Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Factors Associated with Influenza and Pneumococcal Vaccine Hesitancy Among Patients with AECOPD: A Cross-Sectional Study in China Using the 3C Model
Authors Xin Y, He R, Ren X, Yang T ![]() , Wang Y, Su X
, Wang Y, Su X
Received 9 September 2025
Accepted for publication 22 December 2025
Published 28 December 2025 Volume 2025:20 Pages 4159—4171
DOI https://doi.org/10.2147/COPD.S566403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
You Xin,1 Ruoxi He,1,2 Xiaoxia Ren,3– 6 Ting Yang,3– 6 Ye Wang,1,* Xiaoyou Su1,*
1School of Population Medicine and Public Health, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China; 2Department of Respiratory Medicine, National Key Clinical Specialty, Branch of National Clinical Research Center for Respiratory Disease, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China; 3Department of Pulmonary and Critical Care Medicine, Center of Respiratory Medicine, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China; 4Institute of Respiratory Medicine, Chinese Academy of Medical Sciences, Beijing, 100029, People’s Republic of China; 5National Center for Respiratory Medicine, Beijing, 100029, People’s Republic of China; 6National Clinical Research Center for Respiratory Diseases, Beijing, 100029, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ye Wang, Email [email protected] Xiaoyou Su, Email [email protected]
Background and Aims: COPD patients are prioritized for influenza and pneumococcal vaccines, yet vaccination rates remain low, indicating vaccine hesitancy. This study aimed to investigate the vaccination rates and the underlying determinants of vaccine hesitancy, as the primary behavioral driver of low coverage, among patients hospitalized for Acute Exacerbation of COPD (AECOPD).
Methods: From September 2022 to October 2023, 536 patients hospitalized due to AECOPD from eight hospitals in China were surveyed on their vaccination status (influenza or pneumococcal). Data on vaccination status and a structured 3C model (confidence, complacency, convenience) questionnaire were collected. Logistic regression identified factors associated with vaccination behavior, while structural equation modeling (SEM) elucidated the pathways through which the 3C components directly influence vaccine hesitancy.
Results: The overall vaccination rate was 16.8% (90/536). Key factors associated with the vaccination behavior included high CAT score (aOR=5.64), pulmonary infection (aOR=2.28), former smoking (aOR=0.35), regular inhaled medication (aOR=0.47), high mMRC score (aOR=0.29), and bronchiectasis (aOR=0.40). Critically, the SEM analysis revealed that vaccine hesitancy was primarily driven by complacency, manifesting as a “lack of perceived need” (78%). This complacency was significantly influenced by a lack of confidence in vaccine safety and effectiveness, and compounded by convenience barriers like geographical inaccessibility and financial costs. The 3C model analysis quantified these relationships, with convenience (path coefficient=0.896) and confidence (0.375) positively impacting vaccination, while complacency showed a slight negative effect (− 0.002).
Conclusion: Low vaccination rates in AECOPD patients were mainly due to perceived lack of necessity, linked to vaccine hesitancy. This hesitancy was mainly driven by underestimation of disease severity. Integrated interventions are essential to improve vaccination uptake in this at-risk group.
Keywords: chronic obstructive pulmonary disease, COPD, vaccine hesitancy, influenza and pneumococcal vaccine
Introduction
Chronic obstructive pulmonary disease (COPD) is a common condition marked by progressive, irreversible airflow limitation.1 Moving beyond this traditional physiological definition, contemporary understanding reframes COPD as a disease of failed lung repair and regeneration, characterized by aberrant differentiation of distal airway progenitor cells that leads to irreversible structural remodeling.2 This pathophysiological insight aligns with ongoing scholarly discourse advocating for a fundamental revision of the COPD definition itself, emphasizing its essential nature as a condition that places patients at a biological disadvantage due to these structural and regenerative failures, rather than relying solely on airflow criteria.3 As the third leading cause of death globally, it affects over 200 million people and causes 3.3 million deaths annually.4 The burden of COPD continues to rise, with increasing morbidity and mortality expected through at least 2030.5 Globally, COPD poses significant social and economic challenges, with a disproportionate impact on the elderly.6 In China, while age-standardized COPD rates have declined, it remains a leading cause of death and disability, primarily attributable to widespread risk factors like smoking (46.0% of DALYs globally) and air pollution, which continue to impose high costs and impair the quality of life for millions.4 A large nationwide representative study conducted during 2014–2015 estimated the overall prevalence of COPD among adults aged 40 years and above in China to be 13.6%, underscoring the vast population affected by this condition.7 Exacerbation prevention is a key goal of therapy in COPD.8 Acute exacerbations of COPD (AECOPD), often triggered by infections, pollutants,9 and comorbid conditions, worsen lung function,10 increase hospitalizations and contribute to mortality, which can not only increase the healthcare burden but also significantly impair patients’ daily activities and overall well-being.11,12
Vaccination against influenza and pneumococcus is key to preventing hospitalizations and mortality in AECOPD patients, as these infections are major triggers of exacerbations.5,13,14 Evidence confirms that co-infections significantly increase the clinical burden in AECOPD. For instance, patients with concomitant pneumonia (involving pathogens such as S. pneumoniae and influenza viruses) had a significantly higher risk of admission to the intensive care unit (RR=2.79, 95% CI: 1.47–5.28) and prolonged hospital stays.15 Furthermore, a systematic review and meta-analysis demonstrated that AECOPD patients with concomitant pneumonia faced significantly elevated mortality risks during hospitalization (RR=2.29, 95% CI: 1.40–3.73), within one month after discharge (RR=1.84, 95% CI: 1.09–3.13), and in long-term follow-up (HR=2.30, 95% CI: 1.15–4.61) compared to those without pneumonia.16 The need for such protection is further underscored by the finding that cigarette smoking is the strongest independent risk factor for invasive pneumococcal disease, with a population attributable risk of 51%.17 Crucially, vaccination serves as a powerful protective measure. Evidence from the Advisory Committee on Immunization Practices (ACIP) indicates that influenza vaccination is effective in preventing hospitalizations for pneumonia and influenza among high-risk adults.6,17 This protective effect is corroborated by a large cohort study in the elderly, which demonstrated that influenza vaccination significantly reduced in-hospital mortality for COPD (Relative Risk: 0.53).18 The critical importance of vaccination for the Chinese COPD population is strongly supported by recent local evidence. A real-world prospective cohort study in China confirmed that influenza vaccination significantly reduces the risk of future exacerbations. Multivariate analysis demonstrated that it was associated with a reduction in the risk of any acute exacerbation (aOR = 0.48; 95% CI = 0.33–0.68, P < 0.01), that in frequent acute exacerbations (aOR = 0.47; 95% CI = 0.27–0.82, P = 0.01), and that in severe acute exacerbations (aOR = 0.38; 95% CI = 0.23–0.63, P < 0.01).19
