Back to Journals » International Medical Case Reports Journal » Volume 17
Extracorporeal Membrane Oxygenation (ECMO)-Assisted Tracheostomy in a Patient with a “Woody Neck” Due to Radiation Therapy and Complicated by Bilateral Internal Jugular Vein Occlusion: A Case Report
Authors Bales T, Hamid A, Fadumiye CO ![]()
Received 25 February 2024
Accepted for publication 20 July 2024
Published 6 August 2024 Volume 2024:17 Pages 739—744
DOI https://doi.org/10.2147/IMCRJ.S465848
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xudong Zhu
Travis Bales,1,* Abdulaziz Hamid,2,* Christopher O Fadumiye1
1Department of Anesthesiology, Medical College of Wisconsin, Milwaukee, WI, USA; 2Medical College of Wisconsin, Milwaukee, WI, USA
*These authors contributed equally to this work
Correspondence: Christopher O Fadumiye, Department of Anesthesiology, Medical College of Wisconsin, 8701 Watertown Plank Road, Milwaukee, WI, 53226, USA, Email [email protected]
Abstract: Radiation for head and neck cancer (HNC) can lead to neck fibrosis, commonly known as “woody neck”, limiting neck mobility. We report the case of a 46-year-old male with a history of tonsillar squamous cell carcinoma, with a “woody neck” following multiple radiation treatments. Facial swelling and impending airway loss prompted emergent intubation. Despite nasotracheal tube placement, bilateral internal jugular vein occlusion led to a difficult tracheostomy. An airway exchange catheter (AEC) facilitated multiple attempts at tracheal cannulation, but due to challenging anatomy, prolonged nasotracheal intubation was maintained. Tracheostomy was attempted again with extracorporeal membrane oxygenation (ECMO) support, which resulted in successful tracheal cannulation.
Keywords: case report, head and neck cancer, “woody neck”, neck fibrosis, extracorporeal membrane oxygenation
Introduction
Head and neck cancer (HNC) consists of tumors in the lip, oral cavity, salivary glands, pharynx (including the oropharynx, nasopharynx, and hypopharynx), and larynx. The oropharynx, the middle component of the pharynx, consists of the soft palate, the base of the tongue, and the tonsils.1 Globally, HNC ranks as the sixth most common cancer, with over 940,000 new cases and 480,000 deaths in 2022.2 In the United States, there were approximately 71,100 newly diagnosed HNC cases and 16,110 deaths in 2024.3 The treatment of HNC, including tonsillar carcinoma, depends on factors such as the type, stage, and location of the cancer. Treatment for HNC includes chemotherapy, surgery, radiation, or a combination of these methods.1
Radiation can result in several physiologic and anatomic changes that must be assessed prior to anesthesia. Among these changes, the development of radiation fibrosis syndrome is particularly significant. Radiation fibrosis syndrome, which develops as a clinical manifestation of radiation fibrosis (RF), can involve any part of the neuromuscular system and visceral organs. Radiation fibrosis syndrome can result in clinical symptoms within months or years after treatment, depending on the specific tissue involved.4 There are three stages of RF that can be found across a multitude of cases: the pre-fibrotic phase, the constitutive fibrotic phase, and the late fibroatrophic phase.5 The pre-fibrotic phase occurs in the first few months after RT and is often asymptomatic, although it may present with signs of nonspecific chronic local inflammation.5 This is followed by the constitutive organized fibrotic phase, which occurs during the first few years after RT. This phase is characterized by the disappearance of inflammation signs, with tissues becoming thickened and hardened, and the presence of irregular widened capillaries, such as telangiectasia.5 The last phase is the late fibroatrophic phase, which can last from 5 to 30 years after RT. This phase involves retractile atrophy and the gradual destruction of normal tissues within the irradiated area.5 As radiation therapy-induced neck fibrosis is progressive and presents challenges in managing airway complications, understanding these stages is vital.
Treatment of HNC with radiation can lead to a “woody neck”, characterized by fibrosis in both the skin and underlying tissue.6 Radiation to the neck can limit neck mobility, a common side effect which makes securing the airway challenging.7 This case report describes the successful management of a difficult airway in a patient with prior neck radiation and bilateral internal jugular vein occlusion with extracorporeal membrane oxygenation (ECMO).
