Back to Journals » International Journal of Women's Health » Volume 18
Factors Affecting Pregnancy Outcomes in Patients Undergoing in vitro Fertilization/Intracytoplasmic Sperm Injection-Embryo Transfer (IVF/ICSI-ET) After Hysteroscopic Adhesiolysis: A Clinical Analysis
Authors Jin X, Wang Y, Wang X, Li C, Hong X, Hong F, Zhang S
Received 27 March 2026
Accepted for publication 19 June 2026
Published 9 July 2026 Volume 2026:18 611737
DOI https://doi.org/10.2147/IJWH.S611737
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Xiaoying Jin,1– 3 Yangyang Wang,1– 3 Xiufen Wang,1– 3 Chao Li,1– 3 Xia Hong,1– 3 Fang Hong,1– 3 Songying Zhang1– 3
1Assisted Reproduction Unit, Department of Obstetrics and Gynecology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China; 2Zhejiang Key Laboratory of Precise Protection and Promotion of Fertility, Hangzhou, People’s Republic of China; 3Zhejiang Provincial Clinical Research Center for Reproductive Health and Disease, Hangzhou, People’s Republic of China
Correspondence: Songying Zhang, Assisted Reproduction Unit, Department of Obstetrics and Gynecology, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, People’s Republic of China, Email [email protected]
Purpose: To identify the independent risk factors for placenta accreta spectrum (PAS) and assess the impact of endometrial thickness (EMT) on outcomes after transcervical resection of adhesions (TCRA) for intrauterine adhesions(IUA) prior to in vitro fertilization/intracytoplasmic sperm injection-embryo transfer (IVF/ICSI-ET).
Methods: This single-center retrospective cohort study included 819 post-TCRA patients between March 2018 and March 2023. Propensity score matching (PSM) was used to balance baseline characteristics. Univariate and multivariate logistic regression analyses identified independent risk factors for PAS. Pregnancy outcomes (biochemical pregnancy, clinical pregnancy, live birth) and adverse obstetric outcomes (PAS, gestational diabetes, preterm delivery, low birth weight) were compared between EMT groups using different cutoffs (6– 8 mm).
Results: EMT and moderate-to-severe IUA were independent PAS risk factors (severe IUA: aOR=4.998, 95% CI:2.021~12.362). After PSM, the EMT < 7 mm group had significantly lower live birth rates (40.3% vs. 55.7%,P=0.005) and higher rates of gestational diabetes,preterm delivery and low birth weight compared to EMT ≥ 7 mm. Using an 8 mm cutoff, the EMT < 8 mm group consistently showed a higher PAS incidence both before (26.4% vs. 13.9%, P=0.001) and after PSM (26.4% vs. 14.7%, P=0.018).
Conclusion: In post-TCRA IVF/ICSI-ET patients, EMT and IUA severity are independent PAS risk factors. EMT< 7 mm worsens pregnancy outcomes, Exploratory analyses suggested that EMT < 8 mm may be associated with higher PAS risk,but this finding requires validation in larger, prospective studies. Given the single-center retrospective design, these results should be interpreted as associative rather than causal. We think optimizing endometrial preparation to achieve a thickness of at least 8 mm may be crucial for reducing PAS and improving reproductive prognosis.
Keywords: TCRA, IVF/ICSI-ET, EMT, PAS, pregnancy outcomes
Introduction
Intrauterine adhesions (IUA), also known as Asherman syndrome, result from fibrosis and adhesion formation within the uterine cavity, typically following damage to the endometrial basal layer due to infection, trauma (such as surgical injury), or other causes. Clinical features include hypomenorrhea, amenorrhea, and infertility, largely attributable to endometrial fibrosis. Studies report that IUA occurs in 15–20% of women following induced abortion,1 accounts for approximately 43% of infertility cases, and is present in about 13% of infertile patients.2
IUA impairs endometrial thickness (EMT) and receptivity, elevating risks for failed conception and adverse pregnancy outcomes such as miscarriage and preterm birth. Current standard management involves hysteroscopic transcervical resection of adhesions (TCRA), often followed by placement of an intrauterine barrier and estrogen therapy.3 Nevertheless, recurrence rates remain high (33.3%–45.7%) in moderate-to-severe cases,4 and live birth rates after TCRA are only 23.7%–27.7%.5
Beyond recurrence and live birth, recent evidence has raised concern about placenta accreta spectrum (PAS) – a life-threatening condition where trophoblastic tissue abnormally adheres to or invades the myometrium. The biological link between IUA/TCRA and PAS is plausible: damage to the endometrial basal layer disrupts decidualization, which normally limits trophoblast invasion. Defective decidualization allows deeper trophoblast penetration, predisposing to PAS.6 Repeated TCRA procedures may further compromise the endometrial–myometrial junction zone and impair neoangiogenesis, creating a hypoxic, fibrotic microenvironment that promotes abnormal placentation.7 Moreover, thin endometrium – a common sequela of severe IUA – has been associated with reduced expression of integrins and other implantation-related molecules, potentially altering the maternal–fetal interface and increasing PAS risk.
Among patients conceiving via assisted reproductive technology (ART), those with a history of IUA – particularly after multiple adhesion surgeries – face significantly increased risks of adverse obstetric outcomes including PAS, placenta previa, and postpartum hemorrhage. Notably, while one study8 found comparable implantation and live birth rates between IVF patients with and without surgically treated IUA, the IUA group had a higher risk of placental complications.
Despite these findings, most existing studies have compared obstetric outcomes between IUA and non-IUA patients, with limited focus on post-TCRA patients undergoing IVF/ICSI-ET. In particular, the optimal EMT threshold for minimizing PAS risk after TCRA remains unknown. While EMT <7 mm is widely accepted as “thin” and associated with lower pregnancy rates,9,10 it is unclear whether a higher threshold (eg., ≥8 mm) is needed to reduce PAS – a rare but catastrophic complication.