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) recommends influenza vaccination for COPD patients due to its ability to reduce hospitalizations and mortality rates associated with AECOPD. Additionally, GOLD recommends pneumococcal vaccination for COPD patients to prevent community-acquired pneumonia, which is a common cause of exacerbations and increased morbidity.20 In line with GOLD, the Chinese national guidelines for COPD diagnosis and management21 also strongly recommend influenza and pneumococcal vaccination for COPD patients. However, this preventive strategy is critically underutilized globally, with substantial disparities in coverage. While countries like France achieve influenza and pneumococcal vaccination rates of 73.0% and 53.0% respectively in COPD patients, and the United States reports rates around 30–50% for influenza,22 coverage in China remains alarmingly low, with weighted rates of only 2.09% for influenza, 1.25% for pneumococcal, and 2.72% for both vaccines.23 Exploring effective interventions to bridge this gap is paramount. Evidence suggests that clinician-led intensive health education—comprising face-to-face communication, distribution of health brochures, and text message reminders—can dramatically improve uptake. This approach was shown to increase the influenza vaccination rate among COPD outpatients in China from a baseline of 1.6% to 12.2% (P < 0.01), corresponding to an 8.86-fold higher odds of vaccination (aOR = 8.86; 95% CI = 6.71–11.6, P < 0.01).19
Vaccine hesitancy, defined by the WHO as the delay in acceptance or refusal of vaccination despite the availability of vaccination services, is a major challenge to global immunization efforts.24 It is driven by misconceptions about natural immunity, cognitive biases (such as prioritizing immediate costs over long-term benefits), and safety concerns amplified by social media misinformation. The WHO listed vaccine hesitancy as a top global health threat in 2019,24 highlighting the need to address it to improve vaccination coverage. Globally, significant disparities exist: vaccination rates in China is significantly lower than in other countries. Given the low vaccination rates and the limited research on vaccine hesitancy regarding influenza and pneumococcal vaccines among patients with AECOPD in China, the objective of this study is to investigate the vaccination rates and identify the factors contributing to vaccine hesitancy in this population.
Methods
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committees of the Chinese Academy of Medical Sciences and Peking Union Medical College (No. CAMS&PUMC-IEC-2022-024). Written informed consent was obtained from all participants.
Study Population
This cross-sectional study was conducted from September 2022 to October 2023. The sample size calculation for this study was based on the primary objective of the cross-sectional survey: to estimate the vaccination coverage rate among AECOPD patients. Based on previous literature, the overall vaccination rate (P) for either influenza or pneumococcal vaccines in AECOPD patients was assumed to be 2.5%. The sample size was calculated using the formula for cross-sectional studies:
Where α was set at 0.05 (two-sided), yielding Z1-α/2≈1.96, and the margin of error (δ) was set at 0.02. The minimum required sample size was calculated to be approximately 234. Furthermore, accounting for a potential 50% rate of invalid questionnaires and loss to follow-up, the sample size was increased accordingly. The final plan was to recruit at least 468 patients. Ultimately, this study successfully enrolled 536 eligible AECOPD patients (refer to Supplementary Material 2). These hospitals were located across different regions (Beijing, Tianjin, Hebei, Hunan, Jiangxi, Guangxi, and Guangdong) to ensure diversity in the sample (see Supplementary Material 4).
Eligibility criteria for the participants were as follows: 1) Age ≥18 years; 2) Hospitalization for confirmed AECOPD; 3) Written informed consent was obtained from participants. Exclusion criteria included: 1) Refusal to sign the informed consent form; 2) Being enrolled in other drug clinical trials or interventional studies. Additionally, those without a confirmed diagnosis of COPD (based on spirometry) were excluded. The diagnosis of COPD was confirmed using a post-bronchodilator forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) ratio (FEV1/FVC) of <0.7.25 AECOPD was defined as a spirometry-confirmed COPD with acute worsening of respiratory symptoms requiring additional therapy.26
Procedures and Measurements
The study utilized a comprehensive questionnaire to gather detailed information from participants (refer to Supplementary Material 1). The questionnaire was divided into several sections, each designed to capture specific aspects of the participants’ health status and behaviors. The sections included: 1) Demographic characteristics and smoking history; 2) Medical history related to COPD, including time since diagnosis, history of acute exacerbations, and prior treatments; 3) Self-reported vaccination status against influenza and pneumonia; 4) Assessment of respiratory symptoms and functional status using validated scales such as the mMRC dyspnea scale and the CAT; 5) Documentation of complications and comorbid conditions; and 6) A dedicated section to explore reasons for vaccine hesitancy.
Upon enrollment, clinicians recorded participants’ demographic characteristics (age group, gender, education level, smoking status) and medical history (years since diagnosis with COPD, frequence of severe acute exacerbation in the past year, regular inhaled medication treatment in the past year). Self-reported influenza and pneumococcal vaccination status were determined using the following question: “Have you ever received an influenza vaccine or a pneumonia vaccine to prevent acute exacerbations of COPD?” Data on other clinical variables, including Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage, modified Medical Research Council (mMRC) dyspnea scale, COPD assessment test (CAT), complications and comorbidities like pulmonary infection and bronchiectasis were also collected.
In addition, the study gathered insights into vaccine hesitancy through a dedicated questionnaire section entitled “Reasons for not receiving influenza and pneumonia vaccines,” which offered multiple-choice options, each accompanied by a checkbox for selection. The options provided were as follows: 1) I am unaware that I need to get vaccinated (Lack of perceived need), 2) I am very healthy and do not need to be vaccinated (Health status overconfidence), 3) I believe the diseases are not harmful enough, so there is no need (Disease severity underestimation), 4) I am concerned about the potential adverse reactions to the vaccine (Vaccine safety concerns), 5) I think the vaccines are ineffective or have limited effectiveness (Vaccine effectiveness doubt), 6) I consider the vaccine prices too expensive (Financial barriers), 7) The vaccination sites are inconveniently located (Geographical inaccessibility), and 8) I do not know where to get vaccinated (Lack of vaccination site awareness). An additional “Other” option was available, offering a blank space for respondents to provide further comments or specify reasons not listed. In the 3C model, the options 1, 2 and 3 are grouped into Complacency, options 4 and 5 are grouped into Confidence, and options 6, 7, and 8 are grouped into Convenience. The questions assessing reasons for vaccine hesitancy were developed based on the World Health Organization (WHO) SAGE Working Group’s “3C” model of vaccine hesitancy (Complacency, Confidence, Convenience). The model provides a well-established conceptual framework for understanding hesitancy, and the questions were designed to directly map onto its core dimensions, ensuring content validity.
