Back to Journals » Infection and Drug Resistance » Volume 19
Factors Associated with Parental Involvement in Efforts to Prevent Drug-Resistant Tuberculosis in Children: A Scoping Review
Authors Rhamelani P ![]() , Rakhmawati W
, Rakhmawati W ![]() , Fitri SYR
, Fitri SYR ![]() , Mujar NMM
, Mujar NMM
Received 9 October 2025
Accepted for publication 23 January 2026
Published 7 February 2026 Volume 2026:19 573094
DOI https://doi.org/10.2147/IDR.S573094
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Putri Rhamelani,1,* Windy Rakhmawati,2,* Siti Yuyun Rahayu Fitri,2,* Noor Mastura Mohd Mujar3,*
1Master of Nursing Program, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Department of Pediatric Nursing, Faculty of Nursing, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Community Health, Cancer Research and Specialist Centre, Universiti Sains Malaysia, Kepala Batas, Penang, Malaysia
*These authors contributed equally to this work
Correspondence: Windy Rakhmawati, Email [email protected]
Abstract: Drug-Resistant Tuberculosis (DR-TB) in children remains highly prevalent and requires long-term treatment. Parental involvement is crucial in preventing DR-TB in children, but often faces various challenges. This review aims to describe and analyze research on factors related to parental involvement in DR-TB prevention efforts in children. This study used a scoping review design following the JBI scoping review guidelines. The literature search used five primary databases, including PubMed, ScienceDirect, Scopus, Sage Journals, and Taylor & Francis. Inclusion criteria included articles focusing on parental involvement in DR-TB prevention in children and its factors, written in English, original research, and published between 2010 and 2025. Exclusion criteria included review articles and research protocols. Based on the results of the literature review, we analyzed 14 relevant articles. Efforts to prevent DR-TB in children include preventing exposure to DR-TB in children in the household and preventing active TB treatment failure in children. There are various factors related to parental involvement through DR-TB preventive therapy in children as a representation of emotional support (stigma, support from health workers, concerns, family openness), instrumental or logistical (logistical burden factors, economic, concurrent treatment with parents, side effects), informational (level of knowledge, level of awareness), and appraisal (trust in the health system). Meanwhile, parental involvement in efforts to provide TB treatment to children represents emotional support (stigma factors, psychosocial burden, attitudes of health workers, concerns, motivation, community support, child gender), instrumental or logistical (factors of access to health services, economic, difficulty administering drugs, age and gender of parents, drug side effects, child age, ability to provide nutritious food, child character), informational (educational factors, education level, knowledge level), and appraisal (trust in health services). These findings suggest that strengthening parental support through tailored health education, counseling, and close collaboration with health workers is crucial to prevent DR-TB in children.
Keywords: associated factors, childhood tuberculosis, drug-resistant tuberculosis prevention, parental involvement
Introduction
Tuberculosis (TB) is an infectious disease caused by Mycobacterium tuberculosis and is the second leading cause of death in the world. The latest data from the World Health Organization (WHO) shows that the population of children experiencing TB is 12% of the 10.8 million people diagnosed with TB in 2023.1 World Health Organization (WHO) data in 2023 also shows that there are as many as 410,000 people experiencing resistance to rifampicin (RR) and multidrug resistance (MDR).2 Every year there are 25,000–32,000 children under 15 years old who experience DR-TB where DR-TB treatment takes longer and has many challenges.2 This is shown from the report in the 2018–2022 period, only 21,600 children underwent DR-TB treatment, while the target was 115,000 children.2 The Tuberculosis Inventory Study Report from the Ministry of Health in 2023–2024 shows that the second-ranked TB burden countries in the world in 2022 is Indonesia, and contributes more than two-thirds of TB cases globally in 2022.3
The cause of DR-TB is Mycobacterium tuberculosis infection that is resistant to rifampicin and/or isoniazid due to inadequate TB treatment or direct transmission of DR-TB from patient to child. Therefore, the main risk factors for DR-TB in children include non-adherence to treatment and high exposure to DR-TB contacts from adults to children in the home environment.4 Increased adherence to TB treatment goes hand in hand with family support during the child’s treatment.5 The level of adherence to TB treatment in children is known to be more complex because they still depend on parents to take their medication.6 Families, especially parents, are the most involved in supporting TB care to prevent DR-TB in children compared to other social groups. Meanwhile, as many as 65% of children under 5 years of age are at high risk of contracting TB, including DR-TB.4 This is due to the immaturity of the immune system and the high intensity of interaction between children and their parents.
However, parental involvement in child care is often suboptimal. Parental involvement in DR-TB prevention efforts in children faces various challenges. Regarding DR-TB prevention in children who are in close contact with DR-TB sufferers in the household, challenges for parents to actively engage include stigma, catastrophic costs associated with treatment, psychological distress, health system barriers, and other social, economic, and psychological barriers.7,8 Meanwhile, parental involvement in adherence to childhood TB treatment also faces obstacles, including forgetting doses, having other activities, changes in routine, and child refusal.9 Children’s refusal to take medication is an emotional reaction to the bitter taste of the medication and the long duration of treatment, which is also another challenge. These various obstacles can increase the risk of treatment failure and contribute to the development of DR-TB in children.
TB disease has a detrimental impact on children’s health. TB in children has unique impacts compared to TB in adults, including poor lung function, lower growth and development status, and even death.10 Children will face even greater impacts if they experience DR-TB because treatment requires regular injections, a higher pill load, additional side effects, and a longer treatment duration.11,12 Even in the management of DR-TB requires close consultation with disease experts and more active parental involvement during monitoring the therapy phase, side effects, and complications.13 Given the severity of these impacts, preventing DR-TB in children requires more attention from both parents and health workers. Effective strategies in TB treatment need to be optimized so that children with TB can recover completely and do not progress to DR-TB.
Children are still dependent on their parents and require a special approach in TB care as a preventative measure for DR-TB.14 The scope of parents’ role in preventing DR-TB in children includes preventing children from being exposed to DR-TB from adult DR-TB sufferers in the household and prevention through successful treatment of active TB in children. Irregular or interrupted treatment can cause children to develop drug resistance.13 Both require active parental involvement and optimal collaboration between parents and health workers. WHO has recommended parental involvement in TB care in children as a holistic approach because it can ensure compliance and successful treatment in children as a preventative measure for DR-TB.15
Although parental involvement is important, previous research has shown that parental involvement is considered less than optimal in treatment due to minimal awareness and knowledge.16,17 Approximately 67% of parents of children with TB are not well involved in their child’s care.18 This has a negative impact on the level of child compliance, which is one of the causes of DR-TB. The level of compliance and success of TB treatment is still relatively low,19 with 74.4% of 82 children showing non-compliance.20 Another study showed that only 16.9% of children were compliant in TB treatment.21 Therefore, prevention of DR-TB exposure and childhood TB care need to be optimized to prevent TB drug resistance in children.
Optimal home-based TB care for children by parents is a public health priority. However, parental involvement in TB care to prevent DR-TB in children still faces various challenges related to the complexity of parental behavior.22 In general, this is influenced by internal factors, such as treatment duration, drug side effects, or disease awareness, as well as external factors, such as stigma or psychosocial support.23,24 Currently, the TB elimination program by 2030 has been launched by the government, especially in Indonesia, to address the high mortality rate from TB, including in children. This effort is in line with efforts to prevent DR-TB in children and the WHO strategy, namely End TB Strategies, which includes TB prevention, monitoring, and treatment.
These various efforts can increase TB recovery rates and prevent DR-TB in children. However, their implementation has not been optimal because several key challenges to parent involvement have not been addressed. The challenges faced by every parent who wants to be actively involved are certainly based on various factors related to parental involvement. These factors need to be properly identified to create effective solutions to increase parental involvement in DR-TB prevention efforts in children. Nurses have a strategic role in increasing parental involvement in effective DR-TB prevention in children for families.25
Although parental involvement is crucial for successful TB treatment in children, which is also crucial for preventing DR-TB, current research has not addressed the factors associated with parental involvement, specifically focusing on DR-TB prevention efforts in the pediatric population. Most existing studies have focused on treatment adherence in TB patients broadly, with limited attention to the unique challenges faced by parents in supporting children with TB. To date, no scoping review has systematically mapped the factors associated with parental involvement in pediatric DR-TB prevention.