Therefore, this study analyzes data from patients who underwent IVF/ICSI-ET after TCRA at our center, aiming to identify independent risk factors for PAS, with special attention to EMT and IUA severity and provide evidence-based guidance for endometrial preparation before embryo transfer in this high-risk population.
Material And Methods
Ethical Approval
This retrospective study was approved by the Ethics Committee of Sir Run Run Shaw Hospital (Approval No2026-2002). The requirement for informed consent from individual patients was waived by the Ethics Committee, as this study involved retrospective analysis of anonymized clinical data extracted from existing medical records, with no direct interaction with patients and no more than minimal risk to the subjects. Obtaining individual informed consent was not practicable due to the retrospective nature of the study and the large sample size, and the waiver did not adversely affect the rights or welfare of the patients. All patient data were deidentified prior to analysis, and strict confidentiality measures were implemented to protect patient privacy throughout the study. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Study Population and Group Allocation
This was a retrospective study carried out at the Sir Run Run Shaw Hospital, Zhejiang University,Hangzhou,China,We enrolled patients who underwent IVF/ICSI-ET at our institution between March 2018 and March 2023, all with a history of TCRA (1–9 previous procedures.The inclusion criteria were as follows: (1) Aged 24–48 years; (2) Underwent fresh or frozen embryo transfer via IVF-ET or ICSI following TCRA for IUA between March 2018 and March 2023. Patients were excluded from recruitment if they had any of the following issues: (1) Severe reproductive dysfunction, including Male factor infertility (abnormal semen analysis); Ovarian failure (FSH >40 U/L) (2) Chromosomal abnormalities in either partner (3) Incomplete clinical data compromising reliability.
Patients were categorized into two groups based on EMT: Thin endometrium group: EMT <7 mm and Normal endometrium group: EMT ≥7 mm. EMT was measured by transvaginal ultrasound on either the day of human chorionic gonadotropin (hCG) administration for ovulation triggering (hCG trigger day) or the day of endometrial transformation (for frozen embryo transfer cycles). EMT was defined as the maximal distance between the two endometrial-myometrial interfaces in the mid-sagittal plane, measured at the thickest part of the endometrium. It refers to the maximum anterior-posterior thickness of the endometrial echo on a long-axis transvaginal view of the uterus.11 For fresh IVF-ET cycles, EMT was measured on the day of trigger, whereas for FETs it was measured before progesterone was initiated or luteinizing hormone surge or HCG administration was documented.
Research Methods
Diagnosis of IUA
The diagnostic criteria for IUA is assessed in line with the Chinese Expert Consensus on Clinical Diagnosis and Treatment of Intrauterine Adhesions formulated by the expert panel organized by the Obstetrics and Gynecology Society of the Chinese Medical Association in December 2015.
Hysteroscopic Examination and TCRA
All patients underwent TCRA under intravenous anesthesia 3–7 days post-menstruation, with ultrasound or laparoscopic guidance as needed. A 4.5 mm hysteroscope (Storz, Germany) was used, and adhesions were sharply dissected with micro-scissors. The surgical endpoint was restoration of normal uterine cavity shape and bilateral tubal ostium visualization, or termination when cavity normalization was unachievable and perforation risk increased significantly. Postoperatively, all patients received prophylactic antibiotics and postoperative artificial cycle therapy.
Regimen for artificial menstrual cycle: Oral administration of estradiol valerate 2mg every 12 hours daily for 21–28 consecutive days. During the last 7–10 days of the cycle, medroxyprogesterone acetate 6mg was taken once daily in an overlapping manner. Both medications were discontinued to await menstruation. After menstruation occurred, the artificial menstrual cycle therapy was continued. A three-dimensional color Doppler ultrasound re-examination was performed within 1 week after menstruation. If adhesions were still indicated, a hysteroscopic re-examination was conducted.
Methods for IVF, ICSI-ET and Endometrial Preparation in Frozen-Thawed Embryo Transfer Cycles
All subjects underwent ovulation induction according to the routine protocols of the Reproductive Center of our hospital, including the follicular phase long protocol, antagonist protocol, or ovarian stimulation under progesterone priming. Follicular development was monitored by transvaginal B-ultrasound, and hCG 5000–10000 IU or Decapeptyl (triptorelin acetate injection) 0.2 mg was administered at the optimal time. Oocyte retrieval was performed under B-ultrasound guidance 36 hours later. The obtained oocyte-cumulus complexes were cultured for 2–6 hours, followed by insemination according to routine protocols or ICSI. Fertilization status was examined under a microscope 16–20 hours after fertilization. Fresh embryo transfer was conducted 72 hours after oocyte retrieval. Methods for endometrial preparation in frozen-thawed embryo transfer cycles included natural cycle, estrogen-progesterone artificial cycle, and mild stimulation cycle.
Embryo Quality Assessment and Embryo Transfer
Embryo quality was assessed and classified into 4 grades based on embryonic morphology and growth rate:12 Grade 1: Blastomeres are of equal size with no cellular fragments;Grade 2: Blastomeres are either equal or unequal in size with ≤20% cellular fragments;Grade 3: Blastomeres are either equal or unequal in size with 21%-49% cellular fragments; Grade 4: Blastomeres are of equal size with ≥50% cellular fragments.
