Back to Journals » International Medical Case Reports Journal » Volume 19
Exudative Retinal Detachment During Induction Therapy for Acute Promyelocytic Leukemia: A Manifestation of Differentiation Syndrome
Authors Zheng X ![]() , Zhang X, Yu H
, Zhang X, Yu H ![]() , Zang S
, Zang S
Received 6 August 2025
Accepted for publication 30 December 2025
Published 14 January 2026 Volume 2026:19 558934
DOI https://doi.org/10.2147/IMCRJ.S558934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Xudong Zhu
Xianqi Zheng,1,2 Xiayin Zhang,1,3 Honghua Yu,1,4 Siwen Zang1,5
1Guangdong Eye Institute, Department of Ophthalmology, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Southern Medical University, Guangzhou, People’s Republic of China; 2Guangzhou Aier Eye Hospital, Jinan University, Guangzhou, People’s Republic of China; 3Singapore Eye Research Institute, Singapore National Eye Centre, Singapore; 4Guangdong Provincial Key Laboratory of Artificial Intelligence in Medical Image Analysis and Application, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, Guangzhou, People’s Republic of China; 5Department of Ophthalmology, Guangdong Provincial People’s Hospital Ganzhou Hospital (Ganzhou Municipal Hospital), Ganzhou, People’s Republic of China
Correspondence: Siwen Zang, Guangdong Provincial People’s Hospital, Guangdong Academy of Medical Sciences, No. 106, Zhongshan Second Road, Yuexiu District, Guangzhou, People’s Republic of China, Tel +86 13925198097, Email [email protected]
Background/Aim: This report describes a case of exudative retinal detachment as an ocular manifestation of differentiation syndrome (DS) during induction therapy for acute promyelocytic leukemia (APL). A concise review of the literatures is also provided.
Case Presentation: A 25-year-old female with APL received induction therapy with all-trans retinoic acid (ATRA), arsenic trioxide (ATO), and daunorubicin. On day 15 of induction therapy, she developed dyspnea with pulmonary infiltrates, alongside bilateral epiphora and blurred vision in her right eye. Ophthalmic examination revealed a best-corrected visual acuity (BCVA) of 20/40 in the right eye and 20/20 in the left. Fundus examination demonstrated macular edema, mild optic disc edema, undulating exudative retinal detachment in the posterior pole and mid-peripheral retina, and scattered superficial hemorrhages bilaterally. Optical coherence tomography demonstrated corrugated retinal pigment epithelium elevation with subretinal fluid (SRF), choroidal thickening in both eyes, and neurosensory epithelium detachment in the right macula. Fundus fluorescein angiography confirmed diffuse vascular leakage bilaterally. A diagnosis of DS was established. Management with systemic corticosteroids, ATRA dose reduction, and ATO discontinuation led to the complete resolution of SRF and restoration of BCVA to 20/20 in both eyes within one month.
Conclusion: Exudative retinal detachment can be an ocular manifestation of DS during APL induction therapy, likely attributable to systemic capillary leakage. Prompt intervention with systemic corticosteroids is effective and generally associated with a favorable visual prognosis.
