Back to Journals » International Journal of General Medicine » Volume 18
Factors Associated With Multi-Drug Resistant Organisms Among Bronchiectasis Patients: A Retrospective Study of Bronchiectasis Patients in Jordan
Authors Al Oweidat K ![]() , Toubasi AA, Khraisat FA
, Toubasi AA, Khraisat FA ![]() , Al-Sayegh TN, Al-Harasis LM, Albtoosh AS
, Al-Sayegh TN, Al-Harasis LM, Albtoosh AS
Received 4 October 2024
Accepted for publication 15 January 2025
Published 25 January 2025 Volume 2025:18 Pages 391—402
DOI https://doi.org/10.2147/IJGM.S490196
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Khaled Al Oweidat,1 Ahmad A Toubasi,2 Farah A Khraisat,2 Thuraya N Al-Sayegh,2 Layla M Al-Harasis,3 Asma S Albtoosh1
1Department of Respiratory and Sleep Medicine, Department of Internal Medicine, School of Medicine, The University of Jordan, Amman, Jordan; 2Faculty of Medicine, The University of Jordan, Amman, Jordan; 3Faculty of Medicine, the Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Ahmad A Toubasi, Faculty of Medicine, the University of Jordan, Amman, 11942, Jordan, Tel +962798035061, Email [email protected]
Background: Bronchiectasis, a respiratory ailment, significantly impacts the life expectancy of individuals. This study aimed to explore the prevalence of multidrug-resistant organisms (MDROs) among bronchiectasis patients, the resistance patterns within various antibiotic classes, and the associated factors with these organisms.
Methods: A retrospective observational analysis was conducted on adult bronchiectasis patients attending clinics at Jordan University Hospital. The diagnosis of bronchiectasis was established through lung Computerized Tomography (CT) scans and clinical symptom assessment.
Results: The study encompassed 235 patients, revealing a notably higher occurrence of MDROs among non-cystic fibrosis patients compared to their counterparts (P-value=0.001). Additionally, MDROs showed significant associations with the usage of inhaled beta agonists, anti-cholinergics, corticosteroids, and inhaled antibiotics (P-value< 0.050). Patients with MDROs experienced a significantly elevated mean number of hospitalizations, exacerbations, and antibiotic courses compared to their counterparts (P-value< 0.050). Moreover, those with MDROs exhibited a higher incidence of requiring O2 device support and faced an increased risk of mortality (P-value< 0.050).
Conclusion: The observational nature of our study limits the associations in our study. However, we provided evidence that it is imperative for clinicians to assess their bronchiectasis patients for MDRO risk factors, facilitating appropriate initial antibiotic selection. Nevertheless, the validation of MDRO risk factors necessitates further exploration through larger studies with extended follow-up periods.
Keywords: human, respiratory diseases, bronchiectasis, antibiotic resistance, microbiology
Introduction
Bronchiectasis, a chronic and severe lung condition, manifests through a persistent cough, excessive sputum, and recurrent chest infections, often accompanied by wheezing, chest pain, and systemic symptoms.1 Computed tomography scans are used to confirm the diagnosis, which is based on the persistent dilatation of the bronchi as seen radiographically.2 A computed tomography scan confirms the diagnosis.2 When an underlying cause cannot be identified in around half of the cases, bronchiectasis is divided into two categories: cystic fibrosis and non-cystic fibrosis.1 Inhaled corticosteroids, bronchodilators, physical therapy, patient education, and long-term antibiotics are all part of the care of bronchiectasis.1
Multidrug-resistant (MDR) microorganisms represent a serious danger to global health, increasing morbidity and death and placing a heavy financial strain on healthcare systems.3 These drug-resistant infections, which are frequently linked to antibiotic misuse, can originate from nosocomial as well as community-acquired sources.4 MDR infections are more common in patients with long-term respiratory conditions, such as bronchiectasis, than in the general population.5 Haemophilus influenzae, Streptococcus pneumoniae, Pseudomonas aeruginosa, and, to a lesser extent, Enterobacteriaceae are common MDR pathogens in bronchiectasis patients.6 Because there are few antibiotic choices available, the emergence of multidrug resistant (MDR) organisms is a major and potentially fatal worry. Among patients with bronchiectasis, Pseudomonas aeruginosa and extended-spectrum beta-lactamase (ESBL) Enterobacteriaceae are commonly found.6
Previous studies in western countries demonstrated that the prevalence of MDR was 20% with the most prevalent organism being pseudomonas aeruginosa followed methicillin resistant staphylococcus aureus (MRSA) while data from eastern countries suggest that MRSA and ESBL Klebsiella pneumoniae are more common than pseudomonas aeruginosa suggesting variation in the prevalence of MDR and the organisms associated with it.