High-quality embryos were defined as those with a normal cleavage rate (reaching 3–4 cells on Day 2 and 6–8 cells on Day 3) and <20% cellular fragments.12 Vitrification freezing and thawing technology was used for embryo cryopreservation and thawing.13 The criteria for embryo freezing were as follows: Day 3 embryos with ≥4 blastomeres, <50% cellular fragments, and an embryo score of grade 3 or better. Thawed embryos were re-scored, and an embryo was considered viable if at least half of its cells remained intact after revival. The interval between embryo thawing and transfer ranged from 10 minutes to 6 hours. Embryos were transferred to the mid-uterine cavity using a Wallace catheter (Smiths, UK). After transfer, luteal phase support was enhanced with either 40mg progesterone via intramuscular injection or 90mg progesterone vaginal sustained-release gel (Crinone, Fleet Laboratories Limited, UK) administered vaginally.
Observation Indicators
(1) Outcomes of biochemical pregnancy, clinical pregnancy, and live birth after embryo transfer. (2) Adverse pregnancy outcomes, including placenta previa, gestational diabetes mellitus, gestational hypertension, premature rupture of membranes, PAS, postpartum hemorrhage, preterm birth, and fetal birth weight, etc. (3) The primary outcome variable of this study is PAS. PAS diseases are a series of diseases with abnormal adhesion of trophoblastic tissue and invasion through uterine serosa. According to the different degrees of placental invasion, it can be divided into placenta accreta, placenta increta, and placenta percreta. The diagnosis criteria for PAS in this study were based on The International Federation of Gynecology and Obstetrics (FIGO) guideline, which involve either direct visualization during laparotomy or subsequent histopathological examination.14 For women who delivered vaginally, the diagnosis was primarily made using clinical criteria.14,15
Statistical Methods
Data were analyzed using SPSS 22.0 and R 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables are presented as mean ± standard deviation or median (IQR), compared using t-test or Kruskal–Wallis test. Categorical variables are expressed as frequencies and compared by chi-square test.
To balance baseline differences between cohorts, propensity score matching (PSM) was performed using 1:2 nearest-neighbor matching without replacement, with a caliper of 0.2. Balance was assessed using standardized mean difference (SMD), with SMD <0.25 considered well-balanced. Multivariate logistic regression was applied to evaluate the effect of TCRA on adverse pregnancy outcomes after fresh or frozen-thawed embryo transfer. All tests were two-tailed, with P < 0.05 considered statistically significant.To explore the optimal EMT threshold associated with PAS and pregnancy outcomes, multiple cutoffs (6, 6.5, 7, 7.5, and 8 mm) were tested. These analyses were exploratory and hypothesis-generating, not prespecified. Consequently, the risk of type I error due to multiple comparisons should be considered when interpreting the EMT <8 mm finding. No formal adjustment for multiple comparisons was applied because these analyses were intended to guide future hypothesis testing rather than confirm a prespecified threshold.
Results
General Information
A total of 819 patients were included in this study. Among them, 660 cases had an EMT of ≥7 mm, and 159 cases had an EMT of <7 mm. After PSM, there were 194 patients and 159 patients in the two groups, respectively. A total of 462 patients achieved pregnancy after IVF/ICSI-ET treatment.
Comparison of Clinical Data and Univariate Analysis Results between Pregnant Patients with and without PAS after IVF/ICSI-ET following TCRA
In this study, we first divided all patients who achieved pregnancy after IVF/ICSI-ET into two groups based on whether PAS occurred. Of the 462 patients who became pregnant, 376 did not develop PAS and 86 did.
The PAS group exhibited higher rates of secondary infertility (95.3% vs. 86.2%, P=0.02), scanty menstrual flow or amenorrhea before surgery (48.8% vs. 32.7%; 1.2% vs. 0.5%, P=0.01), and history of uterine curettage (91.9% vs. 78.7%, P=0.01). The number of prior curettages was also higher (1.58±1.06 vs. 1.36±1.14, P=0.04). On the day of embryo transfer, endometrial thickness (EMT) was thinner (7.82±1.23 mm vs. 8.65±1.64 mm, P=0.0001). The PAS group also had more previous TCRA procedures (2.16±1.22 vs. 1.60±0.95, P=0.0001), a higher proportion of moderate and severe intrauterine adhesions (66.3% vs. 48.9%; 14.0% vs. 4.8%, P=0.0001), and a greater rate of frozen embryo transfer (84.9% vs. 73.1%, P=0.02) (Table 1).
