Back to Journals » International Journal of Nanomedicine » Volume 21
Extracellular Vesicles for Therapeutic Applications: A Translational Framework Integrating Sources, Administration Routes, Indications, Quality Control, and Regulatory Systems
Authors Zhang F ![]() , Xing L, Chu W, Wang Q, Sun H, Liu Y, An G, Liang X
, Xing L, Chu W, Wang Q, Sun H, Liu Y, An G, Liang X ![]()
Received 6 May 2026
Accepted for publication 15 June 2026
Published 26 June 2026 Volume 2026:21 622474
DOI https://doi.org/10.2147/IJN.S622474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. RDK Misra
Fen Zhang,1,* Lan Xing,1,* Wanglong Chu,1 Qingfang Wang,1 Haojie Sun,1 Yajun Liu,1 Gang An,2 Xiao Liang1
1Cell Preparation Center, Shenzhen Beike Biotechnology Co., Ltd., Shenzhen, Guangdong, People’s Republic of China; 2Fujian Branch, National Engineering Research Center of Foundational Technologies for CGT Industry, Fuzhou, Fujian, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Gang An, Fujian Branch, National Engineering Research Center of Foundational Technologies for CGT Industry, Fuzhou, Fujian, People’s Republic of China, Email [email protected] Xiao Liang, Shenzhen Beike Biotechnology Co., Ltd., Shenzhen, Guangdong, 518000, People’s Republic of China, Email [email protected]
Abstract: Extracellular vesicles (EVs) are nanoscale membranous vesicles that mediate intercellular communication via the transport of bioactive cargos. With context-dependent intrinsic targeting, source- and cargo-dependent favorable biocompatibility and loading capacity, EVs represent promising acellular therapeutic platforms with context-dependent translational potential. However, their clinical application is hindered by source-associated functional heterogeneity, unclear matching relationships between administration routes and disease indications, as well as imperfect quality control specifications and fragmented global regulatory frameworks alongside insufficient clinical trial data. This review systematically summarizes the biological features of EVs originating from mesenchymal stem cells, immune cells, tumor cells, plants, milk, microbes and platelets, and compares the pros and cons and applicable scenarios of intravenous, oral, nasal, inhaled, and multiple local injection delivery modalities. We further recapitulate the research progress of EV therapeutics across regenerative medicine, immunotherapy, oncology, neurological and metabolic disorders, and analyze worldwide regulatory policies while sorting out the up-to-date industrial-sponsored global clinical pipeline updated to April 2026. Centered on a core five-dimensional matching framework integrating EV sources, administration routes, disease indications, critical quality attributes (CQAs) and global regulatory requirements, this work elaborates current translational bottlenecks and commercialization obstacles of EV products. This review provides theoretical support for precision EV therapy optimization, unified quality criterion establishment, international regulatory coordination and accelerated clinical and industrial transformation of EV-based medicines. The diagram outlines a framework for using extracellular vesicles (EVs) in therapy, detailing sources, administration methods and therapeutic uses. EVs originate from mesenchymal stem cells, immune cells, tumor cells, edible plants, microbes, bovine milk and others like platelets and neural stem cells. Engineering modifications include gene and targeting ligand modifications and drug loading. Administration is categorized into systemic (intravenous, oral), non-invasive local (nasal, aerosol) and invasive local (subcutaneous, intravitreal, intrathecal, intra-articular, intraperitoneal) methods. Therapeutic uses cover tissue repair, immune regulation, tumor therapy, neurological and metabolic diseases and others such as intervertebral disc degeneration, bone regeneration, anti-infection, respiratory and eye diseases.A translational framework for extracellular vesicles: sources, administration routes and therapeutic applications.
Keywords: extracellular vesicles, source heterogeneity, administration route, precision therapy, clinical translation, regulatory specification
Introduction
Extracellular vesicles (EVs) are lipid bilayer-delimited nanoparticles actively released by all living cells. Based on biogenesis, size, and molecular profiles, EVs comprise multiple subsets including exosomes (endosome-derived EVs), microvesicles, and apoptotic bodies.1 By shuttling proteins, nucleic acids, lipids, and other bioactive cargos between cells, EVs govern intercellular communication and modulate a wide array of physiological and pathological processes, ranging from immune regulation and tissue repair to tumor progression and metabolic disturbance.2 Accordingly, EVs have emerged as a transformative class of diagnostic biomarkers and cell-free therapeutic agents with enormous clinical potential.
EVs were first observed in sheep reticulocytes in 1983 but were long dismissed as metabolic waste.3,4 The field expanded dramatically from the early 2000s onward, driven by innovations in isolation and purification methods (eg., ultracentrifugation, density gradient separation, ultrafiltration, microfluidics) and high-resolution omics tools (eg., proteomics, high-throughput sequencing). To promote global standardization, the International Society for Extracellular Vesicles (ISEV) has established the Minimal Information for Studies of Extracellular Vesicles (MISEV) guidelines, which unify EV definition, classification, experimental reporting, and quality control.5 Among EV subtypes, exosomes (30–150 nm, endosome-derived, positive for CD63, TSG101, CD9, and CD81) remain the most extensively investigated EV subset.
Three inherent properties underpin the high clinical translatability of EVs: they are produced by nearly all cell types with distinct parent-cell specificity, making them promising diagnostic biomarkers; their natural phospholipid bilayer protects cargos from enzymatic degradation, affords excellent biocompatibility and barrier-crossing capacity, qualifying them as ideal drug delivery vehicles; and they can be delivered via versatile routes that directly shape their in vivo biodistribution, targeting efficiency, and indication compatibility.6,7 Despite growing translation into clinical trials, several critical bottlenecks persist: marked functional heterogeneity among EVs from different cellular sources; incomplete understanding of their therapeutic mechanisms; unvalidated correlations between EV sources, administration routes, and disease indications; lack of scalable and standardized manufacturing; insufficient quality control systems; and an incomplete and fragmented global regulatory framework.8
This work was performed as a systematic review. Literature searches were conducted in three core databases including PubMed, Web of Science Core Collection and Scopus, using keywords such as extracellular vesicles, exosomes, source heterogeneity and administration route. The retrieval deadline was April 30, 2026. We included peer-reviewed original studies and authoritative reviews, and excluded non-peer-reviewed conference abstracts, preprints, and researches that only focused on diagnostic applications.
Against this background, this review provides a comprehensive and systematic overview of the biological characteristics and functional differences of EVs derived from multiple sources, including mesenchymal stem cells, immune cells, tumor cells, plants, milk, microorganisms, and platelets. We compare the strengths, limitations, and clinical scenarios of major delivery routes, including intravenous, oral, subcutaneous, nasal, inhaled, intrathecal, intraocular, intra-articular, and intraperitoneal administration. We then synthesize preclinical and clinical advances of EVs in tissue repair and regeneration, immune modulation, oncotherapy, neurological disorders, metabolic diseases, and other conditions. We further analyze the global regulatory frameworks and summarize the current global clinical landscape of industry-sponsored EV therapeutic products entering registered trials or regulatory review.
Distinguished from prior reviews that provide only fragmented or descriptive overviews, this review systematically consolidates the interrelationships among EV sources, administration routes and disease indications, and forms a translational framework that integrates quality control requirements and global regulatory systems. It also presents the updated global industrial EV clinical pipeline up to April 2026, compares regulatory discrepancies across major regions in depth, and puts forward targeted reflections for overcoming core translational hurdles, thereby offering distinct incremental value for the field.
By integrating these dimensions, this review aims to clarify the core principle of precise matching among source characteristics, administration routes, and therapeutic indications, in order to furnish a robust theoretical foundation and evidence-based reference for optimizing EV-directed precision therapy, establishing standardized quality control, promoting ongoing efforts toward global regulatory harmonization, and accelerating clinical translation.
Biological Characteristics of Extracellular Vesicles from Different Sources
On the basis of the above overview of EV basic properties, this section systematically elaborates the biological characteristics of EVs from diverse sources and their source-dependent functional heterogeneity.
Mesenchymal Stem Cell-Derived Extracellular Vesicles
Mesenchymal stem cells (MSCs) are mesoderm-derived adult stem cells with self-renewal and multilineage differentiation potential, obtainable from bone marrow, umbilical cord, adipose tissue, and other vascularized tissues. Mounting evidence demonstrates that the therapeutic effects of MSCs in tissue repair and immunomodulation are largely attributed to paracrine signaling, in which mesenchymal stem cell-derived EVs (MSC-EVs) serve as the primary functional carriers.9
MSC-EVs recapitulate the key bioactivities of parental MSCs, including tissue regeneration, immunoregulation, and anti-inflammation, while eliminating the safety risks associated with living cell therapy such as abnormal proliferation and ectopic differentiation.10 Mechanistically, MSC-EVs suppress pro-inflammatory M1 macrophage polarization, promote anti-inflammatory M2 macrophage polarization, modulate CD4+ T-cell differentiation, inhibit target cell apoptosis, enhance proliferation, and facilitate angiogenesis and extracellular matrix (ECM) remodeling to accelerate tissue reconstruction.11
Molecularly, MSC-EVs express canonical EV markers (CD9, CD63, CD81, CD107) and MSC-specific surface antigens (CD29, CD44, CD73, CD90, CD105, CD117).12 Importantly, MSC-EVs display source-dependent molecular and functional heterogeneity. Adipose-derived MSC-EVs are enriched in proteins involved in tissue repair and inflammation regulation, whereas bone marrow-derived MSC-EVs preferentially express factors related to osteogenesis and angiogenesis.13
Accordingly, MSC-EVs from distinct tissues show divergent therapeutic preferences, where umbilical cord-derived MSC-EVs are extensively investigated for type 2 diabetes mellitus (T2DM) and diabetic complications by preserving β-cell function, restoring insulin sensitivity, and promoting diabetic wound healing,14–16 while adipose-derived MSC-EVs exhibit preclinical efficacy in osteoarthritis (OA) by enhancing collagen synthesis, repairing ECM, and attenuating synovial inflammation.17,18
Immune Cell-Derived Extracellular Vesicles
Immune cells are the core effector populations of innate and adaptive immunity and major EV producers. Immune cell-derived EVs (IC-EVs) exhibit functional heterogeneity and bidirectional immunomodulatory effects, determined by parental cell subtype, activation state, and microenvironmental context. Major immune lineages, including T cells, B cells, natural killer (NK) cells, dendritic cells (DCs), macrophages, and neutrophils, can secrete EVs with specialized immunoregulatory activities.19 IC-EVs stably retain source-derived membrane proteins, cytokines, and microRNAs (miRNAs); their phospholipid bilayer protects cargos from circulation degradation, enabling tuned immune regulation in infection, cancer, and autoimmune diseases.20
As a core population of antigen-presenting cells, DC-derived EVs carry major histocompatibility complex (MHC) molecules and costimulatory molecules from the surface of parental cells, enabling direct antigen presentation to T cells, efficient activation of naive T cells, and initiation and regulation of specific adaptive immune responses.21 NK cell-derived EVs are the most extensively studied innate immune subset, which are armed with perforin, granzyme, granulysin, FasL, and TRAIL, enabling direct and potent cytotoxicity against breast cancer, melanoma, and hematological malignancies through multiple mechanisms.22,23
Tumor Cell-Derived Extracellular Vesicles
Tumor cell-derived extracellular vesicles (TEVs) are actively secreted by cancer cells and inherit the specific molecular signatures of parental tumor cells, acting as critical communicators in the tumor microenvironment (TME). TEVs are enriched with three major classes of tumor-specific components: tumor-associated membrane and soluble proteins, tumor-specific antigens and neoepitopes, and oncogenic nucleic acids including mutated genes, miRNAs (microRNA), long non-coding RNAs (lncRNAs), and circular RNA (circRNAs).24 Through paracrine and endocrine signaling, TEVs regulate nearly all hallmarks of cancer, including proliferation, invasion, angiogenesis, immune suppression, chemoresistance, and the formation of pre-metastatic niches, thereby reshaping local and systemic tumor-promoting microenvironments.25,26
Owing to their high stability in biofluids and disease-specific molecular profiles, TEVs represent ideal candidates for liquid biopsy. They exhibit great clinical value in early cancer detection, molecular subtyping, therapeutic monitoring, and prognostic assessment.27,28 In addition, TEVs can be developed as tumor vaccines or targeted delivery vehicles, providing a flexible platform for precision cancer immunotherapy and drug delivery.
Plant-Derived Extracellular Vesicles
Plant-derived EVs (PDEVs) are nanosized vesicles secreted by plant cells, with a typical lipid bilayer structure and a diameter of 30–200 nm. They can be reliably isolated from numerous edible plants including ginger, grape, grapefruit, and broccoli, and possess exceptional stability in the gastrointestinal tract, low immunogenicity, and excellent biosafety, supporting oral administration feasibility.29,30 PDEVs exert intrinsic anti-inflammatory, antioxidant, antitumor, and regenerative activities mainly by inhibiting the nuclear factor-kappa B (NF-κB) pathway, reducing oxidative stress, inducing ROS-dependent tumor cell apoptosis, and blocking cell cycle progression.31–34
Beyond direct therapeutic effects, PDEVs represent promising natural carriers for drug delivery. Compared with synthetic liposomes, PDEVs display lower immunogenicity and higher biocompatibility, and can function across species. Compared with mammalian EVs, they are more cost-effective and scalable. PDEVs can efficiently load chemotherapeutic agents, proteins, and nucleic acids via electroporation or co-incubation, and targeted modification further enhances lesion accumulation for precise disease intervention.35–37
Microbe-Derived Extracellular Vesicles
Gut microbiota plays a fundamental role in host homeostasis, and microbe-derived extracellular vesicles (MEVs) are key mediators of host-microbe cross-talk. MEVs include outer membrane vesicles (OMVs) from Gram-negative bacteria and cytoplasmic membrane vesicles (CMVs) from Gram-positive bacteria, ranging from 20 to 400 nm, and carry pathogen-specific molecules such as lipopolysaccharide (LPS), peptidoglycan, proteins, and metabolites.38,39 MEVs mediate microbial communication and regulate host physiology by crossing the intestinal barrier and modulating immune cell functions systemically.40
Probiotic-derived MEVs can skew macrophage polarization toward either pro-inflammatory M1 or anti-inflammatory M2 phenotypes in a context-dependent manner, enhance intestinal barrier integrity by upregulating tight junction proteins, and restore gut microbial balance. These properties render MEVs effective in ameliorating inflammatory bowel disease, intestinal barrier dysfunction, and metabolic disorders.41,42 With controllable immunogenicity, MEVs also serve as candidate vaccine carriers and immunomodulators for anti-infective and antitumor applications.
