Back to Journals » Integrated Pharmacy Research and Practice » Volume 14
Factors Affecting Data Quality and Reporting Rates for Real-Time ARV Stock Status (RASS) in the West Acholi Sub-Region, Uganda: A Mixed Methods Cross-Sectional Study
Authors Ankwatsa I ![]() , Aguma HB
, Aguma HB ![]() , Atwiine F
, Atwiine F ![]() , Kalidi R
, Kalidi R
Received 30 December 2024
Accepted for publication 13 March 2025
Published 18 March 2025 Volume 2025:14 Pages 45—57
DOI https://doi.org/10.2147/IPRP.S514648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fawaz Alasmari
Ignatius Ankwatsa,1 Herbert Bush Aguma,1 Fredrick Atwiine,2 Rajab Kalidi1
1Department of Pharmacy, Makerere University, College of Health Sciences, Kampala, Uganda; 2Department of Pharmacy, Mbarara University of Science and Technology, Mbarara, Uganda
Correspondence: Ignatius Ankwatsa, Makerere University, College of Health Sciences, Kampala, Uganda, Tel +256772188993, Email [email protected]
Background: “The World Health Organization aims for universal HIV control by 2030, requiring robust healthcare infrastructure and efficient supply chain management”. In Uganda, a functional real-time ARV Stock Status (RASS) monitoring system and dashboard was developed to provide real-time intelligent data and reliable and accurate information on antiretroviral drugs and other HIV commodities. This integrates data from different information systems for timely decision-making and supports evidence-based ARV commodities supply chain management solutions. This study aimed to identify the factors influencing the quality and reporting rate for Real-Time ARV Stock Status (RASS) weekly reporting in public health facilities in the West Acholi sub-region of Uganda.
Methods: A mixed-methods cross-sectional study was conducted in six public health facilities of the West Acholi sub-region. Quantitative data involved a review of 312 reports for the reporting rate. The available 180 RASS reports were reviewed for data quality; supplemental qualitative data was gathered through key informant interviews with 11 healthcare workers and stakeholders. Quantitative data was then cleaned using EPI data, and all the variables were coded and analyzed using SPSS version 21. The tables were then computed using the analyzed data from the software, and the pie charts were constructed using the Excel 2019 version. Thematic analysis was done for the key informant qualitative interviews.
Results: Analysis of RASS reports revealed a mixed level of quality, with only 40 reports (22%) categorized as good quality. The overall reporting rate was slightly more than half, with only 180 reports (57.7%) of the expected reports. Key factors influencing data quality were infrastructural limitations, such as unreliable internet, lack of proper equipment, and staff transfers. Lack of training on RASS and limited leadership support were documented to influence the data quality and RASS reporting rate.
Conclusion: The quality of RASS reports could have been better than the national set targets. The reporting rate was slightly above average but far below the national set targets. Several factors affecting both the reporting rate and quality of reports were cited. These include staff attitude, knowledge gap, Staff transfers, poor internet connectivity, and lack of internet data bundles.
Keywords: quality, reporting rate, accuracy, completeness, timeliness
Intrduction
The global fight against HIV/AIDS has made significant strides in recent decades following the development of effective antiretroviral drugs. However, the availability of ARVs remains a critical challenge in many countries, particularly in resource-limited settings. Universal access to antiretroviral therapy (ART) has gathered momentum for the past ten years as a global health priority.1 Over the last decade, many “universal test and treat” trials have been implemented across sub-Saharan Africa and have tested the real-world efficacy of “universal” access to ART.2
In Uganda, the overall aim was to diagnose 95% of all HIV-positive individuals, provide antiretroviral therapy (ART) for 95% of those diagnosed, and achieve viral suppression for 95% of those treated by 2030.3
Supply Chain Digitalization is essential for improving performance, operations, and sustainability. It offers an opportunity to integrate innovative technologies, focus on client care, reduce organizational costs, and create more value for supply chain systems. In Uganda, a functional real-time ARV Stock Status (RASS) monitoring system and dashboard was developed to provide real-time, reliable, and accurate information on antiretroviral drugs and other HIV commodities. This is crucial in timely decision making.4 RASS is currently implemented in all the ART-providing public and some private health facilities in all 136 districts of Uganda. The health facilities report physical stock status and any HIV commodities received weekly through a short text message via a mobile handset or through the online RASS System integrated with the District Health Information System electronic national database.5 However, the RASS system, like other digital real-time reporting systems, may be affected by factors such as poor infrastructure, lack of good equipment, poor internet connectivity, unskilled staff, and insufficient resources for building staff capacity across the health facilities stores.6
Other factors reported to affect digital systems include the lack of collaboration between stakeholders for LMIS programs, the presence of duplicated stock-reporting systems, and national server breakdown times. The stock management techniques in place have proven to be inaccurate due to the poor quality of the data they generate and the complexity associated with their usage.7
The quality and timeliness of Real-Time ARV Stock Status (RASS) reporting plays a crucial role in ensuring the availability, tracking, and redistribution of ARV commodities, leading to improved HIV treatment outcomes.4 In Uganda, the reported data quality in the health sector remains low, with levels of care showing 33% in lower-level facilities and 20% in hospitals.6 A study conducted in 15 government health facilities in Western Uganda reported that the overall data quality was 64.8%, and overall timeliness was 65.3%.8 This is below the Ministry of Health’s set target for quality and reporting rates of 95% and 100%, respectively.8 This study aimed to identify the factors contributing to Real-Time ARV stock status (RASS) data quality and reporting rate in the West Acholi subregion, Uganda. The specific objectives of this study determined the current quality of RASS weekly reports generated from public health facilities by assessing their completeness, accuracy, and timeliness and ascertained the current RASS reporting rates in the West Acholi subregion. Health facility, infrastructural, and staff-related factors influencing the quality of RASS data and reporting rate for public health facilities were also identified.