Despite a scarcity of studies exploring the risk factors for MDR microorganisms in bronchiectasis patients, particularly in the Middle East, this study was initiated to address this critical gap.6 The research intends to investigate the characteristics related with the isolation of multi-drug resistance bacteria during bronchiectasis exacerbations and evaluate their clinical impact on outcomes, taking into account the fact that risk factors can differ depending on geographic locations, genetics, and ethnicity. The theory suggests that routine therapies and previous medical interactions are associated with MDR exacerbations, and that reducing the use of unnecessary antibiotics may be made easier by having a better understanding of these aspects.
Methods
We carried up a retrospective observational analysis of adult patients with bronchiectasis who visited our clinics between 2014 and 2022 at the Jordan University Hospital (JUH), a tertiary referral university hospital in Amman, Jordan. Patients from primary care, other hospitals, other specializations, or any other medical facilities are referred to our particular specialist clinic. A Computerized Tomography (CT) scan of the lungs and clinical signs were used to diagnose bronchiectasis. Patients who had their first exacerbation and needed hospitalization or antibiotic therapy were included in our study; any further exacerbations were excluded from the analysis. Ages under eighteen and severe immunosuppression, including those undergoing chemotherapy or immunosuppressive medication, as well as cancer patients, were the exclusion criteria.
This study was conducted in concordance with human ethical practices and the declaration of Helsinki. The Institutional Review Board (IRB) at the University of Jordan approved the conductance of this study and waived the need for informed consent (IRB# 10/2022/2493).
Study Protocol
Data on the patients’ smoking habits, demographics, and concomitant conditions—such as diabetes, asthma, COPD, heart disease, kidney, liver, and history of tuberculosis infection—were gathered. Additionally, information was gathered on the number of antibiotic courses used in the preceding year, the number of bronchiectasis exacerbations that occurred in the previous year, and the FACED scores for bronchiectasis. Proton pump inhibitors, corticosteroids, theophylline, inhaled/nebulized antibiotics, bronchodilators, and other chronic and concurrent medication use were noted.
Exacerbation Definition and Follow-up
Exacerbation was characterized as a sudden alteration in sputum attributes (such as heightened volume, alterations in viscosity, or increased purulence), accompanied by or without escalated dyspnea, subsequent to the exclusion of other potential causes. This also involved the necessity for a new antibiotic regimen or hospitalization. The decision to admit to the hospital, Intensive Care Unit (ICU) admission, and the utilization of oxygen-related devices, including intubation, was at the discretion of the attending physician. Throughout the exacerbation episode, data collection included information on complications, both invasive and noninvasive mechanical ventilation, and 1-year mortality. The duration of hospitalization was documented for patients admitted to the hospital.
Microbiological Evaluation and Diagnosis
The microbiological diagnosis relied on sputum samples. A sputum sample was deemed acceptable if it exhibited more than 25 leukocytes and fewer than 10 squamous cells per low-power microscope field. The identical methodologies employed in prior publications were applied for confirming the presence of microorganisms.7 The Kirby-Bauer disk diffusion method was utilized to assess antimicrobial susceptibility, employing either Muller-Hinton or sheep blood agar based on the growth requirements of the microorganism. The resistance was determined based on the zone inhibition diameter using the standardized charts for each antibiotic. Multidrug Resistant Organisms (MDROs) were classified according to the criteria set by the Centers for Disease Control and Prevention (CDC) which defined MDRO as microorganisms, primarily bacteria, exhibiting resistance to one or more classes of antimicrobial agents.8
Data Analysis
Patient data was inputted into Microsoft Office Excel 2019 and subsequently imported into IBM SPSS v.25 software for analysis. Continuous variables were presented as mean and standard deviation, while categorical variables were expressed as counts and percentages. The comparison between patients with Multidrug Resistant Organisms (MDROs) in their cultures and those without was conducted using the chi-square test and T-test, as deemed appropriate. A P-value below 0.05 was considered statistically significant for all the conducted tests.
Results
Characteristics of the Included Patients
Among the 235 patients included, 52.8% were male, with a mean age of 58.57 ± 19.37 years. Additionally, 11.4% were smokers. Hypertension was present in 50.8% and diabetes in 44.3% of the patients. COPD and asthma were reported in 14.4% and 27.5% of the patients, respectively. Furthermore, 17.9% had pulmonary hypertension, and 1.3% had a history of pulmonary tuberculosis. The majority (86.8%) had non-cystic fibrosis bronchiectasis. Commonly used medications included inhaled corticosteroids (71.9%), beta agonists (69.8%), and oral antibiotics (61.3%). The average number of hospitalizations and exacerbations in the last year was 0.61 ± 1.27 and 0.80 ± 1.59, respectively. On average, patients received 0.78 ± 1.61 courses of antibiotics in the last year, with a mean FEV1 of 73.84 ± 26.34. The mean FACED score was 3.05 ± 1.95. Table 1 describes the characteristics of the included patients.
