Back to Journals » Risk Management and Healthcare Policy » Volume 14
Factors Associated with Musculoskeletal Disorders Among Female Readymade Garment Workers in Bangladesh: A Comparative Study Between OSH Compliant and Non-Compliant Factories
Authors Nabi MH ![]() , Kongtip P
, Kongtip P ![]() , Woskie S, Nankongnab N, Sujirarat D, Chantanakul S
, Woskie S, Nankongnab N, Sujirarat D, Chantanakul S
Received 13 December 2020
Accepted for publication 24 February 2021
Published 15 March 2021 Volume 2021:14 Pages 1119—1127
DOI https://doi.org/10.2147/RMHP.S297228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Marco Carotenuto
Mohammad Hayatun Nabi,1,2 Pornpimol Kongtip,2,3 Susan Woskie,4 Noppanun Nankongnab,2,3 Dusit Sujirarat,5 Suttinun Chantanakul2
1Department of Public Health, School of Health and Life Sciences, North South University, Dhaka, Bangladesh; 2Department of Occupational Health and Safety, Faculty of Public Health, Mahidol University, Bangkok, Thailand; 3Center of Excellence on Environmental Health and Toxicology, Bangkok, Thailand; 4Department of Public Health, Zuckerberg College of Health Sciences, University of Massachusetts Lowell, Lowell, MA, USA; 5Department of Epidemiology, Faculty of Public Health, Mahidol University, Bangkok, Thailand
Correspondence: Pornpimol Kongtip
Department of Occupational Health and Safety, Faculty of Public Health, Mahidol University, 420/1 Ratchawithi Road, Ratchathewi District, Bangkok, 10400, Thailand
Tel +66 26444070
Fax +66 23548561
Email [email protected]
Purpose: Musculoskeletal Disorders (MSDs) are one of the most common occupational diseases responsible for work restriction and absenteeism. The purpose of the study was to compare the prevalence of MSDs between ready-made garment (RMG) factories that are compliant versus non-compliant with International Labor Organization (ILO) based Occupational Safety and Health (OSH) standards, and to identify other factors associated with a higher prevalence of MSDs.
Methods: A multicenter cross-sectional study was conducted among 410 randomly selected female workers (age: > 18 years; ≥ 1 year of work experience) from 12 randomly selected RMG factories in the Dhaka district of Bangladesh from February to December 2019. Factories were stratified as OSH compliant or non-compliant. Data were collected using a structured questionnaire consist of socio-demographic, work-related factors, and Nordic Musculoskeletal Questionnaire (NMQ) for MSD assessment. Robust Poisson regression was used to investigate the association of MSDs with OSH compliance, socio-demographic and other work-related factors.
Results: Respondents’ mean age was 26.9 ± 5.9 years. A total of 235 (57%) of the workers reported musculoskeletal pain in at least one body part during the last month. Among the nine reported MSDs, the prevalence of lower back pain was highest (41%) followed by pain in the knees (33%). Multivariable analysis showed lower prevalence of any MSD among workers in OSH compliant factories [aPR = 0.43, 95% CI: 0.31– 0.58], and workers with regular working hours (8 hrs/day) [aPR = 0.79, 95% CI: 0.62– 1.00]. The risk of developing any MSD was significantly higher for age group 25– 30 years [aPR = 1.16, 95% CI: 1.01– 1.33] and age group ≥ 31 years [aPR = 1.21, 95% CI: 1.04– 1.1.39].
Conclusion: The study found a high burden of musculoskeletal disorders among female RMG workers, especially those in non-OSH compliant factories that work long hours. Enforcement of minimum ILO-based OSH standards and introduction of low-cost interventions to improve working conditions in non-compliant factories would help sustain the pace of development in this sector in Bangladesh, and ensure the health of the women who work there.
Keywords: Nordic Musculoskeletal Questionnaire, back pain, neck pain, knee pain, occupational health, garment factory, work-related, aging, International Labor Organization
Introduction
Musculoskeletal Disorders (MSDs) are a group of inflammatory and degenerative conditions that affect the muscles, tendons, ligaments, joints or peripheral nerves, usually leading to aches, pains or discomfort.1,2 MSDs usually result from repetitive manual labor, lifting heavy loads, prolonged static work, overexertion, vibration, or working in an awkward posture.3–6 MSDs are a major public health problem in both industrialized and developing countries and may result in work restriction, absenteeism, or even the need to change jobs, which are themselves associated with major economic costs resulting in serious impacts on the person's quality of life.7,8 Compared to the average nonfatal workplace injury or illness, MSDs need longer recovery times and are responsible for millions of lost workdays every year.9
The Readymade Garment (RMG) sector of Bangladesh has grown during the last couple of decades to become a leader in the world garment manufacturing industry.10 The RMG sector plays an important role in the economy of the country through contributions to export, employment, and poverty alleviation.11 The sustainability of this industry largely depends on meeting the expectations of international consumers who have become more concerned about occupational safety and health (OSH) issues. Consequently, the compliance of the Bangladesh RMG industry with world labor and OSH standards has attained new attention, and international buyers prefer to place orders with OSH-compliant factories. Compliance for the RMG industry in Bangladesh requires upholding a code of conduct originally developed by the International Labor Organization (ILO) to cover core labor standards, employment conditions, and occupational health and safety standards.12,13 However, now most of the codes adopted by the global buyers tend to cluster around a set of internationally recognized standards, such as Business Social Compliance Initiative (BSCI),14 Supplier Ethical Data Exchange (SEDEX),15 Worldwide Responsible Accredited Production (WRAP),16 and Initiative for Compliance and Sustainability (ICS).17 The codes of conduct require adherence to labor law and building codes, including adequate building structures, staircases, fire/emergency exits, and waste management; the prohibition of forced labor and harassment; rules on working hours, wages, leave and holidays; upholding the freedom of association and rights to unionize; as well as the provision of health checkups, work environment safety measures and occupational health and safety training.12,13 Table 1 describes the OSH topics covered in compliance designations for RMG factories in Bangladesh.