Definitions
The independent variables in this study were the sociodemographic and clinical characteristics of the participants. Demographic characteristics included age group, categorized as <65 years and ≥65 years. Education level was classified into three categories: primary school and below, junior high school, and senior high school or above. As for smoking status, participants were categorized as current smokers, former smokers, or never smoked. The medical history of participants was detailed, including the number of years since their COPD diagnosis (<1, 1–5, 6–10, and >10), the occurrence of severe acute exacerbations in the past year (yes/no), and their regular use of inhaled medication treatment (yes/no). Clinical variables such as the GOLD stage, mMRC dyspnea scale, and CAT were recorded to evaluate the disease severity and impact on patients’ daily lives. The GOLD stage was classified into four stages based on post-bronchodilator percentage predicted FEV1 (FEV1%pred), with ≥80.0%, 50% to <80%, 30% to <50%, and <30% representing GOLD stages 1–4, respectively.27 The mMRC is a widely accepted and validated instrument for assessing dyspnea, and its use and categorization (scores 1–2 vs ≥2) are supported by established guidelines.28 The CAT is a validated, patient-completed questionnaire for assessing health status in COPD.29 In our study, the internal consistency of the CAT, as measured by Cronbach’s alpha, was 0.82, indicating high reliability. Complications and comorbidities include pulmonary infection and bronchiectasis.
Statistical Analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics of both vaccinated and unvaccinated patients, including key factors such as age, gender, underlying health conditions, and vaccination status. The distribution of vaccine hesitancy reasons was analyzed and presented as percentage breakdowns, with further classification in the largest patient groups to provide deeper insights into the primary causes of hesitancy. Additionally, a breakdown of vaccine hesitancy reasons across various demographic and clinical factors was conducted. Categorical variables were presented as numbers (%) and compared using the Chi-squared test. To determine the factors associated with vaccination rates, multivariable logistic regression models were used, adjusting for demographic and clinical factors. Adjusted Odds Ratios (aORs) and their 95% confidence intervals (CIs) were calculated.
Given the relatively low vaccination rates, Structural Equation Modeling (SEM) was employed to investigate the relationship between the 3C model and vaccination status. The numbers represent the path coefficients between different variables, with the absolute value reflecting the strength of the effect. A larger coefficient indicates a stronger influence. The sign of the path coefficient reveals the direction of the relationship: a positive sign (+) indicates a positive effect, meaning that an increase in one variable leads to an increase in another, whereas a negative sign (-) indicates a negative effect, meaning that an increase in one variable results in a decrease in another.30 Pearson correlations were utilized to analyze relationships between reasons for vaccine hesitancy. Missing values were imputed using the multiple imputation by chained equations method,31 specifically to fill in the FEV1%pred values for 160 patients. All statistical analyses were performed using SPSS 26.0 for data management, R 4.41 for analysis, and Mplus 8.3 for SEM analysis. Two-tailed P value <0.05 was considered statistically significant.
Results
Characteristics of the Study Participants
A total of 536 AECOPD patients from eight Chinese hospitals were surveyed for this study. The overall influenza or pneumococcal vaccination rate among COPD patients was 16.8% (90/536). Table 1 shows that vaccinated patients were less likely to be current smokers and had a longer history of COPD. They also experienced more severe acute exacerbations in the past year and were more likely to adhere to regular inhaled treatments. Patients with a lower mMRC score were less likely to receive vaccination. Additionally, patients with pulmonary infections had a lower vaccination rate, while those with bronchiectasis had a higher vaccination rate.
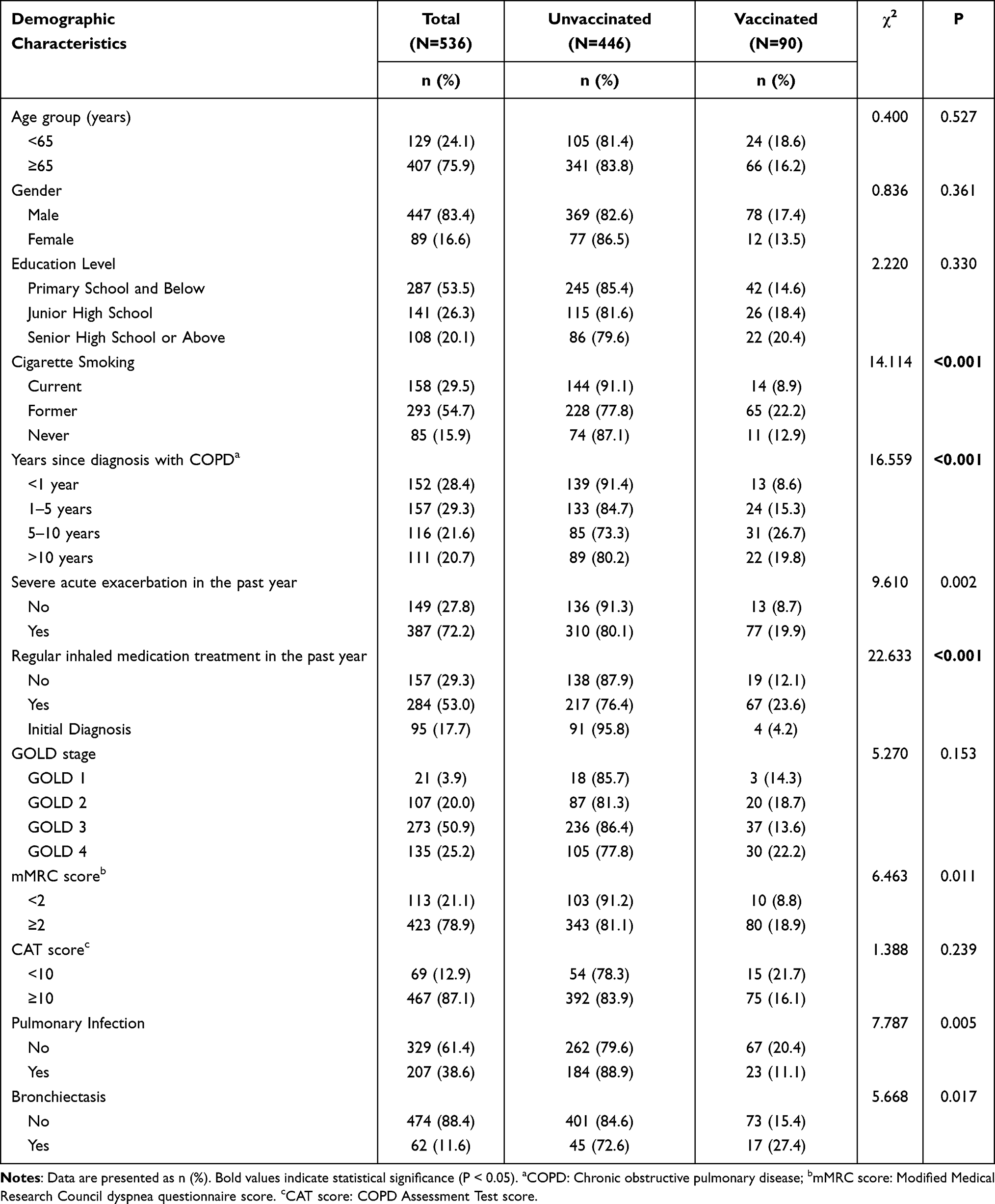 |
Table 1 Basic Characteristics of Patients with AECOPD and the Influenza or Pneumococcus Vaccination Rate by Characteristics. (N=536) |
Influenza and Pneumococcal Vaccination Coverage
