Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Facilitators and Barriers to Prescription Medication Sharing: A Qualitative Study from the Public’s Perspective in Saudi Arabia
Authors Alhomoud F ![]() , Alhaddad K, Aldaqdouq Y
, Alhaddad K, Aldaqdouq Y ![]() , Aljuzair ZH, Alhomoud FK, Alsaleh FM, Alfageh B, Alrasheed MA
, Aljuzair ZH, Alhomoud FK, Alsaleh FM, Alfageh B, Alrasheed MA ![]() , Aladwani M
, Aladwani M ![]() , Almanasef M
, Almanasef M ![]()
Received 13 July 2025
Accepted for publication 8 November 2025
Published 14 November 2025 Volume 2025:17 Pages 221—237
DOI https://doi.org/10.2147/DHPS.S553530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemalkumar B Mehta
Faten Alhomoud,1 Kawthar Alhaddad,2 Yaqeen Aldaqdouq,2 Zahrah Hassan Aljuzair,2 Farah Kais Alhomoud,1 Fatemah M Alsaleh,3 Basmah Alfageh,4 Marwan A Alrasheed,4 Mohra Aladwani,5 Mona Almanasef6
1Department of Pharmacy Practice, College of Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Department of Pharmacy Practice, College of Pharmacy, Kuwait University, Kuwait City, Kuwait; 4Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 5Department of Clinical Pharmacy, College of Pharmacy, Taif University, Taif, Saudi Arabia; 6Department of Clinical Pharmacy, College of Pharmacy, King Khalid University, Abha, Saudi Arabia
Correspondence: Faten Alhomoud, Department of Pharmacy Practice, College of Pharmacy, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia, Tel +966133335547, Email [email protected]
Background: Prescription medication sharing (PMS) poses significant health risks, including side effects, delayed care, and worsening of illness. Despite these risks, evidence explaining why people share or avoid sharing prescription medicines remains scarce. To address this gap, the present study explored the perceived facilitators and barriers to PMS among the public in the Kingdom of Saudi Arabia (KSA) using a qualitative approach.
Methods: A qualitative study using face-to-face, semi-structured interviews was conducted in the Eastern Province with 60 participants, selected through a convenience sampling strategy. Eligibility criteria included the ability to communicate in Arabic or English, age ≥ 18 years, and taking a prescribed medication. Interviews continued until data saturation was achieved. Audio recordings were transcribed verbatim and analysed thematically using QSR NVivo 10 software.
Results: The study included 60 participants. Most participants were female, younger adults, and university educated. Thematic analysis identified two main themes: facilitators and barriers of PMS. Facilitators included saving time and cost, limited access to medicines or healthcare services, availability of leftover medicines, socio-cultural factors, and prior experience or knowledge about an illness and its treatment. Barriers included unsafe or ineffective treatment, awareness of public health risks, risk of dependence, and risk of non-adherence among lenders. These themes reflected a complex interaction of individual, cultural, and system-level influences. While some drivers aligned with international findings, others were more specific to the Saudi context, such as over-prescribing by doctors, brand preferences, misuse of insurance, medicine accumulation, strong family ties, cultural expectations of generosity, stigma-related communication gaps, and personal illness experiences.
Conclusion: This study provides the first qualitative insight into PMS in Saudi Arabia, highlighting how cultural norms, family dynamics, and healthcare system factors shape this behavior. The findings underscore the need for culturally informed policies and public health strategies to reduce risks and promote safe medication practices. Pharmacist-led counselling and community-based campaigns focused on safe medication use and proper disposal can further support safer medication practices and reduce the risks associated with PMS.
Keywords: borrowing, lending, sharing, prescription, drug, medicine
Introduction
Prescription medication sharing (PMS) is defined as a situation where lending or giving and borrowing or taking of prescribed medication occur, and the recipient is not the person for whom the prescription is intended.1–9 It represents a significant public health concern due to its potential to cause adverse drug reactions, allergies, resistance, teratogenic effects, dependence, and delays in seeking appropriate care.1,7,8 PMS also involves safety and legal risks, particularly when controlled or semi-controlled medications are shared. Furthermore, it may lead to drug–drug interactions, inappropriate duplication or contraindication, avoidable emergency department visits, and increased healthcare costs, highlighting the importance of addressing this issue within public health frameworks.1,7,8 The prevalence of PMS varies globally, ranging from 5% to 66%.1,2,7,9–12 Evidence from Saudi Arabia indicates that 14% of individuals borrowed and 16% lent prescription medicines, while 20% shared medications with another child and 75% kept leftover prescriptions at home.13 A regional review also reported self-medication with antibiotics—often involving shared or leftover prescriptions—ranging from 19% to 82%.14 These high rates reflect common practices in the Middle East, driven by access barriers, limited awareness, and the tendency to store unused medicines for future use or sharing.13,14
In Saudi Arabia, strong family ties, traditions, and religious values significantly influence individual behaviors. Medication sharing is reinforced by large and extended families and a deep cultural and religious duty to care for relatives, elders, and those in need.15 Offering medicines is often viewed as an act of kindness and solidarity, sometimes leading individuals to prioritize helping others over adhering strictly to medical advice. Social expectations may also make it difficult to refuse medication requests from family or friends.15 Beyond cultural influences, structural and healthcare system factors also shape PMS practices in Saudi Arabia. The country provides free healthcare and medicines to citizens and public-sector expatriates through government facilities.16 However, expatriates in the private sector often have only basic insurance, leading to out-of-pocket expenses and limited access to medical care.16 While free access for citizens reduces financial barriers, it may also increase the availability of medicines and, consequently, the likelihood of medication sharing. Together with cultural norms, these structural factors contribute to the accumulation of unused medicines in households, creating conditions that promote PMS. The ready availability of unused medicines stored at home appears to be an important contextual factor associated with PMS. This behavior carries several health risks, including antibiotic resistance resulting from incomplete or inappropriate antibiotic courses, and teratogenic effects when medications are shared during pregnancy, potentially leading to congenital malformations or developmental harm.13,14,17 Addressing these challenges requires engagement at multiple levels, particularly from healthcare providers. Healthcare providers play a key role in addressing PMS through counseling, education, and promotion of safe medication practices.3,10 Safe disposal and take-back programs have proven effective in reducing medication misuse and accumulation.1–7,9,10,13 Moreover, international strategies, such as pharmacist-led counseling, public awareness campaigns, and stronger prescribing oversight, have helped reduce sharing behaviors and improve medication safety.1–7,9,10,13
Previous reviews show that most PMS studies have relied on quantitative surveys, with limited exploration of patients’ perspectives or motivations.1,18 These surveys often used predefined lists of influencing factors, restricting the discovery of new reasons for sharing and limiting deeper insights into public attitudes.1,2,7,9–12,18 Only a few qualitative studies worldwide have examined PMS from participants’ viewpoints.15,19 To date, no studies in Saudi Arabia have qualitatively explored PMS from the public’s perspective to identify its facilitators and barriers.13 Our previous quantitative research described the prevalence and types of shared medications in Saudi Arabia;13 however, the current study builds upon that work by using a qualitative approach to explore in depth the sociocultural, behavioral, and systemic factors influencing PMS. Thus, this study aimed to explore perceived facilitators and barriers to prescription medication sharing among the Saudi public using a qualitative approach to gain deeper insight into beliefs, motivations, and experiences. The findings can inform healthcare policy, patient education, and harm reduction strategies. Understanding the reasons behind PMS is essential for developing effective interventions and policies to enhance medication safety and public health.
Materials and Methods
Study Design, Setting, Recruitment, Data Collection and Ethical Considerations
This qualitative research design employed semi-structured interviews. Eligible participants were individuals aged 18 years or older who spoke Arabic or English and had used prescription medications. People who had used only non-prescription medicines and healthcare providers were excluded from the study. A convenience sampling technique, supplemented by snowball sampling, was used to select and recruit individuals located in the Eastern Province of Saudi Arabia. Students from the College of Pharmacy at Imam Abdulrahman Bin Faisal University contacted their friends at various colleges via Email and telephone, asking them to recommend potential participants from their family members, friends, and neighbors who met the inclusion criteria to participate in the current study. Recruitment efforts were promoted across the entire university to help reach participants with varied educational, occupational, and socio-economic backgrounds, thereby enhancing diversity within the sample. Telephone calls were made, and invitation letters were sent via Email to invite potential subjects. Once they had been located and informed about the study, all potential individuals were approached and invited to participate. If they were willing to participate, a suitable date and time were arranged to conduct the interview, either one-to-one at the participants’ homes or over the telephone. The data collection was conducted over a period of five months.