This review not only identifies and maps the factors underlying parental involvement but also provides new insights into these factors by integrating fragmented evidence across behavioral, social, and health systems research. It describes how multidimensional factors interact to influence parental involvement in DR-TB prevention. Furthermore, it identifies critical evidence gaps in parental involvement, health system support, and sociocultural determinants that have been underexplored in previous research. This is a crucial gap, given the central role of parents in ensuring treatment adherence and preventing resistance in children. Therefore, this review aims to describe and analyze previous studies on factors related to parental involvement in preventing DR-TB in children through preventing DR-TB exposure and TB treatment care. The question of this review is “What are the factors related to parental involvement in efforts to prevent DR-TB in children?”. The results of this review are expected to be a reference for health workers and parents in evaluating and improving all factors asscociated suboptimal parental involvement in preventing DR-TB in children.
Materials and Methods
Study Design
This study uses a scoping review research design that maps various relevant research findings.26 This review was conducted based on the JBI methodology and using the writing guidelines from the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR).27 The article review process is carried out through various stages including identifying research questions, formulating keywords for the article search process, determining inclusion and exclusion criteria, identifying various sources of information, selecting relevant literature that meets the criteria, extracting and mapping results from selected articles, and compiling a report on the results of the article analysis.
Eligibility Criteria
The research questions and eligibility criteria in this review use the PCC (Population, Concept, Context) approach as follows:
P (Population): parents, children with TB, and children exposed to DR-TB
C (Concept): parental involvement and its factors
C (Context): prevention of DR-TB in children
In the article search process, the author applied selection criteria consisting of inclusion and exclusion criteria. Inclusion criteria for the population included articles with subjects of parents who have children with TB and parents of children exposed to DR-TB in the household; for the concept included articles that focused on discussing parental involvement and its factors; for the context included articles on parental involvement in efforts to prevent DR-TB in children; and for the source type included articles in English, original research, and publication years 2010–2025. This review focused on English-language articles to minimize the risk of translation inaccuracies that could impact the analysis and interpretation of the articles. Exclusion criteria included articles with review studies and research protocols. This literature review includes a publication year limitation starting from 2010 because in that year WHO began to pay global attention to DR-TB in the pediatric.
Data Collection
Search Strategy
Based on the JBI methodology, there are three stages of the search strategy. In the first stage, researchers conducted an initial search limited to three databases (PubMed, Scopus, and ScienceDirect). In the second stage, researchers conducted a keyword search across all available databases. Each keyword was expanded using MeSH (Medical Subject Headings) terms and synonyms to find potentially all relevant articles using the Boolean operators “AND” and “OR” on each syllable. The literature used in this review was obtained from five primary databases: PubMed, ScienceDirect, Scopus, Sage Journals, and Taylor & Francis.
The resulting inclusion and exclusion criteria were applied to the article search process. The authors used structured queries and specific search parameters to search literature databases such as Scopus and PubMed, as well as publisher platforms such as Sage Journals, ScienceDirect, and Taylor & Francis. All found articles were analyzed and their titles and abstracts screened for relevance to the research objectives. In the third stage, researchers conducted a bibliography search of the found articles for additional references.
Study Selection and Quality Appraisal
After the literature search, all articles found were selected by applying the established inclusion and exclusion criteria. The literature selection in this review is presented in the PRISMA-ScR flowchart (Figure 1).28 The literature selection process was carried out by eliminating duplicate articles and articles that did not meet the inclusion criteria for this review. All articles obtained from the databases used were screened through title, abstract, and full-text review to ensure they were relevant to the focus of this review. Articles that did not meet the inclusion criteria were excluded. After the literature selection process was completed, the authors conducted a thorough analysis of each article. Although a scoping review does not require a critical assessment of the included studies, such assessments are included in this review to provide additional context regarding the methodological rigor and credibility of the reviewed studies. The authors used the Joanna Briggs Institute (JBI) critical assessment checklist to assess the eligibility and credibility of each article.
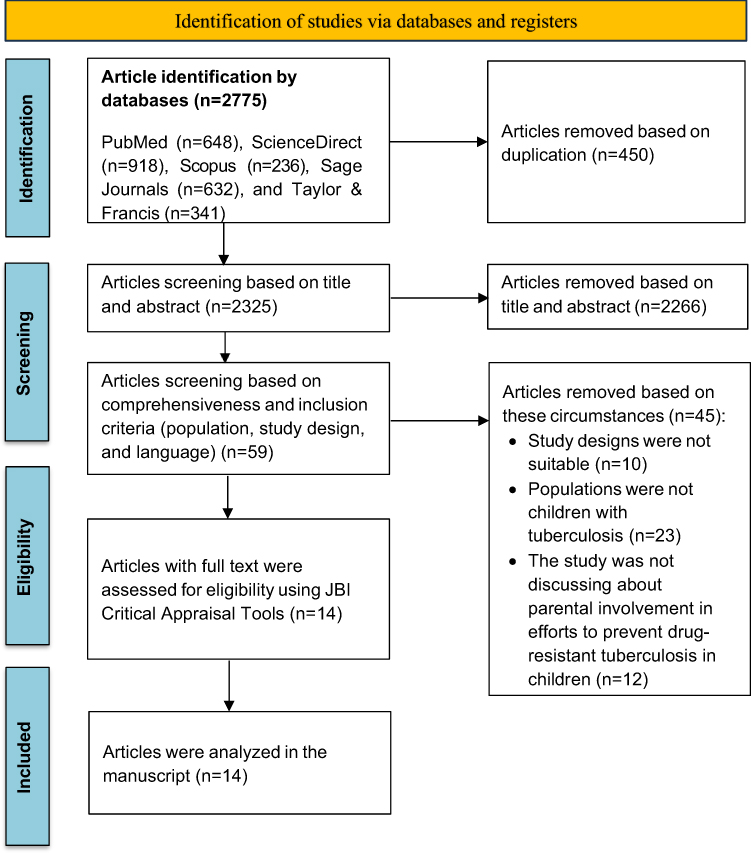 |
Figure 1 PRISMA Flowchart. Bolded text denotes the key stages of the scoping review process and major headings describing the identification, screening, eligibility assessment, and inclusion of studies. This heading represents the initial literature search conducted across electronic databases. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372: n71. Creative Commons.29. |
The JBI critical assessment checklist consisted of 10 questions for articles with qualitative study designs, 8 questions for articles with quantitative cross-sectional study designs, and 11 questions for articles with prospective and longitudinal observational studies.30 Each critical assessment question had four answer options: “yes”, “no”, “not applicable”, and “unclear.” The authors calculated the critical assessment score by dividing the number of “yes” answers by the total number of “unclear”, “no,” and “yes” answers. The “not applicable” answer was excluded from the calculation. Articles with a JBI score of less than 70% were eliminated from the review process. If discrepancies were found during the selection process, all authors reviewed the articles to make a joint decision. During the review process, no disagreements were found regarding the suitability of the selected studies.
Data Extraction and Analysis
In this study, the authors analyzed 14 articles. The article extraction and analysis process in this review used a matrix table that included the author’s name, year of article, country, research objective, research sample, research method, parental involvement (domain or area of parental involvement, type of parental involvement, related factors), and research results. All articles reviewed in this study were primary studies consisting of qualitative study designs, quantitative cross-sectional studies, prospective studies, and observational longitudinal studies. This review ensured that all reviewed research articles supported the review’s objective of exploring various factors related to or influencing parental involvement in DR-TB prevention efforts in children.
The author analyzed the data through an identification process, and then presented all data obtained from the articles in a matrix table The data for each finding was then analyzed and interpreted based on the areas and types of parental involvement in DR-TB prevention efforts in children. The author mapped each parental involvement factor found in the reviewed research articles into the types of parental involvement, including emotional support, instrumental or logistical support, informational support, and appraisal support.
