Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Facilitating High Quality Cancer Care: A Qualitative Study of Australian Chairpersons’ Perspectives on Multidisciplinary Team Meetings
Authors Fradgley EA, Booth K ![]() , Paul C, Zdenkowski N
, Paul C, Zdenkowski N ![]() , Rankin NM
, Rankin NM
Received 12 August 2021
Accepted for publication 29 October 2021
Published 16 December 2021 Volume 2021:14 Pages 3429—3439
DOI https://doi.org/10.2147/JMDH.S332972
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Elizabeth A Fradgley,1,2 Kate Booth,1 Christine Paul,1,2 Nicholas Zdenkowski,1 Nicole M Rankin3
1School of Medicine and Public Health, University of Newcastle, Callaghan, New South Wales, Australia; 2Priority Research Centre for Health Behaviour, University of Newcastle, Callaghan, New South Wales, Australia; 3Faculty of Medicine and Health Sciences, University of Sydney, Camperdown, New South Wales, Australia
Correspondence: Christine Paul Level 4 West, HMRI Building, Callaghan, New South Wales, 2308, Australia
Tel +61 2 4042 0693
Email [email protected]
Aim: Multidisciplinary team meetings (MDMs) are a critical element of quality care for people diagnosed with cancer. The MDM Chairperson plays a significant role in facilitating these meetings, which are often time-poor environments for clinical decision making. This study examines the perceptions of MDM Chairpersons including their role and the factors that determine the quality of a Chair, as well as the Chairperson’s perception of the value of personally attending meetings.
Methods: This qualitative study used telephone interviews to explore the experiences of MDM Chairpersons from metropolitan and regional New South Wales, Australia. Using a state-wide register, 43 clinicians who chaired lung, genitourinary, gastrointestinal, and breast cancer meetings were approached to participate. Thematic data analysis was used to develop and organise themes.
Results: Themes from the 16 interviews identified the perceived need for an expert and efficient MDM Chairperson with emphasis on personal rather than technical skills. The remaining themes related to the benefits of meetings to ensure quality and consistency of care; improve inter-professional relationships; and provide communication with and reassurance for patients.
Conclusion: The role of the MDM Chairperson requires expert management and leadership skills to ensure meetings support quality patient-centred care. MDMs are perceived to provide multiple benefits to both clinicians and patients. Efforts to train Chairs and to maximise clinician and patient benefits may be warranted given the costly and time-consuming nature of MDMs.
Keywords: multidisciplinary care, oncology, quality outcomes, cancer, clinical leadership
Introduction
Multidisciplinary teams are defined as a group of health-care providers with differing areas of expertise who work together with the intent to form consensus or evidence-based clinical decisions.1 Research demonstrates various improvements to patient outcomes when care is led by multidisciplinary teams,2–8 such as improved survival rates across cancer types, increased adherence to oral chemotherapy and pain medication, and improved patient satisfaction.2,3
Multidisciplinary management is accepted internationally as being essential to high quality care9–15 and considered the optimal approach in delivering quality care for people diagnosed with cancer.16 Multidisciplinary team meetings (MDMs) provide clinicians with ongoing opportunities to discuss and manage the complexities of diagnosis, treatment and management of cancer.1,2 In Australia, the 2016 New South Wales (NSW) Cancer Plan encouraged health services to take a multidisciplinary care approach to enhance the provision of high quality, patient-centred care and reduce clinical variation. This was further echoed in the Victorian state government’s guide to achieving best practice cancer care, arguing the benefits of multidisciplinary teams.17 Patients perceive there to be benefit in engaging in multidisciplinary care.18
MDMs are held at a regular time with the primary objective to discuss and agree on a treatment plan and confirm staging for each patient based on the best available information, with input from an array of specialities such as surgery, radiation oncology, medical oncology, and pathology under the guidance or leadership of a meeting Chair.2,7,19–21 In following this consensus format, MDMs are intended to encourage coordination, streamline care, and reduce variation.20
It is recommended that MDMs result in a documented plan for each patient case that has been discussed, and those plans be subject to audit and review on a routine basis.20 Thus, effective communication, thorough preparation and documentation are paramount to ensuring optimal care via MDMs.18 However, there is little information reported about how multidisciplinary teams achieve their desired ends21,22 and in particular, how the Chairperson perceives they facilitate this process. The MDM Chairperson likely plays a crucial role in navigating an open, inclusive discussion and is typically responsible for deciding the number and order of referred cases to be discussed.10,23
Although previous research has provided insight into team perceptions of MDMs,16,24 there are no known qualitative studies that specifically report on the perception of MDM Chairpersons on how best to provide quality patient-centred care within this time-poor and multi-skilled environment. The views of Chairpersons may be vital to the ongoing success of the MDM model and how improvements can be best implemented in practice. This aim of this study is to address this research gap by examining Australian MDM Chairpersons’ perceptions of: (i) the role of the Chairperson and factors that determine the quality of leadership and (ii) reasons or perceived value of MDM attendance for MDM Chairpersons including any perceived benefits or risks.
Methods
Design
A qualitative methodology was employed to develop a comprehensive understanding of the views of MDM Chairpersons in Australia. Semi-structured telephone interviews were conducted in line with the consolidated criteria for reporting qualitative research (COREQ) guidelines.25 The project was approved by Hunter New England and University of Newcastle Research Human Research Ethics Committees.
Study Setting and Participants
Participants were recruited from cancer services located in New South Wales, Australia. Clinicians across several tumour types were identified via a government state-based registry and sent personalised emails to complete an online expression of interest. Personal invitations were also distributed to MDM Chairpersons known to the research team. Members of the research team have participated in extensive research into MDM settings prior to this study. To be eligible to participate, individuals must have had at least one year of experience with referring patients with cancer to MDMs and have acted as an MDM Chairperson. Of the 43 contacted and eligible, 16 MDM Chairpersons chose to participate.