The semi-structured interview guide developed by Beyene et al5 was used to conduct an in-depth exploration of the public’s beliefs about and experiences with PMS behaviors. The guide covered key questions, including:
- What types of prescription medicines have you shared or borrowed?
- Why did you or others share prescription medicines?
- What were the perceived benefits and risks of sharing prescription medicines?
- How did you decide if a prescription medicine was safe to share?
- What influences (eg, media, advertisements) affected your sharing practices?
- What were your experiences, whether positive or negative, of sharing prescription medicines?
The authors obtained permission from Beyene et al to use and adapt the tool for use in Saudi Arabia. The guide was translated into Arabic using the parallel translation technique by two independent translators.20 Their versions were then reviewed and compared by the authors and a bilingual pharmacy expert to ensure consistency and cultural appropriateness. Minor modifications were made to ensure cultural and contextual relevance for Saudi participants.
Use of a semi-structured interview format provided flexibility to explore issues that emerged during the interviews but were not anticipated in advance. Participants’ characteristics were collected, including age, gender, nationality, educational status, occupation, and health status. Before each interview, participants were given distinguishing statements between prescribed and non-prescribed medicines, and between medication borrowing and lending, and were instructed to exclude over-the-counter medicines when responding.
All eligible participants who wished to participate were provided with a participant information sheet that contained detailed information about the study. Informed consent was obtained from all participants prior to the commencement of each interview. The participants were reminded that they are free to withdraw from the study at any time, and that their consent included permission for the use and publication of anonymized responses and direct quotes. The interviews were conducted in Arabic or English, according to each participant’s preference. Each interview lasted between 15 and 30 minutes. Interviews were digitally recorded with the participants’ permission. Handwritten notes were taken for participants who refused to be audio recorded during the interviews. The sample size was determined based on data saturation (when no new themes emerge), which was considered to have occurred after 60 interviews.
Ethical approval was obtained from the Deanship of Scientific Research at Imam Abdulrahman Bin Faisal University (IAU) [IRB-2025-05-0041]. This study was conducted by the ethical principles outlined in the Declaration of Helsinki.
Data Processing, Analysis and Quality Assurance
Interviews transcription and analysis were ongoing throughout the data collection process to enable making a judgment regarding data saturation and to identify the point at which no new information arose. QSR International’s NVivo 10 (NVivo qualitative data analysis software version 10, 2012) was used to organise the data and facilitate analysis. The analysis drew on thematic analysis techniques informed by Braun and Clarke’s work and the constant comparative method style,21 allowing for the examination of data both within individual transcripts and across the sample.
A combined coding approach was applied: deductive codes were derived from a pre-existing coding frame (Beyene et al’s 2016 PMS coding frame),5 while inductive codes were developed during the identification of new themes emerging from the data to capture patterns related to the study objectives. The coding framework was thus developed by integrating the Beyene et al coding frame with inductively generated codes. Any references to non-prescribed medications (OTC) were excluded from coding and theme development to maintain focus on prescription medications.
The analysis process was led collaboratively by FA, FA and FA with support provided by KA, YA, and ZA. Familiarity with the data was achieved through audio recordings and line-by-line reading of transcripts. The analysis team reviewed all transcripts. Specifically, transcripts 1–20 were reviewed by YA, transcripts 21–40 by ZA, transcripts 41–60 by KA, and the full dataset was further reviewed by BA, MA, MA and MA to ensure consistency and accuracy. Each analyst made notes capturing themes and sub-themes of interest, similar to “memo-ing” in grounded theory20. Emerging findings and interpretations were discussed and verified during eight team meetings, where coding discrepancies were resolved through discussion until consensus was reached. Team discussions provided fresh insights, both personal, professional, and methodological, enabling FA to reflect on potential biases and assumptions. A final review of all transcripts was conducted to ensure that all text was accounted for and that all codes were appropriately incorporated into themes. Minor editing of some exemplar quotes was performed to ensure clarity and preserve anonymity, and representative verbatim comments were selected for presentation. Reflexivity was maintained throughout the analysis by documenting researcher assumptions, perspectives, and decisions in analytical memos.
Results
Study Response and Participants’ Characteristics
Of the 65 participants approached to take part, 60 agreed to participate in this study (response rate: 92%). The majority were female (75%) and Saudi nationals. Most participants were younger adults, with 48% aged between 18 and 30 years. Over 40% of participants were current students (full-time or part-time), while the remainder were employed or homemakers. In terms of living arrangements, most participants lived with their families (90%). Regarding monthly income, approximately 53% reported a low income (< $1,330 US dollars), while 28% reported a higher income (> $2,660 US dollars). Almost half of the participants did not have private medical insurance and relied on government-provided healthcare services. A detailed description of participants’ characteristics is shown in Table 1.
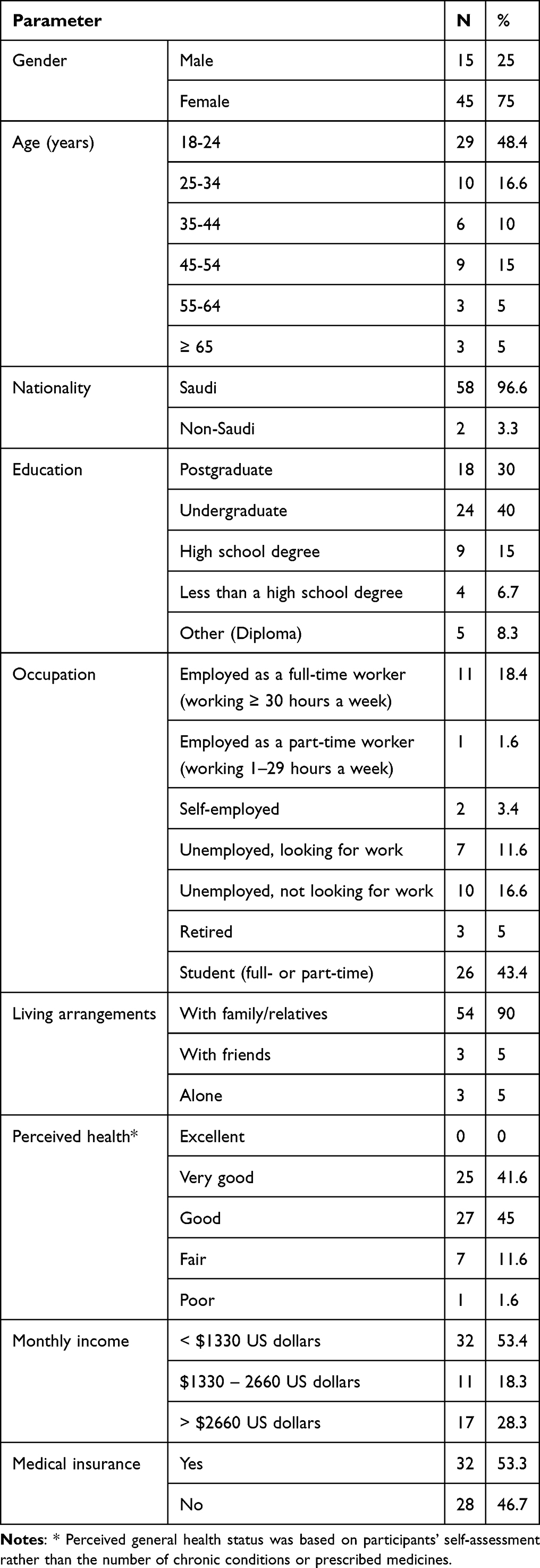 |
Table 1 Characteristics of Participants Recruited into the Study (N=60) |
Types of Shared Medicines
A wide range of prescription medicines was shared by study participants (see Box 1). All participants reported that sharing practices were mainly for medical use.
