Back to Journals » Patient Preference and Adherence » Volume 12
Factors affecting patient and nursing staff adherence to an integrated physical activity and nutritional intervention targeting functional decline on an acute medical ward: a qualitative study
Authors Andreasen J, Soendergaard LN, Holst M
Received 15 March 2018
Accepted for publication 29 May 2018
Published 10 August 2018 Volume 2018:12 Pages 1425—1435
DOI https://doi.org/10.2147/PPA.S168193
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Jane Andreasen,1,2 Lise Noerregaard Soendergaard,3 Mette Holst4
1Department of Physical and Occupational Therapy, Aalborg University Hospital, Aalborg, Denmark; 2Public Health and Epidemiology Group, Department of Health, Science and Technology, Aalborg University, Alborg, Denmark; 3Department of Health Promotion, Aalborg University Hospital, Aalborg, Denmark; 4Center for Nutrition and Bowel Disease, Department of Gastroenterology, Aalborg University Hospital, Aalborg, Denmark
Background: Medical patients are particularly at risk of developing complications during and after hospitalization, due to impaired nutritional intake, physical inactivity, or immobilization. Evaluations of implementation studies on health-promoting interventions for medical patients in hospitals are scarce. The aim of this study was to identify factors affecting the adherence of patients and staff to an integrated physical activity and nutritional intervention on a medical ward.
Methods: Two focus group interviews were conducted: one with patients and another with staff. Three individual telephone interviews were conducted, as three patients were not available at the time of the group interview. An inductive thematic analysis was fundamental to the findings of the study.
Findings: Nine themes describe factors affecting adherence to integrated physical activity and nutrition intervention. Positive factors described by the patients were new knowledge and insight, and that they felt seen and believed in, which made a significant difference to their motivation. The nursing staff felt that the intervention provided important knowledge related to daily practice, prevented bad consciences due to time issues, and that they experienced happier and more active patients. Both staff and patients found that the approaches of the physiotherapist and the dietician positively changed their behavior, however staff members experienced limited resources as a barrier, and a lack of knowledge seemed to hinder full integration of the intervention. Patients reported that their illness situation, “being on their own,” and failure to negotiate a shared goal with the project staff were barriers to adherence.
Conclusions: Both the nursing staff and patients described positive experiences with the integration of a multifaceted health promotion intervention on physical activity and nutrition, however the nursing staff did not fully participate in the intervention and patient adherence differed; particularly, it tended to diminish when the patients were expected to act on their own.
Keywords: qualitative study, focus group interview, physical activity, nutrition, medical ward, barriers and facilitators, nursing staff and patients
Introduction
Physical inactivity, impaired nutritional intake and the environment in the hospital ward are potential risk factors that can lead to hospitalization-associated functional decline after discharge.1–3 Functional decline may lead to post-hospitalization-associated disability. Hospitalization-associated disability is a serious condition which may, among other things, lead to institutionalization, poor quality of life, and death.4 Medical patients are particularly at risk of developing complications during and after hospitalization, due to old age, impaired nutritional intake, physical inactivity, and prolonged immobilization. Medical patients, even patients who can walk independently, spend, on an average, more than 80% of their hospital stay in bed.5 In hospitals, however, the ambulation and physical activity of medical patients seems to be of low priority in practice, perhaps even lower than patient nutrition intake.6–10
Older hospitalized patients had positive expectations of the exercises during hospitalization, but only a few actually exercised, because staff rarely addressed the issue and the patients lacked support and encouragement.10–12 A study by Casey,13 showed that nurses had a primarily disease-oriented approach to patients and that health promotion occurred infrequently and was only sometimes added if a nurse had time.13 The barriers to implementing mobility and physical activity interventions are generally reported to be of limited time and competence, along with a lack of patient motivation and resources, according to staff personnel.12,14 Patients report symptoms and illness, a lack of staff to assist, and fear of falling as barriers to being physically active.9–12 There is established evidence that physical activity5–18 and nutritional interventions in hospitalized medical patients are important elements in preventing functional decline and nutritional risk status in medical in-patients.19–22 Furthermore, mobilization and physical activity not only seem to be beneficial for physical function, but also for psychological and social outcomes for the patients, and beneficial organizational outcomes are reduced length of stay, mortality rates, and costs.18 Evidence suggests that a multifaceted and multidisciplinary strategy is desirable4,14 and individual exercise recommendations, encouragement and the education of staff are recommended.23 Reduced mobility and subsequent potential functional decline will cause serious consequences for both individuals and for society in general. Due to demographic developments, there is a rapidly increasing number of, and therefore more hospitalized, older people, and there is therefore an increasingly challenging economic burden to society. It is thus important to design, test and evaluate interventions targeting physical activity and nutritional status on several levels, including patients, staff, and organizational and environmental levels, to accommodate the serious challenges of functional decline in older medical patients during hospitalization.2,5,24 The “Training and Eating for Medical Patients study” (TEMP)25 was developed using an ecological framework14 to ensure a tailor-made approach to the specific setting in order to improve the functional and nutritional status of patients, and to develop ward culture in relation to physical activity and nutrition. Generally, the patient outcomes were positive and statistically and clinically significant for physical activity measures, the fulfilling of daily protein and energy requirements, and health-related quality of life for the group of patients with functional decline on the time of inclusion.25 However, there was registered substantial variety regarding funtional improvements within the included patients. The TEMP intervention was developed in collaboration with ward staff and the management. Experiences from this study will therefore provide new and important knowledge about preferences and adherence, from both patient and staff perspectives, on a multi-faceted and integrated intervention. Identifying factors that affect adherence to the intervention, again from both a patient and a staff perspective, is crucial to improving future evidence-based initiatives targeting functional decline in acutely admitted medical patients, as well as for obtaining knowledge of how to successfully implement health-promoting interventions regarding physical inactivity and impaired food intake in an acute hospital context.