Bovine Milk-Derived Extracellular Vesicles
Milk-derived EVs (M-EVs) are secreted by mammary epithelial cells and immune cells in milk, and are highly abundant in bovine milk. They possess a remarkably diverse molecular cargo including proteins, lipids, mRNAs, and miRNAs, and exhibit extraordinary stability that resists gastric acid, digestive enzymes, and thermal processing. This stability allows M-EVs to bypass intestinal degradation and enter the circulation, overcoming the major limitation of poor oral bioavailability of most mammalian EVs.43,44
M-EVs exert multifaceted biological functions, including promoting immune cell maturation, regulating macrophage and T-cell polarization, maintaining intestinal mucosal integrity, modulating gut microbiota, and participating in neurodevelopment and systemic metabolic regulation. With wide availability, low cost, low immunogenicity, and excellent oral compatibility, M-EVs are promising for oral drug delivery, intestinal immune regulation, and the treatment of metabolic and inflammatory diseases.45,46
Extracellular Vesicles from Other Sources
In addition to the aforementioned sources, several somatic and tissue-specific stem cells also secrete functionally distinct EVs. Platelet-derived EVs (PEVs) are released by resting or activated platelets and are enriched in coagulation factors, growth factors, chemokines, and functional miRNAs, contributing to hemostasis, wound repair, angiogenesis, and tissue regeneration.47–49
Neural stem/progenitor cells (NSCs/NPCs)-derived EVs carry neuron-specific miRNAs and neurotrophic factors, participating in neurogenesis, neural protection, anti-neuroinflammation, and blood-brain barrier (BBB) homeostasis. Importantly, these EVs can effectively cross the BBB, providing a potential delivery strategy for central nervous system (CNS) diseases.50–52 Cardiomyocyte-derived EVs (CM-EVs) harbor cardiac-specific miRNAs and antifibrotic factors, which attenuate myocardial fibrosis by inhibiting fibroblast activation and ECM deposition, thereby preserving cardiac function after injury.53
The diverse sources and biological characteristics of EVs are illustrated in Figure 1 and systematically compared across different sources in Table 1.
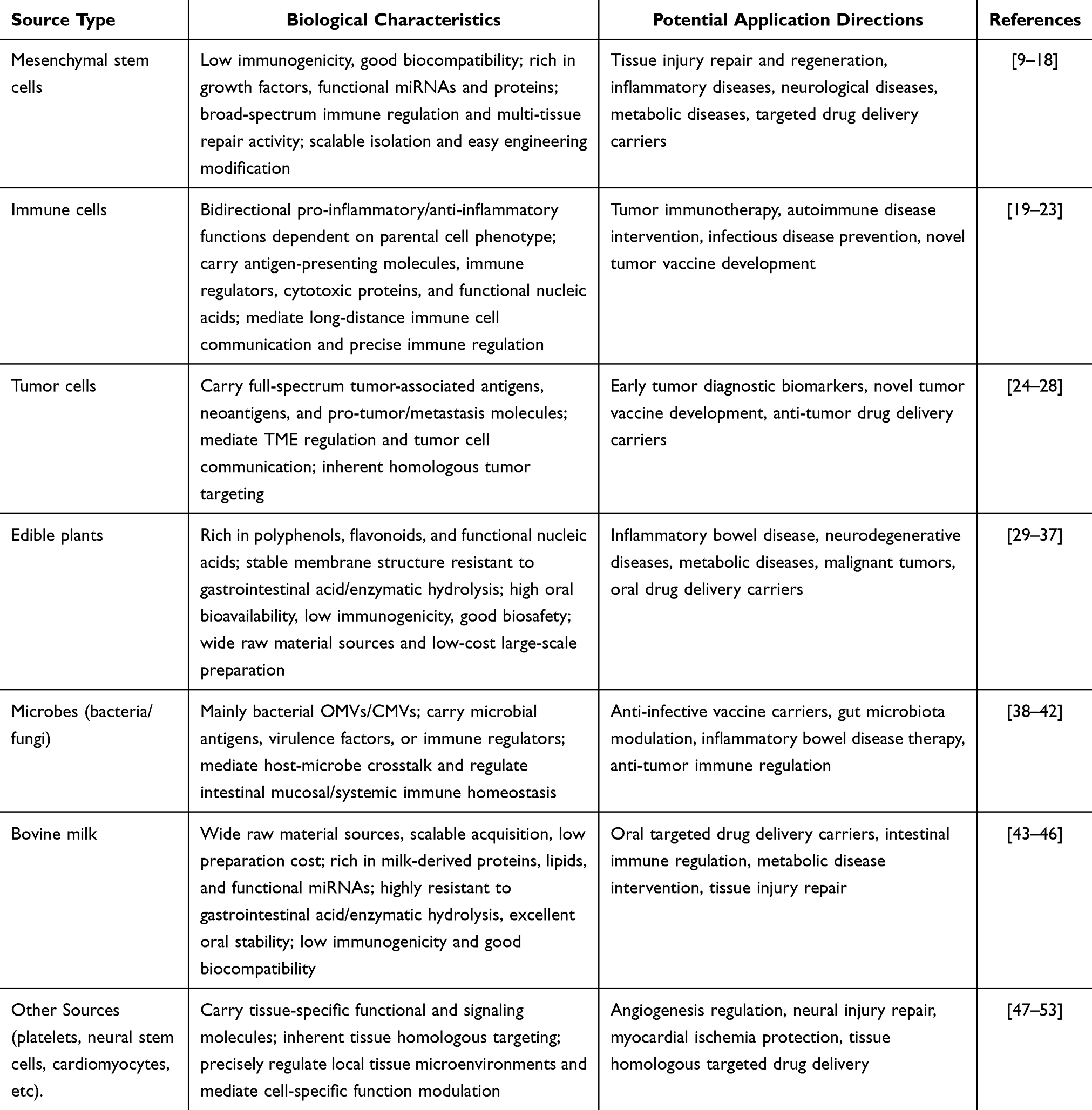 |
Table 1 Comparison of Biological Characteristics of Extracellular Vesicles from Different Sources |
 |
Figure 1 Schematic overview of diverse sources and application directions of extracellular vesicles (EVs). The diagram categorizes EVs by biological origins (including MSCs, immune cells, tumor cells, plant, milk, and microbial sources) and highlights their corresponding therapeutic applications, as well as key engineering modification strategies for enhanced translational potential. Created in BioRender. Fen, (Z) (2026) https://BioRender.com/e79ener. |
Administration Routes of Extracellular Vesicles
Intravenous Injection
Intravenous injection is the most commonly employed systemic administration route for extracellular vesicles (EVs) in both preclinical research and clinical trials. It allows for precise control of the administered dose and enables widespread biodistribution of EVs through the systemic circulation, and is applicable to systemic diseases such as metabolic disorders, CNS diseases, and malignant tumors.16,54,55 Specifically, intravenously infused EVs can improve peripheral insulin resistance in T2DM by restoring the phosphorylation levels of insulin receptor substrate 1 (IRS-1) and protein kinase B (Akt), reduce β-amyloid (Aβ) deposition in Alzheimer’s disease (AD), and suppress tumor growth and metastasis by regulating systemic immune responses and downregulating the activation of regulatory T cells (Tregs).
However, intravenously delivered EVs are rapidly recognized and cleared by the mononuclear phagocyte system in organs such as the liver and spleen, resulting in a short circulating half-life (usually several minutes to hours) and relatively low enrichment in target lesions. Therefore, repeated administration or surface engineering modifications are often required to prolong their in vivo retention time and enhance targeting efficiency.56
Oral Administration
Oral administration is a non-invasive route with high patient compliance, which may support long-term clinical application. This route is feasible for PDEVs and M-EVs, which possess inherent stability against gastric acid and digestive enzyme degradation in the gastrointestinal tract.30,44 Orally administered EVs can cross the intestinal mucosal barrier to enter the systemic circulation, exerting therapeutic effects in inflammatory bowel disease, malignant tumors, and even neurodegenerative disorders via the microbiota-gut-brain axis. For example, M-EVs loaded with anthocyanins exhibit dose-dependent cytotoxicity against tumor cells, while ginger-derived PDEVs can improve behavioral symptoms in Parkinson’s disease (PD) models.57–59
Despite these advantages, the oral bioavailability of EVs remains relatively low-only a small fraction can cross the intestinal barrier, with most retained in the intestinal lumen or degraded during digestion.60 To address this, formulation strategies such as hydrogel encapsulation have been developed to protect EVs from gastric acid and digestive enzymes, thereby improving their intestinal absorption and bioavailability.61
Nasal Instillation
Nasal instillation is a non-invasive, repeatable administration route that allows EVs to bypass the BBB via olfactory and trigeminal nerve pathways, enabling direct targeting of the CNS. This unique advantage makes it the preferred route for treating CNS diseases such as AD, PD, and ischemic stroke.62–64 For example, adipose-derived MSC-EVs delivered via nasal instillation can efficiently enter the brain, reduce Aβ deposition, and improve cognitive function in AD model mice; bitter melon-derived PDEVs can target ischemic brain regions to alleviate neuronal damage in stroke models.
However, the nasal mucociliary clearance system rapidly removes free EVs, and the nasal epithelial barrier restricts their trans-mucosal transport. These factors reduce the bioavailability and brain-targeting efficiency of EVs, requiring formulation optimization to enhance their retention and penetration.
Aerosol Inhalation
Aerosol inhalation enables direct, site-specific delivery of EVs to the lungs as an aerosol, achieving high local concentrations with minimal systemic exposure. This route is used for respiratory diseases such as pulmonary fibrosis, asthma, chronic obstructive pulmonary disease (COPD), lung cancer, and postoperative lung metastasis.65,66 Inhaled EVs can modulate the pulmonary immune microenvironment, promote alveolar epithelial repair, and inhibit tumor progression—for example, M1 macrophage-derived EVs loaded with PD-L1 inhibitors can suppress postoperative lung metastasis by repolarizing tumor-associated macrophages and activating anti-tumor immunity.
A major challenge is that traditional nebulizers (eg., ultrasonic and jet nebulizers) may damage EV structural integrity through shear stress or thermal effects, leading to cargo leakage and reduced bioactivity. Additionally, significant EV adhesion and residue in delivery tubes compromise dosing accuracy, requiring specialized nebulization systems and optimized formulations.67
Subcutaneous Injection
Subcutaneous injection is a minimally invasive, easily operated local delivery route, where EVs are injected into the space between the dermis and subcutaneous fat. A key feature of this route is that injected EVs are preferentially transported to regional lymph nodes through the lymphatic system, supporting its use for skin wound repair, inflammatory skin diseases (eg., atopic dermatitis), tumor vaccines, and systemic immune regulation.68–70 For instance, human umbilical cord blood-derived EVs injected subcutaneously can promote angiogenesis and collagen synthesis to accelerate wound healing and reduce scar formation, while MSC-derived EVs can alleviate skin inflammation and repair the skin barrier.
Nonetheless, free EVs diffuse rapidly in subcutaneous tissue and are quickly cleared, leading to short local retention time and unstable therapeutic concentrations. Microneedle-based delivery systems have been developed to overcome this limitation, enabling precise and controlled delivery of EVs to the dermis for sustained release and prolonged therapeutic effects.71,72
Intravitreal Injection
Intravitreal injection directly delivers EVs into the vitreous cavity, bypassing the blood-retinal barrier to achieve high-efficiency targeting of the retina and optic nerve. This route is employed for posterior segment eye diseases such as age-related macular degeneration (AMD), diabetic retinopathy (DR), glaucoma, and retinitis pigmentosa (RP).73,74 MSC-derived EVs injected intravitreally can protect retinal pigment epithelial (RPE) cells from oxidative stress via the nuclear factor erythroid 2-related factor 2 (Nrf2)/Kelch-like ECH-associated protein 1 (Keap1) pathway, while plasma-derived small EVs can alleviate retinal ganglion cell degeneration in glaucoma models.
As an invasive procedure, this route carries risks of complications including retinal detachment, vitreous hemorrhage, and endophthalmitis. Repeated injections further increase these safety concerns, limiting its application for long-term therapy.
Intrathecal Injection
Intrathecal injection delivers EVs directly into the subarachnoid space, allowing them to enter the cerebrospinal fluid (CSF) and distribute to the spinal cord and brain without being blocked by the BBB or blood-spinal cord barrier. This route enables delivery for severe CNS diseases such as spinal cord injury (SCI), neuropathic pain, multiple sclerosis, and intracranial infections.75,76 Clinical studies have confirmed that intrathecally delivered umbilical cord MSC-EVs can improve sensory and motor function in SCI patients, while red blood cell-derived EVs can serve as safe carriers for CNS gene therapy with no obvious acute toxicity.
Nevertheless, the invasive nature of this procedure carries risks of intracranial infection, subarachnoid hemorrhage, cerebrospinal fluid leakage, and arachnoiditis. Poor patient compliance and the unsuitability for repeated administration remain major translational obstacles.
Intra-Articular Injection
Intra-articular injection directly delivers EVs into the joint cavity, achieving high local concentrations in articular cartilage, synovium, and meniscus while minimizing systemic exposure. This route is applied to joint diseases such as OA and rheumatoid arthritis (RA).77,78 Adipose-derived EVs injected intra-articularly can delay cartilage degeneration, inhibit synovial inflammation, and repolarize macrophages toward an anti-inflammatory phenotype; M2 macrophage-derived EVs loaded with interleukin-10 (IL-10) can further enhance anti-inflammatory effects and promote joint repair.
The primary limitation is that EVs are rapidly cleared from the joint space, requiring frequent injections to maintain therapeutic effects. Local infection and inflammatory reactions are also potential risks associated with repeated administration.