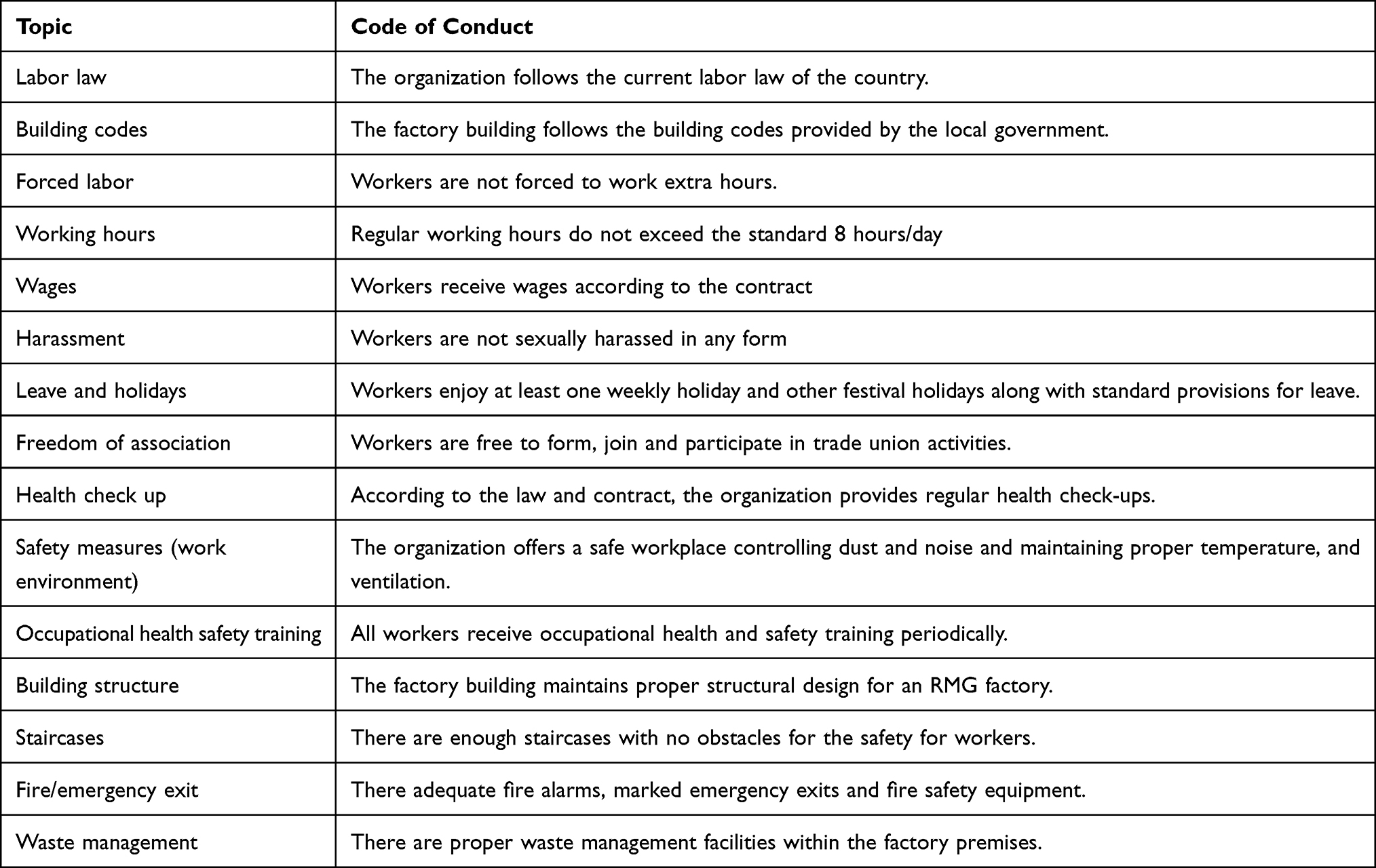 |
Table 1 Brief Description of ILO Based OSH Topics Used to Determine Compliance for RMG Factories in Bangladesh |
Though the conditions related to compliance have improved in the recent past, universal compliance does not occur throughout the industry. Factories who comply with labor and occupational safety and health standards can become certified as “compliant” by international organizations. However, the widespread practice of noncompliance with these workplace standards makes RMG workers more vulnerable to develop occupational diseases.18 They work in unsafe working environments and are often exploited by their managers and supervisors due to their gender.13,19 Poor working conditions that include extended working hours, awkward postures, repetitive motions, heavy lifting and lack of occupational health safety measures have been identified as risk factors for work-related MSDs in the garment industries of other countries.20,21 This study aims to compare the prevalence of MSDs between OSH compliant and non-compliant garment factories, and to identify other factors associated with a higher prevalence of MSDs.
