Back to Journals » Clinical Ophthalmology » Volume 17
Factors Associated with Annual Vision Screening in Diabetic Adults: Analysis of the 2019 National Health Interview Survey
Authors Jotte A ![]() , Vander Kooi W
, Vander Kooi W ![]() , French DD
, French DD ![]()
Received 20 December 2022
Accepted for publication 9 February 2023
Published 18 February 2023 Volume 2023:17 Pages 613—621
DOI https://doi.org/10.2147/OPTH.S402082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alec Jotte,1 Willow Vander Kooi,2 Dustin D French1,3– 5
1Feinberg School of Medicine, Northwestern University, Chicago, IL, USA; 2Northwestern University, Evanston, IL, USA; 3Departments of Ophthalmology and Medical Social Sciences, Northwestern University, Chicago, IL, USA; 4Center for Health Services and Outcomes Research, Northwestern University, Chicago, IL, USA; 5Veterans Affairs Health Services Research and Development Service, Chicago, IL, USA
Correspondence: Dustin D French, 645 N. Michigan Ave., Suite 440, Chicago, IL, 60611, USA, Tel +1 312 503 5590, Fax +1 312 503 8152, Email [email protected]
Purpose: To determine the association(s) between receiving an annual eye exam and various economic, social, and geographic factors assessed in the 2019 National Health Interview Survey (NHIS) among adults with diabetes.
Patients and Methods: Data from adults 18 years of age and older relevant to self-reported non-gestational diabetes diagnosis and eye exam within the last 12 months were extracted from the 2019 NHIS dataset. A multivariate logistic regression model was used to determine associations between receiving an eye exam in the preceding 12 months and various economic, insurance-related, geographic, and social factors. Outcomes were reported as odds ratios (OR) with 95% confidence intervals (CI).
Results: Among diabetic adults in the US, receiving an eye exam within the last 12 months was significantly associated with female sex (OR 1.29; 95% CI 1.05– 1.58), residence in the Midwestern United States (OR 1.39; 95% CI 1.01– 1.92), use of Veteran’s Health Administration healthcare (OR 2.15; 95% CI 1.34– 3.44), having a usual place to go for healthcare (OR 3.89; 95% CI 2.16– 7.01), and the use of Private, Medicare Advantage, or other insurance (OR 3.66; 95% CI 2.42– 5.53), use of Medicare only excluding Medicare Advantage (OR 3.18; 95% CI 1.95– 5.30), dual eligibility for Medicare and Medicaid (OR 3.88; 95% CI 2.21– 6.79), and use of Medicaid and other public health insurance (OR 3.04; 95% CI 1.89– 4.88) compared to those without insurance. An educational attainment of less than high school (OR 0.66; 95% CI 0.48– 0.92), and an educational attainment of high school or GED without any college (OR 0.62; 95% CI 0.47– 0.81) reduced the odds of having an annual eye exam.
Conclusion: Economic, social, and geographic factors are associated with diabetic adults receiving an annual eye exam.
Keywords: diabetic retinopathy, insurance, high deductible health plan, veteran, social determinants of health, preventative health
Introduction
The prevalence of diabetes worldwide and in the United States is on the rise.1 In 2019, 28.7 million people in the United States—or 8.7% of the US population—had diagnosed diabetes mellitus and an additional 8.5 million people were estimated to have undiagnosed diabetes.2 Diabetic retinopathy (DR) is a common ocular complication of diabetes and the leading cause of new cases of blindness among adults aged 18–64 years in the United States.3 About one in three people living with diabetes has some degree of diabetic retinopathy and one in ten will develop a vision-threatening form of the disease with these numbers expected to increase in the coming years.1,4 Minority Americans, rural Americans, and low-income adults have higher rates of DR and are less likely to receive regular screening exams than their non-minority and wealthier counterparts.5–15
A routine annual eye exam to detect early DR and consequent treatment could prevent 90% of vision loss caused by diabetes.16,17 For this reason, the American Academy of Ophthalmology (AAO) recommends that all individuals with diagnosed diabetes receive annual dilated eye exams, and the American Diabetes Association (ADA) recommends screenings minimally once every other year if there is no sign of retinopathy and glycemia is well controlled.18,19 Yet, studies have reported that between 23% and 65% of patients with diabetes are not receiving guideline-concordant care.11,20–25 Further, the proportion of Americans with diabetes who receive an annual dilated eye exam has not changed between 2005 and 2016.22 The US Department of Health and Human Services has identified increasing the proportion of adults with diabetes who have a yearly eye exam as a national public health objective in its Healthy People 2030 Report.26
Various factors are associated with receiving guideline-concordant annual eye exam screenings including insurance coverage, higher educational attainment, older age, good glycemic control, presence of vision symptoms, participation in a cohesive diabetes control program, living in urban centers, and having a regular primary care provider.8,15,20,27–39 Those with high deductible health plans (HDHPs) are more likely to have poor management of their diabetes, attend fewer primary care appointments, and delay intervention for complications.40,41 In 2019, HDHPs were defined by the Internal Revenue Service (IRS) as insurance plans with an annual deductible of >$1350 for an individual or >$2700 for two or more persons.42
The aim of this paper is to assess various insurance-related, geographic, and social factors (also commonly referred to as social determinants of health (SDH)) of adults with self-reported non-gestational diabetes diagnoses who received an eye exam in the preceding 12 months using data collected in the 2019 National Health Interview Survey (NHIS). Currently published studies have not used a nationally representative sample to examine correlations between HDHPs and receiving guideline-concordant DR screening or used national data to evaluate geographically where the need for improved interventions is highest. We seek to describe characteristics that differentiate individuals receiving guideline-concordant screenings and those that are not based on insurance type (including HDHPs), regional geography, key measurements of the social determinants of health, and other demographic factors in this nationally representative sample. This information can be used to tailor national interventions designed to increase the proportion of adults with diabetes who receive guideline concordant diabetic retinopathy screenings.