The vaccination rates differed significantly across patient groups. Former smokers exhibited the highest rate at 22.2% (65/293), whereas non-smokers and current smokers had rates of 12.9% (11/85) and 8.9% (14/158), respectively (P<0.001). Patients diagnosed with COPD for 5–10 years had the highest vaccination rate (26.7%, 31/116), followed by those diagnosed for more than 10 years (19.8%, 22/111) and for 1–5 years (15.3%, 23/157), while those diagnosed for less than a year had the lowest rate (8.6%, 13/152, P<0.001). Patients with severe acute exacerbations in the past year were more likely to be vaccinated (19.9%, 77/387) than those without (8.7%, 13/149, P=0.002). Those who received regular inhaled medication treatments in the past year had a higher vaccination rate (23.6%, 67/284) compared to those without regular treatment (12.1%, 19/157) and newly diagnosed patients (4.2%, 4/95, P<0.001). An mMRC score less than 2 was associated with a lower vaccination rate (8.8%, 10/113) compared to a score of 2 or higher (18.9%, 80/423, P=0.011). Patients with pulmonary infections had a lower vaccination rate (11.1%, 23/207) compared to those without (20.4%, 67/329, P=0.005), and those with bronchiectasis had a higher rate (27.4%, 17/62) compared to those without (15.4%, 73/474, P=0.017). The influenza and pneumococcal vaccination coverage in patients with different characteristics was also shown in Table 1.
Multivariable Analysis for Factors Associated with Vaccination
In the multivariable analysis, factors associated with higher vaccination rates included former smoking (aOR=0.35, P=0.002), regular inhaled medication treatment (aOR=0.47, P=0.016), high CAT score (aOR=5.64, P<0.001), high mMRC score (aOR=0.29, P=0.014), having a pulmonary infection (aOR=2.28, P=0.004), and having bronchiectasis (aOR=0.40, P=0.009). Factors associated with influenza and pneumococcal vaccines were shown in Figure 1.
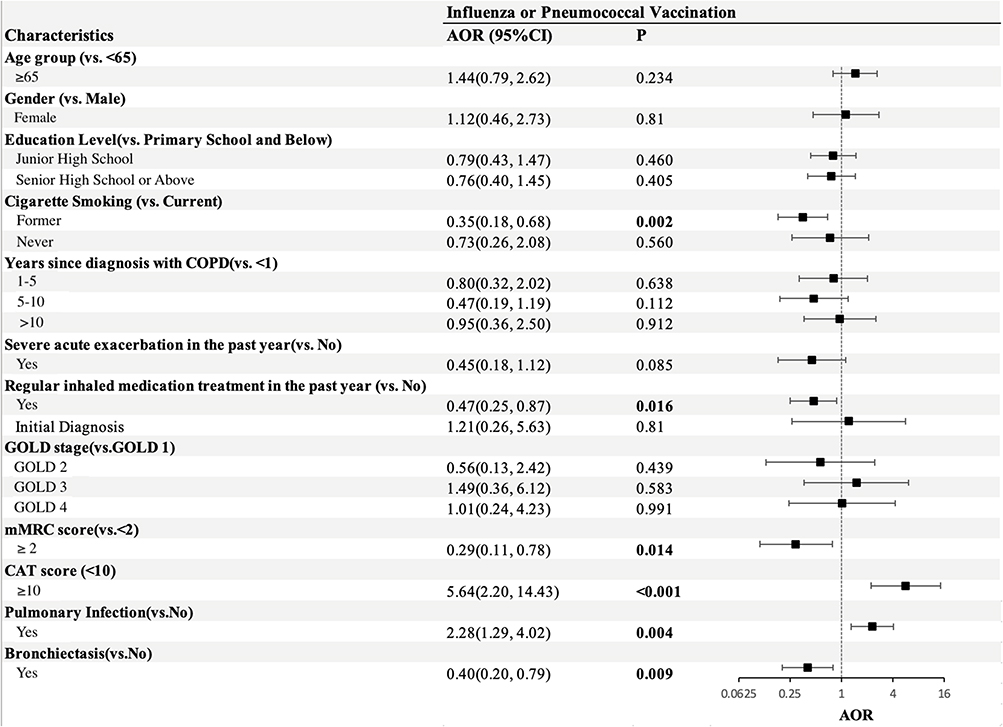 |
Figure 1 Forest plot for associated factors of influenza or pneumococcal vaccination among patients with AECOPD (N=536). Bold values indicate statistical significance (P < 0.05). |
Reasons for Vaccine Hesitancy Among AECOPD Patients Based on the 3C Model
Based on the 3C model, it can be seen from Figure 2 that the primary reasons for vaccine hesitancy were “lack of perceived need” in Complacency (78%), followed by “lack of awareness of vaccination sites” in Convenience (27%), and “vaccine safety concerns” in Confidence (13%). Other contributing factors included overconfidence in health status (7%), doubts about vaccine effectiveness (7%), geographical inaccessibility (6%), underestimation of disease severity (4%), and financial barriers (3%). To further explore the reasons for vaccine hesitancy among AECOPD patients in each group, A table of Factors Contributing to Vaccine Hesitancy in AECOPD Patients (see Supplementary Material 3) was generated, revealing that patients requiring more intensive treatment—such as those with severe exacerbations in the past year, high mMRC or CAT scores, or those with pulmonary infections and bronchiectasis—were more likely to cite “geographical inaccessibility” and “financial barriers” as reasons for not getting vaccinated, compared to their counterparts.
 |
Figure 2 Reasons for vaccine hesitancy among AECOPD patients (n=449). Colors correspond to the 3C model dimensions: purple for Complacency, green for Confidence, and yellow for Convenience. |
Figure 3 presents the SEM analysis of the 3-C model components influencing vaccination. The results indicate that convenience (coefficient=0.896) and confidence (coefficient=0.375) positively affect vaccination uptake, with convenience exerting a stronger influence. Conversely, complacency has a negligible negative impact (coefficient=−0.002) on vaccination willingness. Specifically, convenience is negatively impacted by geographical inaccessibility (−13.762), financial barriers (−1.000), and lack of awareness of vaccination sites (−3.762). Among these factors, geographical inaccessibility stands out as the most significant barrier to convenience. Confidence is increased in the absence of vaccine safety concerns (−3.052) and doubts about vaccine effectiveness (−1.000), with safety concerns having a more pronounced negative impact. Meanwhile, complacency is driven by underestimating disease severity (0.016), lack of perceived need (0.001), and health status overconfidence (0.049), all of which slightly diminish the willingness to get vaccinated.