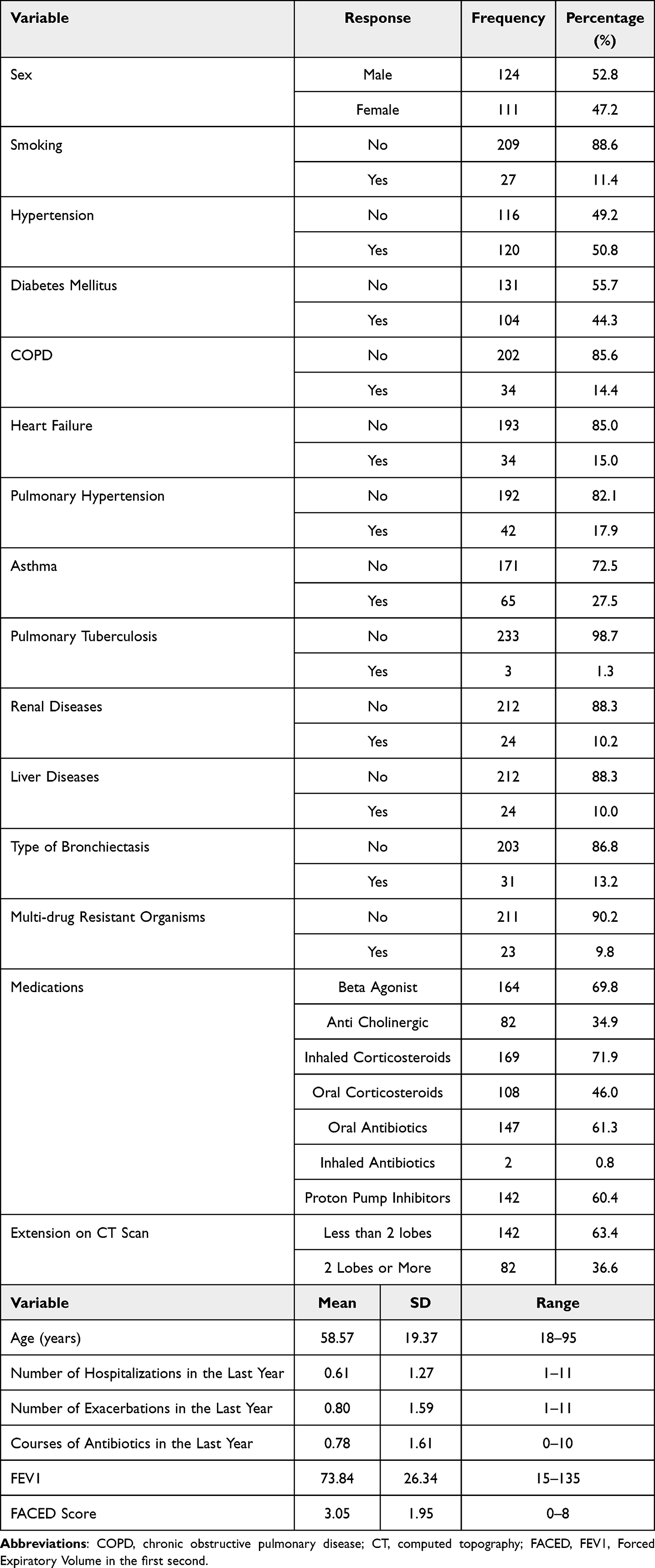 |
Table 1 The General Demographics of the Participants |
Patients Outcomes in the Hospitalization
Complications during hospitalization occurred in 36.9% of patients, with 10.1% requiring admission to the ICU. Additionally, 28.9% needed O2 support, and 4.6% required intubation. The mean total length of hospital stay was 6.56 ± 9.00 days, with 5.6% mortality (Table 2).
 |
Table 2 Patients Outcomes in the Hospitalization |
Microbiological Profile and Antibiotic Resistance Patterns of the Patients’ Culture
The most commonly isolated microorganisms from patient cultures were Candida albicans (20%), Pseudomonas aeruginosa (7%), and Staphylococcus aureus (3%) (Figure 1). MDROs were found in 9.8% of cultures, with Pseudomonas aeruginosa (70%), Candida albicans (48%), and Staphylococcus aureus (22%) being the most common (Figure 2). Resistance was most frequently observed against beta-lactams (6%), quinolones (4%), and glycopeptides (Figure 3).