Materials and Methods
The National Health Interview Survey (NHIS) is a large-scale household interview survey coordinated through the National Center of Health Statistics (NCHS) under the auspices of the Centers for Disease Control and Prevention (CDC) and was the primary source of information for this study. The survey has been conducted annually since 1957 and involves a statistically representative sample of the civilian non-institutionalized population of the United States. The main objective of the NHIS is to monitor the health of the US population through the collection and analysis of data on a broad range of health topics through household interviews. In 2019 the questionnaire structure was redesigned to improve the measurement of covered health topics, reduce respondent burden by shortening the length of the questionnaire, and better synergize with other federal health surveys.43 The NHIS is comprised of sample adult and sample child surveys which consist of four components: the annual core, rotating core, sponsored content (sustaining and periodic), and emerging topics. Annual core is content that is included in the NHIS every year. Rotating core is scheduled to appear on a periodic basis of every other year, one out of every three years, or two out of every three years. Sponsored content includes questions that are funded by other agencies and are included when funding is provided. Sustaining sponsors fund content every year, whereas other sponsors fund content periodically. Finally, emerging content is new content that is sponsored by NCHS on emerging topics. More information on the 2019 redesign of the NHIS can be found on the CDC website.43 Extensive documentation, questionnaires and code books are available on-line from the CDC.
All methods adhered to the tenets of the Declaration of Helsinki. The de-identified, publicly available NHIS data does not constitute human subjects research as defined at 45 CFR 46.102 and thus this study was considered exempt by the Northwestern University Institutional Review Board. The study population consisted of 31,997 adults, ages 18 and over. These interviewed adults represent an unweighted national sample. Statistical Analysis Software 9.3 (Proc Survey) have been developed that calculate the population estimate based on sample weights, strata, and cluster information.
The comprehensive 2019 NHIS survey of 31,997 adults interviewed was narrowed to the subset of 3355 adults who responded “yes” to the question “Not including (gestational diabetes, prediabetes), has a doctor or other health professional EVER told you that you had diabetes?” Those responding “yes” includes all adults within the sample who self-report type I and type II diabetes. This group of 3355 adults represents the study population. The outcome of interest was receiving an annual eye exam in the preceding 12 months as indicated by a response of “yes” to the question “During the past 12 months, have you had an eye exam from an eye specialist such as an optometrist, ophthalmologist, or eye doctor?” The factors of association selected for this analysis were based on previously reported metrics associated with receiving guideline-concordant annual vision screenings for diabetic adults and the Healthy People 2030 approach to the social determinants of health.44
For those 65 years and older, medical insurance status was stratified as private, dual eligible, Medicare Advantage, Medicare only excluding Medicare Advantage, uninsured, or other. For those under age 65, insurance status was stratified as private, Medicaid and other public, uninsured, or other. In a separate analysis, those with Medicaid and private health insurance plans with deductibles were grouped into those with plans qualifying as high deductible health plans (>$1350 for an individual or >$2700 for two or more persons) and those that do not.
Geographic location was divided by region (Northeast, Midwest, South, or West). Respondents were classified along an urban-rural continuum based on county of residence (large central metro, large fringe metro, medium and small metro, or nonmetropolitan).
A previous study has shown that patients receiving diabetes care at a Veteran’s Health Administration funded hospital are more likely to receive annual DR screenings.34 Use of VA healthcare was measured by self-reported care received at a Veteran’s Health Administration facility or health care paid for by the VA.
Since the variables within the NHIS are not always congruent with the established five domains of the SDH, a review of the available literature was used to select variables that best aligned with several of the SDH domains. Economic stability (income, inability to pay medical bills, eating less than needed due to financial strain), education access and quality (completion of high school), and health care access and quality (established regular place of care) were the three domains assessed in our study.5,8,45,46 Two of the domains of the SDH, neighborhood and built environment and social and community context, were not analyzed in this study as no questions within the 2019 NHIS assessed these domains.
