Back to Journals » OncoTargets and Therapy » Volume 12
Extrapancreatic Neuropathy Correlates with Early Liver Metastasis in Pancreatic Head Adenocarcinoma
Authors Lu M, Xiu D, Guo L, Yuan C, Zhang L, Tao L ![]()
Received 4 July 2019
Accepted for publication 7 November 2019
Published 16 December 2019 Volume 2019:12 Pages 11083—11095
DOI https://doi.org/10.2147/OTT.S221844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Arseniy Yuzhalin
Meng Lu,1 Dian-rong Xiu,2 Li-mei Guo,3 Chun-hui Yuan,2 Ling-fu Zhang,2 Lian-yuan Tao2
1Department of Pulmonary Oncology, Tianjin Medical University Cancer Institute & Hospital, Tianjin, People’s Republic of China; 2Department of General Surgery, Peking University Third Hospital, Beijing, People’s Republic of China; 3Department of Pathology, Peking University Third Hospital, Beijing, People’s Republic of China
Correspondence: Dian-rong Xiu
Peking University Third Hospital, 49 North Garden Road, Haidian District, Beijing, People’s Republic of China
Tel +86 156 1190 8135
Email [email protected]
Background: Pancreatic ductal adenocarcinoma has a devastatingly poor prognosis, and most prognostic factors reflected the tumor stage more than the tumors’ biology. The peripheral nerve plexus is densely distributed in the tumor micro-environment, and there are interactions between tumor cells and these nerves. Perineural invasion is an important risk factor for tumor recurrence and metastasis in pancreatic head adenocarcinoma, but the concrete types of extrapancreatic neuropathy and its role in predicting prognosis are still not clear.
Objective: To clarify the role of extrapancreatic neuropathy in the early postoperative liver metastasis and tumor-related mortality in pancreatic head adenocarcinoma and to study the mechanism of tumor recurrence and liver metastasis in pancreatic head adenocarcinoma.
Methods: We reported a retrospective study of 60 patients with resectable pancreatic head adenocarcinoma, all of whom accepted radical pancreaticoduodenectomy. Plexus pancreaticus capitalis II (PLX-II) was the representation of extrapancreatic plexus in our study, and all of these plexus had immunohistochemical staining. We defined the postoperative tumor recurrence and tumor-related mortality within 6 months as the early prognostic indicators and analyzed the pathological alterations in PLX-II among different prognosis groups.
Results: There were 18 patients suffering early postoperative liver metastasis; these two groups differed significantly in the average number of nerve trunks (P<0.001), the proportion of neuritis (P=0.003), the content of sympathetic nerve fibers (P=0.004) and parasympathetic nerve fibers (P<0.001) per unit area of PLX-II. There were 15 patients suffering early postoperative mortality, and there were significant differences between these two groups in the average number of nerve trunks (P<0.001), the proportion of neuritis (P=0.009), the content of sympathetic nerve fibers (P=0.023) and parasympathetic nerve fibers (P<0.001) per unit area of PLX-II.
Conclusion: The patterns of extrapancreatic neuropathy could reflect the biological behavior of resectable pancreatic head adenocarcinoma, and the pathological features of PLX-II were closely related to early liver metastasis and mortality.
Keywords: pancreatic adenocarcinoma, extrapancreatic neuropathy, liver metastasis, neural remodeling
Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the digestive tumor with extremely high malignancy, characterized by the high risk of early recurrence and mortality. Pancreatic head is the most common place where pancreatic tumor developed.1 The biological behavior of pancreatic head adenocarcinoma is evaluated mainly by the tumor staging, the pathological grading and the tumor’s resectability.1,2 Nowadays, the pancreatic head tumor without metastasis could be classified into the resectable, the borderline resectable and the locally advanced tumor. The classification is due to the differences in the efficacy of surgery in improving long-term survival and can reflect the distinction of the tumors’ biological behavior.3,4 Radical resection (pancreaticoduodenectomy, PD) is suggested in resectable pancreatic head tumor to obtain the R0/R1 resection margin.
However, patients with resectable pancreatic head adenocarcinoma differed significantly in the prognosis even after radical PD. Patients with early tumor stage (Stage I/II) or well histologic grade still had early recurrence or metastasis after radical surgery and would ultimately succumb to their illness.5 Thus, efforts to identify factors that predict early recurrence or metastasis in patients with resectable pancreatic head adenocarcinoma are warranted.
Perineural invasion was one of the most important pathological patterns in PDAC and was proved to be related with the tumor recurrence and metastasis.6 According to the anatomy of peripancreatic plexus, the perineural invasion could be divided into the intrapancreatic and extrapancreatic neural invasion.7,8 The intrapancreatic neural invasion was found in more than 90% of the patients and correlated with lymph node metastasis, whereas the extrapancreatic neural invasion would lead to worse prognosis.8 The peripancreatic plexus belonged to the tumor microenvironment, which played an important role in the progression of PDAC. The intrapancreatic plexus tends to manifest profound alterations, which were called neuroplastic changes. This neuropathy correlated strongly with the severity of pancreatic neuropathic pain and patient’s quality of life.9,10 But the extrapancreatic neural alterations were less focused in previous studies for the extrapancreatic plexus was complex and difficult to obtain.11 Therefore, this study aimed to examine the predictors of early recurrence and mortality after resection in patients with resectable pancreatic head adenocarcinoma, with a particular emphasis on the extrapancreatic neuropathy.
Methods and Materials
Patients Selection
We performed a retrospective case–control study of patients who underwent surgical resection for pancreatic head adenocarcinoma from January 2010 to December 2015 at Peking University Third Hospital. The Ethics Institutional Review Board approved the study protocol. Patient consent to review their medical records was not required in this study for the reason that all samples were obtained in standard surgical procedures, and waiving informed consent will not adversely affect subjects’ health and rights. We declared all patient data confidentiality and our compliance with the Declaration of Helsinki. Patients with clinically and pathologically confirmed resectable pancreatic head adenocarcinoma were included in this study. Patients who had perioperative complications-related death and received neoadjuvant therapy were excluded.
We collected data regarding demographic, clinical and pathological variables from the electronic medical records. The tumor stage and resectability were determined by the treating surgeon in accordance with consensus-based definitions. From pathology reports, we obtained information about surgical resection status (R0 or R1), histologic grade (well, moderate or poor differentiation), lymph node status, lymphovascular and intrapancreatic neural invasion.
Tissue Processing
All patients in this study received standard radical PD. The operation is usually performed with a right paramedian incision in the upper abdomen. First, we open the gastrocolic ligament and explore the front surface of the pancreas. After moving the colon, the superior mesenteric vein (SMV) below the pancreas is exposed. The small omentum is separated along the hepatic artery to the starting of celiac trunk. The gastroduodenal artery and inferior pancreatoduodenal artery are then dissociated and ligated. Then, we remove the gallbladder, cut off the hepatobiliary tube, stomach and jejunum, and sever pancreatic neck anterior to SMV. If the vascular walls of SMV or portal vein (PV) are invaded by the tumor, then the SMV/PV is partially resected and end-to-end anastomosis is conducted according to the scope of the affected vein. There were no artery resection procedures, all pancreatic tumors were resectable in this study.
The plexus pancreaticus capitalis II (PLX-II) was the most important part of extrapancreatic plexus, where neural invasion mostly occurred.11 Plexus was removed from the same regions, which were defined by the Japan Pancreatic Society grouping criteria.12 In the criteria, pancreatic head plexus can be further divided into two parts, one being the direct route from the right celiac ganglia to the upper internal side of the uncinate process and the other route extending from the superior mesenteric artery (SMA) to the upper internal side of the uncinate process. In the clinical experiences, the root of the mesenteric artery was dissected to open the vascular sheath, and then the membranous fold at the uncinate process was removed along its right side, followed by the dissection of the nerves and soft tissues at the right half. In order to obtain the complete SMA margin, electric knife burning and ligation rather than the use of a cutting closure were preferred in the anatomy of unciform process. The anterior, right and posterior parts of SMA were completely dissociated, and the PLX-II and unciform processes were separated from the right side of the SMA wall completely (Figure 1).
