Back to Journals » Risk Management and Healthcare Policy » Volume 16
Factors Associated with Maternal Healthcare Utilization Before and After Delivery Among Migrant Pregnant Women in China: An Observational Study
Authors Gao M, Fang Y, Liu Z, Xu X, You H ![]() , Wu Q
, Wu Q
Received 19 June 2023
Accepted for publication 17 August 2023
Published 23 August 2023 Volume 2023:16 Pages 1653—1665
DOI https://doi.org/10.2147/RMHP.S423723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Maoze Gao,1,* Yaohui Fang,1,* Zhangrui Liu,1 Xinpeng Xu,1,2 Hua You,1,2 Qifeng Wu1
1School of Public Health, Nanjing Medical University, Nanjing, People’s Republic of China; 2Institute of Healthy Jiangsu Development, Nanjing Medical University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinpeng Xu, School of Public Health, Nanjing Medical University, Nanjing, 211166, People’s Republic of China, Email [email protected]
Background: Effective healthcare utilization throughout pregnancy is essential in protecting mother and child health, but the maternal healthcare utilization and its associated factors among migrant women are still underexplored.
Methods: The data came from the 2018 China Migrants Dynamic Survey. Our analysis included 6337 pregnant migrant women. Prenatal healthcare utilization comprises receiving at least 5 antenatal care (ANC) times and establishing the maternal health record within the first 12 weeks of pregnancy. Postnatal healthcare utilization refers to whether an individual received a postpartum visit and a physical health examination within 28 days and 42 days following delivery. A multivariate binary logit model was employed to investigate the factors related to maternal healthcare utilization.
Results: 67.15% of the 6337 participants established health records within the first 12 weeks of pregnancy, and 88.35% received at least five ANC visits. 76.88% and 84.20% of migrant pregnant women received a postpartum visit and a health examination respectively. Age was positively correlated with receiving at least five ANC visits (OR:1.245, 95% CI: 1.038– 1.493), a postpartum visit within 28 days (OR: 1.272, 95% CI: 1.107– 1.460) and a physical examination within 42 days after delivery (OR=1.174, 95% CI: 1.002– 1.376). Education, household income, health insurance and maternal health education were positively associated with prenatal and postnatal healthcare utilization (P< 0.05). Number of Children negatively correlated with ANC times (OR: 0.742, 95% CI: 0.613– 0.898) and receiving health examination after delivery (OR: 0.720, 95% CI: 0.610– 0.849).
Conclusion: There is still potential for improvement in the maternal healthcare utilization, particularly in postnatal healthcare. Strengthening the follow-up, focusing on those who are younger, have lower socioeconomic status, and are members of ethnic minorities, and continuing to strengthen maternal health education for them can promote the maternal healthcare utilization before and after delivery.
Keywords: maternal healthcare utilization, prenatal and postnatal, migrant pregnant women, China
Background
Despite the decline since 2014, China has a large migrant population. According to the findings of China’s seventh National Census in 2020, the total number of migrant populations in China has exceeded 370 million in 2020.1 During the development of population mobility, the phenomenon of family migration has progressively emerged, and many women of reproductive age choose to accompany their husbands on migration.2 Existing research indicated that one-fourth of all married women in China are migrant women of childbearing age.3,4 The number of migrant women of reproductive age who utilize maternal healthcare services in the inflow areas is rising.5 Therefore, it is necessary to pay attention to the utilization of maternal health care of migrant women.
Maternal healthcare is a high priority agenda that governments around the world attach great importance to. The Sustainable Development Goals of the United Nations proposed in 2015 that the global maternal mortality rate per 100,000 live births should fall below 70 by 2030.6 Effective management of maternal health is crucial for preventing maternal and fetal mortality and safeguarding the health of mothers and children.7–9 Since 2009, China has implemented national essential public health services (NEPHS) to improve mother and child health, including maternal health management services for pregnant women from the start of their pregnancies until 42 days after delivery.10 All pregnant women who have lived in the community for at least half a year, whether they are migrant population or registered residents, are entitled to health management services in the primary medical institutions in the place of residence, including the establishment of maternal health records in early pregnancy, physical examination, health status assessment and lifestyle guidance during different time of pregnancy, postpartum visits and health examinations after childbirth.11 The above-mentioned services are provided free of charge by grass-roots medical institutions represented by community health service centers, and residents do not need to bear any additional costs. The financing of these services is fully borne by the state finance.
However, studies have shown that maternal healthcare utilization during pregnancy of migrant women is significantly lower than that of local women, both prenatally12 and postnatally.13 Some earlier studies explored the factors related to maternal healthcare utilization from the perspective of providers and revealed that inadequate maternal healthcare during pregnancy is associated with poor service accessibility and quality.14,15 Several studies examined the relationship between different factors and maternal healthcare utilization for migrant women from a demand-side perspective, such as sociodemographic characteristics, socioeconomic status, and migration characteristics,12,16–20 in an effort to comprehend the reasons for the inadequate utilization of maternal healthcare among this population.
Although studies on maternal healthcare utilization among migrant women from a prenatal or postnatal viewpoint were conducted, most of these studies were limited to the investigation of a single location or medical institution in China, with limited representation. Additionally, the most recent national study was conducted in 2014. In light of the ongoing growth of migrant population and evolution of health policies, it is essential to continue focusing on the utilization of prenatal and postnatal maternal healthcare among migrant women. Based on the newly released national-level survey data on migrant population conducted by the National Health Commission in 2018, this study analyzed the current status of maternal healthcare utilization (including the utilization of prenatal and postnatal healthcare services) among the migrant population, and explored the relevant factors associated with prenatal and postnatal healthcare utilization, so as to provide useful references for further optimization of maternal health management in the migrant population.
Methods
Data Source
The data utilized in this study came from the 2018 China Migrants Dynamic Survey (CMDS) conducted by the National Health Commission of the People’s Republic of China. From 31 provinces (autonomous regions and municipalities) and the Xinjiang Production and Construction Corps, migrant populations aged 15 and older who had lived in the place of migration for at least one month were selected using a stratified, multi-stage, and size-proportional sampling technique. The CMDS data survey adopts face-to-face survey. Before the survey, the National Health Commission is responsible for the training of the investigators. When filling in the questionnaire in the household survey, the smart phone (or PAD) equipped with computer-assisted interview system is directly used. The 2018 survey provided information on maternal healthcare utilization, allowing us to investigate it and its associated determinants.
