Back to Journals » Clinical Ophthalmology » Volume 17
Face and Content Validity of an Artificial Eye Model for Secondary Intraocular Lens Fixation via Yamane Technique
Authors Huang JJ, Waldner D, Huang JJ, Huang JM, Huang P, Teichman JC, Darvish-Zargar M, Gooi P
Received 1 May 2023
Accepted for publication 10 July 2023
Published 21 July 2023 Volume 2023:17 Pages 2063—2069
DOI https://doi.org/10.2147/OPTH.S419464
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jordan J Huang,1 Derek Waldner,1,2 Jaxon J Huang,3 Joshua M Huang,1 Paul Huang,1,2 Joshua C Teichman,4,5 Mahshad Darvish-Zargar,6 Patrick Gooi2
1Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada; 2Division of Ophthalmology, University of Calgary, Calgary, Alberta, Canada; 3John A. Burns School of Medicine, University of Hawaii, Honolulu, HI, USA; 4Department of Ophthalmology and Vision Sciences, University of Toronto, Toronto, Ontario, Canada; 5Division of Ophthalmology, Trillium Health Partners, Mississauga, Ontario, Canada; 6Division of Ophthalmology, McGill University, Montreal, Quebec, Canada
Correspondence: Jordan J Huang, Cumming School of Medicine, University of Calgary, 3330 Hospital Dr NW, Calgary, AB, T2N 4N1, Canada, Tel +1 403 991 8897, Email [email protected]
Purpose: To assess the face and content validity of an artificial eye model for secondary intraocular lens (IOL) fixation via the Yamane technique.
Methods: Ophthalmologists and residents participated in a 90-minute simulation session on secondary IOL fixation via the Yamane technique. Hands-on practice of this technique was performed on an artificial eye, the Bioniko Okulo BR8. After, all ophthalmologists answered an 18-question survey assessing the face and content validity of the model. Survey responses were recorded on a 5-point double-headed Likert scale, ranging from strongly agree (1)-to-strongly disagree (5) (Figure 1).
Results: Twenty-three surveys were completed. Respondents rated the survey with a median response of 1 (strongly agree)-to-3 (neutral). Highest ratings for the model were received for “usefulness for training residents”, and “easier to set up and clean-up compared to a cadaver”. Lowest ratings were received for realism of the model compared to cadaveric eyes. Statistical analysis revealed no significant difference among identified groups. Ratings for face and content validity were viewed favorably, both with an overall median response of 2.00 (agree).
Conclusion: The Bioniko Okulo BR8 shows promise as a valid tool for practicing secondary IOL fixation via the Yamane technique. Considering recent guidelines in competency-based ophthalmology education programs, this model may be a valuable tool over traditional techniques for teaching and improving surgical skill amongst trainees.
Keywords: training, cataracts, Bioniko, Okulo, model
Introduction
Techniques used to date for secondary IOL fixation with lack of capsular support include placement of the IOL in the anterior chamber, suture or clip fixation to the iris, suture fixation to the sclera using traditional or flanged methods, or intrascleral haptic fixation.1–4 These are technically challenging procedures to perform and are associated with post-operative complications such as glaucoma, corneal endothelial cell loss, wound leak, hyphema, lens tilt/dislocation, cystoid macular edema, and peripheral anterior synechiae.1–4 Scleral fixation via suturing also carries the risk of the same complications as listed above as well as risk of suture knot erosion and breakage.5,6
Over the last two decades, sutureless intrascleral fixation (SFIOL) has risen in popularity amongst ophthalmologists.7,8 In general, SFIOL techniques involve the fixation of the IOL haptics within the sclera without the use of sutures.8 For the beginner trainee, mastering these technically challenging procedures can be difficult, as typically the IOL haptics need to be housed in scleral tunnels or flaps. Torsion of the haptics, scleral erosion, or IOL dislocation are common problems involved in SFIOL.7–9 In 2007, Gabor et al demonstrated a technique for sutureless fixation of the posterior chamber lens via two straight sclerotomies ab externo using a 24-gauge cannula parallel to the limbus to create a scleral tunnel.9 Each haptic arms/tails of a standard 3-piece IOL is then pulled through the sclerotomy and left externalized. Forceps are then used to grasp each externalized tip and pull the IOL haptic into the scleral tunnel. Challenges associated with the Gabor technique included difficulties in grasping the haptics for subsequent placement into the scleral tunnels, as well as problems around achieving sufficient haptic fixation power, and postoperative IOL dislocation.7–9
Subsequently, new, revised techniques have been developed to target these problems. The Yamane technique (flanged intrascleral IOL fixation with double-needle technique) has become increasingly popular.10 Developed in 2014 by Yamane et al, the Yamane technique is a SFIOL technique that involves the firm fixation of the haptics of an IOL to the sclera via creation of a flange at the end of the IOL haptic.10 To achieve this, the ends of the haptics are cauterized using an ophthalmic cautery device, creating a flange of ~0.3mm. The advantage of this method is that it allows for better fixation of the haptics in the scleral tunnels.