Keywords: exudative retinal detachment, differentiation syndrome, acute promyelocytic leukemia, all-trans retinoic acid, arsenic trioxide
Introduction
Acute promyelocytic leukemia (APL) is a subtype of acute myelocytic leukemia, characterized by the chromosomal translocation t(15;17) coding a PML/RARα fusion protein, which arrests myeloid differentiation at the promyelocyte stage.1
Differentiating agents, specifically all-trans retinoic acid (ATRA) and arsenic trioxide (ATO), have revolutionized APL treatment.2–4 The ATRA-ATO combination is the standard of care across all risk strata, demonstrating superior efficacy and a more favorable toxicity profile compared to traditional ATRA plus chemotherapy regimens.5–7 In patients with low-to-intermediate-risk APL, ATRA-ATO regimens achieve complete remission rates approaching 100% and a 50-month overall survival rate of 99.2%.5
However, the terminal differentiation of leukemic blasts may trigger differentiation syndrome (DS), a potentially life-threatening complication typically occurring within the first 1–2 weeks of therapy.8 DS pathogenesis involves upregulated cytokines, chemokines, and adhesion molecules,9 leading to systemic inflammatory states. Clinical manifestations include dyspnea, pulmonary infiltrates, pleural/pericardial effusions, fever, hypotension, edema, acute febrile neutrophilic dermatosis and renal dysfunction.10,11
In contrast to these well-characterized systemic manifestations, ocular manifestations of DS remain rare and underrecognized. Ocular manifestations, such as retinal hemorrhages, exudative retinal detachment and papilledema, may be overlooked amid life-threatening systemic manifestations, yet they can serve as critical early indicators of DS. This report describes a case of DS-associated exudative retinal detachment and reviews the literature to emphasize its potential as an early indicator of DS in APL patients undergoing induction therapy.
Case Description
A 25-year-old female presented to the hematology department with a three-day history of unexplained fever, spontaneous skin petechiae, and menorrhagia. Physical examination revealed a body temperature of 38.3°C and scattered ecchymoses on the upper extremities. Initial laboratory tests revealed a normal white blood cell (WBC) count (6.67×109/L), thrombocytopenia (14×109/L), and anemia (red blood cell count 3.38×1012/L, hemoglobin 105 g/L). Coagulation studies were consistent with disseminated intravascular coagulation, revealing elevated D-dimer (>20,000 ng/mL), hypofibrinogenemia (0.77 g/L), prolonged prothrombin time [PT 19.4 seconds; international normalized ratio (INR) 1.64], and activated partial thromboplastin time (APTT 54 seconds). Serum biochemistry indicated hypokalemia (2.70 mmol/L), hyponatremia (134.0 mmol/L), and elevated lactate dehydrogenase (580 U/L) and α-hydroxybutyrate dehydrogenase (299 U/L) levels. Bone marrow aspirate confirmed hypercellularity with granulocytic hyperplasia (95% of nucleated cells), predominantly comprised of abnormal promyelocytes (91.5%), alongside erythroid hypoplasia. A concurrent peripheral blood smear showed that abnormal hypergranular promyelocytes accounted for 68% of the white blood cells. These findings confirmed the diagnosis of APL.
Induction therapy was initiated with oral ATRA. The dosing was adjusted from 13.3 mg/m2 once daily to 6.7 mg/m2 twice daily (total daily dose: 20 mg) on the second day of APL diagnosis. Hydroxyurea (1 g three times daily) was added for leukocytosis control, and prophylactic oral dexamethasone (10 mg daily) was administered. Supportive care included antipyretics and transfusions to maintain platelet counts above 50×109/L, fibrinogen above 150 mg/dL, and hemoglobin above 80 g/L, per standard guidelines. Intravenous daunorubicin (43 mg/m2 daily, total daily dose: 65 mg) was started on day 4 and last for 3 days, followed by intravenous ATO (5 mg/m2 daily, total daily dose: 7.5 mg) on day 13.
On day 15 of APL treatment, the patient developed acute dyspnea and chest tightness. Laboratory tests showed a WBC count of 3.15×109/L, hemoglobin of 57 g/L, and a platelet count of 28×109/L. Coagulation profile indicated a D-dimer level >6600 ng/mL, a fibrinogen level of 4.20 g/L and a PT of 13 seconds. Chest computed tomography (CT) revealed bilateral diffuse pulmonary infiltrates, supporting a diagnosis of DS. Concurrently, she reported new-onset bilateral excessive tearing and blurred vision in the right eye. Ophthalmic examination revealed a best-corrected visual acuity (BCVA) of 20/40 in the right eye and 20/20 in the left. Intraocular pressures and anterior segment examination were unremarkable. Dilated fundus examination demonstrated bilateral macular edema, mild optic disc edema, undulating exudative retinal detachment in the posterior pole and mid-peripheral retina, and scattered superficial retinal hemorrhages (Figure 1). Optical coherence tomography (OCT) showed corrugated retinal pigment epithelium (RPE) elevation with subretinal fluid (SRF) accumulation, choroidal thickening bilaterally, and neurosensory epithelium detachment in the right macula (Figure 2). Given the coincidence of exudative retinal detachment and systemic manifestations of DS, we speculated that this was exudative retinal detachment secondary to DS.