Results
Study Selection
The initial literature search process was conducted by identifying articles from several databases, resulting in a total of 2,775 articles. All articles were then screened based on duplicate articles, titles, and abstracts, leaving 59 articles. Further selection was carried out by the author using inclusion criteria, resulting in 14 articles to be assessed for quality using the JBI critical assessment checklist. Based on the JBI assessment results, 14 articles were of good quality with a JBI score of more than 70%, allowing for further analysis in this review (Table 1). The article selection process is explained visually using a PRISMA flow diagram (Figure 1).
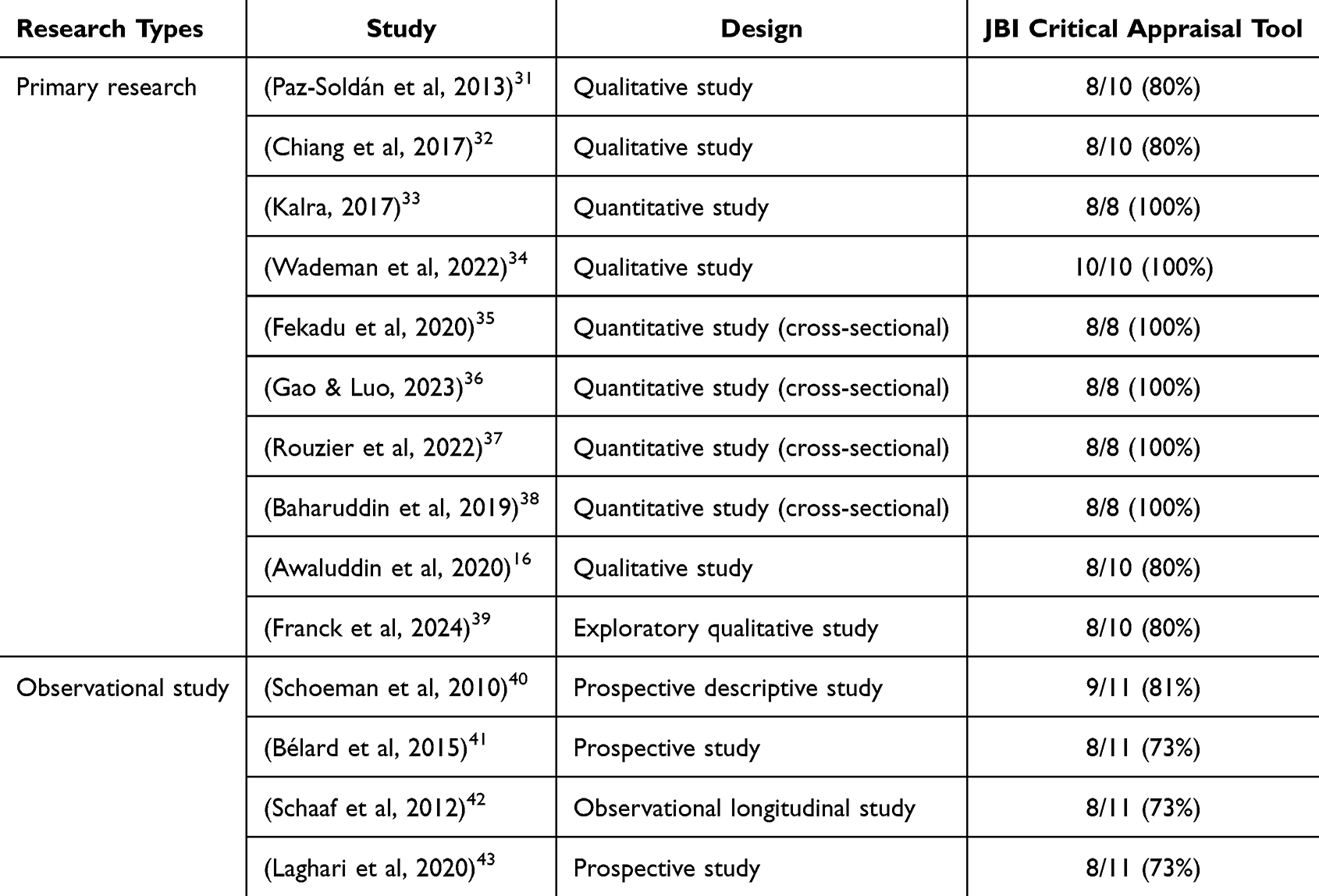 |
Table 1 JBI Critical Appraisal Results |
Study Characteristic
From the 14 articles analyzed, there were 5 qualitative studies, 5 quantitative studies, 3 prospective studies, and 1 observational longitudinal study, all involving a population of parents of children with TB (currently undergoing TB treatment) and parents of children who were in close contact with DR-TB in the household (Table 1). These articles came from various countries, including Peru (n=2), South Africa (n=5), India (n=1), Ethiopia (n=1), Malaysia (n=2), China (n=1), Indonesia (n=1), and one article was from a multi-country study (Botswana, Brazil, Haiti, India, Kenya, Peru, South Africa, and Thailand). The total number of participants in this review was 1,789 parents, consisting of parents of children with TB (n=1,480) and parents of children who were in close contact with DR-TB in the household (n=309). In this review, the article with the largest sample size was 443 parents,43 and the smallest sample size only involved 15 parents.16
Factors Associated with Parental Involvement
This review highlights that parents play a central role in ensuring adherence and continuity of treatment in children to prevent DR-TB. Specifically, parents greatly influence the regularity of their children’s medication consumption on time through daily supervision so that the entire course of treatment is completed to prevent drug resistance. Fourteen articles examined factors related to parental involvement in DR-TB prevention efforts in children. Efforts to prevent DR-TB in children include preventing DR-TB transmission in children who are in close contact in the household and preventing the development of active TB in children into DR-TB through adherence to TB treatment. From each of these efforts, various factors were identified related to parental involvement, manifested in the form of family support, including emotional support, instrumental or logistical support, informational support, and appraisal support. These types of support reflect how parents are involved in various dimensions of parental involvement, including sharing knowledge, making decisions, monitoring and supporting children’s health, and advocating for children through collaboration with health professionals. Based on Coyne et al (2016), these various dimensions of parental involvement are contained in the concept of parental involvement adapted from the Family Centered Care (FCC) framework.44 Details of the mapping of factors related to all types of parental involvement in efforts to prevent DR-TB in children can be seen in (Table 2).