As a beginner trainee, common difficulties in mastering the Yamane technique include performance of an angled sclerotomy, introduction of the leading haptic into the lumen of a 30-gauge needle, and externalization of the haptics.11–15 As such, it is important for ophthalmologists and trainees to learn and continually refine their skills on model eyes prior to performance on patients.
Traditional methods to practice and enhance surgical skills without causing patient harm include use of cadaveric eyes.16 Advantages of cadavers include accurate ocular anatomy and realistic experience of tool–tissue interaction forces. However, concerns have been raised regarding the ethics associated with their use, high costs to obtain, biohazard risks upon disposal, and limits in both quantity available and timing of when they must be used by (preservation and storage).16 As a result, artificial eye models have risen in popularity as training tools for ophthalmologists and residents.17–20 This study analyzes the feasibility of an artificial eye model, the Bioniko Okulo BR8 as an alternative training tool to cadaveric specimens for secondary IOL fixation via Yamane technique. Valued at $200 USD, the Bioniko Okulo BR8 is designed for simulation of cataract surgery and its associated complications. The model features a clear cornea, flexible pigmented iris and angle, flexible sclera, and a variety of lens options that permit practice of cataract surgery in different contexts. The ability to remove the capsule from the model permits surgical practice of secondary IOL insertion and management of weak zonules. Importantly, unlike a cadaveric specimen, the models are reusable (up to a certain number of replications), affordable, realistic, easy to use, and disposable without biohazard concerns. Despite these potential benefits, no validation of this model has been reported in the literature to date. Thus, the purpose of this study was to assess the face and content validity of the Bioniko Okulo BR8 model for secondary IOL fixation via Yamane technique.
Methods
Ethics was approved by the University of Calgary Research Ethics Board. The tenets of the Declaration of Helsinki were followed. Verbal consent was obtained from participants and approved by the ethics committee.
Ophthalmologists and residents of varied surgical experience were surveyed following a 90-minute skills transfer course on secondary IOL fixation via Yamane Technique at the 2021 Canadian Ophthalmological Society Annual Meeting in Halifax, Nova Scotia, Canada. An 18-question survey was designed to assess the face and content validity of the Bioniko Okulo BR8 (Table 1) (Figure 2). Adapted from McDougall, face validity was defined as a subjective assessment of the realism of the Bioniko Okulo BR8 model compared to a human eye.21 Content validity was defined as the suitability of the model for teaching purposes.21 A video presentation by a trained ophthalmologist on secondary IOL fixation via Yamane Technique was shown to the participants prior to beginning the skills course. The surgical steps involved in the Yamane technique were explained and demonstrated. Participants then engaged in hands-on practice of secondary IOL fixation via Yamane Technique on the Bioniko Okulo BR8 model. Two participants were seated per table, each with a Bioniko Okulo BR8 model, a complete set of surgical instrumentation, and a conventional surgical microscope. During the hands-on session, instructors circulated the room and provided guidance to participants. Following completion of surgery on the models, both instructors and participants completed the survey prior to the conclusion of the session. Survey responses were collected on a 5-point Likert scale, ranging from strongly agree (1) to strongly disagree (5). Respondents also self-reported their past year and lifetime experience performing secondary IOL fixation via Yamane Technique. Further, participants and instructors were provided the opportunity to provide comments on their experience using the Bioniko Okulo BR8 model. We compared survey responses from instructors (n=6) vs participants (n=17), as well as for expertise performing the Yamane technique (n=6) vs non-experts (n=17), We defined expertise in secondary IOL fixation via Yamane Technique as having performed over >20 lifetime cases. Statistical analysis was not performed given the low sample size. Graph generation was performed using GraphPad Prism 8.2.0. There were no financial incentives provided to participants for completing the survey.
