. Vaccination knowledge and family income <5000 were nine times less informed [AOR:9.63, 95% CI: (2.2–42.13)] over higher income groups.
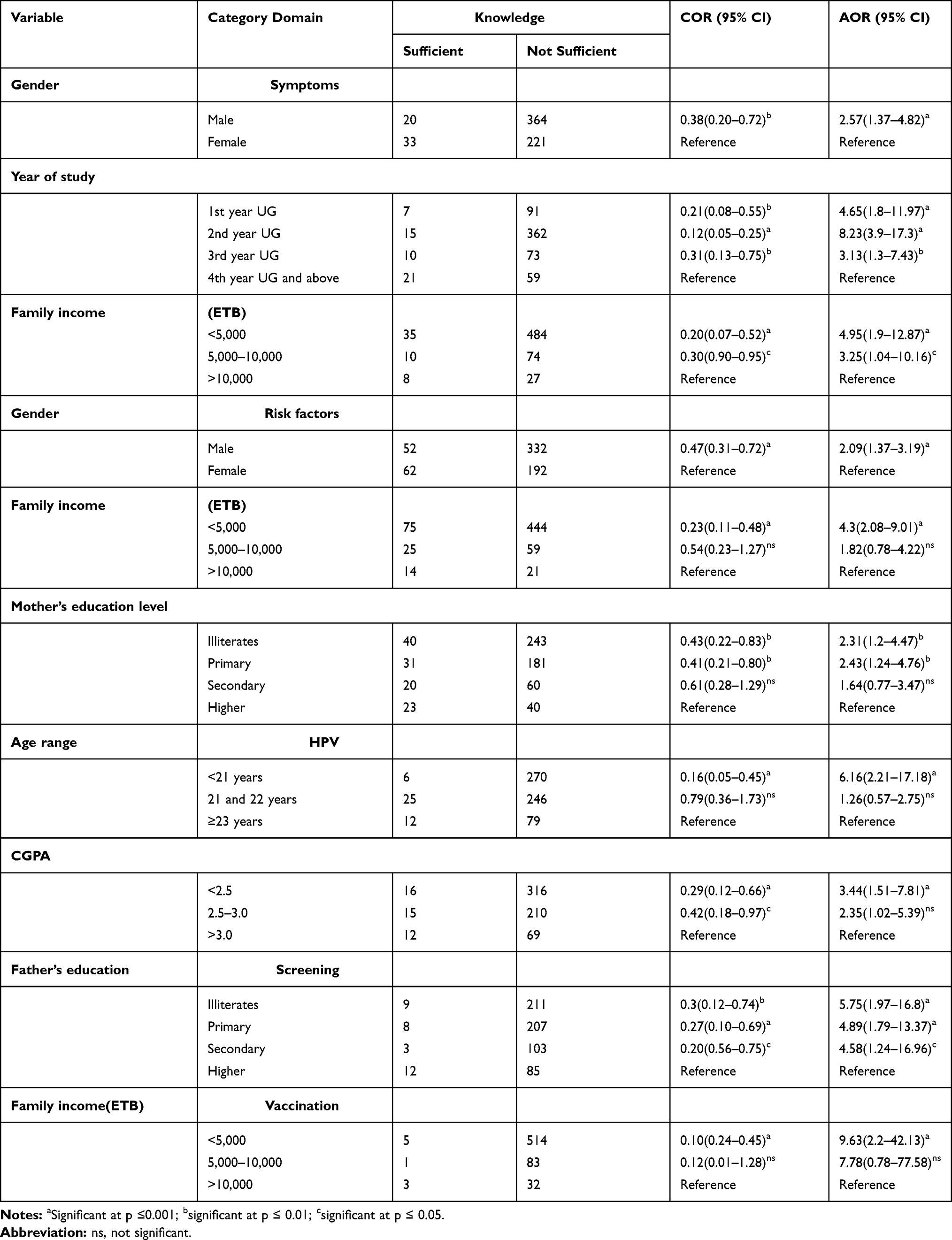 |
Table 4 Bi-Variable and Multi-Variable Logistic Regression Analysis of Potential Factors Associated with Cervical Cancer Knowledge Before Education Intervention, N=638 |
Factors Associated with Post-Intervention Cervical Cancer and HPV Knowledge Among Study Participants
The multivariate analysis showed that post-intervention overall knowledge and different domains of cervical cancer were under the influence of the year of study (Table 5). Overall cervical cancer knowledge was strongly associated with the year of study, area, and CGPA. Students from rural [AOR:1.75, 95% CI: (1.25–2.43)] over urban, year of study 1st-year students [AOR:0.27, 95% CI: (0.14–0.51)] over third years and above, CGPA2.5–3.0 [AOR:2.16, 95% CI: (1.13–4.13)] over higher were less knowledgeable. Knowledge on symptoms, age <21 years [AOR:0.5, 95% CI: (0.26–0.97)] over ≥23 years, year of study 1st-year students [AOR:0.34, 95% CI: (0.12–0.94)] over a third-year and higher, mother’s occupation employed [AOR:2.23, 95% CI: (1.08–4.59)] over homemaker were less knowledgeable.