Aim
The aim of this study was to identify positive and negative factors affecting the adherence of patients and staff to an integrated physical activity and nutritional intervention on a medical ward.
Methods
Setting
An investigator-developed intervention (TEMP) was initiated over a 10-month period at a medical ward specializing in infectious diseases in a Danish University Hospital. The aim of the intervention was to be closely integrated into the daily activities on the ward, and it consisted of four core elements: teaching nursing staff to acquire knowledge and competences in relation to mobilization, physical activity and nutrition; advising staff about nutritional advice and physical activity targeting individual patients when needed; Intervention A for patients with functional decline or nutritional risk, and Intervention B for patients with minimal functional decline and no nutritional risk. Prior to the onset of the intervention, the Steering Group for Health Promotion Management at the Hospital, the lead ward physician, and the lead nurse, approved and agreed that resources were used to educate staff and to prepare the intervention. Prior to the commencement of study, a dialog was established with members of the nursing staff to identify potential barriers to implementing new routines regarding physical activity and nutrition. Nudging environmental initiatives were arranged on the ward, including distance markers in the hall for ambulation purposes; exercise bicycles, pamphlets, pedometers, and exercise equipment were provided; and protein-enriched drinks were easily accessible for all patients. A physiotherapist and a dietician were employed for 30 and 10 hours a week, respectively, to exercise and advise patients and provide individualized exercise programs and diet plans, to educate and counsel the staff, and, overall, to be supportive and establish a health-promoting culture on the ward (Figure 1). Adherence to the intervention was defined as good if the patients performed their individualized program by themselves once a day in the afternoon or evening and afterwards had a protein-rich drink, and also at least once a day at the weekends. At home they were advised to undertake their training program followed by a protein-rich drink at least once a day. The findings regarding the quantitative outcome measures of patients included in Intervention A have previously been published.25
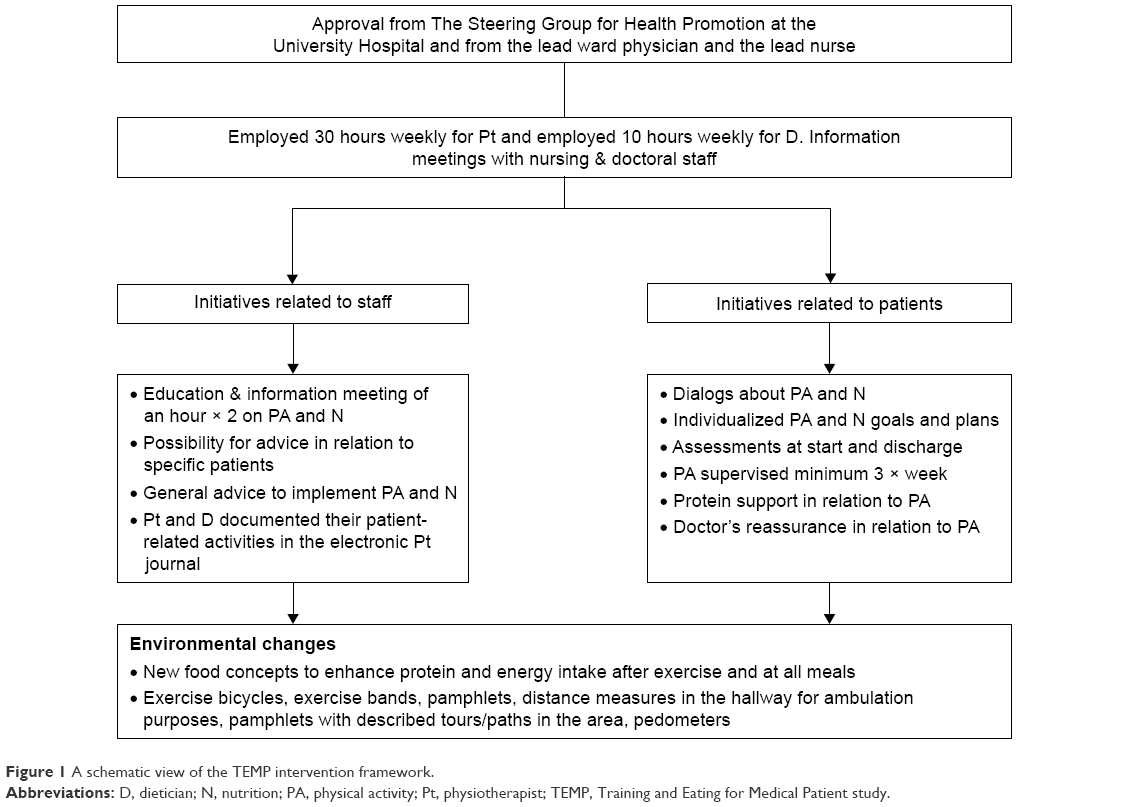 | Figure 1 A schematic view of the TEMP intervention framework. |
Study design, participants, and data collection
This study was a qualitative study and data was gathered using semi-structured interviews.26 Two focus group interviews were conducted to reveal in-depth knowledge of how patients and nursing staff experienced and participated in the intervention. Focus group interviews are considered useful as an evaluative tool. Data can be obtained in a group where the environment can make the participants feel safe in sharing and discussing information, and thus provide important data.27,28 Three individual telephone interviews were also performed, as three participants were not able to attend the focus group interview.
