Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Factors Associated with HIV Testing Uptake in Cameroon: Data from the 2018 Cameroon Demographic and Health Survey
Authors Buh Nkum C ![]() , Nanfak A
, Nanfak A ![]() , Guenou E
, Guenou E ![]() , Fri Kami R, Murhabazi Bashombwa A
, Fri Kami R, Murhabazi Bashombwa A ![]() , Tchio-Nighie KH, Nangue C, Ateudjieu J
, Tchio-Nighie KH, Nangue C, Ateudjieu J
Received 16 September 2024
Accepted for publication 15 January 2025
Published 22 January 2025 Volume 2025:17 Pages 9—17
DOI https://doi.org/10.2147/HIV.S496572
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Collins Buh Nkum,1 Aude Nanfak,1 Etienne Guenou,1– 3 Rosine Fri Kami,1 Augustin Murhabazi Bashombwa,1,2,4 Ketina Hirma Tchio-Nighie,1,2 Charlette Nangue,1 Jerome Ateudjieu1,2,5
1Department of Health Research, M.A. SANTE (Meilleur Accès Aux Soins de Santé), Yaounde, Cameroon; 2Department of Public Health, Faculty of Medicine and Pharmaceutical Sciences, University of Dschang, Dschang, Cameroon; 3National Public Health Laboratory, Ministry of Public Health, Yaounde, Cameroon; 4Faculty of Medicine, University of Kaziba, Kaziba, Democratic Republic of the Congo; 5Division of Health Operations Research, Ministry of Public Health, Yaounde, Cameroon
Correspondence: Augustin Murhabazi Bashombwa, Email [email protected]
Background: HIV represents a significant public health challenge, contributing to increased mortality and morbidity within the population. Despite the implementation of various HIV testing strategies, the uptake rate of HIV testing remains low.
Objective: This study aims to assess the factors associated with HIV testing uptake among women and men in Cameroon.
Methods: A secondary analysis of the 2018 Cameroon demographic and health survey (DHS) was conducted using data of sexually active men and women aged 15– 64. Multivariate logistic regression was employed to identify the key factors associated with HIV testing in Cameroon.
Results: We included a total of 18,112 participants (12563 women and 5549 men). The study found that 47.8% (95% CI 46.9– 48.7) of women and 45% (95% CI 43.7– 46.3) of men were tested for HIV in the past 12 months. Among women and men, age above 20– 24 years (AOR= 1.3, p< 0.01 vs AOR= 2.3, p< 0.001), a high level of education (AOR= 2.1, p< 0.001 vs AOR= 2.3, p< 0.001) and high wealth (AOR= 1.9, p< 0.001 AOR= 2.0, p< 0.001) were positively associated with HIV testing uptake. Conversely, residing in the northern regions (AOR= 0.5, p< 0.001 vs AOR= 0.4, p< 0.001), was negatively associated. Among men, no independent significant association was found between HIV testing uptake and never being married.
Conclusion: This study, utilizing data from the Cameroon DHS, provides valuable insights into HIV testing in Cameroon. To achieve UNAIDS targets of “zero new infections and zero deaths” by 2030, interventions must prioritize less educated individuals, younger age groups and low income earners. The findings from this research can inform recommendations for decision-makers and contribute to the development of effective public health interventions to combat HIV in Cameroon.
Keywords: HIV, testing, factors, Cameroon
Introduction
The Human Immunodeficiency Virus (HIV), which causes AIDS (Acquired Immuno Deficiency Syndrome) remains one of the most significant public health challenges worldwide. To date, 85.6 million individuals have contracted HIV, resulting in 40.4 million deaths recorded.1 Recent data from the World Health Organization (WHO) in 2022 indicated that in Africa, an estimated 25.6 million people were living with HIV, with 660,000 new cases and 380,000 deaths attributed to HIV-related causes within the year.2 According to the 2020 Cameroon spectrum, there were about 506,432 PLHIV in 2019 and 14,058 HIV-related deaths recorded in Cameroon.3 The prevalence of HIV in Cameroon, as per the 2018 Demographic and Health Survey, stands at 2.7%, with six out of ten regions reporting a prevalence higher than the national average.3
While there is no cure for HIV, preventive measures, early diagnosis, and treatment play crucial roles in reducing its impact. UNAIDS has established a global strategy aiming to ensure that, by 2025, 95% of all individuals are aware of their HIV status, 95% of people living with HIV/AIDS (PLHIV) are receiving life-saving antiretroviral treatment (ART), and 95% of those on treatment have achieved viral suppression.4 In Cameroon, only 46.9% of people living with PLHIV aware of their status, 91.3% of them were on ART and 80.0% of those on ART had viral suppression in 2018.5 This highlights the extra efforts needed to reach the UNAIDS target. A national strategic plan (NSP) 2021–2023 was implemented, outlining objectives to mitigate the HIV burden in the country.3 However, data indicates that key targets, including reducing new HIV infections by 65% and HIV-related deaths by 62%, were achieved at rates of only 31.6% and 23.9%, respectively, with the impact on the quality of life not being assessed.6 There are significant challenges posed by HIV prevalence and the ambitious policy targets set to combat this epidemic, it becomes essential to assess the multifaceted factors that influence HIV testing uptake. Thus, it is imperative to understand the determinants of HIV testing in Cameroon to inform targeted interventions that align with the goal of improving HIV status awareness coverage in the country.