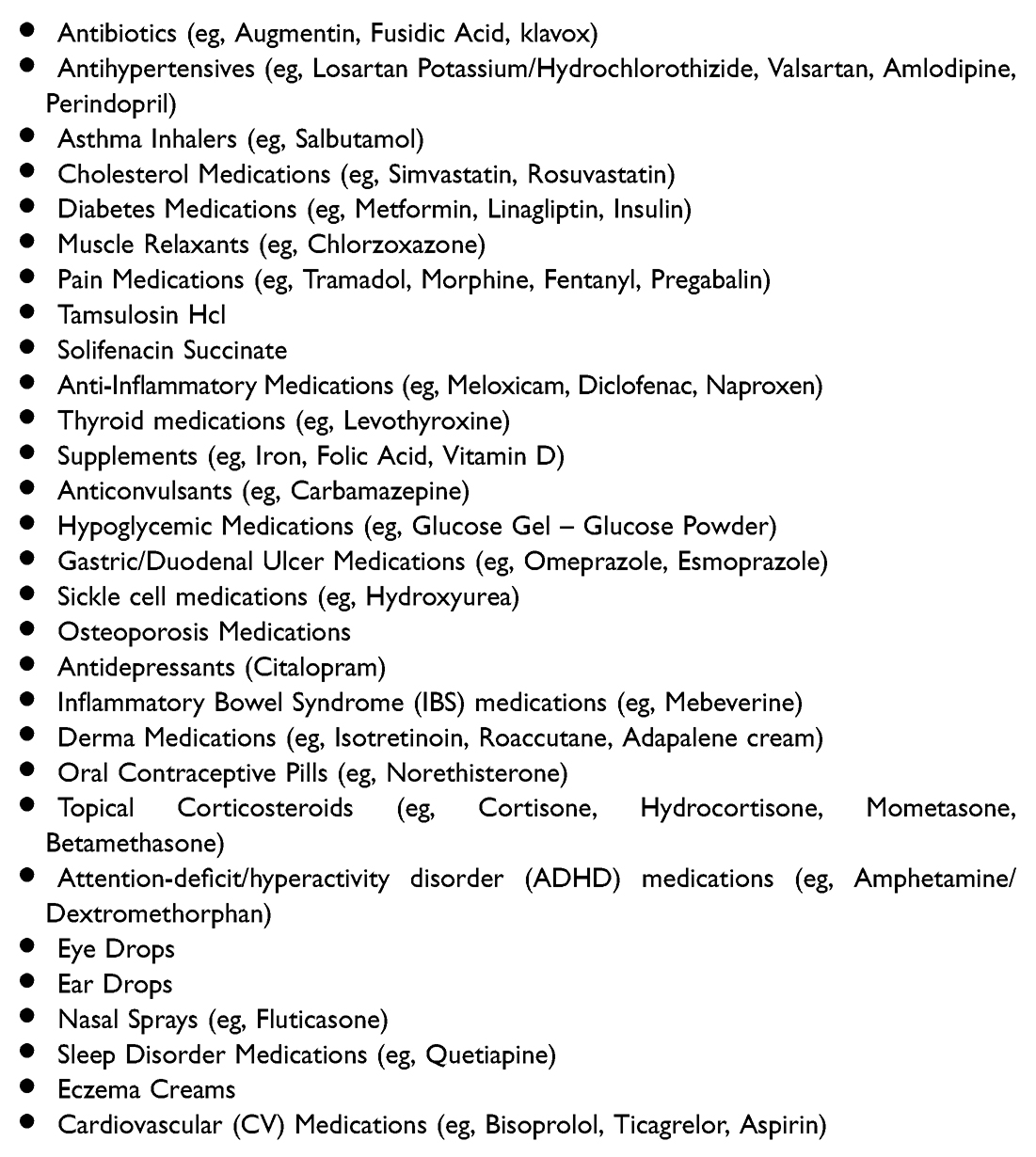 |
Box 1 List of Medicines Shared by Study Participants |
Perceived Facilitators of Sharing Medicines
Facilitators of medication sharing included saving time and cost, limited access to medicines and health services, the availability of leftover medicines, socio-cultural factors, and prior experience or knowledge about the illness and its treatment. Some were speculations as to the reasons that facilitate sharing, while others were based on actual stories. These are described below and summarized in Table 2.
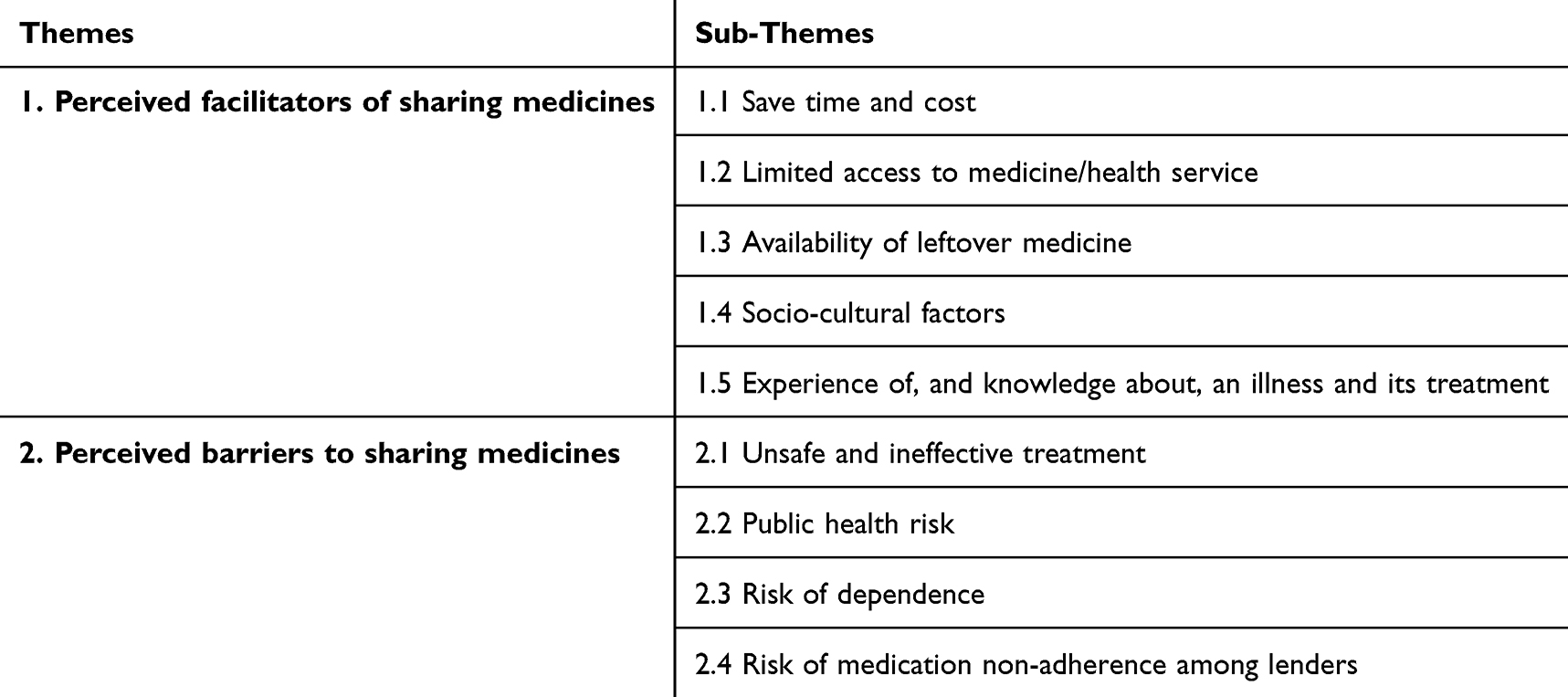 |
Table 2 Main Themes and Sub-Themes Emerged from Data Analysis |
It is important to note that participants’ motivations for sharing medicines were often multifaceted, with overlapping patterns across these themes. For example, using leftover medicines at home could reflect not only a desire to save time and cost, but also a way to overcome limited access to health services. Similarly, avoiding general practitioner consultations might address convenience and cost-saving, while also relating to healthcare access challenges. Sharing during emergencies was also a cross-cutting factor linked to both saving time and cost, as well as limited access to health services. The sub-themes are presented separately for clarity, but their interconnections are acknowledged, reflecting the complexity of participants’ experiences.
Save Time and Cost
Participants shared prescription medicines to avoid GP consultations, citing convenience, similar symptoms to those of the lender, or the availability of leftover medicines. For example, one participant preferred to borrow pain medication from her husband for familiar symptoms before consulting a doctor. Another, who disliked visiting doctors since childhood, irregularly refilled her metformin and instead borrowed it from her mother when she ran out [Table 3, quote 1].