An inability to pay medical bills and eating less than needed due to cost were the two variables used to assess the “economic stability” domain of the SDH. We selected these two variables to measure economic stability rather than a purely income-based analysis as income level itself does not necessarily correlate to overall financial stability given variability in expenses due to family size, life stage, and geographic location.
Statistical Analysis
Table 1 represents bivariate comparisons of select independent variables (P<0.05) among the study population comparing those who received an eye exam in the last 12 months and those who did not receive an eye exam in the last 12 months. According to the instructions published with the 2019 NHIS, sampling weights were used to produce representative national estimates for the study population.43 Information regarding the proper use of the survey data files and weighting is available in the annual survey description documents by data year.47
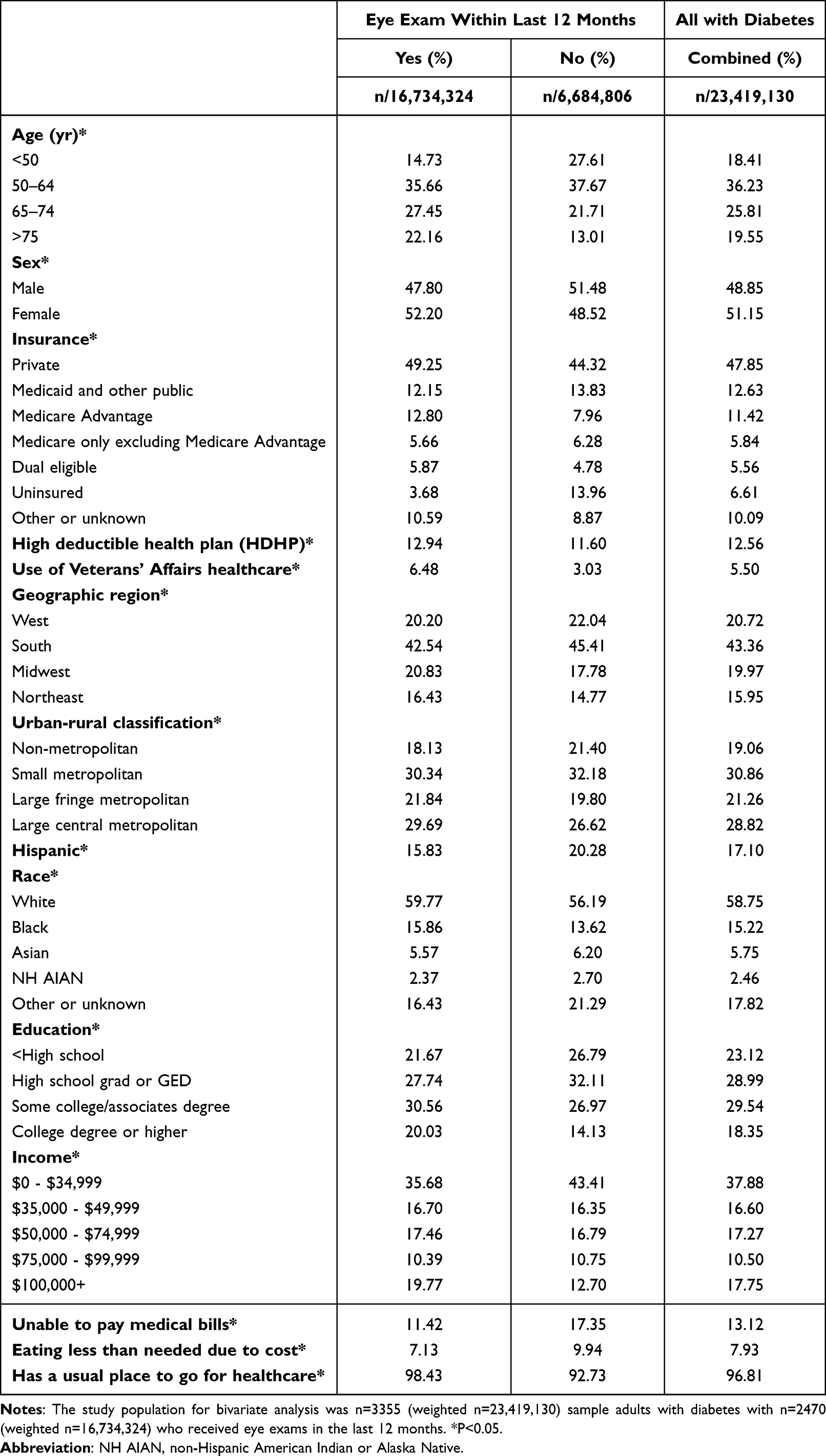 |
Table 1 Bivariate Analysis of US Adults Ages 18 Years and Older with Diabetes Diagnosis (Non-Gestational) by Eye Exam in Last 12 Months |
We used a multivariate logistic regression model that controlled for age, sex, race (white, black, Asian and other), ethnicity (Hispanic and non-Hispanic), and co-morbidities. Odds ratios (OR) and 95% CI statistical analyses were generated with Statistical (SAS) Version 9.3, SAS Institute Inc. Cary, NC using proc survey logistic and survey means to account for NHIS specific weights and strata. To minimize multicollinearity, we examined the variance inflation factors (VIF). VIF is used to measure how much of the variance of an estimated regression coefficient increases in the event of high correlation between two or more independent variables. The VIF were generated using the proc reg command in SAS to assess for multicollinearity in the regression analysis.