Numerous studies have identified various factors associated with HIV testing. Research in sub-Saharan African countries has linked individual demographic characteristics (such as gender, age, and marital status), socio-economic status (including education and wealth), cultural practices (such as religion and circumcision), and sexual behavior risk factors to HIV testing.7–9 However, in Cameroon, a study revealed factors associated with the risk of HIV infection among specific targets like women, but the determinants of this infection at the national level targeting the general population are not known.10 Therefore, this study aims to identify the socio-demographic, economic, and regional factors influencing HIV testing among adults in Cameroon. The findings from this study have the potential to inform public health interventions and HIV control programs in Cameroon, guiding efforts to eliminate the HIV burden in the country.
Materials and Methods
Study Design and Setting
The data utilized in this study were obtained from the Demographic and Health Survey (DHS) conducted in Cameroon in 2018. The survey was carried out by the National Institute of Statistics (NIS) in collaboration with the Ministry of Public Health. The survey aimed to gather information on the awareness and attitudes of both men and women regarding sexually transmitted infections (STIs) and acquired immunodeficiency syndrome (AIDS). Blood samples were collected anonymously for HIV screening to estimate HIV prevalence in the adult population. Data on household and individual characteristics were collected through face-to-face interviews using four pre-tested questionnaires: the household questionnaire, individual women’s questionnaire, individual men’s questionnaire, and the biomarkers questionnaire.11
Sampling and Sample Size Estimation
The sampling methodology involved individuals selected through a stratified, two-stage random sampling process. Initially, 470 clusters were systematically selected with a probability proportional to cluster size. Subsequently, a sample of 28 households per cluster was systematically chosen with equal probability. At the national level, the sample size comprised 13,160 households, with 6,860 households in 245 urban clusters and 6,300 households in 225 rural clusters. Adjustments were made for missing responses, leading to an estimated population size of 12,563 women and 5,549 men (Figure 1). The study population distribution was designed to ensure adequate representation of urban and rural areas, as well as the 12 study areas encompassing the 10 regions, Douala, and Yaoundé.
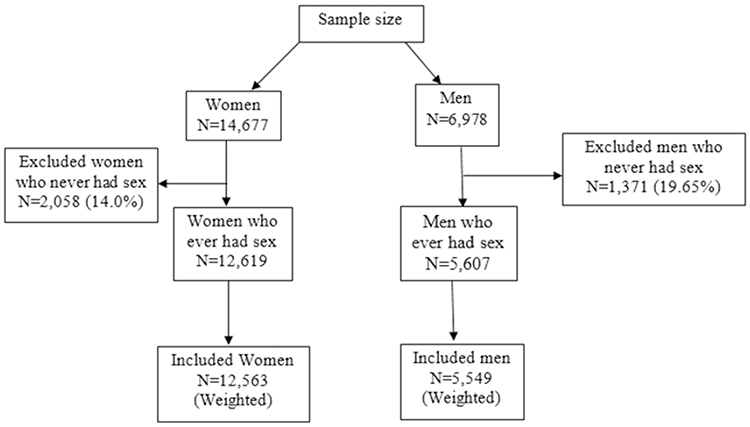 |
Figure 1 Study population flow diagram. |
Study Population
The secondary data analyzed in this study included men and women aged 15–64, excluding participants who had never engaged in sexual activity.
Variable of Interest
Dependent Variable
The primary variable of interest, used to evaluate access to HIV testing, was “Have you been tested for HIV in the last 12 months” This question was considered for sexually active individuals aged between 15 and 64.