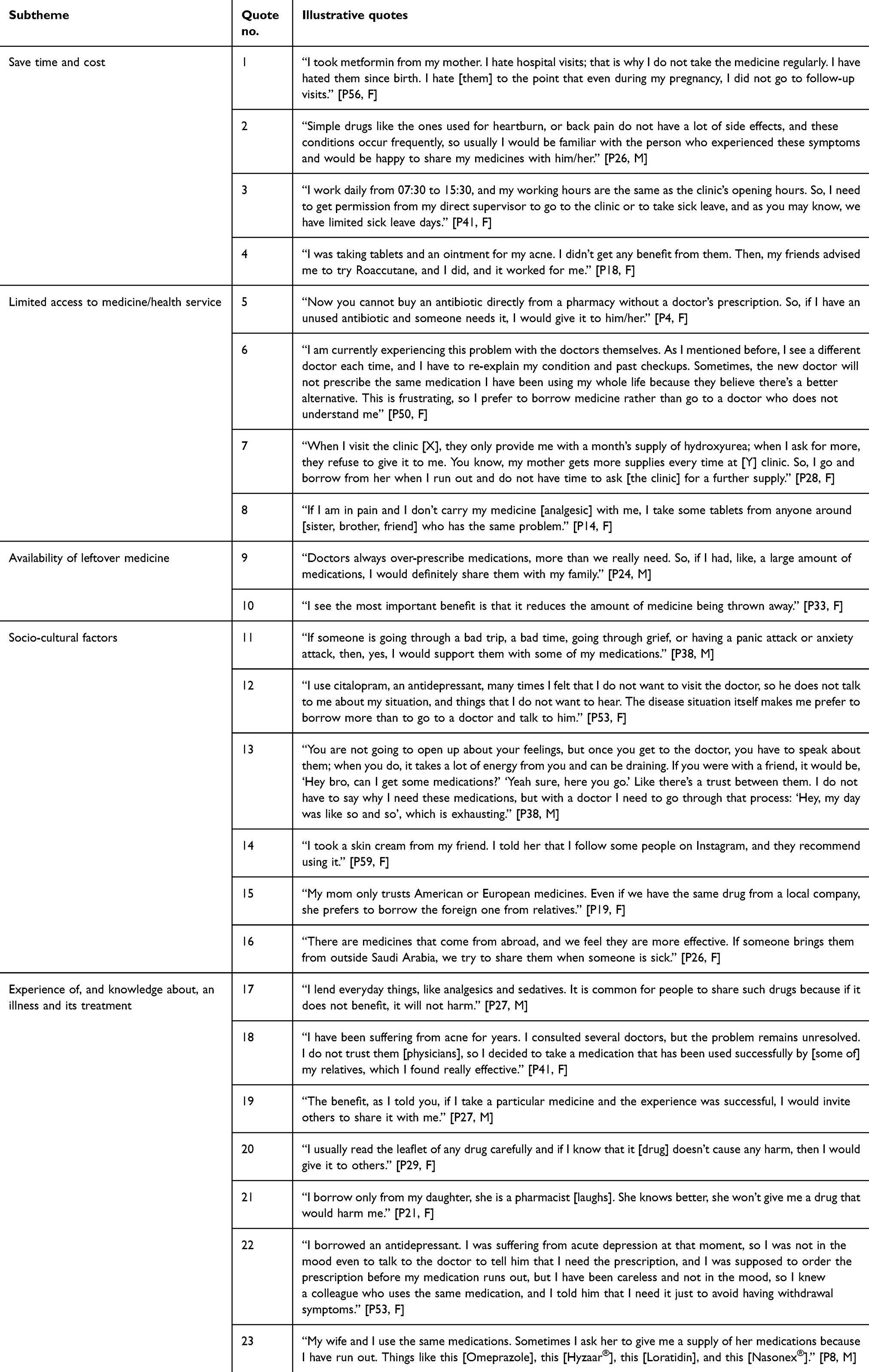 |
Table 3 Quotes Illustrating Perceived Facilitators of Medicine Sharing |
Sharing was seen as acceptable for minor conditions like pain and gastrointestinal issues [Table 3, quote 2]. In this quote, the participant was referring to prescription medication provided to her by her husband, not an OTC product. Some preferred sharing to avoid taking time off work, given conflicting working hours and healthcare access [Table 3, quote 3]. Others shared widely known medicines to try before obtaining their own supply [Table 3, quote 4].
Limited Access to Medicine/Health Services
Drug shortages, prescription restrictions for antibiotics, transportation issues, discontinuity of care, long waiting times to see a doctor or obtain an appointment, and limited availability of appointments after hours, on weekends, and during religious and official holidays also influenced participants’ sharing practices. In Saudi Arabia, there is a new regulatory enforcement law that bans the buying or selling of antibiotics without a prescription. People who used to buy them without a prescription before this regulatory enforcement demonstrated the tendency to borrow them instead of seeking a medical prescription. Some participants reported seeking medical advice from a doctor for the first episode of a specific illness. When they experienced similar symptoms again, they felt comfortable borrowing antibiotics from others instead of revisiting a doctor for a similar symptom complex. Others reported having had previous successful experiences with certain antibiotics, which led them to prefer borrowing them instead of visiting a doctor and requesting a prescription [Table 3, quote 5].
Discontinuity of care and frequent physician rotations led some participants to prefer sharing medicines over attending repeated consultations. This was often justified by the repeated tests and examinations ordered by each new physician. In some cases, this resulted in patients receiving different medications from those previously prescribed [Table 3, quote 6].
Sharing was also reported during travel emergencies when participants forgot, lost, or ran out of their medicines and could not visit their doctor in time. In such cases, they borrowed a few pills to maintain their dosing regimen until they could obtain a new supply. The unavailability of certain medications—such as psychotropic drugs—or of specific dosages or strengths at government pharmacies, as well as delays in renewing prescriptions after supplies ran out, were seen as emergencies that led to sharing. In particular, the standard 28-day prescription length was viewed by some participants as problematic, as it did not meet individual needs and contributed to running out of medications. One participant noted inequalities in how hospitals dispensed supplies, with some providing larger quantities than others, which further encouraged sharing [Table 3, quote 7]. Sharing was also seen as beneficial in urgent situations, such as severe pain episodes or asthma attacks, where narcotics or inhalers were provided to those in need [Table 3, quote 8].
Availability of Leftover Medicines
Many participants reported sharing leftover medications for various reasons. Some stopped treatment early, such as a participant who gave her remaining antibiotics to someone else after she felt better. Others had excess medicines due to refusing prescribed treatments or receiving more than needed from refills. Several participants believed doctors overprescribed without thoroughly assessing necessity, leading to leftover medicines that were shared with those in need [Table 3, quote 9]. Additionally, a lack of clear disposal options and a desire to avoid waste motivated sharing, as one participant explained that the most important benefit of sharing was reducing the amount of medicine being thrown away [Table 3, quote 10].
Socio-Cultural Factors
Providing social support was a key motivator for PMS. Participants viewed sharing medicines with family and close friends as a way to care for loved ones, particularly those with chronic conditions or during times of interrupted supply, such as shortages, delays in refills, or emergencies [Table 3, quote 11]. A wide range of medications—including insulin, thyroxine, salbutamol inhalers, metformin, and even narcotics—were shared for these reasons.
Cultural beliefs also shaped sharing practices. For example, in sensitive conditions like depression, some participants avoided approaching medical care due to stigma, fear of judgment, or the emotional difficulty of discussing their struggles. Instead, they found it easier to borrow medicines from trusted friends or family members [Table 3, quotes 12 and 13]. Related cultural values, such as the belief among some elderly individuals that a medicine that benefits one person will help others, further encouraged sharing.
Modern influences, such as social media, also played a role. Some participants borrowed prescription-only dermatological treatments, such as medicated skin creams or acne medications, after seeing them promoted on platforms like Instagram [Table 3, quote 14]. Finally, perceptions about the quality of medicine influenced sharing—several participants believed Western brands were more effective than local alternatives, which sometimes led to lending medications viewed as superior [Table 3, quotes 15 and 16].
Experience of, and Knowledge About, Illness and Its Treatment
Perceived experience with an illness or its treatment was a key facilitator of medication sharing. Participants who felt knowledgeable about their condition—often due to long-term experience—believed they could judge whether sharing a medicine was safe, particularly when lending to others with the same condition. However, some were cautious about sharing with individuals who had complex illnesses, such as sickle cell disease, due to fears of harmful consequences. Others viewed certain medications, such as gastrointestinal tablets, as safe because they had few side effects.
Participants’ attitudes toward specific medicines also influenced their willingness to share. Analgesics, sedatives, and antibiotics were commonly shared, as many perceived them as safe and viewed sharing as a way to maintain good relationships. One participant described this perception by stating that such medicines are shared because “if it does not benefit, it will not harm” [Table 3, quote 17]. Those unaware of the risks, such as antibiotic resistance, misdiagnosis, or side effects, were generally more open to sharing. At the same time, participants who were more conscious of these dangers expressed caution or avoided sharing altogether.
Participants’ attitudes toward specific medicines also influenced their willingness to share. Analgesics, sedatives, and antibiotics were commonly shared, as many viewed this as safe and a way to maintain good relationships. Those unaware of the risks (eg, antibiotic resistance, misdiagnosis, side effects) were more willing to share, while those conscious of these dangers avoided sharing [Table 3, quote 17].