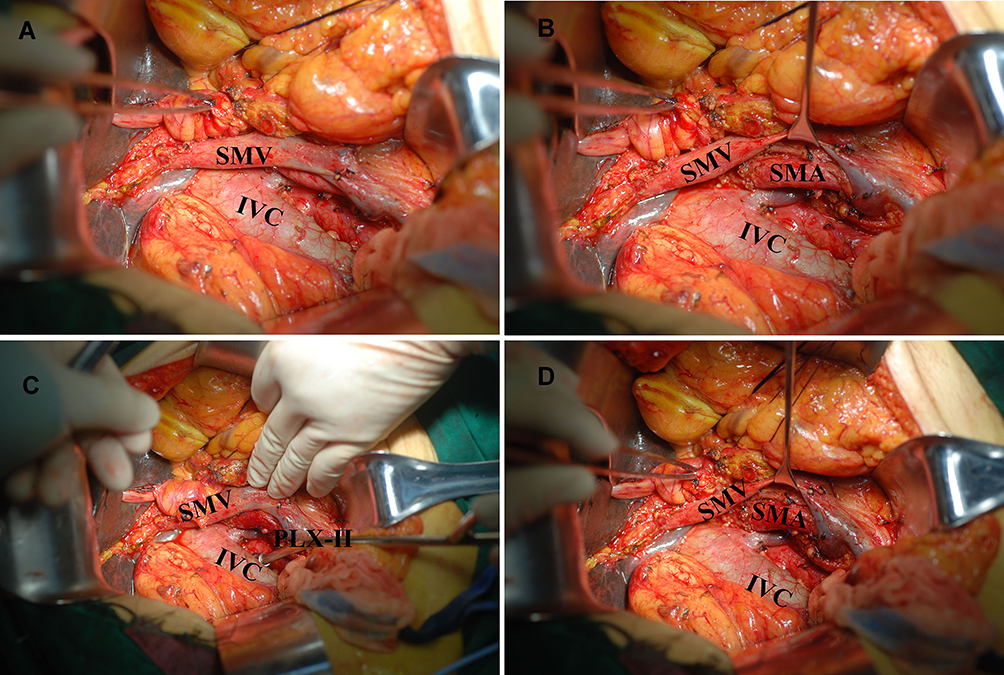 |
Figure 1 The obtainment process of integrate tissues in SMA margin in pancreaticoduodenectomy. (A) The anatomy of abdominal blood vessels. (B) The exposure of SMA. (C) The PLX-II was ligated by the silk thread from the SMA. (D) The vascular surface of SMA margin.Abbreviations: SMA, superior mesenteric artery; SMV, superior mesenteric vein; PLX-II, plexus of pancreatic head II; IVC, inferior vena cava. |
Plexus Immunohistochemistry
Plexus tissues obtained in SMA margin were pathologically examined individually. Five paraffin-embedded sections (3 μm) of PLX-II tissues were obtained from each patient, and immunohistochemical staining was performed in every section. A rabbit polyclonal antibody against the tyrosine hydroxylase (TH) was used to observe the sympathetic nerves, and the vesicular acetylcholine transporter (VAChT) was used to observe the parasympathetic nerves. All sections were deparaffinized with xylene and rehydrated, and antigen retrieval was performed by heating in an autoclave in 10 mmol/L sodium citrate buffer (pH 6.0). The sections were then immersed in 3% hydrogen peroxide in methanol to quench the activity of endogenous peroxidase and in 1% bovine serum albumin to block non-specific binding, followed by incubation with TH or VAChT overnight at 4°C. The sections were incubated with a biotinylated secondary antibody after being washed with phosphate-buffered saline (PBS) and followed by incubation with the streptavidin-horseradish peroxidase complex. Finally, the sections were immersed in 3,3ʹ-diaminobenzidine for 6 mins, counterstained with 10% Mayer’s hematoxylin, dehydrated and mounted in crystal mount. PBS was used instead of a primary antibody for the negative control. To minimize variation in immunopositivity, all sections were stained in 3,3ʹ-diaminobenzidine for the same amount of time.
Analysis of Extrapancreatic Neuropathy
One pathologist who was blinded to the clinical outcome independently scored the results of the staining. The extrapancreatic neuropathy in this study included the neural hyperplasia, the neural hypertrophy, the neuritis, the neural invasion and the autonomic innervation changes. A digital pathological section scanner (NanoZoomer-SQ, Hamamatsu Photonics, Japan) in combination with the Image Pro Plus 6.0 software (Windows 10, Media Cybernetics, Inc.) was used for measurements.
Five sections of PLX-II were made from each patient, and the features of neurological changes were calculated based on the mean value of all these sections. The mean number of all nerve trunks in five sections was counted as the degree of neural hyperplasia; the mean area of each nerve trunks was representative of neural hypertrophy; the proportion of the immunostained area within a nerve trunk to the whole area of the same nerve trunk was regarded as the autonomic innervation. The details of the above neuropathies could be calculated with the Image Pro Plus 6.0 software. Image Pro Plus 6.0 software was used to measure the optical density (OD) value of immunostained sympathetic or parasympathetic nerve fibers in a single visual field, and the OD value could be used as the index of immune reactivity of autonomic nerve fibers. The OD is a value automatically matched by the software according to the staining intensity of nerve fibers and is calculated as pixel, which can be used as a semi-quantitative analysis index of the content of nerve fibers. The quantification of neural immunoreactivities for TH or VAChT was carried out as defined in Figure 2.
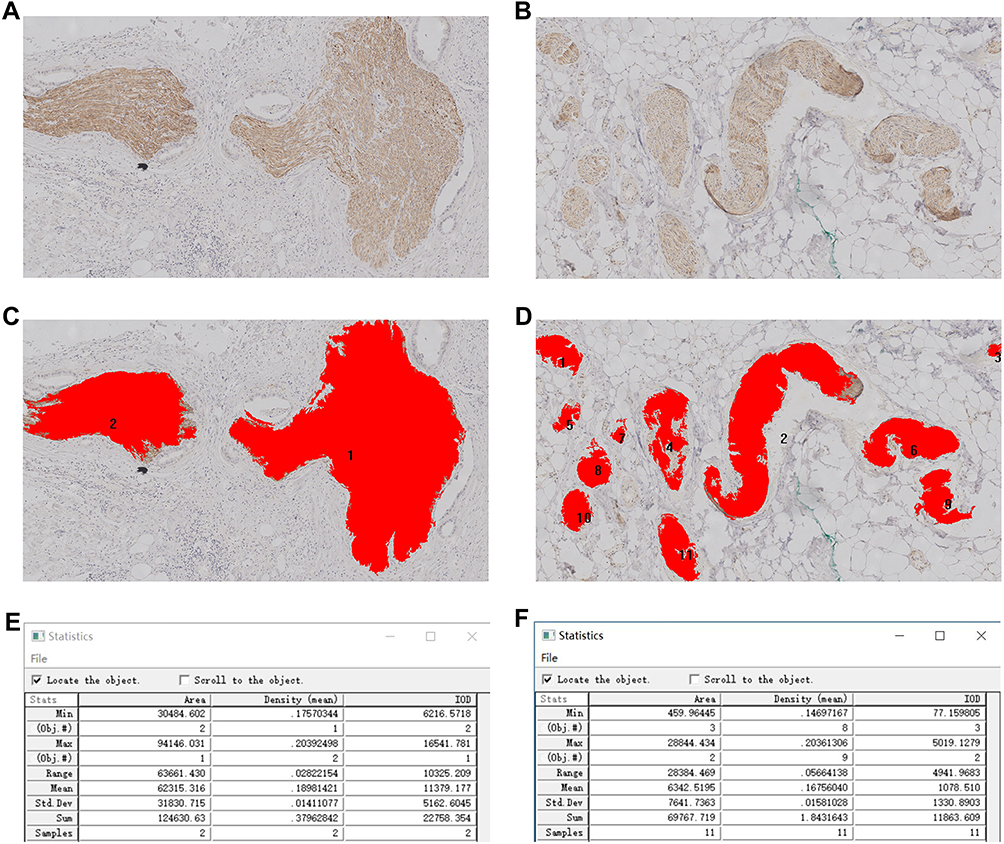 |
Figure 2 The statistics of mean area per nerve and the mean optic density value per unit area in hot spot areas by Image Pro Plus 6.0 software. (A) Sparse subareas of nerve distribution; (B) Dense subareas of nerve distribution; (C) Software automatically recognizes the immune staining nerves and count the number (2 trunks); (D) Software automatically recognizes the immune staining nerves and count the number (11 trunks); (E) Average calculation results of 2 nerves; (F) Average calculation results of 11 nerves. |
The histomorphological evaluation of the specimen included the existence of pancreatic neuritis and neural invasion in PLX-II. The neuritis indicated the phenomena that nerve bundles were surrounded by inflammatory cells such as the lymphocyte. The lymphocytes obviously gathered around the nerve bundles in this study, and the neural inflammatory infiltration was observed. Any nerve inflammatory infiltration in one section was deemed to be neuritis. The neural invasion indicated the phenomena that tumor cells invaded the membrane of nerve trunks or nerve bundles. The existence of tumor cells around nerve membranes was the indicator of the neural invasion. Tumor cells are characteristic of atypical hyperplasia, breaking the epineurium or penetrating into the endoneurium, resulting in destruction of neural structures. The pathological patterns of neuritis and neural invasion are shown in Figure 3.