 |
Figure 1 Fundus photographs on initial assessment revealed macular edema (blue arrows), mild optic disc edema (green arrows), undulating edematous detachment in the posterior pole and mid-peripheral retina (dashed circles) accompanied by scattered superficial retinal hemorrhages (white arrows) in the right eye (A–C) and the left eye (D–F). |
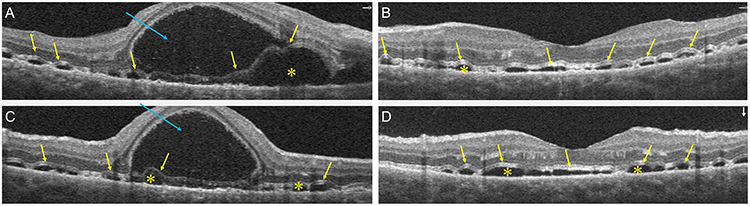 |
Figure 2 Optical coherence tomography on initial assessment demonstrated corrugated retinal pigment epithelium elevation (yellow arrows) with subretinal fluid accumulation (yellow asterisks) bilaterally (A–D) and neurosensory epithelium detachment (blue arrows) in the right macula (A and C). |
In response to these complications, ATO was discontinued, and the ATRA dose was reduced by 50% on day 15. This regimen maintained for two weeks. The dexamethasone dose was increased to 10 mg intravenously twice daily, supplemented with topical prednisolone acetate eye drops every 8 hours. Fundus fluorescein angiography (FFA) performed on day 19 revealed diffuse late-phase leakage from retinal vessels at the posterior pole and around the optic disc, with intermittent hemorrhages obscuring fluorescence bilaterally (Figure 3).
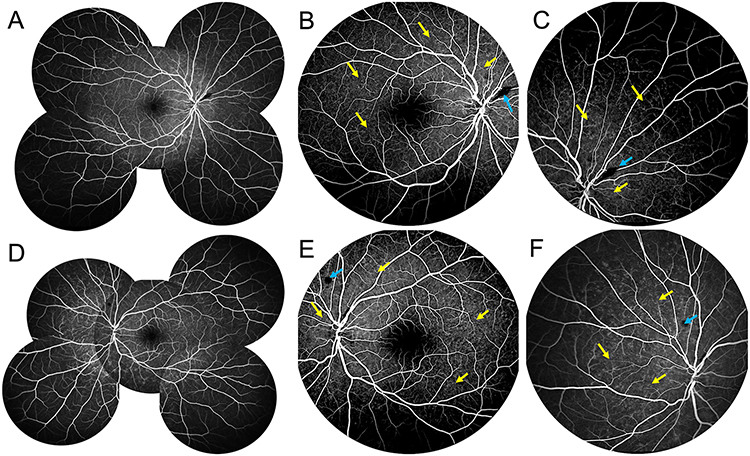 |
Figure 3 Fundus fluorescein angiography on day 19 revealed diffuse late-phase leakage from retinal vessels at the posterior pole and around optic disc (yellow arrows) with intermittent hemorrhages (blue arrows) obscuring the fluorescence in the right eye (A–C) and the left eye (D–F). |
The patient’s respiratory symptoms improved with resolution of pulmonary infiltrates on repeat chest CT over the following week. On day 24, she reported mild bilateral blurred vision and blood-tinged sputum. Significant chest tightness or shortness of breath was absent. BCVA improved to 20/30 (right eye) and 20/20 (left eye) after 11 days of DS treatment and normalized to 20/20 bilaterally after one month. Serial OCT examinations demonstrated symmetrical choroidal thickness reduction and SRF resorption in both eyes with corticosteroid administration (Figure 4).