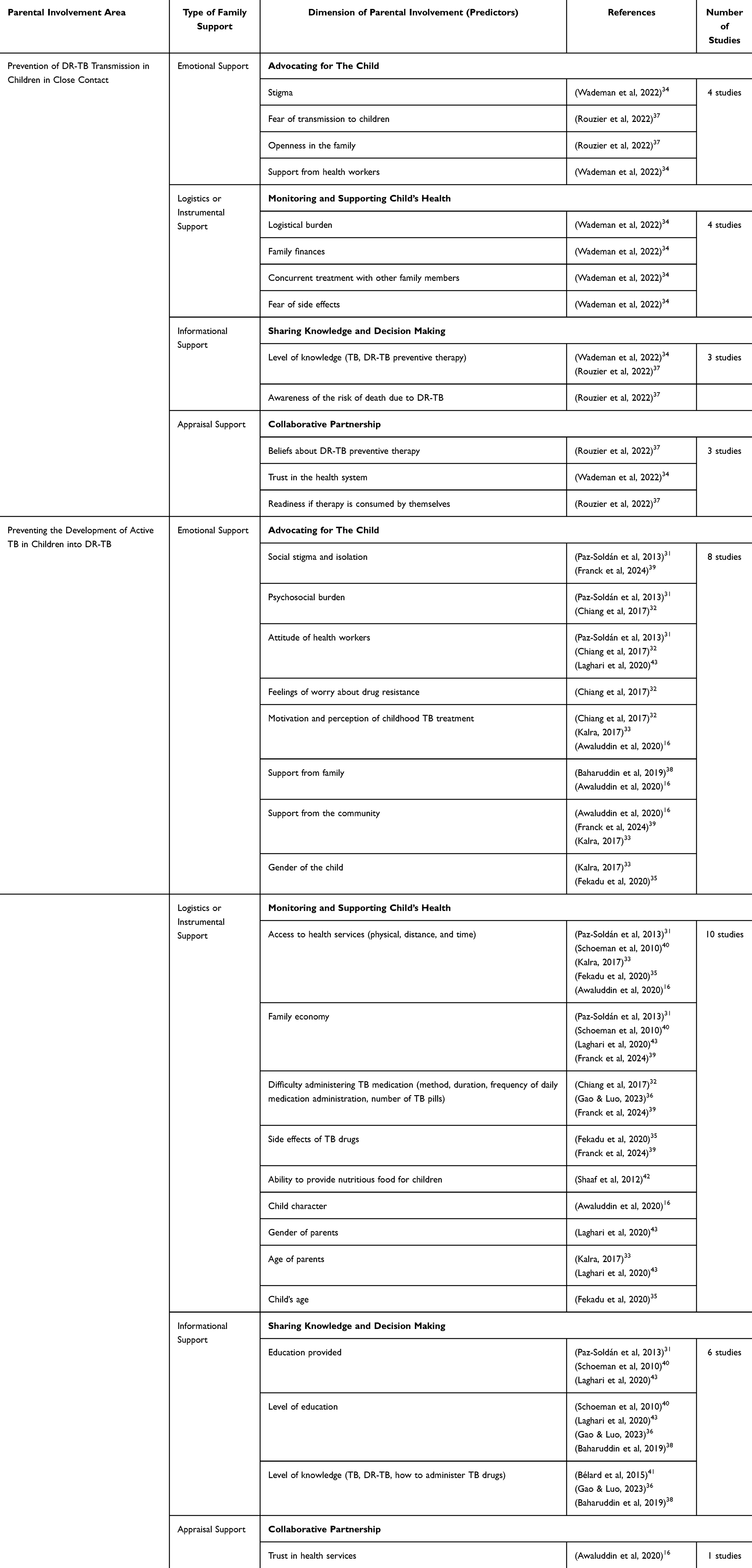 |
Table 2 Mapping of Factors Related to Parental Involvement |
Based on parental involvement in efforts to prevent DR-TB transmission in children who are in close contact, parental involvement is influenced by emotional support,34,37 instrumental or logistical support,34 informational support,34,37 and appraisal support.34,37 The stigma,34 support from health workers,34 anxiety,37 and family openness were related to parental involvement in advocating for their children’s health, which represents emotional support.37 The logistical burdens, family economy, concurrent treatment with parents, and fear of side effects were related to the ability of parents to provide direct care that represents instrumental or logistical support.34 Parental knowledge and awareness of the risk of child death due to TB can influence parental involvement in seeking information and making health decisions for children, which represents informational support.34,37 Meanwhile, parental involvement through their trust in the health system, which represents appraisal support, is related to the trust factor in the health system,34 as well as the parental belief factor regarding DR-TB preventive therapy.37
Based on parental involvement in efforts to develop active TB in children into DR-TB through adherence to TB treatment, parental involvement is influenced by emotional support,16,31–33,35,38,39 instrumental or logistical support,16,31–33,35,36,39,40,42,43 informational support,31,36,38,40,41,43 and appraisal support.16 Stigma factors;31,39 psychosocial burden;31,32 attitudes of health workers;31,32,43 anxiety;32 motivation and perception;16,32,33 community support;33,39 child gender;35 and family support which is related to parental involvement in providing motivation and advocacy for TB care for their children which represents emotional support.38 Parental involvement in monitoring and supporting child care, which represents instrumental or logistical support, is related to health service access factors which are specifically related to time and distance;16,31,35,40 economic factors;31,39,40,43 difficulty in administering medication which is specifically related to high frequency and high number of pills;32,36 parent age;33,43 drug side effect;35,39 child age;35 ability to provide food factors nutritious;42 parental gender;43 and child character factors.16
Parental involvement in providing information and making decisions about children’s health together with health workers who represent informational support is related to educational factors provided;31,40,43 educational level factors;31,36,38,40 and knowledge level factors regarding TB disease, the method and time of administering medication.36,38,45 Finally, the results show that the trust factor in health services is related to parental involvement in establishing partnerships and shared responsibilities with health workers who represent appraisal support.16 Overall, these findings highlight that parental involvement is shaped by a variety of interrelated family supports and reflects the dimensions of parental involvement in DR-TB prevention. Further analysis of each factor related to DR-TB prevention efforts in children can be seen in (Table 3).
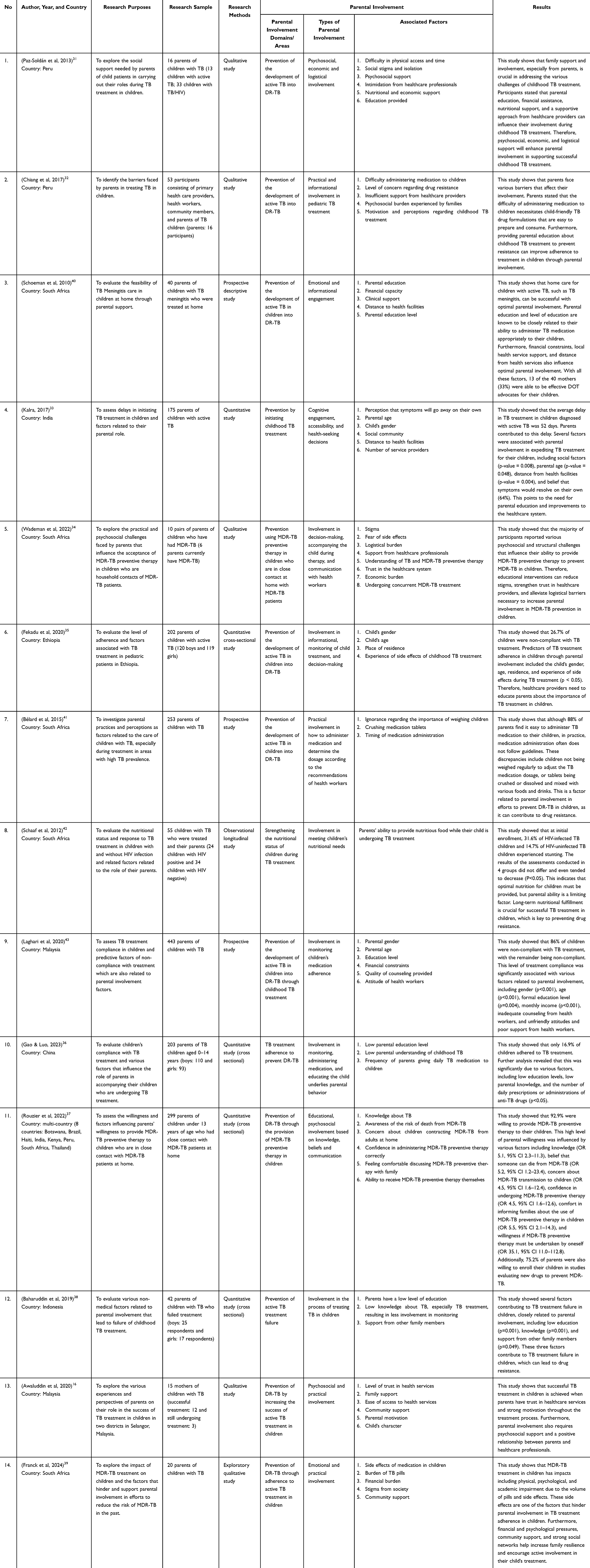 |
Table 3 Results of Article Analysis |
Discussion
Parents are crucial in preventing DR-TB in children. There are two areas of DR-TB prevention in children: preventing exposure to DR-TB in children who are in close contact with them in the household and improving adherence and success of TB treatment in children.