 |
Table 1 18-Question Survey Designed to Assess the Face and Content Validity of the Bioniko Okulo BR8 Model |
Results
A total of 23 ophthalmologists completed the survey. Survey respondents comprised 17 participants and 6 instructors. Six respondents had no prior experience performing the Yamane technique for secondary IOL fixation in a live patient prior to the course and survey. Two patients had significant prior experience, performing >60 lifetime procedures in live patients. The self-reported experience performing secondary IOL fixation via Yamane technique of the respondents in the past year and lifetime is shown in Table 2 and Table 3.
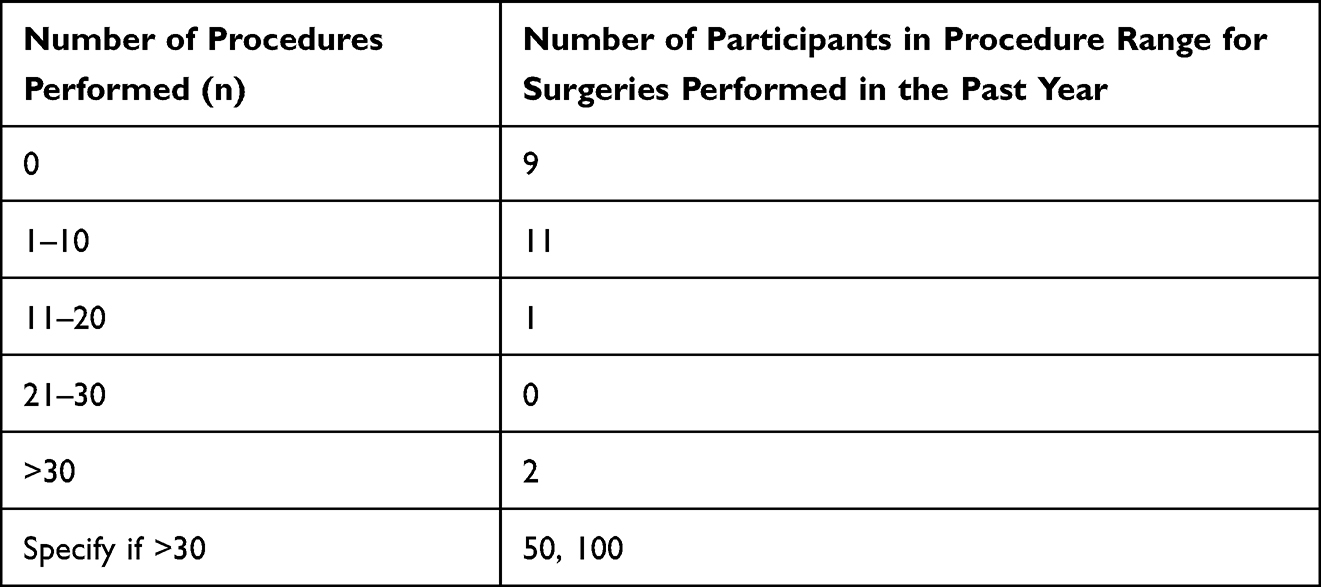 |
Table 2 Respondent’s Self-Reported Experience Over the Last Year Performing Secondary IOL Fixation via Yamane Technique Procedures on Live Patients Prior to the Training Course |
 |
Table 3 Respondent’s Self-Reported Lifetime Experience Performing Secondary IOL Fixation via Yamane Technique Procedures on Live Patients Prior to the Training Course |
Respondents rated the survey with a median response of 1 (strongly agree) to 3 (neutral), with highest ratings for the model received for the topics of usefulness for training residents, and easier to set up and clean-up compared to a cadaver (Figure 1). Lowest ratings were received for how realistic the model was compared to cadaveric eyes. Ratings for face validity (survey questions 1–3, 17 in Table 1) were viewed favorably, with an overall median response of 2.00 (agree) (Figure 1). In this category, survey question 2 (anatomically accurate) was rated the highest. Content validity, (survey questions 4–7, 11–15 in Table 1) was also viewed positively, with a median response of 2.00 (agree).