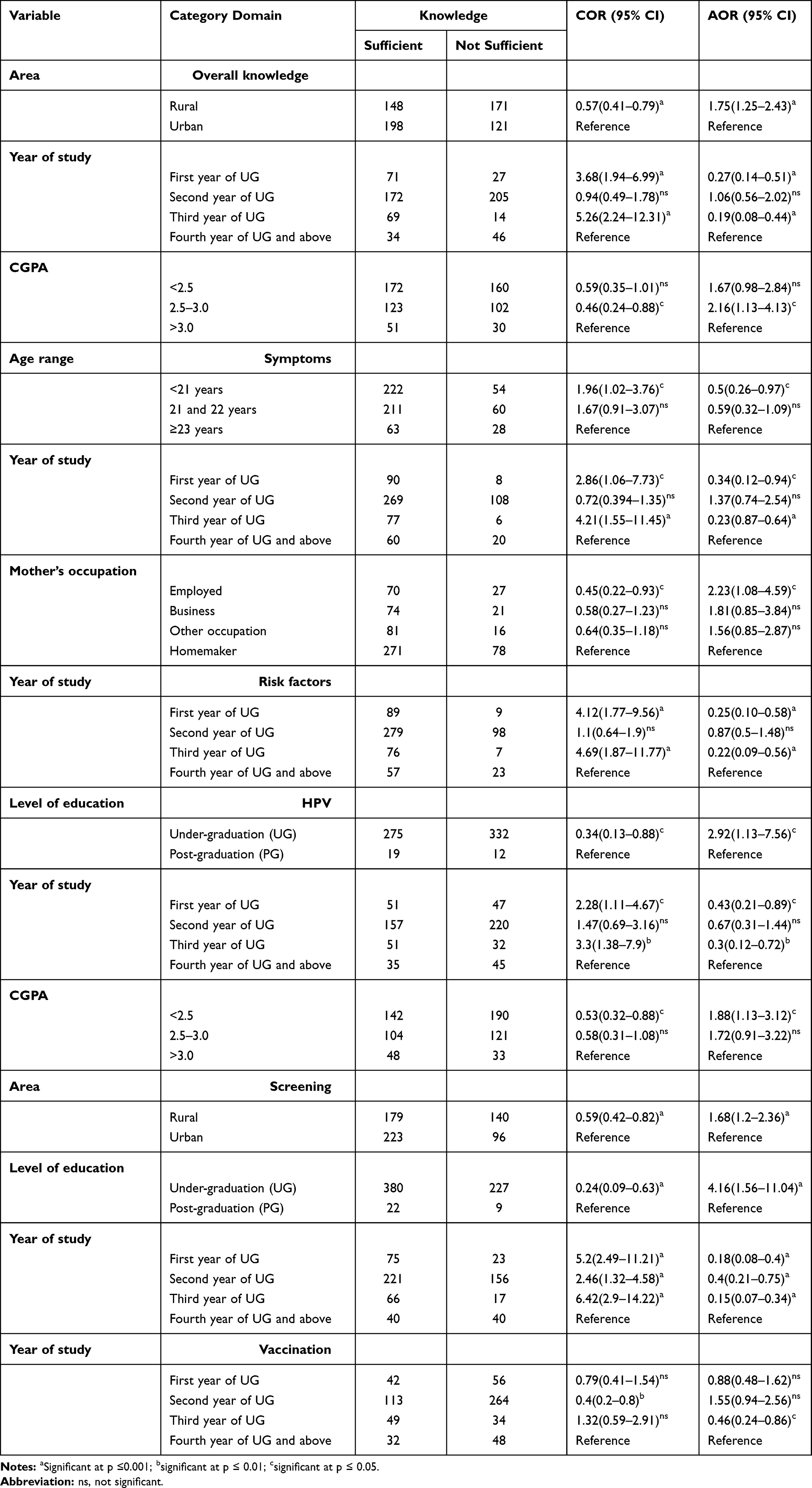 |
Table 5 Bi-Variable and Multi-Variable Logistic Regression Analysis of Potential Factors Associated with Cervical Cancer Knowledge After Educational Intervention, N=638 |
On risk factors, 1st year students [AOR:0.25, 95% CI: (0.10–0.58)] were less aware over second years and above. Similarly, knowledge of HPV was associated with level of education, year of study and CGPA. Undergraduates [AOR:2.92, 95% CI: (1.13–7.56)] over postgraduates,1st year students [AOR:0.43, 95% CI: (0.21–0.89)], CGPA<2.5 [AOR:1.88, 95% CI: (1.13–3.12)] were less knowledgeable over other counterparts. Knowledge on cervical cancer screening, rural [AOR:1.68, 95% CI: (1.2–2.36)], undergraduates [AOR:4.16, 95% CI: (1.56–11.04)], 2nd year students [AOR:0.4, 95% CI: (0.21–0.75)] were less knowledgeable over others. Knowledge on vaccination, 3rd year students [AOR:0.46, 95% CI: (0.24–0.86)] less knowledgeable over 4th year and above.
Discussion
The current study found that study participants lacked information about cervical cancer and the several domains examined. This finding is consistent with a comparable study conducted in Texas among medical and non-medical students.36
Several studies revealed that a brief educational intervention could improve college students’ overall understanding of cervical cancer and HPV, and similar findings have been reported in several intervention studies.32,36,37 In our study, adopting a theory-based educational intervention resulted in a fivefold increase in general knowledge about cervical cancer, symptoms, risk factors, HPV, screening, and vaccination, consistent with prior Jamaican studies.37 The majority of respondents lack awareness of the risk factors and symptoms of cervical cancer, HPV, and its vaccines. This corresponds to other research undertaken in Ghana.38 The discrepancy could result from information being disseminated via various mass media and the availability of screening programs in Ghana.38 After an intervention, despite considerable increases of 8.5% to 53% in the number of participants who believed cervical cancer was preventable, 47% still believed cervical cancer was not preventable. This observation is consistent with the research findings conducted in Jamaica.37