Methods
A mixed methods cross-sectional study employing both quantitative and qualitative data collection methods data collection techniques was conducted in six public health facilities of the West Acholi sub-region of Uganda comprised of five districts: Gulu, Omoro, Amuru, and Nwoya, and Gulu City, for one month.
The West Acholi subregion is found in the mid-northern region of Uganda, about 334 km north of the Ugandan capital city, Kampala. Its total population is 1,054,547 people 8. It is comprised of four rural districts: Gulu, Omoro, Amuru, and Nwoya, and urbanized Gulu City, which gained city status in 2020 (The New Vision, 19 Nov 2020).
The dependent variables of the study were the quality of RASS reports and the reporting rate. The first dependent variable included constructs of accuracy and completeness of reports, including the contributing factors. A facility was scored “1” If the figures reported correspond to the physical stocks on the stock cards with the correct unit of measure (Accuracy) and if all data sets for the report fields were all entered (Completeness). A zero “0” was awarded for wrong or non-corresponding figures for the RASS report and stock card information. These scores were computed as percentages based on a denominator of 52 weeks and later categorized as good-quality reports if the overall score was 95% and poor if below 95%.
The second dependent variable was the reporting rate, measured based on the timeliness of reporting and the number of reports submitted annually by the health facility. A facility scored a “1” if the RASS weekly report was submitted from Monday to Friday of the reporting week and a “0” score if the report was submitted beyond Friday midnight of the reporting week. These scores were computed as percentages based on a denominator of 52 weeks.
The independent variables included constructs of Health facility-related factors, staff-related factors, leadership, and governance. These were majorly assessed qualitatively and reported as verbatims.
Inclusion Criteria: All Public hospitals and level of care Health Centre IV facilities accredited for ART services and implementing RASS reporting by 1st July 2022. They provide ART enrollment for new clients’ retention of existing clients into care and provision of linkage services with the communities. Facility RASS reporting focal personnel, district medicine management supervisors, DHT members, regional implementing partners, and hospital pharmacists were purposively selected. Exclusion Criteria: All public hospitals and level of care HCIV that had missing stock cards for ARV basket commodities for the FY 2022/2023 were excluded.
The sample size for public health facilities: The West Acholi subregion has three public hospitals and three levels of care IV health facilities accredited for ART, totaling six. All these facilities were selected; thus, the sample size for health facilities was six.
The sample size for RASS reports: Each of the selected six health facilities is expected to produce Fifty-two RASS reports annually. Thus, three hundred and twelve copies of report samples were expected to be reviewed against the stock cards to ascertain the completeness, accuracy, and timeliness of the data reported.
Twelve key informants were expected to respond to a key informants’ guide, and these included five DMMS, five DHOs/CHO purposively selected, and two Supply chain advisors chosen from the two IPs working in the West Acholi sub-region.
Two data collection tools were used in the study, namely, a checklist for quantitative data and a key informant guide for qualitative data. The checklist collected data on accuracy, completeness, and timeliness, and this was cross-checked against the stock cards in the drug store to ensure that the figures reported accurately tallied with the physical count for that particular week while ensuring that all data sets on the RASS report were completed as required. The number of weekly reports was also ascertained for the available reports to estimate the reporting rate. The checklist was administered by the principal investigator together with two research assistants. The assistants were one Pharmacy Technician at the Diploma level and an Information Technology specialist at the graduate level, both currently working within the West Acholi sub-region. They were trained for six days on the tools and data collection procedures before the commencement of the exercise.
A key informants guide formulated by the author with open-ended questions was administered to obtain in-depth information about the factors contributing to the RASS data quality and reporting rate in the west Acholi subregion, the study participants were asked to discuss predetermined themes related to health facility staff, resources for reporting, leadership/governance and facilitators of quality and timely reporting. This information was collected by the principal investigator by audio recording, then transcribed into written verbatims, and later on analyzed using thematic analysis. Each interview session with the key informants lasted for 30 minutes.
Permission was sought from the District/City Health officers for each district, who gave written introductory letters authorizing the investigators to access the facility premises. Upon arrival at the facility, the permission of the in-charge was obtained upon presentation of the authorized letters from the IRB and DHO/CHO to access the RASS focal person and the medicines store.
For data quality control and management, a pretest was conducted using the data collection tools at the Gulu Regional Referral Hospital, Atiak HCIV, USAID/UHA Acholi office, and DHO/DMMS office in Gulu City. The hard copies of the checklists and KIG were sorted, organized, and coded for easy transformation into electronic information format. For long-term storage of electronic information, Google Drive and strong passwords were used to limit unauthorized access of the collected information to nonparties for confidentiality purposes. To ensure the quality of data that was collected, the investigator-oriented research assistants on how to collect accurate, complete, and reliable data. The gadgets were re-checked at the start of every discussion session to ensure functionality.
Reliability and validity of Instruments were ensured by obtaining expert opinions from the stakeholders to ensure that the variables answer the research questions. We employed Cronbach’s test for content validity and construct validity.
Regarding the data analysis Plan, the collected data was analyzed using Statistical Package for the Social Sciences (SPSS) version 209 and Microsoft Excel 2021 for aggregation of statistical data.
Descriptive data was analyzed using SPSS version 20 for quantitative data. The quality of RASS data obtained using the health facility checklist and the weekly reporting scores summarized numerically, where each element in the parameter assessed was given a score of (1) for a positive outcome or a score of (0) for a negative or null outcome. The above scores were then aggregated to produce a composite variable score to indicate the quality of RASS reporting. These were presented in the results as tables and bar graphs. The aggregate score of a facility was then changed to a percentage and classified as poor if the calculated value was below 95% and good if it was 95% and above.