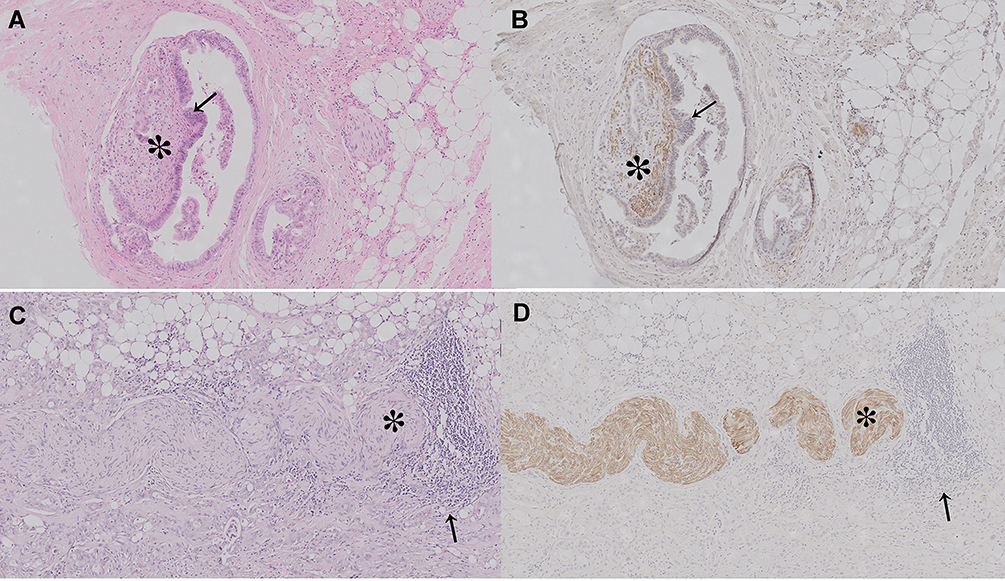 |
Figure 3 Representative photomicrographs (100×) showing staining of nerves. (A) The phenomenon of neural invasion in HE staining. (B) The phenomenon of neural invasion in immunochemistry staining. (C) The phenomenon of peripheral lymphocytes aggregation in HE staining. (D) The phenomenon of peripheral lymphocytes aggregation in immunochemistry staining. The black arrow indicates the cancer cells in A and B, the lymphocytes in C and D. The asterisk indicates the nerves which were destroyed or surrounded by the tumor cells or lymphocytes. |
Prognostic Analysis
The primary study endpoint was early recurrence and mortality, defined as recurrence or death within 6 months after surgery. We censored data from patients alive at the last follow-up (December 31, 2017) on that date. All patients were followed up by physical examination and abdominal CT every 3–6 months. Follow-up time was defined as the time from the date of the first surgery to the date of the last follow-up and was recorded in months. Follow-up information were obtained from office charts, hospital records and telephone interviews. Overall survival (OS) time was defined as the time from the date of the first surgery to the date of death by recurrence. Disease-free survival (DFS) time was defined as the time from the date of the first surgery to the date of the first evidence of recurrence.
Early recurrence was defined as relapse within 6 months. The patterns of recurrence sites were subdivided into loco-regional recurrence (LR) and liver metastasis (LM). The former indicated a recurrence presumably due to occult residual tumor cells left behind at the time of resection, whereas the latter is the most common cause of death among PDAC patients who undergo radical surgery.
Statistical Analysis
We compared demographics and clinical characteristics for patients with early mortality or recurrence versus those with non-early mortality or recurrence using Student t-test for the continuous variables and χ2 or Fisher exact test for the categorical variables as appropriate. To determinate factors associated with early mortality and recurrence, we used multivariable logistic regression with purposeful selection of covariates. The Mann–Whitney test, recommended for the comparison of two independent groups, was performed when required. Differences were considered significant if P value was less than 0.05. All P values were calculated using the SPSS 23.0 software.
Results
Characteristics of Patients
The study cohort included 60 patients with a mean age of 63.3 years (range, 44–84 years), of them there were 35 males and 25 females. There were 21 (35.0%) patients with radiologically diagnosed SMV/PV invasion, 10 of which received vascular resection because of the tumor’s direct contact. The pathological staging of pancreatic tumor was based on the 8th AJCC staging system. The poor differentiation was mostly common (46.7%, 28/60) in our study. Intrapancreatic neural invasion was popularly existed (88.3%, 53/60), and 33.3% (20/60) of the patients had intravenous carcinoma embolus. The R1 resection accounted for 56.7% of all patients (36/60), whereas 28.3% (17/60) of the patients had a positive SMA margin. Twenty-seven (45.0%) patients had adjuvant therapy after radical surgery. The characteristics are listed in Table 1.
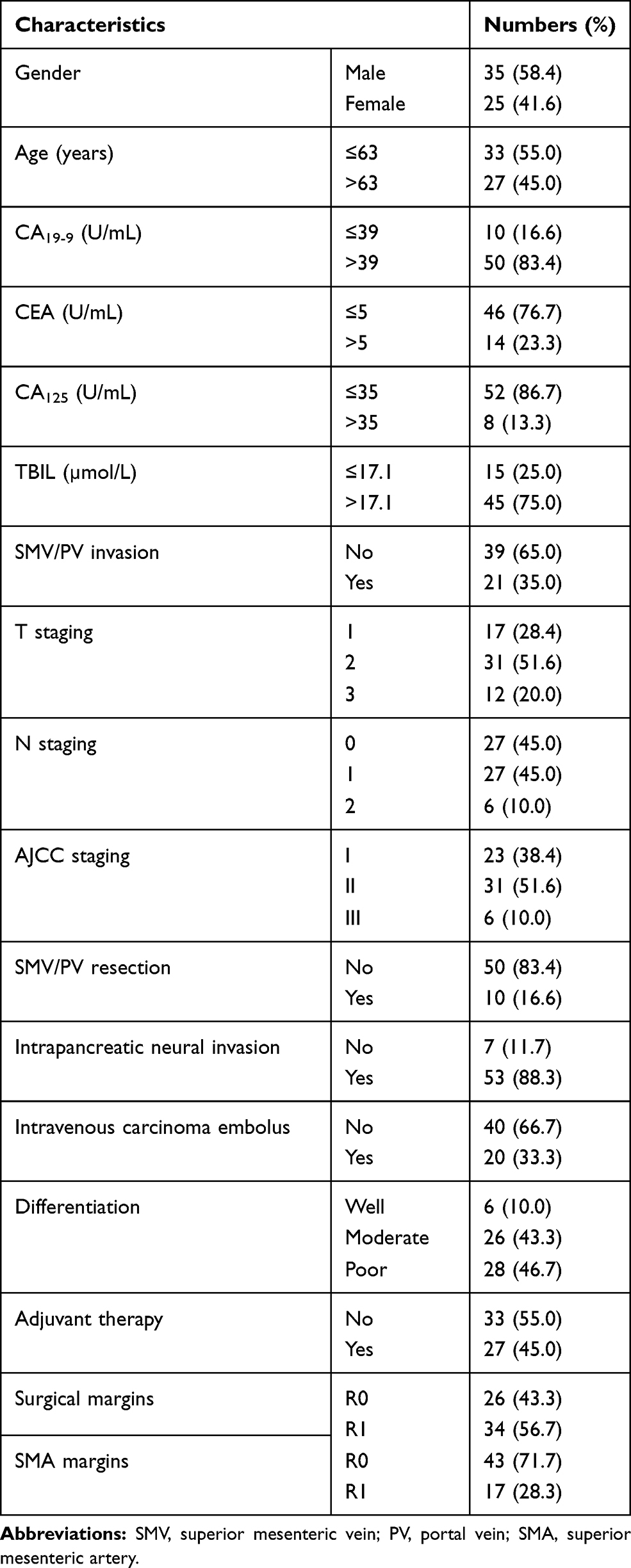 |
Table 1 The Clinicopathological Characteristics of Patients with Resectable Pancreatic Head Adenocarcinoma |
The Prognosis Analysis
Until the last follow-up time, there were 15 (25.0%) patients who had early mortality, 11 (18.3%) patients had early local recurrence and 18 (30.0%) patients had early liver metastasis. There were 49 patients who had 58 recurrences, including 24 local recurrences and 34 liver metastases. The Kaplan–Meier univariate survival analysis of OS, DFS, LR and LM is listed in Table 2. The Cox multivariate survival analysis is listed in Table 3. The results showed that the elevated CA125 level was the independent risk factor for OS and LR, the lymph node metastasis was the independent risk factor for OS and LM, patients in N2 staging had a higher risk suffering from the early mortality (P=0.011) and early liver metastasis (P=0.044). However, all of the above factors had no influence on DFS, only SMV/PV resection had the tendency for predicting DFS (P=0.061). Furthermore, the SMV/PV invasion was the independent risk factor for OS (P=0.002).