Case Description
A 46-year-old male with history of tonsillar squamous cell carcinoma status post multiple radiation treatments to the neck resulting in significant fibrosis described as “woody neck” presented with facial swelling. At presentation, he had difficulty speaking, limited ability to open his mouth, a fixed, flexed neck, and impending airway loss. He was treated with racemic epinephrine, steroids, and an antihistamine before being brought to the operating room (OR) for emergent intubation.
Following induction with ketamine, dexmedetomidine, and midazolam, an airway was established by placing a nasotracheal tube with a fiber optic scope. The patient was admitted to the intensive care unit (ICU) in stable condition. Evaluation revealed bilateral internal jugular vein occlusions (Figure 1) as the most likely etiology of his facial swelling. The patient’s internal jugular veins were not amenable to endovascular repair, thus a definitive airway via tracheostomy (Figure 2) became necessary.
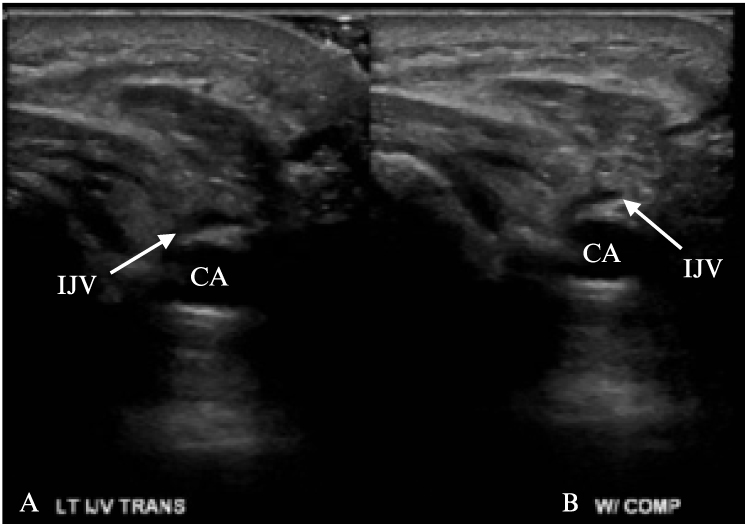 |
Figure 1 Transverse ultrasound image of left IJV obliteration with and without compression. (A) Before compression with ultrasound probe. (B) After compression. There is only a slight change in the IJV, demonstrating the severity of the occlusion. Abbreviations: CA, carotid artery; IJV, internal jugular vein. |
 |
Figure 2 CT scan following admission and 1st intubation in OR. |
The patient was again brought to the OR and induced without any incidence. An 11 French airway exchange catheter (AEC) was passed through the endotracheal tube in anticipation of difficulty with reintubation. The dissection of the trachea was challenging due to the severe, fixed flexion of the neck. Once the trachea was opened, attempts at tracheal cannulation were unsuccessful despite multiple maneuvers and trials of device types. The AEC allowed for re-advancement of the endotracheal tube between attempts and prolonged attempts via passive oxygenation. However, due to the extremely challenging anatomy there was not enough apnea time to fully evaluate the problem. Therefore, the patient was kept nasotracheally intubated and returned to the ICU. A discussion was held with the patient about a second tracheostomy attempt with ECMO to which he agreed.
Again, the patient was brought to the OR and induced without any complications. His femoral vessels were cannulated for ECMO without issue. He did not require support from the ventilator and thus the airway was free to allow a more extensive dissection. Tracheal cannulation was successful. ECMO was discontinued in the OR uneventfully and the patient returned to the ICU with minimal ventilator support. He was discharged home two weeks later.
Discussion
In this case report, we report a patient with a failed tracheostomy with prior neck radiation. The treatment of HNC generally consists of surgery, chemotherapy, and/or radiation therapy.1 Patients with HNC can have airway distortion due to tumor growth and surgery.8 Furthermore, radiation can cause airway and physiological changes, leading to complications such as pharyngoesophageal stenosis, lymphedema, hypothyroidism, osteoradionecrosis, an elevated risk of dental caries, and fibrosis.7,9 Radiation-induced neck fibrosis can manifest as a woody texture, often referred to as “woody neck”, resulting in restricted neck mobility and limited extension.7 This condition can pose challenges for anesthesiologists, particularly in managing the airways of cancer patients, including difficulties with mask ventilation, laryngoscopy, intubation, bleeding, and dislodgment of teeth.9 The incidence of a difficult airway is estimated to be 50% in patients with prior head and neck radiation.10 Therefore, anesthesiologists should consider neck radiation history when managing airway access in patients with prior head and neck radiation.