A purposive sampling was used to include patients and staff. A wide range of diagnoses and demographic characteristics were sought in order to represent nuances to facilitate a sufficient richness of data from patients. The inclusion criteria was participation in Intervention A on the ward for more than three days. Exclusion criteria were terminal illness, cognitive impairment, and language other than Danish. Fifteen patients were contacted by mail ~3 months after discharge with information about the study. The rationale for performing the interviews at 3 months was to interview the staff following a period of time after intervention had ended at the ward, to allow them to reflect on the differences. The rationale was to interview the patients after they had been at home for a while, to allow them to reflect on their ability to adhere to the intervention after discharge. They were asked to contact the researcher (MH) on the phone if they accepted the invitation. Seven patients agreed, however three were not able to attend the focus group interview and, therefore, three individual interviews were performed. The seven patients who were interviewed had a length of stay on the specific ward between five and 16 days. Some of the patients were admitted to other wards before their admission to the infectious medical ward.
A purposive sampling of staff was conducted to ensure differences in experience. The staff members were contacted through email correspondence, and five agreed to participate. The characteristics of the participants are presented in Table 1.
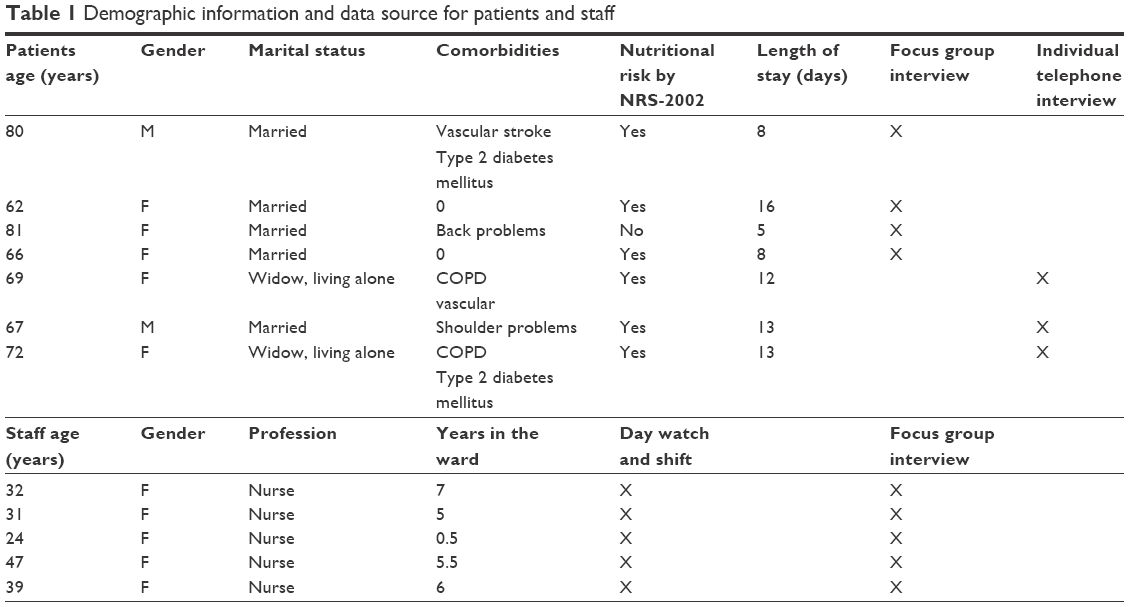 | Table 1 Demographic information and data source for patients and staff |
The focus group interviews lasted 1½ hours each, and each individual interview lasted ~30 minutes. One researcher and a research assistant performed the focus group interviews and functioned as moderator and moderator’s assistant to ensure a focused discussion.28 The moderators had not been actively involved in the interventions on the ward. The focus group interviews took place in a quiet, non-clinical room at the University Hospital and beverages were provided. The semi-structured interview guide (Table 2) was topic-based.26 Both focus group interviews were audiotaped and fully transcribed verbatim immediately afterwards. The individual interviews were audiotaped and the relevant parts of each interview were transcribed and included in the data analysis.
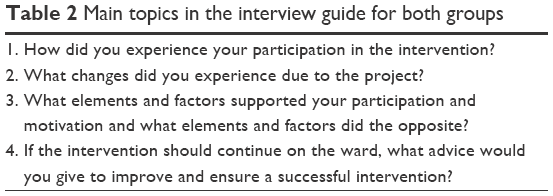 | Table 2 Main topics in the interview guide for both groups |
Data analysis
A six-step data-driven thematic analysis was used to analyze the data, as recommended by Braun and Clark.29–31 Firstly, initial readings of both focus group interviews and individual transcriptions were performed in order to familiarize ourselves with the data. Thereafter, we generated initial codes, and identified and reviewed themes. Themes were then defined and named, and, finally, the results were reported. An iterative approach was used to qualify the findings. All authors were involved in the analytical process and differences were solved by rereading, reanalysis and dialog.
Ethics
The Regional Ethics Committee, Denmark, confirmed that no approval was necessary according to Danish Law. The study was approved by the Danish Data Protection Agency (number 2008-58-0028). All participants were given written and oral information regarding the study before informed verbal consent was obtained from all participants. The consent was audiotaped at the beginning of the interviews. Confidentiality and anonymity was ensured and it was emphasized that the participants could withdraw their consent at any time without excuse or consequences for further care.
Results
The analyses resulted in nine themes in total: five themes describing factors that affected adherence to the intervention positively, and four themes describing factors that negatively affected adherence. A summary of the findings is presented in Table 3. Quotations are used to describe and validate the findings.