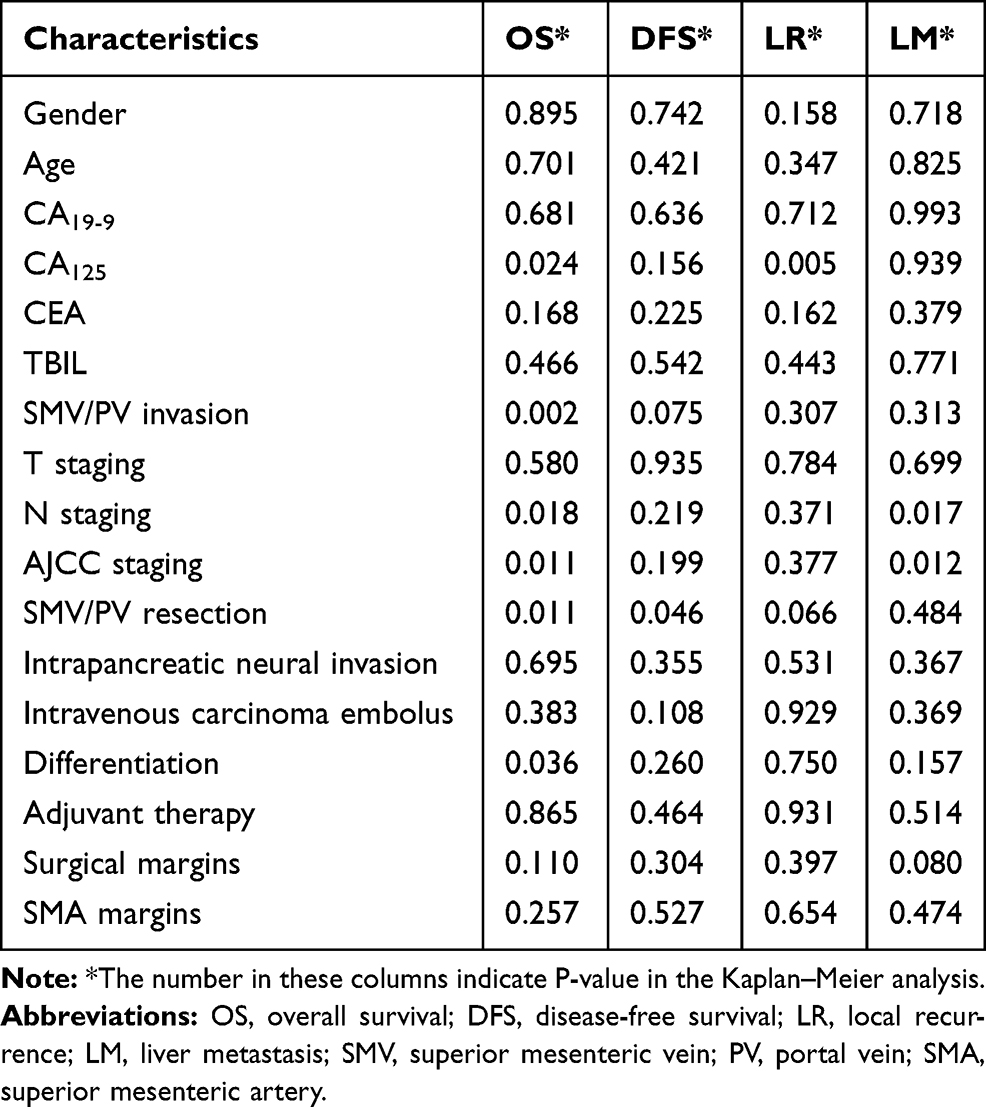 |
Table 2 The Kaplan–Meier Analysis of Clinicopathological Features |
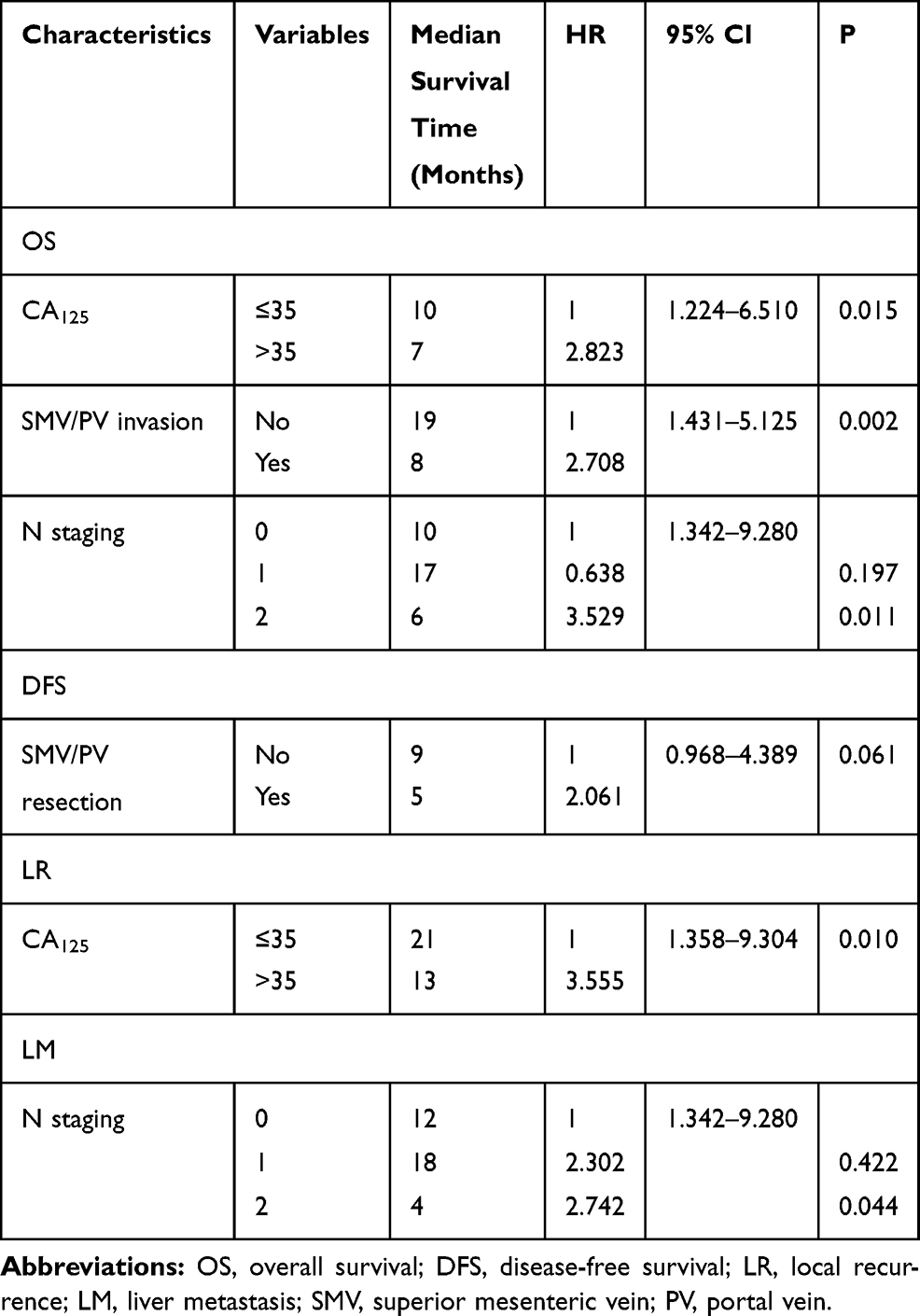 |
Table 3 The Cox Multifactor Prognosis Analysis of Clinicopathological Features |
The Characteristics of Extrapancreatic Neuropathy
The overall patterns of extrapancreatic neuropathy in 60 patients are shown in Table 4. For each patient, the density and average area of nerve trunks, the neuritis and neural invasion, and the distribution of sympathetic fibers and parasympathetic fibers per nerve trunk were all analyzed. The distribution characteristics of sympathetic fibers and parasympathetic fibers were different among individuals. The immunohistochemistry showed that the staining strength of the same nerve with different antibodies (TH or VAChT) was also significantly distinct, suggesting that the sympathetic and parasympathetic nerve fibers in the same nerve had significant differences in composition. Immunohistochemical staining with the same antibody was performed in different sections, and the results showed that the overall staining strength of the nerves in the region was also significantly different. The autonomic innervation in nerve trunk is presented in Figure 4.
