Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Facial Wrinkling is Not Associated with Chronic Obstructive Pulmonary Disease Severity in Thai Patients: A Cross-Sectional Study
Authors Suchonwanit P ![]() , Eittidachachote T
, Eittidachachote T ![]() , Pongpitpitak B, Tejapira K
, Pongpitpitak B, Tejapira K ![]() , Ketprapakorn N, Amornputtisathaporn N
, Ketprapakorn N, Amornputtisathaporn N ![]() , Chamnanvej P
, Chamnanvej P
Received 19 April 2026
Accepted for publication 8 July 2026
Published 18 July 2026 Volume 2026:21 618288
DOI https://doi.org/10.2147/COPD.S618288
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Zijing Zhou
Poonkiat Suchonwanit,1 Tanat Eittidachachote,1 Bunlung Pongpitpitak,1 Kasama Tejapira,1 Narikun Ketprapakorn,1 Naparat Amornputtisathaporn,2 Phichaya Chamnanvej2
1Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 2Division of Pulmonary and Critical Care Medicine, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Phichaya Chamnanvej, Division of Pulmonary and Critical Care Medicine, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama VI Road, Ratchathewi, Bangkok, 10400, Thailand, Tel +66-2-2011666, Email [email protected]
Background: Western studies have reported associations between facial wrinkling and chronic obstructive pulmonary disease (COPD), suggesting a shared susceptibility to tissue aging. However, data on Asian populations are limited, and population-specific differences in skin biology may modify these relationships.
Objective: To investigate the association between facial wrinkle severity and COPD characteristics in Thai patients and to identify independent predictors of wrinkle severity.
Methods: This cross-sectional study enrolled 93 Thai patients with COPD. Facial wrinkles were assessed using the Daniell grading scale (a validated six-point subjective clinical grading system) and the Antera 3D imaging system (an objective three-dimensional topographic imaging device). Multivariable linear and logistic regression analyses were performed to identify independent predictors of wrinkle severity after adjustment for age, sex, body mass index (BMI), cumulative smoking exposure, occupational sun exposure, and post-bronchodilator FEV1 % predicted.
Results: Mean age was 72.6± 8.8 years (90.3% male). Severe facial wrinkling, defined as a Daniell score ≥ 4, was present in 41.9% of the patients. The Daniell grading scale and Antera 3D measurements showed a moderate-to-strong correlation (Spearman’s ρ=0.68, p< 0.001). In multivariable analyses, age was consistently associated with both objective wrinkle depth (β=0.08; 95% CI: 0.01– 0.24; p=0.042) and severe wrinkling (OR=1.15; 95% CI: 1.06– 1.23; p< 0.001). Higher body mass index was inversely associated with objective wrinkle severity (β=− 0.34; 95% CI: − 0.65 to − 0.03; p=0.031) but not with severe Daniell-grade wrinkling. COPD-related characteristics, including FEV1 % predicted, cumulative smoking exposure, and smoking-related COPD status, showed no significant associations with wrinkle severity after adjustment.
Conclusion: Among Thai patients with spirometry-confirmed COPD, no significant association was detected between facial wrinkle severity and the COPD-related characteristics assessed. Age was the most consistent independent predictor of wrinkle severity, while higher BMI showed an inverse association with objective wrinkle measurements only. These findings differ from those reported in Western populations and support population-specific validation before applying facial wrinkling as a cutaneous marker of COPD-related disease burden.
Keywords: Asian population, chronic airway diseases, COPD, cutaneous markers, facial aging, wrinkle severity
Introduction
Chronic obstructive pulmonary disease (COPD) is a major global health burden, affecting an estimated 174 million individuals worldwide.1 The disease is characterized by persistent airflow limitation resulting from chronic bronchial inflammation and emphysematous destruction of lung parenchyma, leading to progressive dyspnea and reduced exercise tolerance.2 Cigarette smoking remains the predominant risk factor, while exposure to biomass fuel combustion also contributes significantly in developing regions; however, only a subset of exposed individuals develop clinically significant disease, suggesting important host susceptibility factors.3 In Thai and other Asian settings, both COPD risk and visible skin aging may also be shaped by regionally variable environmental and lifestyle exposures.3
The pathogenesis of emphysema involves systemic inflammation, elevated levels of pro-inflammatory mediators, oxidative stress, and protease-antiprotease imbalance.4,5 These mechanisms extend beyond the lung and contribute to various COPD-related comorbidities, including osteoporosis, cardiovascular disease, skeletal muscle atrophy, and accelerated skin aging.6–11 COPD has also increasingly been conceptualized as a disorder of accelerated biological aging, in which oxidative stress, mitochondrial dysfunction, telomere dysfunction, impaired autophagy, and cellular senescence may contribute to airway and parenchymal injury as well as extrapulmonary manifestations.12,13 Cellular senescence, including the senescence-associated secretory phenotype, has been linked to telomere dysfunction, DNA damage, and oxidative stress in COPD.14,15 These overlapping aging-related pathways provide a biologically plausible basis for examining cutaneous aging features as potential external correlates of COPD, while recognizing that such associations may vary between populations.
Previous studies in predominantly Caucasian cohorts have reported associations between facial wrinkling, skin connective tissue changes, and COPD or emphysema-related phenotype.16,17 Patel et al reported that Daniell facial wrinkle grading correlated with computed tomography (CT)-assessed emphysema extent among smokers, while other studies examined dermal elastic fibers, Daniell grading, total wrinkle length, or skin elasticity in relation to lung function and emphysema.16,17 Although objective non-invasive assessment of skin elasticity has been incorporated in prior work, COPD-focused studies of facial wrinkling have generally relied on clinical grading rather than objective measurements of wrinkle characteristics, which provide an additional quantitative dimension to wrinkle evaluation.18,19 The biological basis for a potential skin-lung connection centers on shared extracellular matrix (ECM) vulnerability, as cigarette smoke exposure can accelerate cutaneous aging and promote inflammatory processes through oxidative stress, matrix metalloproteinase activation, and altered collagen-elastin homeostasis.20–25 These pathological changes overlap conceptually with mechanisms involved in ultraviolet-induced photoaging.26–29
Ethnic and population-specific differences in cutaneous biology may be relevant when interpreting these associations. Asian skin has been reported to differ from Caucasian skin in dermal architecture, fibroblast and collagen characteristics, melanin distribution, and clinical aging phenotype.30–33 Several studies suggest that coarse wrinkling may appear later or be less prominent than pigmentary aging in many Asian populations, although these observations should be viewed as potential modifiers rather than deterministic explanations.30–32 Visible wrinkle severity in Asian patients may also be influenced by extrinsic factors such as photoprotection behavior, occupational sun exposure, air pollution, and occupational dust or particulate exposure.34–38 Therefore, associations between COPD-related systemic aging and visible wrinkle formation observed in Western cohorts may not be directly generalizable to Asian patients without population-specific validation.
Given the paucity of data from Thai and other Asian populations, this study aimed to investigate the relationship between facial wrinkle severity and COPD characteristics in Thai patients using both subjective and objective assessments and to identify independent predictors of wrinkle severity. Based on reported population differences in skin-aging phenotype and environmental or behavioral exposures, we hypothesized that the positive association between facial wrinkle severity and COPD severity reported in Western populations would be weaker, rather than completely absent, in Thai patients with COPD.