Materials and Methods
Study Design, Study Site and Settings
A multicenter cross-sectional study was conducted in two industrial zones in the Dhaka district of Bangladesh – Savar and Ashulia. These two zones were chosen for having the highest geographic concentration of RMG factories and workers. A total of 12 RMG factories were randomly selected using the Bangladesh Garment Manufacturers and Exporters Association (BGMEA) factory list, and stratified as compliant or non-compliant as described below.22 All of the selected factories provided permission and a list of female workers from which to recruit. A total of 410 female workers were randomly selected from those factories (205 per compliance strata). Inclusion criteria of the participants included being 18 years of age or older and having at least 1 year of work experience in the RMG sector. Women who were pregnant or had a history of any joint or bone disorder were excluded. Data were collected through face-to-face interviews after receiving informed written consent from the participants. Data collection was done after working hours and on weekends at local trade union offices close to the factories. The study was carried out from February 2019 to December 2019.
Study Variables
Exposure: Compliance Category in Bangladeshi RMG
Factories were considered “compliant” if they had received certificates from one or more of the recognized compliance bodies. Table 2 provides the list of factories included in this study with a description of their compliance certifications.
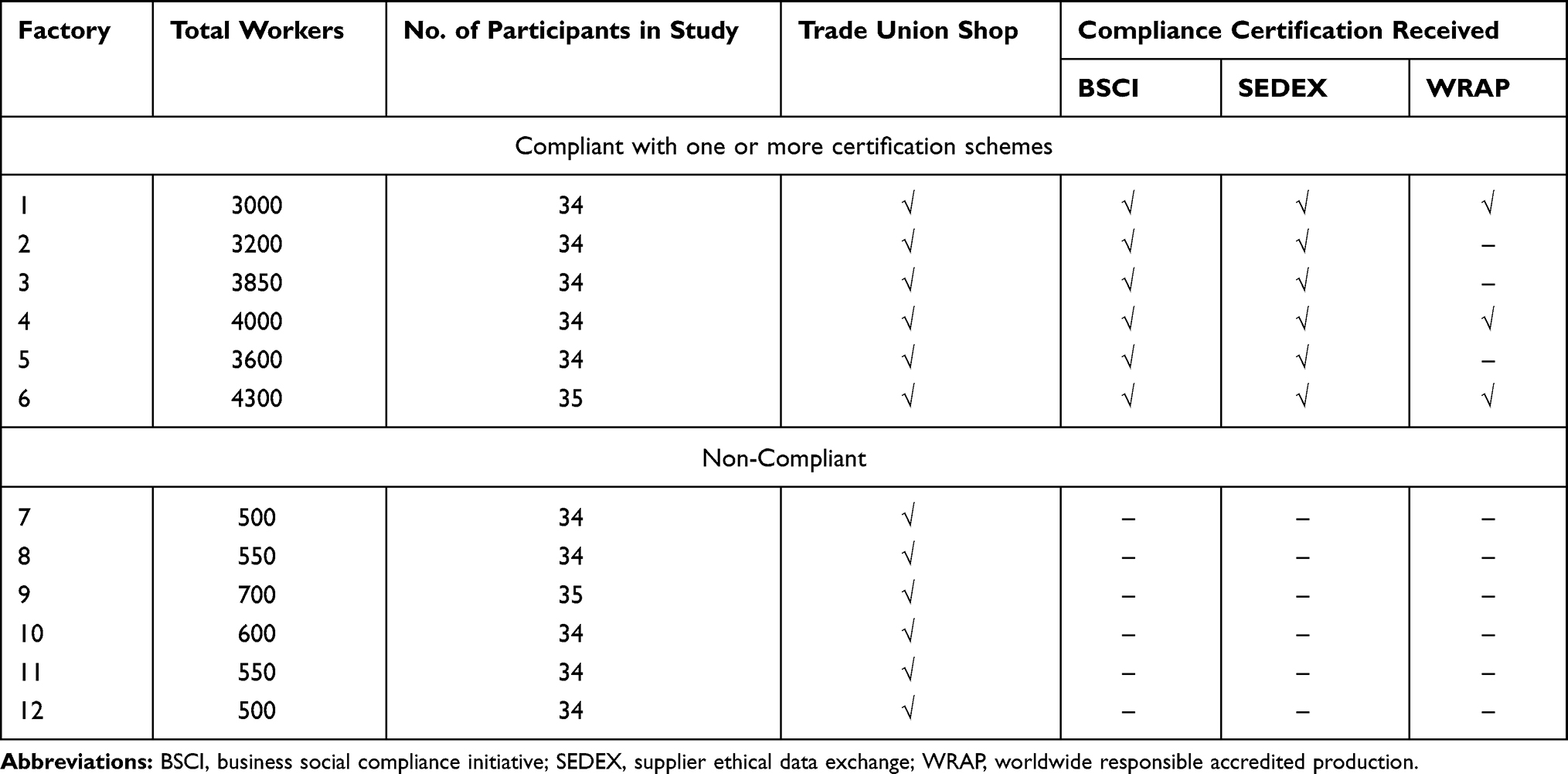 |
Table 2 List of Factories with Description of Compliance Certification |
Measurement of Musculoskeletal Disorders
The questions on musculoskeletal disorders were based on a modified Nordic Musculoskeletal Questionnaire (NMQ) that measures musculoskeletal complaints in terms of pain experienced during the last 1 month.23 The NMQ has been used among a wide variety of occupational groups in different setting, including rice farmers,24 nurses,25,26 truck drivers,27 physical therapist,28,29 and garment workers.3 It encompassed nine body regions: neck, shoulder, upper back, elbows, wrists/hands, lower back, hips/thighs, knee, and ankle/feet.23 The responses were recorded in a dichotomous scale where 0 = no pain and 1 = pain. The questionnaire underwent forward and backward translation from English and Bengali to ensure translational accuracy.