Independent Variables
The socio-demographic and economic variables included: age (15–19, 20–24, 25 and above); region of residence, the 12 study areas selected in the DHS were grouped into two geographical regions: Northern Regions (Adamawa, North, Far North) and Southern region (Centre, South, Littoral, East, West, South-West, North-West, Douala, Yaoundé); level of education was grouped into two: Low level (no education, primary) and high level (secondary, higher); Never married (Yes/No), Wealth index,12 was grouped into two: low wealth (poorest, poorer) and high wealth (middle, richer, richest) and occupation was grouped into two: Not working and working (professional/technical/managerial, clerical, sales, agricultural, self-employed, services, skilled manual, and unskilled manual).
The dichotomous variables concerning knowledge of HIV were: knowledge of a place to go for an HIV test; knowledge of mother-to-child transmission of HIV; knowledge of taking medication to prevent transmission of HIV to the baby during pregnancy; knowledge of HIV and sexually transmitted infections.
Statistical Analysis
Statistical analysis was conducted in two stages using STATA version 17 software: a descriptive analysis of the sample based on study variables, and explanatory analysis to identify factors associated with HIV testing. The descriptive analysis involved presenting the variables in terms of numbers and percentages. Following the individual presentation of the variables, a comparison table was prepared between the dependent and the independent variables, and intergroup comparisons were made using the Chi2 test. The significance level was at 5% and confidence intervals (CI) at 95%.
To identify factors associated with HIV testing, adjusted logistic regression analyses were performed for women and men, and adjusted odds ratios (AORs) were calculated with their 95% confidence intervals. Independent variables that failed to reach significance at the 5% level in the bivariate regression analysis were excluded from the multivariate model. Data were weighted to account for the sampling.
Ethical Consideration