Results
Table 1 shows the demographic characteristics of the 3355 surveyed adults (representing a national estimate of 23,419,130 individuals) who have self-reported type 1 and type 2 diabetes split by those who did and did not have an eye exam in the prior 12-months and indicates that various sociodemographic, insurance, geographic, and select social determinants of health were statistically different between these two groups. In 2019, 2470 individuals within the study population of 3355 (73.62%) received an eye exam in the previous 12 months (Table 1).
Racial self-identity was colinear with several of our variables and not included in our final analysis. Thereafter, the VIF values for our selected social determinant factors were less than 5, which demonstrated a lack of collinearity between the predictors.
Table 2 shows the results of the multivariate logistic regression model. The model found that receiving an eye exam within the last 12 months was positively associated with female sex (OR 1.29; 95% CI 1.05–1.58), residence in the Midwestern United States (OR 1.39; 95% CI 1.01–1.92), use of Veteran’s Health Administration healthcare (OR 2.15; 95% CI 1.34–3.44), having a usual place to go for healthcare (OR 3.89; 95% CI 2.16–7.01), and the use of Private, Medicare Advantage, or other insurance (OR 3.66; 95% CI 2.42–5.53), use of Medicare only excluding Medicare Advantage (OR 3.18; 95% CI 1.95–5.30), dual eligibility for Medicare and Medicaid (OR 3.88; 95% CI 2.21–6.79), and use of Medicaid and other public health insurance (OR 3.04; 95% CI 1.89–4.88) compared to those without insurance. Inversely, an educational attainment of less than high school (OR 0.66; 95% CI 0.48–0.92), and an educational attainment of high school or GED without any college (OR 0.62; 95% CI 0.47–0.81) were associated with not receiving an eye exam in the previous 12 months. Urban-rural classification of county of residence, use of HDHPs, inability to pay medical bills, and eating less than needed due to cost were not significantly associated with receiving an eye exam in the last 12 months among diabetic adults.
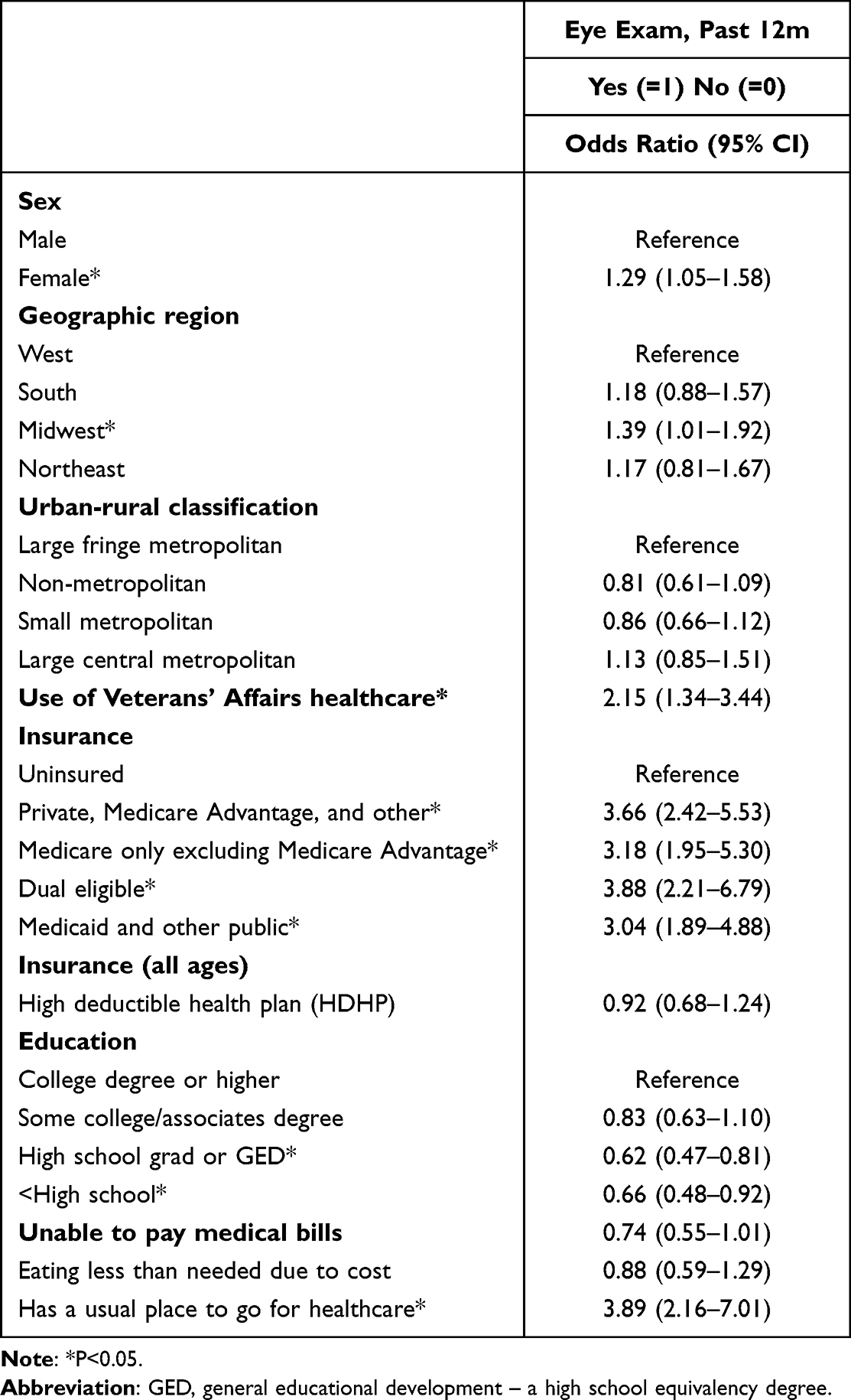 |
Table 2 Multivariate Logistic Regression for Eye Exam in Last 12 Months for US Adults Ages 18 Years and Older with Diabetes (Non-Gestational) |
Discussion
Our study found a significant correlation between female sex and receiving an eye exam in the previous 12 months (OR 1.29; 95% CI 1.05–1.58). Previous research has drawn conflicting conclusions regarding the correlation of sex with adherence to diabetic retinopathy screening guidelines.7,22 The findings of our study are marginally significant and suggest that in 2019 women with diabetes were more likely to receive an eye exam than men with diabetes.