In 2018, the total CMDS sample size was 152,000, and the study population was defined by the following criteria: (1) female migrants with at least one biological child; (2) having a child born after January 2017 (only those give birth after January 2017 were asked questions about maternal healthcare utilization); (3) having lived in the residence for more than one year (Maternal healthcare are offered for those have lived in the residence for half a year and longer); and (4) excluding women with significant age abnormalities from the sample. Finally, a total of 6337 migrant pregnant women were included in the study.
Measurements
Dependent Variables
The dependent variables in this study were prenatal and postnatal healthcare utilization. Two indicators were used to measure prenatal care utilization: whether the maternal health record was established within the first 12 weeks of pregnancy and whether an individual received five times of antenatal care (ANC) during pregnancy. In the CMDS questionnaire, respondents were asked when the maternal health record was established. Respondents could response from five options: 1 = within the first 12 weeks of pregnancy, 2 = between the 13th and 27th week of pregnancy, 3 = between the 28th and 40th week of pregnancy, 4 = heard about the record but did not establish it, 5 =neither heard about the record nor established it. According to the NEPHS standards, pregnant women should establish maternal health records within the first 12 weeks of their pregnancies. Therefore, we generate a dummy variable by recode 2, 3, 4 and 5 as 0 in subsequent regression analysis, indicating whether an individual establish the maternal health record within the first 12 weeks of pregnancy. Each respondent was also asked how many times she received ANC during her pregnancy, with four responses: 1=0 time, 2=1-2 times, 3=3-4 times, 4=5 times and more. Similarly, we recoded 1, 2, 3 to 0 and 4 to 1 in subsequent regression analysis, indicating whether each migrant pregnant woman received at least five ANC visits.
The utilization of postnatal healthcare services was measured using two dichotomous indicators: whether an individual received a postpartum visit within 28 days after delivery (1=yes, 0=no), and whether an individual received a health examination within 42 days after delivery (1=yes, 0=no).
Independent Variables
Referring to previous studies,13,21 four types of independent variables were included in regression analyses: demographic characteristics (age, household registration, ethnic group, family size, number of children), socioeconomic status (education, employment, monthly household income, health insurance), migrant characteristics (migrant range, migrant duration), and maternal health education.
Age is a numeric variable that was encoded as a binary variable based on the average age: 0 indicates an individual is younger than 29, and 1 indicates that an individual’s age is 29 or older. For the household registration, 0 indicates non-agricultural and 1 indicates agricultural household registration. Ethnicity is a binary variable, with 0 representing Han and 1 representing ethnic minorities. Household size is a numeric variable that represents the number of people living with each respondent. The number of children is also a numerical variable denoting the number of biological offspring of a migrant woman. Educational attainment is a three-category variable, with 1 indicating elementary school and below, 2 indicating junior high school, and 3 indicating senior high school and above. Employment is a binary variable, 0 = employment, 1 = unemployment. The quartiles of monthly household income are Q1, Q2, Q3 and Q4, with Q1 representing the group with the lowest income and Q4 representing the highest income group. In addition, we added variables to the model that characterize the type of health insurance an individual participates in, which has five categories: 1 = no medical insurance, 2 =the New Cooperative Medical Scheme (NCMS), 3 = the Urban Resident basic Medical Insurance (URBMI), 4= the Coordinating Urban and Rural Basic Medical Insurance (CURBMI), and 5= the Urban Employees Basic Medical Insurance (UEBMI). The migration range is a variable with three categories: 1=migration across provinces, 2=migration across cities within a province, and 3=migration across counties within a city. Migration duration is a numeric variable which is recorded in regression analysis as a dichotomous variable based on its mean, with 0 = migration time less than 4 years, and 1=migration time 4 years or more. Access to maternal health education is a binary variable, where 0 = did not receive reproduction and contraception education in the previous year, and 1 = received reproduction and contraception education in the previous year.
Statistical Analyses
Descriptive statistics for continuous and categorical variables are performed firstly using mean/standard error or frequency/percentage, respectively. The multivariate logit model was then employed to analyze the relationship between maternal healthcare utilization and independent variables. All analyses were conducted using Stata version 16.0 (Stata Corp., College Station, TX, USA). To be clear, we conducted two multivariate logit models for each dependent variable, one of which included only all the independent variables mentioned above, and the other includes all independent variables, and also adds dummy variables to characterize each province to control the impact of differences in the distribution of medical resources in different provinces.
Results
Characteristics of the Study Population
The average age of migrant women in our study sample was 29.05±4.71 years, and the average number of children per woman was 1.54±0.58. 79.8% of the population are registered in rural areas (Table 1); Among the samples, women with a senior high school or above education make up the majority (60.94%); 10.7% of women are ethnic minorities; The average monthly household income was 9152.12±13,764.98 CNY; 6.52% of women did not participate in any kind of health insurance. In terms of migration characteristics, 44.39% of the population migrated across provinces, followed by 37.72% who migrated across cities within a province, and 17.89% who moved across counties within a city. 46.68% of the individuals have migrated for more than four years. In addition, 62.92% of the women received maternal health education in the previous year.