Data Collection
A semi-structured interview guide was developed based on a rapid literature review and feedback from two MDM Chairpersons who commented on a draft interview guide, before being pilot tested with 2 health professionals. The interview guide included ten open-ended questions focused on the above-mentioned aims (see Supplementary File). Verbal consent was obtained prior to the interviews and data collection. Each of the interviews took under 35 minutes to complete with notes made throughout. Participants were asked questions regarding reasons or perceived value of MDM attendance, referral practices, proportion of discussed cases, organisation structure, and chair and team quality. Telephone interviews were conducted and recorded by members of the study team (LF & CP) between March and October 2019. Verbatim transcripts were imported into the data management program, NVivo, to enable analysis of complex and various themes as data appeared saturated.26
Analysis
Thematic categories were developed using immersion and thematic analysis as outlined by Braun and Clarke’s six-step process.27 First, the two coding team members (LF & KB) listened to audio recordings of the interview for immersion and clarity. All interviews were then double coded by the two coding team members by drawing out initial codes throughout the data and placing themes into categories. Once established, the coding team members collaborated, compared and delivered coding results into tables for analysis. Disagreements were reflexively discussed, and the codes were refined accordingly. The researchers coded 2–5 interviews between meetings, reviewing and defining themes before producing the manuscript. Meetings to discuss themes, codes and results were noted with a diary kept of the ongoing process.27
Results
Participants
A total of 43 MDM Chairpersons were invited to participate, 16 completed an expression of interest and subsequently completed an interview. The sample included male and female Chairpersons located in metropolitan and regional NSW. The MDM Chairpersons spanned gastro-intestinal, colorectal, thoracic, lung and breast tumour groups and included medical oncologists, radiation oncologists, and thoracic physicians.
Qualitative Themes
During analysis phase, themes and sub-themes were developed relating to the perceived value of attending MDMs. The themes are summarised as: 1. An Expert and Efficient Chairperson is critical; 2. Ensuring Quality of Care; 3. Inter-professional Relationships; 4. Communication with and reassurance for the patient.
An Expert and Efficient Chairperson is Critical
Skilled Chairpersons were considered paramount to ensuring the smooth operation of meetings to attain maximum benefit in producing quality patient care. It is important to note that participants did not necessarily attribute these characteristics to themselves personally, but instead perceived these to be ideal characteristics. Several participants noted past experience or other MDMs that had not been efficient as a result of the Chairperson. Poor chairing was described in terms of lack of preparation resulting in poor time management; a lack of clarity on what occurred after the meeting; and instances where a clinician or Chair had dismissed a colleague’s opinion.
Necessary traits to effectively chair an MDM were described as a strong leadership style which combined a variety of intellectual, managerial and emotional competencies (Table 1). Participants noted that it was essential for the Chairperson to be open, collegial, have the respect of their colleagues and possess strong interpersonal skills.
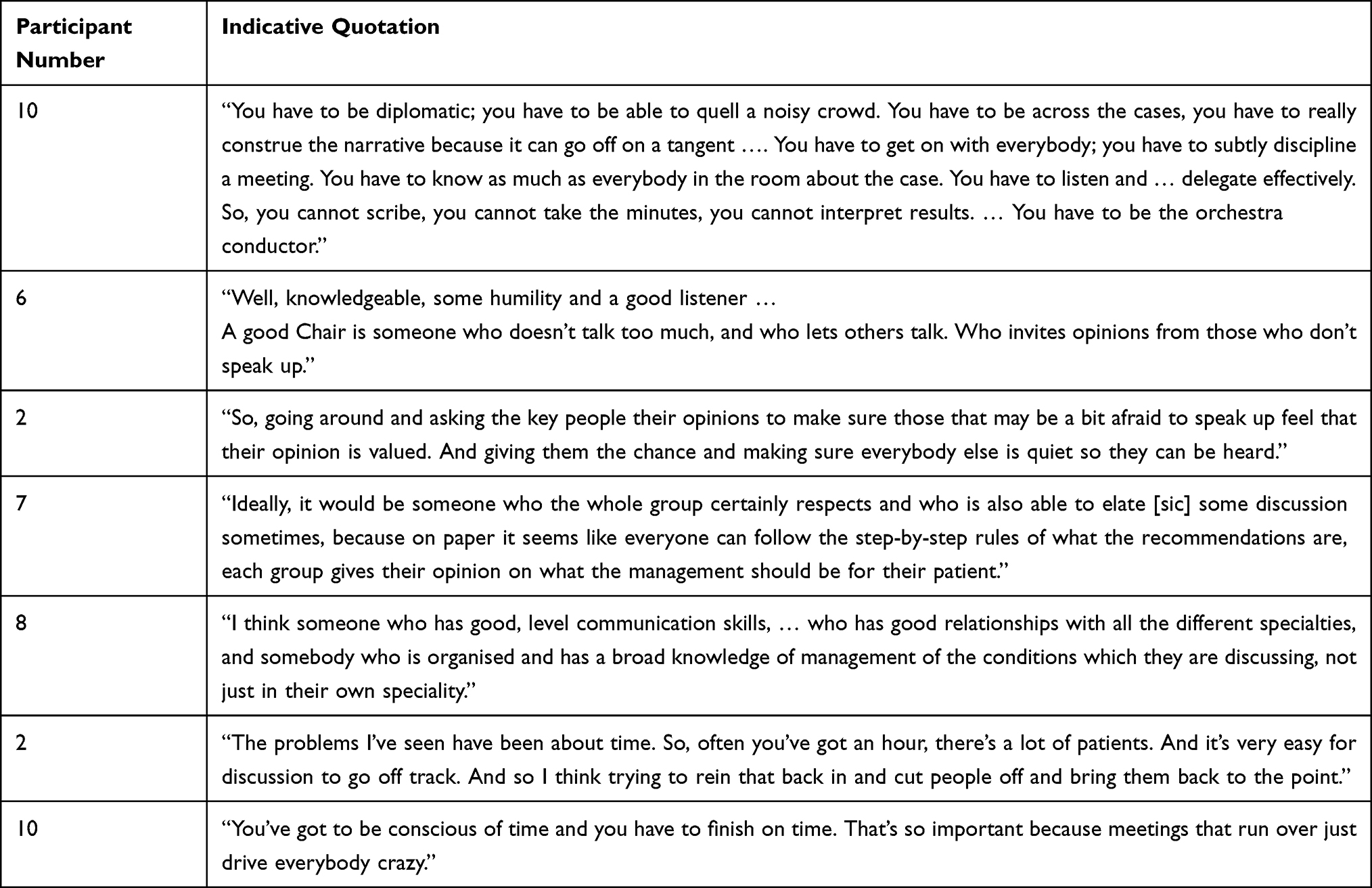 |
Table 1 Quotations About the Theme: The Efficiency and Traits of an Ideal Multidisciplinary Team (MDT) Chairperson |
The ability to control the meeting to ensure each person can discuss their patients was also considered paramount to achieving the full benefits of MDMs (Table 1). Participants indicated that meetings are able to get off track, and emphasised necessity for the Chairperson to control the flow of the meeting. The smooth and timely management of meetings was repeatedly stated by participants as it related to important meeting outcomes such as ensuring all necessary cases are discussed, maintaining order, and retaining collegiality. For the participants, meetings needed to be precise, timely and informative to ensure they reach the standard of patient benefit whilst keeping the attendees engaged and willing to participate.
