Back to Journals » Patient Preference and Adherence » Volume 17
Factors Affecting Immunosuppressive Medication Adherence in Liver Transplant Recipients with Poor Adherence: A Qualitative Study
Authors Ozdemir Koken Z ![]() , Sezer Ceren RE, Karahan S
, Sezer Ceren RE, Karahan S ![]() , Abbasoglu O
, Abbasoglu O
Received 23 November 2022
Accepted for publication 30 March 2023
Published 7 April 2023 Volume 2023:17 Pages 983—993
DOI https://doi.org/10.2147/PPA.S398770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zeliha Ozdemir Koken,1 Rana Elcin Sezer Ceren,1 Sabri Karahan,2 Osman Abbasoglu3
1Surgical Nursing Department, Hacettepe University Faculty of Nursing, Ankara, Turkiye; 2Surgical Nursing Department, Harran University, Faculty of Health Science, Sanliurfa, Turkiye; 3General Surgery Department, Hacettepe University Faculty of Medicine, Ankara, Turkiye
Correspondence: Zeliha Ozdemir Koken, Surgical Nursing Department, Hacettepe University Faculty of Nursing, Ankara, Turkiye, Email [email protected]
Purpose: Preserving graft functions and preventing rejection is closely related to immunosuppressive medication adherence in liver transplant recipients. Therefore, it is essential to determine factors affecting immunosuppressive medication use positively or negatively in liver transplant recipients. This study aimed to explore the use of immunosuppressive medication experience in liver transplant recipients with poor adherence and reveal the factors affecting the medication adherence.
Material and Methods: The study was conducted as a qualitative study with phenomenological approach. Seven adult liver transplant recipients were included in this study, who had poor adherence to immunosuppressive medication. Data was collected via in-depth personal interviews. Data analysis was conducted through inductive content analysis with three steps of preparation, organization, and reporting phases.
Results: Content analysis revealed four main categories, nine categories and 31 sub-categories. Four main categories emerged from the interview data: medication adherence perception, types of medication non-adherence, factors affecting medication adherence negatively and factors affecting medication adherence positively.
Conclusion: This study explored that there are several factors affecting immunosuppressive medication adherence among liver transplant recipients, both positively and negatively. In order to achieve liver transplant recipients’ total adherence to immunosuppressive medication, the factors affecting medication adherence positively and negatively should be understood. The study results are expected to contribute developing strategies to improve immunosuppressive medication adherence in liver transplant recipients.
Keywords: immunosuppressive, liver transplant, medication adherence, medication non-adherence
Introduction
Medication adherence refers to patients’ behavior of taking their medication according to the specifications set by health professionals. Non-adherence, on the other hand, is failing to take the medication in the correct dose, at the correct time and time intervals, skipping or delaying doses, or refusing the medication altogether.1–4 Medication non-adherence can be intentional or unintentional. Intentional non-adherence is a patient’s personal decision to refuse to follow the treatment. Unintentional non-adherence is a patient’s unwitting behavior, such as forgetfulness or carelessness.5,6
Factors affecting medication adherence have been reported as patient, health professional, and health system-related factors.1,4,5,7 The World Health Organization has defined patient-related factors affecting medication adherence as follows: the patient’s level of information and perception of the disease, the patient’s motivation to manage the disease and confidence in managing the disease, expectations from the treatment, information on possible consequences of non-adherence to medication, and failure to totally comprehend the effects of adherence to medication. Also, forgetfulness, stress, anxiety related to possible side effects, complexity of the treatment regime, inadequate motivation, lack of information and skill to manage treatment and disease symptoms, difficulty perceiving the necessity of the treatment, negative thoughts about the effectiveness of the treatment, failure to comprehend their illness or discern their diagnosis, low expectations from the treatment, negative thoughts about the healthcare team, and failure to keep up with follow-up appointments have been listed as other patient-related factors.4
Taking too many medications for a long period of time might cause medication non-adherence in liver transplant recipients. Liver transplant recipients are reported to have high rates of immunosuppressive medication non-adherence.8–10 Lieber et al reported 62% and Kung et al reported 50% immunosuppressive medication non-adherence among adult liver transplant recipients.8,9 The main purpose in the treatment and care of liver transplant recipients is protecting graft function and preventing complications, especially rejection. Achieving these goals is closely related to immunosuppressive medication adherence.11,12 With that in mind, exploring factors affecting liver transplant recipients’ immunosuppressive medication adherence positively or negatively is vital.13 This study aimed to explore the use of immunosuppressive medication experience in liver transplant recipients with poor adherence and the factors affecting the medication adherence. It is expected to contribute to the development of new strategies to improve immunosuppressive medication adherence in liver transplant recipients.
Materials and Methods
The phenomenological method was used in this study. The phenomenological method aims to explore and interpret experiences and comprehend their true nature.14–16 This study aimed to explore liver transplant recipients’ immunosuppressive medication experiences and reveal the factors affecting medication adherence. In-depth analysis with people who are experiencing immunosuppressive medication non-adherence is required to comprehend the factors leading to this phenomenon. Therefore, a phenomenological approach was used to reveal and understand liver transplant recipients’ experiences in depth regarding immunosuppressive medication adherence. In a phenomenological study, data is acquired by conducting interviews, examining written material, and making observations.15 In this study, data was acquired via in-depth personal interviews.
