Back to Journals » Patient Preference and Adherence » Volume 16
Face Mask Practice and Technique During the COVID-19 Pandemic: A Nonrepresentative Cross-Sectional Study in Sudan
Authors Ayed IIA, Khalil R ![]() , Adam I
, Adam I ![]() , Al-Wutayd O
, Al-Wutayd O ![]()
Received 18 March 2022
Accepted for publication 12 April 2022
Published 3 May 2022 Volume 2022:16 Pages 1163—1176
DOI https://doi.org/10.2147/PPA.S366099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Itimad IA Ayed,1,2 Rehana Khalil,3 Ishag Adam,4 Osama Al-Wutayd3
1Department of Basic Medical Sciences, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Saudi Arabia; 2Department of Pharmacology, Faculty of Medicine, International University of Africa, Khartoum, Sudan; 3Department of Family and Community Medicine, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Saudi Arabia; 4Department of Obstetrics and Gynecology, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Kingdom of Saudi Arabia
Correspondence: Osama Al-Wutayd, Email [email protected]
Background: The World Health Organization issued guidelines for face mask use in community settings during the current COVID-19 pandemic. However, data are limited on public compliance with those guidelines in Sudan. Therefore, this study assessed face mask-wearing practice and technique during the COVID-19 pandemic among residents of Sudan.
Methods: A cross-sectional study was conducted from July to September 2021 among Sudanese aged ≥ 18 years. A web-based questionnaire was shared through different social media platforms. Personal characteristics, four knowledge-associated items, three attitude-associated items, one item concerning mask-wearing practice, and five items related to mask-wearing technique were determined. Univariate, bivariate, and multivariable analyses were performed using STATA v17.
Results: The survey included 1059 participants (48% males, 52% females) from different regions of Sudan. The overall mean ± SD was 3 ± 0.73 for knowledge of COVID-19 transmission; 2.3 ± 0.71 for attitude toward wearing face masks; 0.38 ± 0.49 for the practice of wearing a face mask; and 4.17 ± 0.97 for face mask-wearing technique. Approximately one-third (38%) of participants always wore a face mask during the pandemic, with age, sex, education level, family income, face mask attitude, occupation, and history of COVID-19 infection affecting the practice. All steps of face mask-wearing technique were performed by 46% of participants (59% performed hand hygiene before putting on a mask and 86% after removing it; 98% covered mouth and nose; 90% adjusted masks at the nose bridge, and 84% tied masks securely), and associated with age, occupation, family income, history of COVID-19 infection, and face-mask attitude.
Conclusion: Although knowledge and attitude were relatively good, the practice of wearing a face mask and using proper techniques among participants were low. To ensure optimal face mask use and proper mask-wearing techniques, educational intervention and establishing governmental regulations are highly recommended.
Keywords: knowledge, technique, practices, Sudan, face mask, COVID-19, pandemic
Introduction
Because of the COVID-19 pandemic, face masks have been worn for more than one and a half years in public places.1 Effectiveness of wearing face masks in public settings has been subject to worldwide debate.2,3 The World Health Organization (WHO) and the Centers for Disease Control and Prevention have recommended the use of face masks in the community, but direct evidence from such settings to support face mask use is limited.4,5 Multilayer cloth masks block 50% to 70% of small droplets and particles in laboratory experiments;6,7 the filtering respirator masks N95, N99, and N100 block 95%, 99%, and 99.97%, respectively, of particles with a median diameter of 0.3 μm, according to NIOSH standards;8 and surgical masks can reduce the outward emission rate of particles by 90% during speaking and coughing.9 In a systematic review and meta-analysis of six studies with a total of 1233 participants, face mask use was associated with a significant decrease in risk of COVID-19 infection.10 In another systematic review and meta-analysis that included 21 studies, face mask use provided protection against transmission of respiratory viral infection.11 In a recent sample of US Navy staff, rate of COVID-19 infection was lower (55.8%) among those wearing a mask than among those who did not (80.8%).12 However, the sample in that study was nonrepresentative of the general public. In a meta-analysis that examined the effects of face mask use, physical distancing, and eye protection on the spread of COVID-19, SARS, and MERS in both health care and public settings, face masks helped to significantly reduce the risk of those infections.13 Although the effects of consensual or mandatory face mask use on COVID-19 infection rates have been examined in some studies, none were conducted in African countries.14–18
Sudan is among the largest African countries and covers 1.886 million km2. It has a diverse ethnic (African and Afro-Arab) population of 40.53 million, but the country is underdeveloped.19 From January 3, 2020, to February 8, 2022, total confirmed COVID-19 cases were 59,294 with 3632 deaths. A total of 4,991,228 vaccine doses had been administered as of October 16, 2021.20 The first COVID-19 case was diagnosed on March 12, 2020, and the Sudanese government initially imposed national restrictions on domestic travel and implemented a partial lockdown as preventive measures. However, those measures were ineffective because of poor adherence within the community.21 A steady increase occurred in numbers of cases and deaths in Sudan because of limited testing capacity and hospital beds.19,21 In response, a mandatory face mask-wearing policy in state institutions, workplaces, schools, public transport, and all gathering places subject to overcrowding was announced by Sudan’s Minister of Health.22
The practice of wearing masks in the community can limit the spread of the SARS-CoV-2 virus.23 Therefore, the more widely the community adopts mask wearing, the greater the protection for the whole community, which is similar to the principle of herd immunity for vaccination.24 Thus, widespread mask use in the community is more important than the type of mask worn,25 and public compliance with WHO recommendations is a key feature of successful risk management for highly contagious diseases such as COVID-19. The WHO issued guidelines on the correct use of masks in the context of COVID-19, derived from best practices in health-care settings.26 An understanding of knowledge, attitudes, and practices (KAPs) regarding face mask use during the COVID-19 pandemic is essential for health-care authorities to determine readiness to accept behavioral change measures. Assessing KAPs of the general population could help identify gaps in understanding of KAPs, and such an assessment could serve as a guideline to develop timely and required strategies to promote health. This study is the first to assess the practice and technique of wearing face masks among Sudanese residents during the COVID-19 pandemic.