We also observed a significant correlation between receiving an eye exam in the previous 12 months and residence in the Midwestern United States when compared to the Western, Northeastern, and Southeastern United States (OR 1.39; 95% CI 1.01–1.92). This effect was moderate. Given the strong ties between insurance coverage and likelihood of receiving an eye exam in the previous 12 months, we anticipated that those residing in regions with higher rates of Medicaid expansion (the Western and Northeastern United States) may have been more likely to receive an eye exam in the previous 12 months, although our findings did not confirm this suspicion.
Interestingly, our study did not find any significant difference in receiving an eye exam in the previous 12 months based on classification of county of residence as non-metropolitan, small metropolitan, large fringe metropolitan, or large central metropolitan. This contrasts the results of previous studies demonstrating that those living in rural areas are less likely to receive regular screenings for diabetic retinopathy and eye exams generally.15,36 These data should be interpreted within the context of existing literature as disparities in DR screenings between urban and rural populations are well described.15,36
Another finding from our study showed that those who received care at a Veteran’s Health Administration facility or health care paid for by the VA in the previous 12 months were significantly more likely to have received an eye exam in the previous 12 months compared to those who did not (OR 2.15; 95% CI 1.34–3.44). This is congruent with findings from previous studies demonstrating that patients in the VA system were more likely than patients in commercial managed care to receive diabetic eye exams.34 This is also consistent with previously published findings that those in comprehensive and well-connected healthcare organizations are more likely to receive care consistent with established guidelines for diabetes.35
We also show that those who are insured are significantly more likely to have received an eye exam in the previous 12 months regardless of the type of insurance when compared to those who are uninsured. This is consistent with findings from previous studies showing that those without insurance are less likely to receive guideline-concordant care for diabetic retinopathy.11,21,22,27,28,37 Cost-related barriers to care and a lack of coordination of diabetes care among the uninsured may explain why diabetics without insurance are less likely to receive guideline-concordant care and highlights an important area to be targeted by public health professionals.
Our study is also one of the first to look at the relationship between HDHPs and the likelihood of receiving an eye exam among diabetic adults. Previous studies have shown that patients enrolled in HDHPs are more likely to delay interventions for complications of diabetes and less likely to engage in preventative screenings related to diabetes.40,41 However, our findings showed no significant difference in the likelihood of receiving an eye exam in the previous 12 months for those with HDHPs compared to those with deductibles beneath the HDHP threshold.