Participants
The study population consisted of adult patients who had undergone a liver transplant at a Liver Transplant Center in Turkiye. Seven liver transplant recipients over the age of 18 volunteered to participate. The participants in this study were selected via the purposive sampling method. Purposive sampling relies on selecting a sample of people that researchers want to explore, understand, and gain insight upon.17 Therefore, purposive sampling requires individuals who have experience with a particular phenomenon and some inclusion criteria.18 The purposive sampling criteria for this study were patients using immunosuppressive medication for at least three months and poor or non-adherence to immunosuppressive medication. Medication adherence is defined as “the extent to which patients take medications as prescribed by their healthcare providers”.4–7 Medication adherence is classified as complete non-adherence, partial adherence, and total adherence.19 Not taking the medication at all due to refusing the medication, constantly forgetting about their medication, and difficulty accessing medications is defined as complete non-adherence.19,20 Not taking the medication as prescribed due to changing the dose, skipping doses, or not taking the medication on time is defined as partial adherence.19,20 The views of patients and interviews with poor or non-adherent patients have been shown to be essential in providing insight into medication adherence.13 In the first phase of this study, we assessed the immunosuppressive medication adherence of 31 liver transplant recipients.21 We determined that 12 patients had poor medication adherence.21 Poor adherence in the form of skipping doses, delaying doses, and taking the medication early or late was determined in the study.21 Seven recipients out of 12, who agreed to participate, were included until the data saturation was reached in this study.
Data Collection
Data were collected between September 2019 and January 2020. Liver transplant recipients who were being followed at the Liver Transplant Center and had poor medication adherence21 were contacted, informed about the study, and invited to participate. Interview dates were set with the patients who agreed to participate. Interviews were conducted in person, in the researchers’ office. Two researchers were present in each interview: one leading the interview (ZOK; female, PhD, experienced in qualitative studies or SK; male, PhD, experienced in qualitative studies) and the other reporting (RESC; female, PhD candidate, experienced in qualitative studies). Demographic data were collected using the descriptive information form prepared by the researchers. The form included questions about age, gender, education level, occupation, reason for transplantation, donor type, and immunosuppressive medications. The interview started once the participant declared himself or herself ready, and the interviews were recorded by audio for further analysis. A semi-structured questionnaire developed by the researchers was used in the interviews. The questionnaire included five open-ended questions to evaluate the perception of medication adherence and non-adherence, challenges with using immunosuppressive medications, reasons for immunosuppressive medication non-adherence, and practices to improve immunosuppressive medication adherence (Figure 1). Each participant was interviewed once. The interviews lasted between 35 and 40 minutes. Polkinghorne stated that researchers should interview five to 25 people who experienced the researched phenomenon.22 Existing qualitative studies have reported that data saturation was achieved when concepts and processes that could be the answer to the research question start to reappear; at that time, the study can be stopped.23 In this study, data saturation was relied on when determining sample size. During the fourth interview, the data started to show a repeating pattern. By the seventh interview, data saturation was reached, and data collection was ended. None of the invited patients refused to participate and none left the study prematurely. The interviews were held in Turkish so that the participants could express themselves easily. The participants were labelled 1 to 7 to maintain anonymity; eg, the first participant was Participant 1 and coded as P1.
 |
Figure 1 Semi-structured questionnaire. |
Data Analysis
Data analysis was conducted using the content analysis method, which is recommended by Strauss and Corbin. According to Strauss and Corbin, data analysis includes bringing likewise data together in specific categories and subcategories and interpreting them through inductive analysis.24 In this study, liver transplant recipients’ statements were categorized with an inductive content analysis using the three steps of preparation, organization, and reporting phases (Figure 2).25 This approach enabled analysis of various statements of liver transplant recipients and categorization of factors affecting immunosuppressive medication adherence as main category, category, and subcategory. In the preparation phase of the inductive content analysis, recorded interviews were transcribed and, each transcription was reviewed several times by the researchers independently to gain a sense of the whole content. Meaningful units were extracted from the statements of the participants and line-by-line coding was performed. The researchers carefully examined the meaning units based on similarities and differences in order to generate categories. Following repeated discussion and an exchange of opinions between the researchers, categories were generated. In the organization phase, the categories were organized into two main areas (categories and sub-categories) by the researchers independently. The relationships between categories, sub-categories and codes were discussed by the researchers until an agreement was reached. The categories with similar meanings were then gathered to main categories. In the reporting phase, a pattern of the experiences of liver transplant recipients related to factors affecting immunosuppressive medication adherence was created (Figure 3). The transcription of the interviews was done in Turkish and, the selected expressions of the participants were translated into English by an expert fluent in both Turkish and English.