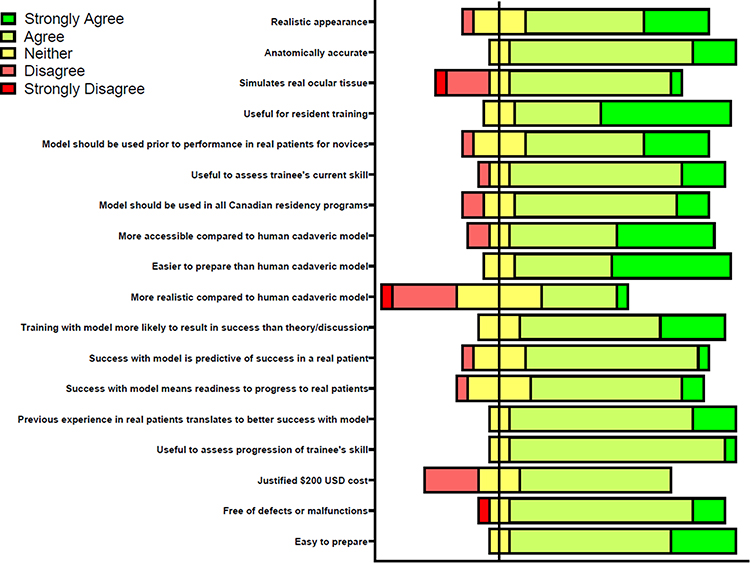 |
Figure 1 Diverging stacked bar chart displaying Likert responses to survey questions regarding the Alcon Bioniko Okulo BR8 Cataract surgery intraocular lens model at the 2021 Canadian Ophthalmological Society Annual Meeting in Halifax, Nova Scotia, Canada, after a 90-minute training session on secondary IOL fixation via the Yamane technique. |
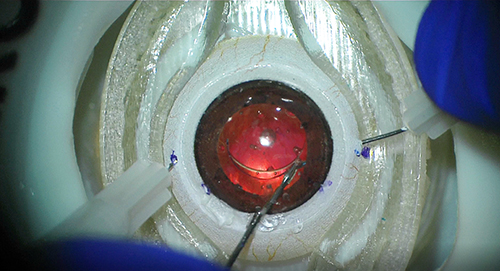 |
Figure 2 The Bioniko Okulo BR8 for secondary intraocular lens fixation via the Yamane technique. |
Discussion
Secondary IOL fixation via the Yamane technique is a technically challenging surgical procedure to master. The development of low-cost, re-usable hands-on training tools may aid in resident acquisition of surgical skills and performance on live patients. Survey results revealed that the Bioniko Okulo BR8 model performed favorably across all items assessed. Survey questions involving content validity (usefulness in training residents) were rated the highest, highlighting this model’s potential for use as a surgical training tool. Positive implications of transitioning to use of artificial eye models over traditional cadaveric eyes include increased availability and resources to practice surgery, elimination of biohazardous risks associated with cadaveric eyes (preservation, storage and disposal), and lower financial burden.22–28 Survey responses regarding face validity (realism of the model) were also rated favorably. Anatomical accuracy and the realistic simulation of ocular tissue are critical components of a model. Questions not related to face and content validity (survey questions 8–10, 16–18), were also viewed favorably, and primarily consisted of the ease of set-up, ease of use, and accessibility/costs of the model. Although statistical analysis could not be performed, median responses from both instructors vs participants, and experts vs non-experts answered the survey questions in favor of the Bioniko Okulo BR8 model. As can be expected, the realism of the model compared to a cadaveric eye was rated the lowest. A missing feature of the model that may contribute to this rating include the lack of conjunctival blood vessels. Written comments provided by respondents were mainly positive and related to the ease of set-up, storage, and value as a training tool for practicing secondary IOL fixation via the Yamane Technique. Negative feedback was received from respondents relating to the costs of the model, and that the artificial shell around the eye that simulates the orbit gets in the way of surgery. It should be noted that although the Bioniko Okulo BR8 model costs $200 USD, the cost of a human cadaveric eye is ~$500 USD per globe.22
One limitation of this study is its small sample size (n=23). Due to the ongoing COVID restrictions at the time of the study, the number of participants permitted during the skills transfer course at the 2021 Canadian Ophthalmological Society Conference was limited. As a result, statistical analysis could not be performed. Additionally, other modalities of surgical training were not investigated and compared during the skills transfer course to the Bioniko Okulo BR8, such as use of surgical simulators as well as cadaveric specimen. Future studies with larger sample sizes focusing on the comparison of multiple training modalities for learning secondary IOL fixation via the Yamane technique may provide additional insights on which modalities would be best for use in ophthalmology residency training programs.
