Back to Journals » Infection and Drug Resistance » Volume 15
Factors Associated with Multi-Drug-Resistant Non-Typhoidal Salmonella in the Invasive Disease, Thailand
Authors Hengkrawit K, Tangjade C
Received 1 September 2022
Accepted for publication 29 October 2022
Published 10 November 2022 Volume 2022:15 Pages 6563—6576
DOI https://doi.org/10.2147/IDR.S387037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Kitchawan Hengkrawit,1 Chidchanok Tangjade2
1Pediatric Infectious Disease Unit, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, Nonthaburi, Thailand; 2Pediatrics Gastroenterology and Hepatology Unit, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, Nonthaburi, Thailand
Correspondence: Chidchanok Tangjade, Pediatrics Gastroenterology and Hepatology Unit, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, P.O. Box 222 Moo 1, Tiwanon Road, Pak Kret, Nonthaburi, 11120, Thailand, Tel +66 2 502 2345, Fax +66 2 502-2305, Email [email protected]
Purpose: Invasive non-typhoidal Salmonella disease, iNTS is a major global health concern, especially multi-drug resistant non-typhoidal Salmonella, MDR-NTS. Information about risk factors of MDR-NTS in the invasive disease patient group was limited. This study aimed to identify those risk factors.
Methods: This retrospective study examined data from patients who had non-typhoidal Salmonella, NTS infection, from 10 hospitals between June 2011 and June 2020. The multivariate regression analysis included demographic data, clinical data, culture reports, and antimicrobial susceptibility.
Results: A total of 166 patients were invasive salmonellosis. where the median age was 8.3 years (IQR 1.8– 79). 52% were the under-15-years-old group. Most of the patient data, 64.5% (107/166), was from a tertiary hospital. The majority of cases were bacteremia 95.7% (159/166). Serogroup C was the most common serogroup (39%). MDR-NTS was present in 68.8% (95% CI 7.17– 11.06) of patients. Univariate analysis showed that onset of illness > 3 days PTA (p=0.11), age over 60 years old (0.014), diabetic (p=0.002), or serogroup C infection (p=0.43) were significant factors for MDR-NTS infection. Multivariate analysis showed that the onset of symptoms more than 3 days before admission (p=0.001), and age over 60 years were significant factors. The patient who had white blood cells > 15,000 cells/uL (p< 0.001), a peak of fever ≥ 39 C° (p=001), and illness for more than 3 days before admission (p=0.035) were significantly related to invasive infection by multivariate analyses.
Conclusion: The iNTS patients who were over 60 years old or had onset of illness more than 3 days before admission were associated with MDR-NTS infection. Therefore, the choice of antimicrobials selected must be appropriate for the local prevalence and epidemiology of MDR-NTS including clinical correlation.
Keywords: risk factor, multi-drug resistance, non-typhoidal Salmonella, invasive infection, invasive non-typhoidal Salmonella disease
Introduction
Non-typhoidal Salmonella (NTS) is a common cause of infectious diarrhea. It causes invasive diseases, including bacteremia, meningitis, and other focal infections, which result in hospitalization, morbidity, and mortality.1 Some of the diseases caused by NTS which are not typically related to diarrhea are non-specific febrile illnesses with symptoms that are clinically inseparable from other febrile illnesses, which complicates diagnosis and treatment.
Previous studies have shown that malnourished infants, elderly people, sickle-cell disease, HIV, acute or recent malaria, and antimicrobial-resistant NTS are risk factors for invasive diseases, especially MDR-NTS.1–3 MDR-NTS is associated with poorer clinical outcomes and higher case fatality.4 The extended-spectrum ß-lactamases (ESBL), and AmpC ß-lactamases (AmpC) were major mechanisms of cephalosporine resistance. The mutations of the DNA gyrase enzyme are important mechanisms which are resistance to fluoroquinolone. The organisms also have gene transfers of point mutations between them, which affected to increase of MDR-NTS from more reported worldwide.4–13 Studies about risk factors associated with MDR-NTS in invasive diseases are limited, particularly in Asia. Previous studies in Africa show children younger than 5 years, elderly people (aged ≥70 years), people with HIV infection, and patients who are infected with Salmonella serogroups B (S. Typhimurium, S. Heidelberg), and D (S. Enteritidis, S. Dublin,) had more invasive infection with MDR-NTS.1,2 The studies in Thi-Qar Governorate Iraq found that children from households with domestic animals supplied with pipe water had a higher risk compared to households without them.13 In Bangladesh children under five years of age with severe malnutrition who presented with a duration of fever ≥ 5 days were at risk. However, those studies differed from Southeast Asia in population, living conditions, economic characteristics, and access to health systems. This study was conducted to determine the risk factors of MDR-NTS in invasive diseases in Thailand. This study is a continuation of a previous study of the prevalence and trend of antimicrobial susceptibility patterns of multidrug-resistant non-typhoid salmonella in the central region, 2012–2019, which is the same researcher.14
Materials and Method
Methods
This study was conducted retrospectively, by collecting patient data from ten hospitals: six district hospitals, three private hospitals, and one tertiary hospital, with permission from the hospital directors. Patients who were diagnosed with Salmonella infections based on ICD-1015 between June 2011 and June 2020 were included. The research includes patients who had invasive diseases (bacteremia, meningitis, and severe focal infections). Demographic data including age, gender, lab investigation, culture (blood, stool and/or other body fluid), and clinical, and antimicrobial susceptibility testing reports were reviewed. The patients without serogroup and/or antimicrobial sensitivity testing results were excluded.