Ensuring Quality of Care
Participants believed MDMs are key to ensuring that consistent care was provided to their patients. High quality care via the MDM model was perceived as the combined expertise of multiple disciplines being focused on the complex facets of diagnosis and treatment; inter-clinician accountability; and, achieving consistent approaches to care.
Combined Expertise
Participants perceived that the combined expertise present in an MDM was vital (Table 2). The combination of specialties, disciplines and subspecialities was considered an opportunity to reach consensus on a person’s diagnosis and develop or modify a patient’s treatment plan where input was required from multiple expert opinions. The Chairpersons acknowledged complementary expertise, specialties, experience, and perceptions as a notable benefit to patient care.
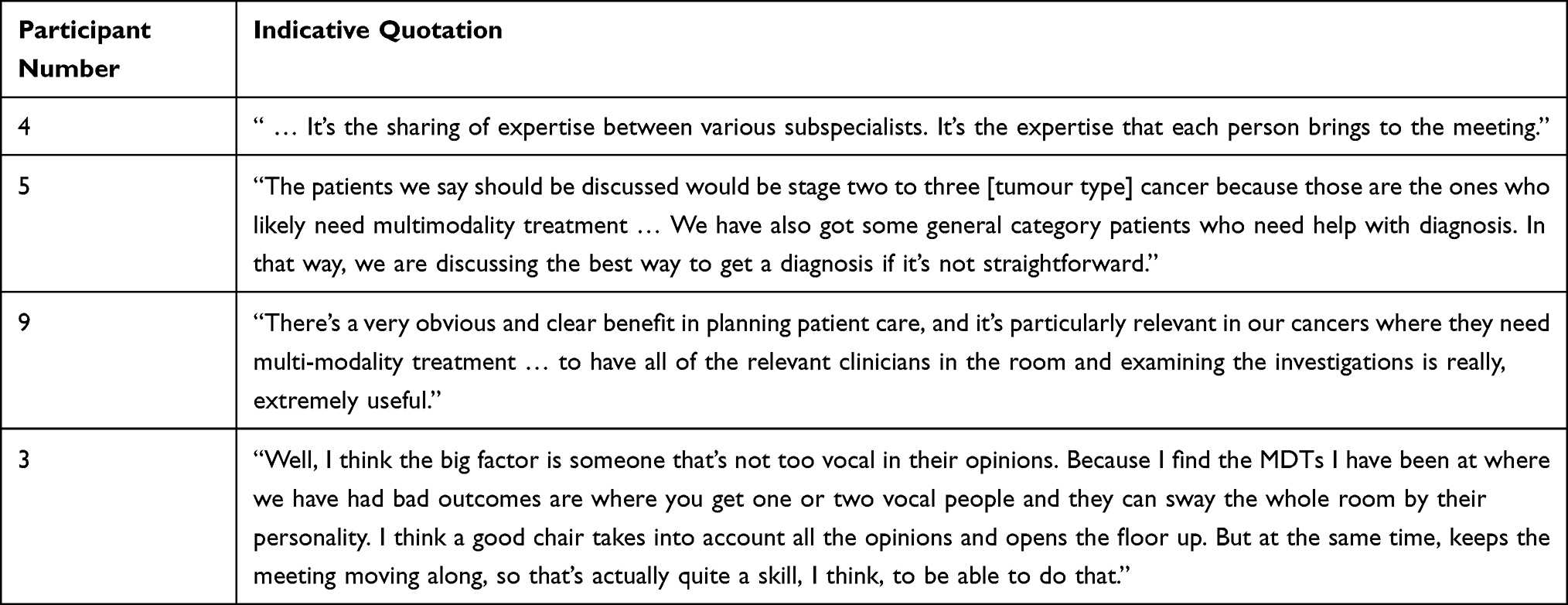 |
Table 2 Quotations About the Theme: Combined Expertise and Consensus |
Consensus on Complex and Comprehensive Care
As shown in Table 3, the perceived value of treatment discussions across specialties was considered to be particularly important for cases where care was very complex. In-person meetings were considered to provide clearer communication between clinicians and specialties for complex cases. Participants noted that collective discussion of complex patients was necessary for identifying all potential issues when providing quality, comprehensive care.