Methods
Study Design and Setting
A web-based, nonrepresentative cross-sectional study of Sudanese adults was conducted from July to September 2021 during the COVID-19 pandemic.
Questionnaire Preparation and Description
An online questionnaire was prepared using Google Forms, and the link was shared through social media platforms, initially to the contacts of one of the authors. Participants were asked to send the survey link to family and friends on their contact lists whom they considered would fulfill the criteria for this study; their friends were also encouraged to send the link to their own contact networks. The questionnaire was based on a literature review of face masks and WHO guidelines.26–29 Content and face validity of the questionnaire were ensured by experts. The questionnaire was pilot-tested among a sample of 35 subjects, and the final version was reviewed and approved. The questionnaire comprised five sections: sociodemographic information, knowledge of route of transmission of COVID-19, attitude toward face masks, practice of face mask use during the pandemic, face mask-wearing technique, and barriers to wearing a face mask. Monthly family income was grouped into three categories: ≤US$23 (≤10,000 Sudanese pounds (SDG)) per month (low income), >$23 (>10,000 SDG) to $125 (55,000 SDG) per month (middle income), and >$125 (>55,000 SDG) per month (high income).30 Knowledge about route of transmission of COVID-19 was assessed by four items (K1–4), which were used to calculate a knowledge score. Three items (A1–3) were used to assess attitudes toward COVID-19 and use of face masks, with each item categorized as either positive or negative. Practice of face mask use was assessed by one item (P1), categorized as always or sometimes/never. Face mask-wearing technique was assessed in five steps (S1–5), and categories were either always performed all steps of face mask-wearing technique or sometimes/never. In knowledge, practice, and technique sections, each correct question received one point, with zero given for an incorrect one. In the attitude section, a positive attitude received one point, with zero assigned for a negative attitude (Table 1). The objective and inclusion/exclusion criteria of the study were included on the cover page of the survey, and consent to participate was required before beginning the questionnaire.
 |
Table 1 Knowledge, Attitudes, Practice, and Technique Regarding Wearing of Face Masks During the COVID-19 Pandemic in Sudan (n = 1059) |
Sample Size Calculation
Sample size was calculated using OpenEpi software. The minimum sample size was 500 participants with 80% statistical power and 5% type I error. The practice of wearing face masks was assumed to be 50% in order to attain the maximum sample size, taking into account 30% expected incomplete and missing responses.
Statistical Analyses