Microbial Definition
The study reported Salmonella culture by using O antigen to classify them as serogroups A, B, C, D, and E, based on the Kauffman-White classification.15 Antimicrobial susceptibility testing was performed using the agar disk diffusion method. The antimicrobial susceptibility was interpreted according to the guidelines of the Clinical and Laboratory Standards Institute (CLSI),16 which is under control standards set by the Department of Medical Sciences in the Ministry of Public Health.17 CLSI defines drug resistance non-typhoidal Salmonella (DR-NTS) as NTS resistant to at least one class of antimicrobials. MDR-NTS was defined as acquired non-susceptibility to at least one agent in three or more antimicrobial categories.18
Statistical Methods
Descriptive statistics were used to analyze demographic data and prevalence. The differentiation between groups was analysed by Pearson’s Chi-square and 95% confidence interval. The quantitative data analyses use multivariate. SPSS version 21 was used as the analysis tool.
Results
The Prevalence and Characteristics of Invasive Disease
A total of 166 (38.3%) from 433 NTS were diagnosed with invasive disease. The median age of these patients was 8.3 years, IQR (1.8–47). The patients with invasive diseases were subdivided into three age groups: <15 years 52.4% (n= 87/166), 15–60 years 25.3% (n=42/166), >60 years 22.2% (n= 37/166). 55.4% (n= 92/166) of the patients were male and 44.6% (n= 74/166) were female. The patient data came from a tertiary hospital 64.5% (n=107/166), district hospitals 11.4% (n= 19/166) and private hospitals 24.1% (n=40/166). The invasive diseases encountered were 159 bacteremias,1 meningitis, 1 meningitis with brain abscess, 2 osteomyelitis, 2 arthritis, and 1 urinary tract infection with bacteremia. The patients infected with non-drug resistant non-typhoidal Salmonella (NDR-NTS) were 9.6% (n=16) (95% CI 1.08–4.62). Twenty percent (n=20/166) (95% CI 9.85–23.19) had NTS resistant to one class of antimicrobial (1-DR-NTS). 17.5% (n=29/166) (95% CI 8.20–53.07) were resistant to two classes of antimicrobial (2-DR-NTS), and 68.8% (n=101/166) (95% CI 7.17–11.06) were resistant to at least one agent in three or more antimicrobial categories (MDR-NTS). Serogroup C was the main serogroup at 39% (n=66/166) (95% CI 2.00–9.87). The most common underlying diseases were metabolic diseases 24.6% (n=41/166) (16 diabetes, 5 diabetes with hypertension, 4 diabetes with hyperlipidemia, 8 diabetes with other), hematologic disorders 15% (n=25/166) (7 thalassemias with regular blood transfusion, 6 thalassemias with non-regular blood transfusion, 8 Iron deficiency anemia, 1 G6PD, 3 other), and hyperlipidemia 2.4% (n=4/166). The 5 Immunological disorders were all HIV-infected patients. 59% (n=98/166) patients had white blood cells >15,000 cells/uL with a median concentration of 21,000 cells/uL (IQR 2200–35,000 cells/uL), and 59% (n=99/166) of patients had anemia (hemoglobin <12 g/dl). Almost all patients came with a high-grade fever of more than 39 C° (95.2% (n=158/166). Of the 91/166 invasive disease patients for which date of onset was known, 84% (n=77/91) of patients had symptoms of illness more than 3 days before admission, with a median of 1.5, IQR (1–5) (Table 1).