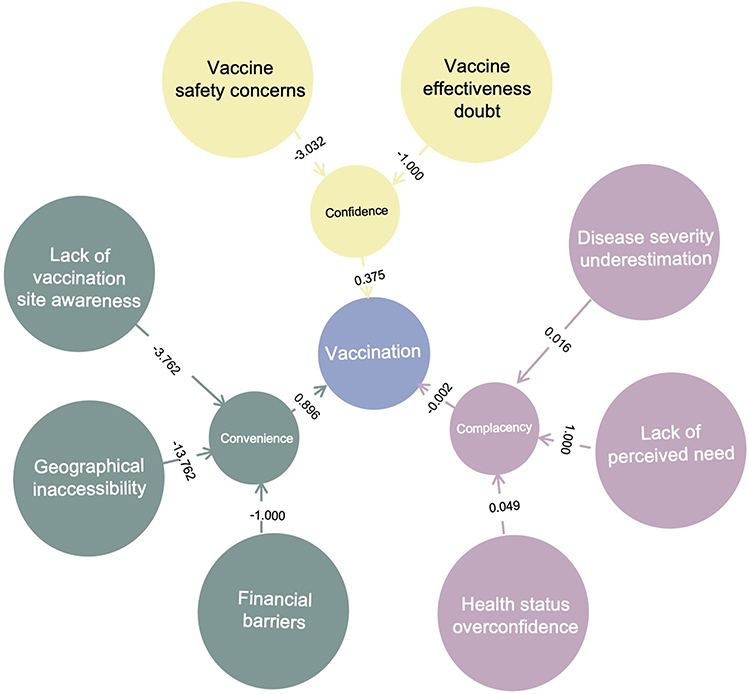 |
Figure 3 Structure Equation Model (SEM) of the reasons for vaccination among patients with AECOPD. Colors correspond to the 3C model dimensions: purple for Complacency, green for Convenience, and yellow for Confidence. |
Pearson correlation analysis clearly shows that the reason “Lack of perceived need” is negatively correlated with other factors, particularly “vaccine safety concerns” (see Figure 4). Building on this, Figure 5 further compares other reasons for vaccine hesitancy between AECOPD patients who lack a perceived need and those who perceive one. Among patients without a perceived need, 33% frequently doubted vaccine effectiveness, while 42% of those who perceived a need tended to underestimate disease severity.
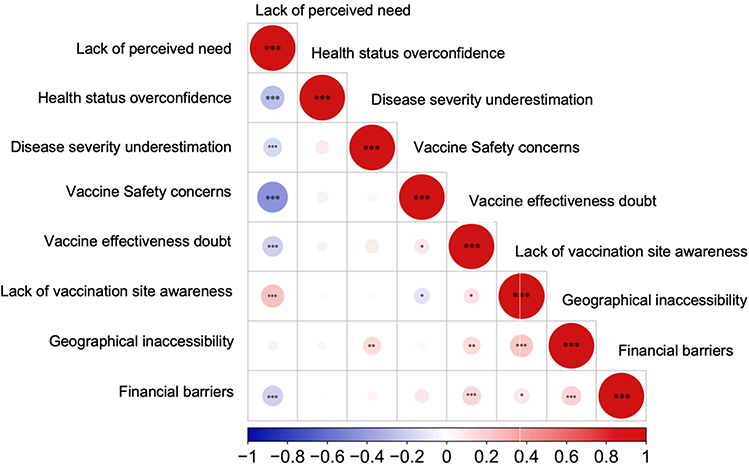 |
Figure 4 Pearson correlation figure of reasons for vaccine hesitancy among AECOPD patients (n=449). ***P < 0.001, **P < 0.01, *P < 0.05. |
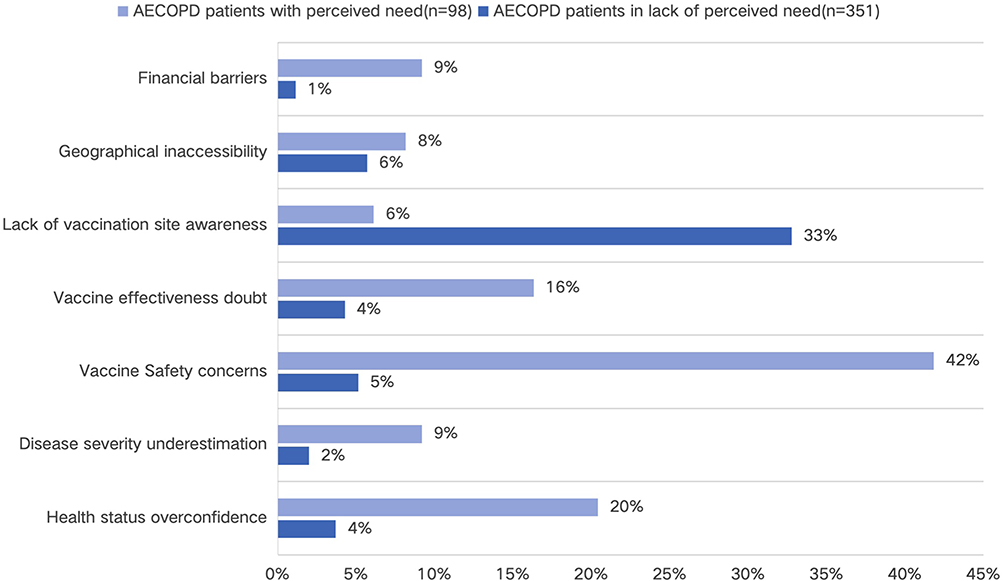 |
Figure 5 Comparison of other reasons for vaccine hesitancy between those in lack of perceived need and those with it among AECOPD patients. |
Discussion
COPD patients are highly vulnerable to respiratory infections, which can lead to exacerbations, hospitalizations, and increased mortality.5 Despite being a priority group for vaccination, COPD patients in China exhibit strikingly low vaccination coverage, with only 16.8% of AECOPD patients receiving influenza or pneumococcal vaccines, an improvement from the previous 2.72% recorded between 2017−2021.23 Yet, it remains substantially lower than the 12.2% uptake achieved through a clinician-led educational intervention in another Chinese study.19 This contrast underscores both the persistent coverage gap and the significant potential of targeted strategies to improve vaccination rates.This modest increase may reflect reduced vaccine hesitancy due to public health initiatives and heightened disease awareness during the COVID-19 pandemic. However, significant gaps in vaccination coverage remain, highlighting the need for continued efforts to address vaccine hesitancy and improve uptake.32,33 For instance, Turkey reported 36.5% for influenza and 14.1% for pneumococcal vaccination in COPD outpatients; Italy had 30.5% and 13.3%, respectively; Spain had 49.4% for influenza and 32.5% for pneumococcal; Germany showed 46.5% and 14.6%, while France had the highest rates, with 73.0% for influenza and 53.0% for pneumococcal vaccines. The UK had 36.1% and 16.8%, respectively.22 In Norway, the influenza vaccination rate among hospitalized COPD patients was 70.6%, while in Canada, it was 58.7%.32,33
One of the key findings is that smoking cessation acts as a protective factor for vaccination uptake. Smokers who quit are more likely to get vaccinated, likely because they recognize the harm that smoking does to the lungs and its role in exacerbating COPD.34 This pattern is not unique to China. For instance, a study on Japanese healthcare workers revealed that smoking was a significant risk factor for lower antibody titres after COVID-19 vaccination, and importantly, current smokers had significantly lower antibody levels than former smokers. This finding suggests that quitting smoking, even before vaccination, can enhance the vaccine’s immunological outcome, potentially motivating smokers to engage in vaccination as a more beneficial health intervention when they cease smoking.35 This behavior contrasts with the complacency effect described in the 3C model, specifically health status overconfidence for smokers who quit are less likely to underestimate the severity of their condition or assume that their health is sufficient. To reduce smoking rates and increase vaccination coverage among AECOPD patients, government-sponsored anti-smoking campaigns and smoking cessation programs targeting COPD patients in communities36 should be expanded.