Methods
This cross-sectional study was conducted at Ramathibodi Hospital, Bangkok, Thailand. The study was approved by the Institutional Review Board for Ethics in Human Research (MURA2023/810), and written informed consent was obtained from all participants. Because of the cross-sectional design, this study evaluated associations at a single time point and was not designed to establish temporal or causal relationships.
Study Participants
Patients aged ≥40 years with suspected or physician-diagnosed COPD were screened if they had at least one of the following criteria: (1) post-bronchodilator spirometry demonstrating airflow limitation defined as FEV1/FVC ratio <0.70 according to the 2025 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines,39 or (2) radiographic evidence of emphysema on high-resolution CT in the absence of an alternative diagnosis. High-resolution CT emphysema was used as a secondary screening criterion to avoid missing emphysema-predominant patients who might subsequently meet spirometric criteria; however, COPD for the final analytic cohort was defined strictly by post-bronchodilator spirometric airflow obstruction. Patients with CT emphysema alone were therefore excluded from the final analysis. Other exclusion criteria included a diagnosis of asthma with positive bronchodilator reversibility, connective tissue diseases affecting the skin, and prior facial laser treatment. A total of 119 patients were initially screened, of whom 93 had spirometry-confirmed COPD and were included in the final analysis; no CT-only patients were included in the primary analytic cohort.
Demographic and Baseline Characteristic Assessment
The demographic information collected included age, sex, body mass index (BMI), ethnicity, and occupation. Comorbidities were documented from the medical records. Current medication use, particularly inhaled and oral corticosteroids, was systematically recorded. Occupational sun exposure was classified into three categories based on the time spent outdoors: low exposure was defined as less than 2 hours per day, moderate exposure as 2–4 hours per day, and high exposure as more than 4 hours per day. Sun-protective behaviors, including sunscreen use, hats, umbrellas, long-sleeved clothing, and other physical photoprotection measures, were not systematically recorded and therefore were not controlled for in the multivariable analyses. Recreational sun exposure, cumulative lifetime ultraviolet exposure, and urban versus rural residence were also not systematically collected. Accordingly, occupational sun exposure was interpreted as a limited proxy for outdoor work-related ultraviolet exposure rather than as a comprehensive measure of cumulative lifetime photodamage.
Detailed smoking history was recorded in pack-years. Participants were classified as never smokers if they had smoked fewer than 100 cigarettes in their lifetime, former smokers if they had quit more than six months prior to enrollment, and current smokers if they were still smoking or had quit within the preceding six months. Patients with ≥10 pack-years of cumulative exposure were classified descriptively as having smoking-related COPD, following the established methodology.40 Duration since smoking cessation, passive smoking exposure, and lifetime smoking intensity patterns were not consistently available and therefore were not included in the multivariable models.
Spirometry results from the most recent assessment within 12 months were extracted from the medical records. COPD severity was classified according to 2025 GOLD criteria as follows: GOLD stage 1 (mild disease) was defined as FEV1 ≥80% predicted, GOLD stage 2 (moderate disease) as FEV1 50–79% predicted, GOLD stage 3 (severe disease) as FEV1 30–49% predicted, and GOLD stage 4 (very severe disease) as FEV1 <30% predicted.39
Facial Wrinkle Assessment
Facial wrinkles were evaluated using both subjective clinical grading and objective three-dimensional imaging to provide complementary assessments of wrinkle severity. Standardized digital photographs of bilateral temporal regions were obtained under controlled lighting conditions. Images were independently evaluated by a board-certified dermatologist who was blinded to clinical data. Wrinkling was graded using the validated Daniell six-point scale with the following criteria:18 Grade I indicates essentially unwrinkled skin with minimal to no visible lines; Grade II consists of several wrinkles numbering 2–6 per side, each measuring ≤3 cm in length; Grade III includes several prominent wrinkles per side, each measuring 3–4 cm long; Grade IV is defined by wrinkles extending both superiorly and inferiorly, each measuring ≥5 cm in length; Grade V involves extensive wrinkles extending from the crow’s feet area to the cheeks and forehead; and Grade VI indicates profound wrinkling over most of the face. For analytical purposes, severe facial wrinkling was defined as a Daniell score of ≥4.16
Quantitative wrinkle analysis was performed using a standardized three-dimensional imaging system (Antera 3D®, Miravex, Ireland). This device captures high-resolution skin surface topography to assess the wrinkle depth and severity. Participants were asked to sit upright with a neutral facial expression. Hair was moved away from the temporal and lateral periorbital region. Images were obtained in the same examination room under standardized lighting conditions. The region of interest was standardized using the lateral canthus and temporal crow’s-feet area as anatomical landmarks. The device was calibrated according to the manufacturer’s instructions before image acquisition. Images were acquired from both sides of the face by the same operator. Each side was measured twice by the same operator, and the mean values from both sides were used for the final analysis to enhance the measurement reliability. The Antera 3D indentation index was defined as the device-derived quantitative measure of negative skin-surface deviation within the selected region of interest, reflecting wrinkle depth and severity. For intra-rater reliability assessment, duplicate Antera 3D indentation-index measurements were used before final averaging. For each participant, a first bilateral mean was calculated from the first right and left temporal measurements, and a second bilateral mean was calculated from the second right and left temporal measurements. Reliability between these duplicate bilateral mean values was assessed using a two-way mixed-effects, absolute-agreement intraclass correlation coefficient (ICC).
Statistical Analysis
Given the paucity of data on facial wrinkling in Asian COPD populations and the reported population-specific differences in skin-aging patterns, we designed this exploratory cross-sectional study. While Western cohorts report a 30.8% prevalence of severe wrinkling in patients with COPD,16 the expected prevalence in Asian populations remains uncertain. Because robust prevalence estimates for severe facial wrinkling among Thai patients with COPD were unavailable, no formal hypothesis-driven sample-size calculation was performed. We aimed to recruit a minimum of 90 participants to enable multivariable regression analysis with adequate statistical power, following the guideline of at least 10 events per predictor variable.41 A total of 93 participants were enrolled, yielding a 41.9% prevalence of severe wrinkling (39 events), which was considered sufficient for exploratory multivariable modeling. Given the modest cohort size, all multivariable findings were interpreted cautiously, with particular attention to potential type II error and model overfitting.
Normally distributed continuous data are presented as mean ± standard deviation, whereas non-normally distributed continuous data are presented as medians with interquartile ranges (IQR). Categorical variables were presented as frequencies and percentages. Participants were stratified by smoking exposure level using a threshold of <10 pack-years versus ≥10 pack-years. Groups were compared using independent t-tests for normally distributed continuous variables or Mann–Whitney U-tests for non-normally distributed data. Categorical variables were compared using the chi-squared or Fisher’s exact test.