Independent Variables
Data on socio-demographic and work-related factors were collected using a pretested structured questionnaire. The socio-demographic data included age, years of education, marital status, number of family members, monthly income, and current job designation. In this study, age was categorized into three groups: 19–24 years, 25–30 years and ≥31 years. In addition to the factory category (compliant vs non-compliant), personal information about participation in a worksite annual health examination, occupational health safety training and working hours was collected.
Statistical Analysis
Data analysis was conducted by using the IBM Statistical Package for Social Sciences (SPSS) Version 23. Descriptive statistics were used for all of the categorical variables (presented as frequencies and percentages). A directed acyclic graph (DAG) was created to account for confounders in the association between factory compliance status and MSDs. The function of this graphical method was the identification of minimally sufficient adjustment sets for estimating causal effects, diagnosis of insufficient or invalid adjustment via the identification of biasing paths, identification of instrumental variables, and derivation of testable implications.30 MSDs were considered the outcome variable, and the type of factory (compliance status) were considered the main exposure variable. The minimally sufficient adjustment set for estimating the direct effect of the exposure (compliance status) on MSDs contained age and working hours. The DAG was constructed through DAGitty and is given in Supplementary Figure 1. The statistical association between MSDs and the exposure along with associated factors was modeled using robust Poisson regression. The adjusted prevalence ratio (aPR) and corresponding 95% confidence intervals (CIs) were used to report the results. A p-value less than 0.05 was considered statistically significant.
Results
Prevalence of MSDs
The one-month prevalence of reporting each type of MSD stratified by factory compliance category for the 410 female RMG workers is reported in Figure 1. A total of 235 (57%) of the workers reported musculoskeletal pain in at least one body part during the last month. Among the nine MSDs, the prevalence of lower back pain was highest (41%) followed by pain in the knees (33%), neck pain (28%), upper back pain (24%), pain in the ankles (21%), pain in the shoulder (14%), and pain in the wrists/hands (13%). Participants who worked in non-compliant factories were significantly more likely to report at least one MSD in the previous month compared to compliant factories (72% versus 42%).
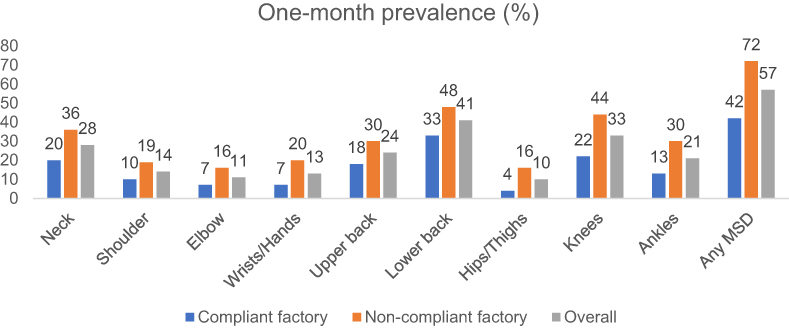 |
Figure 1 Prevalence of MSDs in different body regions from subjects working in compliant and non-compliant factories. |
Univariate Analysis: Socio-Demographic and Work-Related Factors
Participants’ socio-demographic and work-related characteristics are presented in Table 3. The mean ± SD age of the 410 participants was 26.9 ± 5.9 years. Most of the participants (46%) were in the category of 25–30 years of age, followed by the category of 19–24 years (27%). There was a significant association between age groups and the prevalence of any MSD, with the age group 19–24 years being less likely to report having experienced an MSD in the previous month (48%) compared to those 25–30 years (58%) and ≥35 years (65%). The majority of the participants (80%) had an operator job. Although not statistically significant, 59% of the operators reported an MSD in the previous month compared to the helper (44%) or trainee operator (39%) jobs. There was no significant association between the risk of reporting an MSD in the previous month and marital status. Likewise, there was no association between the years of education and the risk of an MSD in the previous month. However, there was a significantly higher proportion of MSDs among those not reporting having an annual physical examination or training in OSH. Participants with extended working hours were significantly more likely to report an MSD in the previous month (p-value <0.001).