AEC plays an important role in airway management, providing benefits in cases of anticipated difficult reintubation and facilitating oxygenation. The AEC is inserted through an existing endotracheal tube before extubation, and serves as a conduit for passive oxygenation, manual ventilation, insufflation, or jet ventilation-administered oxygenation.11,12 Moreover, the AEC acts as a stylet to facilitate repeated intubation.11,12 However, AEC does have associated risks, including the potential for barotrauma, bronchial perforation, and no guarantee of success if the endotracheal tube cannot pass over the AEC.11,12 In high-risk patients, it is prudent to consider ECMO cannulation before airway manipulation to prevent airway loss. ECMO facilitates airway access by allowing nearly indefinite absence of ventilation and removing support devices from the surgical field. ECMO has demonstrated success in airway procedures for obstructing tumors, tracheal stenosis, and mediastinal masses.13 However, to our knowledge “woody neck” alone has not been described as an instance of ECMO-assisted tracheostomy. With the airway free and oxygenation independent of the patient’s ventilation, the operation can proceed uninterrupted.
In our case report, femoral-femoral veno-venous-ECMO (VV-ECMO), was utilized to maintain stable oxygenation and ventilation, allowing for a controlled environment to perform the tracheostomy. ECMO is indicated in patients with reversible respiratory failure who do not respond to mechanical ventilation or medical treatment.14
VV-ECMO involves draining blood from the right atrium or superior and inferior vena cava and returning it to the right atrium. This method positions the artificial lung in series with the patient’s normal lungs, allowing oxygenated blood from the ECMO circuit to mix with the native venous return.14 This arterial blood, consisting of a mix of oxygen-rich extracorporeal and oxygen-poor native venous blood, provides adequate oxygen to support metabolic activity. During extracorporeal gas exchange, this method maintains the patient’s own hemodynamics, thus maintaining cardiac output and vascular resistance, which allows for the management of the airway at rest.14
By providing continuous respiratory support, VV-ECMO reduces the need for repeated intubation attempts, minimizing the risk of additional trauma and complications associated with intubation. Physiological support provided by VV-ECMO is crucial in managing difficult airway cases, which highlights its value in aiding tracheostomy procedures in patients with severe neck fibrosis.
Moreover, in other studies, VV-ECMO has also been demonstrated to be effective in managing difficult airways. In one study, VV-ECMO was utilized in the endoscopic treatment of severe benign airway stenosis in a patient unable to tolerate standard ventilation.15 In this study, a 68-year-old male with esophageal cancer was treated with radiation therapy who developed severe cervical tracheal stenosis.15 VV-ECMO was used to maintain adequate oxygenation and to secure the airway. The study also included a literature review that found that ECMO was important in maintaining oxygenation in nine of the 14 patients with various types of cancer.15 This study demonstrates the importance of ECMO in managing airway emergencies.
To our knowledge, incidence rates for “woody neck” resulting from radiation-induced neck fibrosis and internal jugular vein (IJV) occlusion are not widely documented in the literature. This case report addresses this research gap in HNC patients treated with radiation therapy. One limitation of this study is the paucity of literature available for the comparison of management approaches. However, a strength of this case report is the positive outcome achieved through ECMO, demonstrating its role in facilitating prolonged attempts and increasing apnea time for evaluating and addressing challenging tracheal anatomy. These findings provide insights into managing severe airway complications in similar cases in the future.