 |
Figure 4 Optical coherence tomography demonstrated bilateral anatomical recovery during differentiation syndrome (DS) treatment. On day 4 of DS treatment, subretinal fluid (SRF) was significantly resorbed at the posterior pole, but choroidal thickness remained in the right eye (A) and the left eye (B). On day 13 of DS treatment, SRF was further resorbed at the posterior pole but remained in the fovea, choroidal thickness was reduced in the right eye (C) and the left eye (D). On day 35 of DS treatment, there was complete resolution of the SRF in the right eye (E) and the left eye (F). The red lines indicate choroidal thickness assessment while the yellow arrows indicate SRF. |
After one month of DS treatment, her systemic condition had significantly improved, with only a minor cough and expectoration remaining. Laboratory tests showed marked improvement in coagulation and hematological parameters (INR 1.05, PT 13.50 seconds, APTT 30.3 seconds, fibrinogen 2.00 g/L, hemoglobin 83 g/L, platelets 380×109/L, WBC 3.57×109/L). She was discharged on a tapering course of oral dexamethasone (2.25 mg once daily for 7 days) and ongoing topical prednisolone acetate. At the 35-day follow-up, fundus examination and OCT confirmed complete resolution of SRF, retinal hemorrhages, retinal detachment and edema, with restoration of normal retinal architecture in both eyes (Figure 5).
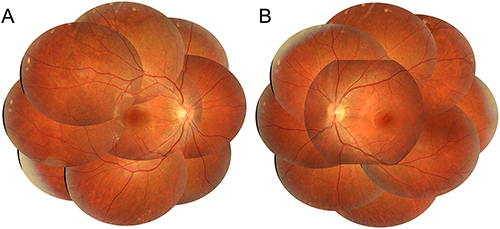 |
Figure 5 Fundus photographs at the 35-day follow-up revealed complete remission of retinal edema, retinal detachment, retinal hemorrhage, papilledema and macular edema in the right eye (A) and the left eye (B). |
Discussion
DS is a well-established complication of induction therapy for APL. While systemic manifestations of DS like fever and respiratory distress are common, ocular involvement remains rare but increasingly recognized. This case underscores exudative retinal detachment as a potential early indicator of DS.
A review of the literature reveals 9 reported cases of DS-associated retinal manifestations, involving 5 females and 4 males, with ages ranging from 25 to 66 years. All cases showed bilateral eye involvement. Ocular symptoms occurred 5 to 20 days after induction therapy initiation (median: 14 days), coinciding with the typical onset of systemic DS. 5 cases received DS prophylaxis through corticosteroids while others did not. Ocular manifestations included blurred vision (9/9), epiphora (1/9), phosphenes (1/9), yellowing of vision (1/9), visual dimness (1/9), increased intraocular pressure (1/9), and anterior chamber angle closure (1/9). Visual acuity ranged from mild impairment (20/25) to severe loss (finger count/3 ft). Fundus manifestations included retinal hemorrhages (7/9), exudative retinal detachment (3/9), macular edema (3/9) and optic disc edema (2/9). Typical signs of leukemic retinopathy, such as Roth spots (1/9), cotton wool spots (1/9), and chorioretinal lesions (3/9), may occur before or alongside ophthalmic DS. OCT demonstrated SRF accumulation (7/9), RPE elevation (5/9) and choroidal thickening (3/9), while FFA predominantly showed vascular leakage (6/9). The anterior segment was universally unaffected. Ocular manifestations typically coincided with systemic manifestations but could also follow 1–3 days later. In one case, ocular symptom was the first manifestations of DS.1
Management primarily involved systemic corticosteroids (8/9), induction therapy adjustment (6/9) and topical corticosteroids (2/9). All patients exhibited significant visual improvement and anatomical recovery within one month. Most patients (7/9) achieved favorable visual outcomes. A summary of these cases is provided in Table 1.