Before the educational intervention, 27.3% of students ever heard about cervical cancer. It is high compared to a study in Nigeria, 22.6%;39 however, it is very low compared to a study in Eastern Ethiopia that reported 50%.40 This difference could be different in study settings and the age of the study participants. Only 12.9% had base-level knowledge about vaginal bleeding after coitus could be a sign of cervical cancer, which is low compared to a study in India, 27%,41 very low compared to different studies reported.38,40 The baseline knowledge levels on vaginal bleeding between periods and foul-smelling vaginal discharge as a symptom of cervical cancer were lower than studies reported.38,41 After menopause, vaginal bleeding may be an indication of cervical cancer. Before the intervention, only 7.4% of students correctly responded; after the intervention, 64.3% of students correctly responded. This score is extremely low compared to a study conducted in Jamaica on women before and after intervention (50.3% vs 94.1%).37 This could be a difference in respondents’ gender and age.
Before the intervention, only 42.6% of research participants were aware of risk factors, which is low compared to a study conducted in Ghana, which found that 63.8% of participants were aware of cervical cancer risk factors.38 At the base level, 57.4% of study respondents did not know any risk factors. This score is lower than a study done in Eastern Ethiopia, 24.2%.40 At the base level, 25.7% of study participants knew that multiple sex partners could be a risk factor, which is higher than a study of 6%.41 This difference in awareness could be due to awareness of HIV education received as a part of the curriculum.
Before the intervention, 8.9% of students responded that high parity could be a risk factor, and it can be compared with a 12% awareness reported in a study.41 After the intervention, 44.4% of students indicated that high parity could be a risk factor; however, this score is extremely low compared to research conducted in Ghana,38 owing to the country’s cultural differences, and high parity is very common.