Excel was used to tally scores to determine the quality of reports and the accuracy, completeness, and timeliness of the reports reviewed for each facility. Percentages were computed for accuracy and completeness based on only the available RASS weekly reports for FY2022/ 2023. Excel also created tables and bar graphs, presenting the quantitative findings reported as counts and percentages. To measure the RASS reporting rate, percentages were calculated based on the availability of RASS reports for each facility and a denominator of 52 expected weekly reports from each public health facility for FY 2022/2023. This was reported as a percentage and classified as poor if the calculated value was below 95% and good if it was 95% and above.
Thematic analysis was also used to analyze the qualitative data, subthemes, and themes that were later developed, analyzed, and reported verbatim corresponding to each study objective. These findings were incorporated into a comprehensive report or presentation for discussion, ensuring a clear connection between objectives, quantitative data, and qualitative insights.
Results
Demographic Characteristics of Research Participants
A total of eleven participants participated in this study. The majority of respondents (81.8%) were male. Concerning educational qualifications, the data showed that 63.6% of respondents possessed a bachelor’s degree, while 36.4% held diplomas. Doctors constituted the largest cadres at 36.4%, the lowest being Inventory officers and nurses at 9%. (Table 1)
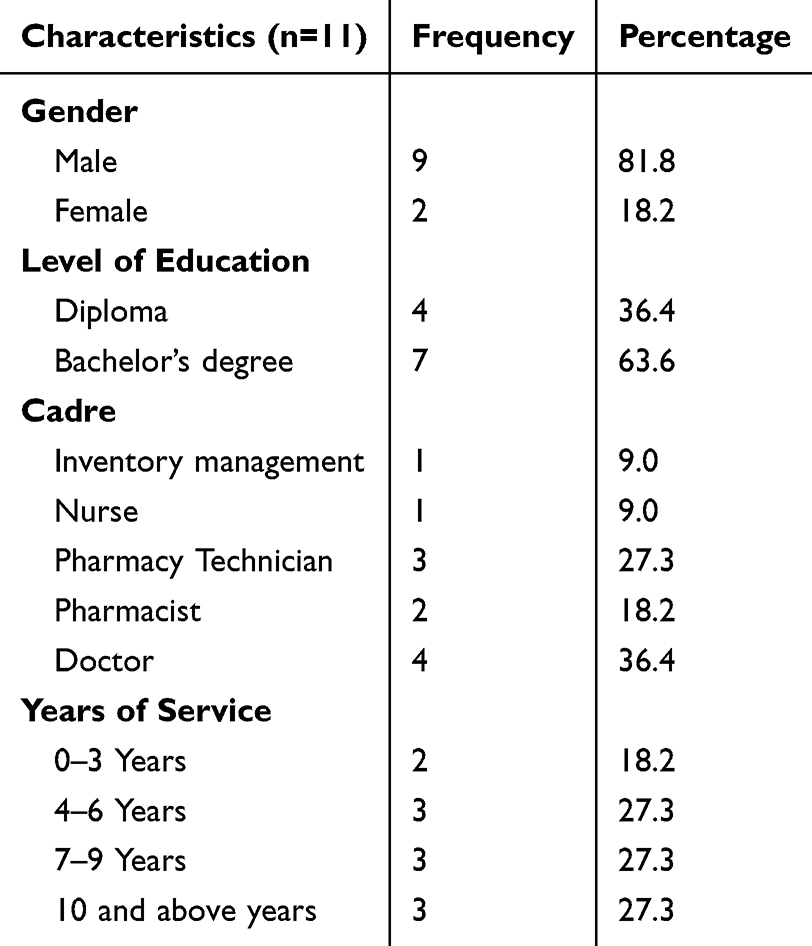 |
Table 1 Demographic Characteristics of Research Participants |
Data Quality of RASS Reports
Only 180 RASS reports were submitted for RASS weekly reports for the six high-volume facilities for the 52 weeks of FY2022/2023. All the six selected health facilities for this study had at least a RASS report available for this study, hence making the study findings generalizable. The investigators opted to study all the expected reports instead of random sampling to cater for any missing reports that would affect the validity and generalizability of the study findings. Data quality was defined as reports being both accurate and complete. The overall data quality was 22%. The regional referral hospital had the highest quality reports (9.4%), followed by the HCIVs (7.2%), and lastly, the general hospitals (5.6%) (Table 2).
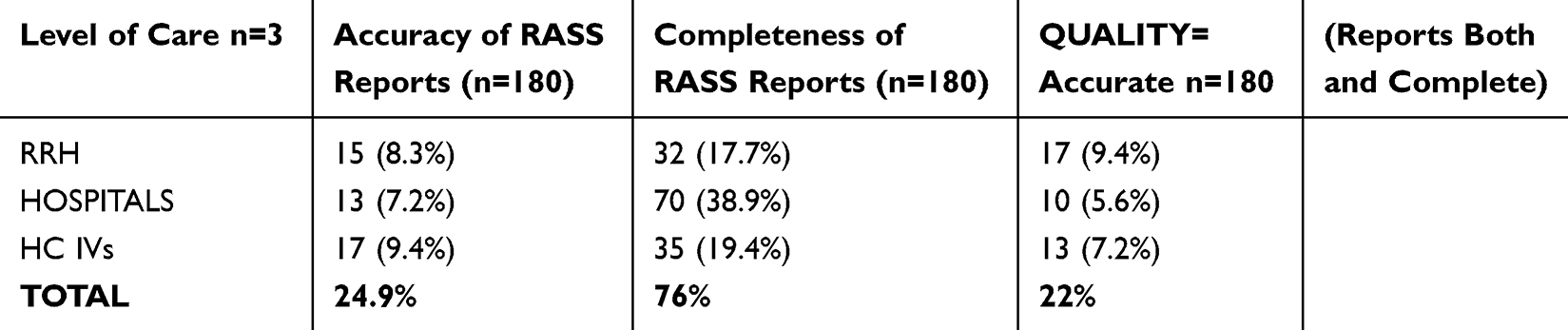 |
Table 2 Summary of Overall Data Quality |
Accuracy and Completeness of RASS Weekly Reports per Health Facility
For RASS data accuracy, Gulu Regional Referral Hospital took the lead with 42.9% of the reports tallying figures for both the RASS report and the stock cards. Gulu military hospital had the poorest report accuracy at 6.5%. For completeness of all the required reporting fields and datasets for RASS, the hospitals performed better than low-level Health Centers (Figure 1).