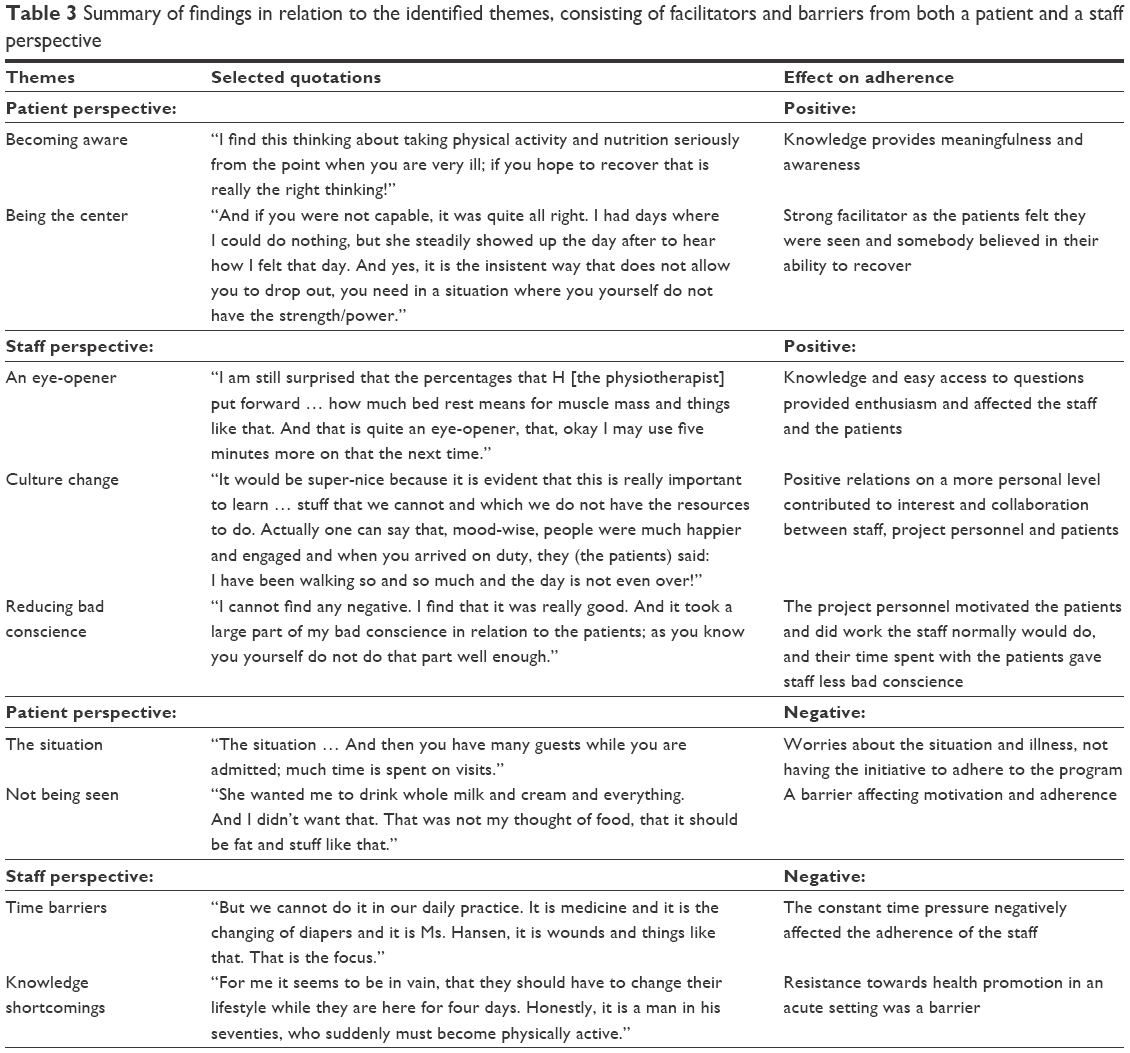 | Table 3 Summary of findings in relation to the identified themes, consisting of facilitators and barriers from both a patient and a staff perspective |
Positive factors affecting adherence
Patients
The Becoming Aware theme describes how the patients experienced the intervention as meaningful, with a positive impact on their health, and they expressed an understanding of the importance of the initiative. “I find this thinking about taking physical activity and nutrition seriously from the point when you are very ill; if you hope to recover, that is really the right thinking!” The training and the insights from testing gave the patients a new awareness of their physical health condition. “She was outreach and explaining her instructions so that I, myself, became aware of my strengths and my weaknesses.” The patients reported that proteins were strongly emphasized by the dietician and felt the options given by the dietician had a great impact. “She came with all the different nutritional supplement options there were in the hospital and so forth, which was really good for me to gain my strength.”
The expectation and experience of improving health was encouraging and a plan for physical activity, or nutritional intake, or both, encouraged effort and enforced adherence, and being tested provided concrete signs of improvement. “There were a lot of tests we had to go through. Then on a scale from one to a hundred we were assessed to see what we were capable of. And then we had that (test) again when we were finally discharged to see how far we had moved (on the scale).” None of the participants described any deep insight into why and how this intervention was important to their illnesses and health.