Secondly, patients who have adhered to regular inhaled medication treatment in the past year are more likely to receive the vaccine. This adherence indicates a lower risk of complacency about the severity of their condition and suggests they are less prone to experiencing health status overconfidence. Additionally, these patients may have greater trust in medical interventions in general, which could reduce concerns about vaccine safety and effectiveness.37 To foster a greater sense of trust in medical treatments like vaccination, it is critical to increase public awareness of its benefits by taking measures like initiating public awareness campaigns in communities,38 or incentivizing healthcare providers to emphasize the importance of vaccination.39 Additionally, providing subsidies for the medication and vaccines with strict supervision40 could possibly lower financial barriers for patients, especially for those on long-term treatment plans.
Thirdly, the mMRC score, which measures the severity of dyspnea, reveals that patients with lower scores might experience complacency and underestimate the need for vaccination when their symptoms are manageable. A key intervention here would be patient education16 on the risks associated with influenza and pneumococcal diseases, regardless of the current severity of their COPD symptoms. Tailored educational campaigns41 should emphasize that vaccinations can prevent exacerbations and hospitalizations, reducing the long-term impact of these diseases.
Interestingly, higher CAT scores, which indicate more severe COPD, are associated with lower vaccination rates. Patients with severe symptoms often face physical limitations and may suffer from psychological issues such as depression or anxiety, which can impact their willingness to engage in health-promoting behaviors, including vaccination. This reflects the convenience barrier such as geographical inaccessibility8, and psychological and physical limitations that create a perceived difficulty in getting vaccinated. A holistic approach to managing COPD should be adopted. In addition to physical treatments, mental health support must be integrated into the management of severe COPD.42
Additionally, patients with a history of pulmonary infections may exhibit vaccine hesitancy, likely due to concerns about vaccine safety and effectiveness, particularly if they fear the vaccine might worsen their pulmonary condition43. This behavior can be explained by the vaccine safety concerns and vaccine effectiveness doubts associated with the confidence barrier. This indicates that public health campaigns should focus on dispelling myths regarding the safety and efficacy of vaccines in patients with pulmonary infections.43. Health communication strategies should involve trusted healthcare providers in educating patients about the scientific evidence supporting vaccination for those with respiratory conditions.39
As for patients with bronchiectasis, they are more likely to receive vaccinations. This may be because they are less prone to complacency and are more attuned to their health needs, likely due to the chronic nature of their condition.44 Such patients tend to avoid health status overconfidence, which can lead to underestimating the severity of their disease and a lack of perceived need for vaccination. This indicates that continued education on the importance of vaccination as part of their ongoing health management is effective and should be further strengthened to help reduce complacency and increase vaccine uptake. We can provide personalized educational materials41 about the risks associated with respiratory infections such as influenza and pneumococcal diseases, explaining how vaccinations can help reduce exacerbations and hospitalizations. Besides, healthcare providers can be influential in continuing to advocate for vaccination.39
An analysis of the reasons for vaccine hesitancy identifies three major barriers: a lack of perceived need, a lack of awareness of vaccination sites, and concerns about vaccine safety. While the first and third barriers can be addressed through educational campaigns, the lack of awareness of vaccination sites can be tackled by increasing information dissemination through multiple channels such as TV, radio, social media, SMS, and printed materials like flyers and posters45 at community health centers, hospitals, and pharmacies. Community health workers and volunteers46 can also be mobilized to directly inform residents, while organizing local health events and consultations to raise awareness. Additionally, developing a dedicated website or app for site search and appointments, along with integrating vaccination locations on popular map platforms, will make it easier for people to find nearby sites.47 Clear signage at key public locations and recognizable markers at vaccination sites will further guide individuals. Lastly, providing real-time updates48 on site availability ensures that people receive the most current information, addressing any closures or changes promptly. Pearson correlation analysis further suggests that for patients who do not perceive a need for vaccination, educational efforts, as mentioned above, should focus on the effectiveness of the vaccine. For patients who do perceive a need, education should emphasize the dangers of exacerbating their condition without vaccination, specifically highlighting the risks of influenza and pneumonia—even in relatively stable patients.
The study’s strengths lie in its focus on AECOPD patients in China, an underexplored population, its application of the 3C model to assess vaccine hesitancy, and its robust statistical analyses. These elements collectively provide comprehensive insights into the vaccination barriers faced by AECOPD patients in China.This study also has several limitations. First, vaccination status was based on self-reported data rather than medical records, which is susceptible to recall bias and may have led to misclassification, though previous studies show self-reported data are generally reliable.49 Future research would benefit from verifying vaccination history through linkage with electronic medical records or regional immunization registries to enhance data accuracy. Second, the study was conducted from September 2022 to October 2023, during China’s COVID-19 recovery period, which may have increased health awareness and vaccination prevalence among AECOPD patients, introducing potential health awareness or temporal bias. Additionally, seasonal variations could have affected patient outcomes and vaccination campaigns. The study also lacked analysis of regional factors and geographical influences on vaccination prevalence and outcomes. Selection bias may have been introduced as participating hospitals were not randomly selected. Some confidence intervals (CIs) were wide, suggesting a small sample size and insufficient statistical power. While this study employed robust statistical methods, the sample size may have limited the statistical power for more nuanced subgroup analyses. Therefore, the findings from these subgroup analyses should be interpreted with caution and warrant validation in larger, future studies. The GOLD staging primarily reflects lung function impairment, not patient symptoms or quality of life, while mMRC and CAT scores are more directly related to symptoms and quality of life, making their impact on vaccination willingness more significant. While the study provides valuable insights into vaccination barriers among AECOPD patients in China, it would benefit from a more detailed analysis of regional, socioeconomic, and healthcare access disparities that may influence vaccination uptake. Addressing these limitations is crucial for future research.