Data were obtained in an Excel sheet after exporting to STATA v17 (StataCorp, College Station, TX, USA). Data are presented as mean ± SD for continuous variables and as percentage for categorical variables. Continuous variables were compared using either Student’s t-tests or one-way ANOVAs for more than two groups, and chi-squared tests were performed to compare categorical variables. Multivariable regression analysis was performed to identify determinants of knowledge, attitude, practice, and technique of wearing face masks. Variables at p < 0.25 in the bivariate analysis were included in the multivariable analysis. A multiple linear regression analysis was conducted to determine factors that affected the knowledge score. A multiple logistic regression analysis was performed to identify factors that affected attitudes, practice, and technique of face-mask wearing. Odds ratios (ORs), beta coefficients, and 95% confidence intervals (CIs) are reported. A p-value ≤0.05 was considered as strong evidence against the null hypothesis.
Results
Sociodemographic Characteristics
A total of 1059 participants responded to the survey. Of the participants, 664 (63%) were aged 18 to 30 years, 548 (52%) were females, 527 (50%) had secondary school education or higher, 711 (67%) were single, 507 (48%) were employed, 504 (48%) had family income of 10,000 to 55,000 SDG, 203 (19%) had chronic disease, and 257 (24%) had a history of COVID-19 infection (Table 2).
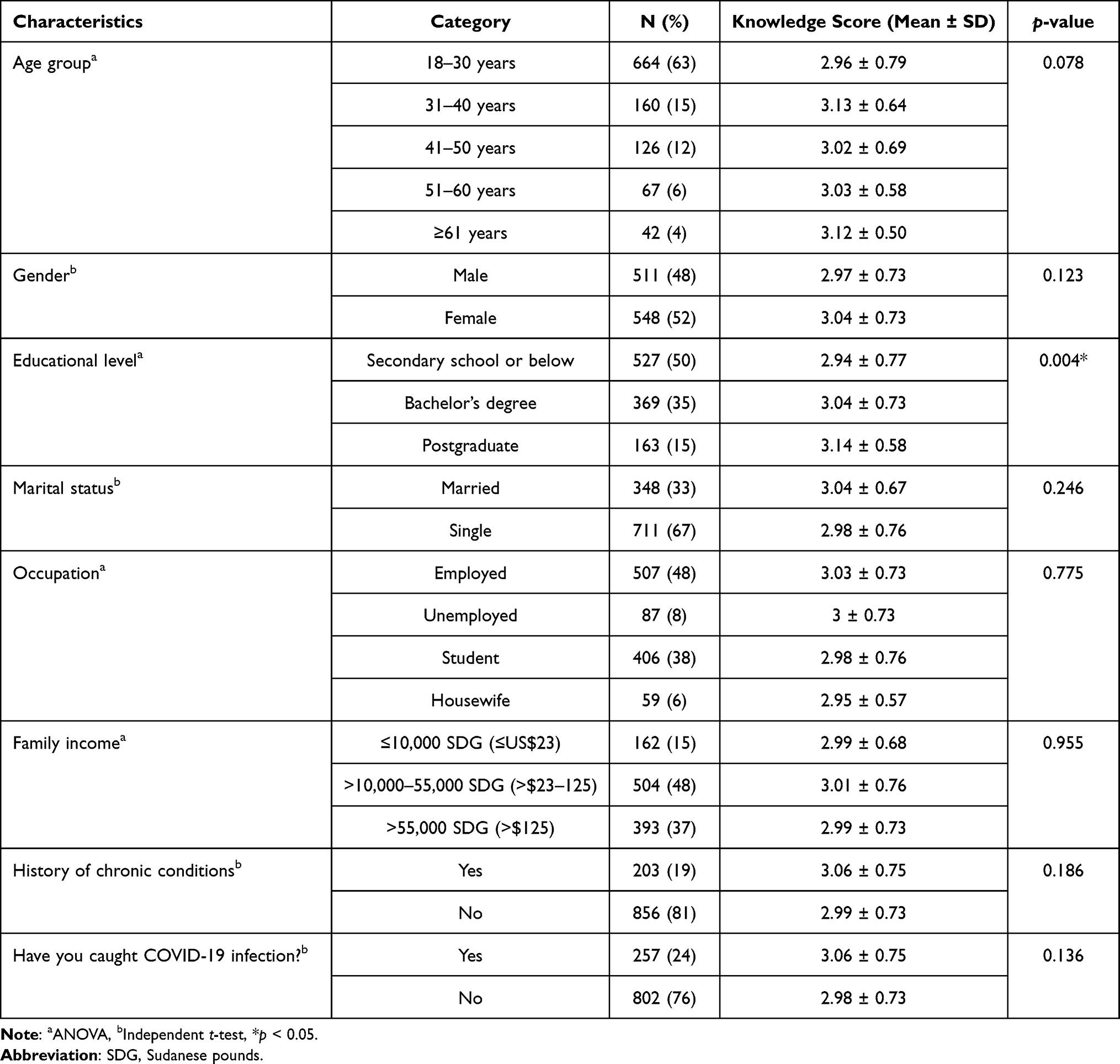 |
Table 2 Participant Socioeconomic Characteristics and Knowledge Level About Route of Transmission of COVID-19 in Sudan |
Knowledge About Route of Transmission of COVID-19
The mean score for knowledge was 3 (SD = 0.73, range 1–4), and the range of correct responses was from 49% to 94%. According to bivariate analysis, respondents with a higher level of education had significantly higher knowledge scores (p = 0.004; Table 2).
Table 3 displays the multiple linear regression on age group (31–40 vs 18–29 years; β = 0.15 [CIs: −0.01, 0.31]; p = 0.074), gender (female vs male; β = 0.08 [CIs: −0.01, 0.17]; p = 0.075), and education level (postgraduate vs bachelor’s degree; β = 0.15 [CIs: −0.003, 0.29]; p = 0.056), which had a borderline positive influence on the knowledge mean score.
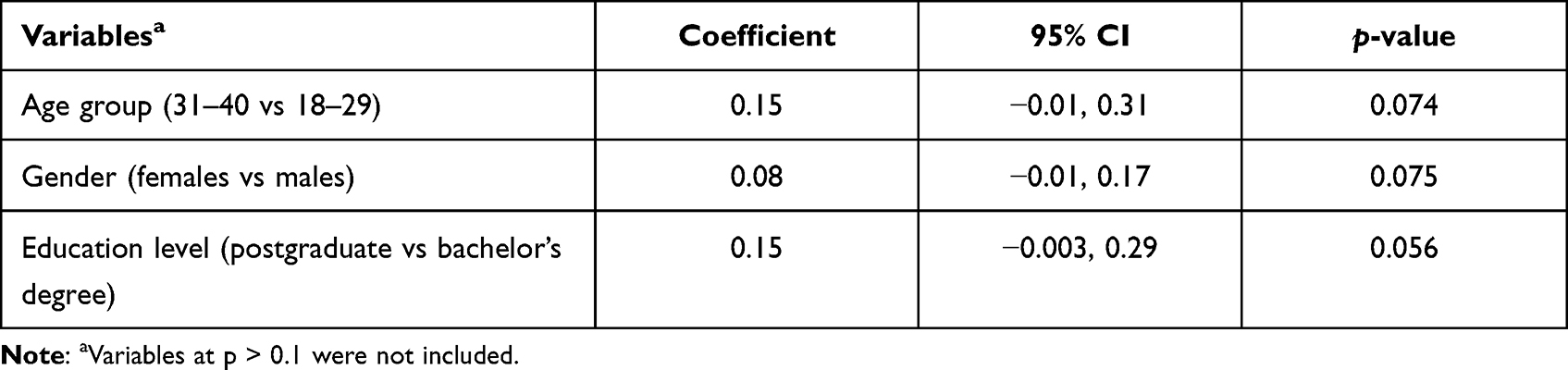 |
Table 3 Multiple Linear Regression on Factors Associated with Knowledge About Route of Transmission of COVID-19 |
Attitude Toward Wearing Face Masks
The mean attitude score was 2.3 (SD = 0.71, range 0–3), and the positive attitude rate ranged from 48% to 94% (Table 1). Associations between attitudes and independent variables in bivariate analyses are displayed in Table 4. The multiple logistic regression showed negative responses to A1 (“Do you think that you are vulnerable to infection?”) more often among males (vs females; aOR 1.48, p = 0.005) and those with history of COVID-19 infection (vs no history of COVID-19 infection; aOR 1.99, p < 0.001) and less often among those with postgraduate education (vs secondary school education or below; aOR 0.57, p = 0.026). Negative responses to A3 (“Do you think wearing a mask can reduce the chance of getting COVID-19?”) were more common among those with a family income of ≤$23 (vs >$23–125; aOR 2.28, p = 0.015; Table 5).