The Being the Center theme describes how the patients felt they were seen as individuals and how they were supported and acknowledged for their efforts and gains. One patient had found it really difficult to eat correctly, as she suffered from diabetes, COPD, and was overweight. With guidance from the dietician, she felt that her conditions were taken into consideration and that they both appreciated the result. “In the end, we finally found a drink (nutritional supplement) that I think was really good – one of those energy things. I had it twice a day for the last 14 days. I was quite proud, and so was she.” This individualized approach was very motivating and it became clear that relationships with the physiotherapist and the dietician were a cornerstone of patient adherence to the programs and goals. “At the time it felt as if this was just for me. And that I am the center and this is the only important thing.” The patients knew that they sometimes needed a “push” otherwise they would easily become inactive. The physiotherapist was described as encouraging and persistent, but with feelings and understanding. “It was the good way she took a hold of it – by being a little insistent without being uncomfortably forceful.” The environment on the ward was described as facilitating, for instance with exercise bicycles, and the marked ambulation routes in the hallway. The delicacy wagon was also a facilitating element, which contained all the foods that the dietician had recommended. “It is pure luxury. Even if you had no appetite. Because it was all so small, a tiny cream bun, a tiny cheese pie that was just made, well, it was simply amazing and manageable. I could eat it despite otherwise having no appetite at all.” Overall, the patients felt that the project staff saw them as individuals, and patience and steadiness were emphasized as important. “And if you were not capable, it was quite all right. I had days where I could do nothing, but she steadily showed up the day after to hear how I felt that day. And yes, it is the insistent way that keeps you from dropping out; you need in a situation, where you yourself don’t have the strength.”
Nurses
The An Eye-Opener theme describes how the nursing staff felt that the project provided insight and understanding concerning patient nutrition and physical activity and how the insight changed their behavior in daily practice. The physiotherapist and dietician provided new insights, which changed their focus from preventing complications to promoting healthy options regarding physical activity and nutrition. “I am still surprised that the percentages that H (the physiotherapist) put forward … how much bed rest means for muscle mass and things like that. And that is quite an eye-opener, that, okay I may use five minutes more on that the next time.” The staff gained a new understanding of the competencies of the physiotherapist and the dietician, and felt they could ask for advice and knowledge at any time. “Knowing that the whole ward has access to somebody who has other information than we normally use, that really makes a huge difference. We really benefitted from the multidisciplinary approach.” A nurse described that she felt competent in a more health-promoting role. “They were always very helpful for continuously following up on issues if you had any questions. I felt well-equipped to take care of what I should in relation to the collaboration.”
The Culture Change theme shows how the nurses interviewed found there were several elements in the project that improved the culture in the ward. They were very positive and emphasized that a lack of meaningful activities for the patients was no longer an issue. “The period of stay at the hospital did not seem quite as long either, you know, because there was actually something for the patients to do instead of staying in bed.” The nursing staff experienced the way in which patients were motivated and participated in the interventions, and saw how the patients built a strong relationship with both the project staff and with other patients as they competed in a constructive manner. The nurses felt that the culture on the ward changed. “But it is also very much about the social element. If we sometimes have patients that “click” with each other, then they compete a little – for instance when using the bicycle.” Finally, they felt the whole atmosphere on the ward changed and the staff wished the intervention would become permanent as it clearly had a positive impact on the patients, the staff and the culture of the ward. “It would be super-nice because it is evident that this is really important to learn … stuff that we cannot do, and for which we do not have the resources. Actually, one can say that, mood-wise, people were much happier and engaged, and when you arrived on duty, they (the patients) said: I have been walking so and so much and the day is not even over!”
Reducing Bad Conscience describes how the intervention reduced the bad conscience nurses normally had in relation to patients, and this was therefore a positive factor for adherence. The project personnel reduced the bad conscience of the nurses as they performed tasks that were normally their responsibility, such as nutritional risk screenings and documentation. “I cannot find anything negative. I find that it was really good. And it took away a large part of my bad conscience in relation to the patients; as you know that you yourself do not do that part well enough.” The nursing staff also emphasized that the presence of the physiotherapist and the dietician, and the related documentation was important, as presence is the key to high collaboration and adherence. “They were very much present, the dietician and the physiotherapist. That worked really well. That you could talk with them. They were visible. But also … they themselves wrote in “Clinical” (the electronic patient journal). This was pleasant for us, as we always could read what was agreed on with the patients.” The nursing staff described the patients as taking responsibility for their activities and that their own involvement in the daily schedule in relation to the intervention for the patients was minor.
Negative factors affecting adherence
Patients
The Situation describes how the patients felt that their illness and related circumstances had a negative impact on adherence to the intervention. They did not proceed with the self-training program or ambulation, or the protein supplementation in the evenings and at weekends. Visitors, illness, and impaired physical condition were considered great barriers to performing exercises after daytime routines in the hospital. “The situation … And then you have many visitors while you are admitted; much time is spent on visits.” Barriers that decreased adherence to the intervention program were, in particular, reported in relation to the presence or absence of the physiotherapist as having somebody to guide you, which was considered important in order to ensure continued adherence. One patient reflected on hospital admissions and the lack of meaningful activities that normally characterize patient life at a hospital ward. “The easiest is to just stay in bed. Otherwise, you tend to feel a little homeless and just walk about a bit. So the bed is where you are housed.”
Not Being Seen reflects how a mismatch in individual targeting decreased patient adherence and motivation. This is illustrated by one patient, who did not find that the dietary advice was beneficial to her. She did not agree on the defined goals and did not understand the dietician’s approach to making her regain the weight she lost during her illness. “She wanted me to drink whole milk and cream and everything. And I didn’t want that. That was not my idea of food – that it should be fat and stuff like that.” At an organizational level, the patients felt that the staff, including the physicians, did not generally take an active part in the intervention or support the patients, or give them incentive to do so. When asked if the doctors and subsequently the nurses had been involved in the intervention, a patient replied. “No I did not experience that. They (the physicians) expected they had people that took care of that … And they [the nursing staff] actually had enough to do. So I don´t at all think they have the capacity to manage that part as well.”
Nurses
Nursing staff repeatedly mentioned Time Barriers as a factor that continually affected their own motivation and adherence to the intervention for health-promoting practice barriers. The nurses felt that their daily tasks on the ward were numerous and they were forced to prioritize. “But we cannot do it in our daily practice. It is medicine and it is the changing of diapers and it is Ms. Hansen, it is wounds and things like that. That is the focus.” This prioritization affected the nurses negatively and had consequences on their relationship with the patients. “But it is because, if you do not have the time to listen to what they (the patients) say, then you stand there tripping over yourself to get away again. You actually wish that they don´t ask about too much.”