Prevention of DR-TB Transmission in Children with Close Contact
Preventing adult-to-child transmission of DR-TB is a secondary prevention effort. This review identified several factors related to parental involvement in preventing children from being exposed to DR-TB at home, representing various forms of family support. This parental involvement is crucial to prevent children from developing DR-TB when there is a DR-TB patient in the household.4 Children who have close contact with DR-TB patients at home are at high risk of DR-TB infection due to prolonged exposure.46
Identifying pediatric populations exposed to DR-TB and providing preventive therapy for DR-TB has become a universal public health priority.34,47 Several child-friendly DR-TB preventive therapy regimens have been developed.48 However, psychosocial burdens remain a key determinant of parental involvement. Parents must work together to support each other in providing preventive therapy for DR-TB to their children. The limited WHO guidelines complicate parental decision-making, necessitating family-centered support.49
Several factors have been found to be associated with parental involvement, representing emotional support in preventing children from being exposed to DR-TB in the household. Emotional support reflects parental involvement in providing affection, empathy, a sense of security, and attention to children, enabling them to advocate for DR-TB preventive therapy for children. Factors associated with this involvement include stigma, anxiety, family openness, and support from health workers.34,37 Parents with DR-TB also face barriers to treatment due to stigma, catastrophic costs of care, psychological distress, health system barriers, and social, economic, and psychological barriers.7,8 These challenges relate to optimizing their role in providing therapy to children.45
Parents’ perceptions can be shaped by the stigma surrounding them. Several studies have shown that parental involvement in preventing DR-TB in children is influenced by their ability to cope with guilt, shame, and stigma related to the DR-TB they experience.34,50 Parents or children with DR-TB experience depression due to the impact of stigma.51 Parents, especially mothers, bear greater responsibility in preventing DR-TB in children,52 where their involvement is closely related to the level of concern regarding the potential for their child to contract DR-TB at home and the feeling of comfort in discussing it with the family.37 Children who contract TB at home can cause parents to feel guilty and blame themselves, which affects their emotional involvement in providing therapy to their children. Therefore, family support and support from health workers in effective education are needed so that parents are actively involved in providing therapy.34,53
Factors found to be associated with parental involvement that represent instrumental or logistical support in preventing children from being exposed to DR-TB in the household include family economics, logistical burdens, drug side effects, and concurrent treatment with other family members.34 Instrumental or logistical support reflects parental involvement in providing actions or practices in DR-TB prevention. Research has shown that economic barriers to DR-TB prevention in children cause depression in parents.54 Most parents feel that providing DR-TB preventive therapy to their children is an economic burden because they need to constantly develop various strategies to get their children to take their medication. In addition, parents with DR-TB face greater challenges in managing the side effects of medication in their children, in addition to experiencing side effects from the medications themselves.34 However, parents undergoing DR-TB treatment have a positive impact on their involvement because they do not want their children to experience DR-TB like themselves.55
Factors found to be associated with parental involvement that represent informational support include the level of knowledge and awareness of the risk of death from DR-TB.34,37 Informational support reflects parental involvement in making decisions about children’s health and understanding and explaining to children the importance of DR-TB preventive therapy. Previous studies have shown that many parents refuse to give their children DR-TB preventive therapy.49,56 Limited parental understanding reduces their willingness to be involved in providing DR-TB preventive therapy to children, especially if there is concern about the stigma of TB in the community.37,57 These findings emphasize the important role of nurses in providing clear and consistent education to increase knowledge and support parental decision-making.
Meanwhile, factors found to be associated with parental involvement that represent appraisal support include confidence in DR-TB preventive therapy in children, trust in the health system, and readiness to use therapy on themselves.34,37 Appraisal support reflects parental involvement in providing children with confidence in their ability to undergo therapy through appreciation, reinforcement, and positive assessment. Research by Rouzier et al (2022) showed that 92% of parents were willing to provide DR-TB preventive therapy to their children who were in close contact with DR-TB sufferers at home.37 This willingness is related to parental belief in the effectiveness and benefits of DR-TB preventive therapy.37 Parents who are confident in the positive effects of therapy tend to strive for their children’s compliance. Parents’ desire and readiness, especially if they are willing to take DR-TB preventive therapy themselves, support their involvement in providing DR-TB preventive therapy to their children.37,58
Preventing the Development of Active TB in Children Into DR-TB
Preventing the development of active TB in children into DR-TB through adherence to active TB treatment is a secondary prevention effort. Child adherence to treatment indicates that the child is undergoing treatment according to the recommendations of health workers. Children who are not compliant with TB treatment can develop drug resistance, which increases morbidity and mortality due to the high prevalence of DR-TB in children.59 Research shows that only 16.9% of children are compliant with TB treatment.36 Parents are the main determinants of child adherence to TB treatment, so various factors that influence it are automatically related to parental involvement in preventing DR-TB in children. This review found factors of parental involvement in children’s treatment that represent emotional, instrumental/logistical, informational, and appraisal support.
There are various internal and external factors related to parental involvement that represent emotional support during TB treatment in children. Emotional support reflects parental involvement in providing encouragement and attention to children. The stigma associated with TB makes the majority of parents depressed after their child is diagnosed with TB.60 This makes parents reluctant to actively participate in their child’s TB treatment due to fear of discrimination by their surroundings.61 The most common cause of childhood TB stigma is due to inaccurate perceptions regarding TB.
Compliance is further complicated by anxiety and depression, so mental health is essential for optimal treatment.62 Parents often hide their emotions to protect their children’s feelings. Health care providers need to understand the perspectives of parents of children with TB, such as fear and worry.31 This can motivate parents to improve their children’s treatment adherence and encourage them to be open with their healthcare providers. Research by Paz-Soldan et al (2013) showed that social support from family members and healthcare providers is important for improving psychosocial well-being and motivation during TB treatment.31 These findings highlight the need to address psychosocial well-being as an integral component of pediatric TB care.
Family support is related to parental involvement, especially mothers, because it motivates better child care to prevent DR-TB. Several studies have shown that family support can motivate parents to achieve successful TB treatment.63,64 This is in contrast to research by Baharuddin et al (2019) that found that family support was not statistically related to failure of childhood TB treatment, but only as a protective factor for parental involvement.38 Community support is related to parental involvement due to supportive communication from neighbors and friends.16 Minimal support from the surrounding environment makes parents feel alone in caring for their children.33 Therefore, community support can make them feel more able to share their burden.39
Child gender also has a relationship with parental involvement in childhood TB treatment. The level of compliance in girls is 3.3 times higher than in boys.35 This result is in line with research by Herrero et al (2015) that parents are better able to regulate the compliance of girls who mostly stay at home compared to boys who often play outside with their peers.22 Research conducted by Kalra et al (2017) also shows that child gender influences the delay in children starting TB treatment after being diagnosed with TB.33 Delaying treatment in children who have been diagnosed with TB has greater consequences for DR-TB. Parents often assume that the child’s symptoms will disappear without treatment. 96% of the child population dies from TB without starting treatment.35
Various factors related to parental involvement that represent instrumental or logistical support during childhood TB treatment. Instrumental or logistical support reflects parental involvement in directly meeting the child’s needs. Parents face many challenges in optimizing childhood TB care, including time management, transportation, medication administration, finances, and personal conflicts.33 Time and cost of access to health care facilities are determining factors for parental involvement.40 Families with TB patients often come from low-income families. Although TB treatment costs are covered, parents still incur transportation costs and other operational costs.31 This results in suboptimal parental involvement.
Research by Fekadu et al (2020) shows that children with TB living in urban areas have 3.73 times higher adherence than those living in rural areas.64 Parents in urban areas have better awareness and are supported by easy access to health care facilities to undergo routine childhood TB treatment than parents living in rural areas.6 Families also tend to be unable to meet the basic health care needs for children with TB which are important for preventing malnutrition and disease worsening.43 Research by Shaaf et al (2012) shows that children with TB experience malnutrition during TB treatment.42 These barriers highlight the need for social and health system support to reduce parental burden and maintain treatment continuity.