The study utilized secondary data from the Cameroon Demographic and Health Survey. The survey protocol was reviewed and approved by the Cameroon National Committee on Research Ethics for Human Health (CNERSH) and the ICF Institutional Review Board. Written informed consent was obtained from all participants and from the parent/guardian for participants under 18 years of age. Permission to access the Cameroon DHS 2018 survey dataset was granted by the DHS program at https://dhsprogram.com/Data/terms-of-use.cfm. All DHS data were treated as confidential, and no effort should was made to identify any household or individual respondent interviewed in the survey.
Results
Background Characteristics of the Study Population
Table 1 provides an overview of the socio-demographic characteristics of sexually active women and men aged 15–64 in the study. A total of 18,112 participants were included, consisting of 12,563 women and 5,549 men. The majority of both women and men were aged above 25, with percentages of 70.8% and 75.9% respectively. More participants, both women (68.6%) and men (73.4%), resided in the Southern regions. A higher proportion of women had a low education level (92.4% vs 87.5% for men). Household wealth distribution varied between men and women, with 31.4% of men having low wealth compared to 36.2% of women.
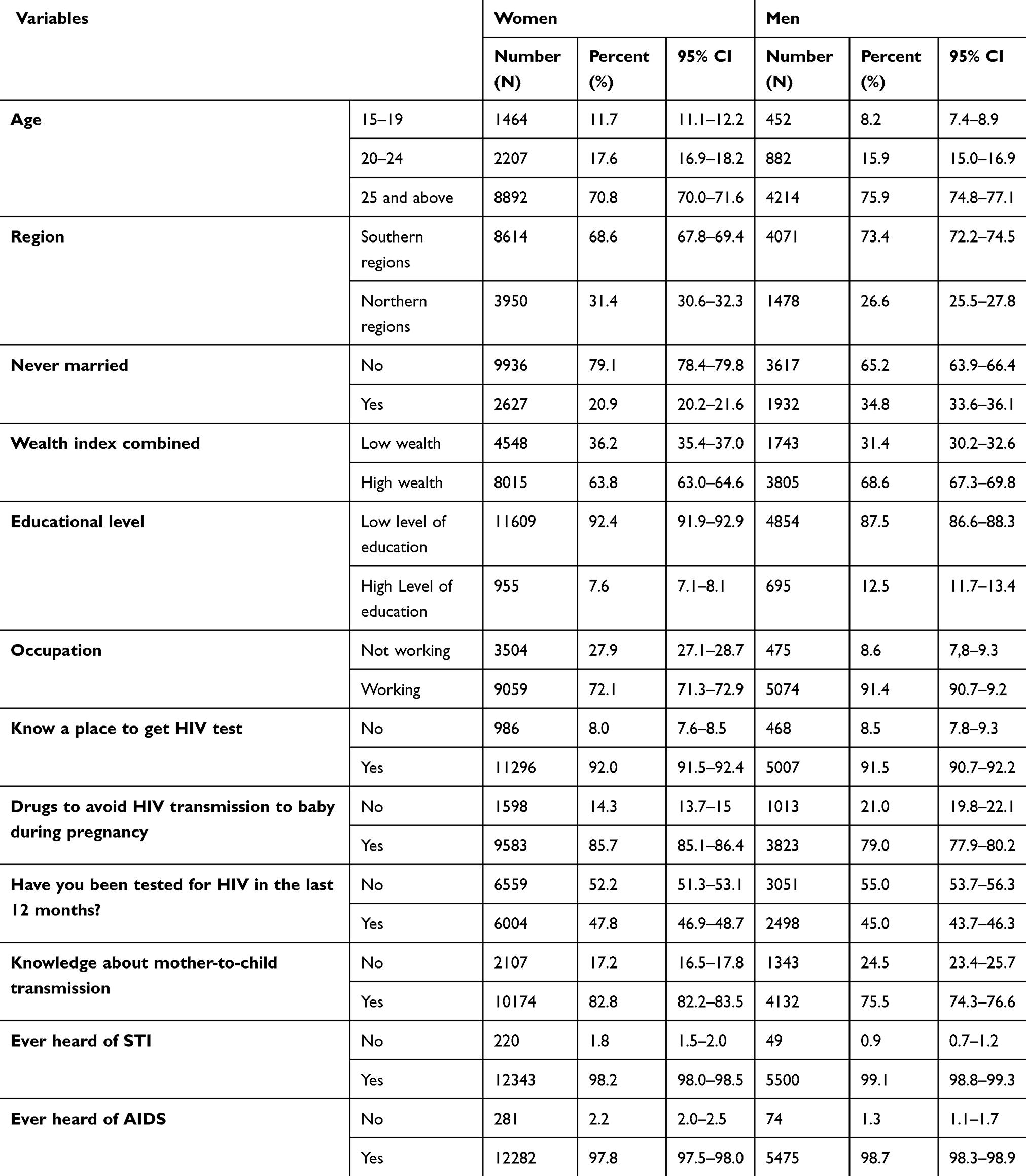 |
Table 1 Socio-Demographic Characteristics of the Study Population |
Women had a better knowledge of place to get HIV test compared to men (92%; vs 91.5%). Awareness of mother-to-child transmission of HIV was higher among women than men (82.8% vs 75.5%). The HIV testing rate in the 12 months before the survey was higher for women than men, at 47.8% versus 45%.
Association Between HIV Testing Uptake and Socio-Demographic, Economic Factors and Knowledge of HIV Among Women and Men
Table 2 presents factors associated with uptake of HIV testing among men and women. Regarding socio-demographic and economic factors, for both genders, HIV testing was significantly associated to age, region, never married, wealth index combined, and educational level and occupation. Factors related to knowledge of HIV were found to significantly influence HIV testing.
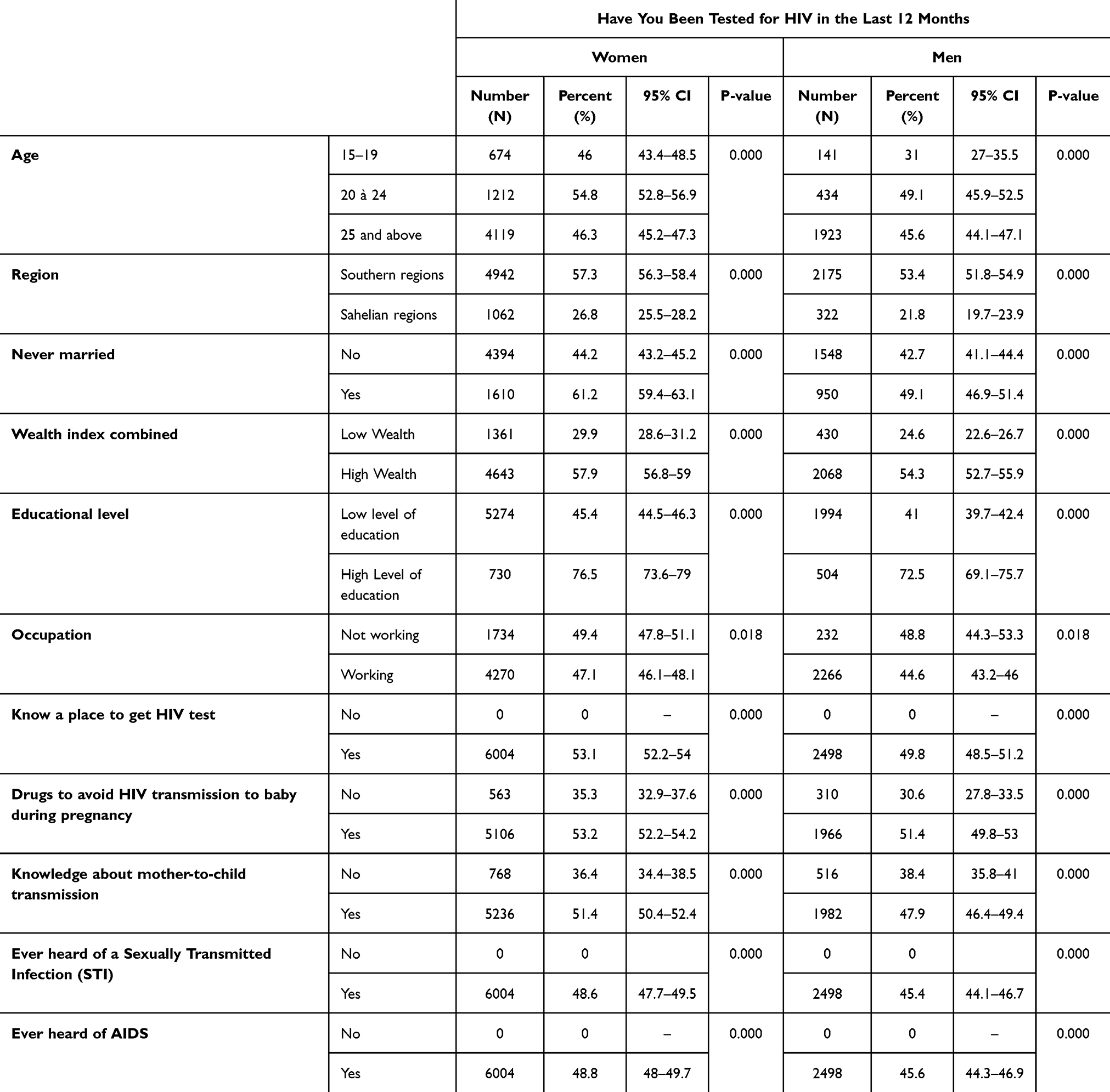 |