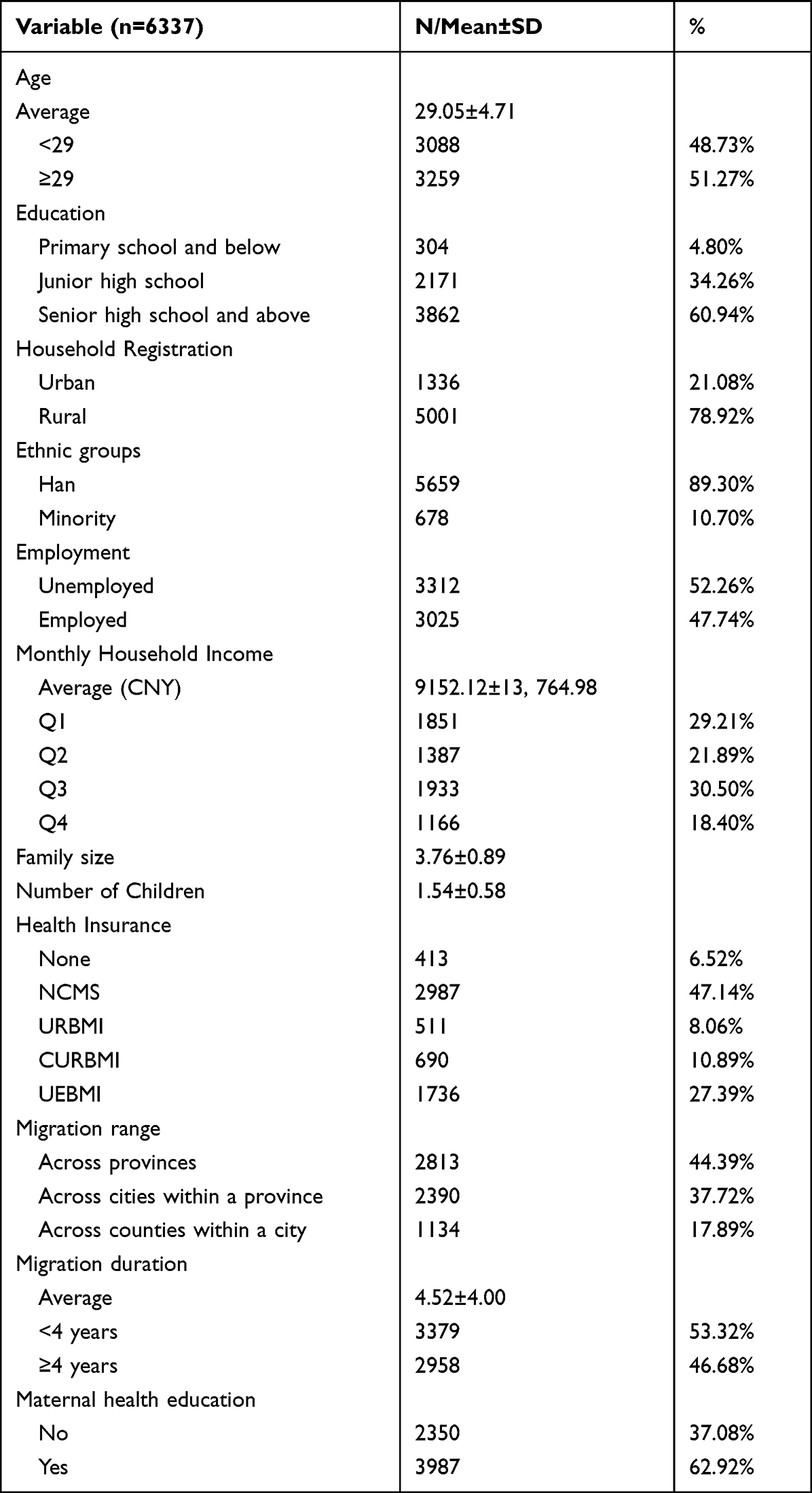 |
Table 1 Descriptive Statistics of Variables |
Maternal Healthcare Utilization Among Migrant Pregnant Women
Figure 1 depicted the maternal healthcare utilization among migrant women. The utilization of prenatal healthcare was shown in Figure 1A and B. It was indicated in Figure 1A that 67.15% of migrant women established maternal health records within the first 12 weeks of pregnancy, and 22.69% of women established maternal records between the 13th to 27th week of pregnancy. 2.76% of individuals who heard about the establishment of the maternal health record but did not establish it, compared to 2.71% of individuals who neither heard about it nor established it. Figure 1B revealed that 0.41% of migrant pregnant women did not receive ANC. The proportion of individuals with 1–2 and 3–4 ANC visits is 2.59% and 8.65%, respectively. Those who received 5 or more ANC visits accounted for the largest proportion (88.35%).
 |
Figure 1 Maternal healthcare utilization among migrant pregnant women (2018). (A) Establishment of Maternal Record (B) ANC visits (C) Postpartum visit within 28 days after delivery (D) Health examination within 42 days after delivery. |
Figure 1C and D showed the postnatal healthcare utilization among migrate pregnant women. 76.88% of migrant pregnant women received a postpartum visit within 28 days following delivery, whereas 23.12% did not. 15.80% of individuals did not receive a health examination within 42 days after delivery, compared to 84.20% who did.
Factors Associated with Prenatal Maternal Healthcare Utilization Among Migrant Pregnant Women
The relationship between each of the aforementioned independent variables and prenatal healthcare utilization of migrant women was shown in Table 2. To ensure the robustness and reliability of the results, we reported both results regardless of whether the province dummy variables were included in the regression. We found that educational attainment, monthly household income, number of children, type of health insurance, migration duration, and maternal health education were significantly associated with the establishment of maternal health records within the first 12 weeks of pregnancy (P<0.05). Individuals with an education level of junior high school (OR=1.379, P<0.05) and senior high school or above (OR=1.516, P<0.01), within the highest income group (Q4: OR=1.352, P<0.01), and participating in any type of health insurance (P<0.1) were more likely to establish the health records within the first 12 weeks of pregnancy; In terms of migration characteristics, migrant pregnant women who have migrated for over 4 years were 1.15 times more likely to establish health records within the first 12 weeks than their counterparts (OR=1.150, P<0.05), and those receiving maternal health education in the previous year were 1.25 times more likely to establish health records within the first 12 weeks of pregnancy (OR=1.245, P<0.01). Additionally, the likelihood that migrant women established the health record within the first 12 weeks of pregnancy decreased with the number of children (OR=0.842, P<0.05).