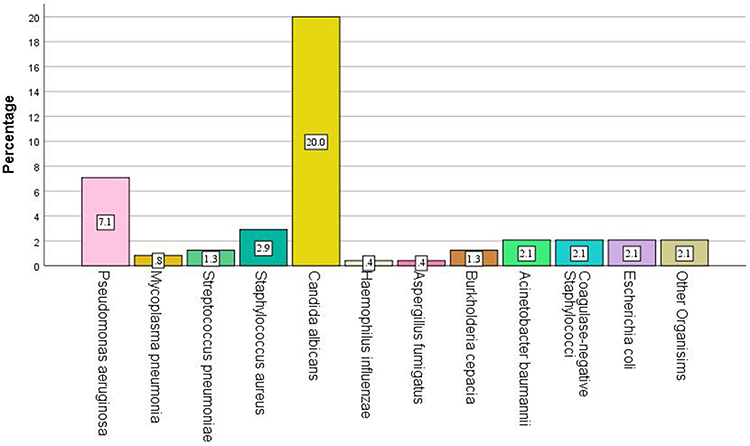 |
Figure 1 Distribution of Microorganisms in Patients Cultures. |
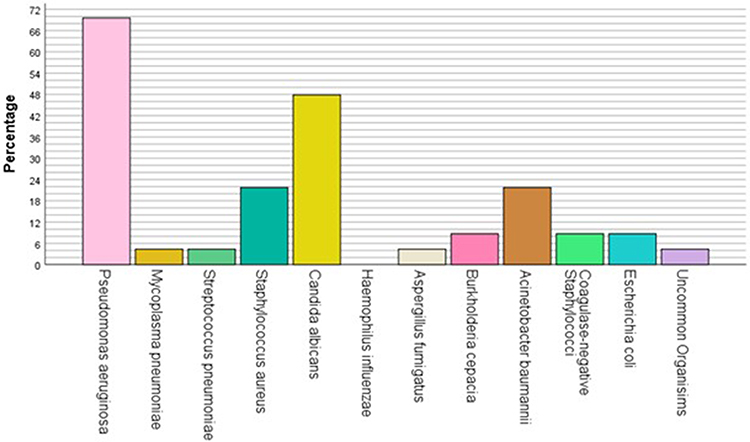 |
Figure 2 MDROs Isolated from the Patients Cultures. The resistance was determined based on the zone inhibition diameter using the standardized charts for each antibiotic. Multidrug Resistant Organisms (MDROs) were classified according to the criteria set by the Centers for Disease Control and Prevention (CDC) which defined MDRO as microorganisms, primarily bacteria, exhibiting resistance to one or more classes of antimicrobial agents. |
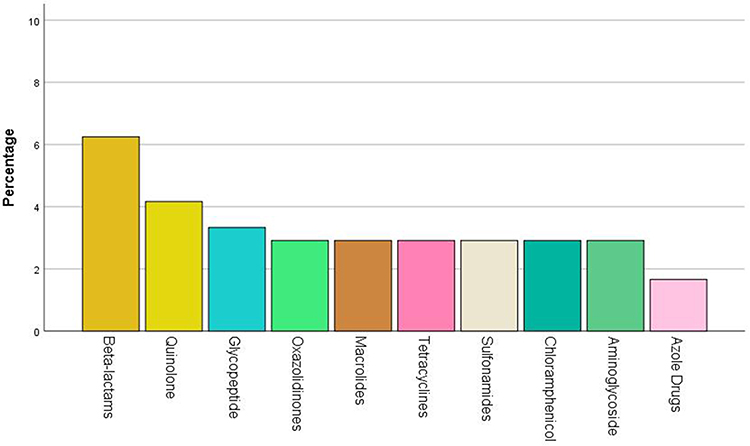 |
Figure 3 Patterns of Resistance across Antibiotics Classes. |
Differences Between Patients Who Had MDRs and Patients Who Did Not Have MDRs in Their Cultures
In the analysis regarding the differences between patients who had MDROs and patients who did not have it, MDROs was significantly more common among non-cystic fibrosis patients (65.2%) compared to their counterparts (34.8%) (P-value=0.001). Furthermore, MDROs were significantly associated with the use of inhaled beta agonists, anti-cholinergics and corticosteroids (P-value=0.017, 0.005, 0.028). The majority of the patients who had MDROs were using inhaled beta agonists (91.3%), anti-cholinergic (60.9%) and corticosteroids (91.3%). In comparison, patients who did not have MDROs were using inhaled beta agonists (67.1%), anti-cholinergic (31.4%) and corticosteroids (69.5%) in lower percentage. Moreover, patients with MDROs had a significantly higher percentage of inhaled antibiotics use (4.3%) compared to their counterparts (0.5%) (P-value=0.050). Also, patients with MDROs needed O2 devices support in higher percentage (47.8%) compared to the other group (27.1%) (P-value=0.038). Furthermore, significantly higher percentage of patients with MDROs died (17.4%) compared to patients without MDROs (4.4%) (P-value=0.010). The mean number of hospitalization and exacerbations was significantly higher among patients with MDROs compared to their counterparts (P-value=0.000, 0.004). In addition, patients with MDROs had significantly higher mean number of antibiotic courses used in the last year before the culture (1.83 ± 2.33) compared to the other group (0.66 ± 1.47) (P-value=0.001) (Table 3).