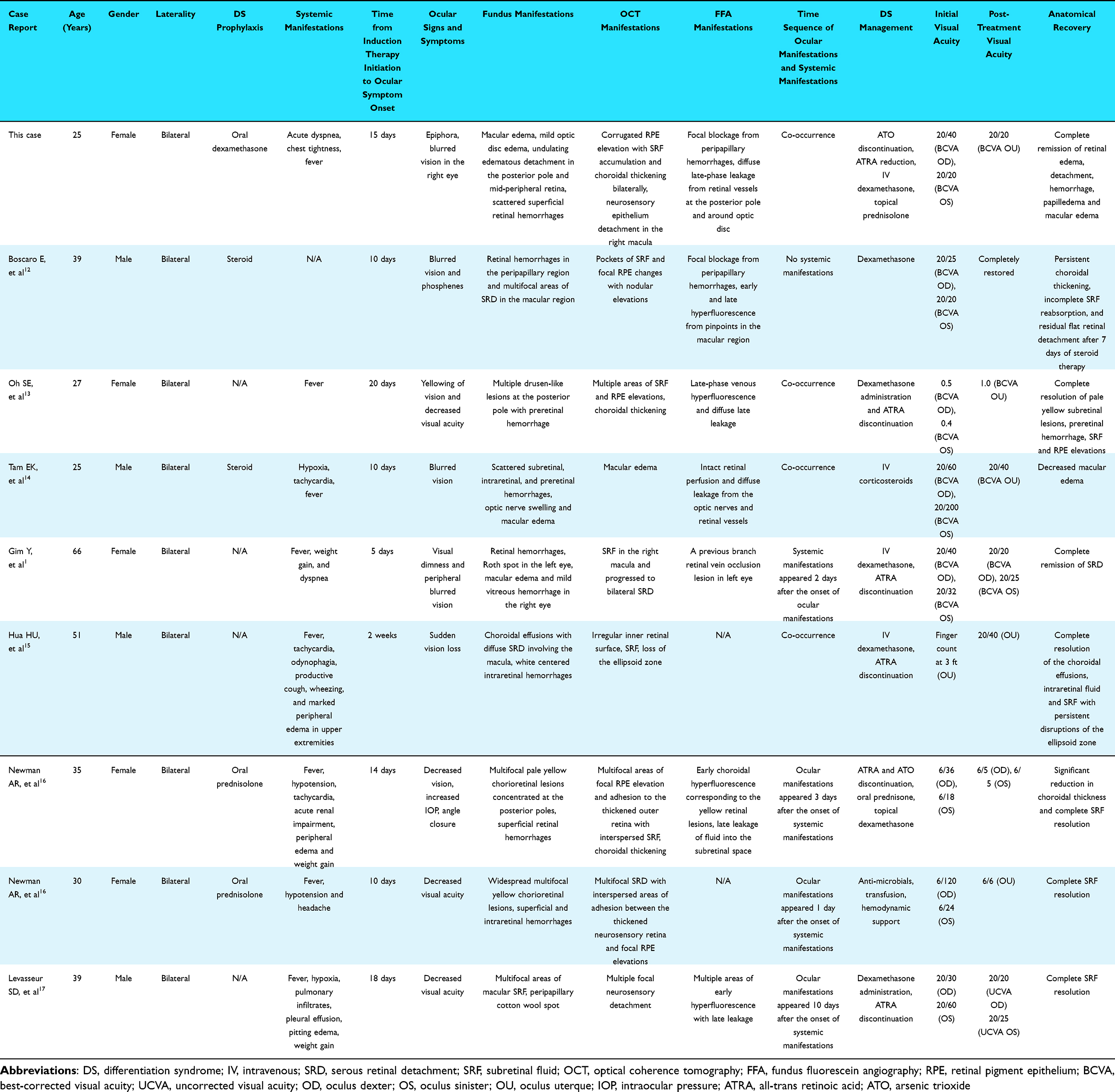 |
Table 1 Summary of Reported Cases with Retinal Manifestations in Differentiation Syndrome |
The pathogenesis of DS is driven by a hyperinflammatory state from differentiating leukemic cells and enhanced cytokine production, leading to endothelial injury and systemic capillary leakage.10 This hyperinflammatory state typically manifests as fever, tachycardia, tachypnea, and hypotension, potentially progressing to shock if untreated.16 The ocular manifestations including papilledema, retinal edema, and exudative retinal detachment, are the direct consequence of ocular microvasculature disturbance.17 Blood-retinal barrier (BRB) is crucial for maintaining retinal homeostasis by controlling fluid and molecular movement.18 Hypoxia–ischemia secondary to leukemic infiltration and microvascular occlusion may disrupt the integrity of the BRB, which leads to SRF accumulation and exudative retinal detachment.18 Moreover, circulating inflammatory cytokines may interact with vascular receptors, increasing choroidal capillary permeability.19–22 Similarly, other conditions that compromise the integrity of BRB would also cause exudative retinal detachment such as Vogt-Koyanagi-Harada syndrome, autoimmune uveitis, and posterior scleritis.18,23
Ophthalmic DS must be differentiated from other conditions causing exudative retinal detachment in leukemia, including extramedullary relapse,19,21 leukemic retinopathy,24,25 systemic hypertension and drug toxicity. Leukemic retinopathy is characterized by venous dilation, tortuosity, Roth spots and cotton wool spots,24,25 which is managed with systemic chemotherapy or ocular radiotherapy,26,27 whereas ocular DS responds to corticosteroids. Pseudotumor cerebri, a complication of ATRA therapy, may also cause vision loss but typically presents with headache, nausea, vomiting and papilledema without SRF.28