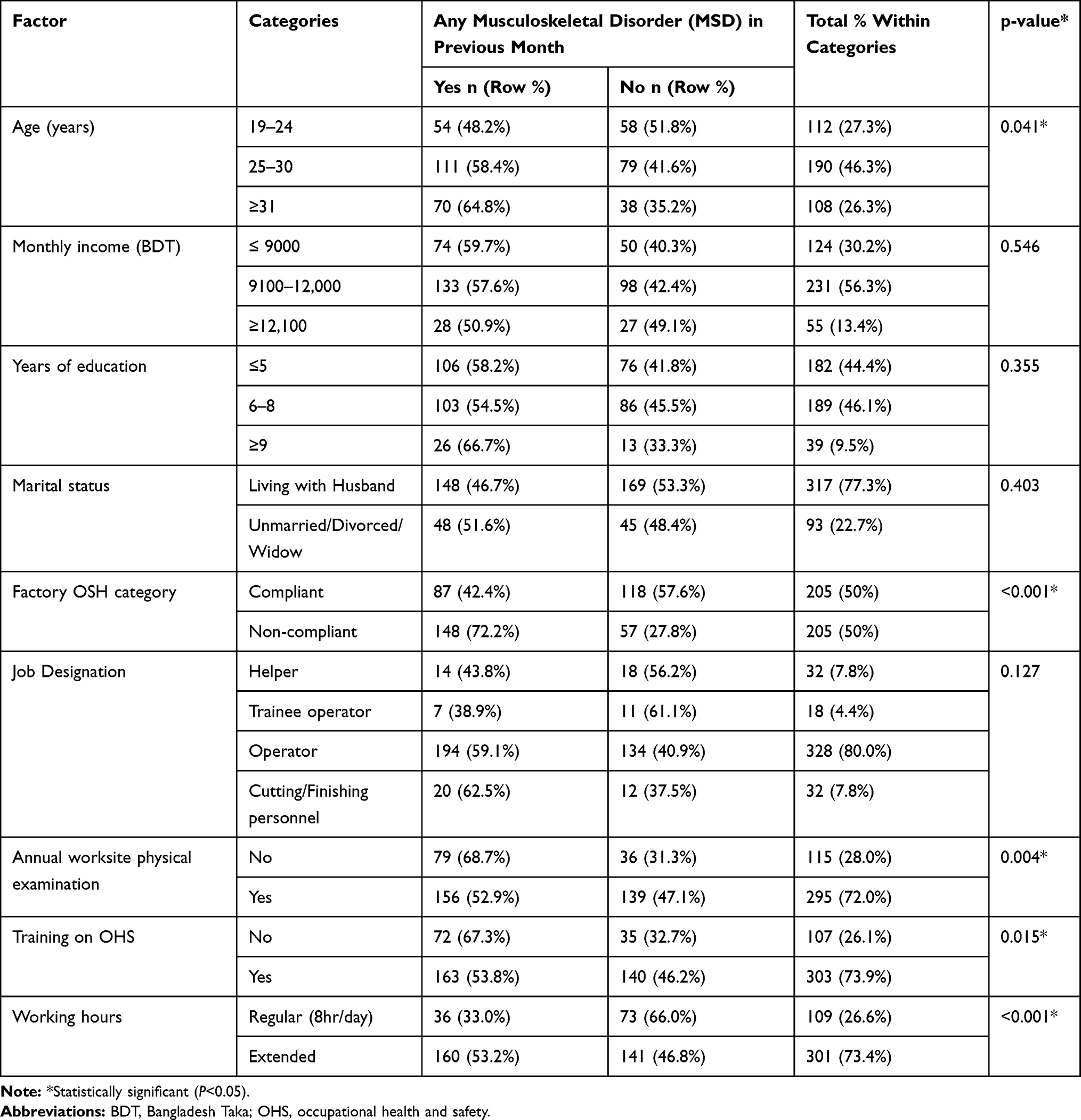 |
Table 3 Stratified Analysis of the Prevalence of Any MSD in the Previous Month by Socio-Demographic and Work-Related Factors |
Multivariable Analysis
In the multivariable analysis, the relationship between potential associated factors and MSDs showed that factory category, age and working hours increased the risk of musculoskeletal disorders among female RMG workers (Table 4). In addition, those working in the compliant factory were significantly less likely to develop an MSD in the neck or shoulder, back (upper or lower) or leg (knee/ankle/hip) region. MSDs of the hand and arm were not significantly associated with factory compliance category. Moreover, workers who worked regular working hours were less likely to develop any MSD. The risk of developing any MSD or a neck/shoulder MSD was significantly higher for the age group 25–30 years and the age group ≥31 years. Age was also found significantly associated with the development of an MSD of the leg region for those over 31 and for the arm region for those 25–30.
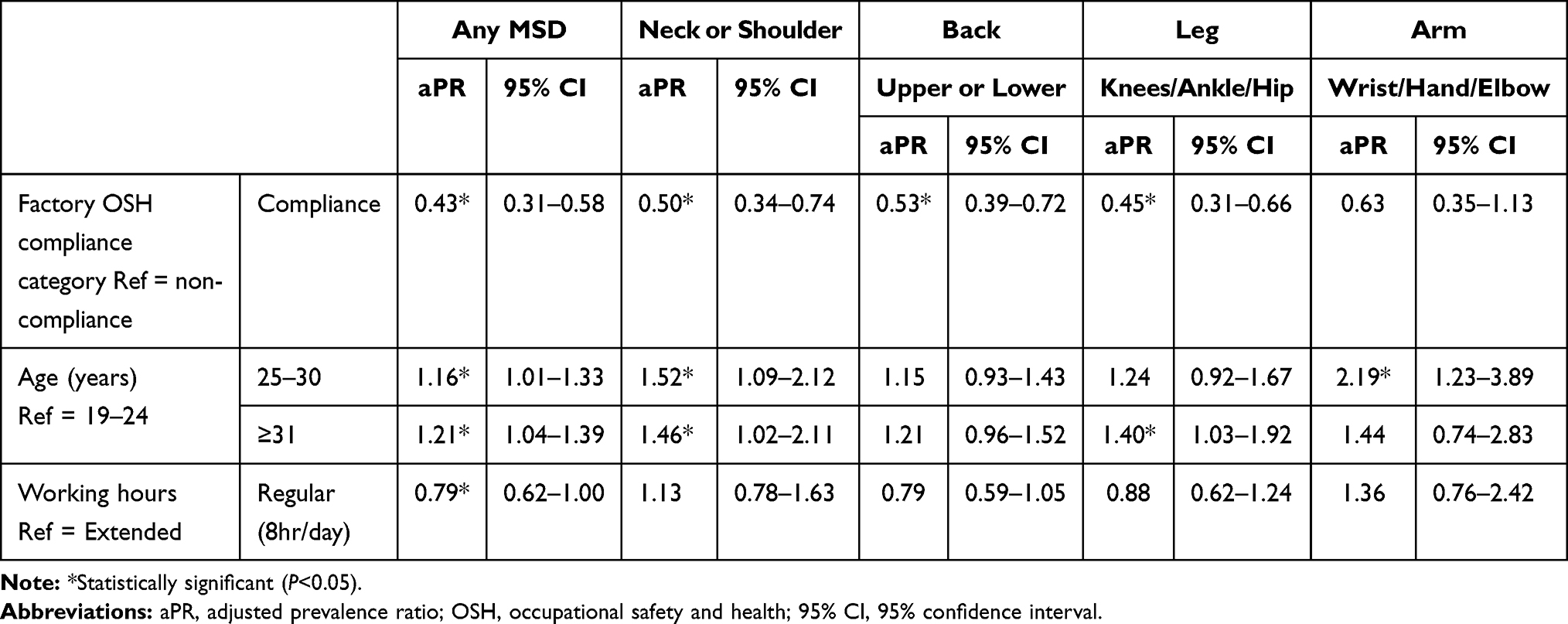 |
Table 4 Robust Poisson Regression for Self-Reported Musculoskeletal Disorders in the Past Month Associated with Factory OSH Compliance Category, Age and Working Hours Among Female Bangladeshi RMG Workers |
Discussion
This study has shown that MSDs are a major health problem among female readymade garment (RMG) workers in Bangladesh. The one-month prevalence of any MSD was 57%. The previous two studies in Bangladesh showed that the prevalence of MSDs among RMG workers was 60%,31 and 57%, respectively.32 Another study in Bangladesh found that the one-month prevalence of musculoskeletal complaints among Bangladeshi full-time bank workers was 57%.33 By comparison, the one-year prevalence rate of MSDs among Iranian official workers was 55%,27 among Iranian steel workers was 61%,34 and among Thai full-time office workers was 63%.35 MSDs have been shown to be responsible for worker’s disability and have considerable economic consequences due to the loss of wages, health expenses, and efficiency losses, particularly in developing countries.27
In this study, the one-month prevalence of lower back pain was 41%, pain in the knees was 33% and neck pain was 28%. However, research conducted among Cambodian RMG workers showed that among MSDs, neck pain was the leading MSD with a 12-month prevalence of 72% followed by lower back pain (62%).36 Similar to the findings of this study, a study conducted among Sri Lankan female RMG workers suggested that among MSDs, lower back pain was the leading MSD with a twelve-month prevalence of 57%, followed by knee pain 31%.37 However, two other studies conducted among Bangladeshi RMG workers found that the prevalence of lower back pain was 24% and 38%, respectively.3,38 Other studies have suggested that possible explanations for the prominence of back, neck and knee pain are the presence of risk factors such as extended work hours, non-neutral working postures, duration of employment, and older age.27,38,39