Two analytical approaches were employed to identify the independent predictors of wrinkle severity. First, a multiple linear regression was used to model the Antera 3D wrinkle score as a continuous outcome variable. Second, multiple logistic regression was employed to identify predictors of severe wrinkling, defined as a Daniell score of ≥4. Candidate variables were selected a priori based on biological plausibility and prior literature. These included age, sex, BMI, occupational sun exposure, cumulative pack-years of smoking, smoking status, smoking-related COPD status, post-bronchodilator FEV1 % predicted, GOLD stage, diabetes mellitus, hypertension, dyslipidemia, inhaled corticosteroid use, and oral corticosteroid use.
To reduce overfitting, the primary multivariable models used a prespecified parsimonious covariate set consisting of age, sex, BMI, occupational sun exposure, cumulative pack-years of smoking, and post-bronchodilator FEV1 % predicted. All variables in the primary model were retained a priori regardless of statistical significance. Automated backward stepwise selection was not used in the analysis. Multicollinearity was assessed using variance inflation factors (VIFs) for the final predictor matrix. A VIF >5 was considered suggestive of potentially important multicollinearity. Smoking status and continuous pack-years were not entered simultaneously in the model because of conceptual overlap among smoking variables. Cumulative smoking exposure was modeled primarily as a continuous variable in pack-years to preserve dose-response information and avoid loss of statistical power from dichotomization. The ≥10 pack-year threshold was used for descriptive comparisons and sensitivity analyses only. For linear regression, model assumptions were assessed by inspection of residual-versus-fitted plots, Q–Q plots of standardized residuals, homoscedasticity, and influential observations using Cook’s distance. Pack-years were inspected for skewness, and sensitivity analyses using smoking-exposure categories were performed where appropriate.
Sensitivity analyses using smoking-related COPD status and smoking-exposure categories were performed where appropriate. Missing data were assessed for all variables included in the primary analyses. There were no missing data for the outcome or primary covariates; therefore, complete-case analysis was performed. No imputation was applied. Statistical significance was set at a two-tailed α level of 0.05 for all analyses. All statistical analyses were performed using SPSS version 30.0 (IBM Corp., Armonk, NY, USA).
Results
Demographic and Clinical Characteristics
Of the 119 initially screened patients, 93 patients had spirometry-confirmed COPD and were included in the study. Participants were predominantly older and male, with a mean age of 72.6±8.8 years and 84 male patients, representing 90.3%. The cohort demonstrated mild-to-moderate disease severity, with mean post-bronchodilator FEV1 of 63.9±18.8% predicted and most patients classified as GOLD stage II (57.0%) or stage I (23.7%). The median smoking exposure was 20 pack-years (IQR 10–40), with 78.5% classified as having smoking-related COPD. Common comorbidities included hypertension (59.1%), dyslipidemia (53.8%), and diabetes mellitus (24.7%). Most patients used inhaled corticosteroids (63.4%), whereas oral corticosteroid use was uncommon (4.3%). The sun exposure distribution was relatively balanced across low (37.6%), moderate (32.3%), and high (30.1%) categories. The complete baseline characteristics are presented in Table 1.
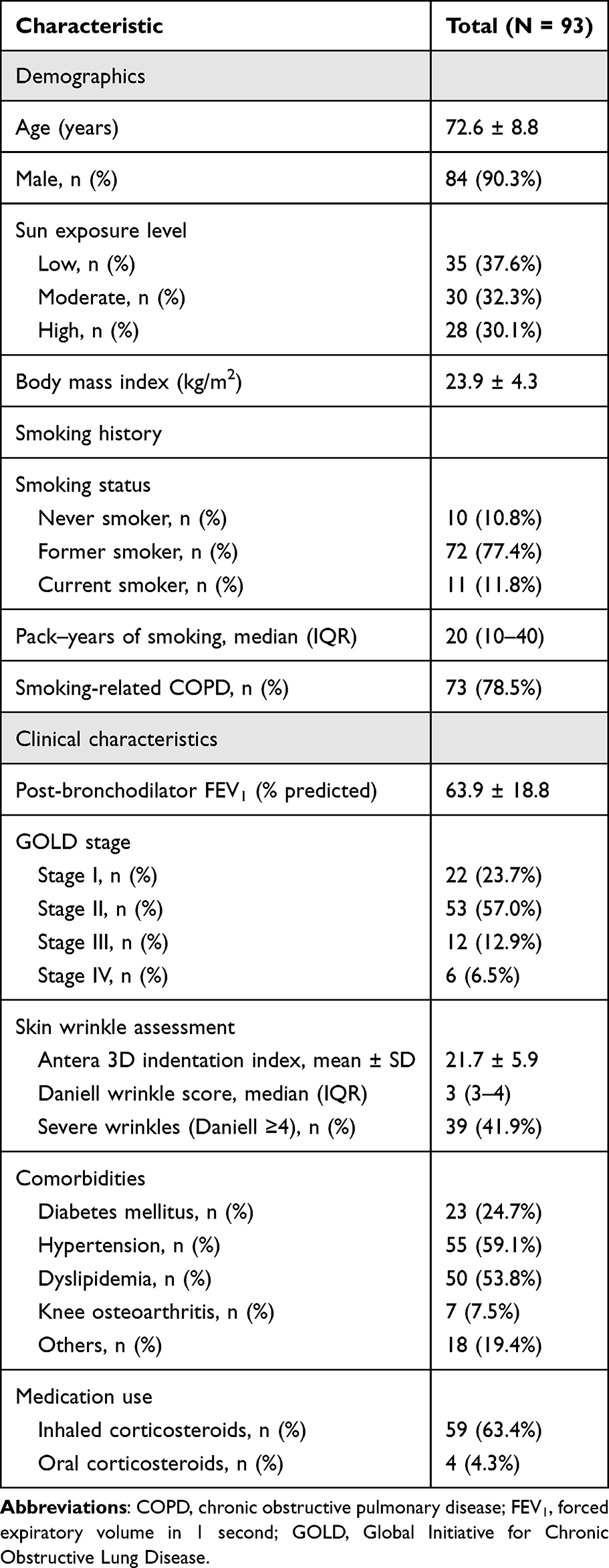 |
Table 1 Characteristics of Patients with Chronic Obstructive Pulmonary Disease in the Study |
Comparison by Smoking Exposure
Participants were stratified according to cumulative smoking exposure into two groups: those with <10 pack-years (n=20) and those with ≥10 pack-years (n=73). The groups were similar in age (p=0.50) and BMI (p=0.82), although the ≥10 pack-years group had a higher male representation (94.5% vs 75.0%, p=0.02). As expected, the smoking status differed markedly (p<0.001). Notably, lung function parameters showed no significant differences between groups: the mean FEV1 % predicted was 69.2±17.7% in the <10 pack-year group versus 62.5±18.9% in the ≥10 pack-year group (p=0.45), and the GOLD stage distribution was comparable (p=0.44). No significant differences emerged in the comorbidity prevalence or medication use patterns between the smoking exposure groups (Table 2).