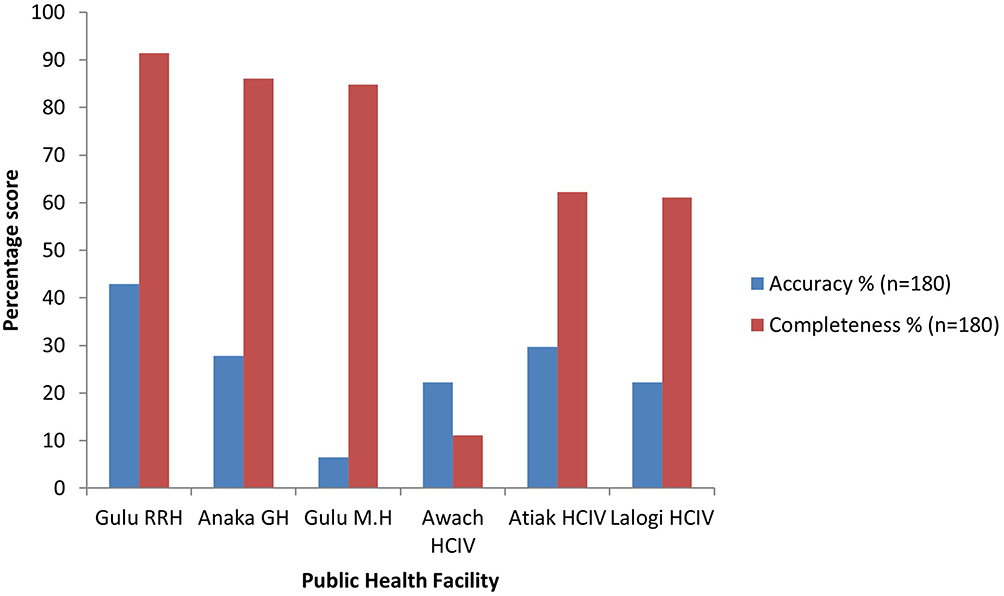 |
Figure 1 Percentage accuracy and completeness of reports from public health facilities in the West-Acholi Subregion. |
Reporting Rate Indicators
Out of the 312 reports expected, 180 (57.7%) were available. This shows that slightly more than half of the public health facilities reported for RASS. Of the available 180 reports, 167 (92.8%) were marked as ‘Yes’ for the timeliness of reporting, indicating that the majority of the reports were submitted on time (Table 3).
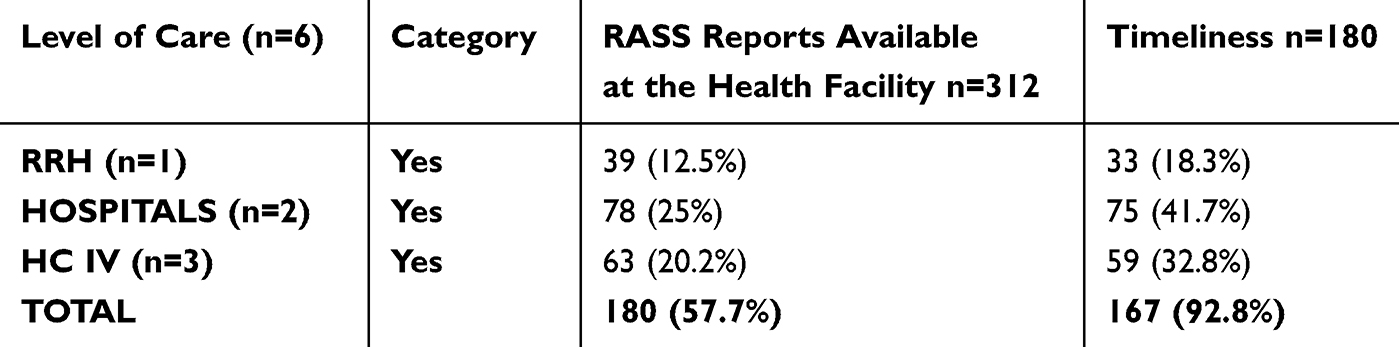 |
Table 3 Summary of the Overall Reporting Rate |
Reporting Rate Indicators per Public Health Facility
Gulu Military Hospital was leading with 44 (85%) reports out of 52 expected reports available for the FY 2022/2023, and Awach HC IV in Gulu district had the lowest number of reports available,9 (17.3%) out of the expected 52 annual reports (Figure 2).