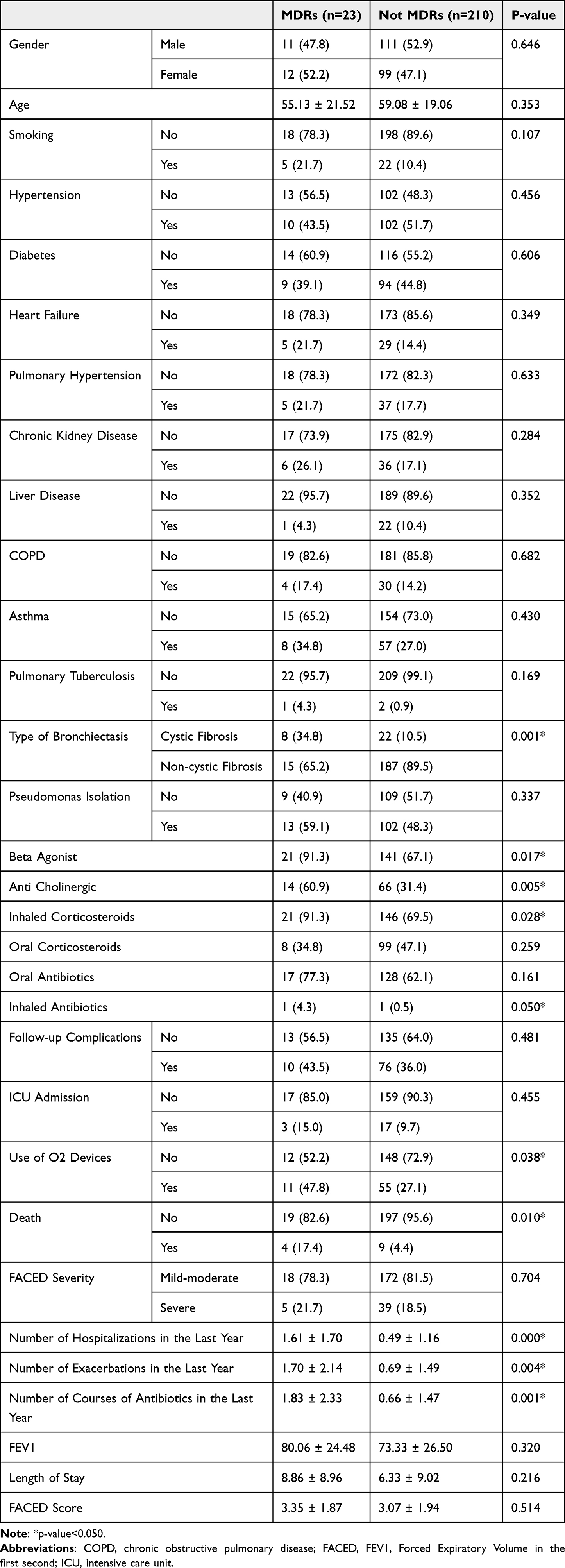 |
Table 3 Differences in the Demographics Between Patients Who Had MDRs Cultures and Patients Who Did Not |
Discussion
Bronchiectasis, a respiratory condition, has a considerable impact on both life expectancy and quality of life,9 placing significant economic burdens on healthcare systems.10 Various factors, including multidrug-resistant organisms (MDROs), have been recognized in the literature as contributors to increased morbidity and mortality among patients with bronchiectasis.9 The main aim of this study was to examine the prevalence of MDROs among individuals with bronchiectasis, analyze resistance patterns across different antibiotic classes, and investigate the factors associated with the presence of these organisms.