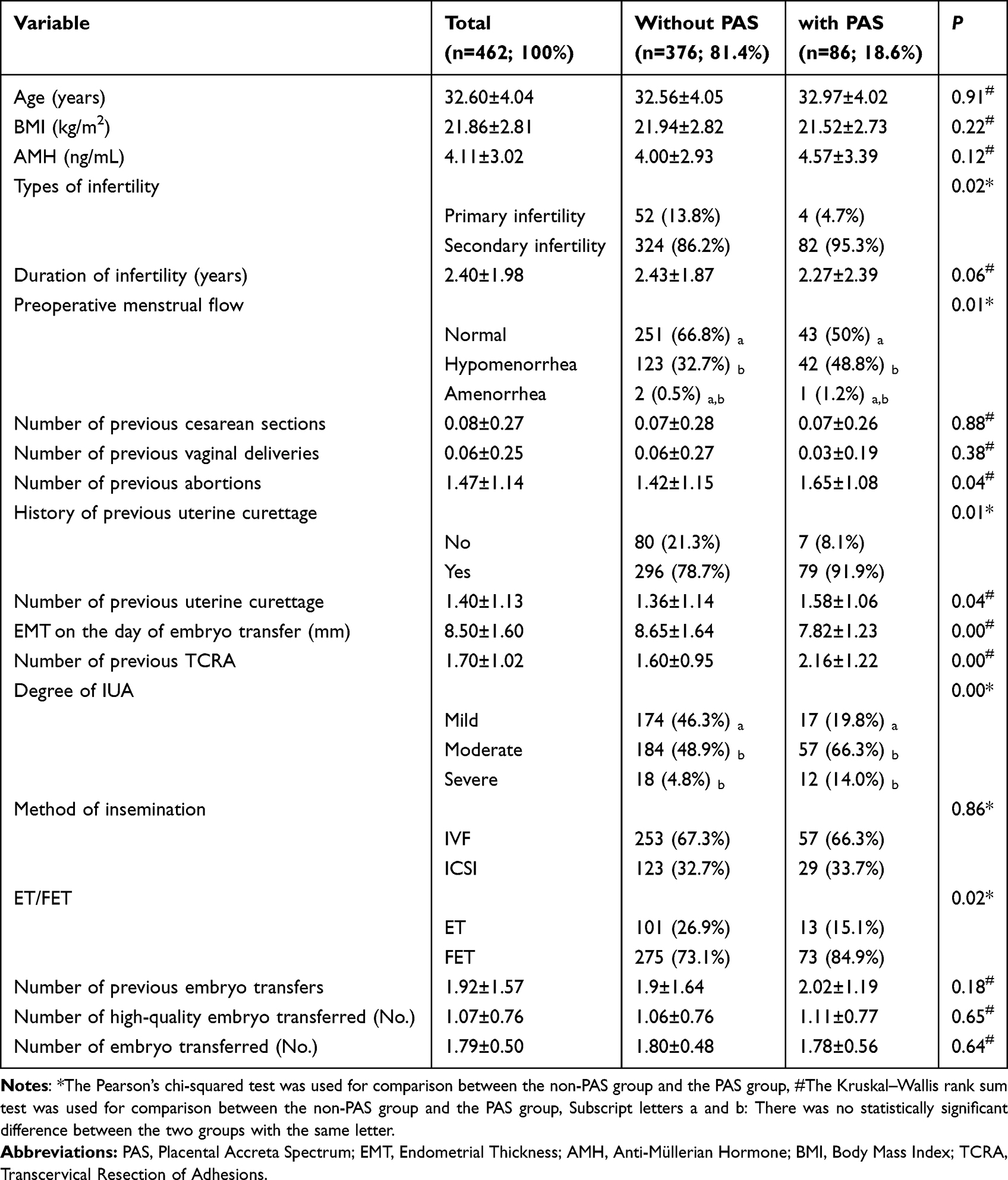 |
Table 1 Clinical Data and Results of Univariate Analysis of All Pregnant Patients Who Underwent IVF/ICSI After TCRA (with or Without PAS) |
Results of Multivariate Logistic Regression Analysis on Factors Influencing the Occurrence of PAS in Patients Undergoing IVF/ICSI-ET Treatment after TCRA
The above findings suggest that PAS incidence is associated with infertility type, preoperative menstrual flow, history and number of prior uterine curettages, EMT on the day of embryo transfer, number of previous TCRA procedures, severity of intrauterine adhesions, and frozen embryo transfer. To further identify factors influencing PAS, multivariate logistic regression (stepwise forward method) was performed, with baseline characteristics as independent variables and PAS occurrence as the dependent variable. The results identified EMT on the day of embryo transfer and moderate-to-severe intrauterine adhesions as independent risk factors for PAS (Table 2 and Supplementary Figure 1).
 |
Table 2 Multivariate Logistic Regression Analysis of Factors Influencing the Occurrence of PAS |
Comparison of Baseline Characteristics and Transplantation Variables Between the EMT ≥7 mm Group and EMT <7 mm Group before and after PSM
Before PSM, significant imbalances in baseline and transplantation variables existed between the two groups. Patients in the EMT <7 mm group were older (34.85±4.59 vs. 33.67±4.65, P=0.004), had more previous abortions (1.81±1.38 vs. 1.52±1.13, P=0.006), more previous uterine curettages (1.82±1.41 vs. 1.45±1.14, P=0.001), a higher proportion of patients with reduced preoperative menstrual flow (57.9% vs. 36.8%, P<0.001), a higher proportion of moderate and severe intrauterine adhesions (72.3% vs. 54.5%, 15.7% vs. 5.8%, P<0.001), more previous TCRA procedures (2.88±1.46 vs. 1.84±1.32, P<0.001), and a higher proportion of frozen embryo transfers (88.7% vs. 79.7%, P=0.012). In contrast, patients in the EMT ≥7 mm group had more previous embryo transfers (2.09±1.60 vs. 1.82±0.97, P=0.041).After PSM, baseline and transplantation variables were well balanced between groups (Supplementary Figure 2). No statistically significant differences remained in age, number of prior abortions or uterine curettages, preoperative menstrual flow, severity of intrauterine adhesions, number of prior TCRA procedures, proportion of frozen embryo transfers, or number of previous embryo transfers (all P>0.05) (Table 3).
 |
Table 3 Baseline Data of All Patients After IVF/ICSI Transfer Before and After Stratification Matching Based on an EMT of 7 mm |
Comparison of Pregnancy Outcomes between the EMT ≥7 mm Group and EMT <7 mm Group before and after PSM
We compared pregnancy outcomes following embryo transfer between the EMT ≥7 mm and <7 mm groups. Both before and after PSM, the EMT ≥7 mm group demonstrated significantly higher rates of biochemical pregnancy (78.5% vs. 54.1%, P<0.001; 72.2% vs. 54.1%, P=0.001), clinical pregnancy (72.1% vs. 47.8%, P<0.001; 64.4% vs. 47.8%, P=0.003), and live birth (62.0% vs. 40.3%, P<0.001; 55.7% vs. 40.3%, P=0.005) compared to the EMT <7 mm group (Table 4).