Before the intervention, students from biological sciences and in their fourth or higher year of study scored higher on knowledge levels than students majoring in non-biological sciences, a finding that corroborated studies done in New York and Mexico.32,42 Baseline knowledge levels were lower for the humanities stream than for the science stream, while the former show a larger gain in scores following the intervention; this can be compared with a study conducted in Texas after the intervention, non-physicians’ knowledge levels improved at par with physicians.36
Only 16.9% of research participants identified smoking as a risk factor, and first-year undergraduate students’ level of awareness was poor over others, a finding consistent with a study conducted in Brazil.43
In the present study, before the intervention, females had a better awareness of cervical cancer symptoms and risk factors than males. This observation is comparable to studies done in New York,32 Texas,36 Ghana,38 Mexico,42 and India,44 but there was little difference between male and female students on HPV-related questions and vaccination, consistent with another study.32 It reflected a trend in public education on sexually transmitted illnesses.
Only 13.5% of study participants were aware that HPV is the causative organism for cervical cancer and that HPV can infect males (4.5%), which is extremely low compared to a study conducted in the USA (58.2% and 55.2%, respectively).45 This study demonstrated that brief educational interventions focusing on HPV successfully increase HPV knowledge, similar to a study conducted with New York adolescents.32 After the intervention, knowledge about HPV was 5.6 times more than before (0.39), and a similar increase was made in a study conducted in Vietnam.46 Brief educational interventions focused on HPV may thus be helpful for primary prevention of all sexually transmitted illnesses, cervical cancer, and other HPV-related diseases.
Before the educational intervention, 12.7% of study respondents were aware of the STD nature of HPV infections, but most women and men lacked basic knowledge that HPV infection is sexually transmitted. This observation is consistent with a study conducted in Berlin,27 but is lower than in the USA (90%).47 The degree of information on HPV was higher for fourth-year students and above, PG students, and students with a higher CGPA and a similar discovery was made in a study in Mexico, where fourth-year health science students had a higher level of knowledge.42
Before the intervention, most participants in our study had never heard of cervical cancer screening and were unaware of the purpose of a Pap test, which contradicts the findings of a Jamaican study.37 Before the educational intervention, only 13.8% of total respondents were aware of screening, comparable with a study in Nigeria, 17.9%,39 however very lower than a study conducted in Eretria Medical students, 46%.48 The huge difference could be a difference in study participants. Before the intervention, 7.4% of study participants knew that the Pap smear test should be done as a screening test to detect cervical cancer early, and less than (27%) a study conducted in India.41 The current study’s findings are consistent with those of earlier intervention studies.37 Knowledge levels on screening were improved over base level and this finding. This observation may be that participants received adequate details about the screening during the education sessions.
Before the educational intervention, 10% of participants had heard of vaccines, only 3% were aware of male-specific vaccines, and 79.5% were unaware of HPV vaccines, comparable with a study conducted in Vietnam, which reported low levels of knowledge about HPV vaccination.46 Awareness and sufficient knowledge on screening and vaccination coupled with effective participation in screening and HPV vaccination, and such observation was reported in multiple studies, including a study conducted in Ghana.38
Following education, there was a rise in positive attitudes for receiving and recommending screening and vaccination. Both males and females showed a favorable attitude about obtaining or advocating HPV screening and vaccination after understanding that vaccines can protect against HPV. A similar observation was reported for the vaccine in a study conducted in India,44 Nigeria,49 and Jamaican investigations.37 Our findings suggest indicating that a theory-based educational intervention can help improve cervical cancer knowledge. Educational interventions can potentially eliminate barriers and elicit positive cervical cancer screening behavior, and these findings may aid future attempts to enhance cancer screening rates in similar low-resource settings. Mean knowledge scores increased dramatically from 4 to 23 following the presentation, regardless of gender, branch, age, and similar observation in a study conducted in Texas observation.36 The overall knowledge of study participants was 54.23% after the intervention, compared with a study in Ethiopia, 55.7%.40
In our study, young adults in their first year had a lower rate of knowledge acquisition following intervention than other age groups, and comparable findings of a study in Berlin, where students of class 11 or below were the least improvement on overall knowledge on HPV.27 All groups had poor baseline knowledge, with older participants scoring higher. A similar observation was made in another study in Texas.36 We observed a strong correlation between increasing age and increased HPV knowledge among study participants, analogous to a study conducted in India.44