Prior positive experiences with a medicine also encouraged sharing. This attitude was reinforced by a cultural belief captured in the Arabic idiom: “Ask an experienced person and do not ask a doctor.” Many participants consulted family, friends, or colleagues with similar illnesses when seeking or lending medicines [Table 3, quotes 18 and 19].
Health literacy further shaped sharing practices. Some participants read medication leaflets or researched medicines to assess the safety of sharing [Table 3, quote 20]. Others trusted healthcare professionals within their family or circle, believing that medicines shared by them would be safe [Table 3, quote 21]. Finally, sharing was often based on symptom similarity or use of the same medicine, with participants assuming this made sharing safer [Table 3, quotes 22 and 23].
Perceived Barriers to Sharing Medicines
Participants reported several barriers to medication sharing (Table 4). Some barriers were hypothetical scenarios, while others were based on patients’ own experiences. These barriers were classified into four sub-themes: unsafe and ineffective treatment, public health risk, risk of dependence, and risk of medication non-adherence among lenders.
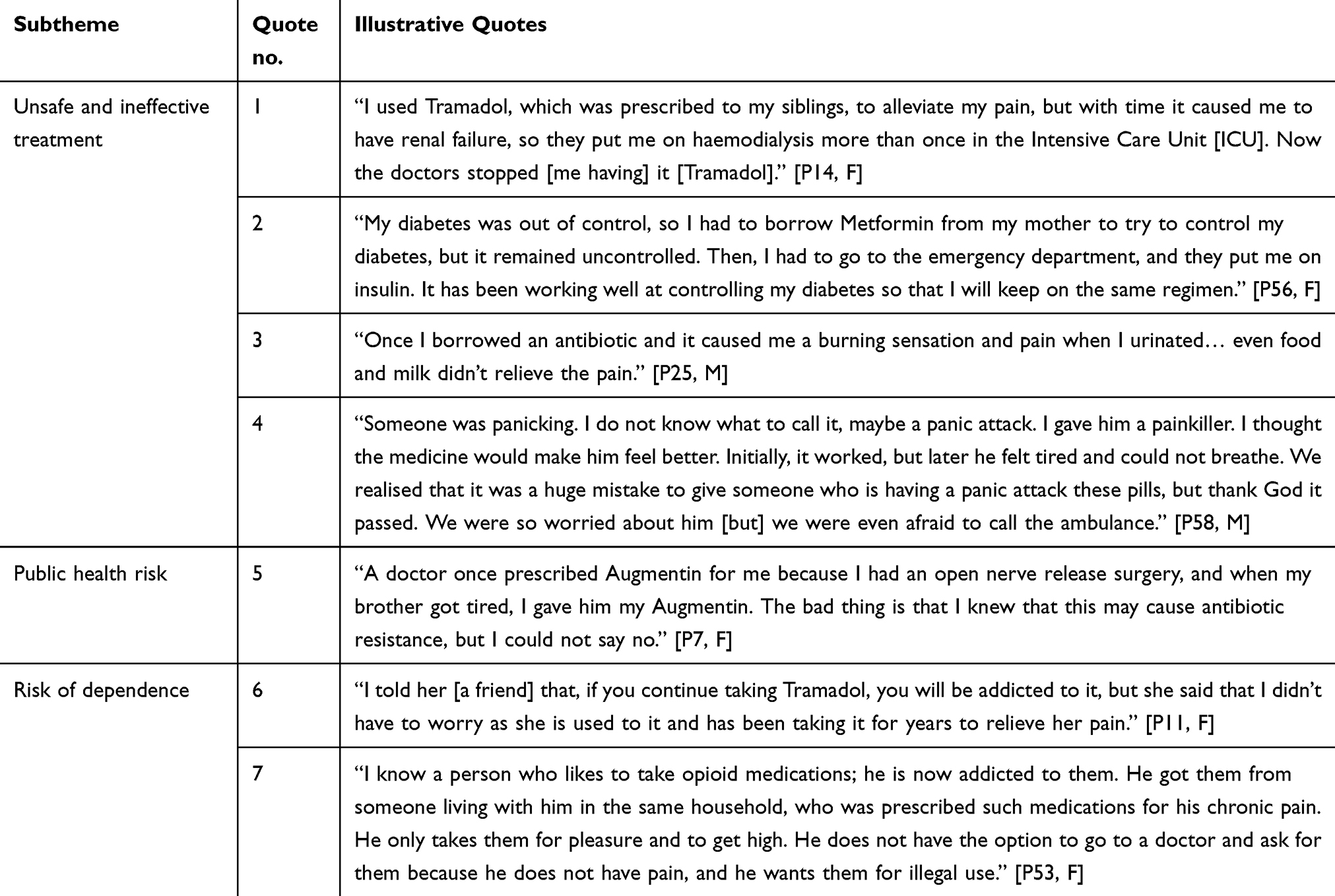 |
Table 4 Quotes Illustrating Perceived Barriers to Medicine Sharing |
Unsafe and Ineffective Treatment
Although participants shared medicines with good intentions—such as helping relatives and friends, offering social support, or saving time and money—many described negative consequences that resulted from this practice. Sharing between individuals without medical training could lead to inaccurate diagnoses, inappropriate doses, or unsuitable treatments. For example, a borrowed medicine might be contraindicated, or cause hypersensitivity, adverse reactions, or dangerous interactions with other medicines.
Some participants experienced serious outcomes from sharing. One borrowed Tramadol from her siblings for pain relief and later developed renal failure, requiring haemodialysis [Table 4, quote 1]. Another borrowed metformin from her mother, but her diabetes remained uncontrolled until she sought emergency care and was prescribed insulin [Table 4, quote 2].
Participants also reported adverse reactions, which they could often link to specific medicines. These included mild issues like digestive disturbance and fatigue, moderate reactions such as rashes and difficulty urinating, and severe, life-threatening problems like breathing difficulties. Pain medications, opioids, and antibiotics were most commonly associated with these harms, yet participants tended to underestimate their risks [Table 4, quotes 3, 4].
While sharing pills was generally seen as riskier, some participants believed topical medicines were safe to share. However, as skin thins with age, even creams and ointments can pose dangers because they may be absorbed more rapidly.
Public Health Risk
Some participants viewed sharing certain prescription medications as unhygienic, particularly for items such as asthma inhalers, antihistamine nasal sprays, or drops. One participant, for instance, chose not to borrow an inhaler during a breathing emergency out of concern for spreading infection. Another said he would only lend medicines to family or close friends with the same condition, or in an emergency.
Beyond hygiene concerns, participants also highlighted the broader public health risks of sharing medicines. Several noted that sharing antibiotics can contribute to the development of antibiotic resistance, making infections more challenging to treat. Despite recognizing this risk, one participant admitted to continuing the practice [Table 4, quote 5].
Risk of Drug Dependence
Participants mentioned a few incidences of medication sharing that resulted in dependence or addiction when participants took the medication regularly. The main types of medicines that led to dependence or addiction were certain pain relief medications (opioids). The most common way that participants reported obtaining these types of drugs involved receiving pills from a family member or someone known personally to them and well enough to be described as a friend. Such medication came from individuals who themselves had a prescription for it, and the medication typically consisted of more than a few pills, as illustrated in the following quotes [Table 4, quotes 6, 7].
Risk of Medication Non-Adherence Among Lenders
An example of this was a woman who visited a pharmacy to request a refill of her insulin and metformin. She said that the pharmacist told her that she had already been provided with a supply of these medications, but she claimed that she had run out because she was sharing them with her husband, who was also prescribed them. She said that this behaviour sometimes prevented her from taking her medications as prescribed.
Discussion
This is the first qualitative study in Saudi Arabia to explore in depth the facilitators and barriers of PMS behaviors among the general public. Our findings align with previous studies that have reported a wide range of commonly shared medicines, including antibiotics, analgesics, and psychotropics.1–3,5,7–9,11,12,22–27 However, while some participants in our study viewed PMS as an appropriate or helpful act despite potential risks, this contrasts with prior research conducted from healthcare providers’ perspectives, which has predominantly characterized PMS as risky, harmful, and undesirable.3,27
Building on this contrast, our study offers unique insights into the lived experiences, motivations, and socio-cultural context that influence PMS in Saudi Arabia, providing a broader and more comprehensive understanding than prior provider-centered research.3,27 Participants’ decisions to lend or borrow medicines were shaped not only by perceived medical need but also by strong family ties, cultural expectations of generosity, convenience, and previous experiences with illness. These findings provide a foundation for developing culturally sensitive interventions that address both the potential risks of PMS and the enduring social values that drive it.