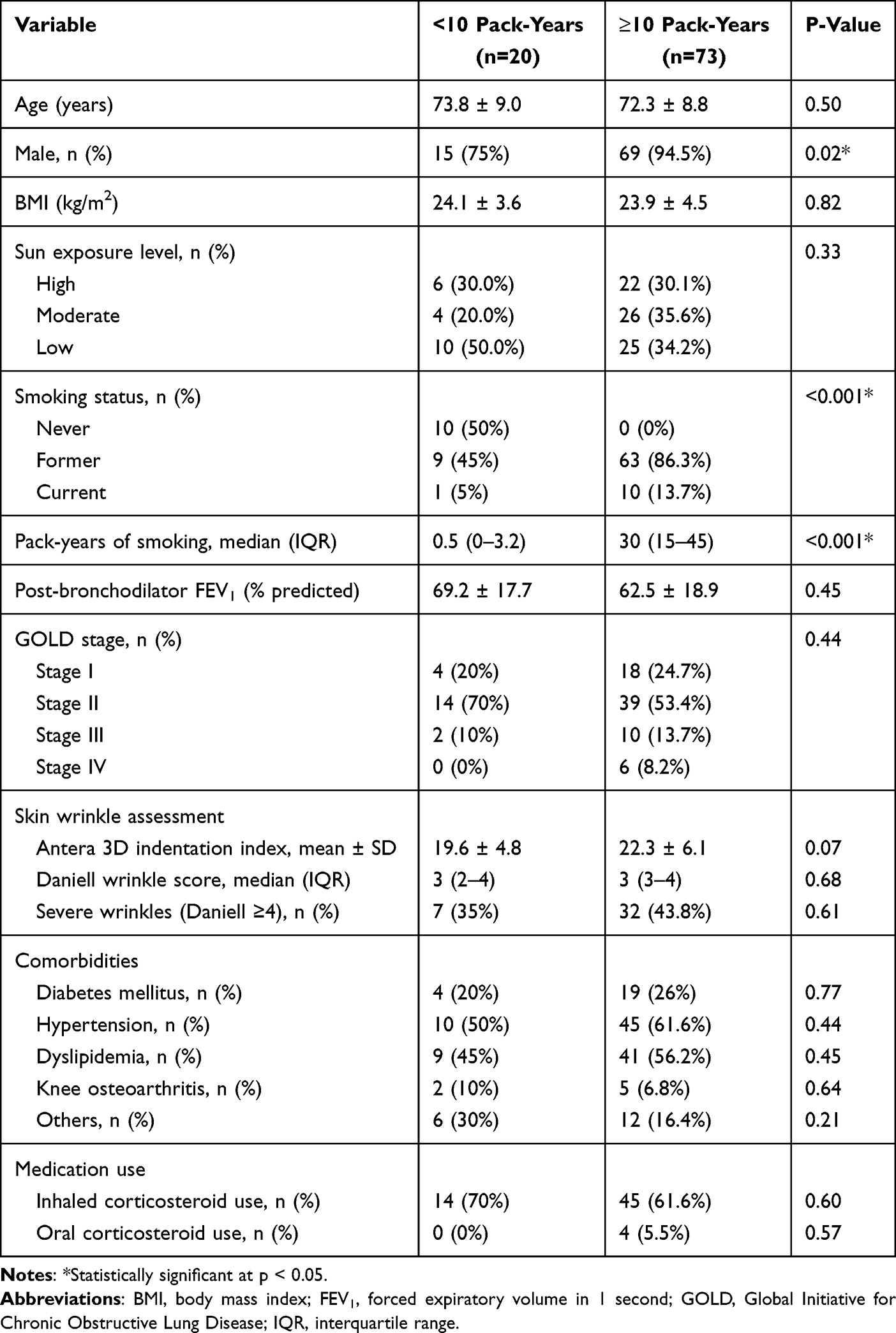 |
Table 2 Characteristics of Patients with Chronic Obstructive Pulmonary Disease by Cumulative Smoking Exposure (<10 vs ≥10 Pack-years) |
Facial Wrinkle Assessment
Objective assessment using Antera 3D yielded a mean indentation index of 21.7±5.9 (range 10.7–40.6), and the duplicate indentation-index measurements demonstrated good intra-rater reliability, with an ICC of 0.86 (95% CI: 0.82–0.97). The subjective Daniell grading showed a median grade of 3 (IQR 3–4), with severe wrinkling (Daniell ≥4) present in 41.9% of patients. The two methods demonstrated a moderate-to-strong positive correlation (Spearman’s ρ=0.68, p<0.001), validating their complementary use. Examination by smoking exposure revealed no significant difference in the prevalence of severe wrinkling: 35.0% in the <10 pack-year group versus 43.8% in the ≥10 pack-year group (p=0.61). Preliminary collinearity assessment demonstrated elevated VIF values when FEV1 % predicted and GOLD stage were included in the same model, with VIF values of 6.71 for FEV1 % predicted and 6.54 for GOLD stage. Post-bronchodilator FEV1 % predicted was selected as the primary continuous lung-function variable because it preserves more information than ordinal GOLD stage. After GOLD stage was removed, multicollinearity was reduced, and the maximum VIF among retained predictors was 1.73.
In the linear regression model, age and BMI were statistically significant predictors of objective wrinkle severity. Age was positively associated with objective wrinkle severity (β=0.08; 95% CI: 0.01–0.24; p=0.042), indicating that each additional year was associated with a 0.08-unit increase in wrinkle score, whereas BMI showed an inverse association (β=−0.34; 95% CI: −0.65, −0.03; p=0.031), suggesting that subcutaneous adipose tissue may attenuate wrinkle severity. Importantly, no COPD-related parameters, including FEV1 %, pack-years of smoking, or smoking-related COPD status, were significantly associated. Similarly, the sun exposure categories, comorbidities, and corticosteroid use showed no significant associations. The overall model had limited explanatory value, with R2=0.29 and adjusted R2=0.16 (Table 3). This indicates that the measured clinical covariates explained only a limited proportion of the variability in objective wrinkle severity.