 |
Table 4 Bivariate Analysis of Factors Associated with Attitudes Regarding Practice of Wearing Face Masks |
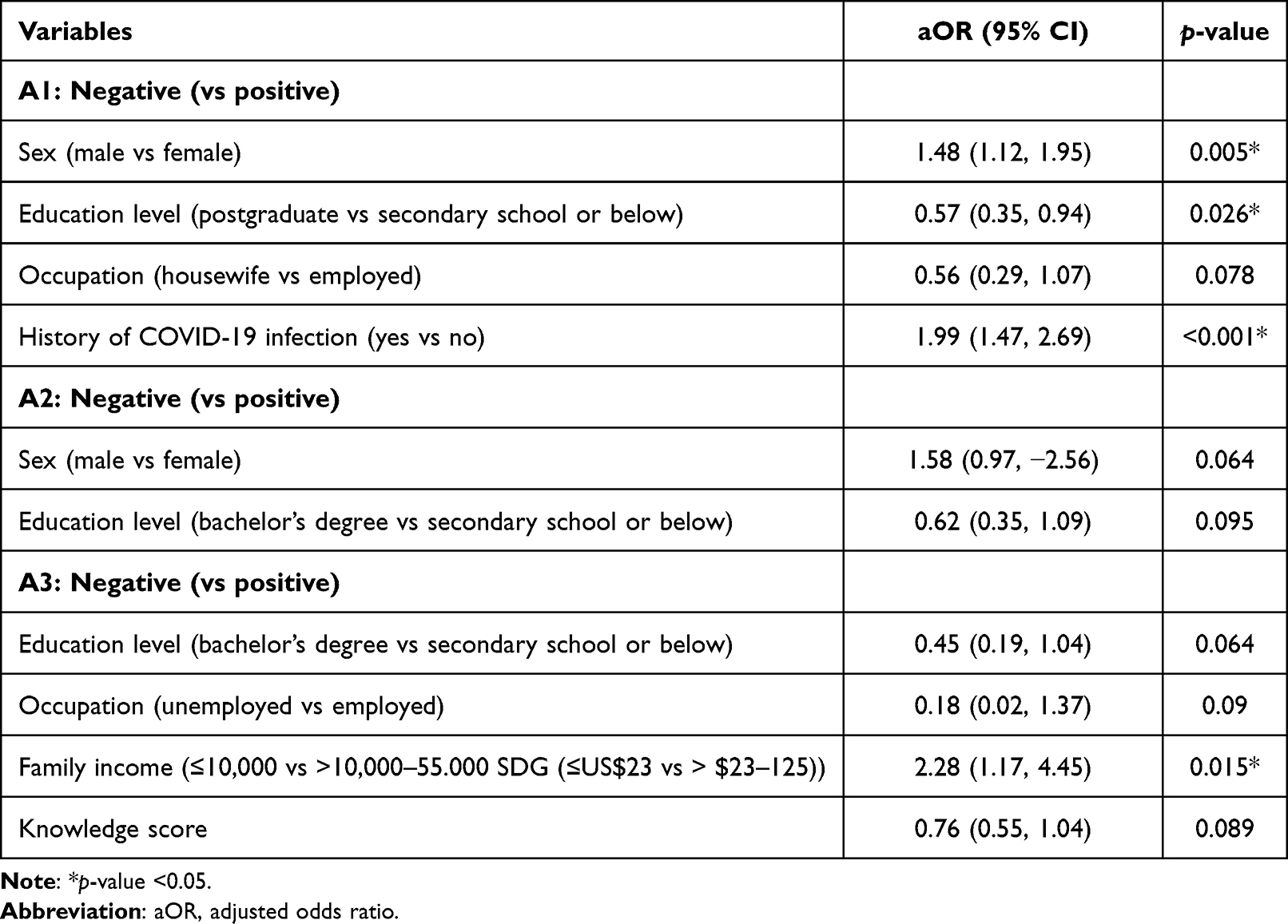 |
Table 5 Multiple Logistic Regression on Factors Associated with Negative Attitudes Regarding Practice of Wearing Face Masks |
Practice of Wearing Face Masks
Of participants, 38% (n = 401) always wore a face mask during the pandemic, 57% (n = 608) used the practice sometimes, and 5% (n = 50) never wore a face mask. Most participants (n = 707, 70%) used medical masks; whereas 30% (n = 302) used cloth masks. Approximately 37% (n = 375) replaced their mask with a new, clean and dry one as soon as it became damp, soiled, or wet, with 29% (n = 293) replacing it at least once daily, 19% (n = 192) replacing it every time they went outside their home, and 15% (n = 149) replacing it with uncertain frequency. According to bivariate analysis, factors significantly associated with never/sometimes wearing face masks were age group of 51–60 years (p < 0.001), males (p < 0.001), educational level of secondary school or below (p < 0.001), single marital status (p = 0.002), students (p = 0.041), family income of >$23–125 (p = 0.029), no history of chronic illnesses (p = 0.001), and attitude score (p < 0.001) (Table 6). A multiple logistic regression analysis on factors revealed that only males (aOR 1.65, p = 0.001) were more likely to never/sometimes wear face masks, whereas education level of postgraduate vs secondary school or below (aOR 0.38, p < 0.001), family income of ≤$23 vs >$23–125 (aOR 0.59, p = 0.008), family income of >$125 vs >$23–125 (aOR 0.70, p = 0.019), and attitude score (aOR 0.69, p < 0.001) were less likely to be associated with never/sometimes wearing face masks (Table 7).
Technique of Wearing Face Masks
The mean score for technique was 4.17 (SD = 0.97, range 0–5). Of the participants, 59% always performed hand hygiene before putting on a mask and 86% did so after removing it, 98% covered the mouth and nose, 90% adjusted masks at the bridge of the nose, and 84% securely tied masks (Table 1). All steps of face mask-wearing technique were performed by 46% (n = 468) of participants. According to bivariate analysis, factors associated with never/sometimes performing techniques of wearing face masks were age group of 18–30 years (p < 0.001), educational level of secondary school or below (p = 0.004), single marital status (p = 0.002), students (p < 0.001), history of COVID-19 infection (p = 0.009), and attitude score (p < 0.001) (Table 6). Multiple logistic regression analysis showed that never/sometimes performing techniques of face-mask wearing was more common among students (vs employed; aOR 1.68, p = 0.032) and those with a history of COVID-19 infection (aOR 1.42, p = 0.027), whereas it was less likely among age group 61+ vs 18–29 (aOR 0.39, p = 0.029), family income ≤$23 vs >$23–125 (aOR 0.65, p = 0.029), and attitude score (aOR 0.69, p < 0.001) (Table 7).