The Knowledge Shortcomings theme addressed the feeling of not having adequate knowledge and competence in relation to the implementation of the intervention in daily practice. The organizational practice and culture experienced in the ward made one nurse emphasize, repeatedly, that it was the nurses who had to change their routines so everybody else would be satisfied. “I don’t think that we should find that it is the nurses once again, who have to learn something. I can get a little tired of that.” The nurses did not feel competent or capable of arguing or informing the patients about the importance of the intervention. “But we do have the; this is important because of this and this and this..., we do not at all have that knowledge.” Finally, a fundamental understanding of the importance of health promotion seemed lacking, as illustrated by a nurse stating that it was a misunderstanding that the staff are required to practice health promotion, since the patients have an entire life at home and only a few days at the hospital. “For me, it seems to be in vain, that they should have to change their lifestyle while they are here for 4 days. Honestly, it is a man in his seventies, who suddenly must become physically active.”
Discussion
The findings of this study showed various factors affecting adherence to an integrated physical activity and nutrition intervention on an acute medical ward. The patients described mixed experiences. Factors that contributed to their adherence to the intervention during admission were that they gained useful knowledge and insight, although they did not explore an in-depth understanding. They also felt seen and believed in as individuals, which made a huge difference for their motivation. The nursing staff felt that the intervention provided important knowledge regarding physical inactivity and nutrition issues related to daily practice, prevented bad conscience due to time issues, and that they encountered more active and happier patients. The personnel also appreciated the opportunity for professional advice regarding patients. Both staff and patients found that the forthcoming and positive approach from the physiotherapist and the dietician facilitated their motivation and changed their behavior, however staff members found limited resources and knowledge to be barriers, which seemed, as previously reported, to hinder a full integration of the intervention into daily practice.12,32 Patients reported that their illness situation, “being on their own” and failure to negotiate a shared goal with the project staff were barriers to their adherence, which, to some extent, has again been previously reported.5,12,32
Even though there was consensus about, and prioritization of, the study from the nurse and physician in charge of the ward prior to intervention, there seemed to be relatively low active engagement during the process. The peripheral involvement of the staff and doctors may have had negative consequences for patient adherence to physical activity and nutritional intake. The key element for the patients was encouragement and supervision from the project staff, and the patients did not perform self-training in the evenings and weekends where the ward staff was supposed to encourage them. Doctors seem to have a strong influence over the exercise behavior of older patients, but addressed the issue infrequently.11 In our study, it seemed that the patients continuously needed external feedback and support, especially when the project staff were absent. Older medical patients are often frail and are generally a vulnerable group that may need continuous support in order to be physically active and eat sufficiently. Peripheral involvement may have long-term consequences, as 47% of hospitalized patients aged 65 years or more are not in contact with the primary health care sector after discharge.33 This adds to the importance of a physical activity and nutrition intervention such as TEMP at hospitals. Recent studies show that such an intervention may have important impact on post-hospitalization function.3,18 King et al34 also used a framework to develop and implement a physical activity intervention. In their study, the nurses primarily described positive experiences regarding their participation. Although we also used a similar strategic and supportive approach, the nurses in our study had a mixed experience, especially of their own active involvement, which they found was outside their basic tasks, and not within reach during their limited time spent with the patients. The nursing staff were positive about the intervention, but felt that the health-promoting intervention was primarily a job for the project personnel, to which they contributed but did not have responsibility. Some even found a health-promoting practice to be somewhat pointless, as the patients were admitted for a short period only. Studies support these findings,13 including that nurses primarily did have a disease-oriented practice or were rarely directly involved in supporting a mobility plan for the patient.13,32 A recent qualitative study by Doherty-King and Bowers35 explored how nurses defined the ambulation of elderly inpatients within their responsibility of practice, or attributed the responsibility to another discipline, and found that both perspectives were present in daily practice. An important finding was that nurses who claimed responsibility for ambulation, focused on patient independence and psychosocial wellbeing.35 The nurses found that responsibility for conducting the intervention was placed on the project personnel. They expressed their belief that the activity and the wellbeing of the patients was very positive and important, however ownership of the intervention primarily appeared to stay with the project personnel; knowledge transfer and initiative transfer to the nurses did not seem to succeed as significantly as intended. This is a well-described and well-known issue when intervention protocols are implemented.35 A lack of in-depth knowledge may have the consequence that staff do not understand the importance of a continuous focus on the intervention elements, so that a key element of motivation is missing. On the other hand, it is important to acknowledge the experience of nursing staff that many elements and responsibilities were delegated into their daily practice as nurses, and that they therefore did not feel that it was possible or reasonable to expect them to achieve the skills that were the specific tasks of the project staff.