Conclusion
In conclusion, this study identifies distinct patient profiles influencing vaccine uptake among AECOPD patients in China. Key facilitators included being a former smoker, maintaining regular inhaled medication, and having bronchiectasis. Conversely, significant barriers emerged among patients with higher symptom burden (elevated CAT/mMRC scores) or pulmonary infections, where convenience barriers like geographical inaccessibility predominated. The 3C model revealed vaccine hesitancy was primarily driven by complacency (78% cited “lack of perceived need”), compounded by confidence concerns and structural convenience barriers.
This study provides novel insights by integrating clinical profiles with the 3C model of hesitancy, offering a new framework for targeted interventions in this population. These findings advocate for tailored interventions: combating complacency through education in less symptomatic patients, addressing physical and logistical barriers in severe cases, and systematically building trust and access across all groups to improve vaccination coverage in this vulnerable population.
Acknowledgments
This paper is available as a preprint on ResearchGate and Researchsquare at: https://assets-eu.researchsquare.com/files/rs-6437931/v1_covered_496d421d-1fc1-4af9-ae97-8da8bfdbf760.pdf?c=1747411074 and https://www.researchsquare.com/article/rs-6437931/v1.
Funding
This study was supported by a grant from the CAMS Innovation Fund for Medical Sciences (No. 2021-I2M-1-049) and National Science and Technology Major Project (No. 2023ZD0506402).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liang Y, Sun Y. Awareness of and attitude toward COVID-19 vaccination among individuals with COPD and the strategies to overcome vaccine hesitation: a mini review. Hum Vaccin Immunother. 2023;19(3):2286686. doi:10.1080/21645515.2023.2286686
2. Confalonieri M, Braga L, Salton F, et al. Chronic obstructive pulmonary disease definition: is it time to incorporate the concept of failure of lung regeneration? Am J Respir Crit Care Med. 2023;207(3):366–367. doi:10.1164/rccm.202208-1508LE
3. Celli B, Fabbri L, Criner G, et al. Definition and nomenclature of chronic obstructive pulmonary disease: time for its revision. Am J Respir Crit Care Med. 2022;206(11):1317–1325. doi:10.1164/rccm.202204-0671PP
4. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
5. McLean S, Hoogendoorn M, Hoogenveen RT, et al. Projecting the COPD population and costs in England and Scotland: 2011 to 2030. Sci Rep. 2016;6(1):31893. doi:10.1038/srep31893
6. Harper SA, Fukuda K, Uyeki TM, et al. Prevention and control of influenza: recommendations of the advisory committee on immunization practices (ACIP). MMWR Recomm Rep. 2004;53(Rr–6):1–40.
7. Fang L, Gao P, Bao H, et al. Chronic obstructive pulmonary disease in China: a nationwide prevalence study. Lancet Respir Med. 2018;6(6):421–430. doi:10.1016/S2213-2600(18)30103-6
8. Simon S, Joean O, Welte T, et al. The role of vaccination in COPD: influenza, SARS-CoV-2, pneumococcus, pertussis, RSV and varicella zoster virus. Eur Respir Rev. 2023;32(169):230034. doi:10.1183/16000617.0034-2023
9. Sethi S, Evans N, Grant BJB, et al. New strains of bacteria and exacerbations of chronic obstructive pulmonary disease. N Engl J Med. 2002;347(7):465–471. doi:10.1056/NEJMoa012561
10. Hurst JR, Han MK, Singh B, et al. Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: a systematic literature review. Respir Res. 2022;23(1):213. doi:10.1186/s12931-022-02123-5
11. Aka Aktürk Ü, Görek Dilektaşlı A, Şengül A, et al. Influenza and pneumonia vaccination rates and factors affecting vaccination among patients with chronic obstructive pulmonary disease. Balkan Med J. 2017;34(3):206–211. doi:10.4274/balkanmedj.2016.1028
12. Wedzicha JA, Singh R, Mackay AJ. Acute COPD exacerbations. Clin Chest Med. 2014;35(1):157–163. doi:10.1016/j.ccm.2013.11.001
13. Shea KM, Edelsberg J, Weycker D, et al. Rates of pneumococcal disease in adults with chronic medical conditions. Open Forum Infect Dis. 2014;1(1):ofu024. doi:10.1093/ofid/ofu024
14. Waterer G. Vaccination in patients with COPD: COVID has raised the bar. Respirology. 2022;27(10):799–800. doi:10.1111/resp.14331
15. Hu R-Y, Liu Y, Zhang -X-X, et al. Adult immunization services in urban and rural areas of nine Chinese provinces, 2019–2021. Chinese J Prev Med. 2023;57(12):2050–2055. doi:10.3760/cma.j.cn112150-20230615-00468
16. Stoilkova A, Janssen DJ, Wouters EF. Educational programmes in COPD management interventions: a systematic review. Respir Med. 2013;107(11):1637–1650. doi:10.1016/j.rmed.2013.08.006
17. Nuorti JP, Butler JC, Farley MM, et al. Cigarette smoking and invasive pneumococcal disease. Active bacterial core surveillance team. N Engl J Med. 2000;342(10):681–689. doi:10.1056/NEJM200003093421002
18. Hedlund J, Christenson B, Lundbergh P, et al. Effects of a large-scale intervention with influenza and 23-valent pneumococcal vaccines in elderly people: a 1-year follow-up. Vaccine. 2003;21(25–26):3906–3911. doi:10.1016/S0264-410X(03)00296-2
19. Liu C, Song Q, Lin L, et al. Impact of intensive health education on influenza vaccination and acute exacerbations in outpatients with chronic obstructive pulmonary disease: a real-world study. J Glob Health. 2025;15:04047. doi:10.7189/jogh.15.04047
20. Ignatova GL, Avdeev SN, Antonov VN. Comparative effectiveness of pneumococcal vaccination with PPV23 and PCV13 in COPD patients over a 5-year follow-up cohort study. Sci Rep. 2021;11(1):15948. doi:10.1038/s41598-021-95129-w
21. Chinese Thoracic Physician Association. C.O.P.D.W.C. Chinese guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease (2021 revision). 2021. Available from: https://www.scdc.sh.cn/shjk/shjk/upload/202402/0201_084334_187.pdf.