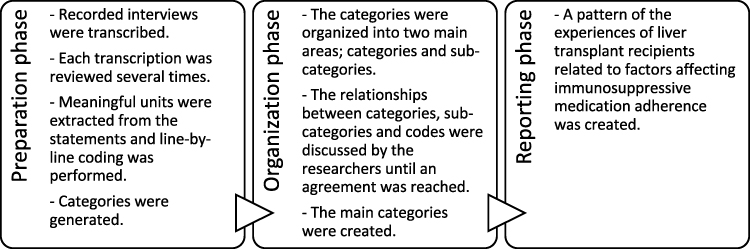 |
Figure 2 Content analysis process. |
 |
Figure 3 The pattern summarising the study results. |
Rigor and Trustworthiness
In this study, credibility, transferability and confirmability recommended by Lincoln and Guba (1985)26 were used to ensure rigor and trustworthiness. To ensure credibility, the interviews were recorded and notes were taken during the interviews. The interviews were transcribed and, the recordings were listened for a second time to check transcription. Each transcription was reviewed several times by the researchers independently. Transferability was achieved through a rich description of data collection and analysis processes and findings of the study. Confirmability was ensured through the use of the COREQ checklist and the discussions within the research team throughout the data analysis process.27,28
Ethics
The study was approved by the Hacettepe University Non-Interventional Clinical Research Ethics Board (decision no: GO18/1178). The current study complies with the Declaration of Helsinki. Written consent was obtained from the participants. The informed consent included publication of anonymized responses. In the transplant center, all organs were donated voluntarily with written informed consent, and the organ donations were conducted in accordance with the Declaration of Istanbul.
Results
This study included six male participants and one female participant, with a mean age of 42.14±15.04 years old. On average, 14.71±3.19 years had passed since their liver transplantation. Six of the participants had undergone cadaveric transplantation, and one had a living donor. One participant was taking one immunosuppressive medication, four were taking two immunosuppressive medications, and two were taking three immunosuppressive medications (Table 1).
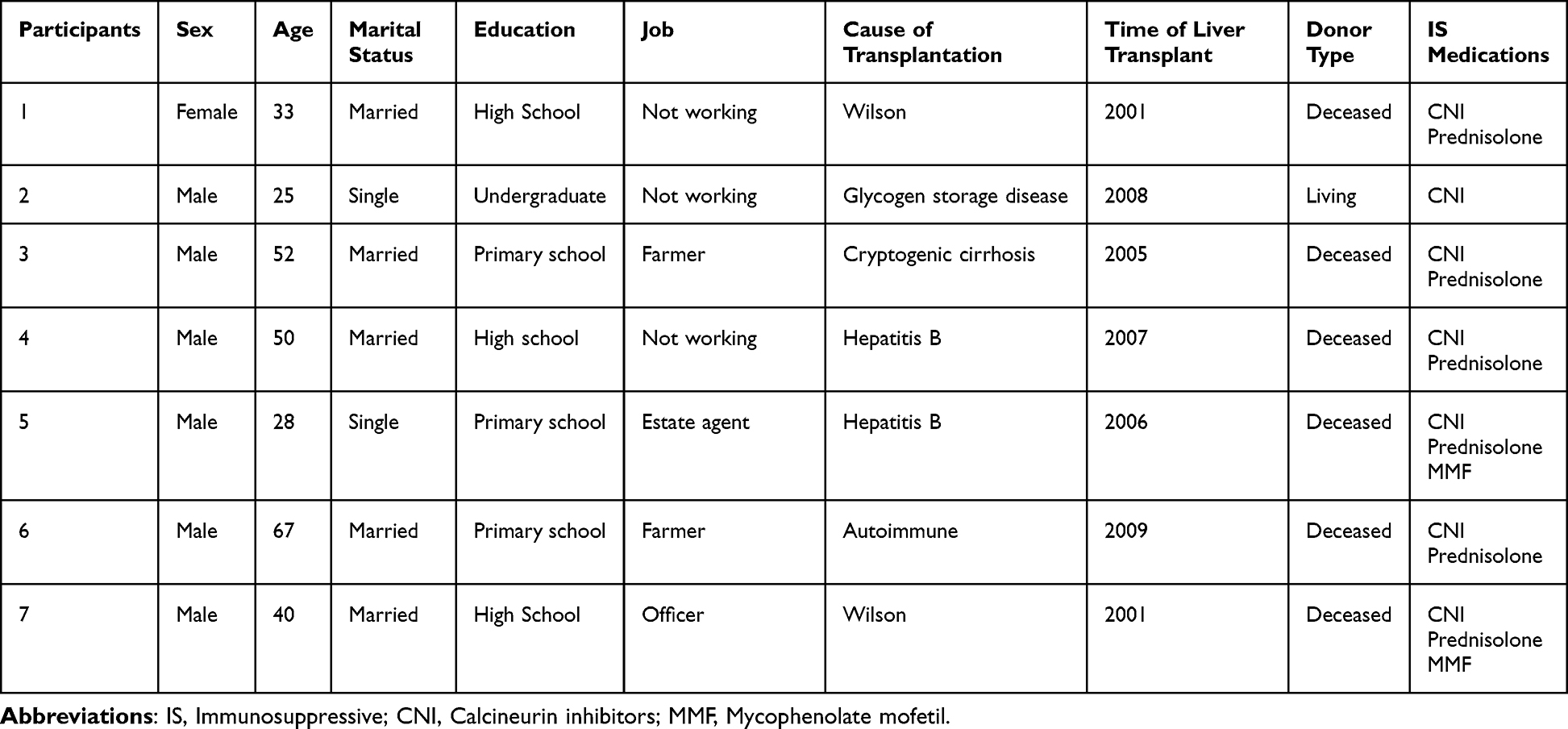 |
Table 1 Demographic Characteristics of Participants |
Content analysis revealed four main categories, nine categories, and 31 subcategories. The four main categories that emerged from the interview data were medication adherence perception, types of medication non-adherence, factors affecting medication adherence negatively, and factors affecting medication adherence positively (Table 2).