Table 2 Association Between HIV Testing Uptake and Socio-Demographic, Economic Factors and Knowledge of HIV Among Women and Men |
Factors Associated With HIV Testing
In multi-variable logistic regression for women and men the following variables were significantly associated with being tested for HIV in the last 12 months: age 20–24, residing in the Northern region, high wealth, high level of education and knowledge of drugs to avoid HIV transmission to baby during pregnancy (Table 3).
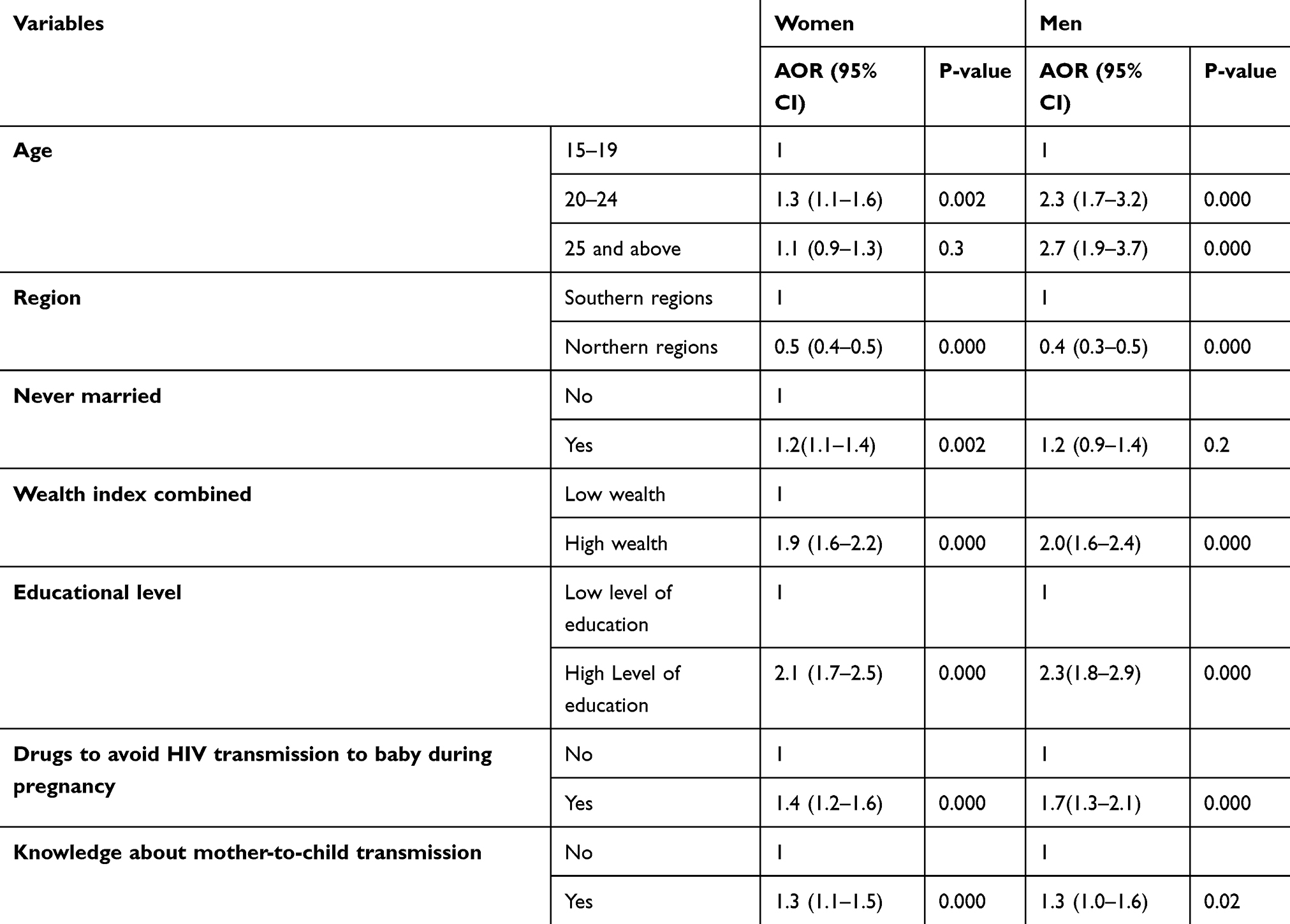 |
Table 3 Multivariable Logistic Model for Correlates of HIV Testing in Cameroon |
Discussion
The aim of this study was to assess the factors associated with HIV testing uptake in Cameroon. Despite the various interventions implemented by health actors in Sub –Saharan Africa (SSA), the rate of HIV testing is still low.13 Our findings indicate that HIV testing rate among women(47.8%) was higher compared to men(45%), which is consistent with the results of other studies.8,14–16 This difference may be attributed to women’s exposure to various HIV prevention programs such as ANC and maternal health services. To enhance the efficiency of HIV testing initiatives, it is essential to include men in these existing programs. Making HIV testing a routine component of ANC process for both women and their partner can create a more inclusive environment, encouraging men’s participation in ANC and maternal health services, and ultimately leading to increased HIV testing and better health outcomes for families.
Age is a significant factor influencing the uptake of HIV testing. Our study revealed that both men and women, in the age groups above 19, were more likely to undergo HIV testing compared to their younger counterparts. Older adults may be more likely to have multiple partnerships than younger individuals and as such more likely to consider themselves in need of an HIV test on an annual basis. Our findings are consistent with other studies that report higher odds of testing among older adults compared to younger age groups.17–20 It is crucial for health policymakers to review current HIV prevention policies to enhance HIV testing among young people.7