In conclusion, ophthalmic evaluation provides a critical window for early DS detection. Since ocular symptoms can precede or coincide with systemic deterioration, comprehensive assessment including OCT is recommended for any APL patient reporting visual disturbances during induction therapy. Ocular manifestations may be unrecognized in DS patients with compromised systemic status. Although the temporary cessation of differentiation therapy is controversial, it may be warranted in cases of severe DS with profound organ dysfunction.11,16 Timely recognition of ophthalmic DS enables prompt corticosteroid administration, which is pivotal for mitigating life-threatening complications. Further investigation of ocular manifestations in DS may offer a non-invasive window into systemic inflammation and improve DS management strategies.
Conclusions
This case underscores that exudative retinal detachment can serve as an early indicator of DS in patients undergoing induction therapy for APL. The pathophysiology is attributed to inflammatory capillary leakage, which is highly responsive to systemic corticosteroids. Early recognition of ocular manifestations and prompt corticosteroid therapy can prevent both visual and life-threatening systemic complications.
Abbreviations
APL, acute promyelocytic leukemia; WBC, white blood cell; PT, prothrombin time; INR, international normalized ratio; APTT, activated partial thromboplastin time; ATRA, all-trans retinoic acid; ATO, arsenic trioxide; DS, differentiation syndrome; OCT, Optical coherence tomography; RPE, retinal pigment epithelium; SRF, subretinal fluid; SRD, serous retinal detachment; FFA, fundus fluorescein angiography; OD, oculus dexter; OS, oculus sinister; OU, oculus uterque; BCVA, best-corrected visual acuity; UCVA, uncorrected visual acuity; IOP, intraocular pressure; CT, computed tomography; BRB, Blood-retinal barrier.
Data Sharing Statement
No datasets were generated or analyzed during the current study.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
We acknowledged the assistance of hematology department in data collection.