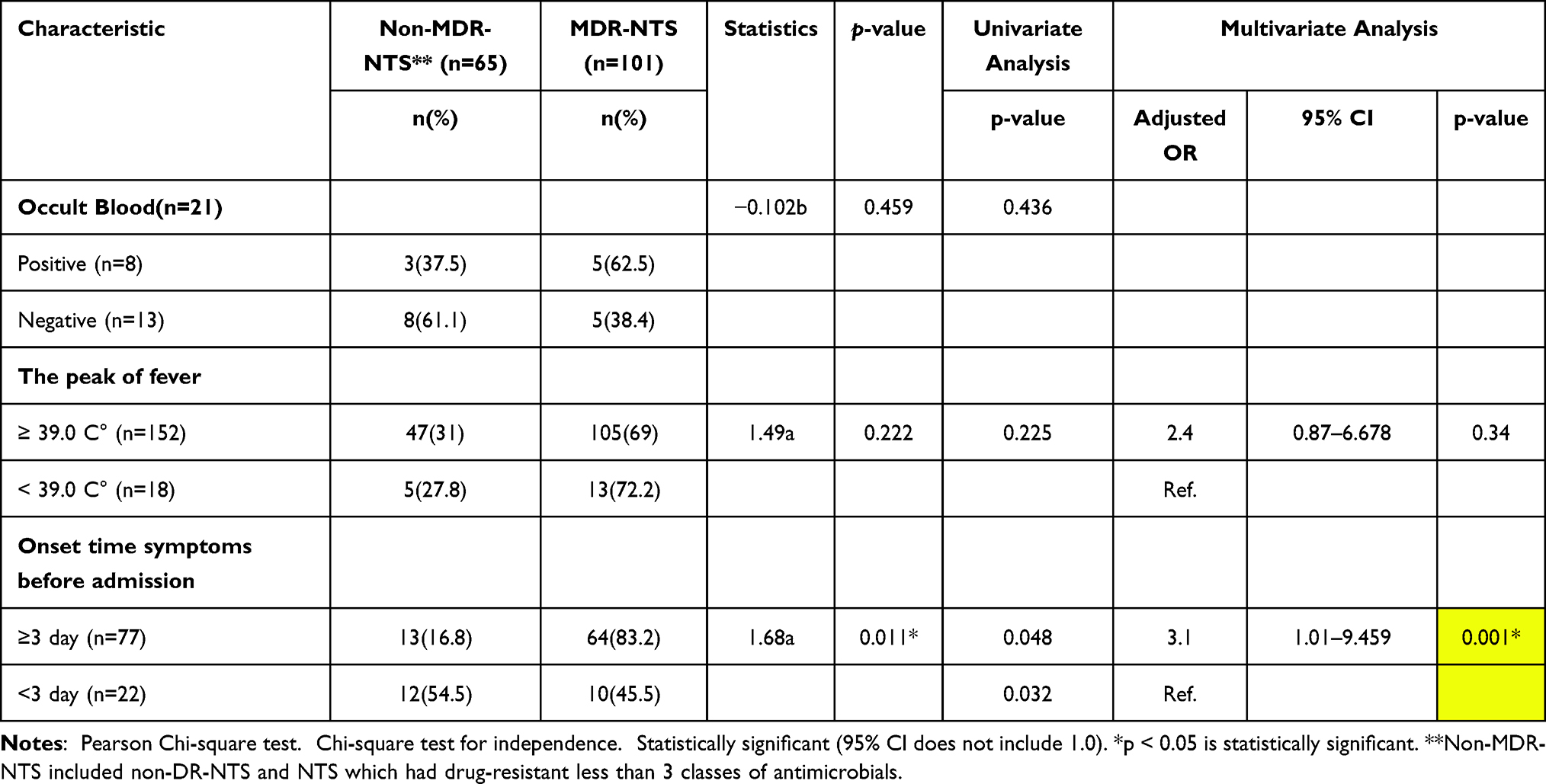 |
Table 1 The Binary Logistic Regression Analysis of the Risk Factors Associated with MDR-NTS in Invasive Patients (n=166). |
Antimicrobial-resistant patterns in invasive disease
Overall, the NTS resistance to ampicillin was 72.3% (n=120/166), norfloxacin was 53.6% (n=89/166), sulfamethoxazole/trimethoprim was 59% (n=98/166), tetracycline was 39% (n=66/166), amoxicillin-clavulanic acid was 46.3% (n=77/166), ciprofloxacin was 41% (n=68/166), ceftriaxone was 33.7% (n=56/166), cefotaxime was 27.1% (n=45/166), amikacin was 10.8% (n=18/166), gentamicin was 6% (n=11/166), ampicillin/sulbactam was 6% (n=10/166), ceftazidime was 1.2% (n=2/166), piperacillin/tazobactam was 0.6% (n=1/166), meropenem was 0.6% (n=1/166).