Conclusion
Overall, the Bioniko Okulo BR8 model was favored positively among ophthalmologists and residents of all levels of experience for the performance of secondary IOL fixation via the Yamane Technique. Validating these models via resident and ophthalmologist feedback is of the utmost importance to assess the suitability of these models for training. This study confirms the face and content validity of the Bioniko Okulo BR8 model as a tool for training residents on secondary IOL fixation via the Yamane technique.
Abbreviations
IOL, intraocular lens; ACGME, Accreditation Council for Graduate Medical Education.
Disclosure
PG is a consultant for Alcon, AbbVie, Bausch and Lomb, Glaukos, Santen, Labtician. PG also has a patent on a glaucoma device that is not commercialized. JTC is a consultant/advisor for Aequus, Alcon, Allergan, Bausch and Lomb, Labtician-Théa, Novartis, Santen, Shire, Sun Pharma. MDZ is a consultant/advisor for Alcon, Allergan, Avir Pharma, Johnson & Johnson, Labtician, Sun Pharma. The authors report no other conflicts of interest in this work.
References
1. Vounotrypidis E, Schuster I, Mackert MJ, Kook D, Priglinger S, Wolf A. Secondary intraocular lens implantation: a large retrospective analysis. Graefes Arch Clin Exp Ophthalmol. 2019;257(1):125–134. doi:10.1007/s00417-018-4178-3
2. Hara T, Hara T. Ten-year results of anterior chamber fixation of the posterior chamber intraocular lens. Arch Ophthalmol. 2004;122(8):1112–1116. doi:10.1001/archopht.122.8.1112
3. Hennig A, Johnson GJ, Evans JR, et al. Long term clinical outcome of a randomised controlled trial of anterior chamber lenses after high volume intracapsular cataract surgery. The Br J Ophthalmol. 2001;85(1):11–17. doi:10.1136/bjo.85.1.11
4. Sawada T, Kimura W, Kimura T, et al. Long-term follow-up of primary anterior chamber intraocular lens implantation. J Cataract Refract Surg. 1998;24(11):1515–1520. doi:10.1016/S0886-3350(98)80176-4
5. Vote BJ, Tranos P, Bunce C, Charteris DG, Da Cruz L. Long- term outcome of combined pars plana vitrectomy and scleral fixated sutured posterior chamber intraocular lens implantation. Am J Ophthalmol. 2006;141(2):308–312. doi:10.1016/j.ajo.2005.09.012
6. Bading G, Hillenkamp J, Sachs HG, Gabel VP, Framme C. Long-term safety and functional outcome of combined pars plana vitrectomy and scleral-fixated sutured posterior chamber lens implantation. Am J Ophthalmol. 2007;144(3):371–377. doi:10.1016/j.ajo.2007.05.014
7. Tamburrelli C, Tamburrelli AC. Sutureless scleral fixated IOL: the “Catcher Pole” technique. Clin Ophthamol. 2021;15:121–128. doi:10.2147/OPTH.S288769
8. Colantuono D, Seknazi D, Miere A, Amoroso F, Glacet-Bernard A, Souied EH. Sutureless intrascleral fixation using a uniquely designed intraocular lens. J Fr Ophthalmol. 2021;44(7):957–961. doi:10.1016/j.jfo.2020.10.025
9. Gabor S, Pavlidis M. Sutureless intrascleral posterior chamber intraocular lens fixation. J Cataract Refract Surg. 2007;33(11):1851–1854. doi:10.1016/j.jcrs.2007.07.013
10. Yamane S, Sato S, Maruyama-Inoue M, Kadonosono K. Flanged intrascleral intraocular lens fixation with double-needle technique. Ophthalmol. 2017;124(8):1136–1142. doi:10.1016/j.ophtha.2017.03.036
11. Li X, Ni S, Li S, et al. Comparison of three intraocular lens implantation procedures for aphakic eyes with insufficient capsular support: a network meta-analysis. Am J Ophthalmol. 2018;192:10–19. doi:10.1016/j.ajo.2018.04.023
12. Yalcinbayir O, Avci R, Ucan Gunduz G, Mavi Yildiz A, Cetin Efe A, Baykara M. Comparison of two techniques in posterior lens dislocations: scleral suture fixation vs. modified Yamane intrascleral lens fixation. J Fr Ophthalmol. 2022;45(1):13–19. doi:10.1016/j.jfo.2021.09.009
13. Kelkar A, Kelkar J, Kothari A, et al. Comparison of two modified sutureless techniques of scleral fixation of intraocular lens. Ophthalmic Surg Lasers Imaging Retina. 2018;49:e129–e134.