On risk factors, first-year students [AOR:0.25, 95% CI: (0.10–0.58)] were less aware than second- and third-year students, which is consistent with a study in Brazil that found medical students up to their third year have lower knowledge levels [PR:0.6, 95% CI: (0.6: 0.7)] than fourth- and higher-year students.43 Franceschi et al reported similar findings in their investigation.50
Factor on risk variables, first-year students [AOR:0.25, 95% CI: (0.10–0.58)] were less conscientious than second- and third-year students. Education level was consistently connected with an increased understanding of cervical cancer.50 Third-year and above were knowledgeable before and after intervention [AOR:3.13, 95% CI: (1.3–7.43)], and a similar association between educational background (p=0.000) and knowledge level of the respondents reported in a community study in Ghana.51 A similar association was reported in a study conducted in Eretria.48
Study participants’ mother’s education level: primary and below [AOR:2.43, 95% CI: (1.24–4.76)] were less knowledgeable than others, and a similar association was reported in a study having an educational level above 12th (AOR: 12.11, 95% CI 4.57–32.09) were more knowledgeable.40 Knowledge level about HPV, age <21 years six times less knowledgeable [AOR:6.16, 95% CI: (2.21–17.18)] over higher age groups, and a similar association was reported in a study.48 After educational intervention, students from rural [AOR:1.68, 95% CI: (1.25–2.36)] were less knowledgeable over urban, and similar associations were reported (AOR=2.5, 95% CI: 1.1–5.7) in a study in Addis Ababa, Ethiopia,52 and Malaysia (OR: 1.96, 95% CI: 1.11–3.46).53 The factor associated with an increase in screening knowledge of the study participants was undergraduates [AOR:2.92, 95% CI: (1.13–7.56)] less improved over postgraduates, and a similar association was reported in a study.48
The factor associated with the increase in screening knowledge of the study participants was higher the year of study [AOR:0.15, 95% CI: (0.07–0.34)] are more knowledgeable and similar observation [OR=2.8, 95% CI: 1.1–7.8] reported in an Addis Ababa study in Ethiopia.52 3rd-year students [AOR:0.46, 95% CI: (0.24–0.86)] less knowledgeable on HPV vaccination over 4th year and above. Furthermore, a similar observation was reported in a study [OR: 1.19, 95% CI: 1.09–1.29].53
Limitation of the Study
This study may contain bias due to time and financial constraints. Due to the cross-sectional nature of the study, causal correlations are difficult to establish. Additionally, because the study included only students present on the sampling days, students with a high absence rate would be less likely to be included. The study’s participation was entirely voluntary. As a result, most participants may have indicated a higher level of interest in the subject. Finally, some participants may have had difficulty comprehending the questions because of their disparate educational backgrounds, contributing to possible bias. The students at UoG may not indicate students from other Ethiopian universities, as most students were from the Amhara region and were predominantly Orthodox Christians.
Strengths of the Study
To our knowledge, ours is the first study to understand the efficacy of an educational presentation on cervical cancer, HPV knowledge, and vaccination among Ethiopian male and female university students.
In Ethiopia, research on male awareness of cervical cancer and HPV has been limited to healthcare personnel, and to our knowledge, this is the first study that focuses on male university students. A phased educational intervention enabled this instructional tool to reach a sizable number of students and assess their knowledge before and after the lecture. While we saw a significant increase in general knowledge among study participants immediately following the intervention, we do not know how well the information was retained over time. As one of the first studies to examine the effect of educational intervention on cervical cancer and HPV knowledge, and given the paucity of research on HPV knowledge in male and female students of Ethiopian universities, this study provides critical information for clinicians, educators, and policymakers. This study is expected to provide critical information on HPV health education and the importance of including males to grasp Ethiopia’s disease burden fully.
Our findings suggest that more inputs are needed to educate the general public, particularly women, about cervical cancer symptoms because early detection of symptoms can prompt medical treatment, leading to a better prognosis and lower death rates. It is critical to guarantee that cervical cancer screening facilities are available in all health centers and the required immunization implementation is reachable. In theory, increasing positive attitudes toward cervical cancer screening and HPV vaccines and behavioral changes would significantly impact cervical cancer prevention in Ethiopia. This educational intervention improves women’s knowledge and encourages men to reduce illness burden in low-resource settings in countries like Ethiopia.