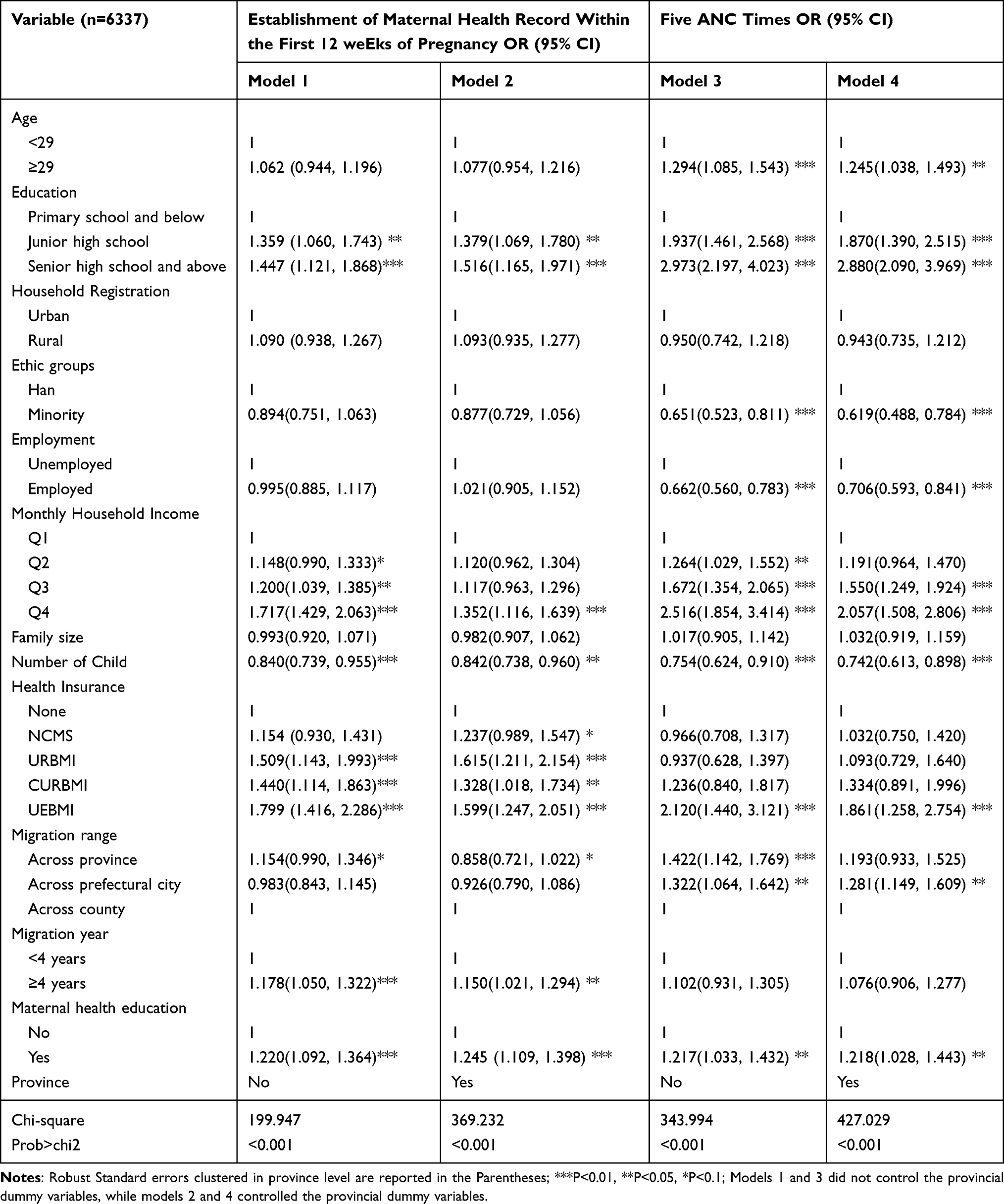 |
Table 2 Factors Associated with Establishment of Maternal Record and ANC Visits |
The number of ANC visit was significantly correlated with age, education level, ethnicity, employment, income, number of children, health insurance, migration range, and maternal health education (P<0.1). Those aged 29 and older (OR=1.245, P<0.05), with junior high school (OR=1.870, P<0.01) and senior high school or above education (OR=2.880, P<0.01), higher income level (Q3 & Q4, P<0.01), participating in UEBMI (OR=1.861, P<0.01), migrating within cities in a province (OR=1.281, P<0.05), and receiving maternal health education in the previous year (OR=1.218, P<0.05) were more likely to have five ANC visits than their counterparts. Those who were members of an ethnic minority (OR=0.619, P<0.01), employed (OR=0.706, P<0.01) and had more children (OR=0.742, P<0.01) were less likely to have five ANC visits.
Factors Associated with Postpartum Maternal Healthcare Utilization Among Migrant Pregnant Women
Factors related to postnatal healthcare utilization of migrant pregnant women were reported in Table 3. Age, education, income, number of children, health insurance, and maternal health education were significantly associated with receiving a postpartum visit within 28 days after delivery (P<0.1). Among them, those aged 29 and older (OR=1.272, P<0.01), with a senior high school or above education (OR=1.502, P<0.01), with higher income (Q2 & Q3 group, P<0.05), participating in URBMI (OR=1.668, P<0.01) and UEBMI (OR=1.612, P<0.01), and receiving maternal health education (OR=2.015, P <0.01) were more likely to receive a postpartum visit within 28 days after delivery. Individuals with more children were less likely to receive a postpartum visit within 28 days after childbirth (OR=0.868, P<0.1). Women who received maternal health education in the previous year were twice as likely to receive a postpartum visit within 28 days after delivery compared to those who did not.