22. Fekete M, Pako J, Nemeth AN, et al. Prevalence of influenza and pneumococcal vaccination in chronic obstructive pulmonary disease patients in association with the occurrence of acute exacerbations. J Thorac Dis. 2020;12(8):4233–4242. doi:10.21037/jtd-20-814
23. He R, Ren X, Huang K, et al. Influenza and pneumococcal vaccination coverage and associated factors in patients hospitalized with acute exacerbations of COPD in China: findings from real-world data. Chin Med J. 2024;137(10):1179–1189. doi:10.1097/CM9.0000000000002790
24. Nuwarda RF, Ramzan I, Weekes L, et al. Vaccine hesitancy: contemporary issues and historical background. Vaccines. 2022;10(10):1595.
25. Moffett AT, Halpern SD, Weissman GE. The effect of a post-bronchodilator FEV(1)/FVC < 0.7 on COPD diagnosis and treatment: a regression discontinuity design. medRxiv. 2024.
26. Claxton S, Porter P, Brisbane J, et al. Identifying acute exacerbations of chronic obstructive pulmonary disease using patient-reported symptoms and cough feature analysis. NPJ Digit Med. 2021;4(1):107. doi:10.1038/s41746-021-00472-x
27. Chen J, Yang Z, Yuan Q, et al. Prediction of gold stage in patients hospitalized with COPD exacerbations using blood neutrophils and demographic parameters as risk factors. BMC Pulm Med. 2021;21(1):329. doi:10.1186/s12890-021-01696-z
28. Ertan Yazar E, Niksarlioglu EY, Yigitbas B, et al. How to utilize CAT and mMRC scores to assess symptom status of patients with COPD in clinical practice? Medeni Med J. 2022;37(2):173–179. doi:10.4274/MMJ.galenos.2022.06787
29. Stridsman C, Svensson M, Johansson Strandkvist V, et al. The COPD Assessment Test (CAT) can screen for fatigue among patients with COPD. Ther Adv Respir Dis. 2018;12:1753466618787380. doi:10.1177/1753466618787380
30. Hair JF, Hult GT, Ringle CM, et al. An Introduction to Structural Equation Modeling, in Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R: A Workbook, J.F. Hair Jr, et al, Editors. Cham: Springer International Publishing; 2021:1–29.
31. Resche-Rigon M, White IR. Multiple imputation by chained equations for systematically and sporadically missing multilevel data. Stat Methods Med Res. 2018;27(6):1634–1649. doi:10.1177/0962280216666564
32. Jouleh B, Erdal M, Eagan TM, et al. Guideline adherence in hospital recruited and population based COPD patients. BMC Pulm Med. 2018;18(1):195. doi:10.1186/s12890-018-0756-8
33. Mulpuru S, Li L, Ye L, et al. Effectiveness of influenza vaccination on hospitalizations and risk factors for severe outcomes in hospitalized patients with COPD. Chest. 2019;155(1):69–78. doi:10.1016/j.chest.2018.10.044
34. Li X, Wu Z, Xue M, et al. An observational study of the effects of smoking cessation earlier on the clinical characteristics and course of acute exacerbations of chronic obstructive pulmonary disease. BMC Pulm Med. 2022;22(1):390. doi:10.1186/s12890-022-02187-5
35. Nomura Y, Sawahata M, Nakamura Y, et al. Age and smoking predict antibody titres at 3 months after the second dose of the BNT162b2 COVID-19 vaccine. Vaccines. 2021;9(9):1042.
36. Verbiest M, Brakema E, van der Kleij R, et al. National guidelines for smoking cessation in primary care: a literature review and evidence analysis. Npj Primary Care Resp Med. 2017;27(1):2. doi:10.1038/s41533-016-0004-8
37. Duarte-de-araújo A, Teixeira P, Hespanhol V, et al. COPD: understanding patients’ adherence to inhaled medications. Int J Chron Obstruct Pulmon Dis. 2018;13:2767–2773. doi:10.2147/COPD.S160982
38. Guan H, Zhang L, Chen X, et al. Enhancing vaccination uptake through community engagement: evidence from China. Sci Rep. 2024;14(1):10845. doi:10.1038/s41598-024-61583-5
39. Chandra S, Mohammadnezhad M, Ward P. Trust and communication in a doctor- patient relationship: a literature review. J Healthcare Commun. 2018;03.
40. Schwalbe N, Hanbali L, Nunes MC, et al. Use of financial incentives to increase adult vaccination coverage: a narrative review of lessons learned from COVID-19 and other adult vaccination efforts. Vaccine. 2022;12:100225. doi:10.1016/j.jvacx.2022.100225
41. Stoilkova-Hartmann A, Franssen FME, Augustin IML, et al. COPD patient education and support – achieving patient-centredness. Patient Educ Couns. 2018;101(11):2031–2036. doi:10.1016/j.pec.2018.05.024
42. Usmani ZA, Heslop CK, Esterman K, De Soyza AJ, Smith BJ, Smith BJ. Psychological therapies for the treatment of anxiety disorders in chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;3(Issue 3):CD010673. doi:10.1002/14651858.CD010673.pub2
43. Geoghegan S, O’Callaghan KP, Offit PA. Vaccine safety: myths and misinformation. Front Microbiol. 2020;11:372. doi:10.3389/fmicb.2020.00372
44. Viniol C, Vogelmeier CF. Exacerbations of COPD. Eur Respir Rev. 2018;27(147):170103. doi:10.1183/16000617.0103-2017
45. Avelino-Silva VI, Ferreira-Silva SN, Soares MEM, et al. Say it right: measuring the impact of different communication strategies on the decision to get vaccinated. BMC Public Health. 2023;23(1):1162. doi:10.1186/s12889-023-16047-2
46. Gibson E, Zameer M, Alban R, et al. Community health workers as vaccinators: a rapid review of the global landscape, 2000-2021. Glob Health Sci Pract. 2023;11(1):e2200307. doi:10.9745/GHSP-D-22-00307
47. Li Q, Peng JC, Mohan D, et al. Using location intelligence to evaluate the COVID-19 vaccination campaign in the United States: spatiotemporal big data analysis. JMIR Public Health Surveillance. 2023;9.
48. Bauer C, Zhang K, Lee M, et al. Real-time geospatial analysis identifies gaps in COVID-19 vaccination in a minority population. Sci Rep. 2021;11(1):18117. doi:10.1038/s41598-021-97416-y
49. Zimmerman RK, Raymund M, Janosky JE, et al. Sensitivity and specificity of patient self-report of influenza and pneumococcal polysaccharide vaccinations among elderly outpatients in diverse patient care strata. Vaccine. 2003;21(13–14):1486–1491. doi:10.1016/S0264-410X(02)00700-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.