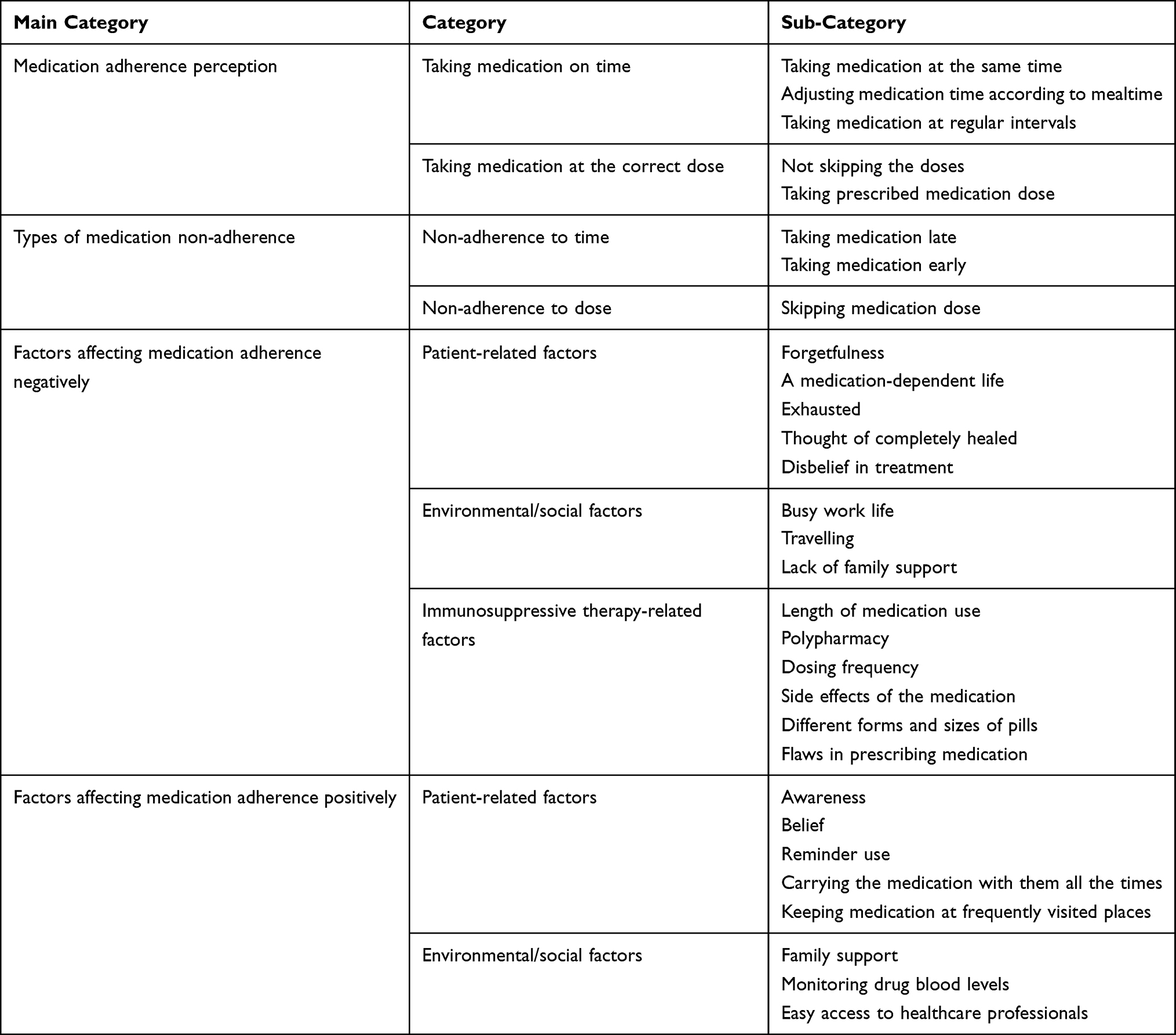 |
Table 2 Overview of the Study Main Categories, Categories and Sub-Categories |
Medication Adherence Perception
Content analysis showed that medication adherence was perceived by the participants as taking medication on time and at the correct dose. Under this main category, there are the two categories “taking medicine on time” and “taking medicine at the correct dose”. Adherence to medication time is defined as taking the medicine every day at the same hour, at regular intervals, and adjusting medication time according to mealtime. Adherence to dose was defined as taking the medication at the correct dose, not skipping doses, and taking daily medication in exactly the correct dose.