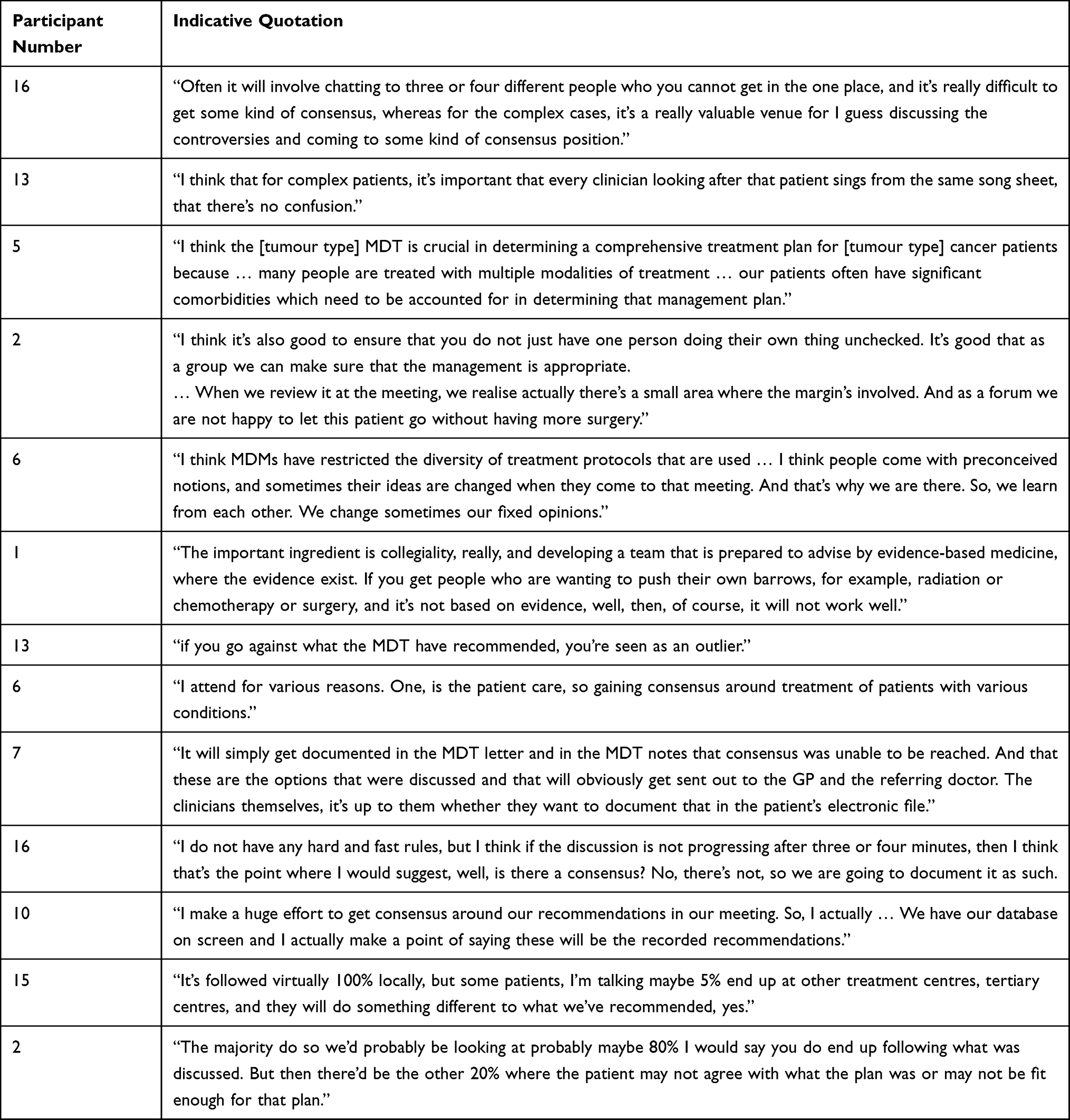 |
Table 3 Quotations About the Theme: Consensus and Accountability on Consistent Care |
Chairs were asked what occurred if a consensus was not achieved. For many, this was perceived to be a “grey” area with most stating that they simply documented it in their letter to the patients’ GP or in the MDM recommendation letter. However, there were no guidelines on how to manage disagreement (see Table 3). One participant, however, noted that this was not an issue as they made sure they always had consensus in their meetings (see Table 3).
It was the general perception of the participants that a high proportion of recommendations from meetings were followed by the treating team; most Chairs indicated that treatment recommendations are followed upwards of 80% of the time (see Table 3). However, given the potential for these recommendations to be driven by group think or “a few vocal participants”, the chairs noted that it was essential to elicit opinions from the wider group. Chairs reported that patient preference was often the reason for treatment recommendations not being followed.
Accountability and Consistent Care
MDMs were also perceived to hold an important role in holding clinicians accountable to following best practice as discussed by the group (Table 3). Chairpersons believed that it was important to ensure that each member was providing care in a consistent manner, and that attendance at MDMs resulted in clinicians developing a practice of seeking team review before making complex or multidisciplinary decisions. The sounding board of peers was perceived to be a quality assurance exercise and a method of ensuring consistent care, particularly where clinicians might hold opinions not based on current evidence or hold fixed opinions. There was also a sense that the group would have a lower tolerance for risk or ambiguity in treatment decisions and management (eg, surgical margins).
When asked their likeliness to follow group consensus, one noted that recommendation was “biblical” and that once reached, a clinician would be unlikely to deviate (Table 3). This demonstrates the way group consensus at meetings can ensure consistent care for this Chairperson.
Chairs acknowledged several areas or circumstances where MDMs struggle to provide consistent and comprehensive care, particularly for complex cases. One common circumstance was when referral information provided to the MDM was incomplete. In this circumstance, chairs either delayed the patient case to the next MDM (potentially wasting scarce time) or a tentative decision was made based on what information was available.
Inter-Professional Relationships
Regular meetings provide opportunity for the participants to engage and interact with their peers and improve communication (Table 4). Engaging face-to-face with others from various clinical settings and expertise was perceived to foster relationships across multiple disciplines. Face-to-face communication in the meeting was perceived to provide an opportunity specifically for developing interpersonal relations as opposed to telephone or electronic communication. Overall, communication and team interaction was seen to be a significant benefit of participating in MDMs.