Risk Factors Associated with MDR-NTS in the iNTS
This study found onset time of symptoms before admission ≥3 days (p=0.011), age >60 years (p=0.014), and diabetes (p=0.022) were significantly associated with MDR infection in the univariate analysis (Table 1).
Patients with symptoms more than three days before hospitalization (p=0.001) and patients older than 60 years were the main predisposing factors to infection by MDR-NTS in a multivariate analysis (Table 1).
Risk Factors Related to Invasive Infection in NTS Patients
The univariate logistic regression analysis showed that white blood cells ≥15.000 cells/uL (p<0.001), haemoglobin less than 12 g/dl (p=0.001), the peak of fever ≥39 C° (p<001), and onset of illness more than 3 days PTA (p=0.009) were the factors significantly associated with invasive infection in all NTS patients (n=433) (Table 2).
 |
Table 2 The Binary Logistic Regression Study of the Factors Related to Invasive Patients in All NST Patients (n=433). |
The multivariate analysis showed that white blood cells >15,000 cells/uL (p<0.001), the peak of fever ≥ 39 C° (p=001), and illness for more than 3 days before admission (p=0.035) were the factors significantly associated with invasive infection in all NTS patient groups (Table 2).
Risk Factors Related to MDT-NTS Infections in NTS Patients
Diabetes patients (p=0.014), Invasive diseases (p=0.023), and serogroup C were significantly associated with MDR infection in the univariate analysis. Invasive infection patients (p=0.024), and serogroup C (p=0.046) were significantly associated with MDR-NTS infection and with ceftriaxone and ciprofloxacin resistance in the multivariate logistic regression analysis (Table 3).
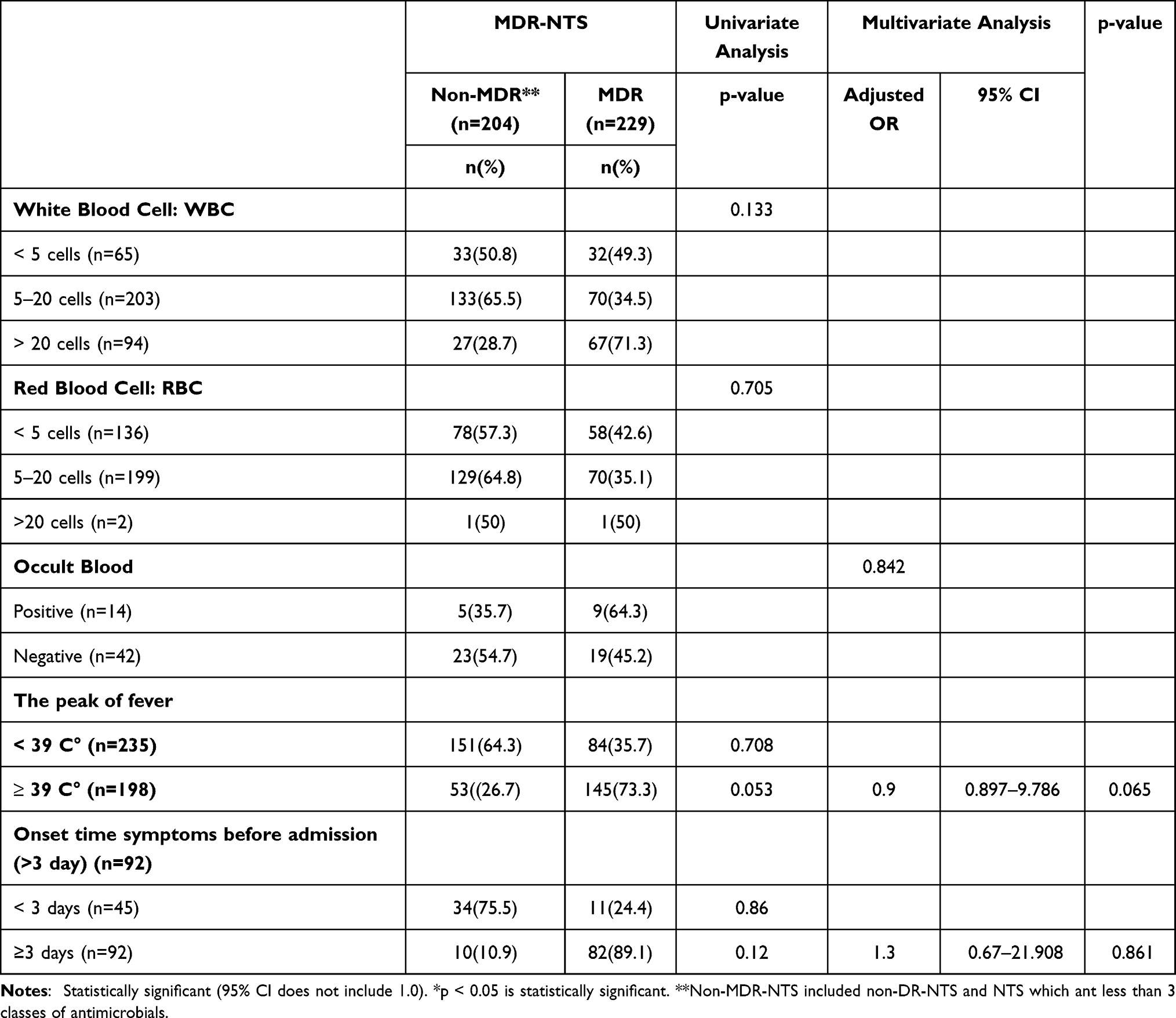 |
Table 3 Binary Logistic Regression Analysis of the Factor Associated with MDR-NTS Compared to Non-MDR-NTS |
Discussion
The increase of MDR-NTS is a worldwide threat to public health. The MDR-NTS causes both invasive diseases and diarrhea. For enteritis, healthy patients can self-recover without the use of antibiotics, but not for invasive infection. The MDR-NTS-related invasive disease affects the failure of treatment.
This study found an Invasive infection rate of 38.4% (166/433), similar to a study in Africa at 39% (1966–2014),19 and higher than a previous systematic review of scientific databases (1990–2017) in Thailand (10–24.9%),1 Australia (2–4.9%), and Taiwan 6.9% (in children).20 However, this incidence may be inflated; it is possible that some patients with diarrhea did not confirm the diagnosis. This study supported that MDR-NTS is associated with invasive disease, and our MDR-NTS rate of 69% was a little higher than a study which compared all NTS patients in Thailand (62.3%)14 but lower than a study in Africa (50–75%).1,21