The ABC classification is a woody hardness classification that provides a framework to describe varying degrees of indurated edema and neck fibrosis secondary to radiation therapy or long-standing pathology.6 This classification system aims to characterize the severity of “woody neck”. The system is based on the hardness of wood from three distinct types of trees. Classification A is extreme woody hardness represented by African Ebony wood, classification B is moderate woody hardness represented by Birch wood, and classification C is mild woody hardness represented by Chestnut wood.6
One study was conducted to assess the clinical utility of the ABC classification in predicting outcomes for patients undergoing salvage laryngectomy after radiation therapy.16 The study included 51 patients categorized into one of the three ABC classifications. One patient in Class A, 30 patients in Class B, and 20 patients in Class C. The primary outcome was the development of pharyngoesophageal strictures. Although statistical significance was not consistently reached, woody hardness was associated with pharyngoesophageal stricture development.16 Interestingly, when cancer diagnosis (squamous cell carcinoma) was controlled, the time to event analysis showed a statistically significant association between higher woody hardness (Class A and B) and time to stricture.16 The study suggests that the ABC classification can be used to predict the formation of pharyngoesophageal strictures in salvage laryngectomy patients, which could guide prevention measures.16
To the best of our knowledge, no study has examined the utility of the ABC classification in HNC patients who have undergone radiation treatment and received anesthesia, which underscores a crucial gap in our understanding of its potential application. Considering the challenges associated with radiation-induced neck fibrosis during anesthesia, incorporating ABC classification might be beneficial. The ABC classification may offer valuable insights into predicting difficult airways in anesthesia patients. The ABC classification may also assist anesthesiologists in anticipating and preparing for the challenges associated with airway management in cases of radiation therapy-induced “woody necks”. Therefore, it is crucial to explore the relationship between woody hardness classification and difficult airway situations, to improve the safety and effectiveness of anesthesia for HNC patients with neck fibrosis after radiation therapy.
Ultrasonography can help anesthesiologists anticipate and prepare for potential difficulties in patients with HNC who have developed neck fibrosis due to radiation therapy. Ultrasonography can be a less intrusive, cost-effective option for managing airway-related conditions non-invasively.17 One study during the SARS-CoV-2 pandemic noted that ultrasonographic imaging of the larynx is often overlooked due to CT and MRI accessibility.17 In emergency situations, ultrasonography can be integrated into Focused Assessment With Sonography in Trauma protocols to determine whether neck trauma has occurred. Since it is non-radiating and allows serial real-time monitoring, ultrasonography can be an ideal choice for obtaining further diagnostic information.17 For complex cancer cases, ultrasonography can potentially enhance airway management safety and success. Ultrasound-guided procedures, such as percutaneous tracheostomy, allow precise and safe tracheal access which can be crucial in emergency settings.17 By utilizing ultrasonography, anesthesiologists can improve patient outcomes through more effective and targeted airway management strategies in these challenging cases.
Furthermore, our case report emphasizes the importance of a multidisciplinary approach to managing HNC patients who have undergone radiation therapy. It is crucial for otolaryngologists, oncologists, radiologists, anesthesiologists, and others to collaborate to develop a comprehensive treatment plan for HNC patients. This multidisciplinary approach ensures that all aspects of the patient’s condition are taken into consideration, contributing to more effective and coordinated care.18–20 This case demonstrates how a multidisciplinary team can successfully navigate the complexities of airway management in patients with “woody neck”.
Conclusion
This case report emphasizes the importance of a multidisciplinary approach to managing a challenging airway in patients with “woody neck” following radiation therapy to the neck. Anesthesiologists should consider a patient’s history of neck radiation when administering anesthesia and anticipate difficulties with the airway when prior neck radiation is present. There should be a low threshold for placing an AEC, however potential complications should be considered. Lastly, ECMO can be an alternative option to manage difficult airways due to “woody neck”.
Abbreviations
AEC, airway exchange catheter; CA, carotid artery; ECMO, extracorporeal membrane oxygenation; HNC, head and neck cancer; ICU, intensive care unit; IJV, internal jugular vein; OR, operating room; RF, radiation fibrosis; VV-ECMO, veno-venous-ECMO.
Consent for Publication
This case report is devoid of patient identifiable information, it is exempt from IRB review requirements as per the Medical College of Wisconsin policy. Informed consent was obtained for the publication of the case. This article adheres to the applicable CAse REport (CARE) guidelines.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Referenced with permission from the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Version 4.2024. © National Comprehensive Cancer Network, Inc; 2024. All rights reserved. Accessed June 29, 2024. To view the most recent and complete version of the guideline, go online to NCCN.org.
2. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
3. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
4. Stubblefield MD. Clinical evaluation and management of radiation fibrosis syndrome. Phys Med Rehabilit Clin North Am. 2017;28(1):89–100. doi:10.1016/j.pmr.2016.08.003
5. Delanian S, Lefaix JL. The radiation-induced fibroatrophic process: therapeutic perspective via the antioxidant pathway. Radiother Oncol. 2004;73(2):119–131. doi:10.1016/j.radonc.2004.08.021
6. Colbert SD, Mitchell DA, Brennan PA. Woody hardness - A novel classification for the radiotherapy-treated neck. Br J Oral Maxillofac Surg. 2015;53(4):380–383. doi:10.1016/j.bjoms.2015.02.019
7. Brook I. Late side effects of radiation treatment for head and neck cancer. Radiat Oncol J. 2020;38(2):84–92. doi:10.3857/roj.2020.00213
8. Zheng G, Hagberg CA. Management of airway in the cancer patients. In: Nates JL, Price KJ, editors. Oncologic Critical Care. Springer International Publishing; 2020:1557–1569.
9. Balakrishnan M, Kuriakose R, Koshy RC. Radiation induced changes in the airway—anaesthetic implications. South Afr J Anaesth Anal. 2004;10(2):19–21. doi:10.1080/22201173.2004.10872356
10. Jain D, Khan Joad AS. Head and neck radiotherapy - a risk factor for anaesthesia? Indian J Anaesth. 2020;64(6):488–494. doi:10.4103/ija.IJA_864_19
11. Benumof JL. Airway exchange catheters: simple concept, potentially great danger. Anesthesiology. 1999;91(2):342–344. doi:10.1097/00000542-199908000-00005
12. Duggan LV, Law JA, Murphy MF. Brief review: supplementing oxygen through an airway exchange catheter: efficacy, complications, and recommendations. Can J Anaesth. 2011;58(6):560–568. doi:10.1007/s12630-011-9488-4
13. Bozer J, Vess A, Pineda P, et al. Venovenous extracorporeal membrane oxygenation for a difficult airway situation-a recommendation for updating the American Society of Anesthesiologists’ “Difficult Airway Algorithm”. J Cardiothorac Vasc Anesth. 2023;37(12):2646–2656. doi:10.1053/j.jvca.2023.04.027
14. Banfi C, Pozzi M, Siegenthaler N, et al. Veno-venous extracorporeal membrane oxygenation: cannulation techniques. J Thoracic Dis. 2016;8(12):3762–3773. doi:10.21037/jtd.2016.12.88
15. Liang Y, Zhu J, Zheng X, et al. Application of extracorporeal membrane oxygenation in the endoscopic treatment of severe benign airway stenosis: a case report and literature review. Laparosc Endosc Robotic Surg. 2021;4(2):48–52. doi:10.1016/j.lers.2021.04.002
16. Djabali EJ, Rotter J, Chheda NN, et al. Woody hardness classification impact on salvage laryngectomy functional outcomes. Am J Otolaryngol. 2021;42(3):102877. doi:10.1016/j.amjoto.2020.102877
17. Cergan R, Dumitru M, Vrinceanu D, Neagos A, Jeican II, Ciuluvica RC. Ultrasonography of the larynx: novel use during the SARS-CoV-2 pandemic (Review). Exp Ther Med. 2021;21(3):273. doi:10.3892/etm.2021.9704
18. Lo Nigro C, Denaro N, Merlotti A, Merlano M. Head and neck cancer: improving outcomes with a multidisciplinary approach. Cancer Manag Res. 2017;9:363–371. doi:10.2147/CMAR.S115761
19. Bossi P, Alfieri S. The benefit of a multidisciplinary approach to the patient treated with (Chemo) radiation for head and neck cancer. Curr Treat Options Oncol. 2016;17(10):53. doi:10.1007/s11864-016-0431-3
20. De Felice F, Tombolini V, de Vincentiis M, et al. Multidisciplinary team in head and neck cancer: a management model. Med Oncol. 2018;36(1):2. doi:10.1007/s12032-018-1227-z
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.