Several factors have been identified that may influence PMS practices, giving an imaginary picture of a patient who is more likely to lend or borrow prescription medications. Some of these factors were broadly in accordance with evidence from the international literature,1–9,11,12,18,19,22–27 although some differences were also found, which may be specific to the Saudi population. For example, in line with the international literature, keeping leftover medicine for “next time”, lack of information about safe disposal, effect of advertisements/internet, and limited access to medicine/healthcare services due to cost, access issues, travelling and forgetfulness were all found to be possible reasons for PMS. Doctors over-prescribing medicines, brands or country of origin of medications, misuse of medical insurance, accumulation of unused medicines at home, strong family ties, cultural expectations of generosity, reluctance to discuss sensitive issues with healthcare professionals due to stigma, and individual knowledge and previous experiences with illness/medicines in deciding whether to share—were all found to be factors specific to the Saudi population that influence prescription medication sharing.
Identifying factors that contribute to PMS is important in developing tailored intervention programmes to prevent this behaviour or at least minimise the risk associated with it. In understanding these influences, it becomes clear that a single driver rarely shapes PMS behavior; instead, it emerges from the interplay of multiple overlapping factors. We also note that the themes often overlapped, as many participants’ experiences were linked to multiple motivators. For instance, actions like borrowing leftover medicines or avoiding GP consultations reflected overlapping concerns about cost, convenience, and access. This interconnectedness highlights the complexity of prescription medication sharing behavior, as a single factor rarely drove participants’ decisions.
Together, these contributing factors not only influence sharing behaviors but also shape participants’ perceptions of the risks associated with PMS, which are often underestimated. Such risks include inappropriate or delayed treatment, adverse drug reactions and interactions, addiction to shared opioids or stimulants, antibiotic resistance from uncontrolled antibiotic use,1,3,5,13,14,26–29 and teratogenic risks from medications like isotretinoin among women of childbearing age.12 Escalating doses of shared opioids could also contribute to life-threatening complications, including respiratory depression and death.26,27
Building on these findings, we propose several approaches for healthcare providers and policymakers that are directly informed by the identified themes. Regarding unsafe and ineffective treatment and the associated public health risks, healthcare providers should identify high-risk medications—such as antibiotics, opioids, and non-steroidal anti-inflammatory drugs (NSAIDs)—at the time of prescribing, dispensing, and medicine reconciliation, and provide targeted counseling that discourages sharing and emphasizes the associated risks. This recommendation is supported by international studies that highlight how targeted interventions, including identifying “at risk” medications, medication reviews, and patient counseling, can reduce medication misuse, sharing, and associated harms such as dependence and adverse reactions.5,6 For example, Ellis and Mullan (2009) noted that healthcare provider engagement is crucial in reducing prescription sharing by promoting understanding of medication risks.7 Similarly, Bekker et al (2018) emphasized that pharmacists’ involvement in identifying medications prone to misuse contributes to harm reduction by limiting inappropriate use and promoting safe disposal.30
While such approaches are promising, their feasibility and impact within the Saudi Arabian healthcare system have not yet been systematically evaluated. The absence of national guidelines or structured programs focusing specifically on PMS highlights a gap in policy and practice. Further research is therefore needed to assess how measures such as labeling warnings against sharing, provider counseling on the risks of sharing, and system-level interventions, including take-back schemes, can be effectively integrated into existing healthcare services in Saudi Arabia. This would help ensure that proposed interventions are both culturally appropriate and practical within the local context.
Participants described barriers such as limited access to medicines and health services, along with efforts to save time and reduce costs. These accounts support the need for strategies to improve timely access to care, such as extending clinic hours and streamlining prescription refill processes, in order to reduce reliance on shared medications. The prevalence of unused medicines further reinforces the need for prescribers to limit excessive refills, educate patients on safe disposal practices, and support the implementation of national take-back programs.5 These findings suggest that overprescribing, excessive medication refills, a lack of patient education on proper disposal, and, in some cases, the misuse of medical insurance collectively contribute to the accumulation of leftover medicines and the practice of sharing prescription medications. Interventions should therefore include not only public awareness campaigns and take-back schemes, but also system-level strategies to improve prescribing practices, monitor refill policies, and ensure appropriate insurance use to reduce unnecessary medication surplus. Finally, given the strong moral and cultural drivers of sharing, educational campaigns should be designed to align with local values, promote safe practices, and engage trusted community figures and family networks in messaging to ensure their relevance and effectiveness.
Beyond access barriers and cultural norms influencing sharing, participants’ perceptions of medication quality also shaped their behaviors and choices. In this study, some participants expressed a preference for Western-branded medicines, perceiving them as more effective than local alternatives. This perception appeared to originate from their own experiences or those of their relatives, who believed that Western medicines produced better therapeutic results. Such views may also reflect broader societal beliefs about the quality of imported versus locally manufactured medicines, despite regulatory controls by the Saudi Food and Drug Authority (SFDA) that ensure the bioequivalence, safety, and effectiveness of generic medicines.31
These perceptions could be linked to the lower price of generics compared to brand-name medicines and a lack of public awareness about their equivalence.32,33 Similar views have been reported among Saudi patients regarding antibiotics14 and among Kuwaiti patients with type 2 diabetes mellitus regarding diabetes medications,34 but this issue remains underexplored in the literature.
Saudi Arabia has a government-funded healthcare system that provides free medical care and prescription medicines to all citizens. Healthcare services are delivered through a network of primary care centers, hospitals, and specialized facilities overseen by the Ministry of Health (MOH) and regulated by the Saudi Food and Drug Authority (SFDA), which is responsible for ensuring the quality of medicines.31,32 The system allows direct access to healthcare professionals, and there are no formal policies that restrict or limit the general public from seeking medical advice or treatment. However, healthcare-seeking behaviors may be shaped by cultural, social, and personal factors, such as privacy concerns, perceived stigma (particularly for mental health conditions), or prior experiences with the healthcare system.
Supporting the use of generic medicines is a key priority under Vision 2030, aimed at localizing pharmaceutical manufacturing and reducing healthcare costs.31,32 However, with only about 30% of pharmaceuticals produced locally, there is a clear need to strengthen generic medicine frameworks, increase public confidence in generics, and expand local production capacity.31,32 Despite the comprehensive nature of the healthcare system, a theme that emerged from our interviews was the overprescribing of medications by doctors, sometimes without thoroughly assessing whether they were necessary. This contributed to the accumulation of unused medicines, which patients subsequently shared with others. Over-prescribing in Saudi Arabia has been linked to several factors, including high patient expectations—studies show that 88% of patients expect a prescription during primary care consultations—and doctors’ efforts to meet these expectations to avoid dissatisfaction or losing patients to other providers.35 Additional contributors include incorrect diagnoses (eg, prescribing antibiotics for viral infections), prescribing by non-specialist practitioners, the provision of free medicines, and limited use of local prescribing guidelines or awareness of international standards such as the Beers, START, or STOPP criteria.30,36
Addressing these challenges requires coordinated efforts from healthcare professionals, policymakers, and the public. Doctors and pharmacists should play a central role in addressing patients’ brand preferences and concerns, reassuring them about the safety and quality of generic medicines, and limiting prescriptions to what is truly needed. Effective doctor-patient communication is crucial for managing expectations, avoiding unnecessary prescriptions, and discussing appropriate dosages of medications. Regular review of prescribed therapies, limiting quantities of high-risk or expensive medications, and setting shorter prescription durations can help reduce leftovers that might otherwise be shared.5,30 Clinical pharmacists should be more involved in the prescription process and supported by user-friendly tools and computerized alert systems to identify potentially inappropriate prescribing.33
Building on these coordinated efforts, it is equally important to highlight how healthcare professionals, particularly pharmacists, can further contribute to empowering patients and supporting rational medication use. In addition to revising national policy to address over-prescribing, our findings highlight the important role that healthcare professionals, particularly pharmacists, can play in empowering patients within the current healthcare system. As trusted and accessible medication experts, pharmacists are well-positioned to provide counseling on the risks of sharing medicines, encourage adherence to prescribed treatments, and educate patients on safe storage and disposal practices.1–3 Their involvement in medication reviews, prescription audits, and efforts to promote the use of cost-effective generic medicines could further help reduce the accumulation of leftover medicines that may otherwise be shared.1,6,7 From the public’s perspective, our study underscores the need for individuals to take a more active role in safeguarding their health by seeking medical advice before using medications not prescribed for them, asking healthcare providers or pharmacists about the safe use of their medications, and resisting social or moral pressures to share prescription medicines. Public engagement in educational initiatives and awareness campaigns aimed at promoting rational medication use and harm reduction is essential for achieving meaningful change.5,6
These individual and professional actions should be complemented by broader public health initiatives and policies designed to reinforce safe medication practices at the community level. Public awareness campaigns and educational resources—including posters, brochures, and online materials—can help promote rational use of medicines, improve understanding of generic medicines, and encourage safe disposal of unused drugs. Establishing a national medication disposal policy, including pharmacy-based take-back initiatives, is a priority. Collaboration among the MOH, SFDA, and other relevant agencies is necessary to develop and oversee such a program. Providing patients with information on safe disposal during medication counseling is also vital.