… Taking medicine on time, use properly and in correct amounts. (P1)
In correct day, hour, just in time and without skipping, in exactly the same amount I always take. (P2)
Types of Medication Non-Adherence
After content analysis, the categories “non-adherence to time” and “non-adherence to dose” appeared under types of medication non-adherence. Participants reported changing medication times to fit into their meal times and taking their medication early or late because of their jobs or due to lingering in front of the computer or television. Participants also reported skipping their immunosuppressive medication doses from time to time.
…If I am lingering in front of computer or TV at home, I might miss it by 1–2 hours. (P2)
Well, it happens inevitably, because we have to adjust, sometimes I have to take early, according to meal. (P3)
Sometimes due to. workload, stress, wandering, there is problem, sometimes I take 3-4-5 hours late… (P7)
… On weekends when I am resting, in fact I have to wake up and have breakfast at 8 and take medicine at 9 but most of the time that does not happen … (P7)
Factors Affecting Medication Adherence Negatively
According to content analysis, factors affecting medication adherence negatively were defined as “patient-related factors”, “environmental/social factors” and “immunosuppressive therapy-related factors”.
Patient-Related Factors
Participants emphasized that forgetfulness is an important factor affecting adherence to immunosuppressive medication. Participants reported that they neglected medication after their transplant because they thought they had healed, or they did not believe in the effectiveness of immunosuppressive treatment. Moreover, using immunosuppressive medication for many years and being dependent on medication for life were defined as reasons for non-adherence.
…I go to farm, I have medication in my pocket, I forget about them even when they are in my pocket. (P6)
… So, you are feeling well, you feel that the illness is over but being dependent on those medications, is tough in your life. (P1)
…You get tired of always taking medication, but I am using it out of necessity. (P4)
So, I am still young, I am still at my 20s, I asked my doctor if I still have to continue medication, if it was to me I wouldn’t want to use them at all. (P5)
…If a person is not taking medication properly, that the person either does not believe in the medication or it is feeling itself healthy in that moment. (P7)
Environmental/Social Factors
Participants reported they were neglecting immunosuppressive medication because of the activity of their work life, traveling in and out of the city, and lack of family support.
… For instance, you go on vacation, you go somewhere err, I don’t know you go somewhere and forget the medication. (P5)
… No-one is asking you if you got your medication, there is no one to ask that (in family). (P6)
…You just forget it because of your job in that moment. (P7)
Immunosuppressive Therapy-Related Factors
Participants reported that some factors related to their treatment regime affected medication adherence negatively. Taking immunosuppressive medication for many years, taking multiple medications frequently, and side effects of the medication were reported as factors leading to medication non-adherence. Patients also noted that different forms and sizes of their pills and flaws in prescribing medication negatively affect adherence.
… Taking the medication for a long time, taking it regularly as a routine is difficult, it is also psychologically wearing you down. (P1)
I was afraid of the thing, deltacortril (prednisolone) is a medicine I was taking with fear, err, since it is cortisone. (P1)
…Some were large, and difficult to swallow. (P2)
…Somehow I swallowed anyway, taking 10 medication every day was psychologically taxing. (P2)
I was taking 5 mg tablets, pharmacy was giving me “0.5” mg, when I saw 0.5, I assumed that 5 was 5 mg, I took 0.5 mg for a month, my lab values went very bad. (P7)
Factors Affecting Medication Adherence Positively
Participants reported that besides factors affecting medication adherence negatively, there were factors that made medication use easier. Content analysis revealed “patient-related factors” and “environmental/social factors” as the categories of factors affecting medication adherence positively.
Patient-Related Factors
Participants reported that they were aware of the importance of immunosuppressive medication, and their beliefs made them accept their situation and more easily adhere to medication use. Participants also reported that reminder use, carrying the medication with them at all times, and keeping medication at frequently visited places made medication adherence easier.
… I always kept in my purse, when I wanted to travel, I packed my medication before anything else… (P1)
You set an alarm, phones have alarms, I have 7–8 reminders just that I don’t forget, if one doesn’t go off, the other one does, I remember that way… (P2)
…I know what will happen to me if I quit medication, I have to, otherwise the (transplanted) liver will be rejected… (P4)
Now I have medication at the office where I work, at home, in my pocket. (P5)
…I know what would happen to me when I cannot take the medication or if I take it incorrectly… (P7)
Environmental/Social Factors
Participants reported that family members who reminded them to take their medication and keeping track of medication use promote medication adherence and have a positive effect on adherence. Participants also found that monitoring drug blood levels at the hospital encourages them to take their medication regularly. In addition, easy access to health professionals for questions related to their immunosuppressive medication was reported to help adherence.