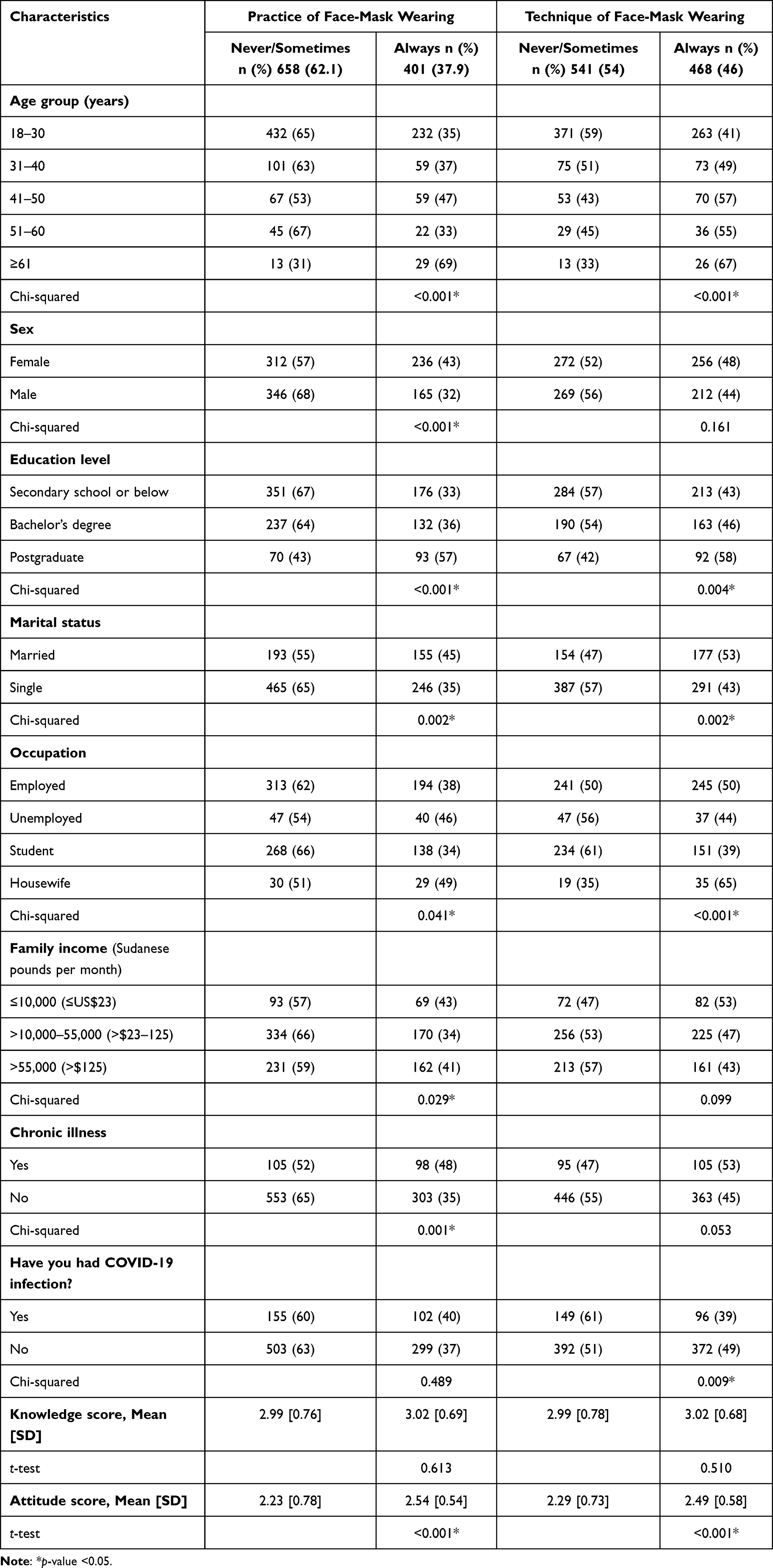 |
Table 6 Bivariate Analysis of Factors Associated with Practice and Technique of Wearing Face Masks |
 |
Table 7 Multiple Logistic Regression on Factors Associated with Never/Sometimes Practicing and Performing Techniques of Wearing Face Masks |
Concerns and Barriers to Wearing Face Masks
Of participants, 19% (n = 193) reported suffocation, 6% (n = 62) reported discomfort due to sweating inside the mask, and 6% (n = 61) held forgetfulness liable for noncompliance with face mask practices. Other reasons were cited by 20% (n = 202) of participants, including cost of face masks, obstructing/hindering verbal communication, conscious awareness of respiration, and difficulty during meals with the need to remove face masks while eating or drinking. However, 47% (n = 491) of participants did not express any concerns with wearing face masks.
Discussion
The overall mean knowledge level score was 3 (of 4 total), which indicated that most study participants had good knowledge of the route of COVID-19 transmission. This result is consistent with those of studies conducted in Sudan, Egypt, Nigeria, and Ethiopia, in which correct knowledge about route of transmission of COVID-19 was 89%, 95%, 94%, and 95%, respectively.31–34 Similarly, in Nepal, knowledge about mode of transmission was overall 95.8%, but in Malaysia, only 43.3% of participants replied correctly when asked whether the virus was airborne, and only 35.7% replied correctly when asked whether touching and eating wild animals could transmit the infection.27,35 In this study, there was an association between knowledge scores and educational level, with higher knowledge among participants with higher levels of education. This result is consistent with those of studies conducted in the general populations of Sudan, Egypt, and Nepal.27,31,32 This association most likely occurs because with a higher level of education, a person is more likely to understand print and electronic information regarding new infections such as COVID-19.36–38 Gender and age group were also associated with knowledge level, which is consistent with previous studies.27,35 Thus, to improve health literacy of both genders, as well as that of aged and illiterate populations in the country, the recommendation is to explore options such as role-play, art, and radio programs. By increasing efforts to inform the public, effects of conflicting information regarding COVID-19 infection, a problem recently termed an “infodemic”, can also be reduced.39–42
In the present study, attitudes toward COVID-19 infection and use of face masks were positive. Less than half of participants thought they were vulnerable to COVID-19 infection, and one significant predictor of positive attitude identified in the regression model was higher educational level. A relatively high level of education could directly increase awareness and therefore also the sense of being at risk of contracting COVID-19 infection. Furthermore, most participants believed that wearing masks during the current pandemic was necessary and were convinced that wearing a mask could reduce the chance of COVID-19 infection. These findings are consistent with those of studies conducted in China and Saudi Arabia, which also show a high level of positive attitude among participants.43,44 The results in this study are also consistent with those of a study conducted in Saudi Arabia in which most participants had a positive attitude toward effective control of the pandemic by compliance with wearing of face masks.28 High income was also associated with positive attitudes regarding wearing masks to reduce the chance of infection. High income likely increases the chances of having a smart television, smartphone, and advanced Internet connection, and the use of such technology ultimately increases access to health education provided through media sources.