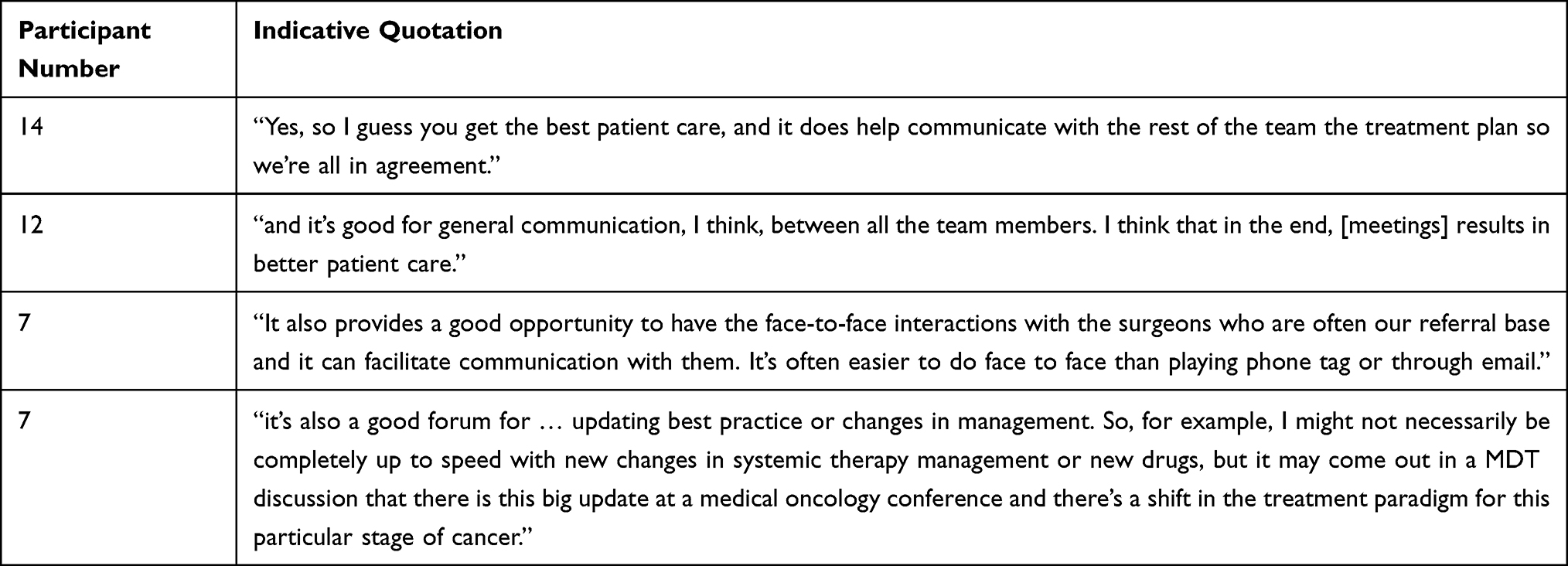 |
Table 4 Quotations About the Theme: Relationships and Relationship Building |
Communication with and Reassurance for the Patient
Participants perceived patient reassurance to be a key benefit of MDM presentation. As shown in Table 5, many commented on how MDM presentation was essentially a process to collate a “second opinion” for patients and communicate that treatment plans were developed based on expert group consensus. For some clinicians, this level of reassurance was helpful in building partnerships with patients.
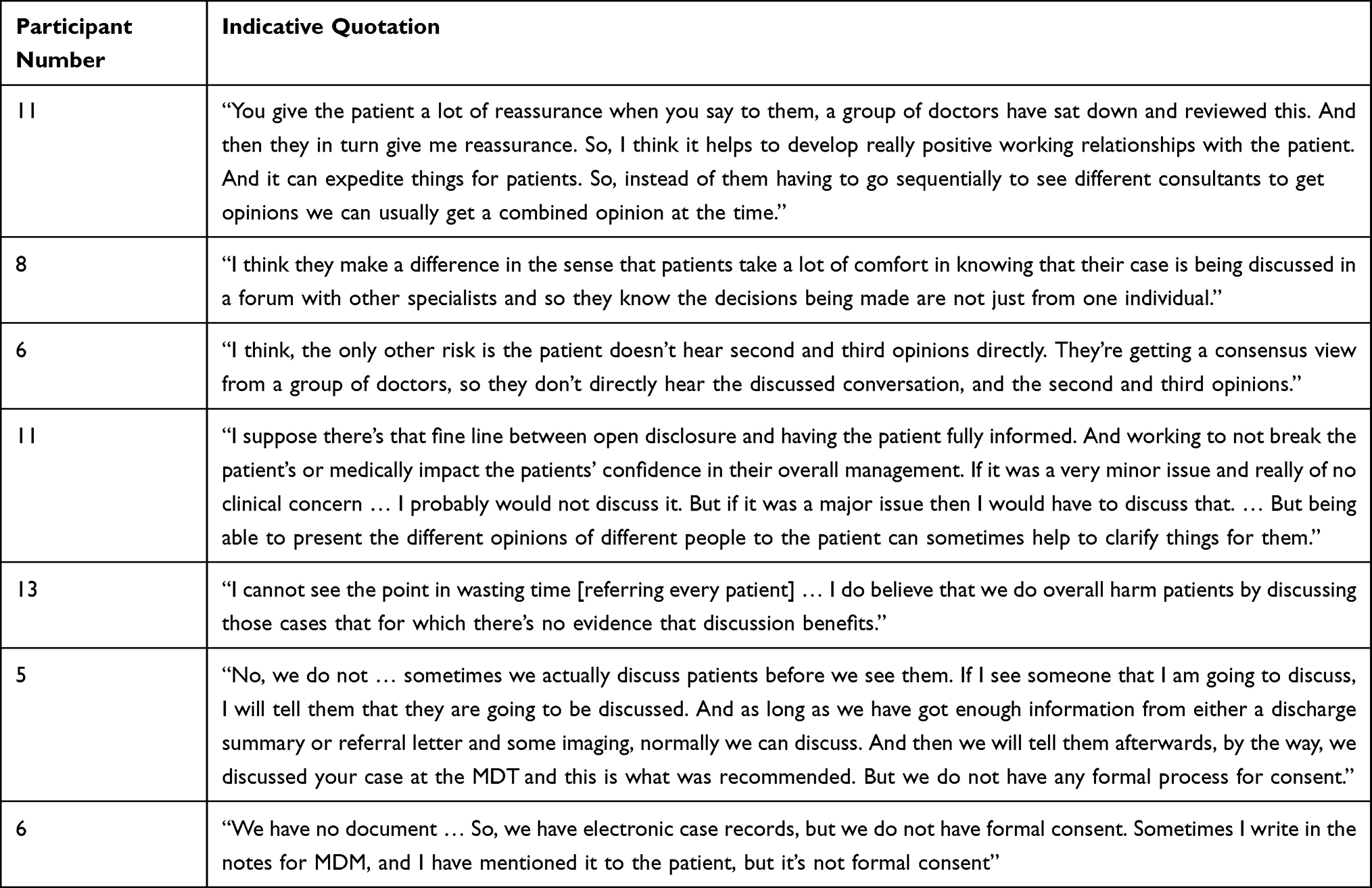 |
Table 5 Quotations About the Theme: Patient Communication |
While group consensus was seen as reassuring for the patient, communicating lack of consensus was perceived as difficult. For some participants, differing opinions on smaller treatment details were considered a non-issue that would not need to be reported to patients, thus ensuring patient confidence in treatment was maintained (Table 5). However, other participants perceived a potential risk in providing patients with a group consensus rather than each individual medical opinion (Table 5). This risk was rationalised by some as the MDM venue providing quick access to a second or third opinion, as opposed a patient independently seeking these additional opinions themselves.