Most parents complain about the difficulty of administering TB medication, which makes them tired and bored. Research by Franck et al (2024) shows that the number and size of pills are factors that influence parents’ decision to administer medication to their children.39 Children who receive medication less frequently have lower adherence rates than children who receive medication three times a day.36 This difference is influenced by the complexity of the child’s TB disease, as parents will be more vigilant if their child is in a severe condition.
In addition, children often complain about side effects from their medications. As many as 39.4% of children are known to experience side effects during TB treatment.36 Another study showed that children were 2.87 times more compliant if they did not experience side effects from TB medication.64 However, another study showed that side effects were not associated with child adherence to treatment.65 These differences in results indicate the possibility of differences in the quality of more optimal clinical pharmacy services in a particular area. Nurses play an important role in health education regarding drug side effects.
The character of a child who is compliant with treatment is also related to parental involvement.64 For parents, an “obedient” child provides a special motivation for the mother to fight for the success of the child’s TB treatment.16 In addition, the child’s physical activity also influences parents to remain calm in carrying out daily routines while giving the child TB medication.16 The child’s age is also related to how involved parents are in TB treatment. Several studies show that the child’s age influences parental involvement,66 where children aged 0–5 years have 5.96 times greater compliance than children aged 11–15 years.35 However, other studies have different results where younger children are more likely to be non-compliant with TB treatment than older children.33 This difference is determined by the support provided by the social environment and parents.
In addition, the gender of parents influences their involvement, where a father is statistically significantly associated with non-compliance in children.43 This is because most men act as family leaders who spend more time outside the home, making them less involved in TB treatment than mothers.22 Parental age is also known to determine parental involvement in DR-TB prevention efforts through TB treatment. Research by Laghari et al (2021) shows that parental age influences their involvement in TB care in children.43 Older parents have less awareness of childhood TB and assume that symptoms will disappear without treatment.31
The study findings also indicate various factors related to parental involvement that represent informational support, including education level, knowledge level, and education provided.31,36,38,40,41,43 Informational support reflects parental involvement in understanding and informing children about the importance of TB treatment to prevent drug resistance. The prevalence of TB is mostly found in low-income areas,22 so that most parents have limited levels of education.36 Education can shape mindsets that consciously make someone live a healthier life. This is in line with other research that a high level of education has an impact on good child compliance because of more optimal parental involvement.64 However, education is not the only factor that determines the success of childhood TB treatment.39
TB treatment adherence in children includes the correct medication schedule, the amount of medication taken, the type of medication, the dosage, and regularly attending appointments with health professionals.64 Information about TB from health professionals is an important component for parents to be able to carry out their role optimally. Parents with good knowledge will be disciplined in ensuring their children’s adherence to taking medication.33 However, other studies have shown that comprehensive parental understanding can reduce fear of TB due to potential misunderstandings.67 This is indicated by 88% of parents saying that giving TB medication to children is easy, but the administration of the medication by parents is different from the administration that should be given.45 Therefore, nurses still need to provide easy-to-understand health education to align with what is expected.
Parents are required to be reliable in administering TB medication to children. Administering TB medication to children must take into account dosage calculations based on the child’s weight, drug formulations, where the required dose is often unavailable and tablets must be split, and the timing of administration.68 Parents are fully responsible for the success of TB treatment to prevent DR-TB in children. Inappropriate drug administration methods can alter drug activity and absorption.45 Health workers need to understand parents’ perspectives on administering TB medication to children so that nurses can increase parental confidence, reduce medication errors, and minimize the risk of drug resistance.
Parental involvement represented by appraisal support is related to parental trust in health services.16 Appraisal support reflects parental involvement in motivating children to continue taking medication compliantly through rewards, reinforcement, and positive assessments of the health system. Trust in health services can guide parents to be ready to face various challenges during their child’s treatment. This is proven because parents who successfully complete TB treatment in children are parents who trust health services, thus parents comply with the recommendations of health workers.65 Through trust in health services, parents become motivated to complete their child’s treatment. Health workers play a crucial role in providing information about TB to children to convince parents that optimal childhood TB care can prevent DR-TB.
Implication for Practice and Policy
This review shows that parental involvement in DR-TB prevention efforts in children is based on interrelated emotional, informational, logistical, and appraisal support. These findings have several implications for practice and policy. First, TB prevention and treatment programs need to be focused on family-centeredness, integrating emotional and informational support for parents. Parental involvement in DR-TB prevention efforts can be optimized by minimizing stigma, anxiety, and psychosocial burden through supportive counseling and communication.
Second, health services can minimize logistical barriers that often hinder parents, such as difficulty accessing care, economic constraints, and challenges in administering TB medication. Strategies that can be implemented include flexible service hours, decentralization of TB services, simplification of treatment regimens, and provision of social or economic support for families. Third, structured education needs to be improved to strengthen parents’ knowledge and capacity in making decisions about their children’s health. Educational interventions should be tailored to parents’ education levels and focus on preventing DR-TB in children. Finally, the level of trust and collaborative partnerships between parents and caregivers needs to be improved to optimize parental involvement. Policies and programs should highlight the importance of communication, continuity of care, and parental involvement as active partners in preventing DR-TB in children.
Strengths and Limitations
This scoping review has several strengths and limitations. Based on a comprehensive literature search, the author found that this review is the first to focus on factors related to parental involvement in DR-TB prevention efforts in the pediatric population. This review successfully mapped factors related to parental involvement that represent various aspects of emotional, instrumental or logistical, informational, and appraisal support in every DR-TB prevention effort in children, thus making a significant contribution to minimizing the occurrence of DR-TB in close contacts and children with TB through parental involvement. Furthermore, all analyzed study findings scored above 70% based on the JBI assessment.
However, this review still has limitations, including using only five major databases in the search for articles. This review only found two research articles discussing factors related to parental involvement in DR-TB preventive therapy efforts in children who are close contacts in the household. This is because existing research related to parental involvement in DR-TB prevention in children, especially regarding DR-TB preventive therapy, is still very limited. Therefore, the authors suggest that future research can further explore parental involvement in DR-TB preventive therapy in children through emotional support, instrumental or logistical support, informational support, and appraisal.
Conclusion
Parental involvement plays a crucial role in preventing DR-TB in children, both through household exposure prevention efforts and through increasing adherence to active TB treatment. Various factors are associated with parental involvement in DR-TB prevention through DR-TB preventive therapy in children which represent four types of family support, namely emotional support (stigma factors, support from health workers, anxiety, family openness), instrumental or logistical support (logistical burden factors, family economy, concurrent treatment with parents, fear of side effects), informational support (level of knowledge, level of parental awareness), and appraisal support (trust in the health system). The factors related to parental involvement as a representation of emotional support (stigma factors, psychosocial burden, health worker attitudes, anxiety, motivation and perception, community support, child gender, family support), instrumental or logistical (health service access factors, economics, difficulty administering medication, age and type of parents, drug side effect factors, child age factors, ability to provide nutritious food, child character), informational (education factors provided, education level, knowledge level), and appraisal (trust in health services factors).
These various factors can influence parental involvement in DR-TB prevention in children. This review is limited and requires further studies exploring parental experiences in the context of DR-TB prevention in children, particularly regarding the provision of DR-TB preventive therapy. The results of this review are expected to provide a basis for health workers, families, and policymakers to increase parental involvement, which is crucial in DR-TB prevention efforts in children.
Acknowledgments
All authors would like to thank Universitas Padjadjaran, Sumedang, West Java, Indonesia, for facilitating the database for this study.
Funding
This study was funded by Universitas Padjadjaran, Bandung, Indonesia, No. 2629/UN6.3.1/PT.00/2025.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Global tuberculosis report. 2024.