…Especially in the beginning my mother would remind me a lot, did you take your medication? Did you take your medication?… (P1)
…My spouse especially always carries in the purse, reminds me when it is the time, prepares my meals regularly and arranges them according to medication. (P4)
… often I consult with my doctor, I call, he tells me either to take it or not to take it, whatever my doctor says… (P4)
… I give blood sample every 2 months, if I am not taking (medication), medication level is seen there, it can be seen in my blood tests. (P5)
Discussion
Immunosuppressive medication adherence remains a cornerstone of therapy to preserve the longevity and function of the grafted liver.4,7 Not taking the immunosuppressive medication at all due to refusing the medication, constantly forgetting about their medication, and difficulty accessing medications is defined as complete non-adherence.19,20 Not taking the medication as prescribed due to changing the dose, skipping doses, or not taking the medication on time is defined as partial adherence.19,20 In this study, participants stated that they did not take their medications on time, at the correct dose, and skipped doses. Therefore, it was found that the liver transplant recipients had partial adherence to immunosuppressive medication in the study.
Participants reported forgetfulness as a leading individual factor affecting medication adherence negatively. Forgetting to take immunosuppressive medication during occupational life and daily activities has been reported to be an important barrier to medication adherence.4,19 Research on kidney transplant recipients indicates that patients forget to take their medication when they are away from their homes.29,30 Claes et al reported in pediatric liver and kidney transplant recipients that forgetfulness is a leading factor for medication non-adherence (70%).31 Patients have developed some personal solutions to overcome forgetfulness.32,33 In the present study, participants reported using a reminder device, always carrying the medication with them, and keeping backup medication at the places they frequently visit. Studies have reported that transplant recipients use reminders such as mobile phone alarms, visual aids, cues, diaries, and calendars to overcome forgetfulness.29,32–37 Family members and caregivers also assume reminder duties for transplant recipients.32,34,38 Despite all these measures and solutions, forgetfulness is still an important factor affecting immunosuppressive medication adherence.
The complex regime of immunosuppressive medications and the need for lifelong treatment make transplant recipients exhausted with the use of immunosuppressive medication.32,33,39 This study defined that taking immunosuppressive medication causes a perception of being dependent on medication for life and leads to weariness with taking the medication. Furthermore, the study revealed that liver transplant recipients’ perception of being completely healed after transplantation or losing belief in treatment also negatively affected medication adherence. Transplant recipients consider themselves fully healed after transplantation due to regression of their primary disease-related symptoms, weakening of the side effects of immunosuppressive medication, and feeling “all right”.33,40 This phenomenon appears to be one of the patient-related factors that diminish immunosuppressive medication adherence.4,19
In addition to patient-related factors, there are some environmental and social factors that affect adherence to immunosuppressive medication.30,41,42 In this study, busy occupational life, travel, and lack of family support were defined as environmental/social factors among liver transplant recipients that negatively affect adherence. Similar to this study, Israni et al defined inflexible work schedule and leaving home for somewhere else as barriers against adherence.29 Gordon et al30 reported that patients cannot reach their routine cues when away from their home, and that causes problems with immunosuppressive medication use. Moayed et al43 reported that insufficient psychosocial and therapeutic support of family members was a barrier to adherence to medical care programs.
Another important barrier against immunosuppressive medication adherence is immunosuppressive treatment-related factors.42 Side effects of immunosuppressive medication are among the leading treatment-related factors.19,33,44 Transplant recipients can make a pros/cons calculation by comparing the side effects of immunosuppressive medication with the risks of not taking the medication. They can exhibit non-adherent behavior like skipping or splitting doses in order to lessen the side effects, without completely abandoning the medication.44 Transplant recipients can also be willing to endure the side effects of immunosuppressive medications with the belief that it is “better to live with side effects than not to live”.33 In this study, liver transplant recipients reported that the side effects of their medication affected medication adherence negatively, which is in contrast to the findings of Tang et al.33 In the present study, taking multiple immunosuppressive medications, frequency of daily medication, and taking medication for many years were defined as other treatment-related factors negatively affecting adherence. A systematic review by Kelly et al reported polypharmacy as a barrier to adherence due to the physical difficulty of taking so many medications.36 Jamieson et al reported that overmedication caused exhaustion in kidney transplant recipients.39 This study also reported that size and different forms of medication and difficulties with obtaining prescriptions make immunosuppressive medication adherence difficult. Similar to this study, Gordon et al reported that medication characteristics like large size, bad smell and taste, and large quantity of medications make adherence difficult in kidney transplant recipients.30
This study revealed not only negative factors but also positive factors affecting adherence. Liver transplant recipients’ awareness of the importance of immunosuppressive medication and their belief in the usefulness of treatment were found to positively affect adherence. Similar to this study, immunosuppressive medication beliefs, including the necessity of immunosuppressive medication and immunosuppressive medication concerns, were reported among the major factors affecting immunosuppressive medication adherence positively in a study by Liu et al.45 It was also found that using a reminder and always keeping backup medication were found to be other patient-related factors affecting adherence positively.