Patient communication of MDM decisions also infers that clinicians had gained consent for patient presentation to the MDM. However, the Chairpersons acknowledged that the process for gaining consent was clinician-dependent with very few having a formalised consent process.
Discussion
This qualitative study indicates that effective MDM Chairpersons are perceived to require a comprehensive set of leadership and interpersonal skills to ensure an efficient decision-making process in MDMs. The benefits of skilled Chairpersons leading these meetings are perceived to ensue from consensus and consistency in care, improved inter-professional relationships and reassurance for patients.
Chairpersons Play a Crucial Role in Providing Care and Managing Meetings
Participants in this study indicated that communication, decision making and willingness to participate in the meetings are key to being efficient. Similar findings were reflected in a recent review.1 Furthermore, our study also indicates that the Chairperson holds primary responsibility for ensuring that the meetings run efficiently. In contrast, a national survey from a cross-sectional study in the UK that aimed to understand MDMs functionality from the perception of the MDM coordinators indicated that some believed that meetings ran just as efficiently when the usual Chairperson was unable to attend.28
The Chairpersons in our Australian study indicate that they believe strong leadership, communication and meeting control skills were key to chairing a meeting. The necessary leadership skills described by the study participants incorporated a variety of intellectual, managerial and emotional competencies.29,30 While our participants emphasised these qualities, our novel findings emphasised that being respected for one’s technical expertise -“You have to know as much as everybody in the room” - was also considered to be very important.
There is a need to address barriers within group dynamics of meetings, with the Chairperson able to play a large role in communication gaps.24 The UK’s National Care Action Team issued a report based on the survey responses from over 2000 MDM members in early 2009.24 The report states that it is essential for the Chairperson to have proficient skills in listening and communication; interpersonal relations; managing disruptive personalities and conflict; negotiations; facilitating effective consensual clinical decision-making; and time management.16,24 Perceptions of an ideal Chair are made up of traits such as assertiveness, good communication and team work rather than technical expertise.31
An effective MDM Chairperson requires a comprehensive set of skills; some of which are not taught as part of traditional medical training. This indicates that there could be room to explore the potential benefits of providing clinicians with leadership skills training specific to optimising MDMs. It may be challenging for an incoming or more junior clinicians to assume this position; MDM Chairpersons who are mentored internally in a service have more opportunity to develop relationships and demonstrate competence. Such comprehensive skills include effective time management during meetings. Australian data indicate that each patient receive 5–8 minutes discussion time in a typical MDM.21 A literature review within the UK identified patients usually receive less than 2 minutes.32 Both timeframes indicate substantial time pressure within MDMs. Due to these workloads, it is vital that MDM Chairs are able to efficiently manage time in the interests of both team members and patients.
MDMs and Attendance Play an Important Role in Providing Quality Care to Patients
MDM Chairpersons identified meetings as necessary to providing patient centred care, which is consistent with other recent studies.33 The main benefits identified by Chairpersons were combined expertise, consensus on complex care, inter-clinician accountability and achieving consistency in care. The specialised expertise that individuals brought to the meeting was considered to be a valuable element of multidisciplinary care. Research has demonstrated that patient complexity should be considered when making treatment plans and providing care.34 Our results emphasise MDM Chairpersons’ beliefs that meetings were particularly useful in discussing more complicated cases and complex treatment options.
It is apparent that patient benefit is an integral component of a successful meeting for MDM Chairpersons, and it therefore may be beneficial to integrate patient-reported outcomes to optimise and assess the successes of MDMs. The inclusion of patient-reported outcomes, including psychosocial aspects of care, is gaining traction among health professionals; for example, an audit of Australian cancer services reported 59% of MDM participants believe psychosocial aspects and outcome measures should be better incorporated into meetings. Emerging information about the complex relationship between multidisciplinary care, patient perspectives and outcomes and how this relationship can drive quality improvements to policy and health-care outcome measurement will shape future research into MDM.35
Improved Interprofessional Relationships
Our Chairpersons indicate that the MDMs were in themselves an important strategy for improving inter-professional communication and relationships. A National Multidisciplinary Care Demonstration Project identified communication to be one of five principles of multidisciplinary care for Australian women with breast cancer.36 A National Breast Cancer Centre report identified inefficient communication between MDM members to be a major barrier in providing quality multidisciplinary cancer care.37 Both of these reports are now over a decade old suggesting that gaps in communication are a long-standing issue and actionable strategies to improve clinician communication skills must be prioritised in national cancer control policy and draw in effective implementation and quality improvement strategies. Lack of communication within a health team can lead to poor decision-making16 and therefore, the capabilities of Chairpersons should include that of fostering inter-professional relationships in the context of MDMs.
Reassurance for Patients
The Chairpersons identified that providing the outcomes of MDM discussions to patients facilitated communication and reassurance for patients, and was therefore a significant patient benefit of MDMs. However, it was noted that approach could pose a potential risk in that patients may only hear a consensus opinion rather than individual various opinions. The manner in which team members navigated this issue was varied and was at the discretion of the individual medical professional regarding how much information they shared.