The risk factor related to MDR-NTS infection in iNTS cases in this study, onset time of symptoms ≥3 days before admission (p=0.011), was similar to a study in the French West Indies22 that showed a delay between onset of symptoms and hospital admission >5 days (P = 0.01) was significantly associated with MDR-NTS in a multivariate analysis, but the different duration may be due to differences in access to treatment and public health systems. This study found the median time of onset before treatment was only 1.5 days in all NST cases. The study in the French West Indies also identified vomiting (P = 0.001) and increased respiratory rate (P = 0.001)22 as risk factors, which this study did not.
The patients who were over 60 years old (p=0.014) were significantly associated with MDR-NTS in this study, which was similar to a systematic research review in a high-income county group that showed elderly people (51·2% among those aged ≥70 years)1 were associated with iNTS. There are also studies relating young patients to MDR-NTS in iNTS,1,23,24 which this study did not find.
Information from WHO found the proportion of the world’s population over 60 years old will nearly double from 12% to 22% between 2015 and 2050. The number of people aged 60 years and older will outnumber children younger than 5 years. And in 2050, 80% of older people will be living in low- and middle-income countries. This demographic shift is a major challenge for all countries to encounter, so they must make health policies to ensure their health.25
The univariate analysis for this research also showed diabetic patients related to MDR-NTS (p=0.022). Many studies have found a relationship between diabetic mellitus (DM) patients and MDR-NST infection. Other multidrug-resistant pathogens also have complications and co-infection26–29,30–35 similar to this study. In general, patients with DM have infections more often than those without DM. Some studies found decreased cellular responses in vitro. No disturbances in adaptive immunity in diabetic patients have been described, and disturbances to release of complement factor 4, and decreased cytokine response after the infection have been noted. Important cellular innate immunity is impaired; most studies show decreased functions [chemotaxis, phagocytosis, and killing of diabetic polymorphonuclear cells and diabetic monocytes/macrophages] compared to cells of controls. Another mechanism which can lead to the increased prevalence of infections in diabetic patients is an increased adherence of microorganisms to diabetes compared to nondiabetic cells. Furthermore, some microorganisms become more virulent in a high glucose environment.30,31 However, diabetes is a dominant underlying disease in this study, that may affect sampling bias, which requires further study. Many past studies present a burden of NTS infection that included iNTS and MDR-NTS among HIV-infected individuals.1,24,32–34 A past study in Thailand (1992–2004)35 showed similar results, but this study did not. This study found only 4 HIV-infected cases, and all of them got treatment and had CD4 >200 cell/cu.mm. However, this research was retrospective, so the number of cases may be under-reported; therefore, randomization bias requires further study.