Conclusion
Before the intervention, awareness was associated with gender and age, and after the intervention, more than four folds increased knowledge on cervical cancer and HPV, and the year of study was the key factor associated with overall improvement. This study suggests that educational intervention effectively strengthens our understanding of the risk factors for spreading HPV and cervical cancer disease. The present study illustrates the need for extra educational interventions to better inform students with disparate educational backgrounds. Finally, planned lectures on cervical cancer and HPV might help university students learn more about these topics. Future research into the effectiveness of this form of educational intervention on cervical cancer screening and HPV vaccine uptake will shed more light on its efficacy.
Data Sharing Statement
The datasets used to support the findings of this study are available on reasonable request. All relevant data are within the manuscript.
Acknowledgment
We want to thank our study participants and data collectors. We also thank the Institute of Biotechnology, University of Gondar, Gondar, Ethiopia, for its invaluable support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no specific funding for this study.
Disclosure
There is no conflict of interest regarding this paper.
References
1. Satterwhite CL, Torrone E, Meites E, et al. Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008. Sex Transm Dis. 2013;40(3):187–193. doi:10.1097/OLQ.0b013e318286bb53
2. WHO. Human Papillomavirus (HPV) and cervical cancer. Available from: https://www.who.int/newsroom/fact-sheets/detail/human-papillomavirus-(hpv)-and-cervical-cancer.
3. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2014. Atlanta: U.S. Department of Health and Human Services; 2015. Available from: https://www.cdc.gov/std/stats/archive/surv-2014-print.PDF.
4. Forman D, de Martel C, Lacey CJ, et al. Global burden of human papillomavirus and related diseases. Vaccine. 2012;30(Suppl 5):F12–F23. PMID: 23199955. doi:10.1016/j.vaccine.2012.07.055
5. Bosch FX, de Sanjosé S. Chapter 1: human papillomavirus and cervical cancer--burden and assessment of causality. J Natl Cancer Inst Monogr. 2003;2003(31):3–13. doi:10.1093/oxfordjournals.jncimonographs.a003479
6. Serrano B, Brotons M, Bosch FX, Bruni L. Epidemiology and burden of HPV-related disease. Best Pract Res Clin Obstet Gynaecol. 2018;47:14–26. doi:10.1016/j.bpobgyn.2017.08.006
7. Castellsagué X, Bosch FX, Muñoz N, et al. Male circumcision, penile human papillomavirus infection, and cervical cancer in female partners. N Engl J Med. 2002;346(15):1105–1112. doi:10.1056/NEJMoa011688
8. Baseman JG, Koutsky LA. The epidemiology of human papillomavirus infections. J Clin Virol. 2005;32(Suppl 1):S16–S24. doi:10.1016/j.jcv.2004.12.008
9. Chaturvedi AK. Beyond cervical cancer: burden of other HPV-related cancers among men and women. J Adolesc Health. 2010;46(4):S20–S26. doi:10.1016/j.jadohealth.2010.01.016
10. Human papillomaviruses. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Vol. 64. Lyons, France: International Agency for Research on Cancer; 1995. Available from: https://publications.iarc.fr/Book-And-Report-Series/Iarc-Monographs-On-The-Identification-Of-Carcinogenic-Hazards-To-Humans/Human-Papillomaviruses-1995.
11. Melbye M, Frisch M. The role of human papillomaviruses in anogenital cancers. Semin Cancer Biol. 1998;8(4):307–313. doi:10.1006/scbi.1998.0081
12. Koutsky L. Epidemiology of genital human papillomavirus infection. Am J Med. 1997;102(5):3–8. doi:10.1016/s0002-9343(97)00177-0
13. Schiffman M, Castle PE. The promise of global cervical-cancer prevention. N Engl J Med. 2005;353(20):2101–2104. doi:10.1056/NEJMp058171
14. Giuliano AR, Lee JH, Fulp W, et al. Incidence and clearance of genital human papillomavirus infection in men (HIM): a cohort study [published correction appears in Lancet. 2011 Jun 11;377(9782):2006]. Lancet. 2011;377(9769):932–940. doi:10.1016/S0140-6736(10)62342-2
15. National Cancer Information Center. Type of Cancers: Uterine cervical Cancer [Internet]. Ilsan: National Cancer InformationCenter; 2015. Available from: https://www.cancer.go.kr/lay1/S1T639C641/contents.do.