While such public health measures are essential for promoting safe medication practices, it is also crucial to address social and cultural barriers—such as stigma—that influence how and why individuals engage in behaviors like prescription medication sharing. In addition, the study highlighted the role of stigma associated with mental illness as a barrier to seeking professional care, leading some individuals to prefer borrowing medicines from family or friends. This reflects broader concerns about the support available to patients with mental health conditions. The widespread stigma across Arab countries37–39 and reliance on family support over professional help40–43 are linked to cultural values around privacy and fear of prejudice from healthcare providers. While Saudi Arabia has a well-established healthcare system, these findings emphasize the need for healthcare providers to integrate cultural values into care plans, promote public awareness to reduce stigma, and improve access to mental health services.4–47 Strategies might include integrating mental health into general health services, launching media campaigns, and incorporating mental health sciences into academic curricula.38,44,45
Alongside addressing stigma and cultural influences, our findings point to the significant role of individual knowledge and educational background in shaping medication sharing behaviors. Our analysis further revealed that participants’ knowledge and educational background played a dual role in shaping sharing behavior. For some, confidence in their understanding of an illness or its treatment encouraged them to share, as they believed they could assess its safety. For others, limited health literacy, incomplete awareness of risks, or reliance on anecdotal evidence facilitated the sharing of information, sometimes inappropriately. These insights underscore the importance of educational strategies that address both overconfidence and knowledge gaps to promote safer behaviors.
Addressing these educational needs is closely tied to improving understanding of the actual harms that may result from medication sharing, an area that remains insufficiently explored. Little is known about the frequency and severity of adverse drug reactions (ADRs) resulting from shared medicines—this is an important area for future research, as some ADRs reported by participants were potentially serious or lethal. Future studies should also explore how patients assess the risks and benefits of sharing medicines and how HCPs can better identify and address sharing behaviors through improved communication. In everyday practice, HCPs should reinforce the importance of taking medicines as prescribed, discourage lending or borrowing of prescription medicines, and provide non-judgmental counseling about the risks of sharing and safe disposal practices.
The study’s findings directly address the research objectives by identifying key facilitators, such as cultural obligations, healthcare access, and prior experience with illness, and barriers, including safety concerns, risk awareness, and fear of dependence. These results align with global literature1–12,47 yet provide additional insight into how cultural norms, family networks, and system-level factors uniquely shape prescription medication sharing in Saudi Arabia. While the findings are context-specific and not generalizable, they offer valuable guidance for policymakers and healthcare providers seeking to design culturally grounded educational campaigns, prescribing practices, and national medication take-back initiatives to reduce sharing and promote safer use.
Strength and Limitations
This study has several notable strengths. This is the first qualitative investigation to explore in depth the facilitators and barriers of PMS among adults in Saudi Arabia, thereby providing a crucial foundation for future policy, practice, and interventions. The use of both one-to-one and telephone interviews allowed participants flexibility, encouraged wider involvement of household members, and fostered a more comfortable atmosphere that supported openness when discussing sensitive issues.
At the same time, some limitations should be considered. The study sample was restricted to Saudi participants from the Eastern Province, which may limit the generalizability of findings to the broader population or to non-Saudi residents. In addition, although the three interviewers were trained to follow the same approach, minor inconsistencies in data collection cannot be entirely excluded. Moreover, the reliance on a convenience sample of 60 participants, supplemented by snowball sampling, may have limited the diversity of perspectives captured and introduced potential bias. Resource constraints also prevented the use of alternative recruitment strategies. Future studies could benefit from employing a broader or stratified sampling strategy to improve representativeness and strengthen the generalizability of findings. Furthermore, the sample was not fully representative of the general population, as most participants were female, relatively young, and highly educated. Finally, because some participants were recruited through pharmacy students, there is a possibility of bias if their families had greater awareness of medication use; however, efforts were made to reduce this by promoting recruitment across the entire university to capture participants with varied backgrounds.
Conclusion
This study provides the first qualitative insight into prescription medication sharing in Saudi Arabia, exploring the facilitators and barriers among the general public and illustrating how cultural, social, and structural factors interact to shape this behavior. Several overlapping factors influenced PMS practices, reflecting a complex interaction of individual, cultural, and system-level drivers. While some factors aligned with international findings, others—such as doctors over-prescribing medicine, brands or country of origin of medications, misuse of medical insurance, accumulation of unused medicines at home, strong family ties, cultural expectations of generosity, reluctance to discuss sensitive issues with healthcare professionals due to stigma, and individual knowledge and previous experiences with illness/medicines in deciding whether to share—appeared more specific to the Saudi context. Recognizing these influences is essential for developing culturally sensitive interventions that minimize the risks of PMS while respecting the values that contribute to this practice. Accordingly, the findings highlight the need for tailored public health campaigns, enhanced patient education on safe medicine use and disposal, and the implementation of national medication take-back programs.
While the findings are not generalizable due to the use of a convenience sample, they offer a foundation for future studies using larger and more diverse populations to validate and extend these results. Future research should also explore whether healthcare providers identify similar factors influencing PMS behavior and examine potential differences in attitudes and practices across age groups. In addition, quantitative studies are needed to assess the prevalence, frequency, and patterns of PMS across broader and more diverse populations.
Funding
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Beyene KA, Sheridan J, Aspden T. Prescription medication sharing: a systematic review of the literature. Am J Public Health. 2014;104(4):e15–26. doi:10.2105/AJPH.2013.301823
2. Gascoyne A, Beyene K, Stewart J, Aspden T, Sheridan J. Sharing prescription medicines: results of a survey of community pharmacy clients in Auckland, New Zealand. Int J Clin Pharm. 2014;36(6):1268–1276. doi:10.1007/s11096-014-0031-x
3. Beyene KA, Aspden TJ, Sheridan JL. A qualitative exploration of healthcare providers’ perspectives on patients’ non-recreational, prescription medicines sharing behaviours. J Pharm Pract Res. 2018;48(2):158–166. doi:10.1002/jppr.1376
4. Goldsworthy RC. Recreational versus nonrecreational prescription borrowing: time for an expanded conceptualization? J Adolesc Health. 2010;46(4):402. author reply 403. doi:10.1016/j.jadohealth.2009.12.016
5. Beyene K, Aspden T, Sheridan J. Prescription medicine sharing: exploring patients’ beliefs and experiences. J Pharm Policy Pract. 2016;9(1):23. doi:10.1186/s40545-016-0075-5
6. Beyene K, Aspden T, McNeill R, Sheridan J. Modifiable risk factors for prescription medicine sharing behaviours. Res Social Adm Pharm. 2019;15(2):154–163. doi:10.1016/j.sapharm.2018.04.005
7. Ellis J, Mullan J. Prescription medication borrowing and sharing: risk factors and management. Aust Fam Physician. 2009;38(10):816–819.
8. Goldsworthy RC, Mayhorn CB. Prescription medication sharing among adolescents: prevalence, risks, and outcomes. J Adolesc Health. 2009;45(6):634–637. doi:10.1016/j.jadohealth.2009.06.002
9. Goldsworthy RC, Schwartz N, Mayhorn CB. Beyond abuse and exposure: framing the impact of prescription-medication sharing. Am J Public Health. 2008;98(6):1115–1121. doi:10.2105/AJPH.2007.123257
10. Mayhorn CB, Goldsworthy RC. Borrowing prescription medication: implications for healthcare warnings and communications. Proc Hum Factors Ergon Soc Annu Meet. 2009;53(20):1608–1611. doi:10.1177/154193120905302014
11. Ward L, Patel NM, Hanlon A, Eldakar-Hein S, Sherlinski K, Ward SH. Prescription medication borrowing among adult patients at an urban medical center. J Urban Health. 2011;88(6):997–1014.