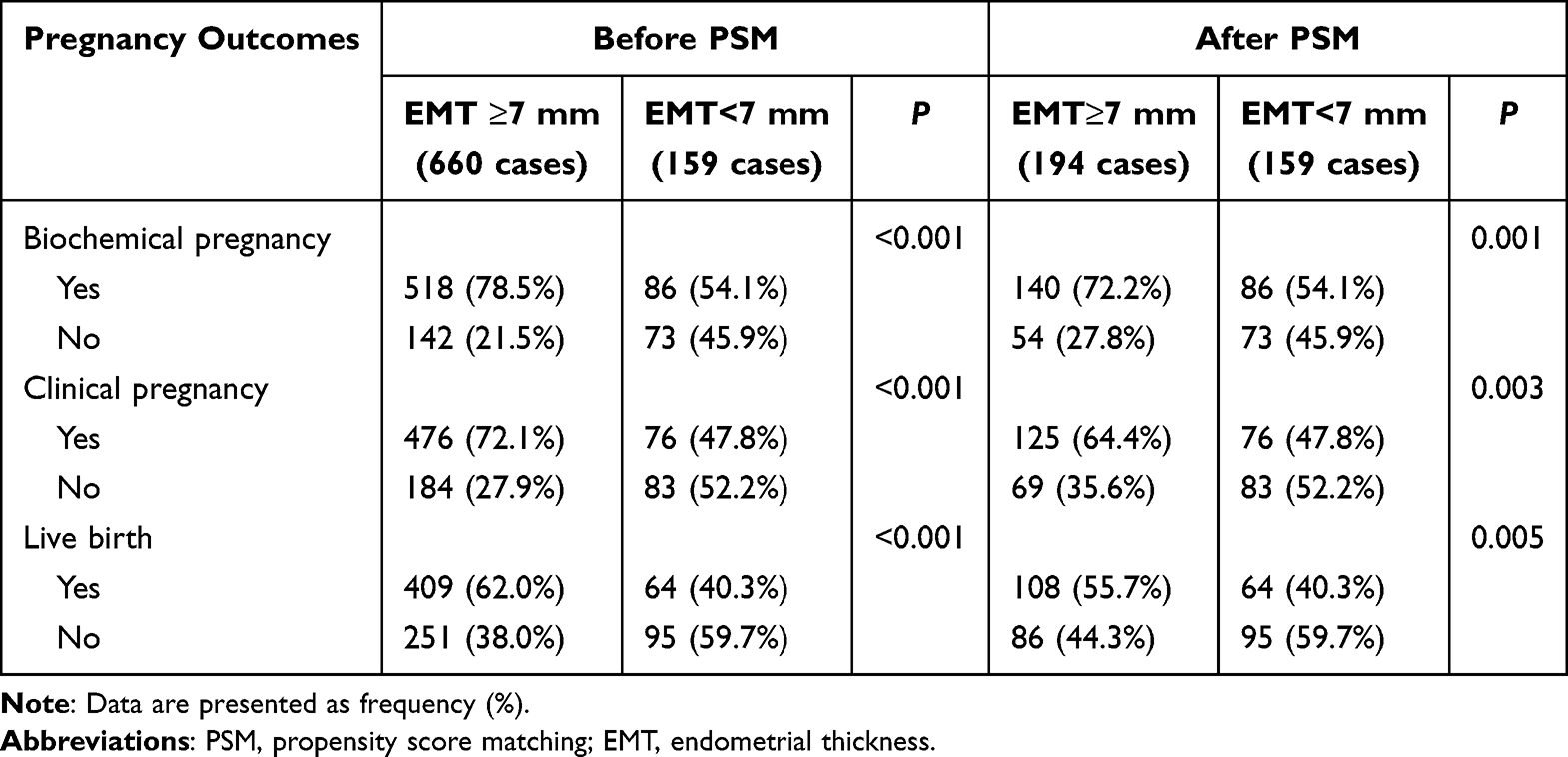 |
Table 4 Pregnancy Outcomes After Transfer in IVF/ICSI Patients Stratified by an Endometrial Thickness of 7 mm |
Adverse Pregnancy Outcomes in the EMT ≥7 mm Group and EMT <7 mm Group before and after PSM
We compared adverse pregnancy outcomes following embryo transfer between the EMT ≥7 mm and <7 mm groups. Both before and after PSM, the EMT <7 mm group had significantly higher rates of gestational diabetes mellitus (25% vs. 12.8%, P=0.017) and preterm birth (43.8% vs. 23.1%, P=0.001). The incidence of PAS was also higher in the EMT <7 mm group before PSM (29.7% vs. 16.8%, P=0.023), but this difference was no longer significant after PSM (29.7% vs. 20.2%, P=0.239). Regarding fetal birth weight, the rate of low birth weight was significantly higher in the EMT <7 mm group after PSM (25.8% vs. 7.5%, P=0.028) (Table 5).
 |
Table 5 Adverse Pregnancy Outcomes After Transfer in IVF/ICSI Patients Stratified by an Endometrial Thickness of 7 mm |
PAS Outcomes of Patients in the EMT ≥ 8 mm Group and EMT < 8 mm Group Before and After PSM
We compared PAS outcomes between the EMT ≥8 mm and <8 mm groups before and after PSM. Both before and after matching, the incidence of PAS was significantly higher in the EMT <8 mm group than in the EMT ≥8 mm group (26.4% vs. 13.9%, P=0.001; 26.4% vs. 14.7%, P=0.018) (Table 6). It should be noted that the 8 mm cutoff was not prespecified but was explored after observing the lack of significance for the 7 mm cutoff in the matched analysis. As such, this finding should be interpreted with caution and requires external validation.
 |
Table 6 PAS Outcomes After Embryo Transfer in IVF/ICSI Patients Stratified by an EMT Cut-off of 8 mm |
Discussion
PAS is a life-threatening obstetric complication, associated with uterine rupture, severe hemorrhage, emergency hysterectomy, and maternal mortality.16 While ART offers fertility solutions, patients with IUA who conceive via ART face increased risks of adverse outcomes--particularly PAS--likely due to endometrial injury and impaired repair.