Family support and accessibility to healthcare practitioners were found to be environmental/social factors that positively affect adherence. There are many studies reporting that family and other kinds of social support increase adherence to medication and treatment.32,36,38,41,46 In the study by Lieber et al, family support and reliance on family were reported as key motivators for survival after transplantation.46 Kelly et al reported that relationships with healthcare practitioners and trust in a healthcare practitioner’s knowledge have positive effects on medication adherence.36 Blood level monitoring of immunosuppressive drugs was found to be another factor increasing adherence in liver transplant recipients in this study. Drug blood level monitoring is one of the direct methods to evaluate immunosuppressive medication adherence in transplant recipients.44 Transplant recipients’ awareness that medication non-adherence can be identified this way is a mechanism of encouragement to take their medication regularly.
Conclusion
This study explored that there are several factors affecting immunosuppressive medication adherence among liver transplant recipients, both positively and negatively. Among the patient-related factors affecting medication adherence, forgetfulness is still an important factor. Among the environmental/social factors, a busy daily life routine was found to affect liver transplant recipients’ medication adherence negatively. Besides these, taking so much medication frequently for a long time, side effects, and different forms of medication are immunosuppressive treatment-related factors affecting medication adherence negatively. In order to achieve liver transplant recipients’ total adherence to immunosuppressive medication, the factors affecting medication adherence positively and negatively should be understood. Also, strategies to improve adherence should be developed by addressing negative factors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Brown M, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
2. Germani G, Lazzaro S, Gnoato F, et al. Nonadherent behaviors after solid organ transplantation. Transplant Proc. 2011;43:318–323. doi:10.1016/j.transproceed.2010.09.103
3. Haynes RB, Ackloo E, Sahota N, Mcdonald HP, Yao X. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008;16:2.
4. World Health Organization. Adherence to long-term therapies; 2003. Available from: https://www.who.int/chp/knowledge/publications/adherence_Section1.pdf.
5. Ho PM, Bryson CL, Rumsfeld JS. Medication adherence its importance in cardiovascular outcomes. Circulation. 2009;119(23):3028–3035. doi:10.1161/CIRCULATIONAHA.108.768986
6. Lehane E, McCarthy G. Intentional and unintentional medication non-adherence: a comprehensive framework for clinical research and practice? A discussion paper. Int J Nurs Stud. 2007;44(8):1468–1477. doi:10.1016/j.ijnurstu.2006.07.010
7. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
8. Lieber SR, Volk ML. Non-adherence and graft failure in adult liver transplant recipients. Dig Dis Sci. 2013;58(3):824–834. doi:10.1007/s10620-012-2412-0
9. Kung M, Koschwanez HE, Painter L, Honeyman V, Broadbent E. Immunosuppressant nonadherence in heart, liver, and lung transplant patients: associations with medication beliefs and illness perceptions. Transplantation. 2012;93(9):958–963. doi:10.1097/TP.0b013e31824b822d
10. De Bleser L, Dobbels F, Berben L, et al. The spectrum of nonadherence with medication in heart, liver, and lung transplant patients assessed in various ways. Transpl Int. 2011;24(9):882–891. doi:10.1111/j.1432-2277.2011.01296.x
11. Driscoll CJ, Gallagher L, Schaeffer MJ. Liver transplantation. In: Cupples S, Lerret S, McCalmont V, Ohler L, editors. Core Curriculum for Transplant Nurses.
12. Sandwijk MS, Bemelman FJ, Berge IJM. Immunosuppressive drugs after solid organ transplantation. Neth J Med. 2013;71(6):281–289.
13. Shemesh E, LaPointe Rudow D. Perspectives of solid organ transplant recipients on taking medications: valuable research, just the beginning. Am J Transplant. 2021;21(10):3221–3222. doi:10.1111/ajt.16620
14. Polit DF, Beck CT. Generalization in quantitative and qualitative research: myths and strategies. Int J Nurs Stud. 2010;47(11):1451–1458. doi:10.1016/j.ijnurstu.2010.06.004
15. Van Manen M. Practicing phenomenological writing. Phenomenol Pedagogy. 1984;2(1):36–69. doi:10.29173/pandp14931
16. Moustakas C. Phenomenological Research Methods. Sage publications; 1994.
17. Chein I. Appendix: an introduction to sampling. In: Kidder LH, editor. Selltiz, Wrightsman & Cook’s Research Methods in Social Relations.
18. Patton MQ. How to Use Qualitative Methods in Evaluation (No. 4). SAGE; 1987.
19. Nevins TE, Nickerson PW, Dew MA. Understanding medication nonadherence after kidney transplant. J Am Soc Nephrol. 2017;28(8):2290–2301. doi:10.1681/ASN.2017020216
20. Tong A, Howell M, Wong G, Webster AC, Howard K, Craig JC. The perspectives of kidney transplant recipients on medicine taking: a systematic review of qualitative studies. Nephrol Dial Transplant. 2011;26(1):344–354. doi:10.1093/ndt/gfq376
21. Özdemir Köken Z, Karahan S, Sezer RE, Abbasoğlu O. Immunosuppressive medication adherence in liver transplant patients: a single center experience. Ahi Evran Med J. 2020;4(3):88–95.
22. Polkinghorne DE. Phenomenological research methods. In: Existential-Phenomenological Perspectives in Psychology. Boston, MA: Springer; 1989:1989.