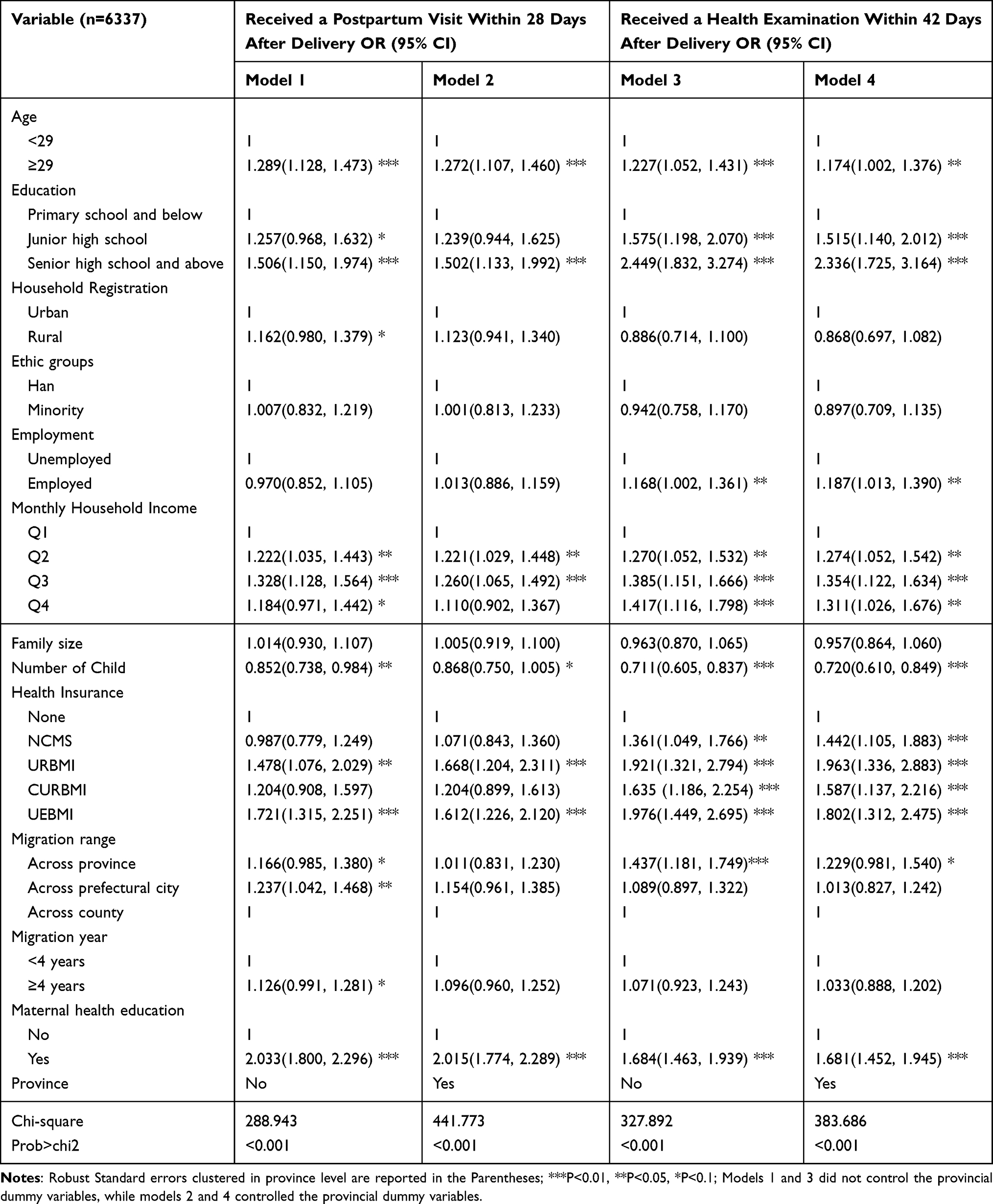 |
Table 3 Factors Associated with Postpartum Visit Within 28 Days and Health Examination Within 42 Days After Delivery |
Age, education, employment status, income, number of children, health insurance, migration range, and access to maternal health education were significantly associated with receiving a health examination within 42 days postpartum. Migrant women were more likely to receive health examination within 42 days after delivery if they met the following criteria: age 29 or older (OR=1.174, P<0.05), with junior high school (OR=1.515, P<0.01) and senior high school or above (OR=2.336, P<0.01) education, with employment (OR=1.187, P<0.05), with higher household income (P<0.05), participating in any type of health insurance (P<0.01), migrating across provinces (OR=1.229, P<0.1), and receiving maternal health education in the previous year (OR=1.681, P <0.01), while those with more children were less likely to receive a health examination after delivery (OR=0.720, P<0.01).
Discussion
China has implemented NEPHS since 2009, providing maternal health management services for pregnant women. Based on the CMDS data implemented by the National Health Commission in 2018, this study examined the current status of healthcare utilization of migrant pregnant women and its associated factors. The results showed that 67.15% of migrant pregnant women established the maternal health record within the first 12 weeks during pregnancy; 88.35% received at least five ANC visits and 0.41% did not received ANC. The proportion of migrant pregnant women receiving a postpartum visit and a health examination within 28 days and 42 days after delivery was 76.88% and 84.20% respectively. Compared with the results of a 2014 national-level study of migrant pregnant women, except for the decrease in the proportion of maternal health records established within the first 12 weeks during pregnancy (89% vs 67.15%), other prenatal and postnatal maternal healthcare utilization rates have increased.3 Maternal healthcare utilization proportion were higher in our study compared to data from a 2018 survey conducted in a city of China.13 This showed that at the national level, although there is still room for improvement, as the coverage of NEPHS expands, more migrant pregnant women benefit from it and hence the prenatal and postnatal healthcare utilization of pregnant women has increased significantly.
In line with earlier research,12,17,21 we discovered that among migrant pregnant women, age was significantly positively correlated with receiving 5 ANC visits, a postpartum visit and a physical examination after delivery, which was consistent with the findings of existing studies. The health risk to the mother and fetus during pregnancy increases with the age of the women. Therefore, regular ANC in the early stages of pregnancy is crucial for the health of the mother and fetus in older pregnant women. Additionally, older primiparous women are more careful when giving birth than younger mothers and therefore utilize ANC more frequently.21 We also found a negative correlation between the number of biological children and the utilization of maternal healthcare for migrant pregnant women, both before and after delivery. This finding is consistent with existing research.9,22,23 According to studies, women who have given birth at least once have a limited grasp of the value of ANC.9 Zong thought that this was a result of the personal poor reproductive experience brought on the overuse of medical care. Many migrant pregnant women thought that they received unnecessary tests and treatments during pregnancy and childbirth, which increased their out-of-pocket health expenses. These individual experiences make migrant pregnant women prefer self-monitoring of their health over professional treatment.13 Minority migrant pregnant women were also less likely to utilize ANC in accordance with the advised standard. Traditional beliefs, low levels of education, poverty, and limited access to health services for women from ethnic minorities cause them to use maternity care less frequently.24
Similar to previous studies,25–28 we found that maternal healthcare utilization increased with education level, which may be related to healthcare awareness. The necessity and advantages of preventive health services are more likely to be understood by people with greater levels of education,29 and as a result, they are more likely to adopt preventive health behaviors.30 There is strong evidence that income affects how often mothers utilize healthcare services.31–34 Pregnant women with greater monthly household income are more financially capable and have better understanding about preventive healthcare. The likelihood of utilizing maternal healthcare services is also increased. According to a research by Rani and Lule, low-income adolescent mothers are more likely to be socially isolated and, as a result, are less likely to be covered by programs that encourage maternal healthcare utilization.35 Our study also found that employed women were less likely to have five or more ANC visits than unemployed women, but they were more likely to receive a physical examination within 42 days of giving birth. Migrant pregnant women with employment could fall short of the recommended ANC times compared to unemployed women because of their jobs. Due to the ample maternity leave, they are more likely to use postnatal healthcare after delivery. Additionally, as employment and income are frequently correlated, migrant pregnant women with employment are more likely to be financially independent, and have greater awareness and access to healthcare resources.36,37
Another factor related to the healthcare utilization of migrant pregnant women is health insurance. According to our study, individuals participating in any type of health insurance were more likely to establish the maternal health record within the first 12 weeks during pregnancy and receive a physical health examination within 42 days after delivery. Health insurance can lower out-of-pocket expenses faced by the insured through the co-payment mechanism, hence facilitating improved their access of healthcare.38 A multi-level medical security system, with different types of health insurance for different groups of population has been gradually established in China. Enterprise employees are required to participate in UEBMI, whereas rural and urban non-employed residents voluntarily choose to participate in NCMS and URBMI respectively.39 China’s basic medical insurance participation rate is currently stabilized at above 95%.40 The reimbursement ratios for different types of health insurance still vary to some extent, nevertheless. In comparison, UEBMI has the highest reimbursement rate and the widest reimbursement catalogue, followed by URBMI and NCMS.41 Due to the large benefits of UEBMI participants in reimbursement, migrant pregnant women with UEBMI have the highest likelihood of using maternal healthcare services. In 2016, China started to gradually integrate URBMI and NCMS to develop CURBMI to make urban and rural residents enjoy more fair health insurance reimbursement.42 Additionally, those who are insured in their hometown may choose not to use health services in the inflow residence due to lower reimbursement rates and cumbersome reimbursement procedures.43