Funding
This study was funded by Guangzhou Municipal Science and Technology Project, China, under Grant (No. 2025A04J4747) and the Jiangxi Provincial Natural Science Foundation, Jiangxi, China, under Grant (No. 20244BAB28027).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gim Y, Kim HJ. Ocular symptom can be the first presentation of differentiation syndrome in acute promyelocytic leukemia. Korean J Ophthalmol KJO. 2021;35(1):94–9. doi:10.3341/kjo.2020.0101
2. Wu Q, Yang X, Zhang J, et al. Improved prevention and treatment strategies for differentiation syndrome contribute to reducing early mortality in patients with acute promyelocytic leukemia. Blood Cancer J. 2024;14(1):113. doi:10.1038/s41408-024-01074-y
3. Ma YF, Lu Y, Wu Q, et al. Oral arsenic and retinoic acid for high-risk acute promyelocytic leukemia. J Hematol OncolJ Hematol Oncol. 2022;15(1):148. doi:10.1186/s13045-022-01368-3
4. Sanz MA, Fenaux P, Tallman MS, et al. Management of acute promyelocytic leukemia: updated recommendations from an expert panel of the European LeukemiaNet. Blood. 2019;133(15):1630–1643. doi:10.1182/blood-2019-01-894980
5. Platzbecker U, Avvisati G, Cicconi L, et al. Improved outcomes with retinoic acid and arsenic trioxide compared with retinoic acid and chemotherapy in non–high-risk acute promyelocytic leukemia: final results of the randomized Italian-German APL0406 trial. J Clin Oncol. 2017;35(6):605–612. doi:10.1200/JCO.2016.67.1982
6. Platzbecker U, Adès L, Montesinos P, et al. Arsenic trioxide and all-trans retinoic acid combination therapy for the treatment of high-risk acute promyelocytic leukemia: results from the APOLLO trial. J Clin Oncol. 2025;43(29):3160–3169. doi:10.1200/JCO-25-00535
7. Lo-Coco F, Avvisati G, Vignetti M, et al. Retinoic acid and arsenic trioxide for acute promyelocytic leukemia. N Engl J Med. 2013;369(2):111–121. doi:10.1056/NEJMoa1300874
8. Luesink M, Pennings JLA, Wissink WM, et al. Chemokine induction by all-trans retinoic acid and arsenic trioxide in acute promyelocytic leukemia: triggering the differentiation syndrome. Blood. 2009;114(27):5512–5521. doi:10.1182/blood-2009-02-204834
9. Fathi AT, Stein EM, DiNardo CD, Levis MJ, Montesinos P, De Botton S. Differentiation syndrome with lower‐intensity treatments for acute myeloid leukemia. Am J Hematol. 2021;96(6):735–746. doi:10.1002/ajh.26142
10. Issa GC, Stein EM, DiNardo CD. How I treat acute myeloid leukemia with differentiation therapy. Blood. 2025;145(12):1251–1259. doi:10.1182/blood.2024024008
11. Stahl M, Tallman MS. Differentiation syndrome in acute promyelocytic leukaemia. Br J Haematol. 2019;187(2):157–162. doi:10.1111/bjh.16151
12. Boscaro E, Cerrano M, Tibaldi T, et al. Atypical differentiation syndrome with sudden vision loss in acute promyelocytic leukemia treated with ATRA plus ATO: a clinical case. Mediterr J Hematol Infect Dis. 2024;16(1):e2024063. doi:10.4084/MJHID.2024.063
13. Oh SE, Choi SY. Differentiation syndrome with ocular manifestations in acute promyelocytic leukemia patients treated with all-trans retinoic acid. J Korean Ophthalmol Soc. 2021;62(4):571–576. doi:10.3341/jkos.2021.62.4.571
14. Tam EK, Ness S, Peeler CE. Exudative hemorrhagic retinopathy related to all-trans retinoic acid differentiation syndrome in a patient with acute promyelocytic leukemia. Int J Ophthalmol. 2021;14(2):323–325. doi:10.18240/ijo.2021.02.22