Intraperitoneal Injection
Intraperitoneal injection delivers EVs directly into the peritoneal cavity, allowing them to act on intra-abdominal organs (eg., intestines, pancreas, liver) by crossing local tissue barriers. This route is used for peritoneal fibrosis, inflammatory bowel disease, acute pancreatitis, and abdominal malignancies.79,80 For example, astragalus-pretreated macrophage EVs injected intraperitoneally can alleviate peritoneal thickening and collagen deposition, while Coptis chinensis-derived PDEVs can target colonic inflammation to repair the intestinal mucosal barrier.
However, the absorption efficiency of EVs is highly dependent on peritoneal integrity and physiological status, leading to individual variability in biodistribution and therapeutic outcomes, which limits the stability of its therapeutic effects.
The administration routes and their corresponding disease applications of EVs are illustrated in Figure 2. The detailed advantages, limitations, and clinical scenarios of each route are further summarized in Table 2.
 |
Table 2 Comparison of Different Administration Routes of Extracellular Vesicles and Their Application Scenarios |
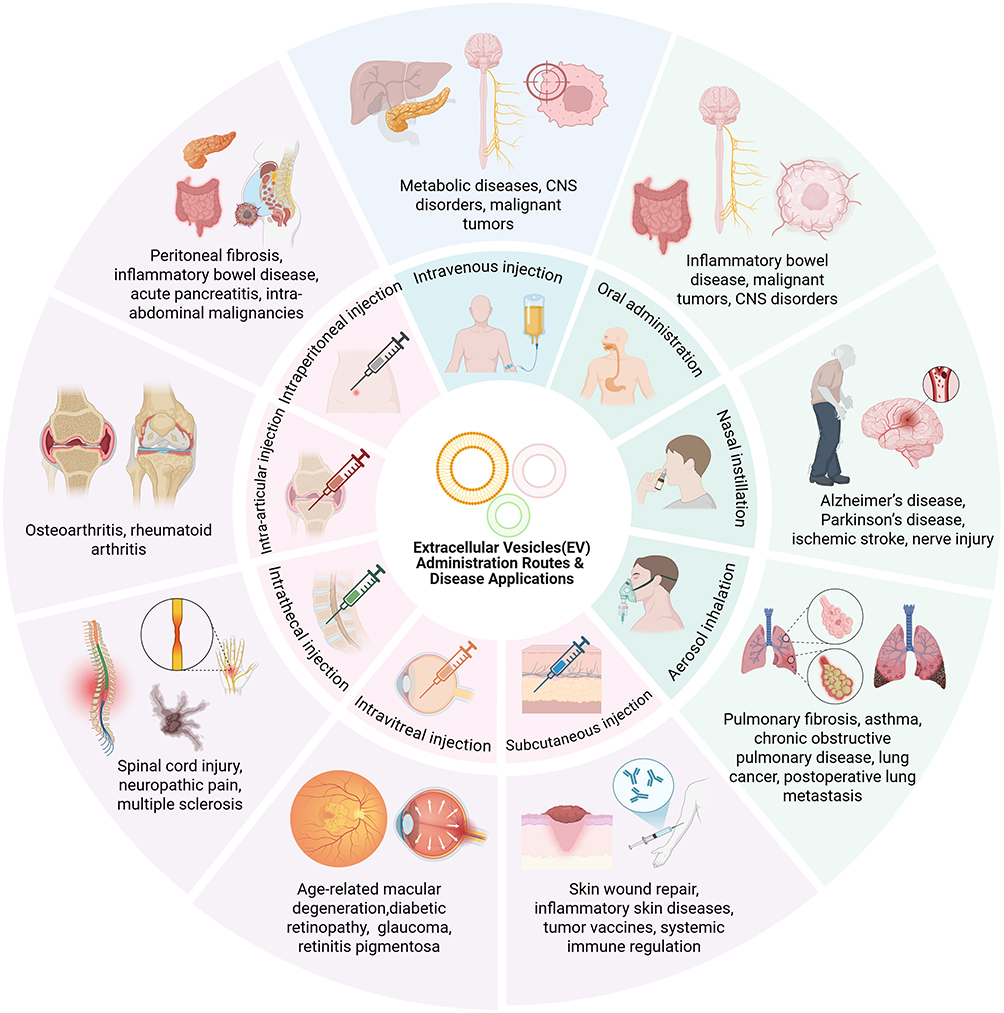 |
Figure 2 Schematic representation of major administration routes and disease applications of extracellular vesicles (EVs). The diagram summarizes common EV delivery routes (including intravenous, oral, nasal, inhalation, subcutaneous, intravitreal, intrathecal, intra-articular, and intraperitoneal injection) and their corresponding disease-specific indications, illustrating route-tailored therapeutic potential. Created in BioRender. Fen, (Z) (2026) https://BioRender.com/e79ener. |
Therapeutic Applications of Extracellular Vesicles From Different Sources in Various Diseases
EVs hold promising therapeutic potential in multiple fields, including tissue repair, immune modulation, oncology, neurological disorders and metabolic diseases. It is noteworthy that the vast majority of research in this field is still limited to preclinical cellular and animal studies, while only a handful of projects have progressed to early-phase clinical trials. Unless otherwise indicated, all therapeutic effects and mechanisms of action presented in this chapter are sourced from published peer-reviewed preclinical studies.
Tissue Repair and Regeneration
Tissue injury involves dysregulated inflammation, impaired cell regeneration, and aberrant ECM remodeling, representing a central focus in regenerative medicine.81 As key paracrine mediators, EVs inherit the bioactive functions of parental cells while avoiding the safety risks of living cell therapy, including abnormal differentiation, tumorigenicity, and immune rejection. EVs orchestrate the entire repair process by regulating inflammatory homeostasis, promoting cell proliferation and migration, and controlling ECM remodeling, with source-dependent functional heterogeneity determining their suitability for different injury types.82
Inflammatory balance is critical for successful repair, and excessive inflammation leads to delayed healing and scarring. EVs maintain local immune homeostasis by modulating macrophage polarization. Lactobacillus reuteri-derived EVs inhibit LPS-induced M1 polarization and promote M2 polarization, thereby reducing inflammation and accelerating wound healing.83 M2 macrophage-derived EVs further enhance angiogenesis via the AKT/mammalian target of rapamycin (mTOR) pathway to promote tissue repair.84 In skin injury, AD-MSC-EVs stimulate fibroblast activity and collagen organization through the phosphatidylinositol 3-kinase (PI3K)/Akt pathway to reduce pathological scarring;18 in bone defects, BM-MSC-sEVs promote osteogenesis via the mitogen-activated protein kinase (MAPK) pathway;85 and in ischemic visceral injury, MSC-EVs attenuate apoptosis and support parenchymal regeneration.86
EVs improve repair quality by fine-tuning collagen deposition and matrix metalloproteinase (MMP)/tissue inhibitor of metalloproteinase (TIMP) balance. AD-MSC-EVs normalize collagen ratios and inhibit myofibroblast differentiation, thus reducing scar formation.87 Similarly, hydrogel-loaded PDEVs enhance diabetic wound healing by regulating angiogenesis, collagen synthesis, and local inflammation.32,33 Bovine milk-derived EVs further support clinical translation due to their high stability, scalability, and low immunogenicity.88
Immune Regulation and Inflammatory Disease Therapy
Dysregulation of innate and adaptive immunity underlies autoimmune diseases, chronic inflammation, and transplant rejection. As key immune communicators, EVs carry proteins, cytokines, and non-coding RNAs to modulate antigen presentation, immune cell activation, and inflammatory responses. EVs from immune cells, MSCs, plants, and microbes exhibit distinct immunomodulatory properties suitable for various inflammatory disorders.89 Macrophage polarization is central to inflammation control, and M2-EVs inherit anti-inflammatory phenotypes to restore immune balance. In RA, M2-EVs suppress synovial M1 activation and protect cartilage;90 in aortic valve calcification, they deliver miRNAs to drive M2 polarization;91 and in OA, they reduce inflammatory and catabolic factors while preserving matrix synthesis.92
Beyond macrophages, EVs coordinate adaptive immunity by regulating T, B, NK, and DC function. T cell-derived EVs induce immune tolerance and suppress excessive effector T cell responses, showing potential in transplant rejection.93,94 B cell-derived EVs mediate long-range immune signaling and enhance anti-infective and anti-tumor immunity.95 MSC-EVs act as broad immunomodulators by inhibiting lymphocyte overactivation and promoting M2 polarization. UC-MSC-EVs correct T helper 17 (Th17)/regulatory T cell (Treg) imbalance in lupus nephritis and alleviate renal injury via the interleukin-6 (IL-6)/signal transducer and activator of transcription 3 (STAT3)/interleukin-17 (IL-17) pathway.96
Plant and probiotic-derived EVs offer safe, oral-compatible options for intestinal inflammation. Catharanthus roseus-derived PDEVs relieve immunosuppression by enhancing immune cell function,97 while probiotic EVs target the mucosal microenvironment to reduce intestinal inflammation and maintain barrier integrity.98
Tumor Therapy
Malignant tumors remain a leading cause of death worldwide, with conventional therapies limited by toxicity, resistance, and immunosuppressive TME.99 With high biocompatibility, barrier-crossing ability, and engineering flexibility, EVs provide a multifaceted platform for precision cancer therapy, with source-specific functions supporting diverse therapeutic strategies.
As acellular tumor vaccines, TEVs carry tumor antigens and neoantigens to activate CD8⁺ T cells without tumorigenic risks, eliciting robust anti-tumor immunity in preclinical models.100,101 Immune cell-derived EVs further reshape anti-tumor immunity: M1-EVs enhance T cell-mediated tumor regression;21 NK-EVs deliver cytotoxic molecules to kill hematologic and solid tumors;102 and CD8⁺ T cell-EVs target stromal and vascular components to inhibit metastasis.103
Plant and microbial EVs exert intrinsic anti-tumor activity. Grapefruit-derived PDEVs induce melanoma cell cycle arrest via Akt/PI3K/mTOR inhibition,31 and bacterial OMVs synergize with chemotherapy to promote apoptosis.104 As delivery carriers, EVs protect chemotherapeutics and nucleic acids from degradation. Folate-modified ginger PDEVs enable targeted siRNA delivery for oral cancer therapy,34 and bovine milk-derived EVs, with outstanding in vivo stability, long circulation, scalable production and low immunogenicity, serve as an candidate carrier for oral tumor-targeted delivery; functionalization with targeting ligands further enhances tumor specificity and reduces off-target effects, showing great potential in personalized cancer therapy.105,106
Notably, MSC-EVs display source-dependent bidirectional effects: they may promote angiogenesis and immune suppression to support tumor progression,107,108 yet can also serve as targeted delivery vehicles for anti-tumor agents.109 Identifying the core determinants of the biphasic regulatory effects of MSC-EVs and standardizing their preparation and quality control are the key issues to be addressed for future clinical translation in this field.
Neurological Disease Therapy
Neurological disorders are hampered by poor neuronal regeneration and limited BBB penetration of conventional drugs. EVs naturally cross the BBB and can be delivered intravenously or nasally, exerting neuroprotective, anti-inflammatory, and pro-regenerative effects in stroke, TBI, SCI, AD, and PD (Parkinson’s disease).110
Persistent neuroinflammation drives neuronal damage, and EVs modulate microglial polarization to alleviate neuroinflammation. Hypoxia-primed microglial EVs promote M2 polarization and reduce post-stroke neuronal death,111 while A2 astrocyte EVs deliver miR-628 to suppress pro-inflammatory signaling in cerebral ischemia.112 In neurodegeneration, MSC-EVs protect neurons via multiple pathways: activating autophagy and Nrf2 in AD,113 inhibiting NF-κB through miR-146a,114 and regulating PTEN-PI3K/Akt via miR-223.115 In PD models, MSC-EVs accumulate in the substantia nigra, reduce dopaminergic neuron loss, and improve motor function.116
PDEVs offer low immunogenicity, oral/nasal deliverability, and inherent neuroactive components.117 Black wolfberry PDEVs attenuate Aβ-induced neurotoxicity,118 and kudzu PDEVs enhance mitophagy to protect dopaminergic neurons and alleviate PD-related deficits,119 supporting their potential for non-invasive CNS therapy.
Metabolic Disease Therapy
Metabolic diseases, including obesity, T2DM, non-alcoholic fatty liver disease (NAFLD), and AS, are driven by systemic metabolic and immune dysregulation.120 Current treatments focus on symptom control, while EVs provide multi-targeted therapy by modulating immune homeostasis, metabolic reprogramming, tissue repair, and gut barrier function.
In metabolic organs, EVs resolve chronic low-grade inflammation. AD-MSC-EVs induce M2 macrophage polarization in adipose tissue to maintain metabolic homeostasis.121 BM-MSC-EVs reduce hepatocyte apoptosis and enhance autophagy in acute liver injury,122 while engineered HEK293T EVs target the liver to improve steatosis and inflammation in metabolic dysfunction-associated steatohepatitis (MASH).123
Edible EVs from plants, milk, and probiotics enable safe, long-term oral intervention via the gut-liver and gut-adipose axes. Shiitake PDEVs attenuate liver inflammation by inhibiting the NOD-like receptor protein 3 (NLRP3) inflammasome;124 bovine milk EVs enhance intestinal barrier function and reduce hepatic steatosis;125 and Akkermansia muciniphila EVs improve insulin sensitivity and body composition in diet-induced obesity.126
Other Indications
EVs also show promise in respiratory, ocular diseases, degenerative, skeletal, and drug-resistant infections. For respiratory diseases, aerosol-inhaled EVs directly target lung tissue, delivering anti-inflammatory and reparative effects for conditions such as pulmonary fibrosis and asthma.65–67 For ocular diseases, intravitreally injected EVs cross the blood-retinal barrier, supporting retinal protection and visual function in AMD, DR, and glaucoma.73,74
In intervertebral disc degeneration (IVDD), hypoxia-conditioned MSC-EVs deliver miR-17-5p to inhibit Toll-like receptor 4 (TLR4)/PI3K-AKT signaling, promoting nucleus pulposus cell survival and matrix synthesis.127 In bone metabolic disorders, DC-derived EVs carry anti-inflammatory factors to suppress osteoclast activity and restore bone homeostasis.128
For drug-resistant infections, EVs penetrate bacterial biofilms and serve as efficient delivery platforms. Ginger-derived PDEVs loaded with Pd-Pt nanosheets exert combined electrodynamic therapy (EDT)/photothermal therapy (PTT) effects to eradicate resistant bacteria and biofilms, offering an antibiotic-free antibacterial strategy.129
The core mechanisms and representative references of EV therapy in various indication categories are listed in Table 3.