We used several variables within the NHIS to capture the impact of the domains of the social determinants of health on the likelihood of receiving an eye exam in the previous 12 months among diabetic adults. We show that an educational attainment of high school grad or GED with no college (OR 0.62; 95% CI 0.47–0.81) or a less than high school education (OR 0.66; 95% CI 0.48–0.92) are negatively associated with receiving an eye exam in the previous 12 months. This is consistent with the findings from other studies which have consistently showed positive associations between higher educational attainment and the likelihood of receiving regular diabetic retinopathy screenings.5,22,27,46
The single most predictive factor for receiving an annual eye exam among diabetic adults was having a usual place to go for healthcare (OR 3.89; 95% CI 2.16–7.01). This is consistent with previous research showing that regular contact with a primary care provider was positively correlated with receiving an annual screening exam for diabetic retinopathy.30 This finding emphasizes the importance of the social determinants of health domain “health care access and quality” in ensuring that diabetic adults receive annual vision screenings.
An inability to pay medical bills did not show a significant inverse correlation with receiving an eye exam in the last year although did come close to exceeding the significance threshold. Similarly, eating less than needed due to cost did not have a significant association with an eye exam in the previous 12 months. These findings were surprising given that income has been cited as a commonly positively correlated factor with receiving annual eye exams for diabetic retinopathy.22,27 This difference may be due to the use of variables in our analysis that capture functional economic stability (via difficulty paying for essential needs) instead of income itself.
This study has several limitations. The NHIS itself is based on self-reported responses and is not verified using insurance claims or the electronic health records. Further, this study was limited by our use of the NHIS variables as they are written. The question used as the primary outcome, “During the past 12 months, have you had an eye exam from an eye specialist such as an optometrist, ophthalmologist, or eye doctor?” does not distinguish between a full dilated diabetic eye exam and a standard vision screening by an optometrist. As a result, we may be overestimating the number of patients who are concordant with their diabetic eye exam screenings by capturing those who received only a refractory exam for a glasses or contacts prescription update.
Due to multicollinearity of race and SDH measures, our study did not examine the direct association between receiving an eye exam in the previous 12 months and self-reported racial identity. Several studies have shown significant racial disparities in diabetic retinopathy screening with strong links to the social determinants of health.6,10,33 Public health efforts that seek to improve the percentage of Americans receiving their annual diabetic eye exam should incorporate previously published literature findings demonstrating the racial disparities in receiving guideline-concordant diabetic retinopathy screenings.
Our study assessed the relationship between various insurance-related, geographic, and SDHs with receiving an eye exam in the preceding 12 months among adults with self-reported diabetes diagnoses using the nationally representative data collected in the 2019 National Health Interview Survey (NHIS). We were able to verify an array of previously reported associations including education, healthcare access, and Veteran’s Health Administration or VA funded healthcare and showed that Medicare Advantage plans were associated with an increased likelihood in eye examinations among diabetic adults. These findings provide important information to policy makers and public health professionals in the endeavor to achieve the goal laid out in the Health People 2030 report to “increas[e] the proportion of adults with diabetes who have a yearly eye exam”26
Conclusion
The results of this study suggest that many factors are associated with diabetic adults receiving an annual eye exam. Female sex, residence in the Midwestern United States, use of VA healthcare, having health insurance, and having a usual place to go for healthcare were positively associated with an eye exam in the previous 12 months. In contrast, educational attainment less than or equal to high school or GED was associated with a decreased likelihood of receiving an eye exam in the previous 12 months among diabetic adults. These findings may be used by public health professionals to develop interventions aimed at increasing the proportion of adults with diabetes who have a yearly eye exam.
Acknowledgments
We thank Joanne Li (Northwestern University) for assistance with manuscript proofreading. The study resulting in this publication was assisted by funding through the Summer Research Scholars Program administered by The Feinberg School of Medicine. The conclusions, opinions, and other statements in this publication are the authors’ and not necessarily those of the sponsoring institution.
Funding
This research was supported by an unrestricted grant from Research to Prevent Blindness (RPB) NY, NY. Alec. N.A. Jotte was supported by the Northwestern University Feinberg School of Medicine’s Summer Research Scholars Program (SRSP).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lin X, Xu Y, Pan X, et al. Global, regional, and national burden and trend of diabetes in 195 countries and territories: an analysis from 1990 to 2025. Sci Rep. 2020;10(1):14790. doi:10.1038/s41598-020-71908-9
2. Centers for Disease Control and Prevention National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States ; 2022. Available from: https://www.cdc.gov/diabetes/data/statistics-report/index.html.
3. National Diabetes Statistics Report. Coexisting conditions and complications; 2021. Available from: https://www.cdc.gov/diabetes/data/statistics-report/coexisting-conditions-complications.html.