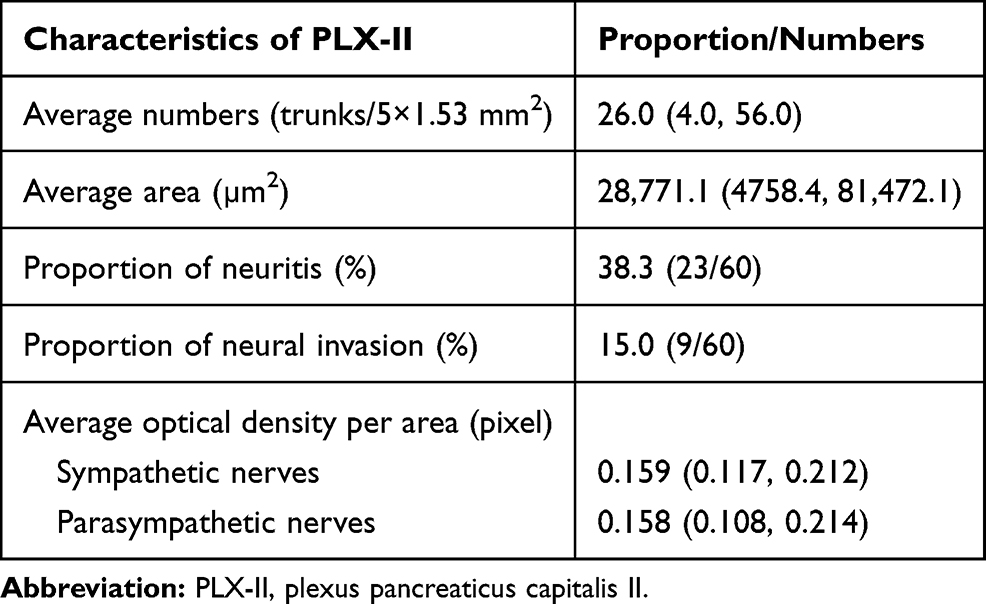 |
Table 4 The Patterns of Extrapancreatic Neuropathy in 60 Patients |
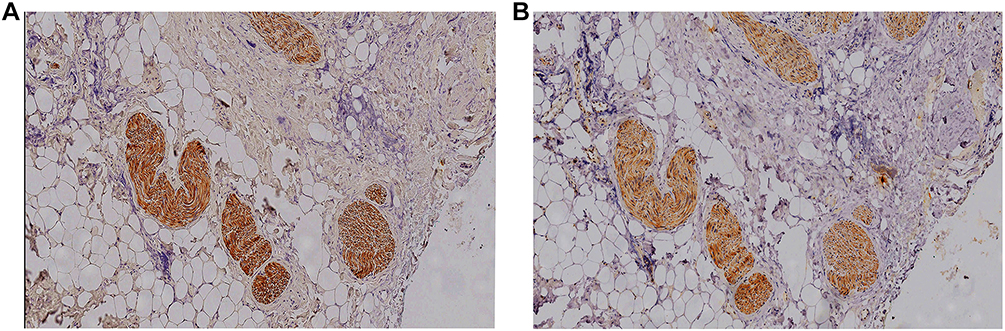 |
Figure 4 The difference of staining intensity after immunostaining of autonomic nerve fibers. (A) TH staining of sympathetic nerve fibers presented a strong staining intensity; (B) VAChT staining of parasympathetic nerve fibers showed a weak staining intensity. |
Extrapancreatic Neuropathy and Early Mortality
Contrary to our experience, the proportion of neural invasion in two groups did not display significant difference (P=0.531). In early mortality group, only 20% (3/15) of the patients had neural invasion in PLX-II, and in non-early mortality group, the proportion was similar, 13.3% (6/45) of the patients had neural invasion in PLX-II. However, the proportion of neuritis in PLX-II in patients with early mortality was 66.7% (10/15), which was higher than that in patients with non-early mortality (P=0.009), the latter was only 28.9% (13/45).
The degree of neurogenesis also differed significantly in these two groups (P<0.001). In early mortality group, the mean number of PLX-II nerve trunks was 35.0 trunks (23.0, 56.0)/(5×1.53 mm2), whereas in non-early mortality group, the mean number was only 23.0 trunks (4.0, 44.0)/(5×1.53 mm2). On the other hand, the degree of neural hypertrophy did not present obvious difference among these two groups (P=0.066).
Interestingly, patients in these two groups had distinct autonomic innervations. Patients in early mortality group tended to have a higher distribution of sympathetic (P=0.023) and parasympathetic (P<0.001) nerves than patients in non-early mortality group. As is shown in Table 5, the OD value per unit area of sympathetic and parasympathetic nerves was 0.157 and 0.152 in non-early mortality group, and it was lower than that in early mortality group, the OD value of which was 0.167 and 0.179, respectively. All of these characteristics are listed in Table 5.
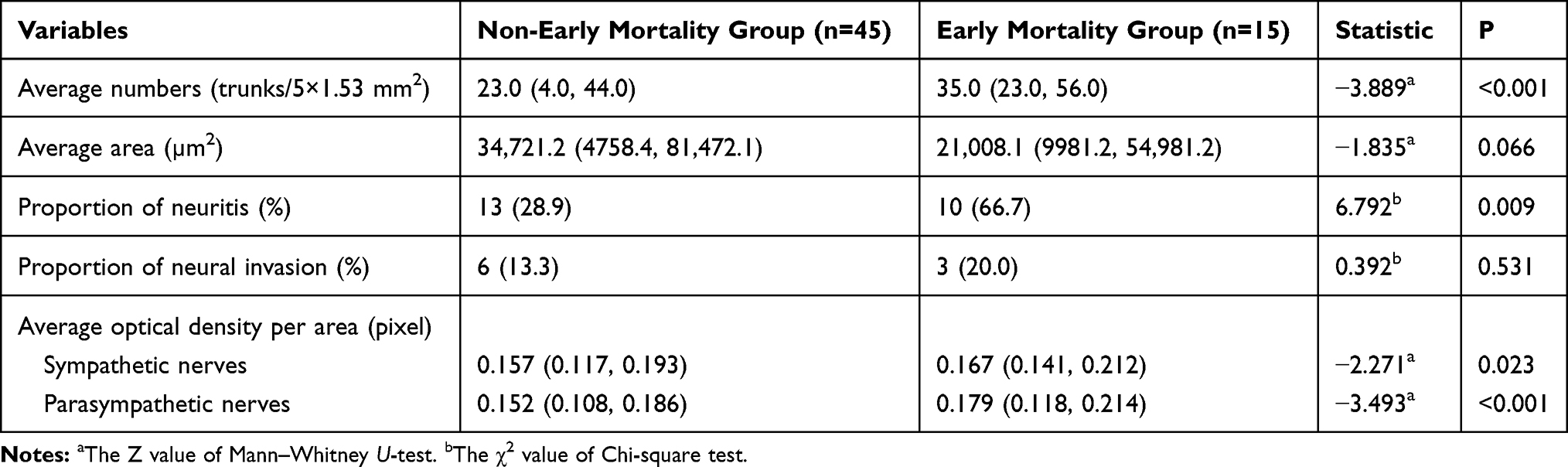 |
Table 5 The Patterns of Extrapancreatic Neuropathy Among Different Prognostic Groups (Early Mortality vs Non-Early Mortality) |
Extrapancreatic Neuropathy and Early Recurrence
The early local recurrence occurred in 11 patients. As is shown in Table 6, the extrapancreatic neuropathy had no difference within the groups of early local recurrence and non-early local recurrence.