This study also investigated the association between work-related factors and MSDs. It appears from the findings that working in OSH compliant factory acts as a protective factor for the development of MSDs among the female RMG workers. Moreover, this study found evidence suggesting that workers who work for regular working hours (8 hrs per day) were less likely to develop MSDs. Earlier Bangladeshi studies reported extended working hours and awkward postures were significantly associated with the risk of MSDs.3,38 Research conducted among the Thai garment workers,21 Ethiopian garment workers,20 Korean wage and hotel workers also reported that extended working hours are a risk factor for the development of MSDs.40,41 Noncompliant factories are characterized by poor working environments, including the lack of basic occupational safety and health measures. Workers often work for extended hours in awkward postures doing repetitive work on machines with vibration, while the compliant factories strictly maintain regular working hours with health examination and OSH safety measures.42 These factors may contribute to the difference between the compliant and non-compliant factory in terms of the development of MSDs among the female workers, and may explain why the addition of working hours to the multivariable model did not reach statistical significance (potential co-linearity). In this study, increasing age was found to be a significant risk factor for the development of any MSD. Studies conducted in Bangladesh,3,31,38 Sri Lanka,37 Nepal,43 and Thailand21 among RMG workers also reported that an increase in age is associated with the development of MSDs.
Limitations
The limitations of this study include its cross-sectional nature, potential recall bias, the reliance on self-report of MSDs and lack of information on the extent of pain or disability of the MSD. In this study, no data were collected on the role of psychosocial factors such as job demands, workplace monotony, social support, or job satisfaction. All of which have been reported in other research studies to be important risk factors for developing MSDs.44,45 This study found that an important protective factor for MSDs was factory OSH compliance status. However, in this study compliant factories were larger in worker population size (Table 2), which may reflect underlying factors such as factory arrangement, task and equipment design and degree of automation, rather than simply OSH compliance status.
Conclusion
The study found a high burden of musculoskeletal disorders among female RMG workers in Bangladesh, with lower back pain being the most common complaint. The high prevalence of MSDs may result in significant absenteeism and loss of productivity in the RMG industry and should be evaluated. Moreover, the results indicate working in an OSH compliant factory is a protective factor for the development of MSDs. There was an indication that having regular working hours (8 hrs/day), which is a common practice in compliant factories, is also a protective factor. However, an increase in age found to be a risk factor for the development of MSDs among these female RMG workers. To reduce the burden of MSDs, it is important to identify appropriate interventions including improvement of the working environment such as an ergonomic, adjustable work station, environmental controls, work rotation and breaks, and low-cost work-related welfare in order to sustain the pace of development in this sector in Bangladesh.