Our study evaluated the impact of EMT at hCG trigger or FET scheduling on pregnancy outcomes, especially PAS, in infertile patients underwent IVF/ICSI-ET after TCRA. Our findings suggest a significant association between thinner EMT, greater IUA severity, and PAS occurrence. In exploratory analyses, an EMT < 8 mm on the day of embryo transfer was associated with a higher incidence of PAS, although this finding was not prespecified and requires prospective validation.
It is important to emphasize that, due to the retrospective, single-center design of this study, all findings should be interpreted as associations rather than causal relationships. The observed associations between thinner EMT, greater IUA severity, and adverse outcomes suggest potential risk markers rather than proven causal factors.
The global incidence of PAS has risen since the 1980s, with a reported rate at 0.17% in the general population.17 Following TCRA,however, the risk is markedly elevated: studies report PAS rates of 23.7% after Asherman syndrome treatment18 and 17.6% after IUA surgery.19 Correspondingly, our data (Table 1) show that 18.6% (86/462) of patients who achieved pregnancy via IVF/ICSI after TCRA developed PAS.
Epidemiological studies have established prior cesarean delivery and placenta previa as major risk factors for PAS, with diagnostic curettage, multiple pregnancies, intrauterine procedures, and ART also contributing.20 In our cohort, univariate analysis (Table 1) showed PAS to be significantly associated with secondary infertility, preoperative hypomenorrhea, repeated curettage or TCRA, moderate-to-severe adhesions, thinner endometrial thickness at transfer, and FET. Notably, parity and prior cesarean history did not differ significantly between groups, likely reflecting the infertility profile of our study population.
Accumulating evidence indicates that conception via ART increases PAS risk compared to natural conception,20 with FET identified as a particular risk factor. In our cohort, 84.9% of PAS cases occurred following FET, compared to 15.1% after fresh embryo transfer (Table 1). This finding aligns with recent large-scale studies. Using Japanese national registry data, Jwa et al reported that 96.3% of PAS cases occurred in FET cycles, with hormone replacement therapy (HRT) cycles conferring the highest risk.21 Matsuo et al similarly found a 14.1% incidence of non-previa PAS in HRT-FET cycles versus 0% in natural-cycle FET and fresh transfer groups.22 The biological mechanism linking FET to PAS is not fully understood but may involve supraphysiological estrogen levels in artificial cycles, which could affect decidualization and trophoblast invasion.21
In our multivariate analysis (Table 2), however, cycle type (FET vs. fresh) was not retained as an independent risk factor after adjusting for EMT and IUA severity. This suggests that the association between FET and PAS may be mediated by endometrial factors (such as thinner EMT) that are more common in FET cycles, rather than FET itself being an independent driver. Further studies are needed to disentangle the effects of cycle type, endometrial preparation protocols, and baseline endometrial characteristics.
Our multivariate analysis (Table 2) revealed that moderate-to-severe IUA and EMT were independently associated with PAS occurrence. Patients undergoing embryo transfer after severe IUA surgery exhibited a significantly increased risk of PAS (aOR=4.998, 95% CI: 2.021~12.362). IUA is a recognized risk factor for PAS, likely due to endometrial inflammation and fibrosis disrupting the intrauterine microenvironment and placental development.6 Although TCRA restores uterine cavity anatomy, achieving adequate endometrial preparation prior to transfer remains challenging in moderate-to-severe cases. Postoperative estrogen therapy may aid repair, but regeneration is often suboptimal, and repeated surgeries can further impair the endometrium and its vasculature. As EMT is a key indicator of endometrial receptivity, its clinical significance in embryo transfer outcomes is well established.
While a consensus definition of thin endometrium is lacking, a threshold of ≤7 mm is widely adopted.23,24 In a meta-analysis, Kasius et al reported that half of the included studies used this cutoff, associating it with lower ongoing pregnancy and live birth rates.9 Patients undergoing ART after TCRA are particularly susceptible to thin endometrium and impaired endometrial development. To inform clinical practice, we stratified patients by EMT (<7 mm vs. ≥7 mm) and assessed pregnancy outcomes and PAS incidence following embryo transfer.Baseline characteristics differed significantly between groups (Table 3). After PSM, the EMT <7 mm group exhibited significantly lower rates of biochemical pregnancy, clinical pregnancy, and live birth (Table 4), consistent with prior evidence linking thinner endometrium to reduced reproductive success.10,25 Thin endometrium has also been associated with adverse obstetric outcomes, possibly due to abnormal placentation.26 Our unmatched analysis (Table 5) showed significantly higher rates of gestational diabetes, PAS, and preterm birth in the EMT <7 mm group. After PSM, gestational diabetes, preterm birth, and low birth weight remained significantly more frequent, whereas the difference in PAS incidence was no longer significant.