15. Hua HU, Rayess N, Moshfeghi AA. Acute promyelocytic leukemia with sudden vision loss. JAMA Ophthalmol. 2020;138(2):206–207. doi:10.1001/jamaophthalmol.2019.4838
16. Newman AR, Leung B, Richards A, Campbell TG, Wellwood J, Imrie FR. Two cases of differentiation syndrome with ocular manifestations in patients with acute promyelocytic leukaemia treated with all-trans retinoic acid and arsenic trioxide. Am J Ophthalmol Case Rep. 2018;9:106–111. doi:10.1016/j.ajoc.2018.01.026
17. Levasseur SD, Tantiworawik A, Lambert Maberley DA. All-trans retinoic acid differentiation syndrome chorioretinopathy: a case of multifocal serous neurosensory detachments in a patient with acute promyelocytic leukemia treated with all-trans retinoic acid. Retin Cases Brief Rep. 2013;7(1):46–49. doi:10.1097/ICB.0b013e3182618d6c
18. Amer R, Nalcı H, Yalçındağ N. Exudative retinal detachment. Surv Ophthalmol. 2017;62(6):723–769. doi:10.1016/j.survophthal.2017.05.001
19. Sharma T, Grewal J, Gupta S, Murray PI. Ophthalmic manifestations of acute leukaemias: the ophthalmologist’s role. Eye. 2004;18(7):663–672. doi:10.1038/sj.eye.6701308
20. Sanz MA, Montesinos P. How we prevent and treat differentiation syndrome in patients with acute promyelocytic leukemia. Blood. 2014;123(18):2777–2782. doi:10.1182/blood-2013-10-512640
21. Sharma H, Majumder PD, Rao C, Biswas J. A case of Acute Myeloid Leukemia masquerading as unilateral exudative detachment. Am J Ophthalmol Case Rep. 2016;4:47–49. doi:10.1016/j.ajoc.2016.08.004
22. Sprague AH, Khalil RA. Inflammatory cytokines in vascular dysfunction and vascular disease. Biochem Pharmacol. 2009;78(6):539–552. doi:10.1016/j.bcp.2009.04.029
23. Chi W, Yang P, Li B, et al. IL-23 promotes CD4+ T cells to produce IL-17 in Vogt-Koyanagi-Harada disease. J Allergy Clin Immunol. 2007;119(5):1218–1224. doi:10.1016/j.jaci.2007.01.010
24. El Salloukh NA, Hage DG, Bashshur AZ, Kheir WJ. Early ophthalmological manifestations of acute myeloid leukemia: current perspectives. Clin Ophthalmol. 2022;16:2119–2127. doi:10.2147/OPTH.S342720
25. Karesh JW, Goldman EJ, Reck K, Kelman SE, Lee EJ, Schiffer CA. A prospective ophthalmic evaluation of patients with acute myeloid leukemia: correlation of ocular and hematologic findings. J Clin Oncol. 1989;7(10):1528–1532. doi:10.1200/JCO.1989.7.10.1528
26. Kim J, Chang W, Sagong M. Bilateral serous retinal detachment as a presenting sign of acute lymphoblastic leukemia. Korean J Ophthalmol KJO. 2010;24(4):245–248. doi:10.3341/kjo.2010.24.4.245
27. Wu L, Calderón M, Hernández G, Marbis J, Ramírez V. Bilateral exudative retinal detachment as the first sign of relapsing acute myelogenous leukaemia. Clin Exp Ophthalmol. 2006;34(6):623–625. doi:10.1111/j.1442-9071.2006.01291.x
28. Holmes D, Vishnu P, Dorer RK, Aboulafia DM. All-trans retinoic acid-induced pseudotumor cerebri during induction therapy for acute promyelocytic leukemia: a case report and literature review. Case Rep Oncol Med. 2012;2012:313057. doi:10.1155/2012/313057
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Highly Curative Treatment of High-Risk Acute Promyelocytic Leukemia: Induction and Consolidation with ATRA+ATO+anthracyclines and Maintenance with ATRA+RIF
Liu D, Tong J, Chen E, Wang L, Xue L, Zhang X, Zhao N, Hu X, Zheng C
Blood and Lymphatic Cancer: Targets and Therapy 2024, 14:63-69
Published Date: 29 July 2024