For all NTS (n=433), the patients who had WBC ≥ 15,000 cell/uL, Hb less than 12 g/dL, or high-grade fever ≥39°C were more frequently found to have iNTS than patients without those symptoms. This is consistent with other studies.1,19,23,36 Delay of more than three days between the onset of symptoms and treatment was significantly associated with iNTS.
iNTS was significantly associated with MDR in all NTS patients (n=433) in this study, which was similar to many past research studies.1,24,32 The study also showed that serogroup C was significantly related to iNTS, while other studies commonly showed D.1,24,35
Other factors may be related to infection with DR-NST, particularly the history of previous antibiotic consumption, including type, frequency, quantity, and duration of antibiotic. Occupations, nutritional status, and frequency of previous diarrhea may also be related to other factors. This needs further study.
The principle of prevention of MDT-NTS infections, whether iNTS or not, is good food, hygiene, and good immunity and controlling MDR-NTS in the environment is essential. Thailand had the Antibiotic Smart Use programs started in 2007.37 They are effective in reducing drug-resistant strains; however, some conditions, such as the easy access to over-the-counter antibiotics without a doctor’s prescription, and antibiotic stewardship38 campaigns include encouraging using the practice guidelines to increase the confidence of doctors and patients. And also includes controlling the use of antibiotics in livestock. This requires government policies that consider the appropriate benefits and risks.
Limitations
This research is a retrospective study, so data for comparison was limited. In addition, the hospitals had different kinds of information, for example, types of antimicrobial tests and sources of specimens (blood, urine, stool, etc.). The data of MIC and serotype of Salmonella classification were limited because these tests are not routinely performed in general hospitals, limiting our data. Lastly, this study’s findings cannot be generalized to a general population, so further studies are needed.
Conclusion
The invasive infection NTS patients who were older than 60 years and had onset of illness >3 days before admission were associated with MDR-NTS infection. The MDR-NTS was related to iNTS. The factors associated with iNTS were WBC ≥ 15,000 cell/uL, hemoglobin <12 g/dL, and the peak of fever ≥39 C°. Therefore, patients with these factors may be infected with MDR-NTS. However, the choice of antimicrobial selected must be appropriate for the local prevalence and epidemiology of MDR-NTS and correlate with the clinical responsiveness.
Ethical Approval
The study protocol was approved by the research ethics committee of Panyananthaphikkhu Chonprathan Medical Center, Srinakharinwirot University. All information was anonymized to maintain patients’ privacy, Declaration of Helsinki. Considering the retrospective and anonymous nature of the study, the Ethics Committee did not require written informed consent provided by patients.
Acknowledgments
The authors thank all patients, health practitioners and directors of all hospitals authorized to collect research data.
Funding
Panyananthaphikkhu Chonprathan Medical Center, Srinakharinwirot University, supported this research.
Disclosure
The authors report no conflicts of interest in relation to this work and declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in the research.
References
1. Stanaway JD, Parisi A, Sarkar K.; Collaborators GBDN-TSID. The global burden of non-typhoidal salmonella invasive disease: a systematic analysis for the global burden of disease study 2017. Lancet Infect Dis. 2019;19(12):1312–1324. doi:10.1016/S1473-3099(19)30418-9
2. Park SE, Pak GD, Aaby P, et al. The relationship between invasive nontyphoidal Salmonella disease, other bacterial bloodstream infections, and malaria in Sub-Saharan Africa. Clin Infect Dis. 2016;62:S23–S31. doi:10.1093/cid/civ893