16. Binka C, Doku DT, Nyarko SH, AwusaboAsare K. Male support for cervical cancer screening and treatment in rural Ghana. PLoS One. 2019;14(11):e0224692. doi:10.1371/journal.pone.0224692
17. Human papillomavirus and related diseases report; 2019. Available from: https://hpvcentre.net/statistics/reports/ETH.pdf.
18. Mapanga W, Girdler-Brown B, Singh E. Knowledge, attitudes and practices of young people in Zimbabwe on cervical cancer and HPV, current screening methods and vaccination. BMC Cancer. 2019;19(1):845. doi:10.1186/s12885-019-6060-z
19. Klug SJ, Hukelmann M, Blettner M. Knowledge about infection with human papillomavirus: a systematic review. Prev Med. 2008;46(2):87–98. doi:10.1016/j.ypmed.2007.09.003
20. Schaefer R, Gregson S, Eaton JW, et al. Age-disparate relationships and HIV incidence in adolescent girls and young women: evidence from Zimbabwe. AIDS. 2017;31(10):1461–1470. doi:10.1097/QAD.0000000000001506
21. Castellsagué X, Bosch FX, Muñoz N. The male role in cervical cancer. Salud Publica Mex. 2003;45(Suppl 3):S345–S353. doi:10.1590/s0036-36342003000900008
22. Maree JE, Wright SCD, Makua TP. Men’s lack of knowledge adds to the cervical cancer burden in South Africa. Eur J Cancer Care. 2011;20:662–668. doi:10.1111/j.1365-2354.2011.01250.x
23. World Health Organization. Comprehensive Cervical Cancer Control: A Guide to Essential Practice. Geneva; 2006. Available from: http://www.who.int/reproductivehealth/publications/cancers/9241547006/en/.
24. World Health Organization. Practice sheet 3.3: what men need to know to help prevent cervical cancer. In: Comprehensive Cervical Cancer Control: A Guide to Essential Practice.
25. Kim HW, Kim DH, Kim Y. Men’s awareness of cervical cancer: a qualitative study. BMC Womens Health. 2018;18(1):155. doi:10.1186/s12905-018-0650-9
26. Kim HW. Comparison of factors associated with intention to receive human papillomavirus vaccine between male and female undergraduate students. Korean J Women Health Nurs. 2011;17(4):415–425. doi:10.4069/kjwhn.2011.17.4.415
27. Blödt S, Holmberg C, Müller-Nordhorn J, Rieckmann N. Human papillomavirus awareness, knowledge and vaccine acceptance: a survey among 18–25 year old male and female vocational school students in Berlin, Germany. Eur J Public Health. 2012;22(6):808–813. doi:10.1093/eurpub/ckr188
28. Williams MS, Amoateng P. Knowledge and beliefs about cervical cancer screening among men in Kumasi, Ghana. Ghana Med J. 2012;46(3):147–151.
29. Denny L, Quinn M, Sankaranarayanan R. Chapter 8: screening for cervical cancer in developing countries. Vaccine. 2006;24(Suppl 3):
30. Anorlu RI. Cervical cancer: the sub-Saharan African perspective. Reprod Health Matters. 2008;16(32):41–49. doi:10.1016/S0968-8080(08)32415-X
31. Ebu NI, Mupepi SC, Siakwa MP, Sampselle CM. Knowledge, practice, and barriers toward cervical cancer screening in Elmina, Southern Ghana. Int J Womens Health. 2014;7:31–39. doi:10.2147/IJWH.S71797
32. Lambert EC. College students’ knowledge of human papillomavirus and effectiveness of a brief educational intervention. J Am Board Fam Pract. 2001;14(3):178–183.