Our study also revealed that pregnant women who migrated across cities within a province were more likely to use five ANC visits, and pregnant women who migrated across provinces were more likely to receive a physical examination within 42 days after delivery, which is different from previous studies. Tang et al found that women wither closer migration distance are more likely to utilize maternal healthcare services due to understanding of the policy of residence.21 We believe that with the implementation of the NEPHS and its increase of publicity, even the inter-provincial migrant pregnant women are aware of the policy of residence. In addition, the estimation results demonstrated women migrating over 4 years were more likely to use prenatal healthcare services, although the estimation results of postpartum healthcare utilization were not statistically significant. It is easier for those with longer migration duration to understand the policy in the place of residence and integrate into the local life.17
Receiving maternal health education was associated with an increase of the likelihood of using prenatal and postnatal healthcare. This is in line with an existing study,21 which highlights the value of reproduction education and contraception education for migrant pregnant women. According to studies, the migrant population had a relatively low level of health literacy, and they are unwilling to receive medical treatment even when they are sick.44 They disregard their own health issues due to a lack of health awareness. Su discovered that female migrant workers rarely visit hospitals only when they feel unbearable pain.45 A key strategy for raising health literacy is health education.46 Studies found that migrants who had access to health education were more likely to utilize healthcare services,44 and their health was also generally better.47 To improve the health literacy of the migrant population, in June 2016, the National Health and Family Planning Commission issued the Migrant Population Health Education and Promotion Action Plan (2016–2020). The plan specifically proposed to increase the health literacy of migrant population in the areas of basic medical care, infectious diseases prevention and treatment, maternity and child health, chronic illness prevention and treatment, and mental health.48 The results of our study supported the effectiveness of this strategy. Reproduction education and contraception education provided by medical personnel enable pregnant women to understand the significance of health management during pregnancy, so that they can make better use of healthcare services before and after delivery, and hence improve health outcomes of women and children.
There are several policy implications of our study. First of all, there has been a significant improvement in prenatal and postnatal healthcare utilization for migrant pregnant women, but there is still potential for improvement, particularly with regard to postnatal healthcare services. Improving the monitoring and tracking of pregnant migrant women will increase their utilization of postnatal healthcare services. Secondly, more focus should be placed on a subset of migrant pregnant women, such as those who are younger, have lower SES, are members of ethnic minorities, migrate over shorter distances and migrate for a shorter time. Targeted interventions can be taken to increase the utilization of maternal healthcare during pregnancy by these underserved groups. Last but not least, maintaining and enhancing the maternal health education for migrant pregnant women, as well as raising their awareness of health management and health literacy during pregnancy are essential steps to encourage their use of maternal healthcare and improve their health outcomes. Personalized healthcare information can be more effectively obtained by migrant pregnant women through publicity and the introduction of one-on-one health consultations.44
There are some limitations in this study. Firstly, the CMDS data are self-reported by participants. Even though the sample of the study is restricted to migrant pregnant with childbirth experience in the year prior to the survey, the potential recall bias cannot be avoided. Secondly, due to the availability of indicators, we are unable to account for all factors related to maternal healthcare, such as access to health services (although we did control regional variations in health resources by using regional dummy variables), which will be improved in future studies. Thirdly, since CMDS is a survey for migrant population, there is a lack of information on maternal health care for non-immigrant women, which makes it impossible to compare the differences in maternal health care utilization between migrant and local residents. In the future, we hope to further compare the differences between the two groups. Finally, because maternal healthcare services are only available to residents who have lived in the area for more than six months, CMDS does not conduct surveys of recently immigrated women. We could not include them for analysis, and the access to care by these women could modify the results of the study.
Conclusion
Using the recently available 2018 CMDS data at the national level, we examined the current state of prenatal and postnatal healthcare utilization among migrant pregnant women and their related factors. Our findings indicated that although there has been significant progress in prenatal and postnatal healthcare utilization for migrant pregnant women, there is still space for improvement. Age, education level, monthly household income, health insurance level, maternal health education during pregnancy were positively correlated with the degree of prenatal and postnatal healthcare utilization for migrant pregnant women. The number of children was negatively associated with the prenatal and postnatal healthcare utilization of this population. Additionally, the degree of prenatal care utilization for those who have been migrating for more than 4 years was higher than their counterparts, while migrant pregnant women who are members of ethnic minorities and employed were less likely to utilize prenatal healthcare. Taking targeted intervention measures, such as strengthening the follow-up of migrant pregnant women, focusing on pregnant women with low utilization degree of maternal healthcare, and continuously enhancing the reproduction education and contraception education of migrant pregnant women, can effectively promote the increase of the healthcare utilization during pregnancy among migrant population.