3. Vugia DJ, Samuel M, Farley MM, et al. Invasive Salmonella infections in the United States, foodNet, 1996–1999: incidence, serotype distribution, and outcome. Clin Infect Dis. 2004;38:S149–S156. doi:10.1086/381581
4. Parisi A, Crump JA, Glass K, et al. Health outcomes from multidrug-resistant Salmonella infections in high-income countries: a systematic review and meta-analysis. Foodborne Pathog Dis. 2018;15:428–436. doi:10.1089/fpd.2017.2403
5. Chen CY, Hsieh PH, Chang CY, et al. Molecular epidemiology of the emerging ceftriaxone resistant non-typhoidal Salmonella in southern Taiwan. J Microbiol Immunol Infect. 2019;52(2):289–296. doi:10.1016/j.jmii.2018.08.007
6. Li WC, Huang FY, Liu CP, et al. Ceftriaxone resistance of nontyphoidal Salmonella enterica isolates in Northern Taiwan attributable to the production of CTX-M-14 and CMY-2 beta-lactamases. J Clin Microbiol. 2005;43(7):3237–3243. doi:10.1128/JCM.43.7.3237-3243.2005
7. Jain P, Chowdhury G, Samajpati S, et al. Characterization of non-typhoidal Salmonella isolates from children with acute gastroenteritis, Kolkata, India, during 2000–2016. Braz J Microbiol. 2020;51(2):613–627. doi:10.1007/s42770-019-00213-z
8. Lee K, Yong D, Yum JH, Kim HH, Chong Y. Diversity of TEM-52 extended-spectrum beta-lactamase-producing non-typhoidal Salmonella isolates in Korea. J Antimicrob Chemother. 2003;52(3):493–496. doi:10.1093/jac/dkg385
9. Narasanna R, Chavadi M, Chandrakanth K. Prevalence of multidrug-resistant Salmonella typhi in typhoid patients and detection of blaCTX-M2 and blaCTX-M9 genes in cefotaxime-mediated extended spectrum β-lactamase-producing Salmonella typhi isolates. Biomed Res. 2018;29(14):3015–3021. doi:10.4066/biomedicalresearch.29-18-794
10. National Antimicrobial Resistant Surveillance Center T. The situation of drug resistance 2000–2020 (6M); 2020.
11. Chang YJ, Chen YC, Chen NW, et al. Changing antimicrobial resistance and epidemiology of non-typhoidal salmonella infection in Taiwanese children. Front Microbiol. 2021;29:648008. doi:10.3389/fmicb.2021.648008
12. Woh PY, Yeung MPS, Goggins WB, et al. Genomic epidemiology of multidrug-resistant nontyphoidal salmonella in young children hospitalized for gastroenteritis. Microbiol Spectrum. 2021;9(1):e0024821. doi:10.1128/Spectrum.00248-21
13. Harb A, O’Dea M, Hanan ZK, Abraham S, Habib I. Prevalence, risk factors and antimicrobial resistance of Salmonella diarrhoeal infection among children in Thi-Qar Governorate, Iraq. Epidemiol Infect. 2017;145(16):3486–3496. PMID: 29103396; PMCID: PMC9148757. doi:10.1017/S0950268817002400
14. Hengkrawit K, Tangjade C. Prevalence and trends in antimicrobial susceptibility patterns of multi-drug-resistance non-typhoidal salmonella in Central Thailand, 2012–2019. Infect Drug Resist. 2022;15:1305–1315. doi:10.2147/IDR.S355213
15. World health organization. 2014-2016 ICD-10-CM Diagnosis Code A02.0-02.9 Salmonella infection. Available from: https://www.icd10data.com/ICD10CM/Codes/A00-B99/A00-A09/A02-/A02.9.
16. CLSI. Performance Standards for Antimicrobial Susceptibility Testing.
17. Bureau of Laboratory Quality S. History and Authority. Available from: http://blqs.dmsc.moph.go.th/en/page-view/22.
18. Magiorakos A, Srinivasan RB, Carey Y, et al. Multidrug-resistant, extensively drug-resistant and pan drug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
19. Uche IV, MacLennan CA, Saul A. A systematic review of the incidence, risk factors and case fatality rates of invasive nontyphoidal salmonella (iNTS) Disease in Africa (1966 to 2014). PLoS Negl Trop Dis. 2017;11(1):e0005118. PMID: 28056035; PMCID: PMC5215826. doi:10.1371/journal.and.0005118
20. Chang YJ, Chen YC, Chen NW, et al. Changing antimicrobial resistance and epidemiology of non-typhoidal salmonella infection in Taiwanese children. Front Microbiol. 2021;12:648008. PMID: 33868207; PMCID: PMC8044818. doi:10.3389/fmicb.2021.648008
21. Kariuki S, Gordon MA, Feasey N, Parry CM. Antimicrobial resistance and management of invasive Salmonella disease. Vaccine. 2015;33(Suppl 3):C21–9. PMID: 25912288; PMCID: PMC4469558. doi:10.1016/j.vaccine.2015.03.102