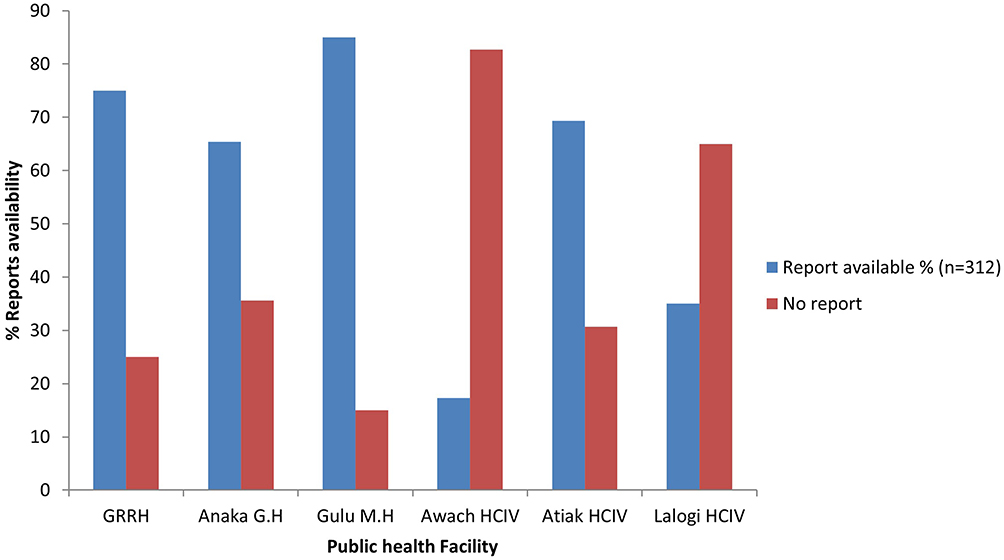 |
Figure 2 Percentage reports availability at public health facilities in the West-Acholi Subregion. |
Factors Influencing Quality of RASS Reports and Reporting Rate
Eleven key informants out of the expected twelve participants responded to the key informants’ guide, responding to the question as to why they think the quality of RASS reports and reporting rate is low in the West Acholi subregion. One of the respondents played duo roles at the district, acting as both the DMMS and DHO.
Only the key informants’ interviews were used to determine the factors associated with data quality and reporting rate to answer objective number three of this study due to the limitation of the small number of high-volume public health facilities in the study region, which gave a small size for correlation. The thematic analysis of the responses from various stakeholders regarding the factors affecting the quality of RASS reports revealed several interconnected issues that contribute to their poor quality. The themes included the knowledge gap, staff attitude, reminders to report RASS, poor gadgets/equipment, leadership, and governance gap.
Knowledge gap among facility staff responsible for RASS reporting: This gap was more frequently highlighted, stating the staff’s unfamiliarity with the indicators they were supposed to report on and failure to interpret the units of measure for ARV commodities, the respondents stated as follows;
There is also a knowledge gap, for example, TB drugs are supposed to be reported in the form of blisters, but you find when someone has reported as boxes, and also a similar case for the HIV testing kits, which are supposed to be reported as tests but some staff report them as boxes. This renders the reports inaccurate. (K008)
Another respondent stated that;
This RASS reporting is centered on how the stock management is done; some of the health facilities receive ART commodities and fail to report them to the store. They opt to use them directly, and that means that the data being captured and reported in the facility store is inaccurate. This pointed to a significant gap in data capture, as the direct usage of commodities without proper reporting led to inaccuracies. (K009)
Interpretation of the units of measure for the ARV basket commodities was also cited by the respondents as follows;
For quality, most of the staff who were assigned this duty failed to give accurate data due to failure to interpret the units of measure provided on the reporting template for RASS, which deems the weekly reports submitted in the system to be inaccurate (K006.)
Leadership and governance gaps regarding RASS reports quality were highlighted. They stated as follows;
RASS data quality is affected by a lack of ownership of this intervention by the district leaders, who need to appreciate the importance of RASS weekly reporting to enable them to follow up with key personnel responsible, such as the facility’s charges and accounting officers, to ensure compliance. (K003)
Weaknesses with the administrative staff were clearly emphasized as follows.
I see that sometimes the facilities’ administrators do not take a keen interest in RASS reporting, leaving it out only for the staff. This should change since leadership and governance are crucial for supply chain activities. (K006)
Staff attitude was highlighted as a contributing factor to the poor quality of RASS reports, primarily focusing on the negative attitudes of staff and the inconsistency of RASS reports. The respondents explained,
Of course, the attitude of the health staff affects RASS data quality and reporting rate. Some staff do not appreciate the use of reported data for ARV stock control, but at the end of the day, that data supports them via redistributions, especially for those who get stock outs. Some facility staff think it is a waste of their time to report for RASS. They probably have work overload and think these are additional responsibilities and a burden. (K008)
In addition to the above, the respondents added the following statement;
Some facility staff think supply chain activities are only for pharmacy cadres and tend to become reluctant to participate in RASS reporting. Sometimes people have negative attitudes and usually find excuses like heavy workload for not reporting. (K005)
The prominent themes emerging from the analysis of reporting rate indicators were the role of proactive reminder systems and benchmarking on good practices. Key areas of the electronic reporting system breakdown, leadership, and governance gaps as possible causes of the low reporting rates in the West Acholi sub-region, including insights on what should be done to improve the status quo, they stated as follows;
Regarding the timeliness, we need to benchmark from the HMIS 033b weekly report strategy where the reports are strictly submitted on Monday by midday. When RASS reporting was introduced, the reporting deadline was set to be by Wednesday of the week but was later adjusted to Friday. If the IPs follow up with the facility people to submit their reports by Monday and Wednesday, it would be good. (K003)
The use of social platforms to make reminders for RASS reporting was highlighted as a facilitator for weekly RASS reporting;
There should be a common platform for reminders in the region. Every financial year, a new focal person should be appointed, and in the case of newly transferred staff, they should be oriented on how to report on time and accurately. (K009)
The respondents also suggested that;
All staff should be compelled to prepare their report by close of business on Fridays of the reporting week such that these reports can be entered into the system by Monday of the following week”. “We are supposed to report by Wednesday midday and then utilize this data for decision-making, but in most cases, staff do not comply even when the period is extended to Thursday or Friday. (K009)
Planning and resource allocation were highlighted to contribute to the reporting rate for RASS;
In most cases, the health facilities fail to plan for internet bundles, thinking that it is only the responsibility of the RASS focal person. Sometimes, the individual staff can fail to get airtime for making a single call to their family. This hinders their ability to submit reports timely in the system, especially when the SMS pre-registered platform is down. (K007)
Staff transfers, staff shortages, and lack of training were highlighted as contributing factors to RASS reporting.