2. World Health Organization. Global tuberculosis report. 2023.
3. Kemenkes. Report on the results of the indonesian tuberculosis inventory study. 2024.
4. Schaaf HS. Diagnosis and management of multidrug-resistant tuberculosis in children: a practical approach. The Indian Journal of Pediatrics. 2019;86(8):717–21. doi:10.1007/s12098-018-02846-8
5. Alinaitwe B, Shariff NJ, Madhavi Boddupalli B. Treatment adherence and its association with family support among pulmonary tuberculosis patients in Jinja, Eastern Uganda. Sci Rep. 2025;15(1):11150. doi:10.1038/s41598-025-96260-8
6. Tesfahuneygn G, Medhin G, Legesse M. Adherence to anti-tuberculosis treatment and treatment outcomes among tuberculosis patients in Alamata District, northeast Ethiopia. BMC Res Notes. 2015;8(1):503. doi:10.1186/s13104-015-1452-x
7. de Vries SG, Cremers AL, Heuvelings CC, et al. Barriers and facilitators to the uptake of tuberculosis diagnostic and treatment services by hard-to-reach populations in countries of low and medium tuberculosis incidence: a systematic review of qualitative literature. Lancet Infect Dis. 2017;17(5):e128–43. doi:10.1016/S1473-3099(16)30531-X
8. Loveday M, Sunkari B, Master I, et al. Household context and psychosocial impact of childhood multidrug-resistant tuberculosis in KwaZulu-Natal, South Africa. Int J Tuberculosis Lung Dis. 2018;22(1):40–46. doi:10.5588/ijtld.17.0371
9. Eticha T, Berhane L. Caregiver-reported adherence to antiretroviral therapy among HIV infected children in Mekelle, Ethiopia. BMC Pediatr. 2014;14(1):114. doi:10.1186/1471-2431-14-114
10. Martinez L, Gray DM, Botha M, et al. The long-term impact of early-life tuberculosis disease on child health: a prospective birth cohort study. Am J Respir Crit Care Med. 2023;207(8):1080–1088. doi:10.1164/rccm.202208-1543OC
11. Triasih R, Padmawati RS, Duke T, Robertson C, Sawyer SM, Graham SM. A mixed-methods evaluation of adherence to preventive treatment among child tuberculosis contacts in Indonesia. Int J Tuberc Lung Dis. 2016;20(8):1078–1083. doi:10.5588/ijtld.15.0952
12. Das M, Mathur T, Ravi S, et al. Challenging drug-resistant TB treatment journey for children, adolescents and their care-givers: a qualitative study. PLoS One. 2021;16(3):e0248408. doi:10.1371/journal.pone.0248408
13. Maphalle LNF, Michniak-Kohn BB, Ogunrombi MO, Adeleke OA. Pediatric tuberculosis management: a global challenge or breakthrough? Children. 2022;9(8):1–42. doi:10.3390/children9081120
14. Snow KJ, Cruz AT, Seddon JA, et al. Adolescent tuberculosis. Lancet Child Adolesc Health. 2020;4(1):68–79. doi:10.1016/S2352-4642(19)30337-2
15. World Health Organization. Guidance for national tuberculosis programmes on the management of tuberculosis in children. World Health Organization. 2015.
16. Awaluddin SM, Ismail N, Yasin SM, et al. Parents’ experiences and perspectives toward tuberculosis treatment success among children in malaysia: a qualitative study. Front Public Health. 2020;8(December):1–8. doi:10.3389/fpubh.2020.577407
17. Dary PD, Puspita D, Mela SKC. Peran Keluarga dalam Merawat Anak yang Menderita Penyakit TB Paru di Wilayah Kerja Puskesmas Getasan. Journal LINK. 2018;13(2):5–11. doi:10.31983/link.v13i2.2840
18. Raji M, Rusdi R. Peran Keluarga dalam Mendukung Keberhasilan Pengobatan pada Penderita Penyakit Tb Paru. JOIN. 2022;1(1):28–39. doi:10.54004/join.v1i1.55
19. Kemenkes RI. Buku Petunjuk Teknis Manajemen dan Tatalaksana TB Anak. 2016.
20. Rutherford ME, Ruslami R, Maharani W, et al. Adherence to isoniazid preventive therapy in Indonesian children: a quantitative and qualitative investigation. BMC Res Notes. 2012;5(1):1–7. doi:10.1186/1756-0500-5-7
21. Gao L, Luo B. Assessment of factors associated with anti-tubercular treatment compliance in children: a cross-sectional study. Glob Pediatr Health. 2024;11.
22. Herrero MB, Ramos S, Arrossi S. Determinants of non adherence to tuberculosis treatment in Argentina: barriers related to access to treatment. Revista Brasileira de Epidemiologia. 2015;18(2):287–298. doi:10.1590/1980-5497201500020001
23. Belay GM, Wubneh CA. Childhood tuberculosis treatment outcome and its association with HIV co-infection in Ethiopia: a systematic review and meta-analysis. Tropical Med Health. 2020;48(1):7. doi:10.1186/s41182-020-00195-x
24. Santos JC, Silva JB, Rangel MA, Barbosa L, Carvalho I. Preventive therapy compliance in pediatric tuberculosis – a single center experience. Pulmonology. 2020;26(2):78–83. doi:10.1016/j.pulmoe.2019.06.002
25. Dias AAL, de Oliveira DMF, Turato ER, de Figueiredo RM. Life experiences of patients who have completed tuberculosis treatment: a qualitative investigation in southeast Brazil. BMC Public Health. 2013;13(1):1–9. doi:10.1186/1471-2458-13-595
26. Peterson J, Pearce PF, Ferguson LA, Langford CA. Understanding scoping reviews: definition, purpose, and process. J Ame Assoc Nurse Practition. 2017;29(1):12–16. doi:10.1002/2327-6924.12380
27. Peters M, Godfrey C, McInerney P, Munn Z, Tricco A, Khalil H. JBI manual for evidence synthesis. JBI. 2024.
28. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
29. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
30. Barker T, Stone J, Sears K, et al. The revised JBI critical appraisal tool for the assessment of risk of bias for randomized controlled trials. JBI Evidence Synthesis. 2023;21(3):494–506. doi:10.11124/JBIES-22-00430
31. Paz-Soldán VA, Alban RE, Jones CD, Oberhelman RA. The provision of and need for social support among adult and pediatric patients with tuberculosis in Lima, Peru: a qualitative study. BMC Health Serv Res. 2013;13(1):290. doi:10.1186/1472-6963-13-290
32. Chiang SS, Roche S, Contreras C, et al. Barriers to the treatment of childhood tuberculous infection and tuberculosis disease: a qualitative study. Int J Tuberc Lung Dis. 2017;21(2):154–160. doi:10.5588/ijtld.16.0624
33. Kalra A. Care seeking and treatment related delay among childhood tuberculosis patients in Delhi, India. Int J Tuberc Lung Dis. 2017;21(6):645–650. doi:10.5588/ijtld.16.0563
34. Wademan DT, Hoddinott G, Purchase SE, et al. Practical and psychosocial challenges faced by caregivers influence the acceptability of multidrug-resistant tuberculosis preventive therapy for young children. PLoS One. 2022;17(7):1–18. doi:10.1371/journal.pone.0268560
35. Fekadu G, Bekele F, Bekele K, et al. Adherence to anti-tuberculosis treatment among pediatric patients at nekemte specialized hospital, Western Ethiopia. Patient Prefer Adherence. 2020;14(null):1259–1265. doi:10.2147/PPA.S258292
36. Gao L, Luo B. Assessment of factors associated with anti-tubercular treatment compliance in children: a cross-sectional study. Glob Pediatr Health. 2024;11:9.