12. Petersen EE, Rasmussen SA, Daniel KL, Yazdy MM, Honein MA. Prescription medication borrowing and sharing among women of reproductive age. J Womens Health. 2008;17(7):1073–1080. doi:10.1089/jwh.2007.0769
13. Alhomoud F. ‘Sharing may not be caring’ – prescription medication sharing among adults in Saudi Arabia. Int J Pharm Pract. 2020;28(3):255–266. doi:10.1111/ijpp.12592
14. Alhomoud F, Aljamea Z, Almahasnah R, Alkhalifah K, Basalelah L, Alhomoud FK. Self-medication and self-prescription with antibiotics in the Middle East: do they really happen? A systematic review of the prevalence, possible reasons, and outcomes. Int J Infect Dis. 2017;57:3–12. doi:10.1016/j.ijid.2017.01.014
15. Almutairi AF, McCarthy A, Gardner GE. Understanding cultural competence in a multicultural nursing workforce: registered nurses’ experience in Saudi Arabia. J Transcult Nurs. 2015;26(1):16–23. doi:10.1177/1043659614523992
16. Walston S, Al-Harbi Y, Al-Omar B. The changing face of healthcare in Saudi Arabia. Ann Saudi Med. 2008;28(4):243–250. doi:10.5144/0256-4947.2008.243
17. Kheir N, El Hajj M, Wilbur K, Kaissi R, Yousif A. An exploratory study on medications in Qatar homes. Drug Health Patient Saf. 2011;3:99–106. doi:10.2147/DHPS.S25372
18. Dawson S, Johnson H, Huntley AL, Turner KM, McCahon D. Understanding non-recreational prescription medication-sharing behaviours: a systematic review. Br J Gen Pract. 2024;74(740):e183–8. doi:10.3399/BJGP.2023.0189
19. Markotic F, Vrdoljak D, Puljiz M, Puljak L. Risk perception about medication sharing among patients: a focus group qualitative study on borrowing and lending of prescription analgesics. J Pain Res. 2017;10:365–374. doi:10.2147/JPR.S123554
20. Sperber AD. Translation and validation of study instruments for cross-cultural research. Gastroenterology. 2004;126(Suppl 1):S124–S128. doi:10.1053/j.gastro.2003.10.016
21. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
22. Sørensen K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12(1):80. doi:10.1186/1471-2458-12-80
23. Goulding E, Murphy M, Di Blasi Z. Sharing and borrowing prescription medication: a survey of Irish college students. Ir J Med Sci. 2011;180(3):687–690. doi:10.1007/s11845-011-0698-0
24. Auta A, Banwat SB, Francis RA. Prevalence of prescription medication sharing behaviour among students. Int J Pharm Life Sci. 2011;2(4):651–654.
25. Hogan DJ, Moreland A, Lane P, Lal S. Exchange of prescription medications by dermatology outpatients. J Am Acad Dermatol. 1990;23(5):953. doi:10.1016/S0190-9622(08)80715-3
26. Thompson S, Stewart K. Prescription medication use practices among non‐institutionalised older persons. Int J Pharm Pract. 2001;9(3):141–151. doi:10.1111/j.2042-7174.2001.tb01042.x
27. Markotic F, Jurisic D, Curkovic M, et al. Sharing of prescription analgesics amongst patients in family practice: frequency and associated factors. Eur J Pain. 2018;22(4):716–727. doi:10.1002/ejp.1157
28. Markotic F, Puljak L. Risks associated with borrowing and sharing of prescription analgesics among patients observed by pain management physicians in Croatia: a qualitative study. J Pain Res. 2016;9:1143–1151. doi:10.2147/JPR.S118945
29. Alhomoud F, Almahasnah R, Alhomoud FK. You could lose when you misuse – factors affecting over-the-counter sale of antibiotics in community pharmacies in Saudi Arabia: a qualitative study. BMC Health Serv Res. 2018;18(1):915. doi:10.1186/s12913-018-3753-y
30. Al-Mohamadi A, Al-Harbi AM, Manshi AM, Rakkah MM. Medications prescribing pattern toward insured patients. Saudi Pharm. J. 2014;22(1):27–31. doi:10.1016/j.jsps.2013.01.002
31. Alhomoud F, Dhillon S, Aslanpour Z, Smith F. South Asian and Middle Eastern patients’ perspectives on medicine-related problems in the United Kingdom. Int J Clin Pharm. 2015;37(4):607–615. doi:10.1007/s11096-015-0103-6
32. Alrasheedy AA, Hassali MA, Wong ZY, Aljadhey H, Al-Tamimi SK, Saleem F. Pharmaceutical policy in Saudi Arabia. In: Babar ZUD, editor. Pharmaceutical Policy in Countries with Developing Healthcare Systems. Cham: Adis; 2017:329–347.
33. Alghasham AA. Generic drug prescribing in central Saudi Arabia: perceptions and attitudes of physicians. Ann Saudi Med. 2009;29(1):24–30. doi:10.4103/0256-4947.51819
34. Jeragh-Alhaddad FB, Waheedi M, Barber ND, Brock TP. Barriers to medication taking among Kuwaiti patients with type 2 diabetes: a qualitative study. Patient Prefer Adherence. 2015;9:1491–1503. doi:10.2147/PPA.S86719
35. Jastaniah NA, Almaqati AS, Alsuraihi AK, Abughanim SA, Aseeri M. Inappropriate prescribing in elderly inpatients at a university hospital in Saudi Arabia. Drugs Real World Outcomes. 2018;5(4):211–216. doi:10.1007/s40801-018-0142-0
36. Kalantan KA. Expectations of Saudi patients for medications following consultations in primary health care in Riyadh. J Family Community Med. 2002;9(3):27–33. doi:10.4103/2230-8229.97915
37. Bekker CL, Gardarsdottir H, Egberts ACG, Bouvy ML, van den Bemt BJF. Pharmacists’ activities to reduce medication waste: an international survey. Pharmacy. 2018;6(3):94. doi:10.3390/pharmacy6030094
38. Al-Krenawi A. Mental health practice in Arab countries. Curr Opinion Psychiatry. 2005;18(5):560–564. doi:10.1097/01.yco.0000179498.46182.8b
39. Dardas LA, Simmons LA. The stigma of mental illness in A rab families: a concept analysis. J Psychiatric and Mental Health Nurs. 2015;22(9):668–679. doi:10.1111/jpm.12237
40. Gearing RE, MacKenzie MJ, Ibrahim RW, Brewer KB, Batayneh JS, Schwalbe CS. Stigma and mental health treatment of adolescents with depression in Jordan. Commun Mental Health J. 2015;51(1):111–117. doi:10.1007/s10597-014-9756-1
41. Gilat I, Ezer H, Sagee R. Help-seeking attitudes among Arab and Jewish adolescents in Israel. British J Guidance Counselling. 2010;38(2):205–218. doi:10.1080/03069881003600983
42. Al-Krenawi A, Graham JR, Al-Bedah EA, Kadri HM, Sehwail MA. Crossnational comparison of Middle Eastern university students: help-seeking behaviors, attitudes toward helping professionals, and cultural beliefs about mental health problems. Community Ment Health J. 2009;45(1):26–36. doi:10.1007/s10597-008-9175-2
43. Rayan A, Jaradat A. Stigma of mental illness and attitudes toward psychological help-seeking in Jordanian university students. Res Psychol Beha Sci. 2016;4:7–14.25.
44. Bilican F. Help-seeking attitudes and behaviors regarding mental health among Turkish college students. Int J Ment Health. 2013;42(2–3):43–59. doi:10.2753/IMH0020-7411420203
45. Berlin EA, Fowkes WC. A teaching framework for cross-cultural health care. West J Med. 1983;139(6):934–938.
46. Arslan M, Başak H. Modeling individuals’ prescription medicine borrowing behavior. Res Social Adm Pharm. 2024;20(6):84–91. doi:10.1016/j.sapharm.2024.02.011
47. Caddick B, McCahon D, Payne R, et al. Understanding perceptions of the safety of prescription medication sharing: a qualitative study with members of the public. Ann Fam Med. 2024;22(Suppl 1):6645. doi:10.1370/afm.22.s1.6645
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
What Do We Know about Medication Adherence Interventions in Inflammatory Bowel Disease, Multiple Sclerosis and Rheumatoid Arthritis? A Scoping Review of Randomised Controlled Trials

King K, McGuinness S, Watson N, Norton C, Chalder T, Czuber-Dochan W
Patient Preference and Adherence 2023, 17:3265-3303
Published Date: 13 December 2023
Think Before You Take: Understanding Adult Medication Literacy in Saudi Arabia
Alhomoud F, Alsaeed W, Alzainaldain F, Alelq K, Alhomoud FK, Alamer KA, Alsultan MM, Alqarni YS, Alshehail B, Alhifany AA
Patient Preference and Adherence 2025, 19:1973-1990
Published Date: 10 July 2025