We have one staff member in the stores who cannot be on duty all the time because she has to get off-duty days during the week; she also has to go for outreaches. This makes it suggestive that at least the staff should be two, not one, to cover the gap. (K004)
Transfer of staff from one facility to another when after gaining experience was highlighted;
There is an issue of staff transfers; I remember Police HCIII had a staff transfer of a new staff from Hoima who did not know RASS reporting, and so we had to send the reports to the implementing partner (LPHS-TASO) to enter it into the system on behalf of the facility. (K001)
The need for comprehensive training for RASS reporting was also emphasized.
The training offered in my district was onsite by coaches; there is a need for comprehensive training on RASS, if possible, to be conducted outside the facilities where concentration is conducive to training. (K003)
The respondents highlighted the attitude of staff towards RASS reporting was frequently mentioned by the respondents;
There is an issue of attitude, for example, one of the facilities in my district has only one person designated to report for RASS, and whenever he is absent for leave, other staff refuse to report despite the facility having a trained medical records officer who is supposed to take the lead in RASS reporting, he is not willing to do the same. The motivation of staff in the form of incentives like airtime and data bundles would also help to change their attitude. (K009)
Key informants highlighted thematic areas such as SMS system breakdown times, lack of internet bundles, poor network connectivity, and lack of electronic gadgets and reporting booklets as factors influencing RASS reporting. They also cited the location of the facilities as one factor affecting the reporting rate.
The infrastructure, such as reporting tools and gadgets, is lacking, some facilities did not receive the hard copy RASS reporting booklets from the implementing partners. Some facilities have no functional computers and internet data bundles. The local revenues generated by our city do not cater for supply chain activities, and we call upon the local implementing partners with the capacity to support our health facilities to be able to report weekly for RASS to improve the quality of reports as well. (K001)
Systems breakdown was also cited as early;
The SMS platform at times experiences shutdown periods warranting the use of the online channel that requires internet data bundles. In such cases, the staff responsible for reporting tend to relax and not report if they do not have their bundles. (K005)
The location of some facilities determined their accessibility to the Internet connection required for online RASS reporting. The respondents stated as follows;
Some facilities are located in remote areas, and the internet is a big challenge for the staff who report for RASS through the DHIS system. Some of these facilities are not connected to the national grid for power and have to rely on the solar battery system, which may not be adequate since it bears its unique challenges. The availability of a local area network (LAN) connected to a national grid would be of great help to reporting online for RASS. The facilities have been relying on us, the IPs in the region, for internet bundles and airtime. However, this support is no longer being relayed due to the lack of funds from our development partners. (K003)
The use of wide-area networks such as WIFI was cited as a facilitator of RASS reporting. The study participant stated as follows.
For the facilities that depend on WIFI, like the hospitals, the connections are always weak, especially when congested with many users. This may interfere with the timeliness and quality of reports. In such scenarios, the individual staff out to be provided with separate data bundle to facilitate timely online reporting for RASS. (K010)
The respondents added that;
Most health centers III in my district have recently been upgraded to the HC III level of care and were pushed ARV medicines without clients or staff. They keep reporting the same amount of stock weekly, which may be inaccurate and expire at their stores. (K011)
Discussion
In this study, the overall data quality of the RASS data collected was 22%. This is below the Health Sector Development Plan (2015/16-2019/20) target of 60%. Also, below the >85% data quality target, according to a USAID report.10 This disparity underscores the difficulty in simultaneously achieving high levels of accuracy and completeness in the reports. The findings suggest that while some reports may be accurate, they often lack completeness, and vice versa. This dual challenge reflects broader issues in Logistics management information systems (LMIS) in low- and middle-income countries, and this is consistent with the literature, which reported that health supply chain systems were performing sub-optimally in several processes and functions across all levels of care, this is in tandem with the findings of Lugada et al, 2022.
However, this contradicts the findings from a study in Mbarara district, Western Uganda where the quality of LMIS reports was 65%.8 This difference can be because this researcher sampled study participants from only one district, and our study had a sample size of five districts that covered only the high-volume facilities.
These findings show that the quality of RASS data collected is still poor in the West Acholi sub-region of Uganda. The primary elements for the poor data quality highlighted by the study participants were failure to update stock cards promptly and wrong interpretation of Units of measure for ARV commodities. The Key informants also cited aspects of the knowledge gap, poor attitude, staff training, and staff turnover as reasons for the poor quality of RASS reporting. It was highlighted that many staff members are unfamiliar with the indicators they must report on, leading to inaccurate and incomplete reports. This issue underscores the need for targeted orientation and training programs to ensure that staff are well-informed and knowledgeable about the reporting indicators. This aligns with the broader literature that stresses the importance of training in improving data quality.11
Misconception regarding supply chain activities: The respondents identified a common misconception among staff regarding supply chain activities. Some health facility staff believe supply chain activities are only for pharmacy cadres, leading to reluctance to participate in RASS reporting. This misconception, combined with negative attitudes and workload excuses, hampers effective reporting, also emphasized in the findings by Tewfik, 2018. Some health facility leaders do not prioritize reporting activities, leaving them solely to staff members, this is similar to the findings of Tewfik et al who reported that attitude is a fundamental perspective towards reporting.