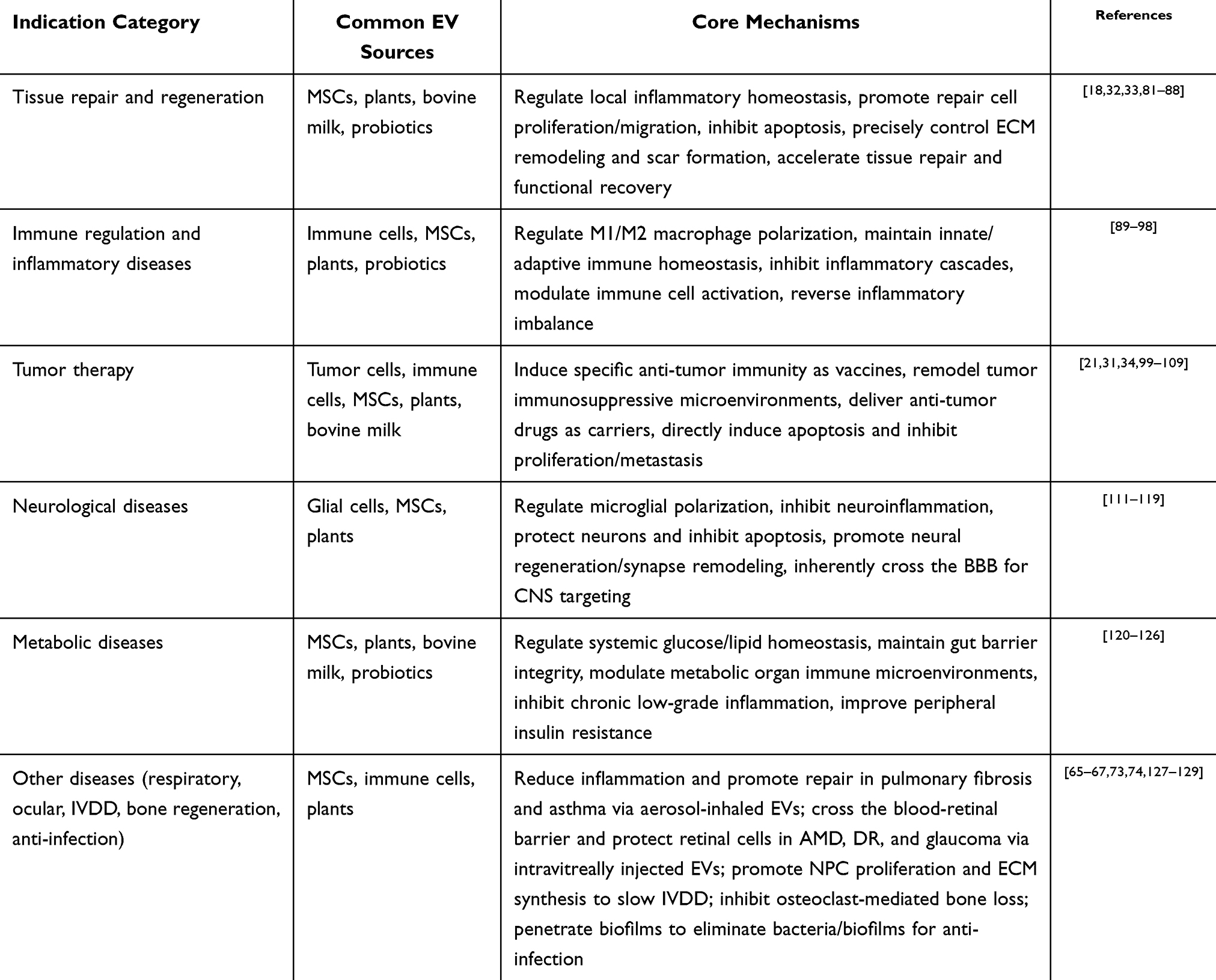 |
Table 3 Main Indications and Mechanisms of Action of Extracellular Vesicles from Different Sources |
Global Regulatory System for Extracellular Vesicle Therapeutic Products
Europe and the United States
Europe and the United States have established relatively mature regulatory frameworks for EV-based therapeutics, which serve as important references for global standardization. In the European Union (Binding regulation), EV products are mainly regulated under Directive 2001/83/EC and Regulation (EC) No 1394/2007 on advanced therapy medicinal products (ATMPs) (Binding regulation). EVs directly isolated from cells without functionally translated nucleic acids are generally not classified as ATMPs (advanced therapy medicinal product), but regulated according to their biological properties and indications. In contrast, EVs carrying functional nucleic acids that mediate therapeutic effects are defined as ATMPs. The European Medicines Agency (EMA) Committee for Advanced Therapies (CAT) further specifies that (Interpretive statement) EVs loaded with recombinant nucleic acids whose efficacy depends on such components meet the definition of gene therapy medicinal products under Article 21 of Regulation (EC) No 1394/2007, and must undergo full ATMP review and approval.130
In the United States, EV therapeutics are overseen by the U.S. Food and Drug Administration (FDA) Center for Biologics Evaluation and Research (CBER). The core legal basis includes Section 351 of the Public Health Service Act (PHS Act) governing human cellular and tissue-based products (HCT/Ps) (Binding regulation), as well as the Federal Food, Drug, and Cosmetic Act (FD&C Act) for drugs and biologics (Binding regulation). The FDA has issued public safety notifications regarding adverse event reporting for EV products and warning letters against unapproved EV-based therapies (Interpretive statement), emphasizing that any EV product intended for human therapeutic use requires formal premarket approval.131
Asia
Regulatory systems for EV therapeutics in Asia have developed rapidly in recent years, with Japan and China as key representatives. In Japan, EV products are regulated by the Ministry of Health, Labour and Welfare (MHLW) and the Pharmaceuticals and Medical Devices Agency (PMDA) under the Pharmaceuticals and Medical Devices Act (Binding regulation). While cell and gene therapy products are classified as regenerative medicine products, non-living EV formulations that act through pharmacological, immunological, or metabolic mechanisms are categorized as general pharmaceuticals.132 In August 2024, the PMDA released the Quality and Safety Assessment Report for Extracellular Vesicle Therapeutic Products (Official formal guidance), representing the world’s first national-level official technical guideline dedicated to EV drug development.133
In China, the National Medical Products Administration (NMPA) is accelerating the establishment of a standardized regulatory system for EV therapeutics. In June 2025, the Center for Drug Evaluation (CDE) issued the Draft for Comment on the Scope, Classification and Interpretation of Advanced Therapy Medicinal Products (ATMPs) (Draft guidance), formally incorporating EV therapeutics into the ATMP framework and classifying them as either novel delivery system drugs or cell derivative products according to their composition and mechanism. In August 2025, the National Institutes for Food and Drug Control (NIFDC) systematically expounded the research and development, quality control, and nonclinical evaluation of EV drugs (Interpretive statement), marking the first official technical review supporting the druggability of EV products.134
Global Clinical Landscape of Extracellular Vesicle Therapeutic Products
To systematically illustrate the industrial translation of extracellular vesicle (EV) therapeutics, this chapter summarizes the global clinical pipeline of EV products with a focus on industry-sponsored candidates undergoing regulatory review or clinical trials. Data collection and verification were completed in April 2026. Systematic searches were performed in official regulatory databases including the CDE, FDA, and Ministry of Food and Drug Safety (MFDS), as well as global clinical trial registries, using keywords such as extracellular vesicles, exosome, Investigational New Drug (IND), and clinical trial. Only commercial-oriented EV therapeutic products that entered formal registration or clinical trials were included, while preclinical candidates and non-commercial academic projects were excluded.
As of April 2026, no EV therapeutic product has been formally approved for marketing worldwide. Among the 9 products that have entered registered clinical trials, only 1 has advanced to Phase III, 2 to Phase II, and the remaining 6 are at Phase I or earlier stages or have been terminated, indicating a low overall level of clinical maturity (detailed in Table 4). All clinical trials listed were registered on ClinicalTrials.gov, except STX11101 which was registered with the CDE of the NMPA of China; the sponsor information for each trial is consistent with the corresponding company name. North America leads in late-phase development: Direct Biologics’ ExoFlo (bone marrow MSC-derived EVs) is in Phase III for acute respiratory distress syndrome (ARDS) (NCT05354141); Rion/INTENT Biologics’ PEP-TISSEEL (platelet-derived exosomes) has completed Phase II for diabetic foot ulcers (DFUs) with FDA Fast Track designation (NCT06319287); Aegle Therapeutics’ AGLE-102 (bone marrow MSC-derived EVs) is in Phase II for burns/epidermolysis bullosa (EB) (NCT05078385, NCT04173650). Notably, Codiak BioSciences’ engEx™ platform-based candidates (CDK-002/003/004) for solid tumors were terminated due to bankruptcy (NCT04592484, NCT05156229, NCT05375604).
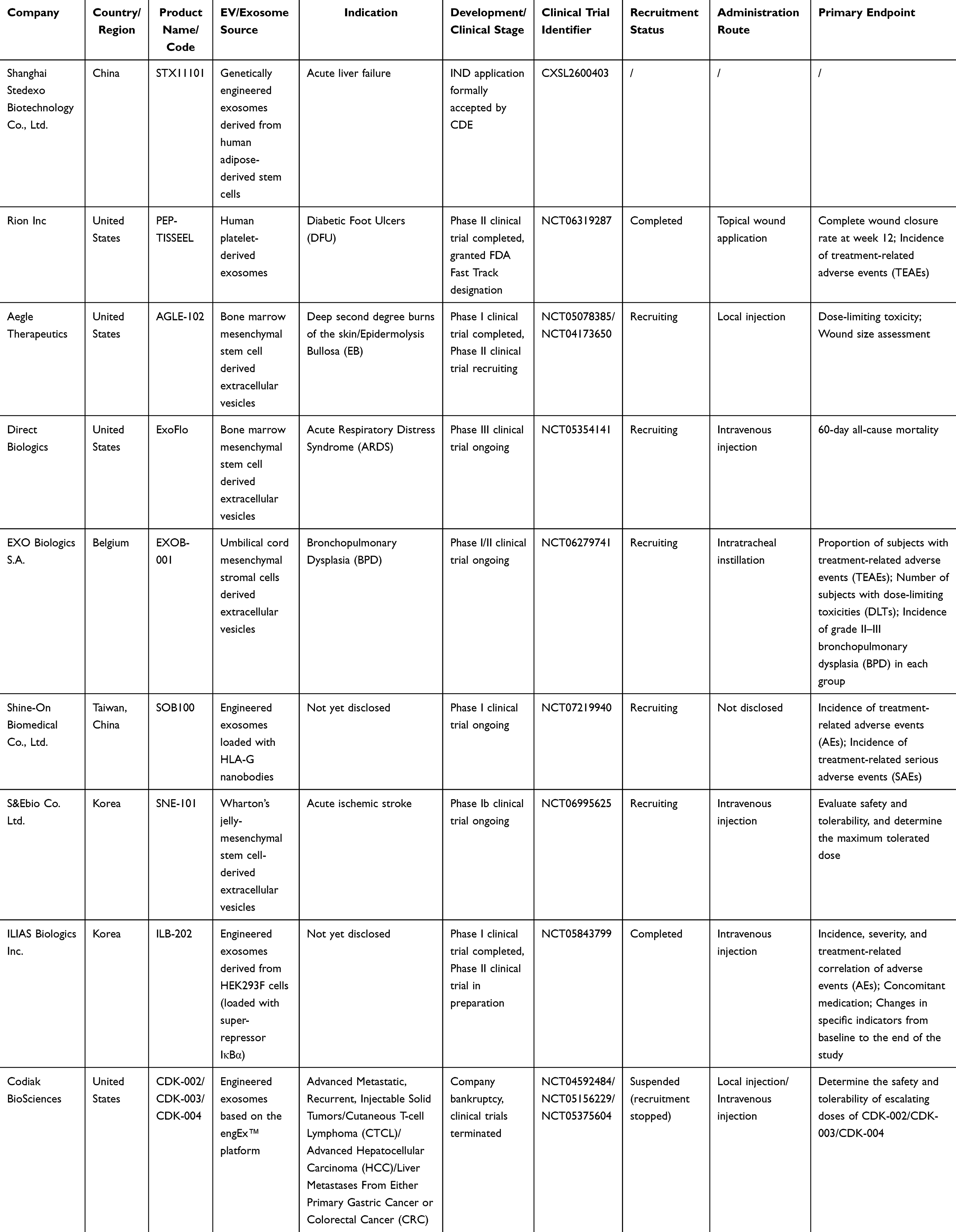 |
Table 4 Clinical Research Projects and Products of Global Exosome/Extracellular Vesicle Therapeutics |
Europe and Asia contribute key growth momentum: Belgium’s EXO Biologics runs Phase I/II of EXOB-001 (umbilical cord MSC-derived EVs) for pediatric bronchopulmonary dysplasia (BPD) (NCT06279741). In Asia, South Korea’s S&Ebio advances Phase Ib of SNE-101 (Wharton’s jelly MSC-derived EVs) for stroke (NCT06995625), and ILIAS Biologics prepares Phase II of ILB-202 (HEK293F-engineered EVs, NCT05843799). In China, Shanghai Stedexo’s STX11101 (engineered adipose MSC-exosomes) has CDE IND acceptance for acute liver failure (CXSL2600403), while Taiwan’s Shine-On Biomedical conducts Phase I of SOB100 (HLA-G nanobody-engineered EVs, NCT07219940).
Technical and indication trends show clear convergence: MSC-derived EVs dominate for broad immunomodulatory/repair effects; engineered EVs (genetic modification, nanobody conjugation, cargo loading) enhance targeting; HEK293F cells address scalability. Respiratory, skin, and neurological diseases are top indications, with rare/pediatric conditions aligned with regulatory priorities. Published clinical results are available for ExoFlo135 and ILB-202;136 results for all other listed trials remain unpublished as of April 2026.