MDMs hold a critical role in holding clinicians accountable to delivering consistent care based on the most recent evidence available. The meeting requires a culture receptive to group critique and where individuals can discuss new evidence, and ensure the benefits are passed on to the patient while supporting the patient to seek additional opinion where relevant or desired. Furthermore, the model discussed by most of the Chairs portrayed patients as a passive participant in the MDM process; few had a formalised consent process, patient preferences were sometimes at odds with the MDM decisions, and the amount of information provided back to the patient was at the discretion of the treating physician. As health services continue to strive for patient-centred care, there is potential for MDMs to examine how they can incorporate patient preferences and communication.
Limitations
This study has some limitations, including a sample size of 16 participants and the focus on Chairpersons may have limited the breadth of experience represented in the data. A larger or more diverse sample may have uncovered unreported themes; however, our sample did include four speciality areas of lung, genitourinary, gastrointestinal, and breast cancers. While numbers of participants in qualitative studies vary, we did reach saturation of themes through the 16 interviews.38 The findings should be further tested via quantitative studies with representative samples of MDM members and Chairs.
We acknowledge that non-Chair team members may have different perceptions of required traits to lead an MDM. We chose to purposively sample Chairpersons as they were expected to have both knowledge of the demands placed upon the role and the experience of leading MDMs. Many participants noted they had dual roles as both Chairperson and regular MDM participant (of a different tumour type) and drew upon these experiences. Participants noted their experience in attending ineffective meetings and had both positive and negative examples of other Chairpersons. Due to the design of questions, the tone of the interviews were from a positive perspective. We acknowledge that this may limit the understanding of the negative attributes of a Chairperson and the impact on meeting efficiency.
Conclusion
The role of MDM Chairperson requires a variety of interpersonal and technical skills which are essential to ensuring that meetings optimally support quality, patient-centred care. Through a unique insight into perceptions of Australian Chairpersons, it is evident that expert management and leadership skills of MDMs are paramount in facilitating quality patient-centred care by bringing consensus and consistency; and fostering inter-professional relationships.
Data Sharing Statement
Due to the nature of confidentiality for our interview participants, data are not available for this study.
Ethics Approval and Informed Consent
The project was approved by Hunter New England and University of Newcastle Research Human Research Ethics Committees. All research subjects gave verbally recorded informed consent to participate in the study prior to study commencement, and to have their anonymised responses published.
Acknowledgments
We would like to acknowledge the kind assistance of The Cancer Institute NSW in providing information regarding participant recruitment and the generous advice and assistance of Anthony Proietto, Jill Lack and Denise Kaminski.
Author Contributions
All authors listed made a significant contribution to the work reported. NR, CP, LF, NZ were responsible for conception, study design, execution, and interpretation. All authors (NR, CP, LF, NZ and KB) have substantially contributed to and revised the article and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, including journal selection. All listed authors agree to take responsibility and be accountable for the contents of the article. LF and CP were responsible for data collection. KB, LF, CP and NR were responsible for initial drafts of the manuscript. NR, CP, LF, NZ and KB contributed to manuscript refinement and proofing. KB and LF were primarily responsible for data coding and initial analysis.
Funding
This project was funded by the Hunter Cancer Research Alliance’s Implementation Flagship Program Grant, which is funded via the Cancer Institute NSW. Dr Elizabeth Fradgley is supported by a CINSW ECR Fellowship and receives infrastructure support from the Hunter Medical Research Institute.
Disclosure
Dr Elizabeth A Fradgley reports grants from Cancer Institute New South Wales, during the conduct of the study. For the remaining authors no conflicts of interest were declared.
References
1. Specchia ML, Frisicale EM, Carini E, et al. The impact of tumor board on cancer care: evidence from an umbrella review. BMC Health Serv Res. 2020;20(1):73. doi:10.1186/s12913-020-4930-3
2. Prades J, Remue E, van Hoof E, Borras JM. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy. 2015;119(4):464–474. doi:10.1016/j.healthpol.2014.09.006
3. Taplin SH, Weaver S, Salas E, et al. Reviewing cancer care team effectiveness. J Oncol Pract. 2015;11(3):239–246. doi:10.1200/JOP.2014.003350
4. Pillay B, Wootten AC, Crowe H, et al. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: a systematic review of the literature. Cancer Treat Rev. 2016;42:56–72. doi:10.1016/j.ctrv.2015.11.007
5. El Saghir NS, Keating NL, Carlson RW, Khoury KE, Fallowfield L, Tumor boards: optimizing the structure and improving efficiency of multidisciplinary management of patients with cancer worldwide. Am Soc Clin Oncol Educ Book. 2014;34:e461–466. doi:10.14694/EdBook_AM.2014.34.e461
6. Lamb BW, Sevdalis N, Mostafid H, Vincent C, Green JS. Quality improvement in multidisciplinary cancer teams: an investigation of teamwork and clinical decision-making and cross-validation of assessments. Ann Surg Oncol. 2011;18(13):3535–3543. doi:10.1245/s10434-011-1773-5
7. Raine R, Wallace I, Nic A’ Bháird C, et al. Improving the effectiveness of multidisciplinary team meetings for patients with chronic diseases: a prospective observational study. Health Serv Deliv Res. 2014;2(37):1–172. doi:10.3310/hsdr02370
8. Ke KM, Blazeby JM, Strong S, Carroll FE, Ness AR, Hollingworth W. Are multidisciplinary teams in secondary care cost-effective? A systematic review of the literature. Cost Eff Resour Alloc. 2013;11(1):7. doi:10.1186/1478-7547-11-7
9. Stone E, Rankin N, Phillips J, et al. Consensus minimum data set for lung cancer multidisciplinary teams: results of a Delphi process. Respirology. 2018;23(10):927–934. doi:10.1111/resp.13307
10. Wihl J, Rosell L, Frederiksen K, Kinhult S, Lindell G, Nilbert M. Contributions to multidisciplinary team meetings in cancer care: predictors of complete case information and comprehensive case discussions. J Multidiscip Healthc. 2021;14:2445–2452. doi:10.2147/JMDH.S309162
11. Swellengrebel HA, Peters EG, Cats A, et al. Multidisciplinary discussion and management of rectal cancer: a population-based study. World J Surg. 2011;35(9):2125–2133. doi:10.1007/s00268-011-1181-9
12. Silbermann M, Pitsillides B, Al-Alfi N, et al. Multidisciplinary care team for cancer patients and its implementation in several Middle Eastern countries. Ann Oncol. 2013;24(Suppl7):vii41–vii47. doi:10.1093/annonc/mdt265
13. Lamb BW, Sevdalis N, Arora S, Pinto A, Vincent C, Green JS. Teamwork and team decision-making at multidisciplinary cancer conferences: barriers, facilitators, and opportunities for improvement. World J Surg. 2011;35(9):1970–1976. doi:10.1007/s00268-011-1152-1