33. Chow S-C, Shao J, Wang H. Sample Size Calculations in Clinical Research.
34. Faul F, Erdfelder E, Lang A-G, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. doi:10.3758/BF03193146
35. Underhill L, Bradfield D. Intro STAT.
36. Berenson AB, Rahman M, Hirth JM, Rupp RE, Sarpong KO. A brief educational intervention increases providers’ human papillomavirus vaccine knowledge. Hum Vaccin Immunother. 2015;11(6):1331–1336. doi:10.1080/21645515.2015.1022691
37. Coronado Interis E, Anakwenze CP, Aung M, Jolly PE. Increasing cervical cancer awareness and screening in Jamaica: effectiveness of a theory-based educational intervention. Int J Environ Res Public Health. 2015;13(1):ijerph13010053. doi:10.3390/ijerph13010053
38. Drokow EK, Zi L, Han Q, et al. Awareness of cervical cancer and attitude toward human papillomavirus and its vaccine among Ghanaians. Front Oncol. 2020;10:1651. doi:10.3389/fonc.2020.01651
39. Abiodun AB, Oluwasola TA, Durodola AO, Ajani MA, Abiodun AD, Adeomi AA. Awareness and perception of risk for cervical cancer among women in Ogbomoso, Nigeria. Trop J Obstet Gynaecol. 2017;34:218–223. doi:10.4103/TJOG.TJOG_56_16
40. Wakwoya EB, Gemechu KS, Dasa TT. Knowledge of cervical cancer and associated factors among women attending public health facilities in Eastern Ethiopia. Cancer Manag Res. 2020;12:10103–10111. doi:10.2147/CMAR.S262314
41. Singh S, Narayan N, Sinha R, Sinha P, Sinha VP, Upadhye JJ. Awareness about cervical cancer risk factors and symptoms. Int J Reprod Contracept Obstet Gynecol. 2018;7(12):4987–4991. doi:10.18203/2320-1770.ijrcog20184953
42. Vogtmann E, Harlow SD, Valdez AC, Valdez JC, Ponce EL. HPV knowledge in Mexican college students: implications for intervention programmes. Health Soc Care Community. 2011;19(2):148–157. doi:10.1111/j.1365-2524.2010.00954.x
43. Costa A, Gomes JM, Germani ACCG, et al. Knowledge gaps and acquisition about HPV and its vaccine among Brazilian medical students. PLoS One. 2020;15(3):e0230058. doi:10.1371/journal.pone.0230058
44. Rashid S, Labani S, Das BC, Natarajaseenivasan K. Knowledge, awareness and attitude on HPV, HPV vaccine and cervical cancer among the college students in India. PLoS One. 2016;11(11):e0166713. doi:10.1371/journal.pone.0166713
45. Katz ML, Krieger JL, Roberto AJ. Human papillomavirus (HPV): college male’s knowledge, perceived risk, sources of information, vaccine barriers and communication. J Mens Health. 2011;8(3):175–184. doi:10.1016/j.jomh.2011.04.002
46. Minh DN, Nutta T, Richard H. Effectiveness of a health talk education program on Human Papillomavirus (HPV) knowledge, attitudes, and intentions to vaccinate children among mothers of secondary school boys in Thua Thien Hue Province, Vietnam. Risk Manag Healthc Policy. 2020;13:1207–1214. doi:10.2147/RMHP.S259097
47. Barnard M, George P, Perryman ML, Wolff LA, De Groot AS. Human papillomavirus (HPV) vaccine knowledge, attitudes, and uptake in college students: implications from the precaution adoption process model. PLoS One. 2017;12(8):e0182266. doi:10.1371/journal.pone.0182266
48. Mekonen Y, Berhe H, Ghebreab L, Teages E. Factors associated with knowledge, attitude and practice of cervical cancer and its screening (Pap smear) among female students of Orotta College of medicine and health sciences in Eritrea: a cross sectional study. MOJ Womens Health. 2021;10(3):
49. Abiodun OA, Olu-Abiodun OO, Sotunsa JO, Oluwole FA. Impact of health education intervention on knowledge and perception of cervical cancer and cervical screening uptake among adult women in rural communities in Nigeria. BMC Public Health. 2014;14(1):814. doi:10.1186/1471-2458-14-814
50. Franceschi S, Plummer M, Clifford G, et al. Differences in the risk of cervical cancer and human papillomavirus infection by education level. Br J Cancer. 2009;101(5):865–870. doi:10.1038/sj.bjc.6605224
51. Ampofo AG, Isaac N, Bukola MI, et al. The level of knowledge and associated socio-demographic factors on cervical cancer among women: a cross-sectional study at Kenyase Bosore community, Ghana. Pan Afr Med J. 2019;34:44. doi:10.11604/pamj.2019.34.44.19471
52. Gelibo T, Roets L, Getachew T, Bekele A. Coverage and factors associated with cervical cancer screening: results from a population-based WHO Steps Study in Ethiopia. J Oncol Res Treat. 2017;2:115.
53. Syafiq T, Norzaher I, Siti NM, Shamsul AS. A systematic review on factors associated with cervical cancer screening among immigrant women. Int J Public Health Clin Sci. 2019;6:1. e-ISSN: 2289-7577.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.