Intra-district transfers of trained staff without proper replacement further exacerbate the problem of inaccurate reporting. Addressing these issues requires targeted training to ensure that all staff can correctly interpret the reporting units and better manage staff transfers to maintain continuity and quality in the reporting process. This finding is consistent with the literature emphasizing the importance of training and proper staffing to ensure accurate data collection and reporting.11
One of the limitations was that some study participants played dual roles at the facilities and the districts, like in some areas where the DMMS was also the RASS focal person for their health facilities or where DHOs gave the DMMS delegated responsibilities. This decreased the sample size, specifically for the key informants. To mitigate this limitation, the investigator recruited the Health sub-district Medicine management supervisors (HSD-MMS) to cover this gap. These cadres deputize the DMMS within their area of jurisdiction within the districts. The response rate for RASS reports was 57.7% of the total expected reports. However, this did not affect the generalizability and validity of the findings since all six selected health facilities for the study had at least reported more than once for RASS during the study period.
Addressing the staffing issues requires comprehensive training programs, better staff transfer management, and adequate incentives to ensure timely and accurate reporting. This aligns with the literature highlighting the negative impact of poor data quality and staff shortages on logistics management and decision-making in health facilities.12
Also highlighted was the SMS reporting platform’s inconsistent performance, making it challenging to submit reports on time. This inconsistency is attributed to issues such as non-payment to service providers or network problems. System breakdown lowers the rate of RASS reporting as the public health facilities will not send reports to the national dashboard. Addressing these issues requires reliable reporting systems and adequate servicing of the national servers to support the reporting process Similar challenges were also reported by Yoweri 2018 who stated that there is sometimes network interference, and this can negatively impact SMS reporting.
A key respondent expounded upon the Initiatives, such as consistently sharing performance dashboards and establishing regional WhatsApp groups, which have proven instrumental in fostering stakeholder collaboration and accountability. By leveraging such platforms, healthcare facilities and stakeholders can maintain heightened awareness and promptly respond to reporting requirements, thereby significantly enhancing the efficiency and efficacy of the reporting process. This aligns with the literature that reported that the transformative influence wielded by technology and communication platforms in improving reporting rates is highlighted by the findings of O’Hagan et al, 2017.
The overall reporting rate determined by this study was 57.7% for the total reports reviewed. This was slightly below the rates reported in a study conducted in Uganda in 2022, which found that only 65% of the health facilities achieved timeliness for reporting in HMIS (Barungi, 2022). The availability of reports is a critical aspect of the Real-time ARV Stock Status (RASS) system. This inconsistency in reporting poses a significant challenge to the effectiveness of the RASS system, as delayed reports can hinder timely decision-making and response measures. Effective data reporting is essential for the success of health information systems, especially in resource-limited settings where timely data is crucial for managing health commodities like antiretroviral drugs, as also reported by Nutley T who emphasized the use of improved data in decision making. This reporting rate is considerably lower than the target of 95% of facilities reporting on time as required by the Health Sector Development Program (HSDP-IV), multiple factors contributed to non-reporting and late reporting by the public health facilities to submit weekly RASS reports on time for reasons such as lack of internet bundles and poor network connectivity. Facilities lack reporting gadgets to report using the online RASS platform. This is also highlighted in the Uganda National Medicines Policy (NMP 2015), which gives an overview of the challenges lower health facilities face, such as the lack of computerized inventory systems, which slow down the process of HMIS reporting.
The investigators encountered limitations with missing RASS report hard copies at some facilities where the focal persons had reported directly into the SMS reporting system.
To overcome these limitations, the investigator requested online access to the DHIS METS live dashboard from the administrators to check the facility’s soft copies retrospectively, and the implementing partners in the region were granted online access.
Failure to report in time by the public health facilities to the national dashboard may result in misinformation about the facility stock status of ARV commodities, affecting health facility service delivery at the district level. This has implications for ARV stock control since the district health teams use the information reported by the health facilities to guide decision-making for restocking and redistribution, similar findings were reported by Ouedraogo et al, 2019.
Timeliness can be significantly improved by aligning the RASS reporting schedule with more successful systems, such as the HMIS 033b weekly report strategy, and developing regional district RASS dashboards. Issuing internal deadlines to ensure compliance with reporting requirements was highlighted as a critical strategy to improve the reporting rate. This structured approach of setting internal deadlines is essential to enhance report availability. This supports the findings of Tiye and Gudeta (2018), who emphasized the need for integrating and harmonizing reporting systems to enhance data quality and timeliness.
The importance of leadership and accountability in the reporting process is highlighted, and the role of the District Medicine Management Supervisor in monitoring compliance through the DHIS system is emphasized. These insights align with the findings of Nutley 2012, which stresses the necessity of solid governance and active engagement from health system leaders to improve data utilization and availability. Alternatively, the reminders can be sent through regional supply chain social media platforms to improve the reporting rate. This technique ensures prompt communication and helps maintain high levels of RASS report availability by keeping staff informed and engaged. These strategies are supported by the literature, which suggests that digital communication tools can enhance the timeliness and quality of health information reporting13 who proposed the establishment of a common platform for reminders and the orientation of new staff to ensure timely and accurate reporting.