4. Diabetes TL. Under the lens: diabetic retinopathy. Lancet Diabetes Endocrinol. 2020;8(11):869. doi:10.1016/S2213-8587(20)30347-8
5. Williams AM, Sahel JA. Addressing social determinants of vision health. Ophthalmol Ther. 2022;11(4):1371–1382. doi:10.1007/s40123-022-00531-w
6. Thomas CG, Channa R, Prichett L, Liu TYA, Abramoff MD, Wolf RM. Racial/ethnic disparities and barriers to diabetic retinopathy screening in youths. JAMA Ophthalmol. 2021;139(7):791–795. doi:10.1001/jamaophthalmol.2021.1551
7. Gange WS, Xu BY, Lung K, Toy BC, Seabury SA. Rates of eye care and diabetic eye disease among insured patients with newly diagnosed type 2 diabetes. Ophthalmol Retina. 2021;5(2):160–168. doi:10.1016/j.oret.2020.07.004
8. Cai CX, Li Y, Zeger SL, McCarthy ML. Social determinants of health impacting adherence to diabetic retinopathy examinations. BMJ Open Diabetes Res Care. 2021;9(1):e002374. doi:10.1136/bmjdrc-2021-002374
9. Yusuf R, Chen EM, Nwanyanwu K, Richards B. Neighborhood deprivation and adherence to initial diabetic retinopathy screening. Ophthalmol Retina. 2020;4(5):550–552. doi:10.1016/j.oret.2020.01.016
10. Shi Q, Zhao Y, Fonseca V, Krousel-Wood M, Shi L. Racial disparity of eye examinations among the U.S. working-age population with diabetes: 2002–2009. Diabetes Care. 2014;37(5):1321–1328.
11. Paz SH, Varma R, Klein R, Wu J, Azen SP. Noncompliance with vision care guidelines in Latinos with type 2 diabetes mellitus: the Los Angeles Latino eye study. Ophthalmology. 2006;113(8):1372–1377. doi:10.1016/j.ophtha.2006.04.018
12. Shah S, Feher M, McGovern A, et al. Diabetic retinopathy in newly diagnosed type 2 diabetes mellitus: prevalence and predictors of progression; a national primary network study. Diabetes Res Clin Pract. 2021;175:108776. doi:10.1016/j.diabres.2021.108776
13. Zhang X, Saaddine JB, Lee PP, et al. Eye care in the United States: do we deliver to high-risk people who can benefit most from it? Arch Ophthalmol. 2007;125(3):411–418. doi:10.1001/archopht.125.3.411
14. Zhang X, Saaddine JB, Chou CF, et al. Prevalence of diabetic retinopathy in the United States, 2005–2008. JAMA. 2010;304(6):649–656. doi:10.1001/jama.2010.1111
15. Liu Y, Zupan NJ, Shiyanbola OO, et al. Factors influencing patient adherence with diabetic eye screening in rural communities: a qualitative study. PLoS One. 2018;13(11):e0206742. doi:10.1371/journal.pone.0206742
16. American Diabetes Association Focus on diabetes: look closer at eye health 2022 . Available from: https://www.diabetes.org/diabetes/eye-health.
17. Ferris FL
18. Committee ADAPP. Retinopathy, neuropathy, and foot care: standards of medical care in diabetes—2022. Diabetes Care. 2021;45(Supplement_1):S185–S194.
19. Flaxel CJ, Adelman RA, Bailey ST, et al. Diabetic retinopathy preferred practice pattern. Ophthalmology. 2020;127(1):PP66–P145. doi:10.1016/j.ophtha.2019.09.025
20. An J, Niu F, Turpcu A, Rajput Y, Cheetham TC. Adherence to the American diabetes association retinal screening guidelines for population with diabetes in the United States. Ophthalmic Epidemiol. 2018;25(3):257–265. doi:10.1080/09286586.2018.1424344
21. Chou CF, Sherrod CE, Zhang X, et al. Barriers to eye care among people aged 40 years and older with diagnosed diabetes, 2006–2010. Diabetes Care. 2014;37(1):180–188. doi:10.2337/dc13-1507
22. Eppley SE, Mansberger SL, Ramanathan S, Lowry EA. Characteristics associated with adherence to annual dilated eye examinations among US patients with diagnosed diabetes. Ophthalmology. 2019;126(11):1492–1499. doi:10.1016/j.ophtha.2019.05.033
23. Bressler NM, Varma R, Doan QV, et al. Underuse of the health care system by persons with diabetes mellitus and diabetic macular edema in the United States. JAMA Ophthalmol. 2014;132(2):168–173. doi:10.1001/jamaophthalmol.2013.6426
24. Centers for Disease Control and Prevention. Self-reported visual impairment among persons with diagnosed diabetes --- United States, 1997–2010. MMWR Morb Mortal Wkly Rep. 2011;60(45):1549–1553.
25. Lee PP, Feldman ZW, Ostermann J, Brown DS, Sloan FA. Longitudinal rates of annual eye examinations of persons with diabetes and chronic eye diseases. Ophthalmology. 2003;110(10):1952–1959. doi:10.1016/S0161-6420(03)00817-0
26. US Department of Health and Human Services Office of Disease Prevention and Health Promotion Increase the proportion of adults with diabetes who have a yearly eye exam — d-04. Healthy People 2030; 2020. Available from: https://health.gov/healthypeople/objectives-and-data/browse-objectives/diabetes/increase-proportion-adults-diabetes-who-have-yearly-eye-exam-d-04.