Additionally, individuals residing in the southern regions were more likely to be tested compared to those residing in the northern regions of Cameroon. Yaounde and Douala being respectively the administrative and economic capitals of Cameroon, host numerous reference hospitals equipped with adequate infrastructure and trained health personnel specializing in HIV prevention and treatment. This situation significantly contributes to the increased uptake of HIV testing in these regions.
Moreover, individuals from wealthier backgrounds had higher odds of being tested compared to the poorest section. Access to HIV intervention programs remains a challenge for economically disadvantaged populations. Furthermore, individuals with higher education levels were more likely to undergo HIV testing, which is consistent with findings in other studies across different settings.9,14,15,20,21 This trend may be attributed to the perception of wealthier, educated individuals considering themselves more at risk and therefore seeking testing more actively compared to the less affluent individuals.9 This observation also underscores the important role of education in raising awareness within communities.22
Knowing where to obtain an HIV test is a significant indicator of whether an individual will seek testing. The awareness of testing locations reduces barriers to access and increases the likelihood of testing. In our study, we found that the knowledge of the place to get tested was significantly associated to HIV testing. Other studies indicate that people who are aware of HIV testing sites are significantly more likely to have been tested for HIV.19 Public health campaigns that increase awareness of testing locations have been shown to increase testing rates.23 Access to HIV testing services plays a pivotal role in determining an individual’s likelihood of being tested for HIV.
Our findings also indicated that knowledge of mother-to-child transmission (MTCT) was significantly associated with HIV testing uptake among women. This finding aligns with existing literature indicating that women who possess knowledge regarding MTCT are more likely to undergo HIV testing during antenatal care visits.24 Also, Understanding the mechanisms behind MTCT of HIV can encourage women to undergo testing during pregnancy.