EMT is a key determinant of ART success, but the optimal threshold after TCRA remains uncertain, particularly for preventing life-threatening complications such as PAS. Several studies have reported varying EMT thresholds for PAS risk following FET. D.J. Kaser et al identified EMT <9 mm as a risk factor,27 while D.A. Carusi et al found significantly higher PAS incidence (16% vs. 3.8%) with EMT <6 mm.28 S. Matsuo et al reported an association with EMT <8 mm,22 and Lai et al concluded that EMT <7 mm is an independent risk factor, with PAS incidence decreasing by 32% per 1 mm increase in EMT ≤10.9 mm.29 We tentatively reanalyzed the data using alternative cutoff values (6, 6.5, 7.5, and 8 mm) (Supplementary Tables 1–7 and Table 6), and found that achieving an EMT of at least 8 mm prior to embryo transfer may effectively reduce the risk of PAS. Thus our exploratory findings suggest a potential threshold around 8 mm. These discrepancies may reflect differences in study populations, ethnicities, and sample sizes.
Unlike prior studies that often compared obstetric outcomes between IUA and non-IUA patients, our work focused specifically on patients undergoing IVF/ICSI-ET after TCRA, offering both a complement and innovation to existing literature. A key strength is the use of PSM to rigorously match groups by EMT. After matching, baseline characteristics and IVF indicators were well balanced, reducing confounding and strengthening the reliability of our comparisons.
Limitations
However, our study has several limitations that need to be acknowledged. Firstly, as a single-center retrospective analysis, although PSM-based case-control analysis was performed to increase the robustness and credibility some extent in this study, the bias could not be overcome entirely. Secondly, PAS diagnosis was not uniformly confirmed by histopathology in all cases; some cases relied on intraoperative findings, which may lead to misclassification. Consequently, the generalizability of our results to other populations (eg., different ethnicities, ART protocols, or surgical techniques) requires further investigation. Multicenter, prospective studies with prespecified hypotheses are needed to validate our findings.
It should be emphasized that the association between EMT <8 mm and increased PAS risk emerged from exploratory analyses testing multiple cutoffs (6, 6.5, 7, 7.5, 8 mm). The primary analysis using the prespecified 7 mm cutoff did not show a statistically significant difference in PAS incidence after PSM (29.7% vs. 20.2%, P=0.239). Therefore, the 8 mm threshold should not be interpreted as a definitive clinical cutoff for PAS prevention. Rather, our findings suggest a potential trend that thicker endometrium (≥8 mm) might confer lower PAS risk, but this hypothesis needs confirmation in larger, ideally prospective, multicenter studies. Clinicians should consider the totality of evidence, including patient-specific risk factors such as IUA severity and number of prior TCRA procedures, rather than relying solely on a single EMT threshold.
Conclusion
In conclusion, EMT and moderate-to-severe IUA were identified as independent risk factors for PAS in patients undergoing IVF/ICSI-ET after TCRA. An EMT <7 mm was associated with significantly lower live birth rates and higher incidences of several adverse obstetric outcomes. Exploratory analyses using multiple EMT cutoffs suggested that an EMT <8 mm might be associated with an increased PAS risk, although this finding was not prespecified and did not remain significant for the 7 mm cutoff after PSM. Given the single-center retrospective design, these associations should not be interpreted as causal. The optimal EMT threshold for PAS prevention remains uncertain, and our findings should be considered hypothesis-generating. Future prospective, multicenter studies are needed to validate whether achieving an EMT ≥8 mm before embryo transfer reduces PAS risk in this high-risk population.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine (No2026-2002).
Acknowledgment
The study has not been published before and is not under consideration for publication anywhere else. Its publication has been approved by all co-authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Zhejiang Province Traditional Chinese Medicine Co-construction Science and Technology Plan Project [GZY-ZJ-KJ-23028],“Pioneer” and “Leading Goose” R&D Program of Zhejiang[2023C03033] and The Zhejiang Province Leading Goose Program[2026C02A1118].
Disclosure
The authors declare no competing interests in this work.
References
1. Gilman AR, Dewar KM, Rhone SA, et al. Intrauterine adhesions following miscarriage: look and learn. J Obstet Gynaecol Can. 2016;38(5):453–12. doi:10.1016/j.jogc.2016.03.003
2. Takai IU, Kwayabura AS, Ugwa EA, et al. A 10-year review of the clinical presentation and treatment outcome of asherman’s syndrome at a center with limited resources. Ann Med Health Sci Res. 2015;5(6):442–446. doi:10.4103/2141-9248.177984
3. Hooker AB, Lemmers M, Thurkow AL, et al. Systematic review and meta-analysis of intrauterine adhesions after miscarriage: prevalence, risk factors and long-term reproductive outcome. Hum Reprod Update. 2014;20(2):262–278. doi:10.1093/humupd/dmt045
4. Yang X, Liu Y, Li TC, et al. Durations of intrauterine balloon therapy and adhesion reformation after hysteroscopic adhesiolysis: a randomized controlled trial. Reprod Biomed Online. 2020;40(4):539–546. doi:10.1016/j.rbmo.2019.11.017