The overall mortality for the disease one year after exacerbation was estimated at 3%.11 However, the mortality rates escalated to over 10% after 5 years post-diagnosis and surpassed 20% after more than 10 years of follow-up.12,13 In our cohort, the 1-year mortality following exacerbation was 5.6%, aligning with literature reports that range from 3% to 6%.11,13 Candida albicans, Pseudomonas aeruginosa, and Staphylococcus aureus were identified as the most frequently isolated organisms during exacerbations.
Regarding the prevalence of Multidrug Resistant Organisms (MDROs), our study found a rate of 9.8% among patients’ cultures. A previous study conducted in Bangladesh reported a higher rate of 34%,14 and another study in Spain found a rate of 20%.6 The lower prevalence of MDROs might stem from the characteristics of our population as our population is considered younger with lower prevalence of comorbidities which reduce the prevalence of MDROs. However, systematic review and meta-analysis indicated a 13% MDRO rate in bronchiectasis patients, consistent with our findings.15 Additionally, a multicentric study involving 3193 patients demonstrated a MDRO rate of less than 10%.16 The variability in the literature regarding MDRO rates may be attributed to differences in sample sizes, the types of pneumonia leading to exacerbations, and the guidelines used to define MDROs.15 The systematic review highlighted that studies including patients with exacerbations due to hospital-acquired pneumonia and ventilator-acquired pneumonia reported higher MDRO rates.15 In our analysis, Pseudomonas aeruginosa emerged as the most prevalent MDRO, followed by Candida albicans and Staphylococcus aureus. This aligns with previous research emphasizing Pseudomonas aeruginosa as the predominant isolate in bronchiectasis patients.11,17,18 However, it’s crucial to note that Candida albicans was not consistently considered in many of these studies. Furthermore, our analysis revealed that MDROs exhibited resistance to beta-lactams, quinolones, and glycopeptides, consistent with previous analyses where these antibiotics were commonly resisted, especially among respiratory pathogens.19 The pathophysiology underlying MDROs in bronchiectasis patients is hypothesized to arise from alterations in the lower airways, promoting shifts in microbiota and the emergence of pathogenic microorganisms.20 This disruption initiates a cycle of tissue damage, infection, immune responses, and inflammation, leading to the emergence of hypermutant microorganisms.20 The use of antibiotics during this cycle is believed to selectively preserve organisms resistant to antibiotics, contributing to the elimination of normal microbiota.20
Our findings reveal a notably higher prevalence of multidrug-resistant organisms (MDROs) in non-cystic fibrosis bronchiectasis patients compared to those with cystic fibrosis. This disparity between the two bronchiectasis populations can be attributed to variations in colonizing organisms. Typically, Staphylococcus aureus, Pseudomonas aeruginosa, and Burkholderia cepacia complex are prevalent in cystic fibrosis bronchiectasis patients, while Haemophilus influenzae and Pseudomonas aeruginosa predominate in non-cystic fibrosis bronchiectasis cases. In our cohort, the use of inhaled antibiotics was associated with an elevated MDRO rate, consistent with findings from previous studies.6 Patients with MDROs experienced a higher average of hospitalizations and exacerbations in the preceding year, aligning with existing literature.6,14 The increased frequency of exacerbations and hospitalizations among bronchiectasis patients indicates greater disease severity, a factor considered in FACED and BSI scores.21 This heightened severity was linked to an elevated MDRO rate, contributing to the reinforcement of the vicious cycle mentioned earlier and an increase in rates of highly resistant organisms, such as Staphylococcus aureus and Pseudomonas aeruginosa.22–24 Additionally, patients with MDROs had a significantly higher average number of antibiotic courses in the past year compared to their counterparts, a phenomenon well-established in the literature where antibiotic use selectively promotes MDRO survival.20 Notably, the use of inhaled beta agonists, anticholinergics, and corticosteroids was significantly associated with higher MDRO rates. Metersky et al reported a similar association between inhaled corticosteroid use and Pseudomonas aeruginosa colonization in healthcare-associated pneumonia.25 The immunosuppressive effects of inhaled corticosteroids are recognized contributors to increased disease severity and infection incidence.25 However, it’s crucial to acknowledge that patients with more severe disease may use corticosteroids more frequently, potentially introducing channelling and confounding biases into this relationship.
Patients with Multidrug Resistant Organisms (MDROs) required the use of O2 devices more frequently during their hospital stay compared to their counterparts. Additionally, those with MDROs had a significantly higher rate of death within 1 year of the exacerbation. These findings suggest that MDROs are associated with severe exacerbations and serve as an important indicator of disease progression.