In this study, approximately two-thirds of participants preferred to use a medical/surgical mask, whereas others used cloth masks for protection. Medical/surgical masks can reduce the outward emission rate of particles by 90% during speaking and coughing.9 Although a similar choice of masks was reported by Al Naam et al28 in Saudi Arabia, it is concerning that the use of any face mask can reduce infection exposure and risk irrespective of its type.25,28 However, the key factor that should be considered while selecting a mask is its ability to protect against exposure to droplets.45 Therefore, on the basis of this property, the N-95-type of face mask is more effective than medical masks.46 By contrast, cloth masks provide 40% to 97% protection, depending on the type of cloth and number of layers.47 Despite these differences, the primary reason most people choose medical masks is because they are disposable and widely accessible.48 The WHO recommends essential mask use for health-care workers, the general population in public places and on transportation, people living in overcrowded places, and vulnerable populations, as well as for anyone showing any symptoms suggestive of COVID-19 infection.5 In this study, more than one-third of participants always practiced wearing a face mask and more than half sometimes, which were lower rates than those in studies from different regions of Hong Kong,49 Saudi Arabia,28 Malaysia,35 and Iran.50 However, differences in the type of questions about the practice of face mask use should be considered.
In this study, most participants properly covered the nose and mouth and adjusted masks at the bridge of the nose for better fit, which are important recommendations for effective use of face masks, and also tied masks securely to minimize any gaps between face and mask. The rates in this study are higher than those in a study conducted in Nepal.27 Particles escape from a mask either by direct penetration through the mask or by leakage from its sides, and both pathways are critical factors affecting mask protection efficacy.7,8,27 Medical masks that fit well to the head can significantly improve control of particle escape.36 Fit can be improved by improved mask design, adjustment at the bridge of the nose, and adhesive tape or fluffed polypropylene fibers.4,5,9 According to the WHO, masks are only effective when coupled with hand hygiene and also with knowledge of proper mask use and disposal.5 In this study, many participants washed their hands after removing a face mask. This result is similar to that in a previous study on knowledge and practices regarding face mask use among the general population.27 Multiple regression analysis revealed a significant association between technique of face-mask wearing and employment status and no history of COVID-19 infection. The association with employment was perhaps due to the perceived high risk of exposure to SARS-CoV-2 of participants within a work environment.51 In addition, those with a previous COVID-19 infection might have felt they were protected by natural immunity after infection.52 In this study, there was a positive correlation between practice and attitude scores, which suggested that a positive attitude can lead to better compliance with techniques of wearing a face mask.28
Some of the challenges associated with consistent use of face masks were also identified in the current study. Suffocation was the major concern of participants, whereas other reasons for not wearing a mask included sweating and forgetfulness. These results are supported by those of a Brazilian study that also identified suffocation as the most cited reason for discomfort caused by face masks.53 Medical masks easily become damp, and sweating is primarily linked with cloth masks because they retain moisture and are reused.54–56 However, discomfort is not the sole determinant of face mask compliance, and social factors are also important. One study found that when more mask-wearing practices are displayed by social groups in a society, the discomfort felt by its residents decreases.57 Therefore, the solution to compliance lies in social acceptance of mask wearing as a new norm and in promotion of its adherence by health authorities.
There were some limitations in the current study. A web-based survey and nonprobability sampling technique were used, which may not be sufficiently accurate to represent the study population. Thus, the study most likely did not include the illiterate, the elderly, those without smartphones, and those with limited Internet access, which might lead to results that were overestimates because of better awareness and practices among the study participants. Another limitation was that the data were self-reported and therefore could have been affected by social desirability bias. Thus, the possibility that participants responded positively to attitude and practice questions on the basis of perceived expectations could not be excluded.
Conclusion
Although knowledge and attitude were relatively good, practice and technique of wearing face masks among Sudanese participants were low. Therefore, to ensure optimal levels of face mask use and proper techniques of wearing a face mask, increasing public awareness with training is highly recommended.
Ethical Approval
Ethical approval was received from the Ethics Committee at International University of Africa at Sudan (reference no. FMEC/21/2). All procedures performed in the study were in accordance with the ethical standards of institutional and national research committees and with the 1964 Helsinki Declaration and its later amendments. Informed consent was obtained from each participant before participating in the study.
Acknowledgments
The researchers would like to thank the Deanship of Scientific Research, Qassim University, for funding the publication of this project.
Author contributions
OW conceived and designed the survey. IA performed the investigation and revised the paper. OW and RK analyzed the data and wrote the original paper. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Greenhalgh T, Schmid MB, Czypionka T, Bassler D, Gruer L. Face masks for the public during the covid-19 crisis. BMJ. 2020;369:m1435. doi:10.1136/bmj.m1435
2. Feng S, Shen C, Xia N, Song W, Fan M, Cowling BJ. Rational use of face masks in the COVID-19 pandemic. Lancet Respir Med. 2020;8(5):434–436. doi:10.1016/S2213-2600(20)30134-X
3. Furukawa NW, Brooks JT, Sobel J. Evidence supporting transmission of severe acute respiratory syndrome coronavirus 2 while presymptomatic or asymptomatic. Emerg Infect Dis. 2020;26:7. doi:10.3201/eid2607.201595
4. Centers for Disease Control and Prevention. Considerations for wearing masks: help slow the spread of COVID-19 2020; 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/cloth-face-cover-guidance.html.