A balance between the level of challenge and the ability of the patient to manage the task was important. When facilitators such as goals and plans, instructions, time, and knowledge were apparent to both the nursing staff and the patients, they experienced success and a change in daily behavior was seen on the ward; but when these facilitators were missing, then the flow was disturbed. The main flow facilitator seemed to be the presence of, and instructions from, the project staff, especially the physiotherapist. The nursing staff expressed barriers such as time, competencies, and knowledge. Staff experiences with a new intervention have previously revealed that time issues, routine, and attitudes affect the implementation level of a new practice.12,37 This demonstrates that complex changes in practice are difficult, and that potential barriers exist at the levels of both patients and nursing staff, but also that the organizational and political context greatly affect the results, and thus the success of the implementation.13,14,36,38 Even though this project was approved and supported by hospital management, and was warranted by the ward and staff, there was no intervention planned that was directly focused on continuous leadership during the intervention phase. Retrospectively, a leadership focus might have improved adherence from all health professionals on the ward, including the physicians. Changes in an organization demand motivation, resources, competences, and the priority and focus of leadership.39 Finally, it may even be detrimental not to have a physical therapist and a dietician continuously involved in an organizational plan when integrating and implementing physical activity and nutrition on an acute medical ward. The MRC (Medical Research Council) argues that a stakeholder analysis may be beneficially performed before intervention. The present study, however, made no such analysis, and involving the leaders of the ward seemed to be insufficient to create ownership of the intervention, as indicated by the results of the present study.40 Leeman et al have developed a theory-based taxonomy of methods for implementing change in practice.41 Applying this taxonomy to the TEMP intervention reveals elements that were not consistently addressed in the present study, although an ecological framework was applied.14 These elements were an external change agent, an opinion leader, guidance from managers, and the designation of a change leader, which all are elements involved in the continual focus and leadership of the intervention.41
Clinical and research implications
It seems very important to thoroughly prepare and continuously support interventions on medical wards that target functional decline by implementing physical activity and nutritional interventions. It seems especially important to have a continuous leadership focus. It may be too optimistic to assume that an intervention can be integrated without continuous external support, as the patients did not adhere to it when they were on their own. The knowledge and initiative transfers to the staff on the ward also did not seem to succeed as intended.
More research is still needed in this complex area, especially regarding adherence to the aim of improving physical activity and nutritional intake on medical wards. Future research should focus on reducing the negative factors for the nursing staff as these may influence the functional levels of many future patients at discharge and beyond.
Methodological considerations
The participants interviewed met the predefined criteria, four of the 15 patients invited participated in the focus group, and three were interviewed by telephone. The character of the telephone interviews and therefore the information collected was different, and not optimal, as the patients did not participate in a group discussion and the face-to-face element was absent, however we found that this was an acceptable solution compared to the alternative of not having any information from these patients. Five staff members were interviewed. Krueger and Casey state that the ideal size of groups may be four to six participants when exploring a specific non-commercial topic, and this size is increasingly used when the aim is to share insights and experiences on specialized knowledge, which is in alignment with this study.13,28
The study was performed in a Danish University Hospital setting on a medical ward, and the findings may thus not be transferable to other settings or populations. A general limitation of qualitative designs is that a qualitative study is unique and highly dependent on the skills of the researcher, thereby also being difficult to replicate. To accommodate this, the analytical process was carried out by the entire group of authors to ensure agreement, and the findings were continually discussed. This rigorous process was performed and presuppositions were reflected upon while seeking to achieve trustworthy and credible findings.
In conclusion, a physical activity and nutrition intervention on an acute medical ward (TEMP) seems a constructive method for integrating a multifaceted health-promoting intervention towards physical activity and nutrition on a medical ward, although nursing staff and patients expressed both positive and negative experiences. The nursing staff did not fully take part in the intervention and patient adherence differed. In particular, it tended to diminish when the patients were required to perform on their own.
Acknowledgments
We thank Line Remmen, OT, MSc in Public Health for participating in focus group interviews and the transcription of interviews. The authors also thank the patients and staff at the Medical Department of Infectious Diseases, Aalborg University Hospital. The study was fully funded by Aalborg University Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
Brown CJ, Friedkin RJ, Inouye SK. Prevalence and outcomes of low mobility in hospitalized older patients. J Am Geriatr Soc. 2004;52(8):1263–1270. | ||
Admi H, Shadmi E, Baruch H, Zisberg A. From research to reality: minimizing the effects of hospitalization on older adults. Rambam Maimonides Med J. 2015;6(2):e0017. | ||
Zisberg A, Shadmi E, Gur-Yaish N, Tonkikh O, Sinoff G. Hospital-associated functional decline: the role of hospitalization processes beyond individual risk factors. J Am Geriatr Soc. 2015;63(1):55–62. | ||