Our study revealed a significant association between HIV testing and drugs to avoid HIV transmission to baby during pregnancy. Consistently with previous reports from other studies, pregnant women who are aware of PMTCT drugs are more likely to seek HIV testing.25 This can be attributed to the fact that educational interventions targeting pregnant women have proven to be efficacious in increasing testing rates.26 Furthermore, having Knowledge regarding the effectiveness of these interventions serve as a motivating factor for pregnant women to undergo HIV testing.
This study faced limitations due to a lack of specific data on certain population groups, such as sex workers and individuals who use drugs. Socio-cultural norms and constraints may have influenced participants’ responses, particularly in regions where discussing HIV is stigmatized. The accuracy of responses may vary based on the particular setting, underscoring the necessity for tailored strategies to improve HIV testing rates across diverse populations.
Conclusion
HIV testing uptake rate in Cameroon is still low despite the introduction of testing strategies. This study examines the factors associated with HIV testing among women and men in Cameroon using data from the 2018 Cameroon Demographic and Health Survey. Key significant factors associated with HIV testing include age, wealth, education level, and geographic region.
To reach the UNAIDS targets “Zero new infections. Zero deaths” by the end of 2030, the effectiveness of HIV testing uptake should be followed by evaluations, in order to assess their weaknesses. This finding will, therefore, provide relevant data that will contribute to formulating some recommendations by decision-makers. It would be beneficial to emphasize on community activities such as awareness-raising in households and public places, and promoting more education in schools in order to reach all the age groups and begin early to demystify the disease, reduce stigma, and promote safe practices. Furthermore, due to the low uptake rate of HIV testing among men, health programs such ANC and other maternal health services will be more beneficial if men are included.
Acknowledgments
We thank the DHS Program, for grant us permission to the 2018 Cameroon Survey database.
Disclosure
The authors report no conflict of interest in this work.
References
1. Global HIV & AIDS statistics — Fact sheet 2023 - World | ReliefWeb. Jul 23, 2023. Available from: https://reliefweb.int/report/world/global-hiv-aids-statistics-fact-sheet-2023.
2. HIV data and statistics WHO. Available from: https://www.who.int/teams/global-hiv-hepatitis-and-stis-programmes/hiv/strategic-information/hiv-data-and-statistics.
3. Cameroon-national-strategic-plan-for-fight-against-hivaids-and-stis-2021-2023.pdf. Available from: https://hivpreventioncoalition.unaids.org/sites/default/files/attachments/cameroon-national-strategic-plan-for-fight-against-hivaids-and-stis-2021-2023.pdf.
4. HIV and AIDS. [
5. Dzudie A, Tchounga B, Ajeh R, et al. Research priorities for accelerating the achievement of three 95 hIV goals in Cameroon: a consensus statement from the Cameroon HIV Research Forum (CAM-HERO). Pan Afr Med J. 2021:40. doi:10.11604/pamj.2021.40.124.31068.
6. Cameroon national strategic plan for the fight against HIV/AIDS and STI 2024-2030. Available from: https://cnls.cm/site/sites/default/files/2024-02/PSN%20VIH%20IST%20_%202024-2030%20Version%20finale%2021.02.24.pdf.
7. Meka AFZ, Billong SC, Diallo I, Tiemtore OW, Bongwong B, Nguefack-Tsague G. Challenges and barriers to HIV service uptake and delivery along the HIV care cascade in Cameroon. Pan Afr Med J. 2020;36:37. doi:10.11604/pamj.2020.36.37.19046
8. Lakhe NA, Diallo Mbaye K, Sylla K, Ndour CT. HIV screening in men and women in senegal: coverage and associated factors; analysis of the 2017 demographic and health survey. BMC Infect Dis. 2019;20(1):1. doi:10.1186/s12879-019-4717-5
9. Jean K, Anglaret X, Moh R, Lert F, Dray-Spira R. Barriers to HIV testing in côte d’ivoire: the role of individual characteristics and testing modalities. PLoS One. 2012;7(7):e41353. doi:10.1371/journal.pone.0041353
10. Spatial analysis of factors associated with subnational HIV prevalence among female adults aged 15-49 years in Cameroon, 2004-2018. Oct 5, 2022. [
11. National Institute of Statistics (Cameroon). and ICF. cameroon DHS summary report. Rockville: NIS and ICF; 2018. Available from: https://dhsprogram.com/pubs/pdf/SR266/SR266.pdf.