5. World Health Organization. Coronavirus disease (COVID-19) advice for the public: when and how to use masks 2020; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks.
6. Lindsley WG, Blachere FM, Law BF, Beezhold DH, Noti JD. Efficacy of face masks, neck gaiters and face shields for reducing the expulsion of simulated cough-generated aerosols. Aerosol Sci Technol. 2021;55:449–457. doi:10.1080/02786826.2020.1862409
7. Ueki H, Furusawa Y, Iwatsuki-Horimoto K, et al. Effectiveness of face masks in preventing airborne transmission of SARS-CoV-2. mSphere. 2020;5(5):e00637–20. doi:10.1128/mSphere.00637-20
8. Centers for Disease Control and Prevention. The National Institute for Occupational Safety and Health (NIOSH); 2020. Available from: https://www.cdc.gov/niosh/index.htm.
9. Asadi S, Cappa CD, Barreda S, et al. Efficacy of masks and face coverings in controlling outward aerosol particle emission from expiratory activities. Sci Rep. 2020;10:15665. doi:10.1038/s41598-020-72798-7
10. Li Y, Liang M, Gao L, et al. Face masks to prevent transmission of COVID-19: a systematic review and meta-analysis. Am J Infect Control. 2021;49(7):900–906. doi:10.1016/j.ajic.2020.12.007
11. Liang M, Gao L, Cheng C, et al. Efficacy of face mask in preventing respiratory virus transmission: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;36:101751. doi:10.1016/j.tmaid.2020.101751
12. Payne DC, Smith-Jeffcoat SE, Nowak G, et al.; CDC COVID-19 Surge Laboratory Group. SARS-CoV-2 infections and serologic responses from a sample of U.S. Navy service members: USS Theodore Roosevelt, April 2020. MMWR Morb Mortal Wkly Rep. 2020;69(23):714–721. doi:10.15585/mmwr.mm6923e4
13. Chu DK, Akl EA, Duda S, et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet. 2020;395(10242):1973–1987. pmid: 32497510. doi:10.1016/S0140-6736(20)31142-9
14. Howard J, Huang A, Li Z, et al. An evidence review of face masks against COVID-19. Proc Natl Acad Sci. 2021;118(4). pmid: 33431650. doi:10.1073/pnas.2014564118
15. Brauner JM, Mindermann S, Sharma M, et al. Inferring the effectiveness of government interventions against COVID-19. Science. 2021;371(6531). pmid: 33323424. doi:10.1126/science.abd9338
16. Leffler CT, Ing E, Lykins JD, Hogan MC, McKeown CA, Grzybowski A. Association of country-wide coronavirus mortality with demographics, testing, lockdowns, and public wearing of masks. Am J Trop Med Hyg. 2020;103:2400–2411. pmid: 33124541. doi:10.4269/ajtmh.20-1015
17. Wang Y, Tian H, Zhang L, et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Glob Health. 2020;5(5):e002794. pmid: 32467353. doi:10.1136/bmjgh-2020-002794
18. Zhang R, Li Y, Zhang AL, Wang Y, Molina MJ. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc Natl Acad Sci. 2020;117(26):14857–14863. pmid: 32527856. doi:10.1073/pnas.2009637117
19. Mukhtar MM, Khogali M. The accelerating COVID-19 epidemic in Sudan. Nat Immunol. 2021;22:797–798. doi:10.1038/s41590-021-00950-0
20. WHO (COVID-19). Sudan: WHO coronavirus disease (COVID-19) dashboard. Available from: https://covid19.who.int/region/emro/country/sd.
21. Ahmed A, Mohamed NS, El-Sadig SM, et al. Covid-19 in Sudan. J Infect Dev Ctries. 2021;15:204–208. doi:10.3855/jidc.14520
22. Ministry of Health, South Sudan. Update on COVID-19 response; 2020. Available from: https://moh.gov.ss/daily_updates.php.
23. Barasheed O, Alfelali M, Mushta S, et al. Uptake and effectiveness of facemask against respiratory infections at mass gatherings: a systematic review. Int J Infect Dis. 2016;47:105–111. doi:10.1016/j.ijid.2016.03.023
24. Chan KH, Yuen K-Y. COVID-19 epidemic: disentangling the re-emerging controversy about medical facemasks from an epidemiological perspective. Int J Epidemiol. 2020;49(4):1063–1066. doi:10.1093/ije/dyaa044
25. Sande VM, Teunis P, Sabel R. Professional and home-made face masks reduce exposure to respiratory infections among the general population. PLoS One. 2008;3(7):e2618. doi:10.1371/journal.pone.0002618
26. World Health Organization. Advice on the use of masks in the context of COVID-19: interim guidance; 2020. Available from: https://apps.who.int/iris/handle/10665/331693.
27. Alam K, Palaian S, Shankar PR, Jha N. General public’s knowledge and practices on face mask use during the COVID-19 pandemic: a cross-sectional exploratory survey from Dharan, Nepal [version 1; peer review: awaiting peer review]. F1000Res. 2021;10:376. doi:10.12688/f1000research.52661.1
28. Al Naam YA, Elsafi SH, Alkharraz ZS, Alfahad OA, Al-Jubran KM, Al Zahrani EM. Community practice of using face masks for the prevention of COVID-19 in Saudi Arabia. PLoS One. 2021;16(2):e0247313. doi:10.1371/journal.pone.0247313
29. Tang CS, Wong CY. Factors influencing the wearing of facemasks to prevent the severe acute respiratory syndrome among adult Chinese in Hong Kong. Prev Med. 2004;39(6):1187–1193. doi:10.1016/j.ypmed.2004.04.032