Data Sharing Statement
The dataset of the current study will be made available upon request.
Ethical Approval and Consent
This research protocol was approved by the Ethics Committee of Human Research, Faculty of Public Health, Mahidol University, Thailand (Protocol No. MUPH 120/2018). Participants gave informed written consent prior to data collection which was approved by the ethical review committee. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We acknowledge the female Readymade Garment workers who generously gave up their time to participate in this study. The authors would also like to thank the factory owners support during the current study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors gave their final approval and agree to be accountable for all aspects of the work.
Funding
The current study is self-funded and we declare that no external funds from any organization/s has been received for performing the study or for the dissemination of the findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chung YC, Hung CT, Li SF, et al. Risk of musculoskeletal disorder among Taiwanese nurses cohort: a nationwide population-based study. BMC Musculoskelet Disord. 2013;14:14. doi:10.1186/1471-2474-14-144
2. Smith D, Kondo N, Tanaka E, Hirasawa K, Yamagata Z. Musculoskeletal disorders among hospital nurses in rural Japan. Rural Remote Health. 2003;3(4). doi:10.22605/rrh241
3. Hossain MD, Aftab A, Al Imam MH, et al. Prevalence of work related musculoskeletal disorders (WMSDs) and ergonomic risk assessment among readymade garment workers of Bangladesh: a cross sectional study. PLoS One. 2018;13(7):e0200122. doi:10.1371/journal.pone.0200122
4. Gopinadh A, Devi KNN, Chiramana S, Manne P, Sampath A, Babu MS. Ergonomics and musculoskeletal disorder: as an occupational hazard in dentistry. J Contemp Dent Pract. 2013;14(2):299–303. doi:10.5005/jp-journals-10024-1317
5. Choobineh A, Tabatabaei SH, Mokhtarzadeh A, Salehi M. Musculoskeletal problems among workers of an Iranian rubber factory. J Occup Health. 2007;49(5):418–423. doi:10.1539/joh.49.418
6. Badley EM, Rasooly I, Webster GK. Relative importance of musculoskeletal disorders as a cause of chronic health problems, disability, and health care utilization: findings from the 1990 Ontario Health Survey. J Rheumatol. 1994;21(3):505–514.
7. Shazzad MN, Ahmed S, Haq SA, et al. Musculoskeletal symptoms and disorders among 350 garment workers in Bangladesh: a cross-sectional pilot study. Int J Rheum Dis. 2018;21(12):2063–2070. doi:10.1111/1756-185X.13423
8. Ghosh T, Das B, Gangopadhyay S. Work-related musculoskeletal disorder: an occupational disorder of the goldsmiths in India. Indian J Community Med. 2010;35(2):321–325. doi:10.4103/0970-0218.66890
9. Gallagher S, Heberger JR. Examining the interaction of force and repetition on musculoskeletal disorder risk: a systematic literature review. Hum Factors. 2013;55(1):108–124. doi:10.1177/0018720812449648
10. Islam MF. Job dissatisfaction of Bangladeshi garment workers: identification of causes & remedies. Stamford J Econ. 2015;2(1):114–127.
11. Alam MN, Azim MT, Alias RB. Social compliance in ready-made garment industry in Bangladesh: challenges for HR personnel. J Appl Environ Biol Sci. 2017;7(10):8–18.
12. Baral LM. Comparative study of compliant & non-compliant RMG factories in Bangladesh. Int J Eng Technol. 2010;10(2):119–131.
13. Rahman MA, Hossain MS. Compliance practices in Garment industries in Dhaka City. J Bus Technol. 1970;5(2):71–87. doi:10.3329/jbt.v5i2.9936
14. amfori BSCI. Amfori BSCI Code of Conduct; 2017:1–9.
15. Supplier Ethical Data Exchange. Code of conduct acceptance programme; 2020 [June 07, 2020]. Available from: https://www.sedex.com/our-services/supplier-code-conduct/.
16. Production WRA. Certification Process; 2020 [June 06, 2020]. https://wrapcompliance.org/certification/.
17. Initiative for Compliance and Sustainability. ICS social and environmental code of conduct; 2020. [June 08, 2020].
18. Islam LN, Sultana R, Ferdous KJ. Occupational health of the garment workers in Bangladesh. J Environ. 2014;1(1):21–24.
19. Reinecke J, Donaghey J. After Rana Plaza: building coalitional power for labour rights between unions and (consumption-based) social movement organisations. Organization. 2015;22(5):720–740. doi:10.1177/1350508415585028
20. Kebede Deyyas W, Tafese A. Environmental and organizational factors associated with elbow/forearm and hand/wrist disorder among sewing machine operators of garment industry in Ethiopia. J Environ Public Health. 2014;2014:1–8. doi:10.1155/2014/732731
21. Chaiklieng S, Suggaravetsiri P, Puntumetakul R. Prevalence and risk factors for work-related shoulder pain among informal garment workers in the northeast of Thailand. Small Enterp Res. 2014;21(2):180–189. doi:10.1080/13215906.2014.11082086
22. Bangladesh Garment Manufacturers and Exporters Association. Members List; 2019 [February01, 2019]. Available from: https://www.bgmea.com.bd/page/member-list.