Covinsky KE, Pierluissi E, Johnston CB. Hospitalization-associated disability: “She was probably able to ambulate, but I’m not sure.” JAMA. 2011;306(16):1782–1793. | ||
Brown CJ, Redden DT, Flood KL, Allman RM. The underrecognized epidemic of low mobility during hospitalization of older adults. J Am Geriatr Soc. 2009;57(9):1660–1665. | ||
Fisher SR, Goodwin JS, Protas EJ, et al. Ambulatory activity of older adults hospitalized with acute medical illness. J Am Geriatr Soc. 2011;59(1):91–95. | ||
Villumsen M, Jorgensen MG, Andreasen J, Rathleff MS, Mølgaard CM. Very low levels of physical activity in older patients during hospitalization at an acute geriatric ward: a prospective cohort study. J Aging Phys Act. 2015;23(4):542–549. | ||
Doherty-King B, Yoon JY, Pecanac K, Brown R, Mahoney J. Frequency and duration of nursing care related to older patient mobility. J Nurs Scholarsh. 2014;46(1):20–27. | ||
Holst M, Staun M, Kondrup J, Bach-Dahl C, Rasmussen HH. Good nutritional practice in hospitals during an 8-year period: the impact of accreditation. Espen J. 2014;9(4):e155–e160. | ||
Holst M, Hansen P, Pedersen L, Paulsen S, Valentinsen C, Kohler M. Physical activity in hospitalized old medical patients; how active are they, and what. J Aging Res Clin Pract. 2015;4(2). | ||
So C, Pierluissi E. Attitudes and expectations regarding exercise in the hospital of hospitalized older adults: a qualitative study. J Am Geriatr Soc. 2012;60(4):713–718. | ||
Brown CJ, Williams BR, Woodby LL, Davis LL, Allman RM. Barriers to mobility during hospitalization from the perspectives of older patients and their nurses and physicians. J Hosp Med. 2007;2(5):305–313. | ||
Casey D. Nurses, perceptions, understanding and experiences of health promotion. J Clin Nurs. 2007;16(6):1039–1049. | ||
Sallis JF, Owen N, Fisher EB. Ecological models of health behavior. In: Glanz K, Rimer BK, Viswanath K, editors. Health Behavior and Health Education. Theory, Research and Practice. 4th ed. San Francisco, CA: Jossey-Bass Public Health; 2008:465. | ||
de Morton NA, Keating JL, Jeffs K. Exercise for acutely hospitalised older medical patients. Cochrane Database Syst Rev. 2007;24(1):CD005955. | ||
Sullivan DH, Wall PT, Bariola JR, Bopp MM, Frost YM. Progressive resistance muscle strength training of hospitalized frail elderly. Am J Phys Med Rehabil. 2001;80(7):503–509. | ||
Kosse NM, Dutmer AL, Dasenbrock L, Bauer JM, Lamoth CJC. Effectiveness and feasibility of early physical rehabilitation programs for geriatric hospitalized patients: a systematic review. BMC Geriatr. 2013;13(1):107–2318. | ||
Kalisch BJ, Lee S, Dabney BW. Outcomes of inpatient mobilization: a literature review. J Clin Nurs. 2014;23(11–12):1486–1501. | ||
Johansen N, Kondrup J, Plum LM, et al. Effect of nutritional support on clinical outcome in patients at nutritional risk. Clin Nutr. 2004;23(4):539–550. | ||
Milne AC, Potter J, Vivanti A, Avenell A. Protein and energy supplementation in elderly people at risk from malnutrition. Cochrane Database Syst Rev. 2009;2:CD003288. | ||
Stratton RJ, Hébuterne X, Elia M. A systematic review and meta-analysis of the impact of oral nutritional supplements on hospital readmissions. Ageing Res Rev. 2013;12(4):884–897. | ||
Cawood AL, Elia M, Stratton RJ. Systematic review and meta-analysis of the effects of high protein oral nutritional supplements. Ageing Res Rev. 2012;11(2):278–296. | ||
So C, Pierluissi E. Attitudes and expectations regarding exercise in the hospital of hospitalized older adults: a qualitative study. J Am Geriatr Soc. 2012;60(4):713–718. | ||
Zisberg A, Gur-Yaish N. Older adults’ personal routine at time of hospitalization. Geriatr Nurs. 2017;38(1):27–32. | ||
Holst M, Søndergaard LN, Bendtsen MD, Andreasen J. Functional training and timed nutrition intervention in infectious medical patients. Eur J Clin Nutr. 2016;70(9):1039–1045. | ||
Kvale S, Brinkmann S. InterViews: Learning the Craft of Qualitative Research Interviewing. London: Sage; 2008. | ||
Onwuegbuzie AJ, Dickinson WB, Leech NL, Zoran AG. A qualitative framework for collecting and analyzing data in focus group research. Int J Qual Methods. 2009;8(3):1–21. | ||
Krueger RA, Casey MA, Groups F. A Practical Guide for Applied Research. 5th ed. London: Sage; 2015. | ||
Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. | ||
Coffey A, Atkinson P. Making Sense of Qualitative Data. London: Sage; 1996. | ||
Ritchie J, Lewis J. Qualitative Research Practice. London: Sage; 2003. | ||
Kneafsey R, Clifford C, Greenfield S. What is the nursing team involvement in maintaining and promoting the mobility of older adults in hospital? A grounded theory study. Int J Nurs Stud. 2013;50(12):1617–1629. | ||
Jan Christensen J, Fredslund EK. The shared older population (De fælles ældre): The National Institut of municipalities and regions analysis and research; 2014. Available from: https://www.kora.dk/media/2065748/10639_de_faelles_aeldre.pdf. Accessed July 26, 2018. | ||
King BJ, Steege LM, Winsor K, Vandenbergh S, Brown CJ. Getting patients walking: a pilot study of mobilizing older adult patients via a nurse-driven intervention. J Am Geriatr Soc. 2016;64(10):2088–2094. | ||
Doherty-King B, Bowers BJ. Attributing the responsibility for ambulating patients: a qualitative study. Int J Nurs Stud. 2013;50(9):1240–1246. | ||
Grol R, Wensing M. What drives change? Barriers to and incentives for achieving evidence-based practice. Med J Aust. 2004;180(6 Suppl):S57–S60. | ||
White JH, Alborough K, Janssen H, Spratt N, Jordan L, Pollack M. Exploring staff experience of an “enriched environment” within stroke rehabilitation: a qualitative sub-study. Disabil Rehabil. 2014;36(21):1783–1789. | ||
Ploeg J, Davies B, Edwards N, Gifford W, Miller PE. Factors influencing best-practice guideline implementation: lessons learned from administrators, nursing staff, and project leaders. Worldviews Evid Based Nurs. 2007;4(4):210–219. | ||
Aarons GA, Sommerfeld DH. Leadership, innovation climate, and attitudes toward evidence-based practice during a statewide implementation. J Am Acad Child Adolesc Psychiatry. 2012;51(4):423–431. | ||
Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Medical Research Council Guidance. Developing and evaluating complex interventions: new guidance. BMJ. 2008;29(337):a1655. | ||
Leeman J, Baernholdt M, Sandelowski M. Developing a theory-based taxonomy of methods for implementing change in practice. J Adv Nurs. 2007;58(2):191–200. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.