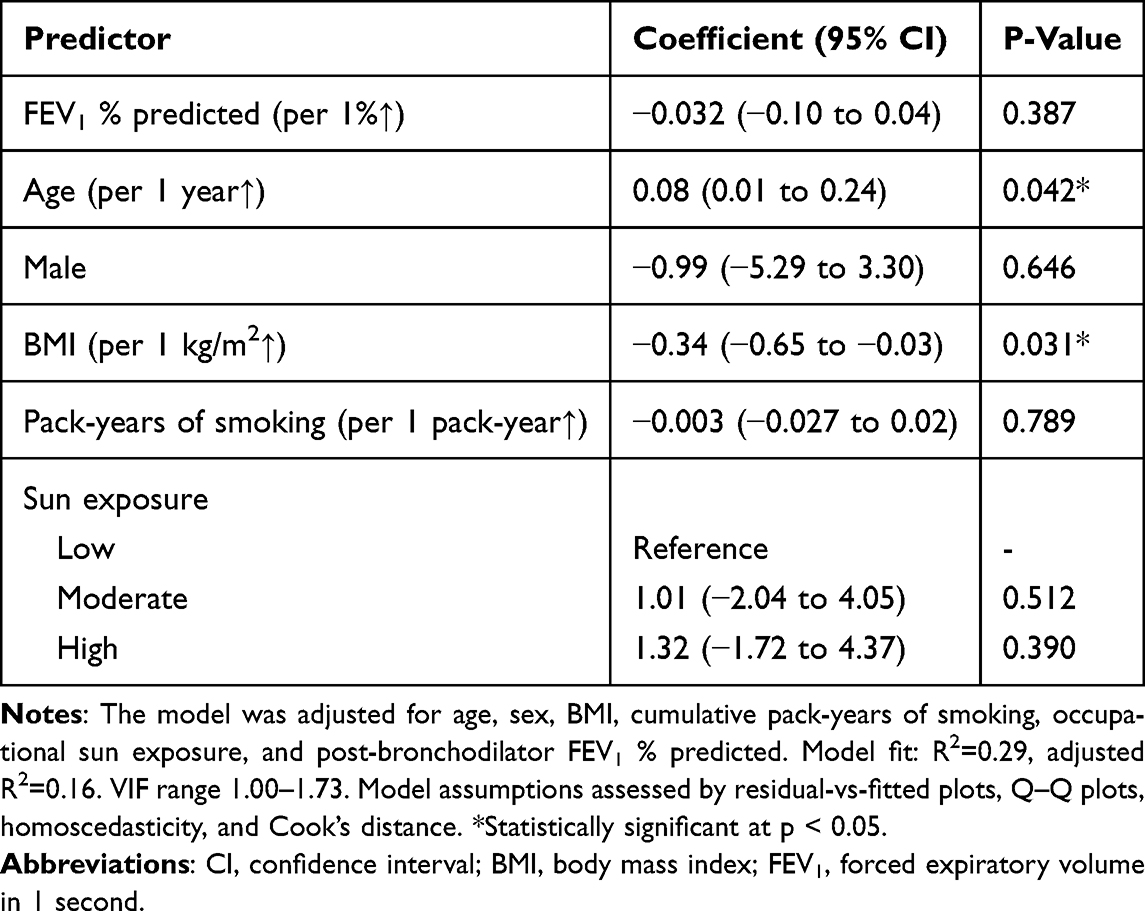 |
Table 3 Multivariable Linear Regression for Objective Wrinkle Assessment |
Logistic regression analysis yielded consistent findings for subjective wrinkle severity. Age remained independently associated with severe wrinkling, with each additional year conferring a 15% increased odds of severe wrinkling (OR=1.15; 95% CI: 1.06–1.23; p<0.001). This translates to 4-fold increased odds over a 10-year period, supporting chronological age as the most consistent predictor of severe wrinkling in this cohort. All COPD-related parameters remained non-significant. The model demonstrated acceptable calibration by the Hosmer-Lemeshow test (χ2=8.26, p=0.43) and explained moderate variance (Nagelkerke R2=0.36) (Table 4).
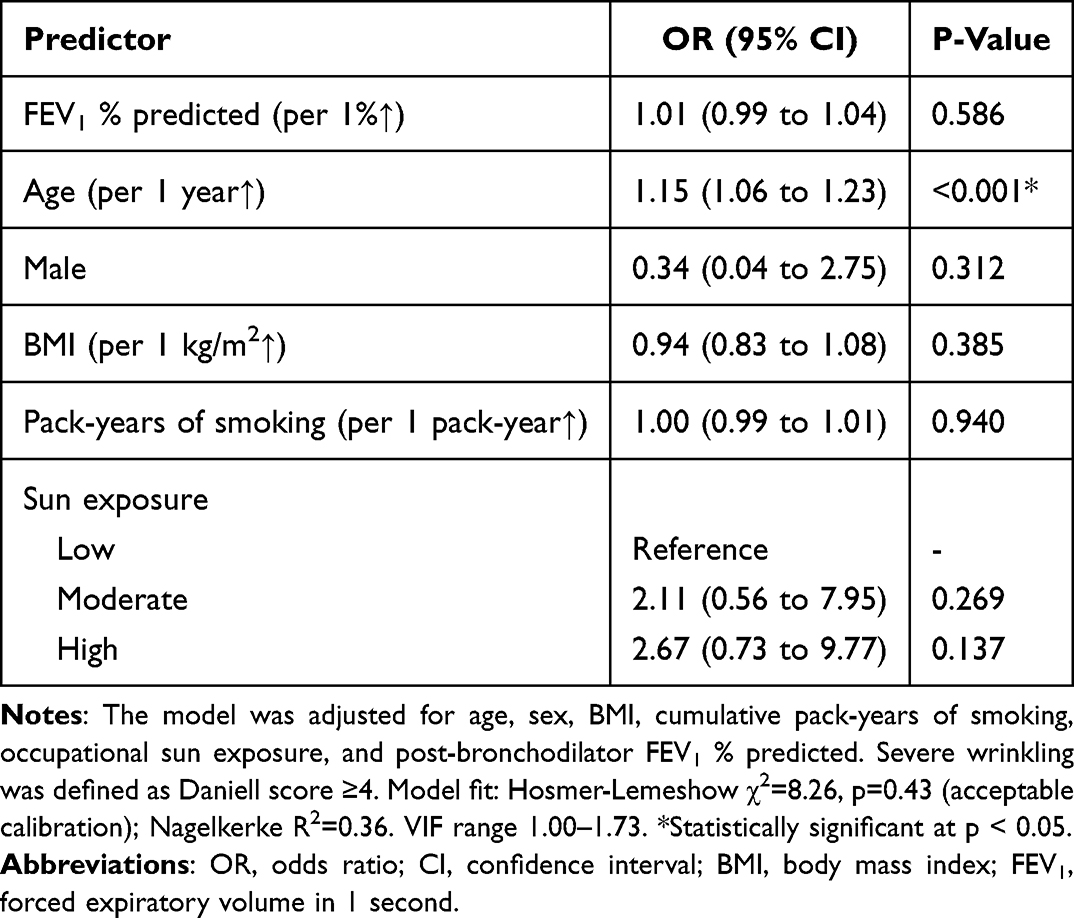 |
Table 4 Multivariable Logistic Regression for Severe Facial Wrinkling |
Sensitivity Analyses
Because no high-resolution CT-only patients were included in the final analytic cohort, sensitivity analysis excluding high-resolution CT-only patients was not applicable. To evaluate whether the findings were influenced by non-smoking COPD, sensitivity analyses were performed. After excluding never smokers, 83 patients remained. The direction and statistical significance of the main findings were unchanged: age remained significantly associated with wrinkle severity, whereas COPD-related variables, including FEV1 % predicted and cumulative pack-years, remained not significantly associated with objective wrinkle severity and severe wrinkling. In the smoking-related COPD subgroup with ≥10 pack-years of exposure (n = 73), the results were similarly unchanged. No significant association was detected in this subgroup between COPD-related variables and facial wrinkle severity. Expanded sensitivity models additionally including smoking-related COPD status, diabetes mellitus, hypertension, dyslipidemia, inhaled corticosteroid use, and oral corticosteroid use yielded similar findings; COPD-related variables remained non-significant.