22. Guyomard-Rabenirina S, Muanza B, Bastian S, et al. Salmonella enterica serovars panama and arechavaleta: risk factors for invasive non-typhoidal salmonella disease in Guadeloupe, French West Indies. Am J Trop Med Hyg. 2018;99(3):584–589. PMID: 30014811; PMCID: PMC6169165. doi:10.4269/ajtmh.18-0192
23. Ke Y, Lu W, Liu W, Zhu P, Chen Q, Zhu Z. Non-typhoidal Salmonella infections among children in a tertiary hospital in Ningbo, Zhejiang, China, 2012–2019. PLoS Negl Trop Dis. 2020;14(10):e0008732. PMID: 33017418; PMCID: PMC7561262. doi:10.1371/journal.pntd.0008732
24. Guyomard-Rabenirina S, Muanza B, Bastian S, et al. Multi-drug resistant non-typhoidal Salmonella associated with invasive disease in western Kenya. PLoS Negl Trop Dis. 2018;12(1):e0006156. PMID: 29329299; PMCID: PMC5785031. doi:10.1371/journal.pntd.0006156
25. World health organization. Ageing and health; 2022. Available from:https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
26. Navaneeth BV, Tripathi R, Abbas M, Belwadi MR. Subcutaneous abscess caused by extended-spectrum beta-lactamase-producing Salmonella senftenberg in a type 2 diabetic--a case report. Int J Infect Dis. 2002;6(4):321–322. PMID: 12725214. doi:10.1016/s1201-9712(02)90170-0
27. Shen CH, Lin YS, Chang FY. Gas-forming parotid abscess in a diabetic patient: an unusual complication of Salmonella enteritidis bacteremia. Am J Med Sci. 2008;336(6):504–507. PMID: 19092325. doi:10.1097/MAJ.0b013e3181626545
28. Fukuda T, Bouchi R, Minami I. Retrograde pyelonephritis and lumbar spondylitis as a result of Salmonella typhi in a type 2 diabetes patient with neurogenic bladder. J Diabetes Investig. 2016;7(3):436–439. doi:10.1111/jdi.12375
29. Matono T, Takeshita N, Kutsuna S, et al. Indolent non-typhoidal salmonella vertebral osteomyelitis in a diabetic patient. Intern Med. 2015;54(23):3083–3086. PMID: 26631898. doi:10.2169/internalmedicine.54.4833
30. Raine T, Zaccone P, Mastroeni P, Cooke A. Salmonella typhimurium infection in nonobese diabetic mice generates immunomodulatory dendritic cells able to prevent type 1 diabetes. J Immunol. 2006;177(4):2224–2233. PMID: 16887982. doi:10.4049/jimmunol.177.4.2224
31. Geerlings SE, Hoepelman AI. Immune dysfunction in patients with diabetes mellitus (DM). FEMS Immunol Med Microbiol. 1999;26(3–4):259–265. doi:10.1111/j.1574-695X.1999.tb01397
32. Feasey NA, Dougan G, Kingsley RA, Heyderman RS, Gordon MA. Invasive non-typhoidal salmonella disease: an emerging and neglected tropical disease in Africa. Lancet. 2012;379(9835):2489–2499. PMID: 22587967; PMCID: PMC3402672. doi:10.1016/S0140-6736(11)61752-2
33. Mermin J, Lule J, Ekwaru JP, et al. Cotrimoxazole prophylaxis by HIV-infected persons in Uganda reduces morbidity and mortality among HIV-uninfected family members. AIDS. 2005;19(10):1035–1042. PMID: 15958834. doi:10.1097/01.aids.0000174449.32756.c7
34. Gordon MA, Banda HT, Gondwe M, et al. Non-typhoidal salmonella bacteraemia among HIV-infected Malawian adults: high mortality and frequent recrudescence. AIDS. 2002; (12):1633–1641. PMID: 12172085. doi:10.1097/00002030-200208160-00009
35. Kiratisin P. Bacteraemia due to non-typhoidal Salmonella in Thailand: clinical and microbiological analysis. Trans R Soc Trop Med Hyg. 2008;102(4):384–388. PMID: 18321543. doi:10.1016/j.trstmh.2008.01.019
36. American Academy of Pediatric. Samonella. In: Kimberlin D, Barnett ED, Lynnfield R, Sawyer MH, editors. Red Book: 2021–2024 Report of the Committee on Infectious Diseases.
37. Sumpradit N, Chongtrakul P, Anuwong K, et al. Antibiotics Smart Use: a workable model for promoting the rational use of medicines in Thailand. Bull World Health Organ. 2012;90(12):905–913. PMID: 23284196; PMCID: PMC3524958. doi:10.2471/BLT.12.105445
38. World health organization. Antimicrobial stewardship interventions: a practical guide; 2022. Available from:https://apps.who.int/iris/bitstream/handle/10665/340709/9789289054980-eng.pdf.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.