37. Rouzier V, Murrill M, Kim S, et al. Caregiver willingness to give TPT to children living with drug-resistant TB patients. Int JTuberculosis Lung Disease. 2022;26(10):949–955. doi:10.5588/ijtld.21.0760
38. Baharuddin K, Bahtiar B, Basri H, et al. Evaluation factors for non medical treatment failure patients tuberculosis lung health in children on Makassar City. Indian J Public Health Res Dev. 2019;10(8):1996–2000. doi:10.5958/0976-5506.2019.02146.6
39. Franck C, Seddon JA, Hesseling AC, Schaaf HS, Skinner D, Reynolds L. Assessing the impact of multidrug-resistant tuberculosis in children: an exploratory qualitative study. BMC Infect Dis. 2014;14(1):426. doi:10.1186/1471-2334-14-426
40. Schoeman J, Malan G, van Toorn R, Springer P, Parker F, Booysen J. Home-based treatment of childhood neurotuberculosis. J Trop Pediatr. 2009;55(3):149–154. doi:10.1093/tropej/fmn097
41. Bélard S, Isaacs W, Black F, et al. Treatment of childhood tuberculosis: caregivers’ practices and perceptions in Cape Town, South Africa. Paediatr Int Child Health. 2015;35(1):24–28. doi:10.1179/2046905514Y.0000000133
42. Schaaf H, Cilliers K, Willemse M, Labadarios D, Kidd M, Donald PR. Nutritional status and its response to treatment of children, with and without HIV infection, hospitalized for the management of tuberculosis. Paediatr Int Child Health. 2012;32(2):74–81. doi:10.1179/2046905512Y.0000000008
43. Laghari M, Talpur BA, Sulaiman SAS, Khan AH, Bhatti Z. Assessment of adherence to anti-tuberculosis treatment and predictors for non-adherence among the caregivers of children with tuberculosis. Trans R Soc Trop Med Hyg. 2021;115(8):904–913. doi:10.1093/trstmh/traa161
44. Coyne I, Hallström I, Söderbäck M. Reframing the focus from a family-centred to a child-centred care approach for children’s healthcare. J Child Health Care. 2016;20(4):494–502. doi:10.1177/1367493516642744
45. Majombozi Z. Care, contagion and the good mother: narratives of motherhood, tuberculosis and healing. Anthropol Southern Africa. 2019;42(4):290–301. doi:10.1080/23323256.2019.1608276
46. Shah NS, Yuen CM, Heo M, Tolman AW, Becerra MC. Yield of contact investigations in households of patients with drug-resistant tuberculosis: systematic review and meta-analysis. Clin Infect Dis. 2014;58(3):381–391. doi:10.1093/cid/cit643
47. Fox GJ, Dobler CC, Marais BJ, Denholm JT. Preventive therapy for latent tuberculosis infection—the promise and the challenges. Int J Infect Dis. 2017;56:68–76. doi:10.1016/j.ijid.2016.11.006
48. Marais BJ. Newer drugs for tuberculosis prevention and treatment in children. Indian J Pediatr. 2019;86(8):725–731. doi:10.1007/s12098-018-02854-8
49. Seddon JA, Johnson S, Palmer M, et al. Multidrug-resistant tuberculosis in children and adolescents: current strategies for prevention and treatment. Expert Rev Respir Med. 2021;15(2):221–237. doi:10.1080/17476348.2021.1828069
50. Thomas BE, Shanmugam P, Malaisamy M, et al. Psycho-socio-economic issues challenging multidrug resistant tuberculosis patients: a systematic review. PLoS One. 2016;11(1):e0147397. doi:10.1371/journal.pone.0147397
51. Naidu T, Pillay SR, Ramlall S, et al. Major depression and stigma among individuals with multidrug-resistant tuberculosis in South Africa. Am J Trop Med Hyg. 2020;103(3):1067. doi:10.4269/ajtmh.19-0426
52. Wong WCW, Holroyd E, Miu HYH, Wong CS, Zhao Y, Zhang J. Secrets, shame and guilt: HIV disclosure in rural Chinese families from the perspective of caregivers. Vulnerable Child Youth Stud. 2017;12(4):292–303. doi:10.1080/17450128.2017.1344343
53. Moore BK, Erasmus L, Ershova J, Smith SE, Ndjeka N, Podewils LJ. Pre-treatment loss to follow-up among children with multidrug-resistant tuberculosis in South Africa, 2008–2010. PLoS One. 2020;15(4):e0230504. doi:10.1371/journal.pone.0230504
54. Tomita A, Ramlall S, Naidu T, Mthembu SS, Padayatchi N, Burns JK. Major depression and household food insecurity among individuals with multidrug-resistant tuberculosis (MDR-TB) in South Africa. Soc Psychiatry Psychiatr Epidemiol. 2019;54(3):387–393. doi:10.1007/s00127-019-01669-y
55. Boffa JM, Fisher DA, Mayan MJ, Sauve RS, Williamson TS. Effectiveness of isoniazid preventive therapy to reduce tuberculosis incidence in the context of antiretroviral therapy. JAIDS J Acquire Immune Deficiency Syndromes. 2020;84(3):e14–7. doi:10.1097/QAI.0000000000002339
56. Adler-Shohet FC, Low J, Carson M, Girma H, Singh J. Management of latent tuberculosis infection in child contacts of multidrug-resistant tuberculosis. Pediatr Infect Dis J. 2014;33(6):664–666. doi:10.1097/INF.0000000000000260
57. Egere U, Sillah A, Togun T, et al. Isoniazid preventive treatment among child contacts of adults with smear-positive tuberculosis in The Gambia. Public Health Action. 2016;6(4):226–231. doi:10.5588/pha.16.0073
58. Williams B, Ramroop S, Shah P, et al. Management of pediatric contacts of multidrug resistant tuberculosis in the United Kingdom. Pediatr Infect Dis J. 2013;32(8):926–927. doi:10.1097/INF.0b013e31829157e9
59. Zegeye A, Dessie G, Wagnew F, et al. Prevalence and determinants of anti-tuberculosis treatment non-adherence in Ethiopia: a systematic review and meta-analysis. PLoS One. 2019;14(1):e0210422. doi:10.1371/journal.pone.0210422
60. Courtwright A, Turner AN. Tuberculosis and Stigmatization: pathways and Interventions. Public Health Reports. 2010;125(4_suppl):34–42. doi:10.1177/00333549101250S407
61. Rakhmawati W, Nilmanat K, Hatthakit U. Moving from fear to realization: family engagement in tuberculosis prevention in children living in tuberculosis Sundanese households in Indonesia. Int J Nurs Sci. 2019;6(3):272–277. doi:10.1016/j.ijnss.2019.06.002
62. Agarwal N, Sarthi P. The necessity of psychological interventions to improve compliance with Tuberculosis treatment and reduce psychological distress. J Family Med Prim Care. 2020;9(8):4174–4180. doi:10.4103/jfmpc.jfmpc_1404_20
63. Rutherford ME, Ruslami R, Anselmo M, et al. Management of children exposed to Mycobacterium tuberculosis: a public health evaluation in West Java, Indonesia. Bulletin World Health Organiz. 2013;91(12):932–941. doi:10.2471/BLT.13.118414
64. Silva TDMVD, Santos MÁD, Almeida FDA. Understanding the experiences of caregivers of children with tuberculosis in directly observed therapy. Revista da Escola de Enfermagem da USP. 2014;48(spe2):39–45. doi:10.1590/S0080-623420140000800007
65. Parmar P, Modi A, Godara N. Understanding pediatric tuberculosis: perspectives and experiences of the parents in a city of India. Int J Med Sci Public Health. 2018;1:132–137.
66. Gebreweld FH, Kifle MM, Gebremicheal FE, et al. Factors influencing adherence to tuberculosis treatment in Asmara, Eritrea: a qualitative study. J Health Popul Nutr. 2018;37(1):1. doi:10.1186/s41043-017-0132-y
67. Nyasulu P, Sikwese S, Chirwa T, et al. Knowledge, beliefs, and perceptions of tuberculosis among community members in Ntcheu district, Malawi. J Multidisciplin Healthcare. 2018;11(null):375–389. doi:10.2147/JMDH.S156949
68. Sari E, Kristina TN, Sujianto U. Parents knowledge and experiences of child TB patients about medicine administration in the intensive phase. Open Access Maced J Med Sci. 2023;11(G):78–81. doi:10.3889/oamjms.2023.9594
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.