Age-Wrinkle Relationship
Age and wrinkle severity showed a positive association, demonstrating a weak but statistically significant correlation (Pearson’s r=0.22, p=0.037). The regression equation, Antera 3D score = 0.08 × age + 15.2, indicated that age explained only a small proportion of the variability in objective wrinkle severity, supporting interpretation of the association as statistically significant but small in magnitude.
Discussion
This cross-sectional study evaluated clinical correlates of facial wrinkle severity within a cohort of Thai patients with spirometry-confirmed COPD, rather than determining whether COPD itself is associated with greater wrinkling compared with non-COPD controls. No significant association was detected between facial wrinkle severity, assessed by both subjective Daniell grading and objective Antera 3D imaging, and the COPD-related characteristics assessed, including post-bronchodilator FEV1 % predicted and cumulative smoking exposure. Instead, chronological age was the most consistent predictor of wrinkle severity in all multivariable analyses, while higher BMI was inversely associated with objective wrinkle severity measured by Antera 3D only. These findings differ from associations reported in Western population studies; however, this difference should be interpreted cautiously because the present cohort included only COPD patients, lacked non-COPD smoker and healthy control groups, and was predominantly composed of patients with mild-to-moderate airflow limitation.
Previous studies in predominantly Western populations have reported positive associations between facial wrinkling, smoking-related COPD, emphysema, and impaired lung-function parameters. Patel et al reported that severe facial wrinkling (Daniell score ≥4) was independently associated with COPD presence and extensive emphysema on CT in a predominantly Caucasian cohort, even after controlling for smoking exposure and age.16 Similarly, Szczegielniak et al demonstrated significant negative correlations between total wrinkle length and spirometric parameters including FEV1 in a Polish COPD population.42 O’Brien et al showed that objective skin elasticity measurements correlated significantly with CT emphysema metrics and circulating biomarkers of systemic inflammation and matrix degradation in American smokers.43 In contrast, our Asian cohort demonstrated no association between wrinkle severity and COPD diagnosis, lung function impairment, disease severity stage, or smoking burden after adjustment. The divergence, therefore, may appear to reflect genuine biological or population-specific differences.
The inverse association between BMI and objective wrinkle severity deserves specific consideration. In the linear regression model, higher BMI was associated with lower Antera 3D wrinkle severity, suggesting that facial soft-tissue volume or subcutaneous adipose tissue may partially attenuate objective wrinkle depth. This interpretation is consistent with previous population-based data showing that lower BMI was associated with greater facial wrinkling in both men and women.44 In COPD, BMI also has clinical relevance beyond skin aging, because low BMI may reflect systemic effects such as nutritional depletion, sarcopenia, or cachexia, and has been associated with poorer COPD prognosis in prior studies.45 Therefore, BMI may influence the observed wrinkle phenotype through both mechanical effects on facial soft tissue and systemic health status. Nevertheless, BMI was associated only with the objective Antera 3D measure and not with severe Daniell-grade wrinkling in this study; thus, this finding should be interpreted as exploratory and hypothesis-generating rather than as evidence that BMI protects against facial aging or COPD-related systemic aging.
One possible explanation is that known ethnic differences in cutaneous structures and aging patterns may modify the clinical expression of smoking- and COPD-related skin aging. Asian skin has been reported to differ from Caucasian skin in dermal architecture, collagen organization, pigmentation, and clinical aging phenotype.30–32 These features may influence whether systemic or environmental aging processes manifest predominantly as coarse wrinkling, pigmentary change, laxity, or other skin-aging features. It is therefore conceivable that COPD-associated systemic aging processes in Thai patients might be expressed through pigmentary or elasticity-related changes rather than coarse wrinkling.30–32 However, the present study did not directly measure dermal thickness, collagen content, elastin integrity, pigmentation, matrix metalloproteinase activity, extracellular matrix remodeling, or photoprotection behavior. Therefore, ethnic or population-specific skin biology should be considered a plausible hypothesis rather than a confirmed mechanism underlying the observed findings.
Smoking remains biologically central to both COPD pathogenesis and cutaneous aging. In this study, cumulative smoking exposure was modeled as continuous pack-years in the multivariable analyses, and no significant association was detected between pack-years and wrinkle severity after adjustment for age, BMI, occupational sun exposure, and lung function. The ≥10 pack-year threshold was used for descriptive comparison rather than as the primary smoking-exposure model. Nevertheless, the smoking analysis remains limited. Duration since smoking cessation, passive smoke exposure, smoking intensity over time, and very high cumulative exposure subgroups were not consistently available. Because smoking can affect skin aging through oxidative stress, inflammation, impaired collagen synthesis, and matrix metalloproteinase activation, the absence of a statistically significant association in this cohort should not be interpreted as evidence that smoking has no effect on facial aging. Rather, it indicates that no independent association was detected using the smoking variables available in this dataset.
Cultural and behavioral factors provide an additional layer of complexity. Many Asian societies place strong cultural emphasis on photoprotection through deliberate sun avoidance behaviors, preference for indoor activities, consistent use of sunscreens, and use of physical sun protection, such as wide-brimmed hats, umbrellas, and long-sleeved clothing.34 However, the present study did not capture cumulative lifetime ultraviolet burden or detailed photoprotective practices, including recreational sun exposure and urban versus rural residence, which are important determinants of extrinsic skin aging. Ultraviolet radiation remains a major contributor to photoaging, and incomplete assessment of these factors may have limited the ability to fully account for wrinkle severity.
Conversely, occupational and environmental exposures that are more prevalent in certain Asian populations, including industrial air pollutants, biomass smoke, indoor particulate matter, occupational dust, and chemical irritants, may represent region-specific extrinsic stressors that contribute to both pulmonary and cutaneous aging through oxidative stress and inflammatory pathways.35–37 These cumulative exposome factors were not systematically quantified in the present study and may partly explain the limited explanatory value of the regression model.
The adjusted R2 of the primary linear regression model was 0.16, indicating limited explanatory value, with measured clinical variables accounting for only a small proportion of the variability in objective wrinkle severity. This finding suggests that important unmeasured determinants of facial aging, including lifetime ultraviolet exposure, photoprotection behavior, air pollution, biomass exposure, occupational particulate exposure, diet, skin-care practices, genetic susceptibility, and hormonal factors, may have contributed substantially to wrinkle severity. The modest explanatory value of the model also supports cautious interpretation of nonsignificant COPD-related predictors.
Supporting this conceptual framework is the observation from some Western studies that the association between skin aging and COPD may be strongest when assessed through diffusion capacity rather than spirometric airflow limitation alone.7,43 This suggests that the skin-emphysema link may be most robust when the disease is phenotyped through physiological markers that directly reflect alveolar-capillary membrane integrity and gas exchange. The relatively restricted COPD severity spectrum in the present study may also have attenuated detectable associations, as most participants had mild-to-moderate airflow limitation, with 80.6% classified as GOLD stage I or II and a mean post-bronchodilator FEV1 of approximately 64% predicted. Therefore, the study may have had limited ability to detect associations that might emerge in patients with more advanced emphysema, greater systemic inflammation, or more severe extracellular matrix degradation. In addition, diffusion capacity (DLCO) and quantitative CT-based emphysema burden were not systematically available. This is relevant because emphysema-related connective-tissue destruction and alveolar-capillary impairment may correlate more strongly with diffusion capacity or quantitative emphysema burden than with spirometric airflow limitation alone. Therefore, subtle structural or diffusion-impaired COPD phenotypes may have remained undetected. Future studies in Asian populations should incorporate a comprehensive assessment of diffusion capacity along with alternative cutaneous aging biomarkers.