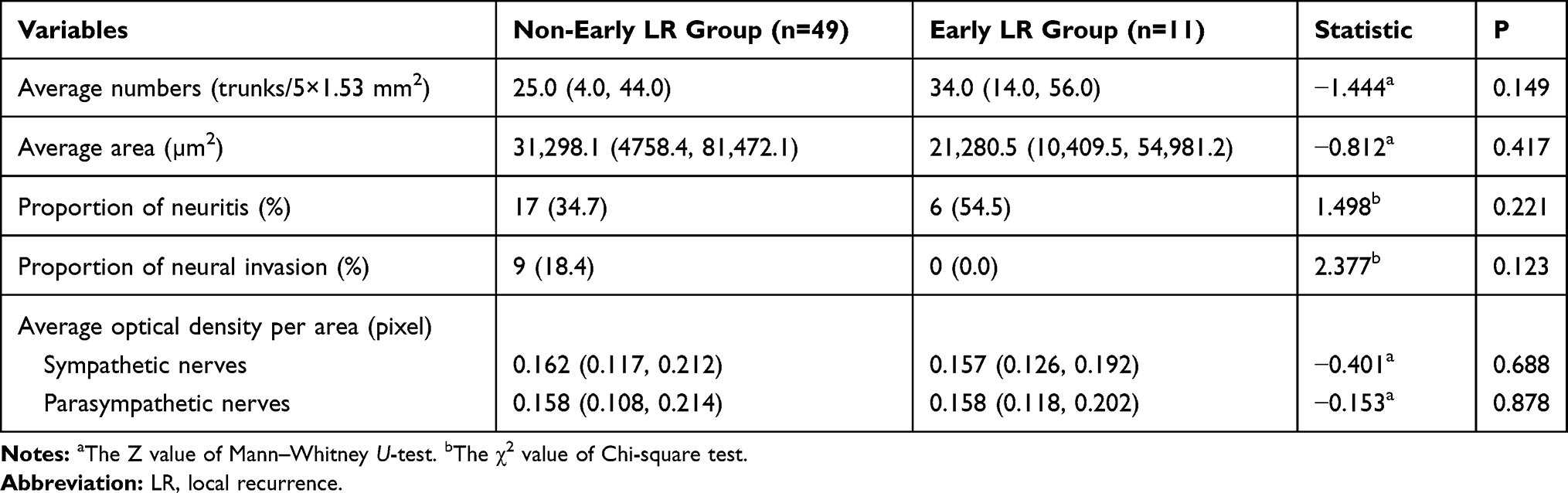 |
Table 6 The Patterns of Extrapancreatic Neuropathy Among Different Prognostic Groups (Early Local Recurrence vs Non-Early Local Recurrence) |
The early liver metastasis occurred in 18 patients. Patients in the early liver metastasis group had a higher proportion of neuritis (P=0.003) and a higher degree of neurogenesis (P<0.001) than patients without early liver metastasis. As is shown in Table 7, the mean number of nerve trunks in early liver metastasis group was 35.5 trunks (28.0, 56.0)/(5×1.53 mm2), which was higher than that in non-early liver metastasis group, the latter was only 22.5 trunks (4.0, 43.0)/(5×1.53 mm2).
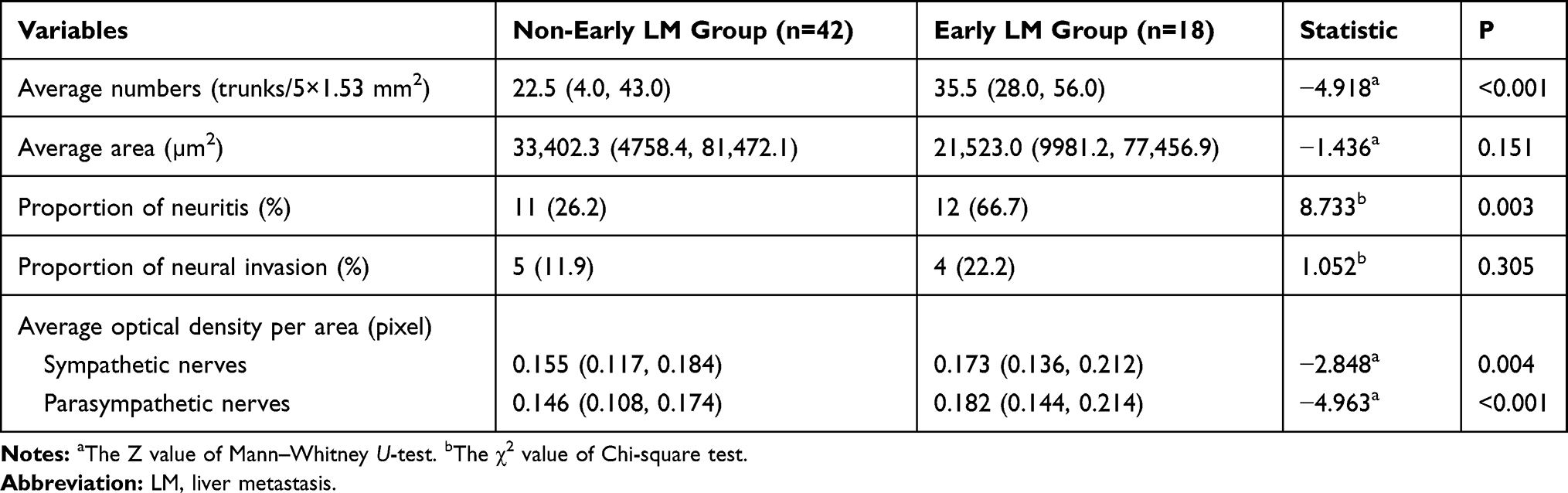 |
Table 7 The Patterns of Extrapancreatic Neuropathy Among Different Prognostic Groups (Early Liver Metastasis vs Non-Early Liver Metastasis) |
The difference of autonomic innervations in these two groups presented the same characteristics as the early mortality group. Patients in early liver metastasis group tended to have a higher distribution of sympathetic (P=0.004) and parasympathetic (P<0.001) nerve fibers than patients in non-early liver metastasis group. As to other characteristics of extrapancreatic neuropathy, these two groups had nothing difference.
Discussion
Pancreatic head adenocarcinoma is characterized by early tumor recurrence after radical resection; liver metastasis is the main reason for patients’ postoperative early mortality and the failure of treatments. Nowadays, the norms that reflect the biological behavior of pancreatic carcinoma included the tumor staging system (tumor-node-metastasis) and the resectability evaluation. However, parts of patients with resectable pancreatic head adenocarcinoma in early stage would have tumor recurrence within 6 months after radical surgery.5 This indicated that there might exist other prognostic factors that influence the biological behavior of pancreatic head adenocarcinoma.
Perineural invasion was proved to be important pathological factors influencing the prognosis of PDAC and might be the routes for tumor recurrence and metastasis in previous study.6 Intrapancreatic neural invasion occurred more frequently and correlated with extrapancreatic neural invasion.13 The mechanism of extrapancreatic neural invasion influencing tumor metastasis was still unclear for extrapancreatic nerve plexus was diverse and hard to obtain.