12. Howe LD, Galobardes B, Matijasevich A, et al. Measuring socio-economic position for epidemiological studies in low- and middle-income countries: a methods of measurement in epidemiology paper. Int J Epidemiol. 2012;41(3):871–886. doi:10.1093/ije/dys037
13. World Health Organization. HIV and adolescents: guidance for HIV testing and counselling and care for adolescents living with HIV: recommendations for a public health approach and considerations for policy-makers and managers. Geneva: World Health Organization; 2013. Available from: https://iris.who.int/handle/10665/94334.
14. Staveteig S, Croft TN, Kampa KT, Head SK. Reaching the ‘first 90’: gaps in coverage of HIV testing among people living with HIV in 16 African countries. PLoS One. 2017;12(10):e0186316. doi:10.1371/journal.pone.0186316
15. Takarinda KC, Madyira LK, Mhangara M, et al. Factors associated with ever being HIV-tested in Zimbabwe: an extended analysis of the Zimbabwe Demographic and Health Survey (2010–2011). PLoS One. 2016;11(1):e0147828. doi:10.1371/journal.pone.0147828
16. Neilan AM, Dunville R, Ocfemia MCB, et al. The optimal age for screening adolescents and young adults without identified risk factors for HIV. J Adolesc Health. 2018;62(1):22–28. doi:10.1016/j.jadohealth.2017.08.028
17. Musheke M, Ntalasha H, Gari S, et al. A systematic review of qualitative findings on factors enabling and deterring uptake of HIV testing in Sub-Saharan Africa. BMC Public Health. 2013;13(1):220. doi:10.1186/1471-2458-13-220
18. Sanga Z, Kapanda G, Msuya S, Mwangi R. Factors influencing the uptake of voluntary HIV counseling and testing among secondary school students in Arusha City, Tanzania: a cross sectional study. BMC Public Health. 2015;15(1):452. doi:10.1186/s12889-015-1771-9
19. MacPhail C, Pettifor A, Moyo W, Rees H. Factors associated with HIV testing among sexually active South African youth aged 15–24 years. AIDS Care. 2009;21(4):456–467. doi:10.1080/09540120802282586
20. Mahande MJ, Phimemon RN, Ramadhani HO. Factors associated with changes in uptake of HIV testing among young women (aged 15–24) in Tanzania from 2003 to 2012. Infect Diseases Poverty. 2016;5(1):92. doi:10.1186/s40249-016-0180-3
21. Godif M, Assefa H, Alemayehu M, et al. Factors associated with HIV counseling and testing among males and females in Ethiopia: evidence from Ethiopian demographic and health survey data. Journal of AIDS and Clinical Research. 2015. Available from: https://www.semanticscholar.org/paper/Factors-Associated-with-HIV-Counseling-and-Testing-Godif-Assefa/268d0d7c655c8ce09d635960f1feb07baee7ecc1.
22. Buh Nkum C, Ateudjieu J, Nanfak A, et al. Long-lasting insecticidal net ownership and use in mogode health district, Cameroon. Cureus. 2024;16(4):e57819. doi:10.7759/cureus.57819
23. Sweat M, Morin S, Celentano D, et al. Community-based intervention to increase HIV testing and case detection in people aged 16–32 years in Tanzania, Zimbabwe, and Thailand (NIMH project accept, HPTN 043): a randomised study. Lancet Infect Dis. 2011;11(7):525–532. doi:10.1016/S1473-3099(11)700603
24. Medley A, Garcia-Moreno C, McGill S, Maman S. Rates, barriers and outcomes of HIV serostatus disclosure among women in developing countries: implications for prevention of mother-to-child transmission programmes. Bull World Health Organ. 2004;82(4):299–307.
25. Stringer EM, Sinkala M, Stringer JS, et al. Prevention of mother-to-child transmission of HIV in Africa: successes and challenges in scaling-up a nevirapine-based program in Lusaka, Zambia. AIDS. 2003;17(9):1377. doi:10.1097/00002030-200306130-00012
26. Mirkuzie AH, Hinderaker SG, Sisay MM, Moland KM, Mørkve O. Current status of medication adherence and infant follow up in the prevention of mother to child HIV transmission programme in Addis Ababa: a cohort study. J Int AIDS Soc. 2011;14(1):50. doi:10.1186/1758-2652-14-50
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
HIV Testing Uptake Among Ethiopian Rural Men: Evidence from 2016 Ethiopian Demography and Health Survey Data
Asresie MB, Worku GT, Bekele YA
HIV/AIDS - Research and Palliative Care 2023, 15:225-234
Published Date: 3 May 2023