It is important to highlight that some clinical care practices such as antibiotic stewardship has a great potential in slowing the development of antibiotic resistance. An example of these practices includes accurate diagnosis of infection, correct drug or combination of drugs to target specific pathogens, proper drug dosage to achieve efficacy while limiting toxicity and appropriate treatment duration.{Shapiro, 2014 #36} In addition, it is fundamental to highlight that these practices should not be only applied in the hospital settings but also outside it as over half of outpatient antibiotic prescription might not be appropriate.{Polk, 1999 #35}
While our study is among the few in the literature investigating factors associated with MDROs in bronchiectasis patients, several limitations need acknowledgment. Firstly, the retrospective design of our study allows for associations to be inferred but not causation. Thus, future prospective cohort studies are needed to identify causal risk factors and detect disease progression. In addition, our samples were mainly sputum derived yet other sample types can be more accurate. Secondly, the single-center design restricts the generalizability of our findings. Thirdly, pathogen identification primarily relied on conventional microbiological tests, and invasive respiratory samples were only obtained if deemed necessary by the attending physician. Additionally, sputum lacked quantitative bacteriology measurements with colony counts to assess the burden of MDROs. Confounding bias is another limitation which can explain our finding about corticosteroids use and MDROs. Lastly, due to the cohort’s size, a secondary analysis to identify specific risk factors for each microorganism was not feasible.
Conclusions
In conclusion, MDROs are common among patients with bronchiectasis with a rate of around 10%. Also, we identified several risk factors associated with MDROs including non-cystic fibrosis bronchiectasis, number of exacerbations and hospitalizations in the past year, number of antibiotic courses used in the last year, the use of inhaled antibiotics, beta agonists, anti-cholinergic and corticosteroids. Additionally, we found a significant association between MDROs and increase in 1 year mortality and need of O2 devices. This data is important to guide clinicians toward the initial antibiotic therapy in exacerbations of bronchiectasis. Clinicians should apply targeted screening protocols and assess their patients regarding the risk factors of MDROs to appropriately select the initial antibiotics and to safely avoid unnecessary anti-MDROs coverage. However, further validation of MDROs risk factors by larger studies with longer periods of follow up is needed.
Data Sharing Statement
The data associated with this manuscript are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the institutional review board (IRB) of the Jordan University Hospital (JUH) (IRB#20202310192810/2022/2493) and the IRB waived the need for consent from the participants as the study only involved reviewing charts of patients without direct contact with them. This study was conducted in accordance with the declaration of Helsinki.
Patient Data Confidentiality
The patients’ data was anonymized and confidentiality was maintained all the times.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they do not have any conflict of interest.
References
1. Murray MP, Hill AT. Non-cystic fibrosis bronchiectasis. Clinical Medi. 2009;9(2):164–169. doi:10.7861/clinmedicine.9-2-164
2. Naidich DP, McCauley DI, Khouri NF, Stitik FP, Siegelman SS. Computed tomography of bronchiectasis. J Comp Assisted Tom. 1982;6(3):437–444. doi:10.1097/00004728-198206000-00001
3. Prevention CfDCa. Biggest Threats and Data: antibiotic/Antimicrobial Resistance. CDC.Available from: https://www.cdc.gov/drugresistance/biggest-threats.html.
4. Koulenti D, Fragkou PC, Tsiodras S. Editorial for Special Issue ”Multidrug-Resistant Pathogens”. Microorganisms. 2020;8(9):1383. doi:10.3390/microorganisms8091383
5. Rouzé A, Boddaert P, Martin-Loeches I, et al. Impact of Chronic Obstructive Pulmonary Disease on Incidence, Microbiology and Outcome of Ventilator-Associated Lower Respiratory Tract Infections. Microorganisms. 2020;8(2):165. doi:10.3390/microorganisms8020165
6. Menéndez R, Méndez R, Polverino E, et al. Risk factors for multidrug-resistant pathogens in bronchiectasis exacerbations. BMC Infect Dis. 2017;17(1):659. doi:10.1186/s12879-017-2754-5
7. Polverino E, Cilloniz C, Menendez R, et al. Microbiology and outcomes of community acquired pneumonia in non cystic-fibrosis bronchiectasis patients. The Journal of Infection. 2015;71(1):28–36. doi:10.1016/j.jinf.2015.03.009
8. Prevention CfDCa. Management of Multidrug-Resistant Organisms in Healthcare Settings. Available from: https://www.cdc.gov/infectioncontrol/guidelines/mdro/background.html#:~:text=importance%20of%20MDROs-,MDRO%20Definition,of%20antimicrobial%20agents%20(1).