23. Crawford JO. The Nordic Musculoskeletal Questionnaire. Occup Med (Chic Ill). 2007;57(4):300–301. doi:10.1093/occmed/kqm036
24. Sombatsawat E, Luangwilai T, Ong-artborirak P, Siriwong W. Musculoskeletal disorders among rice farmers in Phimai District, Nakhon Ratchasima Province, Thailand. J Health Res. 2019;33(6):494–503. doi:10.1108/JHR-01-2019-0009
25. Sikiru L, Hanifa S. Prevalence and risk factors of low back pain among nurses in a typical Nigerian hospital. Afr Health Sci. 2010;10(1):26–30.
26. Zayed HA, Saied SM, El-sallamy R, Shehata WM. Work-related musculoskeletal disorders among nursing staff of Tanta University Hospitals: pattern, risk factors, and coping strategies. Egypt J Community Med. 2019;37(4):51–61. doi:10.21608/ejcm.2019.54290
27. Mozafari A, Vahedian M, Mohebi S, Najafi M. Work-related musculoskeletal disorders in truck drivers and official workers. Acta Med Iran. 2015;53(7):432–438.
28. Cromie JE, Robertson VJ, Best MO. Work-related musculoskeletal disorders in physical therapists: prevalence, severity, risks, and responses. Phys Ther. 2000;80(4):336–351. doi:10.1093/ptj/80.4.336
29. Campo M, Weiser S, Koenig KL, Nordin M. Work-related musculoskeletal disorders in physical therapists: a prospective cohort study with 1-year follow-up. Phys Ther. 2008;88(5):608–619. doi:10.2522/ptj.20070127
30. Textor J, van der Zander B, Gilthorpe MS, Liśkiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package “dagitty”. Int J Epidemiol. 2016;45(6):1887–1894. doi:10.1093/ije/dyw341
31. Jahan N, Das M, Mondal R, et al. Prevalence of musculoskeletal disorders among the Bangladeshi garments workers. SMU Med J. 2015;(2).
32. Ahmad SA, Sayed M, Khan MH, et al. Musculoskeletal disorders and ergonomic factors among the Garment Workers. J Prevent Soc Med. 2007;26(2):97–110.
33. Ali M, Ahsan GU, Uddin Z, Hossain A. Road traffic delays and musculoskeletal health complaints among full-time bank employees: a cross-sectional study in Dhaka city. bioRxiv. 2019. doi:10.1101/763052
34. Aghilinejad M, Choobineh AR, Sadeghi Z, Nouri MK, Bahrami Ahmadi A. Prevalence of musculoskeletal disorders among Iranian Steel Workers. Iran Red Crescent Med J. 2012;14(4):198–203.
35. Janwantanakul P, Pensri P, Jiamjarasrangsri V, Sinsongsook T. Prevalence of self-reported musculoskeletal symptoms among office workers. Occup Med (Chic Ill). 2008;58(6):436–438. doi:10.1093/occmed/kqn072
36. Van L, Chaiear N, Sumananont C, Kannarath C. Prevalence of musculoskeletal symptoms among garment workers in Kandal province, Cambodia. J Occup Health. 2016;58(1):107–117. doi:10.1539/joh.15-0100-fs
37. Lombardo SR, Vijitha de Silva P, Lipscomb HJ, Østbye T. Musculoskeletal symptoms among female garment factory workers in Sri Lanka. Int J Occup Environ Health. 2012;18(3):210–219. doi:10.1179/1077352512Z.00000000029
38. Hossain A. Prevalence and occupational factors associated with low back pain among the female garment workers: a cross-sectional study in Bangladesh. Glob Perspect Med Sci. 2018;2(1):8. doi:10.26535/gpms.v2i1.10
39. Li JY, Sheng W, He LH, et al. Risk factors of low back pain among the Chinese occupational population: a case-control study. Biomed Environ Sci. 2012;25(4):421–429.
40. Lee J-G, Kim GH, Jung SW, Kim SW, Lee J-H, Lee K-J. The association between long working hours and work-related musculoskeletal symptoms of Korean wage workers: data from the fourth Korean working conditions survey (a cross-sectional study). Ann Occup Env Med. 2018;30(1). doi:10.1186/s40557-018-0278-0
41. Lee JW, Lee JJ, Mun HJ, Lee K-J, Kim JJ. The relationship between musculoskeletal symptoms and work-related risk factors in hotel workers. Ann Occup Environ Med. 2013;25(1). doi:10.1186/2052-4374-25-20
42. Chowdhury MMH, Dewan MNA, Quaddus MA. Sustainable supply chain management through compliance of stakeholders’ requirements: a study on ready-made garment (RMG) industry of Bangladesh. Pac Asia Conf Inf Sys. 2013.
43. Paudyal P, Ayres JG, Semple S, Macfarlane GJ. Low back pain among textile workers: a cross-sectional study. Occup Med (Chic Ill). 2013;63(2):129–134. doi:10.1093/occmed/kqs231
44. Ng YM, Voo P, Maakip I. Psychosocial factors, depression, and musculoskeletal disorders among teachers. BMC Public Health. 2019;19(1):234. doi:10.1186/s12889-019-6553-3
45. Smith DR, Leggat PA, Speare R. Musculoskeletal disorders and psychosocial risk factors among veterinarians in queensland, Australia. Aust Vet J. 2009;87(7):260–265. doi:10.1111/j.1751-0813.2009.00435.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.