Abbreviations
NEPHS, National Essential Public Health Service; CMDS, China Migrants Dynamic Survey; NCMS, New Cooperative Medical Scheme; CURBMI, Coordinating of Urban and Rural Basic Medical Insurance; URBMI, Urban Resident Basic Medical Insurance; UEBMI, Urban Employee Basic Medical Insurance; ANC, Antenatal Care.
Data Sharing Statement
The data employed in our study is available on the website of China Migrants Dynamic Survey (https://chinaldrk.org.cn/wjw/#/home). The data belongs to the China National Health Commission and is free for researchers. We submitted the application on the website and received the data package.
Ethics Approval and Consent to Participate
The studies involving human participants were reviewed and approved by The 2018 China Migrants Dynamic Survey was approved by the China National Bureau of Statistics (No. Guotongzhi [2018] No. 45), and written informed consent was obtained from all participants at the time of data collection. All procedures performed in this study were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval was obtained from the Ethics Committee of Nanjing Medical University (REC: NJMU2022040).
Acknowledgments
We thank the Migrant Population Service Center, National Health Commission P.R. China, very much for providing the data of CMDS 2018.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Climbing Engineering-Scientific Research Innovation Project-Innovative Research Cultivation Project, Nanjing Medical University, grant number 06; Innovation Training Program for Students of Nanjing Medical University “Study on Health Effect and Policy Optimization of Urban and Rural Integration of Medical Insurance System”; Innovation Training Program for Students of Nanjing Medical University “Study on the Utilization of Basic Public Health Services for Patients with Chronic Diseases under the Background of Normalization of Epidemic Prevention and Control”.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. National Bureau of Statistics. The bulletin of seventh national census (No. 7); 2022. Available from: http://www.stats.gov.cn/tjsj/zxfb/202105/t20210510_1817183.html.
2. Li Y, Xiong C, Zhu Z, Lin Q. Family migration and social integration of migrants: evidence from Wuhan metropolitan area, China. Int J Environ Res Public Health. 2021;18(24):12983. doi:10.3390/ijerph182412983
3. Han S, Chen W, Ling L. Impact of migrant characteristics on maternal health care utilization among migrant pregnant women in China. Modern Prev Med. 2017;44(01):94–98.
4. You X, Tan H, Hu S, et al. Effects of preconception counseling on maternal health care of migrant women in China: a community-based, cross-sectional survey. BMC Pregnancy Childbirth. 2015;15:55. doi:10.1186/s12884-015-0485-4
5. Huang Y, Merkatz R, Zhu H, Roberts K, Sitruk-Ware R, Cheng L. The free perinatal/postpartum contraceptive services project for migrant women in Shanghai: effects on the incidence of unintended pregnancy. Contraception. 2014;89(6):521–527. doi:10.1016/j.contraception.2014.03.001
6. Sustainable Development Goals. Goal 3: ensure healthy lives and promote well-being for all at all ages. Sustainable Development Goals; 2022. Available from: https://www.un.org/sustainabledevelopment/zh/health/.
7. Beeckman K, Louckx F, Putman K. Determinants of the number of antenatal visits in a metropolitan region. BMC Public Health. 2010;10(1):527. doi:10.1186/1471-2458-10-527
8. Alexander GR, Kotelchuck M. Assessing the role and effectiveness of prenatal care: history, challenges, and directions for future research. Public Health Rep. 2001;116(4):306–316. doi:10.1016/S0033-3549(04)50052-3
9. Fan X, Zhou Z, Dang S, et al. Exploring status and determinants of prenatal and postnatal visits in western China: in the background of the new health system reform. BMC Public Health. 2018;18(1):39. doi:10.1186/s12889-017-4601-4
10. The Central People’s Government of the People’s Republic of China. Opinions on promoting gradual equalization of basic public health services; 2022. Available from: http://www.gov.cn/ztzl/ygzt/content_1661065.htm.
11. National standards for basic public health services. 20170417104506514.pdf; 2022. Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/04/20170417104506514.pdf.
12. Zhao Q, Huang ZJ, Yang S, Pan J, Smith B, Xu B. The utilization of antenatal care among rural-to-urban migrant women in Shanghai: a hospital-based cross-sectional study. BMC Public Health. 2012;12(1):1012. doi:10.1186/1471-2458-12-1012
13. Zong Z, Sun X, Mao J, Shu X. Maternal healthcare and associated factors among married migrant women in Changzhou, China. China popul dev stud. 2021;5(1):69–82. doi:10.1007/s42379-021-00077-7
14. Bryant AS, Haas JS, McElrath TF, McCormick MC. Predictors of compliance with the postpartum visit among women living in healthy start project areas. Matern Child Health J. 2006;10(6):511–516. doi:10.1007/s10995-006-0128-5
15. Tao F, Huang K, Long X, Tolhurst R, Raven J. Low postnatal care rates in two rural counties in Anhui Province, China: perceptions of key stakeholders. Midwifery. 2011;27(5):707–715. doi:10.1016/j.midw.2009.10.001
16. Gu H, You H, Ning W, et al. Internal migration and maternal health service utilisation in Jiangsu, China. Trop Med Int Health. 2017;22(2):124–132. doi:10.1111/tmi.12806
17. Li X, Zhou Z, Zhang W, et al. Health care services and influencing factors of floating pregnant women in Sichuan. Modern Prev Med. 2020;47(22):4098–4101+4120.
18. Hu H, Zhang W, Zhu Y, et al. Analysis on utilization status of maternal health care among the floating population in Changzhou. Maternal and Child Health Care of China. 2016;31(20):4106–4108.
19. Gong S, Wang H, Liu D. Utilization of the prenatal care services among married women of childbearing age in migrant population. Maternal and Child Health Care of China. 2017;32(10):2187–2189.
20. Gong S, Wang H, Liu D. Utilization of the postnatal care services among married women of childbearing age in migrant population. Chin Gen Pract. 2017;20(18):2257–2262.