All patients in our study were radiologically and pathologically diagnosed resectable pancreatic head adenocarcinoma. In preoperative pancreatic contrast-enhanced CT, the SMA was all free from tumor mass, and we obtained the PLX-II located between the SMA and unciform process as the representation of extrapancreatic plexus.11,14,15 Some researchers proposed that pancreatic nerves underwent prominent alterations during the evolution and progression of pancreatic cancer.15–17 Intrapancreatic nerves could increase in size and number, and the proportion of autonomic and sensory fibers is switched.10,17 Besides these, plexus could also be infiltrated by perineural inflammatory cells or invaded by pancreatic cancer cells. But how the autonomic nervous system influence the prognosis of pancreatic head adenocarcinoma was still unknown, and the study on pathological alterations of extrapancreatic plexus was little.
Recent studies suggested that the neural invasion was just one of the characteristics of peripheral neuropathy, which also included peripheral nerve proliferation (neurogenesis), nerve hypertrophy, nerve inflammatory cell infiltration (neuritis) and the change of autonomic innervations.9,18 The nerve hyperplasia and hypertrophy might indicate the increase of neurotrophic substances in the tumor microenvironment and were associated with severe abdominal pain and tumor metastasis in PDAC.15,19 Neurogenesis was found in all PLX-II specimens in this study but more significant in patients with early liver metastasis and early mortality. The nerve density of PLX-II in patients with postoperative early liver metastasis was 35.5 trunks/(5×1.53 mm2), while in patients with non-early liver metastasis, nerve density significantly reduced to 22.5 trunks/(5×1.53 mm2). The nerve density in patients with early mortality was 35.0 trunks/(5×1.53 mm2), and it reduced to 23.0 trunks/(5×1.53 mm2) in patients with non-early mortality. It is worth noting that among all prognostic indicators in this study, there was no significant difference between the two groups in the average nerve area of PLX-II, namely the degree of nerve hypertrophy. The results showed that the degree of neurogenesis of PLX-II might have a certain impact on early liver metastasis after radical surgery in patients with resectable pancreatic head adenocarcinoma, severe nerve hyperplasia might promote the liver metastasis, thus affecting the survival status of postoperative patients. However, the degree of neurogenesis had no significant effect on early local recurrence, suggesting that neurogenesis might not be a risk factor for early local recurrence.
Nerve inflammatory infiltration is a phenomenon in which immune inflammatory cells enter into the nerve spaces. In patients with chronic pancreatitis and pancreatic cancer, the peripheral plexus or nerve bundles of the pancreas can be surrounded by inflammatory cells such as lymphocytes and macrophages, which infiltrate into the nerve tissues through the damaged nerve bundle membrane.10 The infiltration of inflammatory cells through the nerve capsule into the perineural space also reflects the invasiveness of pancreatic head cancer, which may be related with visceral pain and distant metastasis caused by the tumor.20 In the original models of pancreatic cancer, the infringed pancreatic cells presented the process of epithelial to mesenchymal transition (EMT), the mutated cells entered into the blood circulation prior to tumor formation, and the presence of inflammatory cells was essential for EMT and tumor diffusion.21 In this study, qualitative analysis was performed on lymphocytes around the plexus, and the results showed that the proportion of neuritis was 38.3% (23/60), which was a risk factor for early liver metastasis and early mortality. There was no correlation between the proportion of neuritis and early local recurrence, suggesting that the relationship between immune mechanism and local recurrence was not close. Some studies have suggested that pancreatic cancer might mediate the development and deterioration of tumor through activation and destruction of the immune system, which also established the foundation of specific targeted therapy.22 Patient selection was important for the efficacy of drugs targeting the immune system, and targeted application of immunomodulators might achieve better therapeutic effects for pancreatic cancer, which was worthy of further clinical research in the future.
The pathological analysis of PLX-II revealed that extrapancreatic neuropathy might influence the prognosis in pancreatic cancer. Several studies demonstrated that the peripheral nervous system can be regarded as a neuronal circuit, which connected all body parts and organs to the central nervous system, and the internal organs might associate with tumor microenvironment via the autonomic nerves.9,18,23,24 For instance, autonomic nerve sprouting was essential to prostate cancer progression; sympathetic and parasympathetic nerves were found to be necessary throughout all phases of prostate cancer progression in the mouse.25 Furthermore, the autonomic nerves were also an essential component of tumor microenvironment. By reaching most internal organs, they can arrange tissue homeostasis and promote cancer growth and metastasis.23,26 In our study, the contents of sympathetic and parasympathetic fibers differed significantly among prognostic groups, and the phenomenon could be regarded as neural remodeling.
Sympathetic and parasympathetic nerves might regulate the tumor through direct innervation and release of neurotransmitters such as catecholamines and acetylcholine.24,26,27 Nerves infiltrated the tumor microenvironment, termed tumor neoneurogenesis or axonogenesis and played an active role in cancer progression such as the tumor growth and dissemination, reciprocally tumor cells drove nerve outgrowth in a cross-talk that contributes to tumor progression.24 The activation of β-adrenergic receptors accelerated pancreatic cancer cell growth and invasion, as nerve fibers can release these neurotransmitters directly into the vicinity of cancer cells to stimulate their survival, proliferation and ability to spread.24,26 This may explain why the early liver metastasis correlated with an apparent distribution of autonomic nerve system in our study. We inferred that neuropathy such as the sympathetic or parasympathetic neurogenesis will allow tumor cells infiltrating the connective tissues, and then resulted in the liver metastasis.
Sympathetic nerve system played an important role in pancreatic carcinoma, for instance, intratumoral parasympathetic neurogenesis correlated with tumor budding.19,28 Although functions of sympathetic and parasympathetic nervous systems are classically in opposition, they are in fact complementary in cancer, where sympathetic nerves stimulate early phases and parasympathetic nerves activate the late metastatic process.15,29 Prostate tumors with infiltration by parasympathetic cholinergic fibers had the tendency of cancer dissemination, and the density of nerves was directly correlated with tumor aggressiveness.25 Accumulating preclinical evidence demonstrates that the seeding of pancreatic cancer cells in distant organs often occurs even before tumor formation at primary site.15 In our study, however, the sympathetic and parasympathetic nervous systems manifested the same function in stimulating the liver metastasis. Patients with autonomic innervation changes presented with early liver metastasis and thus the short overall survival time compared with the patients without extrapancreatic neuropathy.
Early metastasis is responsible for death after surgery, thus providing a rationale for the use of systemic therapy other than first-line surgery for these patients.5,30,31 The theory of nerve–cancer interactions led to innovative anticancer therapies; the denervation treatment was evaluated to slow the progression of the cancer.32 The rationale for neoadjuvant therapy in this setting is thus very strong, including that for the early treatment of potential micrometastatic disease that is responsible for recurrence after surgery, but this needs to be validated in well-designed randomized trials.30,33 Patients with extrapancreatic neuropathy might develop early liver metastasis after radical surgery and be the potential target population for adjuvant hepatic arterial infusion chemotherapy after resection, which might effectively and safely prevent liver metastases and improve the prognosis, although further research is needed to confirm this hypothesis.34
This study has some limitations. Firstly, some patients were lost to follow-up so that the median follow-up time was only 13 months. But we only focused on early recurrence within 6 months in this study, the results were relatively precise. Secondly, we only observed the relationship between extrapancreatic neuropathy of PLX-II and early prognosis, the concrete mechanism that extrapancreatic neuropathy influenced the prognosis was not studied. Lastly, our study was conducted in a single institution and was not a population-based study.
In conclusion, the resectability of pancreatic head adenocarcinoma was mainly based on anatomic extent, and this carried a high risk for early relapse after surgery due to the intrinsic biological features of the tumor. This meant that upfront surgery was the best approach for only a minority of patients. The extrapancreatic neuropathy such as the neurogenesis, the neuritis and the autonomic innervation changes might be an underlying cause of poor prognosis and was a predictive factor of higher risk of liver metastasis. Therefore, the neuropathy of extrapancreatic plexus might correlate with a more aggressive phenotype of pancreatic head adenocarcinoma and might help stratify patients into prognostic subgroups to aid surgeons determining appropriate therapeutic strategies for individual patients.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allen PJ, Kuk D, Castillo CF, et al. Multi-institutional validation study of the American Joint Commission on Cancer (8th Edition) Changes for T and N staging in patients with pancreatic adenocarcinoma. Ann Surg. 2017;265(1):185–191. doi:10.1097/SLA.0000000000001763
2. Ozturk SK, Erden E. Do the well known prognostic parameters in pancreatic ductal adenocarcinoma really reflect survival? Turk Patoloji Derg. 2017;34(2):127–133.