Discussion
Following the systematic summary of EV sources, administration routes, therapeutic applications, global regulatory systems and clinical pipelines, this section focuses on three core dimensions: rational matching of EV systems, key translational challenges, and comparative advantages of EV therapeutics.
Matching Analysis of EV Sources and Administration Routes
The administration route is a core determinant of EV therapeutic efficacy and clinical feasibility, and its selection must be rationally matched with disease type, lesion location, and the biological characteristics of different EV sources, as well as aligned with critical quality attributes (CQAs) and regional regulatory pathways.6 MSC-EVs exhibit the broadest route adaptability owing to their potent tissue repair and immunomodulatory activities. Intravenous injection enables systemic distribution for metabolic and neurodegenerative diseases such as T2DM and AD; subcutaneous administration facilitates lymph node targeting for skin repair, autoimmune diseases, and tumor vaccines; nasal or intrathecal delivery bypasses the BBB for CNS disorders; and intra-articular injection achieves direct local enrichment for OA.
Immune cell-derived EVs are typically administered intravenously for systemic immune regulation in autoimmune diseases, or via subcutaneous or intratumoral injection for localized immune modulation in cancer therapy. PDEVs and M-EVs possess inherent gastrointestinal stability and are feasible for oral administration in diseases such as colitis and PD, as well as topical application for local anti-inflammatory effects, although large-scale oral application is still limited by production scalability. MEVs are preferably delivered locally to minimize systemic immune risks, such as intra-articular administration for infectious arthritis. PEVs are suitable for subcutaneous or topical delivery in wound repair, and intravenous use in cardiovascular diseases, though strict dose control is required to avoid thrombotic complications.
Overall, the rational matching of EV sources and administration routes follows several core principles: orally stable PDEVs and M-EVs are feasible for oral delivery; CNS diseases require BBB-penetrating EVs administered via nasal or intrathecal routes; and localized lesions are optimally treated with direct local injection to achieve high target enrichment and reduce off-target exposure.
Core Challenges and Strategies for EV Clinical Translation
Despite extensive preclinical therapeutic potential, EV clinical translation faces critical, interconnected bottlenecks requiring targeted solutions.This section strengthens critical discussion of translational barriers and adds the six required core challenges.
Core Clinical Translation Challenges
First, the therapeutic mechanisms and key effector components of EVs remain insufficiently defined. The highly heterogeneous cargoes of EVs, including proteins, nucleic acids, and lipids, make it difficult to identify core active molecules, hindering mechanism-guided optimization and quality control.137 A second prominent obstacle concerns incomplete potency assays, which further restrict quantitative evaluation of EV bioactivity, as no validated functional detection systems are available to reflect real in vivo therapeutic efficacy.
Thirdly, scalable and compliant production remains a major challenge. Current good manufacturing practice (cGMP)-compliant manufacturing processes are incomplete; large-scale culture is limited by restricted expansion of primary cells, while immortalized or tumor cell-derived EVs carry potential safety risks.138 A further associated drawback refers to severe product inconsistency. Significant batch-to-batch variability in particle size and cargo composition and biological activity caused by unstable production processes compromises product consistency and clinical repeatability.139 Additionally, poor comparability between independent studies is aggravated by inconsistent isolation, purification and dosing methodologies across laboratories, which impedes cross-study validation and meta-analysis of EV therapeutic effects.
Another systemic barrier originates from the absence of unified quality evaluation frameworks. No global consensus has been established on standardized CQAs for EV products, including particle concentration, purity, cargo identity and functional activity. Furthermore, unclear in vivo biodistribution due to deficient real-time tracing technologies hinders accurate assessment of EV tissue targeting, accumulation and metabolic fate, while rapid immune clearance by the mononuclear phagocyte system shortens the circulatory half-life of systemically administered EVs and reduces lesion enrichment. Limited in vivo tracing techniques also impede standardized pharmacokinetic, immunogenicity, and toxicity evaluations, further affecting the reliability of safety and efficacy assessment.
Finally, global regulatory alignment is lacking. Classification principles differ across regions, with the FDA and EMA categorizing natural MSC- or immune cell-derived EVs as biologics and engineered EVs as gene therapy ATMPs. At present, only ISEV MISEV guidelines and regional consensus documents are available, with no dedicated global guidelines from the World Health Organization (WHO), FDA, or EMA covering quality control and nonclinical evaluation.140
Mitigation Strategies
To address these challenges, multi-omics approaches including single-cell sequencing, proteomics, lipidomics, and metabolomics should be applied to clarify core active components, dose-effect relationships, and molecular mechanisms, supporting precise quality control and targeted therapeutic optimization. Scalable cGMP production processes can be established through standardized full-cycle standard operating procedures (SOPs) and optimized cell culture systems to improve yield. Microfluidic and affinity purification technologies can enhance purity and recovery, reduce costs, and minimize batch variability to ensure product consistency.
International collaboration among ISEV, WHO, FDA, and EMA is urgently needed to develop dedicated global regulatory guidelines for EV therapeutics, unifying classification standards, quality control indicators, and nonclinical evaluation protocols to advance stepwise progress in global regulatory harmonization. Meanwhile, clinical trial design should be optimized with large-sample, long-term follow-up Phase III studies to validate long-term safety and efficacy. For engineered EVs, particular attention should be paid to in vivo targeting, cargo safety, and metabolic fate to provide robust clinical evidence for translation.
Comparison of Advantages and Disadvantages Between EVs and Mainstream Therapies
To fully understand the clinical value of EVs, it is necessary to systematically compare their performance with conventional small-molecule/biological therapies and living cell therapies, highlighting their unique strengths in precision, safety, and translational practicality.
Compared with conventional drug therapy, EVs exhibit superior targeting ability and physiological barrier penetration. Source-specific membrane proteins enable natural lesion targeting, and the inherent phospholipid bilayer allows EVs to cross the BBB and other biological barriers without additional modification.141 Compared with other organic nanocarriers (eg., cyanine dye nanoparticles), EVs exhibit lower immunogenicity and superior biocompatibility, and do not suffer from poor photostability.142 EVs also demonstrate better biocompatibility and safety, especially those from autologous or edible sources, which reduce the risk of immune rejection and avoid the off-target organ toxicity commonly seen with small-molecule drugs.143 Furthermore, EVs possess high cargo capacity and can co-deliver proteins, nucleic acids, and small molecules to achieve multi-target synergistic therapy, overcoming the single-target limitations of conventional drugs in complex diseases such as cancer and neurodegeneration.144
Compared with living cell therapy, EVs act as cell-free functional surrogates that retain therapeutic efficacy while overcoming key translational bottlenecks. EVs lack proliferative and differentiation potential, thus eliminating risks of abnormal proliferation, ectopic differentiation, tumorigenicity, and allogeneic immune rejection. Notably, MSC-EVs have shown comparable neuroprotective and myocardial repair effects to MSCs with significantly improved safety profiles.145–147
In terms of translational practicality, EVs enable standardized production, cryopreservation, and transportation without viability maintenance, greatly reducing clinical application barriers. They also support more flexible administration routes including oral delivery (especially M-EVs), aerosol inhalation, and local injection, improving patient compliance compared with cell therapies mostly restricted to intravenous infusion. In addition, EV doses can be precisely quantified based on particle number, protein content, or active component concentration, avoiding variability caused by cell viability differences and ensuring more consistent therapeutic effects.
In summary, EVs compensate for the poor targeting and systemic toxicity of conventional drugs and the safety and practicality limitations of cell therapy. Supported by growing global clinical trials and industrial pipelines, EVs are evolving from laboratory tools toward clinically viable therapeutics, providing a precise, safe, and highly accessible strategy for complex multifactorial diseases. Nevertheless, a series of key scientific validation studies are still required to realize the broad clinical translation of EV therapeutics and address the common technical challenges in this field.
Future Research Perspectives
Systematic Comparisons of EVs from Different Sources
Currently, no studies have systematically compared EVs from major sources (MSCs, immune cells, plants, milk, microbes, platelets) under fully unified manufacturing, characterization and the same disease model conditions. Inconsistent isolation, culture and evaluation systems make existing results incomparable and unable to support optimal source selection. Future multi-center standardized studies are needed to assess the physicochemical properties, molecular composition, efficacy, immunogenicity and cost of diverse-source EVs, and establish an EV indication map for precise clinical selection.
Route-Specific Pharmacokinetics, Biodistribution and Clearance Studies
The in vivo fate of EVs determines efficacy and safety, but current pharmacokinetic studies remain limited. EV biodistribution is highly route-dependent: intravenous injection accumulates in the liver, spleen and lungs; inhalation targets the lungs; nasal administration crosses the BBB.148 However, inter-source differences under the same route and metabolic profiles of the same source across routes remain unclear. Nanoprobe-based immunoassays enable high-sensitivity EV quantification and real-time tracing.149 Future studies should use orthogonal multiple tracing methods (fluorescent, genetic, radionuclide, magnetic labeling) to avoid false positives, clarify EV absorption, distribution, metabolism, clearance (ADME-C), and support clinical dosing design.150,151
Standardized Potency Assays, Dose-Response Relationships, Minimum Effective Dose (MED) and Maximal Tolerated Dose (MTD)
EV pharmacology follows general drug principles but faces unique challenges in standardization: inconsistent dose units and uncoupled potency-bioactivity limit cross-study comparison. Most studies use particle count or total protein as dose metrics, which are biased by purity and impurities and fail to reflect real activity. Future work should first identify core active components and mechanisms, then establish mechanism-linked standardized potency assays, define clear dose-response relationships, and quantify the minimum effective dose (MED) and maximal tolerated dose (MTD) per MISEV2023, with proper dose-response, time-course and negative controls to eliminate non-specific interference.140
Comprehensive Safety Evaluations: Toxicology, Risk Profiling, Durability of Effect and Repeated Dosing
EV therapy is safer than living-cell therapy, but a systematic safety framework is lacking. Most studies only perform short-term single-dose tests, without standardized repeated-dose toxicology, long-term safety or special toxicity data.152 A two-dimensional safety system (nonclinical design + clinical risk control) should be established per international drug standards.
Nonclinical studies require species-specific design: normal human-cell EVs need single/repeated-dose tests in one species; engineered or unvalidated EVs need two species. Dosing route, frequency and design should match clinical intent, with maximum dose constrained by tolerated/feasible limits and the 3Rs principle. Toxicokinetics remains challenging due to EV heterogeneity.
Clinical risks include: (1) EV immunogenicity (low for allogeneic EVs); (2) impurity-induced hypersensitivity (reducible by animal-component-free processes); (3) treatment-related immune imbalance including coagulation activation, complement activation, cytokine release and off-target organ accumulation. Durability of therapeutic effect and rational repeated dosing regimens should also be systematically investigated to optimize clinical dosing intervals and courses.133
Cargo Stability and Off-Target Delivery of Engineered EVs
Engineering enhances EV loading and targeting, but suffers from low packaging efficiency, cargo degradation and off-target effects.153 Future studies should evaluate cargo stability across loading methods (electroporation, co-incubation, genetic engineering), quantify retention/release kinetics and off-target distribution, optimize targeting via surface modification and parental cell engineering, and build standardized targeting assays. In addition, the application of precise gene-editing technologies such as CRISPR/Cas9 has provided new avenues for further enhancing the drug-loading capacity and delivery precision of engineered EVs.154 The integration of EVs with nanomotor technologies—harnessing self-propulsion to overcome the high interstitial pressure barrier in tumor tissues and strengthen deep penetration—represents a promising developmental direction for next-generation EV delivery systems.155,156
Conclusion
This review systematically summarizes the core biological characteristics of EVs derived from MSCs, immune cells, tumor cells, plants, microorganisms, bovine milk, and platelets. It clarifies the practical applicable scenarios of diverse administration routes, outlines preclinical and clinical advances of EV interventions in multiple disease, and interprets differentiated global regulatory systems for EV medicinal products. Highlighting the rational matching framework of EV sources, administration routes, disease indications, CQAs and regulatory pathways as its core innovative viewpoint, the manuscript systematically collates the latest global clinical development data of industry-funded EV candidates under regulatory review or registered clinical trials. Cumulative evidence verifies that EVs from disparate origins possess unique therapeutic advantages and constitute innovative intervention alternatives for intractable complex diseases.
Several regular matching rules are concluded from existing research data: MSC-EVs exhibit broad-spectrum reparative and immunomodulatory effects for degenerative and inflammatory illnesses; immune cell-derived EVs realize targeted immune regulation and tumor cytotoxicity for cancer and autoimmune disorders; tumor cell-derived EVs are available for liquid biopsy and anti-tumor vaccine development; PDEVs and M-EVs with excellent gastrointestinal stability fit oral administration against inflammatory and metabolic diseases; MEVs serve as immunomodulatory agents for infectious disorders; platelet-derived EVs are suitable for acute wound repair. Route selection needs comprehensive consideration of EV intrinsic properties, lesion location and disease type: intravenous delivery targets systemic metabolic and malignant illnesses; inhalation acts on localized pulmonary lesions; oral administration is preferred for gastrointestinal diseases with orally stable EV varieties; nasal or intrathecal injection bypasses the BBB for CNS ailments; intravitreal, intra-articular and other local injections achieve high local drug enrichment for ocular and articular disorders, while surface engineering further improves targeted delivery efficiency.
Current translational hurdles include inadequate large-scale standardized production techniques, inconsistent CQA systems, varying regional regulatory classifications, unresolved challenges in potency detection, batch consistency, in vivo biodistribution assessment and long-term safety verification. Though ongoing technical upgrades and accumulating clinical data may ease these restrictions, large-scale confirmatory clinical evidence remains scarce and most research stays at preclinical or early clinical phases.
To accelerate bench-to-bedside transformation, six targeted developmental priorities are proposed: (1) define core functional components and dose-effect correlations based on molecular mechanisms to guide rational EV optimization; (2) establish standardized cGMP-compliant production and purification workflows to reduce batch fluctuation; (3) formulate globally unified CQA specifications and functional potency testing standards to guarantee consistent product quality; (4) launch multi-center, long-term follow-up large clinical trials to validate long-term safety and therapeutic efficacy; (5) develop surface modification and intelligent delivery strategies to enhance lesion accumulation and reduce in vivo immune clearance; (6) promote cross-border regulatory cooperation to unify international evaluation guidelines for EV pharmaceuticals.