21. Tang X, Ding L, Feng Y, Wang Y, Zhou C. Antenatal care use and its determinants among migrant women during the first delivery: a nation-wide cross-sectional study in China. BMC Pregnancy Childbirth. 2019;19(1):355. doi:10.1186/s12884-019-2520-3
22. Agus Y, Horiuchi S. Factors influencing the use of antenatal care in rural West Sumatra, Indonesia. BMC Pregnancy Childbirth. 2012;12(1):9. doi:10.1186/1471-2393-12-9
23. Trinh LTT, Dibley MJ, Byles J. Determinants of antenatal care utilization in three rural areas of Vietnam. Public Health Nurs. 2007;24(4):300–310. doi:10.1111/j.1525-1446.2007.00638.x
24. Huang Y, Martinez-Alvarez M, Shallcross D, et al. Barriers to accessing maternal healthcare among ethnic minority women in Western China: a qualitative evidence synthesis. Health Policy Plan. 2019;34(5):384–400. doi:10.1093/heapol/czz040
25. Wang H, Frasco E, Takesue R, Tang K. Maternal education level and maternal healthcare utilization in the Democratic Republic of the Congo: an analysis of the multiple indicator cluster survey 2017/18. BMC Health Serv Res. 2021;21(1):850. doi:10.1186/s12913-021-06854-x
26. Celik Y, Hotchkiss DR. The socio-economic determinants of maternal health care utilization in Turkey. Soc Sci Med. 2000;50(12):1797–1806. doi:10.1016/S0277-9536(99)00418-9
27. Lu MC, Prentice J. The postpartum visit: risk factors for nonuse and association with breast-feeding. Am J Obstet Gynecol. 2002;187(5):1329–1336. doi:10.1067/mob.2002.126848
28. Gu H, You H, Yan Z, et al. Determinants of the utilization of postpartum family visits: evidence from rural areas of Eastern China. PLoS One. 2018;13(3):e0194061. doi:10.1371/journal.pone.0194061
29. Ononokpono DN, Odimegwu CO, Imasiku ENS, Adedini SA. Does it really matter where women live? A multilevel analysis of the determinants of postnatal care in Nigeria. Matern Child Health J. 2014;18(4):950–959. doi:10.1007/s10995-013-1323-9
30. Kino S, Kawachi I. How much do preventive health behaviors explain education- and income-related inequalities in health? Results of Oaxaca–Blinder decomposition analysis. Ann Epidemiol. 2020;43:44–50. doi:10.1016/j.annepidem.2020.01.008
31. You H, Yu T, Gu H, et al. Factors associated with prescribed antenatal care utilization: a cross-sectional study in eastern Rural China. INQUIRY. 2019;56:004695801986543. doi:10.1177/0046958019865435
32. Li C, Zeng L, Dibley MJ, Wang D, Pei L, Yan H. Evaluation of socio-economic inequalities in the use of maternal health services in rural western China. Public Health. 2015;129(9):1251–1257. doi:10.1016/j.puhe.2015.07.002
33. Doctor HV. Intergenerational differences in antenatal care and supervised deliveries in Nigeria. Health and Place. 2011;17(2):480–489. doi:10.1016/j.healthplace.2010.12.003
34. Mekonnen T, Dune T, Perz J. Maternal health service utilisation of adolescent women in sub-Saharan Africa: a systematic scoping review. BMC Pregnancy Childbirth. 2019;19(1):366. doi:10.1186/s12884-019-2501-6
35. Rani M, Lule E. Exploring the socioeconomic dimension of adolescent reproductive health: a multicountry analysis. Int Fam Plan Perspect. 2004;30(3):110–117. doi:10.1363/3011004
36. Khanal V, Adhikari M, Karkee R, Gavidia T. Factors associated with the utilisation of postnatal care services among the mothers of Nepal: analysis of Nepal Demographic and Health Survey 2011. BMC Women’s Health. 2014;14(1):19. doi:10.1186/1472-6874-14-19
37. Iacoella F, Tirivayi N. Determinants of maternal healthcare utilization among married adolescents: evidence from 13 Sub-Saharan African countries. Public Health. 2019;177:1–9. doi:10.1016/j.puhe.2019.07.002
38. Manning WG, Newhouse JP, Duan N, Keeler EB, Leibowitz A, Marquis MS. Health insurance and the demand for medical care: evidence from a randomized experiment. Am Econ Rev. 1987;77(3):251–277.
39. Yip WCM, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of China’s huge and complex health-care reforms. Lancet. 2012;379(9818):833–842. doi:10.1016/S0140-6736(11)61880-1
40. National Healthcare Security Administration. 2021 National healthcare security development statistics bulletin; 2022. Available from: http://www.nhsa.gov.cn/art/2022/6/8/art_7_8276.html.
41. Li C, Yu X, Butler JRG, Yiengprugsawan V, Yu M. Moving towards universal health insurance in China: performance, issues and lessons from Thailand. Soc Sci Med. 2011;73(3):359–366. doi:10.1016/j.socscimed.2011.06.002
42. Meng Q, Fang H, Liu X, Yuan B, Xu J. Consolidating the social health insurance schemes in China: towards an equitable and efficient health system. Lancet. 2015;386(10002):1484–1492. doi:10.1016/S0140-6736(15)00342-6
43. Tian Y, Chen Y, Zhou M, Zhao S. Institutional design and incentives for migrant workers to participate in social insurance in China: evidence from a policy experiment in Chengdu City. Front Public Health. 2021;9:736340. doi:10.3389/fpubh.2021.736340
44. Tian Y, Luo T, Chen Y. The promotional effect of health education on the medical service utilization of migrants: evidence from China. Front Public Health. 2022;9:818930. doi:10.3389/fpubh.2021.818930
45. Su S, Zhang F, Liu Q, et al. Factors associated with utilization of reproductive healthcare services among migrant women workers in Chong Qing, China. Int J Gynaecol Obstet. 2014;127(1):66–68. doi:10.1016/j.ijgo.2014.04.005
46. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97. doi:10.7326/0003-4819-155-2-201107190-00005
47. Xu X, Zhang Q, You H, Wu Q. Awareness, utilization and health outcomes of national essential public health service among migrants in China. Front Public Health. 2022;10:936275. doi:10.3389/fpubh.2022.936275
48. National Health and Family Planning Commission. The migrant population health education and promotion action plan (2016-2020); 2022. Available from: http://www.nhc.gov.cn/rkjcyjtfzs/zcwj2/201606/07c9bacc1312433ca2860ded46a667e0.shtml.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.