From a clinical perspective, facial wrinkling alone did not appear to function as a reliable marker of COPD-related disease burden within this Thai COPD cohort. However, because this study lacked healthy Thai controls and non-COPD smoker controls, it cannot determine whether COPD patients have more facial wrinkling than non-COPD individuals, nor can it exclude possible associations in other Thai or Asian populations with broader COPD severity, heavier smoking exposure, or different environmental exposures. Dermatologists evaluating Asian patients who present with premature facial wrinkling should therefore exercise caution in attributing such findings to underlying emphysema or recommending pulmonary evaluation based on skin findings alone. The findings therefore support population-specific validation of cutaneous markers rather than direct extrapolation from Western cohorts.
This study has several methodological strengths, including dual wrinkle assessment combining subjective clinical grading with objective three-dimensional imaging, blinded dermatologist evaluation, spirometry-confirmed COPD in the final analytic cohort, comprehensive adjustment for potential confounders in multivariable analyses, and a specific focus on an Asian population that has been underrepresented in prior wrinkle-COPD research. However, several limitations of this study warrant emphasis. The cross-sectional study design precludes causal or temporal inferences. The sample size was substantially modest, which may have increased the risk of type II error, particularly for subtle associations and subgroup analyses. Our cohort was predominantly older and male and consisted exclusively of Thai participants, which limits its generalizability. Finally, potential selection bias may have been introduced through recruitment at a tertiary referral center, which may have over-represented more severe or complex COPD cases compared to community-based populations. Moreover, the study did not include non-COPD controls, DLCO, quantitative CT emphysema assessment, objective cumulative ultraviolet measurement, detailed photoprotection behavior, recreational sun exposure, air-pollution exposure, biomass exposure, passive smoking, smoking-cessation duration, or molecular and structural skin biomarkers. Future studies should include longitudinal designs, control groups, broader COPD severity, quantitative CT and DLCO phenotyping, and more sensitive skin-aging markers such as dermal elasticity, high-frequency ultrasonography, pigmentation analysis, and extracellular matrix biomarkers.
Conclusion
In this cross-sectional study of Thai patients with spirometry-confirmed COPD, no significant association was detected between facial wrinkle severity and the COPD-related characteristics assessed, including airflow limitation and cumulative smoking exposure. Instead, chronological age was the most consistent predictor of wrinkle severity, while higher BMI showed an inverse association with objective Antera 3D wrinkle severity only. These findings should be interpreted cautiously because the study was cross-sectional, the sample size was modest, and most participants had mild-to-moderate COPD, which may have limited the ability to detect subtle associations with advanced emphysema or COPD-related systemic aging. Therefore, the findings describe associations rather than causal relationships and apply specifically to this Thai COPD cohort. Based on these results, facial wrinkling alone may not serve as a reliable standalone screening or severity marker for COPD in Thai patients without further validation. Future studies should evaluate larger multicenter cohorts with broader COPD severity, non-COPD controls, quantitative CT or DLCO phenotyping, and more sensitive cutaneous aging markers.
Data Sharing Statement
The data produced and analyzed in this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Mahidol University Review Board for Ethics in Human Research (MURA2023/810) and performed in accordance with the principles of the Declaration of Helsinki. Informed consent was obtained from all participants before enrollment, and data anonymization was performed before analysis.
Funding
The authors received no financial support for this research.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet. 2016;388(10053):1545–13. doi:10.1016/s0140-6736(16)31678-6
2. O’Donnell DE. Hyperinflation, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2006;3(2):180–184. doi:10.1513/pats.200508-093DO
3. Mannino DM, Buist AS. Global burden of COPD: risk factors, prevalence, and future trends. Lancet. 2007;370(9589):765–773. doi:10.1016/s0140-6736(07)61380-4
4. Brusselle GG, Joos GF, Bracke KR. New insights into the immunology of chronic obstructive pulmonary disease. Lancet. 2011;378(9795):1015–1026. doi:10.1016/s0140-6736(11)60988-4
5. Martinez FJ, Donohue JF, Rennard SI. The future of chronic obstructive pulmonary disease treatment--difficulties of and barriers to drug development. Lancet. 2011;378(9795):1027–1037. doi:10.1016/s0140-6736(11)61047-7
6. McAllister DA, Maclay JD, Mills NL, et al. Arterial stiffness is independently associated with emphysema severity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2007;176(12):1208–1214. doi:10.1164/rccm.200707-1080OC
7. Bon J, Fuhrman CR, Weissfeld JL, et al. Radiographic emphysema predicts low bone mineral density in a tobacco-exposed cohort. Am J Respir Crit Care Med. 2011;183(7):885–890. doi:10.1164/rccm.201004-0666OC
8. Watz H, Waschki B, Kirsten A, et al. The metabolic syndrome in patients with chronic bronchitis and COPD: frequency and associated consequences for systemic inflammation and physical inactivity. Chest. 2009;136(4):1039–1046. doi:10.1378/chest.09-0393
9. Frei A, Muggensturm P, Putcha N, et al. Five comorbidities reflected the health status in patients with chronic obstructive pulmonary disease: the newly developed COMCOLD index. J Clin Epidemiol. 2014;67(8):904–911. doi:10.1016/j.jclinepi.2014.03.005
10. Smith BS, Williamson N, McConkey B. Dermal connective tissue in patients with chronic obstructive airways disease. Lancet. 1967;1(7486):341–343. doi:10.1016/s0140-6736(67)92891-7
11. Chanprapaph K, Mahasaksiri T, Kositkuljorn C, Leerunyakul K, Suchonwanit P. Prevalence and risk factors associated with the occurrence of autoimmune diseases in patients with alopecia areata. J Inflamm Res. 2021;14:4881–4891. doi:10.2147/jir.S331579
12. Viegi G, Pistelli F, Sherrill DL, Maio S, Baldacci S, Carrozzi L. Definition, epidemiology and natural history of COPD. Eur Respir J. 2007;30(5):993–1013. doi:10.1183/09031936.00082507