27. Paksin-Hall A, Dent ML, Dong F, Ablah E. Factors contributing to diabetes patients not receiving annual dilated eye examinations. Ophthalmic Epidemiol. 2013;20(5):281–287. doi:10.3109/09286586.2013.789531
28. Murchison AP, Hark L, Pizzi LT, et al. Non-adherence to eye care in people with diabetes. BMJ Open Diabetes Res Care. 2017;5(1):e000333. doi:10.1136/bmjdrc-2016-000333
29. Hudson SM, Modjtahedi BS, Altman D, Jimenez JJ, Luong TQ, Fong DS. Factors affecting compliance with diabetic retinopathy screening: a qualitative study comparing English and Spanish speakers. Clin Ophthalmol. 2022;16:1009–1018. doi:10.2147/OPTH.S342965
30. O’Keeffe D, Riordan F, Harkins V, Kearney P, Mc Hugh S. Predictors of attendance at diabetic retinopathy screening among people with type 2 diabetes: secondary analysis of data from primary care. Prim Care Diabetes. 2021;15(6):1086–1094. doi:10.1016/j.pcd.2021.08.004
31. Ferm ML, DeSalvo DJ, Prichett LM, Sickler JK, Wolf RM, Channa R. Clinical and demographic factors associated with diabetic retinopathy among young patients with diabetes. JAMA Netw Open. 2021;4(9):e2126126. doi:10.1001/jamanetworkopen.2021.26126
32. Ghamdi AHA. Clinical predictors of diabetic retinopathy progression; a systematic review. Curr Diabetes Rev. 2020;16(3):242–247. doi:10.2174/1573399815666190215120435
33. Fairless E, Nwanyanwu K. Barriers to and facilitators of diabetic retinopathy screening utilization in a high-risk population. J Racial Ethn Health Disparities. 2019;6(6):1244–1249. doi:10.1007/s40615-019-00627-3
34. Kerr EA, Gerzoff RB, Krein SL, et al. Diabetes care quality in the veterans affairs health care system and commercial managed care: the TRIAD study. Ann Intern Med. 2004;141(4):272–281. doi:10.7326/0003-4819-141-4-200408170-00007
35. Lawrenson JG, Graham-Rowe E, Lorencatto F, et al. Interventions to increase attendance for diabetic retinopathy screening. Cochrane Database Syst Rev. 2018;1:CD012054. doi:10.1002/14651858.CD012054.pub2
36. Fathy C, Patel S, Sternberg P
37. Doucette ED, Salas J, Wang J, Scherrer JF. Insurance coverage and diabetes quality indicators among patients with diabetes in the US general population. Prim Care Diabetes. 2017;11(6):515–521. doi:10.1016/j.pcd.2017.05.007
38. Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
39. Lee DJ, Lam BL, Arora S, et al. Reported eye care utilization and health insurance status among US adults. Arch Ophthalmol. 2009;127(3):303–310. doi:10.1001/archophthalmol.2008.567
40. Wharam JF, Lu CY, Zhang F, et al. High-deductible insurance and delay in care for the macrovascular complications of diabetes. Ann Intern Med. 2018;169(12):845–854. doi:10.7326/M17-3365
41. Wu YM, Huang J, Reed ME. Association between high-deductible health plans and engagement in routine medical care for type 2 diabetes in a privately insured population: a propensity score-matched study. Diabetes Care. 2022;45(5):1193–1200. doi:10.2337/dc21-1885
42. IRS. Tax forms and instructions. 26 CFR 601.602. Available from: https://www.irs.gov/pub/irs-drop/rp-18-30.pdf2019.
43. Centers for Disease Control and Prevention Survey Description, National Health Interview Survey; 2019. Available from: https://ftp.cdc.gov/pub/Health_Statistics/NCHS/Dataset_Documentation/NHIS/2019/srvydesc-508.pdf.
44. Social Determinants of Health. Healthy people; 2030. Available from: https://health.gov/healthypeople/priority-areas/social-determinants-health.
45. Daniel H, Bornstein SS, Kane GC, et al. Addressing social determinants to improve patient care and promote health equity: an American college of physicians position paper. Ann Intern Med. 2018;168(8):577–578. doi:10.7326/M17-2441
46. Su NH, Moxon NR, Wang A, French DD. Associations of social determinants of health and self-reported visual difficulty: analysis of the 2016 national health interview survey. Ophthalmic Epidemiol. 2020;27(2):93–97. doi:10.1080/09286586.2019.1680703
47. NHIS Data. Questionnaires and related documentation. National Center for Healthcare Statistics. Available from: https://www.cdc.gov/nchs/nhis/data-questionnaires-documentation.htm.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.