AI Statement
OpenAI Generative Pre-trained Transformer (GPT) was only utilized to assist with English translation during manuscript preparation.
Abbreviations
AD, Alzheimer’s disease; ADME-C, absorption, distribution, metabolism and clearance; AMD, age-related macular degeneration; ARDS, acute respiratory distress syndrome; ATMP, advanced therapy medicinal product; Akt, protein kinase B; BBB, blood-brain barrier; BPD, bronchopulmonary dysplasia; CBER, Center for Biologics Evaluation and Research; CDE, Center for Drug Evaluation; CGT, Cell and Gene Therapy; CM-EVs, cardiomyocyte-derived extracellular vesicles; CMVs, cytoplasmic membrane vesicles; CNS, central nervous system; COPD, chronic obstructive pulmonary disease; CQAs, critical quality attributes; cGMP, current good manufacturing practice; DR, diabetic retinopathy; DFUs, diabetic foot ulcers; DCs, dendritic cells; EB, epidermolysis bullosa; EDT, electrodynamic therapy; ECM, extracellular matrix; EMA, European Medicines Agency; EVs, extracellular vesicles; FD&C Act, Federal Food, Drug, and Cosmetic Act; FDA, U.S. Food and Drug Administration; HCT/Ps, human cellular and tissue-based products; IC-EVs, immune cell-derived extracellular vesicles; IND, Investigational New Drug; IRS-1, insulin receptor substrate 1; ISEV, International Society for Extracellular Vesicles; IL-6, interleukin-6; IL-10, interleukin-10; IL-17, interleukin-17; IVDD, intervertebral disc degeneration; Keap1, Kelch-like ECH-associated protein 1; LPS, lipopolysaccharide; lncRNAs, long non-coding RNAs; MED, minimum effective dose; MFDS, Ministry of Food and Drug Safety; M-EVs, milk-derived extracellular vesicles; MEVs, microbe-derived extracellular vesicles; MISEV, Minimal Information for Studies of Extracellular Vesicles; MHC, major histocompatibility complex; MAPK, mitogen-activated protein kinase; MASH, metabolic dysfunction-associated steatohepatitis; MTD, maximal tolerated dose; MMP, matrix metalloproteinase; MSCs, mesenchymal stem cells; mTOR, mammalian target of rapamycin; NAFLD, non-alcoholic fatty liver disease; NIFDC, National Institutes for Food and Drug Control; NLRP3, NOD-like receptor protein 3; NMPA, National Medical Products Administration; NK, natural killer; Nrf2, nuclear factor erythroid 2-related factor 2; NF-κB, nuclear factor-kappa B; NSCs/NPCs, neural stem/progenitor cells; OMVs, outer membrane vesicles; OA, osteoarthritis; PD, Parkinson’s disease; PDEVs, plant-derived extracellular vesicles; PI3K, phosphatidylinositol 3-kinase; PHS Act, Public Health Service Act; PMDA, Pharmaceuticals and Medical Devices Agency; PEVs, platelet-derived extracellular vesicles; PTT, photothermal therapy; RA, rheumatoid arthritis; RP, retinitis pigmentosa; RPE, retinal pigment epithelial; SCI, spinal cord injury; SOPs, standard operating procedures; STAT3, signal transducer and activator of transcription 3; T2DM, type 2 diabetes mellitus; TEVs, tumor cell-derived extracellular vesicles; TIMP, tissue inhibitor of metalloproteinase; TME, tumor microenvironment; TLR4, Toll-like receptor 4; Th17, T helper 17; Tregs, regulatory T cells; WHO, World Health Organization; circRNAs, circular RNAs; miRNAs, microRNAs.
Acknowledgments
The authors sincerely thank all researchers who have contributed to the development of EV therapeutics. We are grateful for the support and assistance from our research institutions during the writing of this review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Park KS, Lässer C, Lötvall J. Extracellular vesicles and the lung: from disease pathogenesis to biomarkers and treatments. Physiol Rev. 2025;105:1733–27. doi:10.1152/physrev.00032.2024
2. Ripoll L, Zickler AM, Vader P, et al. Biology and therapeutic potential of extracellular vesicle targeting and uptake. Nat Rev Mol Cell Biol. 2026:1–9.
3. Askenase PW. Extracellular Vesicle (EV) targeted cells release secondary effector EVs: indication of how to account for histocompatibility and disease specificity of EV treatments. J Extracell Vesicles. 2025;14:e70076. doi:10.1002/jev2.70076
4. Zhao Z, Wijerathne H, Godwin AK, et al. Isolation and analysis methods of extracellular vesicles (EVs). Extracell Vesicles Circ Nucl Acids. 2021;2:80–103. doi:10.20517/evcna.2021.07
5. Sakamoto Y, Ochiya T, Yoshioka Y. Extracellular vesicles in the breast cancer brain metastasis: physiological functions and clinical applications. Front Hum Neurosci. 2023;17:1278501. doi:10.3389/fnhum.2023.1278501
6. Su X, Wang H, Li Q, et al. Extracellular vesicles: a review of their therapeutic potentials, sources, biodistribution, and administration routes. Int J Nanomed. 2025;20:3175–3199. doi:10.2147/IJN.S502591
7. Zhao S, Di Y, Fan H, et al. Targeted delivery of extracellular vesicles: the mechanisms, techniques and therapeutic applications. Mol Biomed. 2024;5:60. doi:10.1186/s43556-024-00230-x
8. Zhang J, Pan Y, She P, et al. From bench to bedside: the promise and roadblocks of extracellular vesicle therapeutics. Theranostics. 2026;16(9):5044–5064. doi:10.7150/thno.131621
9. Zhuang WZ, Lin YH, Su LJ, et al. Mesenchymal stem/stromal cell-based therapy: mechanism, systemic safety and biodistribution for precision clinical applications. J Biomed Sci. 2021;28:28. doi:10.1186/s12929-021-00725-7
10. Kou M, Huang L, Yang J, et al. Mesenchymal stem cell-derived extracellular vesicles for immunomodulation and regeneration: a next generation therapeutic tool? Cell Death Dis. 2022;13:580. doi:10.1038/s41419-022-05034-x
11. Álvarez-Viejo M. Mesenchymal stem cells from different sources and their derived exosomes: a pre-clinical perspective. World J Stem Cells. 2020;12:100–109. doi:10.4252/wjsc.v12.i2.100
12. Sarvar DP, Effatpanah H, Akbarzadehlaleh P, et al. Mesenchymal stromal cell-derived extracellular vesicles: novel approach in hematopoietic stem cell transplantation. Stem Cell Res Ther. 2022;13(1):202. doi:10.1186/s13287-022-02875-3
13. Gorgun C, Palamà MEF, Reverberi D, et al. Role of extracellular vesicles from adipose tissue- and bone marrow-mesenchymal stromal cells in endothelial proliferation and chondrogenesis. Stem Cells Transl Med. 2021;10:1680–1695. doi:10.1002/sctm.21-0107
14. Sharma R, Kumari M, Mishra S, et al. Exosomes secreted by umbilical cord blood-derived mesenchymal stem cell attenuate diabetes in mice. J Diabetes Res. 2021;2021:9534574. doi:10.1155/2021/9534574
15. Yap SK, Tan KL, Abd Rahaman NY, et al. Human umbilical cord mesenchymal stem cell-derived small extracellular vesicles ameliorated insulin resistance in type 2 diabetes mellitus rats. Pharmaceutics. 2022;14(3):649. doi:10.3390/pharmaceutics14030649
16. Sun Y, Shi H, Yin S, et al. Human mesenchymal stem cell derived exosomes alleviate type 2 diabetes mellitus by reversing peripheral insulin resistance and relieving β-cell destruction. ACS Nano. 2018;12:7613–7628. doi:10.1021/acsnano.7b07643
17. Patel NJ, Ashraf A, Chung EJ. Extracellular vesicles as regulators of the extracellular matrix. Bioengineering. 2023;10. doi:10.3390/bioengineering10020136
18. Zhang W, Bai X, Zhao B, et al. Cell-free therapy based on adipose tissue stem cell-derived exosomes promotes wound healing via the PI3K/Akt signaling pathway. Exp Cell Res. 2018;370:333–342. doi:10.1016/j.yexcr.2018.06.035
19. Chen J, Zhang G, Wan Y, et al. Immune cell-derived exosomes as promising tools for cancer therapy. J Control Release. 2023;364:508–528. doi:10.1016/j.jconrel.2023.11.003
20. Buzas EI. The roles of extracellular vesicles in the immune system. Nat Rev Immunol. 2023;23:236–250. doi:10.1038/s41577-022-00763-8
21. Wang S, Li F, Ye T, et al. Macrophage-tumor chimeric exosomes accumulate in lymph node and tumor to activate the immune response and the tumor microenvironment. Sci Transl Med. 2021;13:eabb6981. doi:10.1126/scitranslmed.abb6981
22. Oelsner S, Waldmann A, Billmeier A, et al. Genetically engineered CAR NK cells display selective cytotoxicity against FLT3-positive B-ALL and inhibit in vivo leukemia growth. Int J Cancer. 2019;145:1935–1945. doi:10.1002/ijc.32269
23. Zhu L, Kalimuthu S, Gangadaran P, et al. Exosomes derived from natural killer cells exert therapeutic effect in melanoma. Theranostics. 2017;7:2732–2745. doi:10.7150/thno.18752
24. Greening DW, Xu R, Rai A, et al. Clinical relevance of extracellular vesicles in cancer - therapeutic and diagnostic potential. Nat Rev Clin Oncol. 2025;22:924–952.
25. Mashouri L, Yousefi H, Aref AR, et al. Exosomes: composition, biogenesis, and mechanisms in cancer metastasis and drug resistance. Mol Cancer. 2019;18(1):75. doi:10.1186/s12943-019-0991-5
26. Iannotta D, A A, Kijas AW, et al. Entry and exit of extracellular vesicles to and from the blood circulation. Nat Nanotechnol. 2024;19(1):13–20. doi:10.1038/s41565-023-01522-z
27. Hoshino A, Kim HS, Bojmar L, et al. Extracellular vesicle and particle biomarkers define multiple human cancers. Cell. 2020;182:1044–1061.e1018. doi:10.1016/j.cell.2020.07.009
28. Dorado E, Doria ML, Nagelkerke A, et al. Extracellular vesicles as a promising source of lipid biomarkers for breast cancer detection in blood plasma. J Extracell Vesicles. 2024;13:e12419. doi:10.1002/jev2.12419
29. Cong M, Tan S, Li S, et al. Technology insight: plant-derived vesicles-How far from the clinical biotherapeutics and therapeutic drug carriers? Adv Drug Deliv Rev. 2022;182:114108. doi:10.1016/j.addr.2021.114108
30. Lian MQ, Chng WH, Liang J, et al. Plant-derived extracellular vesicles: recent advancements and current challenges on their use for biomedical applications. J Extracell Vesicles. 2022;11:e12283. doi:10.1002/jev2.12283
31. Stanly C, Alfieri M, Ambrosone A, et al. Grapefruit-Derived micro and nanovesicles show distinct metabolome profiles and anticancer activities in the A375 human melanoma cell line. Cells. 2020;9(12):2722. doi:10.3390/cells9122722
32. Yang W, Xing Z, Wang X, et al. Microenvironment-responsive collagen hydrogel with houttuynia cordata thunb vesicles for diabetic wound repair. Int J Biol Macromol. 2025;320:145840. doi:10.1016/j.ijbiomac.2025.145840
33. Zhao Q, Hu QX, Li JP, et al. Morinda officinalis-derived extracellular vesicle-like particles promote wound healing via angiogenesis. ACS Appl Mater Interfaces. 2025;17:30454–30464. doi:10.1021/acsami.5c01640
34. Li Z, Wang H, Yin H, et al. Arrowtail RNA for ligand display on ginger exosome-like nanovesicles to systemic deliver siRNA for cancer suppression. Sci Rep. 2018;8(1):14644. doi:10.1038/s41598-018-32953-7
35. Fang Z, Liu K. Plant-derived extracellular vesicles as oral drug delivery carriers. J Control Release. 2022;350:389–400.