14. Whitehouse M. A policy framework for commissioning cancer services. British Medical Journal Publishing Group; 1995.
15. Borras JM, Albreht T, Audisio R, et al. Policy statement on multidisciplinary cancer care. Eur J Cancer. 2014;50(3):475–480. doi:10.1016/j.ejca.2013.11.012
16. Soukup T, Lamb BW, Arora S, Darzi A, Sevdalis N, Green JS. Successful strategies in implementing a multidisciplinary team working in the care of patients with cancer: an overview and synthesis of the available literature. J Multidiscip Healthc. 2018;11:49–61. doi:10.2147/JMDH.S117945
17. Services VGDoH. Achieving best practice cancer care: a guide for implementing multidisciplinary care; 2007.
18. Tanaka H, Medeiros G, Giglio A. Multidisciplinary teams: perceptions of professionals and oncological patients. Rev Assoc Med Bras. 2020;66(4):419–423. doi:10.1590/1806-9282.66.4.419
19. Menon M, Cunningham C, Kerr D. Addressing unwarranted variations in colorectal cancer outcomes: a conceptual approach. Nat Rev Clin Oncol. 2016;13(11):706–712. doi:10.1038/nrclinonc.2016.94
20. Raine R, Nic A’ Bháird C, Xanthopoulou P, et al. Use of a formal consensus development technique to produce recommendations for improving the effectiveness of adult mental health multidisciplinary team meetings. BMC Psychiatry.;15(1):143. doi:10.1186/s12888-015-0534-6
21. Rankin NM, Lai M, Miller D, et al. Cancer multidisciplinary team meetings in practice: results from a multi-institutional quantitative survey and implications for policy change. Asia Pac J Clin Oncol.;14(1):74–83. doi:10.1111/ajco.12765
22. Rankin NM, Fradgley EA, Barnes DJ. Implementation of lung cancer multidisciplinary teams: a review of evidence-practice gaps. Trans Lung Cancer Res. 2019;9(4):1667–1679.
23. Hahlweg P, Didi S, Kriston L, Härter M, Nestoriuc Y, Scholl I. Process quality of decision-making in multidisciplinary cancer team meetings: a structured observational study. BMC Cancer,;17(1):772 doi: 10.1186/s12885-017-3768-5.
24. Team NCA. Characteristics of an effective MDT; 2010.
25. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
26. Nowell LS, Norris JM, White DE, Moules NJ. Thematic Analysis: striving to Meet the Trustworthiness Criteria. Int J Qual Methods. 2017;16(1):1609406917733847. doi:10.1177/1609406917733847
27. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
28. Jalil R, Lamb B, Russ S, Sevdalis N, Green JS. The cancer multi-disciplinary team from the coordinators’ perspective: results from a national survey in the UK. BMC Health Serv Res. 2012;12(1):457. doi:10.1186/1472-6963-12-457
29. Dulewicz V, Higgs M. Assessing leadership styles and organisational context. J Manag Psychol. 2005;20(2):105–123. doi:10.1108/02683940510579759
30. Müller R, Turner R. Leadership competency profiles of successful project managers. Int J ProjManag. 2010;28(5):437–448. doi:10.1016/j.ijproman.2009.09.003
31. Lamb B, Payne H, Vincent C, Sevdalis N, Green JSA. The role of oncologists in multidisciplinary cancer teams in the UK: an untapped resource for team leadership? J Eval Clin Pract. 2011;17(6):1200–1206. doi:10.1111/j.1365-2753.2010.01507.x
32. Soukup T, Lamb BW, Weigl M, Green JSA, Sevdalis N. An integrated literature review of time-on-task effects with a pragmatic framework for understanding and improving decision-making in multidisciplinary oncology team meetings. Front Psychol. 2019;10:1245. doi:10.3389/fpsyg.2019.01245
33. Mistry R, Walker A, Walker N, Ofo E. Royal Society of Medicine surgical innovation day Adrian Tanner prize winner 2019: multidisciplinary care and surgical innovation for the benefit of the patient with head and neck cancer of unknown primary. JRSM Open. 2020;11(7):2054270420921066. doi:10.1177/2054270420921066
34. Soukup T, Morbi A, Lamb BW, et al. A measure of case complexity for streamlining workflow in multidisciplinary tumor boards: mixed methods development and early validation of the MeDiC tool. Cancer Med. 2020;9(14):5143–5154. doi:10.1002/cam4.3026
35. Kaiser L, Bartz S, Neugebauer EAM, Pietsch B, Pieper D. Interprofessional collaboration and patient-reported outcomes in inpatient care: protocol for a systematic review. Syst Rev. 2018;7(1):126. doi:10.1186/s13643-018-0797-3
36. Zorbas H, Rainbird K, Luxford K, Barraclough B, Redman S. Multidisciplinary care for women with early breast cancer in the Australian context: what does it mean? Med J Australia. 2003;179(10):528–531. doi:10.5694/j.1326-5377.2003.tb05678.x
37. National Breast Cancer Centre. Making multidisciplinary care a reality; 2006.
38. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148. doi:10.1186/s12874-018-0594-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.