9. Magge A, Ashraf S, Quittner AL, Metersky ML. Quality of life in patients with bronchiectasis: a 2-year longitudinal study. Ann translat Med. 2019;7(14):334. doi:10.21037/atm.2019.06.62
10. Goeminne PC, Hernandez F, Diel R, et al. The economic burden of bronchiectasis – known and unknown: a systematic review. BMC Pulm Med. 2019;19(1):54. doi:10.1186/s12890-019-0818-6
11. Huang H-Y, Chung F-T, Lin C-Y, et al. Influence of Comorbidities and Airway Clearance on Mortality and Outcomes of Patients With Severe Bronchiectasis Exacerbations in Taiwan. Original Research. 2022;8. doi:10.3389/fmed.2021.812775
12. Loebinger MR, Wells AU, Hansell DM, et al. Mortality in bronchiectasis: a long-term study assessing the factors influencing survival. Europ resp J. 2009;34(4):843–849. doi:10.1183/09031936.00003709
13. McDonnell MJ, Aliberti S, Goeminne PC, et al. Comorbidities and the risk of mortality in patients with bronchiectasis: an international multicentre cohort study. Lancet Respir Med. 2016;4(12):969–979. doi:10.1016/s2213-2600(16)30320-4
14. Chinese expert consensus on the management of lower respiratory tract infections of Pseudomonas aeruginosa in adults(2022)]. Zhonghua jie he he hu xi za zhi. 2022;45(8):739–752. doi:10.3760/cma.j.cn112147-20220407-00290
15. Chen G, Xu K, Sun F, Sun Y, Kong Z, Fang B. Risk Factors of Multidrug-Resistant Bacteria in Lower Respiratory Tract Infections: a Systematic Review and Meta-Analysis. Canad j Infectious Dis Medimicro. 2020;2020:7268519. doi:10.1155/2020/7268519
16. Villafuerte D, Aliberti S, Soni NJ, et al. Prevalence and risk factors for Enterobacteriaceae in patients hospitalized with community-acquired pneumonia. Respirology. 2020;25(5):543–551. doi:10.1111/resp.13663
17. King PT, Holdsworth SR, Freezer NJ, Villanueva E, Gallagher M, Holmes PW. Outcome in adult bronchiectasis. COPD. 2005;2(1):27–34. doi:10.1081/copd-200050685
18. Inchingolo R, Pierandrei C, Montemurro G, Smargiassi A, Lohmeyer FM, Rizzi A. Antimicrobial Resistance in Common Respiratory Pathogens of Chronic Bronchiectasis Patients: a Literature Review. Antibiotics. 2021;10(3):326. doi:10.3390/antibiotics10030326
19. Han Y, Zhang J, Zhang HZ, Zhang XY, Wang YM. Multidrug-resistant organisms in intensive care units and logistic analysis of risk factors. World Journal of clinical Cases. 2022;10(6):1795–1805. doi:10.12998/wjcc.v10.i6.1795
20. Sahuquillo-Arce JM, Méndez R, Hernández-Cabezas A, RJCAI M. Non-cystic fibrosis bronchiectasis: the long road to multidrug resistant bacteria. Com Acqu Infec. 2016;3(4):110.
21. Goeminne PC, Vandooren J, Moelants EA, et al. The Sputum Colour Chart as a predictor of lung inflammation, proteolysis and damage in non-cystic fibrosis bronchiectasis: a case-control analysis. Respirology. 2014;19(2):203–210. doi:10.1111/resp.12219
22. Jung WJ, Kang YA, Park MS, et al. Prediction of methicillin-resistant Staphylococcus aureus in patients with non-nosocomial pneumonia. BMC Infect Dis. 2013;13:370. doi:10.1186/1471-2334-13-370
23. Callejo-Torre F, Eiros Bouza JM, Olaechea Astigarraga P, et al. Risk factors for methicillin-resistant Staphylococcus aureus colonisation or infection in intensive care units and their reliability for predicting MRSA on ICU admission. Le infezioni in medicina. 2016;24(3):201–209.
24. Gallego M, Pomares X, Espasa M, et al. Pseudomonas aeruginosa isolates in severe chronic obstructive pulmonary disease: characterization and risk factors. BMC Pulm Med. 2014;14:103. doi:10.1186/1471-2466-14-103
25. Metersky ML, Frei CR, Mortensen EM. Predictors of Pseudomonas and methicillin-resistant Staphylococcus aureus in hospitalized patients with healthcare-associated pneumonia. Respirology. 2016;21(1):157–163. doi:10.1111/resp.12651
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.