36. Jiang D, Li Z, Liu H, et al. Plant exosome-like nanovesicles derived from sesame leaves as carriers for luteolin delivery: molecular docking, stability and bioactivity. Food Chem. 2024;438:137963. doi:10.1016/j.foodchem.2023.137963
37. Wang Y, Wu Y, Shen S, et al. Engineered plant extracellular vesicles for natural delivery across physiological barriers. Food Funct. 2024;15:1737–1757. doi:10.1039/D3FO03503D
38. Hosseini-Giv N, Basas A, Hicks C, et al. Bacterial extracellular vesicles and their novel therapeutic applications in health and cancer. Front Cell Infect Microbiol. 2022;12:962216. doi:10.3389/fcimb.2022.962216
39. Xie J, Li Q, Haesebrouck F, et al. The tremendous biomedical potential of bacterial extracellular vesicles. Trends Biotechnol. 2022;40(10):1173–1194. doi:10.1016/j.tibtech.2022.03.005
40. Kaparakis-Liaskos M, Ferrero RL. Immune modulation by bacterial outer membrane vesicles. Nat Rev Immunol. 2015;15:375–387. doi:10.1038/nri3837
41. Kim W, Lee EJ, Bae IH, et al. Lactobacillus plantarum-derived extracellular vesicles induce anti-inflammatory M2 macrophage polarization in vitro. J Extracell Vesicles. 2020;9:1793514. doi:10.1080/20013078.2020.1793514
42. Ashrafian F, Keshavarz Azizi Raftar S, Lari A, et al. Extracellular vesicles and pasteurized cells derived from Akkermansia muciniphila protect against high-fat induced obesity in mice. Microb Cell Fact. 2021;20:219. doi:10.1186/s12934-021-01709-w
43. Salehi M, Negahdari B, Mehryab F, et al. Milk-Derived extracellular vesicles: biomedical applications, current challenges, and future perspectives. J Agric Food Chem. 2024;72(15):8304–8331. doi:10.1021/acs.jafc.3c07899
44. Tian MY, Hao DX, Liu Y, et al. Milk exosomes: an oral drug delivery system with great application potential. Food Funct. 2023;14:1320–1337. doi:10.1039/D2FO02013K
45. García-Martínez J, Pérez-Castillo ÍM, Salto R, et al. Beneficial effects of bovine milk exosomes in metabolic interorgan cross-talk. Nutrients. 2022;14(7):1442. doi:10.3390/nu14071442
46. Maghraby MK, Li B, Chi L, et al. Extracellular vesicles isolated from milk can improve gut barrier dysfunction induced by malnutrition. Sci Rep. 2021;11:7635. doi:10.1038/s41598-021-86920-w
47. Miyazawa B, Trivedi A, Togarrati PP, et al. Regulation of endothelial cell permeability by platelet-derived extracellular vesicles. J Trauma Acute Care Surg. 2019;86:931–942. doi:10.1097/TA.0000000000002230
48. Xu N, Wang L, Guan J, et al. Wound healing effects of a Curcuma zedoaria polysaccharide with platelet-rich plasma exosomes assembled on chitosan/silk hydrogel sponge in a diabetic rat model. Int J Biol Macromol. 2018;117:102–107. doi:10.1016/j.ijbiomac.2018.05.066
49. Hayon Y, Dashevsky O, Shai E, et al. Platelet microparticles promote neural stem cell proliferation, survival and differentiation. J Mol Neurosci. 2012;47(3):659–665. doi:10.1007/s12031-012-9711-y
50. Bond AM, Ming GL, Song H. Adult mammalian neural stem cells and neurogenesis: five decades later. Cell Stem Cell. 2015;17:385–395. doi:10.1016/j.stem.2015.09.003
51. Li X, Zhu Y, Wang Y, et al. Neural stem/progenitor cell-derived extracellular vesicles: a novel therapy for neurological diseases and beyond. MedComm. 2023;4(1):e214. doi:10.1002/mco2.214
52. Joshi BS, Zuhorn IS. Heparan sulfate proteoglycan-mediated dynamin-dependent transport of neural stem cell exosomes in an in vitro blood-brain barrier model. Eur J Neurosci. 2021;53:706–719. doi:10.1111/ejn.14974
53. Prieto-Vila M, Yoshioka Y, Kuriyama N, et al. Adult cardiomyocytes-derived EVs for the treatment of cardiac fibrosis. J Extracell Vesicles. 2024;13:e12461. doi:10.1002/jev2.12461
54. Cui GH, Guo HD, Li H, et al. RVG-modified exosomes derived from mesenchymal stem cells rescue memory deficits by regulating inflammatory responses in a mouse model of Alzheimer’s disease. Immun Ageing. 2019;16:10. doi:10.1186/s12979-019-0150-2
55. Kobayashi S, Kondo N, Tomiyama T, et al. Intravenous injection of tumor extracellular vesicles suppresses tumor growth by reducing the regulatory T cell phenotype. Cancer Immunol Immunother. 2023;72:3651–3664. doi:10.1007/s00262-023-03517-0
56. Xu M, Feng T, Liu B, et al. Engineered exosomes: desirable target-tracking characteristics for cerebrovascular and neurodegenerative disease therapies. Theranostics. 2021;11:8926–8944. doi:10.7150/thno.62330
57. Aqil F, Jeyabalan J, Agrawal AK, et al. Exosomal delivery of berry anthocyanidins for the management of ovarian cancer. Food Funct. 2017;8:4100–4107. doi:10.1039/C7FO00882A
58. Cui W, Guo Z, Chen X, et al. Targeting modulation of intestinal flora through oral route by an antimicrobial nucleic acid-loaded exosome-like nanovesicles to improve Parkinson’s disease. Sci Bull. 2024;69:3925–3935. doi:10.1016/j.scib.2024.10.027
59. Zhu MZ, Xu HM, Liang YJ, et al. Edible exosome-like nanoparticles from portulaca oleracea L mitigate DSS-induced colitis via facilitating double-positive CD4(+)CD8(+)T cells expansion. J Nanobiotechnology. 2023;21:309. doi:10.1186/s12951-023-02065-0
60. Rezaie J, Ajezi S, Avci ÇB, et al. Exosomes and their application in biomedical field: difficulties and advantages. Mol Neurobiol. 2018;55:3372–3393. doi:10.1007/s12035-017-0582-7
61. Lin Z, Wu Y, Xu Y, et al. Mesenchymal stem cell-derived exosomes in cancer therapy resistance: recent advances and therapeutic potential. Mol Cancer. 2022;21(1):179. doi:10.1186/s12943-022-01650-5
62. Haney MJ, Klyachko NL, Zhao Y, et al. Exosomes as drug delivery vehicles for Parkinson’s disease therapy. J Control Release. 2015;207:18–30. doi:10.1016/j.jconrel.2015.03.033
63. Ma X, Huang M, Zheng M, et al. ADSCs-derived extracellular vesicles alleviate neuronal damage, promote neurogenesis and rescue memory loss in mice with Alzheimer’s disease. J Control Release. 2020;327:688–702. doi:10.1016/j.jconrel.2020.09.019
64. Cai H, Huang LY, Hong R, et al. Momordica charantia exosome-like nanoparticles exert neuroprotective effects against ischemic brain injury via inhibiting matrix metalloproteinase 9 and activating the AKT/GSK3β signaling pathway. Front Pharmacol. 2022;13:908830. doi:10.3389/fphar.2022.908830
65. Wang X, Han X, Yuan H, et al. Nebulized inhalation of engineered extracellular vesicles to destruct pre-metastatic niche and inhibit postoperative lung metastasis in a mouse model. ACS Nano. 2025;19:35752–35769. doi:10.1021/acsnano.5c12218
66. Li M, Huang H, Wei X, et al. Clinical investigation on nebulized human umbilical cord MSC-derived extracellular vesicles for pulmonary fibrosis treatment. Signal Transduct Target Ther. 2025;10:179. doi:10.1038/s41392-025-02262-3
67. Chen S, Gao J, Zhang T. From mesenchymal stem cells to their extracellular vesicles: progress and prospects for asthma therapy. Asian J Pharm Sci. 2024;19:100942. doi:10.1016/j.ajps.2024.100942
68. Sakurai Y, Ohtani A, Nakayama Y, et al. Logistics and distribution of small extracellular vesicles from the subcutaneous space to the lymphatic system. J Control Release. 2023;361:77–86. doi:10.1016/j.jconrel.2023.07.043
69. Hu Y, Rao SS, Wang ZX, et al. Exosomes from human umbilical cord blood accelerate cutaneous wound healing through miR-21-3p-mediated promotion of angiogenesis and fibroblast function. Theranostics. 2018;8:169–184. doi:10.7150/thno.21234
70. Park D, Kim JH, Yang H, et al. Mesenchymal stem cell-derived extracellular vesicles exert Th1-mediated anti-inflammatory effects via miR-146a/NF-κB pathway: comparison with dupilumab in a mouse model of atopic dermatitis. Stem Cell Res Ther. 2025;16:496. doi:10.1186/s13287-025-04649-z
71. Song M, Ha M, Shin S, et al. A hierarchical short microneedle-cupping dual-amplified patch enables accelerated, uniform, pain-free transdermal delivery of extracellular vesicles. Nanomicro Lett. 2025;18:11. doi:10.1007/s40820-025-01853-7
72. Shah SWA, Li X, Yuan H, et al. Innovative transdermal drug delivery systems: benefits, challenges, and emerging application. BMEMat. 2025;3.
73. Tang Y, Kang Y, Zhang X, et al. Mesenchymal stem cell exosomes as nanotherapeutics for dry age-related macular degeneration. J Control Release. 2023;357:356–370. doi:10.1016/j.jconrel.2023.04.003
74. Li T, Zhang WM, Wang J, et al. Circulating small extracellular vesicles involved in systemic regulation respond to RGC degeneration in glaucoma. Adv Sci. 2024;11:e2309307. doi:10.1002/advs.202309307
75. Lam BWS, Tan M, Gao C, et al. Extracellular vesicles administered via intrathecal injection mediate safe delivery of nucleic acids to the central nervous system for gene therapy. J Extracell Vesicles. 2025;14:e70116. doi:10.1002/jev2.70116
76. Akhlaghpasand M, Tavanaei R, Hosseinpoor M, et al. Safety and potential effects of intrathecal injection of allogeneic human umbilical cord mesenchymal stem cell-derived exosomes in complete subacute spinal cord injury: a first-in-human, single-arm, open-label, phase I clinical trial. Stem Cell Res Ther. 2024;15:264. doi:10.1186/s13287-024-03868-0
77. Woo CH, Kim HK, Jung GY, et al. Small extracellular vesicles from human adipose-derived stem cells attenuate cartilage degeneration. J Extracell Vesicles. 2020;9:1735249. doi:10.1080/20013078.2020.1735249
78. Li H, Feng Y, Zheng X, et al. M2-type exosomes nanoparticles for rheumatoid arthritis therapy via macrophage re-polarization. J Control Release. 2022;341:16–30. doi:10.1016/j.jconrel.2021.11.019
79. Shan Y, Yu M, Dai H, et al. The role of macrophage-derived exosomes in reversing peritoneal fibrosis: insights from astragaloside IV. Phytomedicine. 2024;129:155683. doi:10.1016/j.phymed.2024.155683
80. Yang Y, Yang L, Deng H, et al. Coptis chinensis-derived extracellular vesicle-like nanoparticles delivered miRNA-5106 suppresses NETs by restoring zinc homeostasis to alleviate colitis. J Nanobiotechnology. 2025;23:444. doi:10.1186/s12951-025-03466-z
81. Schuster R, Younesi F, Ezzo M, et al. The role of myofibroblasts in physiological and pathological tissue repair. Cold Spring Harb Perspect Biol. 2023;15(1):a041231. doi:10.1101/cshperspect.a041231
82. Tienda-Vázquez MA, Hanel JM, Márquez-Arteaga EM, et al. Exosomes: a promising strategy for repair, regeneration and treatment of skin disorders. Cells. 2023;12(12):1625. doi:10.3390/cells12121625
83. Chen Y, Huang X, Liu A, et al. Lactobacillus reuteri vesicles regulate mitochondrial function of macrophages to promote mucosal and cutaneous wound healing. Adv Sci. 2024;11:e2309725. doi:10.1002/advs.202309725
84. Lyu L, Cai Y, Zhang G, et al. Exosomes derived from M2 macrophages induce angiogenesis to promote wound healing. Front Mol Biosci. 2022;9:1008802. doi:10.3389/fmolb.2022.1008802
85. Riau AK, Ong HS, Yam GHF, et al. Sustained delivery system for stem cell-derived exosomes. Front Pharmacol. 2019;10:1368. doi:10.3389/fphar.2019.01368
86. Didamoony MA, Soubh AA, Atwa AM, et al. Innovative preconditioning strategies for improving the therapeutic efficacy of extracellular vesicles derived from mesenchymal stem cells in gastrointestinal diseases. Inflammopharmacology. 2023;31(6):2973–2993. doi:10.1007/s10787-023-01350-6
87. Wang L, Hu L, Zhou X, et al. Author Correction: exosomes secreted by human adipose mesenchymal stem cells promote scarless cutaneous repair by regulating extracellular matrix remodelling. Sci Rep. 2021;11:3245. doi:10.1038/s41598-021-82225-0
88. Ruan J, Xia Y, Ma Y, et al. Milk-derived exosomes as functional nanocarriers in wound healing: mechanisms, applications, and future directions. Mater Today Bio. 2025;32:101715. doi:10.1016/j.mtbio.2025.101715
89. Shi Y, Yao F, Yin Y, et al. Extracellular vesicles derived from immune cells: role in tumor therapy. Int Immunopharmacol. 2024;133:112150. doi:10.1016/j.intimp.2024.112150
90. Kim H, Back JH, Han G, et al. Extracellular vesicle-guided in situ reprogramming of synovial macrophages for the treatment of rheumatoid arthritis. Biomaterials. 2022;286:121578. doi:10.1016/j.biomaterials.2022.121578
91. Pei W, Zhang Y, Zhu X, et al. Multitargeted immunomodulatory therapy for viral myocarditis by engineered extracellular vesicles. ACS Nano. 2024;18:2782–2799. doi:10.1021/acsnano.3c05847
92. Černý J, Stříž I. Adaptive innate immunity or innate adaptive immunity? Clin Sci. 2019;133:1549–1565. doi:10.1042/CS20180548
93. Chen Z, Larregina AT, Morelli AE. Impact of extracellular vesicles on innate immunity. Curr Opin Organ Transplant. 2019;24:670–678. doi:10.1097/MOT.0000000000000701
94. Aiello S, Rocchetta F, Longaretti L, et al. Extracellular vesicles derived from T regulatory cells suppress T cell proliferation and prolong allograft survival. Sci Rep. 2017;7:11518. doi:10.1038/s41598-017-08617-3
95. Lindenbergh MFS, Stoorvogel W. Antigen presentation by extracellular vesicles from professional antigen-presenting cells. Annu Rev Immunol. 2018;36:435–459. doi:10.1146/annurev-immunol-041015-055700
96. Li C, Wu F, Mao J, et al. Mesenchymal stem cells-derived extracellular vesicles ameliorate lupus nephritis by regulating T and B cell responses. Stem Cell Res Ther. 2024;15:216. doi:10.1186/s13287-024-03834-w
97. Ou X, Wang H, Tie H, et al. Novel plant-derived exosome-like nanovesicles from Catharanthus roseus: preparation, characterization, and immunostimulatory effect via TNF-α/NF-κB/PU.1 axis. J Nanobiotechnology. 2023;21:160. doi:10.1186/s12951-023-01919-x
98. Chen X, Li Q, Xie J, et al. Immunomodulatory effects of probiotic-derived extracellular vesicles: opportunities and challenges. J Agric Food Chem. 2024;72(35):19259–19273. doi:10.1021/acs.jafc.4c04223
99. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. doi:10.3322/caac.21660
100. Wang F, Yin L, Hu Y. Progress of extracellular vesicles-based system for tumor therapy. J Control Release. 2025;381:113570. doi:10.1016/j.jconrel.2025.02.066
101. Xu J, Liu H, Wang T, et al. CCR7 mediated mimetic dendritic cell vaccine homing in lymph node for head and neck squamous cell carcinoma therapy. Adv Sci. 2023;10:e2207017. doi:10.1002/advs.202207017
102. Wu CH, Li J, Li L, et al. Extracellular vesicles derived from natural killer cells use multiple cytotoxic proteins and killing mechanisms to target cancer cells. J Extracell Vesicles. 2019;8:1588538. doi:10.1080/20013078.2019.1588538
103. Seo N, Shirakura Y, Tahara Y, et al. Activated CD8(+) T cell extracellular vesicles prevent tumour progression by targeting of lesional mesenchymal cells. Nat Commun. 2018;9:435. doi:10.1038/s41467-018-02865-1
104. Aly RG, El-Enbaawy MI, Abd El-Rahman SS, et al. Antineoplastic activity of salmonella typhimurium outer membrane nanovesicles. Exp Cell Res. 2021;399:112423. doi:10.1016/j.yexcr.2020.112423
105. Zhong J, Xia B, Shan S, et al. High-quality milk exosomes as oral drug delivery system. Biomaterials. 2021;277:121126. doi:10.1016/j.biomaterials.2021.121126
106. Sedykh S, Kuleshova A, Nevinsky G. Milk exosomes: perspective agents for anticancer drug delivery. Int J Mol Sci. 2020;21(18):6646. doi:10.3390/ijms21186646
107. Zhao W, Qin P, Zhang D, et al. Long non-coding RNA PVT1 encapsulated in bone marrow mesenchymal stem cell-derived exosomes promotes osteosarcoma growth and metastasis by stabilizing ERG and sponging miR-183-5p. Aging. 2019;11:9581–9596. doi:10.18632/aging.102406
108. Shi S, Zhang Q, Xia Y, et al. Mesenchymal stem cell-derived exosomes facilitate nasopharyngeal carcinoma progression. Am J Cancer Res. 2016;6:459–472.