23. Glaser BG, Strauss AL, Strutzel E. The discovery of grounded theory; strategies for qualitative research. Nurs Res. 1968;17(4):364. doi:10.1097/00006199-196807000-00014
24. Strauss A, Corbin JM. Grounded Theory in Practice. SAGE; 1997.
25. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
26. Lincoln YS, Guba E. Naturalistic Inquiry. Thousand Oaks: Sage; 1985.
27. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
28. Sutantri S, Cuthill F, Holloway A. ‘A bridge to normal’: a qualitative study of Indonesian women’s attendance in a phase two cardiac rehabilitation programme. Eur J Cardiovasc Nurs. 2019;18(8):744–752. doi:10.1177/1474515119864208
29. Israni A, Dean C, Kasel B, Berndt L, Wildebush W, Wang CJ. Why do patients forget to take immunosuppression medications and miss appointments: can a mobile phone app help? JMIR Public Health Surveill. 2016;2:e15. doi:10.2196/publichealth.5285
30. Gordon EJ, Gallant M, Sehgal AR, Conti D, Siminoff LA. Medication-taking among adult renal transplant recipients: barriers and strategies. Transpl Int. 2009;22(5):534–545. doi:10.1111/j.1432-2277.2008.00827.x
31. Claes A, Decorte A, Levtchenko E, Knops N, Dobbels F. Facilitators and barriers of medication adherence in pediatric liver and kidney transplant recipients: a mixed-methods study. Prog Transplant. 2014;24(4):311–321. doi:10.7182/pit2014873
32. Low JK, Crawford K, Manias E, Williams A. Stressors and coping resources of Australian kidney transplant recipients related to medication taking: a qualitative study. J Clin Nurs. 2017;26(11–12):1495–1507. doi:10.1111/jocn.13435
33. Tang J, Kerklaan J, Wong G, et al. Perspectives of solid organ transplant recipients on medicine-taking: systematic review of qualitative studies. Am J Transplant. 2021. doi:10.1111/ajt.16613
34. Beckmann S, Künzler-Heule P, Biotti B, Spirig R. Mastering together the highs and lows: patients’ and caregivers’ perceptions of self-management in the course of liver transplantation. Prog Transplant. 2016;26(3):215–223. doi:10.1177/1526924816654769
35. Muduma G, Shupo FC, Dam S, et al. Patient survey to identify reasons for non-adherence and elicitation of quality of life concepts associated with immunosuppressant therapy in kidney transplant recipients. Patient Prefer Adherence. 2016;10:27–36. doi:10.2147/PPA.S96086
36. Kelly M, McCarthy S, Sahm LJ. Knowledge, attitudes and beliefs of patients and carers regarding medication adherence: a review of qualitative literature. Eur J Clin Pharmacol. 2014;70(12):1423–1431. doi:10.1007/s00228-014-1761-3
37. Ruppar TM, Russell CL. Medication adherence in successful kidney transplant recipients. Prog Transplant. 2009;19(2):167–172. doi:10.1177/152692480901900211
38. Been-Dahmen JM, Grijpma JW, Ista E, et al. Self-management challenges and support needs among kidney transplant recipients: a qualitative study. J Adv Nurs. 2018;74(10):2393–2405. doi:10.1111/jan.13730
39. Jamieson NJ, Hanson CS, Josephson MA, et al. Motivations, challenges, and attitudes to self-management in kidney transplant recipients: a systematic review of qualitative studies. Am J Kidney Dis. 2016;67(3):461–478. doi:10.1053/j.ajkd.2015.07.030
40. Taher M, Toossi MN, Jafarian A, Rasti A, Nayeri ND. Patients’ experiences of life challenges after liver transplantation: a qualitative study. J Patient Exp. 2021. doi:10.1177/2374373521996956
41. Moayed MS, Ebadi A, Khodaveisi M, et al. Factors influencing health self-management in adherence to care and treatment among the recipients of liver transplantation. Patient Prefer Adherence. 2018;12:2425.
42. Ettenger R, Albrecht R, Alloway R, et al. Meeting report: FDA public meeting on patient-focused drug development and medication adherence in solid organ transplant patients. Am J Transplant. 2018;18(3):564–573. doi:10.1111/ajt.14635
43. Moayed MS, Khatiban M, Toosi MN, et al. Barriers to adherence to medical care programs in liver transplant recipients: a qualitative study. Int J Organ Transplant. 2019;10(3):115.
44. Whitsett M, Levitsky J. Medication adherence. In: Liver Transplantation: Clinical Assessment and Management. Wiley Online Library; 2021:285–298.
45. Liu J, Zhu X, Yan J, et al. Association between regulatory emotional self-efficacy and immunosuppressive medication adherence in renal transplant recipients: does medication belief act as a mediator? Front Pharmacol. 2021;12:243.
46. Lieber SR, Kim HP, Baldelli L, et al. What survivorship means to liver transplant recipients—qualitative groundwork for a survivorship conceptual model. Liver Transplant. 2021;27(10):1454–1467. doi:10.1002/lt.26088
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.