13. Han MK, Agusti A, Calverley PM, et al. Chronic obstructive pulmonary disease phenotypes: the future of COPD. Am J Respir Crit Care Med. 2010;182(5):598–604. doi:10.1164/rccm.200912-1843CC
14. Mercado N, Ito K, Barnes PJ. Accelerated ageing of the lung in COPD: new concepts. Thorax. 2015;70(5):482–489. doi:10.1136/thoraxjnl-2014-206084
15. Rivas M, Gupta G, Costanzo L, Ahmed H, Wyman AE, Geraghty P. Senescence: pathogenic Driver in Chronic Obstructive Pulmonary Disease. Medicina. 2022;58(6):817. doi:10.3390/medicina58060817
16. Patel BD, Loo WJ, Tasker AD, et al. Smoking related COPD and facial wrinkling: is there a common susceptibility? Thorax. 2006;61(7):568–571. doi:10.1136/thx.2005.053827
17. Just M, Monsó E, Ribera M, Lorenzo JC, Morera J, Ferrandiz C. Relationships between lung function, smoking and morphology of dermal elastic fibres. Exp Dermatol. 2005;14(10):744–751. doi:10.1111/j.1600-0625.2005.00353.x
18. Daniell HW. Smoker’s wrinkles. A study in the epidemiology of “crow’s feet”. Ann Intern Med. 1971;75(6):873–880. doi:10.7326/0003-4819-75-6-873
19. Messaraa C, Metois A, Walsh M, et al. Wrinkle and roughness measurement by the Antera 3D and its application for evaluation of cosmetic products. Skin Res Technol. 2018;24(3):359–366. doi:10.1111/srt.12436
20. Yin L, Morita A, Tsuji T. Alterations of extracellular matrix induced by tobacco smoke extract. Arch Dermatol Res. 2000;292(4):188–194. doi:10.1007/s004030050476
21. Lahmann C, Bergemann J, Harrison G, Young AR. Matrix metalloproteinase-1 and skin ageing in smokers. Lancet. 2001;357(9260):935–936. doi:10.1016/s0140-6736(00)04220-3
22. Knuutinen A, Kokkonen N, Risteli J, et al. Smoking affects collagen synthesis and extracellular matrix turnover in human skin. Br J Dermatol. 2002;146(4):588–594. doi:10.1046/j.1365-2133.2002.04694.x
23. Just M, Ribera M, Monsó E, Lorenzo JC, Ferrándiz C. Effect of smoking on skin elastic fibres: morphometric and immunohistochemical analysis. Br J Dermatol. 2007;156(1):85–91. doi:10.1111/j.1365-2133.2006.07575.x
24. Ortiz A, Grando SA. Smoking and the skin. Int J Dermatol. 2012;51(3):250–262. doi:10.1111/j.1365-4632.2011.05205.x
25. Suchonwanit P, Leerunyakul K, Kositkuljorn C. Diagnostic and prognostic values of cutaneous manifestations in COVID-19. Dermatol Ther. 2020;33(4):e13650. doi:10.1111/dth.13650
26. Bosset S, Bonnet-Duquennoy M, Barré P, et al. Photoageing shows histological features of chronic skin inflammation without clinical and molecular abnormalities. Br J Dermatol. 2003;149(4):826–835. doi:10.1046/j.1365-2133.2003.05456.x
27. Iddamalgoda A, Le QT, Ito K, Tanaka K, Kojima H, Kido H. Mast cell tryptase and photoaging: possible involvement in the degradation of extra cellular matrix and basement membrane proteins. Arch Dermatol Res. 2008;300(Suppl 1):S69–76. doi:10.1007/s00403-007-0806-1
28. Kaukinen A, Fitzgibbon A, Oikarinen A, Hinkkanen L, Viinikanoja M, Harvima IT. Increased numbers of tryptase-positive mast cells in the healthy and sun-protected skin of tobacco smokers. Dermatology. 2014;229(4):353–358. doi:10.1159/000365189
29. Rattananukrom T, Suchonwanit P. Are drug treatment strategies really effective against alopecia areata? Expert Opin Pharmacother. 2021;22(3):257–260. doi:10.1080/14656566.2020.1854728
30. Rawlings AV. Ethnic skin types: are there differences in skin structure and function? Int J Cosmet Sci. 2006;28(2):79–93. doi:10.1111/j.1467-2494.2006.00302.x
31. Nouveau-Richard S, Yang Z, Mac-Mary S, et al. Skin ageing: a comparison between Chinese and European populations. A pilot study. J Dermatol Sci. 2005;40(3):187–193. doi:10.1016/j.jdermsci.2005.06.006
32. Lin KH, Liao YH, Wei ML, Sun CK. Comparative analysis of intrinsic skin aging between Caucasian and Asian subjects by slide-free in vivo harmonic generation microscopy. J Biophotonics. 2020;13(4):e201960063. doi:10.1002/jbio.201960063
33. Thadanipon K, Suchonwanit P. Measuring Patient Quality of Life Following Treatment for Alopecia. Patient Prefer Adherence. 2021;15:1601–1610. doi:10.2147/ppa.S282399
34. Goh CL, Kang HY, Morita A, et al. Awareness of sun exposure risks and photoprotection for preventing pigmentary disorders in Asian populations: survey results from three Asian countries and expert panel recommendations. Photodermatol Photoimmunol Photomed. 2024;40(1):e12932. doi:10.1111/phpp.12932
35. Wang XR, Christiani DC. Respiratory symptoms and functional status in workers exposed to silica, asbestos, and coal mine dusts. J Occup Environ Med. 2000;42(11):1076–1084. doi:10.1097/00043764-200011000-00009
36. Li J, Yin P, Wang H, et al. The disease burden attributable to 18 occupational risks in China: an analysis for the global burden of disease study 2017. Environ Health. 2020;19(1):21. doi:10.1186/s12940-020-00577-y
37. Lee S, Lee SH, Lee W. Impact of occupational dust exposure on dermatologic symptoms among Korean workers. Toxicol Ind Health. 2020;36(12):971–978. doi:10.1177/0748233720964636
38. Suchonwanit P, Pakornphadungsit K, Leerunyakul K, Khunkhet S, Sriphojanart T, Rojhirunsakool S. Frontal fibrosing alopecia in Asians: a retrospective clinical study. Int J Dermatol. 2020;59(2):184–190. doi:10.1111/ijd.14672
39. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: 2025 Report. 2024;2024:1–200. https://goldcopd.org/2025-gold-report/.
40. Bhatt SP, Kim YI, Harrington KF, et al. Smoking duration alone provides stronger risk estimates of chronic obstructive pulmonary disease than pack-years. Thorax. 2018;73(5):414–421. doi:10.1136/thoraxjnl-2017-210722
41. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/s0895-4356(96)00236-3
42. Szczegielniak J, Bogacz K, Łuniewski J, Krajczy M, Pilis W, Majorczyk E. Excessive Facial Wrinkling Is Associated with COPD Occurrence-Does COPD Damage Skin Beauty and Quality? Int J Environ Res Public Health. 2023;20(3):1991. doi:10.3390/ijerph20031991
43. O’Brien ME, Chandra D, Wilson RC, et al. Loss of skin elasticity is associated with pulmonary emphysema, biomarkers of inflammation, and matrix metalloproteinase activity in smokers. Respir Res. 2019;20(1):128. doi:10.1186/s12931-019-1098-7
44. Hamer MA, Pardo LM, Jacobs LC, et al. Lifestyle and Physiological Factors Associated with Facial Wrinkling in Men and Women. J Invest Dermatol. 2017;137(8):1692–1699. doi:10.1016/j.jid.2017.04.002
45. Cao C, Wang R, Wang J, Bunjhoo H, Xu Y, Xiong W. Body mass index and mortality in chronic obstructive pulmonary disease: a meta-analysis. PLoS One. 2012;7(8):e43892. doi:10.1371/journal.pone.0043892
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.