3. Isaji S, Mizuno S, Windsor JA, et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology. 2018;18(1):2–11. doi:10.1016/j.pan.2017.11.011
4. Petrelli F, Inno A, Barni S, et al. Borderline resectable pancreatic cancer: more than an anatomical concept. Digestive Liver Dis. 2017;49(2):223–226. doi:10.1016/j.dld.2016.11.010
5. Groot VP, Rezaee N, Wu W, et al. Patterns, timing, and predictors of recurrence following pancreatectomy for pancreatic ductal adenocarcinoma. Ann Surg. 2018;1:936–945.
6. Ozaki H, Hiraoka T, Mizumoto R, et al. The prognostic significance of lymph node metastasis and intrapancreatic perineural invasion in pancreatic cancer after curative resection. Surg Today. 1999;29(1):16–22. doi:10.1007/BF02482964
7. S Q Y, Miwa K, Ohta T, et al. Innervation of the pancreas from the perspective of perineural invasion of pancreatic cancer. Pancreas. 2003;27(3):225–229. doi:10.1097/00006676-200310000-00005
8. Kayahara M, Nakagawara H, Kitagawa H, et al. The nature of neural invasion by pancreatic cancer. Pancreas. 2007;35(3):218–223. doi:10.1097/mpa.0b013e3180619677
9. Demir IE, Ceyhan GO, Rauch U, et al. The microenvironment in chronic pancreatitis and pancreatic cancer induces neuronal plasticity. Neurogastroenterol Motil. 2010;22(4):
10. Ceyhan GO, Demir IE, Rauch U, et al. Pancreatic neuropathy results in “Neural Remodeling” and altered pancreatic innervation in chronic pancreatitis and pancreatic cancer. Am J Gastroenterol. 2009;104(10):2555–2565. doi:10.1038/ajg.2009.380
11. Zuo H. CT and MR imaging patterns for pancreatic carcinoma invading the extrapancreatic neural plexus (Part I): anatomy, imaging of the extrapancreatic nerve. World J Radiol. 2012;4(2):36. doi:10.4329/wjr.v4.i2.36
12. Isaji S, Kishiwada M, Kato H. Surgery for borderline resectable pancreatic cancer: the Japanese experience. Multimodality Management of Borderline Resectable Pancreatic Cancer. Springer, Cham, 2016: 265–287. doi:10.1007/978-3-319-22780-1_17.
13. Mitsunaga S, Hasebe T, Kinoshita T, et al. Detail histologic analysis of nerve plexus invasion in invasive ductal carcinoma of the pancreas and its prognostic impact. Am J Surg Pathol. 2007;31(11):1636–1644. doi:10.1097/PAS.0b013e318065bfe6
14. Patel BN, Giacomini C, Jeffrey RB, et al. Three-dimensional volume-rendered multidetector CT imaging of the posterior inferior pancreaticoduodenal artery: its anatomy and role in diagnosing extrapancreatic perineural invasion. Cancer Imaging. 2013;13(4):580–590. doi:10.1102/1470-7330.2013.0051
15. Stopczynski RE, Normolle DP, Hartman DJ, et al. Neuroplastic changes occur early in the development of pancreatic ductal adenocarcinoma. Cancer Res. 2014;74(6):1718–1727. doi:10.1158/0008-5472.CAN-13-2050
16. Saloman JL, Albers KM, Rhim AD, et al. Can stopping nerves, stop cancer? Trends Neurosci. 2016;39(12):880–889. doi:10.1016/j.tins.2016.10.002
17. Demir IE, Friess H, Ceyhan GO. Neural plasticity in pancreatitis and pancreatic cancer. Nat Rev Gastroenterol Hepatol. 2015;12(11):649–659. doi:10.1038/nrgastro.2015.166
18. Ceyhan GO, Demir IE, Maak M, et al. Fate of nerves in chronic pancreatitis: neural remodeling and pancreatic neuropathy. Best Pract Res Clin Gastroenterol. 2010;24(3):311–322. doi:10.1016/j.bpg.2010.03.001
19. Zhang L, Guo L, Tao M, et al. Parasympathetic neurogenesis is strongly associated with tumor budding and correlates with an adverse prognosis in pancreatic ductal adenocarcinoma. Chin J Cancer Res. 2016;28(2):180–186. doi:10.21147/j.issn.1000-9604.2016.02.05
20. Jamieson NB, Mohamed M, Oien KA, et al. The relationship between tumor inflammatory cell infiltrate and outcome in patients with pancreatic ductal adenocarcinoma. Ann Surg Oncol. 2012;19(11):3581–3590. doi:10.1245/s10434-012-2370-y
21. Rhim AD, Mirek ET, Aiello NM, et al. EMT and dissemination precede pancreatic tumor formation. Cell. 2012;148(1–2):349–361. doi:10.1016/j.cell.2011.11.025
22. Sugimoto M, Mitsunaga S, Yoshikawa K, et al. Prognostic impact of M2 macrophages at neural invasion in patients with invasive ductal carcinoma of the pancreas. Eur J Cancer. 2014;50(11):1900–1908. doi:10.1016/j.ejca.2014.04.010
23. Kiba T. Relationships between the autonomic nervous system and the pancreas including regulation of regeneration and apoptosis: recent developments. Pancreas. 2004;29(2):e51–e58. doi:10.1097/00006676-200408000-00019
24. Jobling P, Pundavela J, Oliveira SMR, et al. Nerve-cancer cell cross-talk: a novel promoter of tumor progression. Cancer Res. 2015;75(9):1777–1781. doi:10.1158/0008-5472.CAN-14-3180
25. Magnon C, Hall SJ, Lin J, et al. Autonomic nerve development contributes to prostate cancer progression. Science. 2013;341(6142):1236361. doi:10.1126/science.1236361
26. Guo K, Ma Q, Li J, et al. Interaction of the sympathetic nerve with pancreatic cancer cells promotes perineural invasion through the activation of STAT3 signaling. Mol Cancer Ther. 2013;12(3):264–273. doi:10.1158/1535-7163.MCT-12-0809
27. Demir IE, Friess H, Ceyhan GO. Nerve-cancer interactions in the stromal biology of pancreatic cancer. Front Physiol. 2012;3:97. doi:10.3389/fphys.2012.00097
28. O’Connor K, Li-Chang HH, Kalloger SE, et al. Tumor budding is an independent adverse prognostic factor in pancreatic ductal adenocarcinoma. Am J Surg Pathol. 2015;39(4):472–478. doi:10.1097/PAS.0000000000000333
29. Ceyhan GO, Demir IE, Altintas B, et al. Neural invasion in pancreatic cancer: a mutual tropism between neurons and cancer cells. Biochem Biophys Res Commun. 2008;374(3):442–447. doi:10.1016/j.bbrc.2008.07.035
30. Felice DE, Musio F, Raffetto DN, et al. Neoadjuvant strategy as initial treatment in resectable pancreatic cancer: concrete evidence of benefit. Anticancer Res. 2014;34(9):4673–4676.
31. Yamada S, Fujii T, Takami H, et al. Evaluation and proposal of novel resectability criteria for pancreatic cancer established by the Japan Pancreas Society. Surgery. 2017;162(4):784–791. doi:10.1016/j.surg.2017.04.023
32. Saloman JL, Albers KM, Li D, et al. Ablation of sensory neurons in a genetic model of pancreatic ductal adenocarcinoma slows initiation and progression of cancer. Proc Natl Acad Sci U S A. 2016;113(11):3078–3083. doi:10.1073/pnas.1512603113
33. Sinn M, Bahra M, Denecke T, et al. Perioperative treatment options in resectable pancreatic cancer - how to improve long-term survival. World J Gastrointest Oncol. 2016;8(3):248. doi:10.4251/wjgo.v8.i3.248
34. Kurosaki I, Kawachi Y, Nihei K, et al. Liver perfusion chemotherapy with 5-Fluorouracil followed by systemic gemcitabine administration for resected pancreatic cancer: preliminary results of a prospective phase 2 study. Pancreas. 2009;38(2):161–167. doi:10.1097/MPA.0b013e31818815f7
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.