The problem of reporting incorrect units of measure was identified, affecting the quality of data reported for RASS. Additionally, some facilities do not update stock transactions in real-time, leading to inaccurate RASS reports. This negatively impacts ARV stock control and reduces the expiry of these commodities, leading to wastage. Addressing these issues requires focusing on staff motivation, training, and accurate data recording to improve the quality of the RASS reports. This finding aligns with the literature that underscores the importance of staff motivation and training in improving data quality.14
Conclusion
The findings reveal that the quality of RASS reports in the West Acholi Sub-region falls short of the national standards. While the reporting rate is marginally above average, it remains significantly below the national targets. Several factors impede quality and reporting rates, including staff attitudes, knowledge gaps, frequent staff transfers, poor internet connectivity, and insufficient internet data bundles. Addressing these challenges through targeted interventions and resource allocation is essential to enhance data quality and reporting rates, which are crucial for effective ARV stock management and overall health service delivery.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; ARV, Anti-retroviral drugs; ART, Antiretroviral Therapy; CDC, Centers for Disease Control; CHO, City Health Officer; DHIS, District Health Information System; DHO, District Health Officer; DHT, District Health Team; DLG, District Local Government; DMMS, District Medicines Management Supervisor; GH, General Hospital; HC, Health Center; HIV, Human Immune-Deficiency Syndrome; HSD, Health Sub-district; IP, Implementing Partner; IRB, Institutional Review Board; JMS, Joint Medical Store; LPHS, Local Partner Health Services; KIG, Key Informant Guide; METS, Monitoring and Evaluation Technical Support; MMS, Medicines Management Supervisor; MaKSPH, Makerere University School of Public Health; m-TRACK, Mobile Tracking; NMS, National Medical Store; PEPFAR, President’s Emergency Plan for AIDS Relief; PIP, Pharmaceutical Information Portal; PL-HIV, People Living with HIV disease; RASS, Real-Time ARV Stock Status; RRH, Regional Referral Hospital; SCM, Supply Chain Management; SDG, Sustainable Development Goals; SMS, Short Message Service; SOPs, Standard Operating Procedures; SSCS, Strengthening Supply Chain Systems; TASO, The AIDS Support Organization; UHA, Uganda Health Activity; UHC, Universal Health Coverage; UNAIDS, Joint United Nations Program on AIDS; UNSCT, Uganda National Council for Science and Technology; USAID, United States Agency for International Development.
Data Sharing Statement
The author will avail the datasets used and analyzed during this study on request.
Ethical Approval and Consent to Participate
Ethical approval was granted from the Makerere University School of Health Sciences Research and Ethics Committee with reference, MAKSHREC-2024-696. Administrative clearance was obtained from the DHOs and CHO at the districts and city for a single recommendation to access the public health facilities before embarking on this study. On arrival at the public health facilities, researchers introduced themselves, then presented approval letters and obtained written informed consent from study participants. The obtained informed consent also included permission for publication of their anonymized responses or direct quotes. To ensure the confidentiality and privacy of the study participants, the data collection tools didn’t record the study participants’ names. Each participant was given a unique code only known by the principal investigator. The collected data was kept under key and lock for the hard copies and the strongly guarded passwords for the electronically transformed data.
Consent for Publication
All authors agree to the submission of this manuscript for publication.
Acknowledgments
I would like to express my gratitude to my dedicated research assistants, Mr. Okidi King Solomon and Mr. Ocan Simon, whose diligent efforts were indispensable in collecting data and obtaining meaningful results. I also extend my sincere thanks to the co-authors of this manuscript, who are lecturers at Makerere and Mbarara universities in Uganda. Finally, I am deeply thankful to my family for their unwavering love, encouragement, and understanding during the research compilation period.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was entirely funded by the author and did not receive any external funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Bekker L-G, Alleyne G, Baral S, et al. Advancing global health and strengthening the HIV response in the era of the sustainable development goals: the international AIDS. Lancet. 2018;392(10144):312–358. doi:10.1016/S0140-6736(18)31070-5
2. Perriat D, Balzer L, Hayes R, et al. Comparative assessment of five trials of universal HIV testing and treatment in sub‐Saharan Africa. J Int AIDS Society. 2018;21(1):e25048. doi:10.1002/jia2.25048
3. Frescura L, Godfrey-Faussett P, A FA, et al. Achieving the 95 95 95 targets for all: a pathway to ending AIDS. PLoS One. 2022;17(8):e0272405. doi:10.1371/journal.pone.0272405
4. Milton K. Strengthening supply chain management systems for HIV commodities: a case study of real-time ARV stock status (RASS) monitoring system in Uganda. 2018.
5. Mets. Real-time ARV stock status monitoring tool. 2018.
6. Lugada E, Komakech H, Ochola I, Mwebaze S, Olowo Oteba M, Okidi Ladwar D. Health supply chain system in Uganda: current issues, structure, performance, and implications for systems strengthening. J Pharmaceutical Policy Pract. 2022;15(1):14. doi:10.1186/s40545-022-00412-4
7. Kabanda J, Mutebi A, Kabagaya M, et al. Managing stock levels of HIV commodities using electronic systems in Baylor Uganda, Rwenzori region. J Int AIDS Society. 2019;64.
8. Barungi M. Factors Affecting the Quality and Timeliness of the Health Management Information System Data of Medicines and Health Supplies in Mbarara District. Makerere University; 2022.
9. George D, Mallery P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference. Routledge; 2019.
10. Belay H, Azim T, Kassahun H. Assessment of health management information system (HMIS) performance in SNNPR, Ethiopia. Measure Evaluation. 2013.
11. Tiye K, Gudeta T. Logistics management information system performance for program drugs in public health facilities of East Wollega Zone, Oromia regional state, Ethiopia. BMC Med Inf Decis Making. 2018;18(1):1–13. doi:10.1186/s12911-018-0720-9
12. Manso JF, Annan J, Anane SS. Assessment of logistics management in Ghana health service. Int J Business Social Res. 2013;3(8):75–87.
13. Beaulieu M, Bentahar O. Digitalization of the healthcare supply chain: a roadmap to generate benefits and effectively support healthcare delivery. Technol Forecasting Social Change. 2021;167:120717. doi:10.1016/j.techfore.2021.120717
14. Chen H, Hailey D, Wang N, Yu P. A review of data quality assessment methods for public health information systems. Int J Environ Res Public Health. 2014;11(5):5170–5207. doi:10.3390/ijerph110505170
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.