30. Average Salary in Sudan; 2021. Available from: http://www.salaryexplorer.com/salary-survey.php?loc=205&loctype=1.
31. Mohamed AAO, Elhassan EAM, Mohamed AO, et al. Knowledge, attitude and practice of the Sudanese people towards COVID-19: an online survey. BMC Public Health. 2021;21(1):274. doi:10.1186/s12889-021-10319-5
32. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;45(5):881–890. doi:10.1007/s10900-020-00827-7
33. Olapegba P, Ayandele O, Kolawole S, et al. A preliminary assessment of novel coronavirus (COVID-19) knowledge and perceptions in Nigeria. Soc Sci Humanit Open. 2020. doi:10.2139/ssrn.3584408
34. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma University medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
35. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
36. Li T, Liu Y, Li M, Qian X, Dai SY. Mask or no mask for COVID-19: a public health and market study. PLoS One. 2020;15(8):e0237691. doi:10.1371/journal.pone.0237691
37. Ting DSW, Carin L, Dzau V, Wong TY. Digital technology and COVID-19. Nat Med. 2020;26(4):459–461. doi:10.1038/s41591-020-0824-5
38. Chan AKM, Nickson CP, Rudolph JW, Lee A, Joynt GM. Social media for rapid knowledge dissemination: early experience from the COVID-19 pandemic. Anaesthesia. 2020;75(12):1579–1582. doi:10.1111/anae.15057
39. Zarocostas J. How to fight an infodemic. Lancet. 2020;395:676. doi:10.1016/S0140-6736(20)30461-X
40. United Nations. UN radio spreads covid-19 information to remote areas. Available from: https://www.un.org/en/un-coronavirus-communications-team/un-radio-broadcasts-spread-covid-19-information-remote-areas.
41. Press Trust of India. Tribal women perform street play on covid-19 to spread awareness among tea garden workers. Available from: https://www.hindustantimes.com/it-s-viral/tribal-women-perform-street-play-on-covid-19-to-spread-awareness-among-tea-garden-workers/story-8AIQBVP0Kn17iUEYmR7eyO.html.
42. Mukami M. Somali artists use art to spread COVID-19 awareness. Artists in Horn of Africa country fight misinformation, rumors and stigma surrounding coronavirus pandemic. Anadolu Agency; 2020. Available from: https://www.aa.com.tr/en/africa/somali-artists-use-art-to-spread-covid-19-awareness/1890554.
43. Zhong B, Luo W, Li H, et al. Knowledge, attitudes and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16:1745–1752. doi:10.7150/ijbs.45221
44. Meo SA, Alqahtani SA, Aljedaie GM, Binmeather FS, AlRasheed RA, Albarrak RM. Face masks use and its role in restraining the spread of COVID-19 pandemic in Saudi Arabia: knowledge, attitude, and practices based cross-sectional study. Front Public Health. 2022;9:818520. doi:10.3389/fpubh.2021.818520
45. Li Y, Guo YP, Wong KC, Chung WY, Gohel MD, Leung HM. Transmission of communicable respiratory infections and facemasks. J Multidiscip Healthc. 2008;1:17–27. doi:10.2147/JMDH.S3019
46. Kim M-N. What type of face mask is appropriate for everyone-mask-wearing policy amidst COVID-19 pandemic? J Korean Med Sci. 2020;35:e186. doi:10.3346/jkms.2020.35.e186
47. Bae S, Kim MC, Kim JY, et al. Effectiveness of surgical and cotton masks in blocking SARS-CoV-2: a controlled comparison in 4 patients. Ann Intern Med. 2020;173:W22–W23. doi:10.7326/M20-1342
48. Martinelli L, Kopilaš V, Vidmar M, et al. Face masks during the COVID-19 pandemic: a simple protection tool with many meanings. Front Public Health. 2021;8:606635. doi:10.3389/fpubh.2020.606635
49. Cheng VC, Wong SC, Chuang VW, et al. The role of community-wide wearing of face mask for control of coronavirus disease 2019 (COVID-19) epidemic due to SARS-CoV-2. J Infect. 2020;8:107–114. doi:10.1016/j.jinf.2020.04.024
50. Rahimi Z, Shirali GA, Araban M, Mohammadi MJ, Cheraghian B. Mask use among pedestrians during the covid-19 pandemic in Southwest Iran: an observational study on 10,440 people. BMC Public Health. 2021;21(1):133. doi:10.1186/s12889-020-10152-2
51. Falco A, Girardi D, Dal Corso L, Yıldırım M, Converso D. The perceived risk of being infected at work: an application of the job demands–resources model to workplace safety during the COVID-19 outbreak. PLoS One. 2021;16(9):e0257197. doi:10.1371/journal.pone.0257197
52. Kirkcaldy RD, King BA, Brooks JT. COVID-19 and postinfection immunity: limited evidence, many remaining questions. JAMA. 2020;323(22):2245–2246. doi:10.1001/jama.2020.7869
53. Cotrin P, Bahls AC, Da Silva DO, et al. The use of facemasks during the COVID-19 pandemic by the Brazilian population. J Multidiscip Healthc. 2020;13:1169–1178. doi:10.2147/JMDH.S281524
54. MacIntyre CR, Seale H, Dung TC, et al. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open. 2015;5(4):e006577. doi:10.1136/bmjopen-2014-006577
55. Offeddu V, Yung C-F, Low MSF, et al. Effectiveness of masks and respirators against respiratory infections in healthcare workers: a systematic review and meta-analysis. Clin Infect Dis. 2017;65:1934–1942. doi:10.1093/cid/cix681
56. Seto WH, Tsang D, Yung RWH, et al. Effectiveness of precautions against droplets and contact in prevention of nosocomial transmission of severe acute respiratory syndrome (SARS). Lancet. 2003;361:1519–1520. doi:10.1016/s0140-6736(03)13168-6
57. Schunemann HJ, Akl EA, Chou R, et al. Use of facemasks during the COVID-19 pandemic. Lancet Respir Med. 2020;8(10):954–955. doi:10.1016/S2213-2600(20)30352-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.