5. Shi X, Saravelos SH, Zhou Q, et al. Prevention of postoperative adhesion reformation by intermittent intrauterine balloon therapy: a randomised controlled trial. BJOG. 2019;126(10):1259–1266. doi:10.1111/1471-0528.15843
6. Jauniaux E, Collins S, Burton GJ. Placenta accreta spectrum: pathophysiology and evidence-based anatomy for prenatal ultrasound imaging. Am J Obstet Gynecol. 2018;218(1):75–87. doi:10.1016/j.ajog.2017.05.067
7. Munro MG. Uterine polyps, adenomyosis, leiomyomas, and endometrial receptivity. Fertil Steril. 2019;111(4):629–640. doi:10.1016/j.fertnstert.2019.02.008
8. Hong W, Wu Z, Li L, et al. Intrauterine adhesions treated with hysteroscopic adhesiolysis and subsequent obstetric outcome: a retrospective matched cohort study. BJOG. 2025;132(2):155-164. doi:10.1111/1471-0528.17793
9. Kasius A, Smit JG, Torrance HL, et al. Endometrial thickness and pregnancy rates after IVF: a systematic review and meta-analysis. Hum Reprod Update. 2014;20(4):530–541. doi:10.1093/humupd/dmu011
10. Baradwan S, Alharbi D, Bashir MS, et al. Short and long-term reproductive outcomes after hysteroscopic adhesiolysis for infertile women. JBRA Assist Reprod. 2023;27(2):191–196. doi:10.5935/1518-0557.20220016
11. ACOG Committee Opinion No. 734: the Role of Transvaginal Ultrasonography in Evaluating the Endometrium of Women With Postmenopausal Bleeding. (2018). Obstetrics Gynecol. 2018;131(5):e124–e129. doi:10.1097/AOG.0000000000002631
12. Lundin K, Ahlstrom A. Quality control and standardization of embryo morphology scoring and viability markers. Reprod Biomed Online. 2015;31(4):459–471. doi:10.1016/j.rbmo.2015.06.026
13. Medicine ASIR. Alpha Scientists In Reproductive. M. The Alpha consensus meeting on cryopreservation key performance indicators and benchmarks proceedings of an expert meeting. Reprod Biomed Online. 2012;25(2):146–167. doi:10.1016/j.rbmo.2012.05.006
14. Jauniaux E, Ayres-de-Campos D, Langhoff-Roos J, et al. FIGO classification for the clinical diagnosis of placenta accreta spectrum disorders. Int J Gynecol Obstet. 2019;146(1):20–24. doi:10.1002/ijgo.12761
15. Hecht JL, Baergen R, Ernst LM, et al. Classification and reporting guidelines for the pathology diagnosis of placenta accreta spectrum (PAS) disorders: recommendations from an expert panel. Mod Pathol. 2020;33(12):2382–2396. doi:10.1038/s41379-020-0569-1
16. Jauniaux E, Chantraine F, Silver RM, et al. FIGO consensus guidelines on placenta accreta spectrum disorders: epidemiology. Int J Gynaecol Obstet. 2018;140(3):265–273. doi:10.1002/ijgo.12407
17. Jauniaux E, Bunce C, Grønbeck L, et al. Prevalence and main outcomes of placenta accreta spectrum: a systematic review and meta-analysis. Am J Obstet Gynecol. 2019;221(3):208–218. doi:10.1016/j.ajog.2019.01.233
18. Tavcar J, Movilla P, Carusi DA, et al. Incidence and clinical implications of placenta accreta spectrum after treatment for asherman syndrome. J Minim Invasive Gynecol. 2023;30(3):192–198. doi:10.1016/j.jmig.2022.11.013
19. Zhang LP, Wang M, Shang X, et al. The incidence of placenta related disease after the hysteroscopic adhesiolysis in patients with intrauterine adhesions. Taiwan J Obstet Gynecol. 2020;59(4):575–579. doi:10.1016/j.tjog.2020.05.018
20. Sugai S, Yamawaki K, Sekizuka T, et al. Pathologically diagnosed placenta accreta spectrum without placenta previa: a systematic review and meta-analysis. Am J Obstet Gynecol MFM. 2023;5(8):101027. doi:10.1016/j.ajogmf.2023.101027
21. Jwa SC, Tamaru S. Takamura M.et al.Assisted reproductive technology-associated risk factors for placenta accreta spectrum after vaginal delivery. Sci Rep. 2024;14(1):7454. doi:10.1038/s41598-024-57988-x
22. Matsuo S, Kotani T, Tano S, et al. Risk factors for non-previa placenta accreta spectrum in pregnancies conceived through frozen embryo transfer during a hormone replacement cycle in Japan. Reprod Med Biol. 2024;23(1):e12592. doi:10.1002/rmb2.12592
23. Holden EC, Dodge LE, Sneeringer R, et al. Thicker endometrial linings are associated with better IVF outcomes: a cohort of 6331 women. Hum Fertil. 2018;21(4):288–293.=–292.712. doi:10.1080/14647273.2017.1334130
24. Zhong Y, Zeng F, Liu W, et al. Acupuncture in improving endometrial receptivity: a systematic review and meta-analysis.BMC. Complement Altern Med. 2019(19):61. doi:10.1186/s12906-019-2472-1
25. Liao Z, Liu C, Cai L, et al. The effect of endometrial thickness on pregnancy, maternal, and perinatal outcomes of women in fresh cycles after ivf/icsi: a systematic review and meta-analysis. Front Endocrinol. 2021;12:81464. doi:10.3389/fendo.2021.814648
26. Oron G, Hiersch L, Rona S, et al. Endometrial thickness of less than 7.5 mm is associated with obstetric complications in fresh IVF cycles: a retrospective cohort study. Reprod Biomed Online. 2018;37(3):341–348. doi:10.1016/j.rbmo.2018.05.013
27. Kaser DJ, Melamed A, Bormann CL, et al. Cryopreserved embryo transfer is an independent risk factor for placenta accreta. Fertil Steril. 2015;103(5):1176–84e2. doi:10.1016/j.fertnstert.2015.01.021
28. Carusi DA, Gopal D, Cabral HJ, et al. A risk factor profile for placenta accreta spectrum in pregnancies conceived with assisted reproductive technology. F S Rep. 2023;4(3):279–285. doi:10.1016/j.xfre.2023.05.004
29. Lai S, Zhang L, Luo Y, et al. A sonographic endometrial thickness <7 mm in women undergoing in vitro fertilization increases the risk of placenta accreta spectrum. Am J Obstet Gynecol. 2024;231(5):557.e1-557.e18. doi:10.1016/j.ajog.2024.02.301
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.