14. Wong HM, Kam KW, Rapuano CJ, Young AL. A systematic review on three major types of scleral-fixated intraocular lens implantation. Asia Pac J Ophthalmol. 2021;10(4):388–396. doi:10.1097/APO.0000000000000369
15. Gelman RA, Garg S. Novel Yamane technique modification for haptic exposure after glued intrascleral haptic fixation. Am J Ophthalmol Case Rep. 2019;14:101–104. doi:10.1016/j.ajoc.2019.03.009
16. Yiasemidou M, Gkaragkani E, Glassman D, Biyani CS. Cadaveric simulation: a review of reviews. Ir J Med Sci. 2018;187(3):827–833. doi:10.1007/s11845-017-1704-y
17. Swift A, Gooi P. Artificial eye models: an opportunity to increase surgical training exposure in ophthalmology during and beyond the COVID-19 pandemic. J Clin Ophthalmol. 2020;4:16–18.
18. Gorner A, Waldner D, Swift A, Docherty G, Schlenker M, Gooi P. Face and content validity of a synthetic eye model for Ab-interno goniotomy and canaloplasty. Clin Res Ophthalmol. 2020;3(1):1–7.
19. Waldner D, Gorner A, Swift A, Ahmed Y, Chung H, Gooi P. Face and content validity of the SimulEYE A-Vit model for anterior vitrectomy. Can J Ophthalmol. 2020;55(5):458–460. doi:10.1016/j.jcjo.2020.04.006
20. Loewen D, Al-Ani A, Penny M, Swift A, Gorner A, Gooi P. Face and content validity of an artificial eye model for secondary IOL fixation. Arch Ophthalmol Opto. 2021;4(1):1–7. doi:10.22259/2638-5120.0401001
21. McDougall EM. Validation of surgical simulators. J Endourol. 2007;21(3):244–247. doi:10.1089/end.2007.9985
22. Human Tissue Banking in Canada: costing and economic analysis - final report. Ottawa; 2003. Available from: https://profedu.blood.ca/sites/msi/files/Human-Tissue-Banking.pdf.
23. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in ophthalmology; 2022.
24. Wentzell DD, Chung H, Hanson C, Gooi P. Competency-based medical education in ophthalmology residency training: a review. Can J Ophthalmol. 2020;55:12–19. doi:10.1016/j.jcjo.2019.07.004
25. Lee GA, Chiang MY, Shah P. Pig eye trabeculectomy – a wet lab teaching model. Eye. 2006;20:32–37. doi:10.1038/sj.eye.6701784
26. Ang JL, Collis SA, Dhillon B, Cackett P. The eye in forensic medicine: a narrative review. Asia Pac J Ophthalmol. 2021;10:486–494.
27. Kawashima W, Hatake K, Kudo R, et al. Estimating the time of death on the basis of corneal opacity. J Forensic Res. 2015;6(1):e1000269.
28. Tsunenari S, Kanda M. The post-mortem changes of corneal turbidity and its water content. Med Sci Law. 1977;17(2):108–111. doi:10.1177/002580247701700208
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.