109. Meng W, Wang L, Du X, et al. Engineered mesenchymal stem cell-derived extracellular vesicles constitute a versatile platform for targeted drug delivery. J Control Release. 2023;363:235–252. doi:10.1016/j.jconrel.2023.09.037
110. Mehdizadeh S, Mamaghani M, Hassanikia S, et al. Exosome-powered neuropharmaceutics: unlocking the blood-brain barrier for next-gen therapies. J Nanobiotechnology. 2025;23:329. doi:10.1186/s12951-025-03352-8
111. Xin W, Pan Y, Wei W, et al. Preconditioned extracellular vesicles from hypoxic microglia reduce poststroke AQP4 depolarization, disturbed cerebrospinal fluid flow, astrogliosis, and neuroinflammation. Theranostics. 2023;13:4197–4216. doi:10.7150/thno.84059
112. Wang Y, Li H, Sun H, et al. A2 reactive astrocyte-derived exosomes alleviate cerebral ischemia-reperfusion injury by delivering miR-628. J Cell Mol Med. 2024;28:e70004. doi:10.1111/jcmm.70004
113. Luo Q, Xian P, Wang T, et al. Antioxidant activity of mesenchymal stem cell-derived extracellular vesicles restores hippocampal neurons following seizure damage. Theranostics. 2021;11:5986–6005. doi:10.7150/thno.58632
114. Nakano M, Kubota K, Kobayashi E, et al. Bone marrow-derived mesenchymal stem cells improve cognitive impairment in an Alzheimer’s disease model by increasing the expression of microRNA-146a in hippocampus. Sci Rep. 2020;10:10772. doi:10.1038/s41598-020-67460-1
115. Wei H, Xu Y, Chen Q, et al. Mesenchymal stem cell-derived exosomal miR-223 regulates neuronal cell apoptosis. Cell Death Dis. 2020;11:290. doi:10.1038/s41419-020-2490-4
116. Chen HX, Liang FC, Gu P, et al. Exosomes derived from mesenchymal stem cells repair a Parkinson’s disease model by inducing autophagy. Cell Death Dis. 2020;11:288. doi:10.1038/s41419-020-2473-5
117. Yu Y, Xu Z, Xu L, et al. Plant extracellular vesicles as emerging neuroprotective agents for central nervous system disorders. J Adv Res. 2026;79:879–889. doi:10.1016/j.jare.2025.03.042
118. Zhang Y, Lu L, Li Y, et al. Response surface methodology optimization of exosome-like nanovesicles extraction from lycium ruthenicum murray and their inhibitory effects on aβ-induced apoptosis and oxidative stress in HT22 cells. Foods. 2024;13.
119. Yu Y, Tan N, Xu Z, et al. Cross-kingdom miRNA delivery by Panax notoginseng-derived extracellular-like nanoparticles vesicles restores neuronal function after ischemic injury. J Nanobiotechnology. 2026;24. doi:10.1186/s12951-026-04103-z
120. Hoffman DJ, Powell TL, Barrett ES, et al. Developmental origins of metabolic diseases. Physiol Rev. 2021;101(3):739–795. doi:10.1152/physrev.00002.2020
121. Zhao H, Shang Q, Pan Z, et al. Exosomes from adipose-derived stem cells attenuate adipose inflammation and obesity through polarizing M2 macrophages and beiging in white adipose tissue. Diabetes. 2018;67:235–247. doi:10.2337/db17-0356
122. Zhao S, Liu Y, Pu Z. Bone marrow mesenchymal stem cell-derived exosomes attenuate D-GaIN/LPS-induced hepatocyte apoptosis by activating autophagy in vitro. Drug Des Devel Ther. 2019;13:2887–2897. doi:10.2147/DDDT.S220190
123. Cho H, Ju H, Ahn Y, et al. Engineered extracellular vesicles with surface FGF21 and enclosed miR-223 for treating metabolic dysfunction-associated steatohepatitis. Biomaterials. 2025;321:123321. doi:10.1016/j.biomaterials.2025.123321
124. Liu B, Lu Y, Chen X, et al. Protective role of shiitake mushroom-derived exosome-like nanoparticles in d-galactosamine and lipopolysaccharide-induced acute liver injury in mice. Nutrients. 2020;12.
125. Mun D, Ryu S, Lee DJ, et al. Bovine colostrum-derived extracellular vesicles protect against non-alcoholic steatohepatitis by modulating gut microbiota and enhancing gut barrier function. Curr Res Food Sci. 2025;10:101039. doi:10.1016/j.crfs.2025.101039
126. Ashrafian F, Shahriary A, Behrouzi A, et al. Akkermansia muciniphila-derived extracellular vesicles as a mucosal delivery vector for amelioration of obesity in mice. Front Microbiol. 2019;10:2155. doi:10.3389/fmicb.2019.02155
127. Zhou ZM, Bao JP, Peng X, et al. Small extracellular vesicles from hypoxic mesenchymal stem cells alleviate intervertebral disc degeneration by delivering miR-17-5p. Acta Biomater. 2022;140:641–658. doi:10.1016/j.actbio.2021.11.044
128. Elashiry M, Elashiry MM, Elsayed R, et al. Dendritic cell derived exosomes loaded with immunoregulatory cargo reprogram local immune responses and inhibit degenerative bone disease in vivo. J Extracell Vesicles. 2020;9:1795362. doi:10.1080/20013078.2020.1795362
129. Qiao Z, Zhang K, Liu J, et al. Biomimetic electrodynamic nanoparticles comprising ginger-derived extracellular vesicles for synergistic anti-infective therapy. Nat Commun. 2022;13:7164. doi:10.1038/s41467-022-34883-5
130. Agency EM. Scientific recommendations on classification of advanced therapy medicinal products. 2025.
131. Administration USFaD. Regulation of human cells, tissues, and cellular and tissue-based products (HCT/Ps): small entity compliance guide. 2022.
132. Agency PaMD. About PMDA: frequently asked questions. Available from: https://www.pmda.go.jp/english/about-pmda/0004.html.
133. Takakura Y, Hanayama R, Akiyoshi K, et al. Quality and safety considerations for therapeutic products based on extracellular vesicles. Pharm Res. 2024;41:1573–1594. doi:10.1007/s11095-024-03757-4
134. Xu G, Jin J, Fu Z, et al. Extracellular vesicle-based drug overview: research landscape, quality control and nonclinical evaluation strategies. Signal Transduct Target Ther. 2025;10:255. doi:10.1038/s41392-025-02312-w
135. Lightner AL, Sengupta V, Qian S, et al. Bone marrow mesenchymal stem cell-derived extracellular vesicle infusion for the treatment of respiratory failure from COVID-19: a randomized, placebo-controlled dosing clinical trial. Chest. 2023;164:1444–1453. doi:10.1016/j.chest.2023.06.024
136. Hyun S, Choi H, Sub Y, et al. Safety and anti-inflammatory effects of engineered extracellular vesicles (ILB-202) for NF-kappaB inhibition: a double-blind, randomized, placebo-controlled phase 1 trial. J Extracell Vesicles. 2025;14:e70141. doi:10.1002/jev2.70141
137. Rakshit T, Pal S. Extracellular vesicles for drug delivery and theranostics in vivo. JACS Au. 2024;4(2):318–327. doi:10.1021/jacsau.3c00611
138. Meng W, He C, Hao Y, et al. Prospects and challenges of extracellular vesicle-based drug delivery system: considering cell source. Drug Deliv. 2020;27(1):585–598. doi:10.1080/10717544.2020.1748758
139. Wang Z, Zhou X, Kong Q, et al. Extracellular vesicle preparation and analysis: a state-of-the-art review. Adv Sci. 2024;11:e2401069.
140. Welsh JA, Goberdhan DCI, O’driscoll L, et al. Minimal information for studies of extracellular vesicles (MISEV2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13:e12404. doi:10.1002/jev2.12404
141. Saint-Pol J, Gosselet F, Duban-Deweer S, et al. Targeting and crossing the blood-brain barrier with extracellular vesicles. Cells. 2020;9(4):851. doi:10.3390/cells9040851
142. An Q, Xiang SR, Zou YQ. Recent progresses in combination cancer therapy using cyanine dye-based nanoparticles. Pharm Sci Adv. 2024;2:100040. doi:10.1016/j.pscia.2024.100040
143. Du S, Guan Y, Xie A, et al. Extracellular vesicles: a rising star for therapeutics and drug delivery. J Nanobiotechnology. 2023;21:231. doi:10.1186/s12951-023-01973-5
144. Herrmann IK, Wood MJA, Fuhrmann G. Extracellular vesicles as a next-generation drug delivery platform. Nat Nanotechnol. 2021;16:748–759. doi:10.1038/s41565-021-00931-2
145. Wei W, Ao Q, Wang X, et al. Mesenchymal stem cell-derived exosomes: a promising biological tool in nanomedicine. Front Pharmacol. 2020;11:590470. doi:10.3389/fphar.2020.590470
146. Ren K. Exosomes in perspective: a potential surrogate for stem cell therapy. Odontology. 2019;107:271–284. doi:10.1007/s10266-018-0395-9
147. Tan F, Li X, Wang Z, et al. Clinical applications of stem cell-derived exosomes. Signal Transduct Target Ther. 2024;9:17. doi:10.1038/s41392-023-01704-0
148. Tolomeo AM, Zuccolotto G, Malvicini R, et al. Biodistribution of intratracheal, intranasal, and intravenous injections of human mesenchymal stromal cell-derived extracellular vesicles in a mouse model for drug delivery studies. Pharmaceutics. 2023;15(2):548. doi:10.3390/pharmaceutics15020548
149. Zhang L, Huang B, Jin J, et al. Advances in nanoprobes-based immunoassays. BMEMat. 2024;2(1). doi:10.1002/bmm2.12057
150. Charoenviriyakul C, Takahashi Y, Morishita M, et al. Role of extracellular vesicle surface proteins in the pharmacokinetics of extracellular vesicles. Mol Pharm. 2018;15(3):1073–1080. doi:10.1021/acs.molpharmaceut.7b00950
151. Morishita M, Takahashi Y, Nishikawa M, et al. Quantitative analysis of tissue distribution of the B16BL6-derived exosomes using a streptavidin-lactadherin fusion protein and iodine-125-labeled biotin derivative after intravenous injection in mice. J Pharm Sci. 2015;104:705–713. doi:10.1002/jps.24251
152. Ghodasara A, Raza A, Wolfram J, et al. Clinical translation of extracellular vesicles. Adv Healthc Mater. 2023;12(28):e2301010. doi:10.1002/adhm.202301010
153. Schwarz G, Ren X, Xie W, et al. Engineered exosomes: a promising drug delivery platform with therapeutic potential. Front Mol Biosci. 2025;12:1583992. doi:10.3389/fmolb.2025.1583992
154. Zhang J, Zhang Y, Khanal S, et al. Synthetic gRNA/Cas9 ribonucleoprotein targeting HBV DNA inhibits viral replication. J Med Virol. 2023;95:e28952. doi:10.1002/jmv.28952
155. Wang W, Gao R, Zhang L, et al. Fuel-propelled nanomotors for acute kidney injury applications. Pharm Sci Adv. 2024;2:100044. doi:10.1016/j.pscia.2024.100044
156. Tang M, Ni J, Yue Z, et al. Polyoxometalate-Nanozyme-Integrated nanomotors (POMotors) for self-propulsion-promoted synergistic photothermal-catalytic tumor therapy. Angew Chem Int Ed Engl. 2024;63:e202315031. doi:10.1002/anie.202315031
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Application and Challenges of Stem Cell-Derived Extracellular Vesicles in Inhalation Lung Injury

Ling D, Wang R, Liu J, Zhai J, Chen J, Li Y, Liu H, Tai Z, Wei H
International Journal of Nanomedicine 2026, 21:564787
Published Date: 8 January 2026
Plant-Derived Nanovesicles: Resolving Conceptual Confusion, Overcoming Isolation Challenges, and Advancing Translational Potential
Zhang Z, Chen G, Zheng K, Lin M, Zheng D, Lu Y, Huang L, Chen X, Gan R
International Journal of Nanomedicine 2026, 21:592968
Published Date: 29 April 2026