Back to Journals » International Journal of Nanomedicine » Volume 21
The Application and Challenges of Stem Cell-Derived Extracellular Vesicles in Inhalation Lung Injury
Authors Ling D, Wang R, Liu J, Zhai J, Chen J, Li Y, Liu H, Tai Z ![]() , Wei H
, Wei H
Received 2 September 2025
Accepted for publication 13 December 2025
Published 8 January 2026 Volume 2026:21 564787
DOI https://doi.org/10.2147/IJN.S564787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. RDK Misra
Dandan Ling,1,* Ruidong Wang,2,* Jun Liu,3,* Jingwen Zhai,1 Jiani Chen,1 Yaqiong Li,1 Hong Liu,1 Zongguang Tai,3 Hua Wei1
1Department of Good Clinical Practice, Medical Guarantee Center, Second Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China; 2Clinical Research Institute, Department of Good Clinical Practice, Third Affiliated Hospital of Naval Medical University, Shanghai, People’s Republic of China; 3Shanghai Skin Disease Hospital, School of Medicine, Tongji University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hua Wei, Email [email protected] Zongguang Tai, Email [email protected]
Abstract: Inhalation-induced lung injury, caused by harmful factors like chemical fumes and dust, leads to acute and chronic inflammation and fibrosis. Traditional treatments, such as mechanical ventilation and anti-inflammatory drugs, can relieve symptoms but fail to promote tissue regeneration. Stem cells and their extracellular vesicles (EVs) offer new treatment possibilities due to their anti-inflammatory and regenerative properties. However, the specific pathological environment of these lung injuries limits the effectiveness and targeting of EVs, challenging their clinical use. This review outlines stem cell EVs’ mechanisms in treating inhalation-induced lung injury, examines recent engineering advancements, and addresses challenges in moving from research to clinical application. It highlights the importance of interdisciplinary collaboration in carrier design, production, and regulation, offering a theoretical foundation for developing precision EV-based treatments.
Keywords: stem cells, extracellular vesicles, inhalation lung injury, optimization strategy, clinical translation
Graphical Abstract:

Introduction
Inhalation lung injury represents a prevalent and severe condition within medical practice, characterized by a complex pathogenesis and challenging treatment modalities. This condition may arise from incidents such as fires, industrial accidents, and exposure to hazardous environments, including chemical leaks, elevated dust concentrations, pathogen aerosols, and high-temperature gases or shock waves generated by explosions, all of which can result in varying degrees of respiratory tract damage (Figure 1). Pathological investigations have demonstrated that this disease follows a distinct biphasic progression pattern: the acute phase, occurring within 72 hours post-injury, is predominantly marked by uncontrolled inflammatory cascade reactions and the disruption of the alveolar-capillary barrier; the chronic phase, extending from several weeks to several months, is characterized by progressive pulmonary fibrosis and irreversible structural remodeling of the tissue.1–3 Epidemiological data from the US National Burn Database indicate that among approximately 40,000 burn patients hospitalized annually, 5% also suffer from inhalation lung injury; the mortality rate for these patients increases by 60% after they develop pneumonia,4–6 underlining the serious clinical challenges posed.
 |
Figure 1 External factors contributing to inhalation lung injury. |
Current clinical treatments for inhalation-induced lung injury mainly involve supportive measures like mechanical ventilation and broad-spectrum anti-inflammatory drugs.1 While these approaches temporarily stabilize patients, they face two key limitations: first, they fail to regulate the pro-/anti-inflammatory balance during the acute phase; second, they cannot halt the vicious cycle of abnormal extracellular matrix deposition in chronic stages.7,8 Crucially, traditional therapies do not effectively promote alveolar epithelial regeneration or functional lung unit reconstruction, often resulting in long-term respiratory impairment and diminished quality of life for survivors.8,9
Recently, mesenchymal stem cells (MSCs) therapy has emerged as a promising approach for lung injury repair due to its notable tissue repair and immunomodulatory properties.10,11 While MSCs promote tissue regeneration via paracrine mechanisms, challenges including immune rejection, tumorigenic risk, and poor survival limit the efficacy of stem cell transplantation.12–15
Research indicates that the therapeutic effects of stem cells are largely mediated by their secreted EVs, particularly exosomes. These EVs can replicate stem cell functions while offering advantages like high stability, low immunogenicity, and ease of storage/delivery, providing a novel cell-free approach for treating lung damage.16 MSC-derived EVs inherit their parent cells’ therapeutic properties and possess three distinct advantages: 1) nanoscale size enhances tissue penetration;17 2) a phospholipid bilayer protects cargo stability;18 3) low immunogenicity minimizes rejection risks.15,19–21 The repair mechanisms of stem cell EVs in lung injury include: 1) regulating macrophage polarization to suppress excessive inflammation;22 2) promoting alveolar epithelial and vascular endothelial cell proliferation while reducing apoptosis;23 3) alleviating oxidative stress damage;24 4) inhibiting fibroblast activation and slowing pulmonary fibrosis progression.25 Enhancing vesicle targeting and efficacy can be achieved by genetic engineering or chemical modification.18,26
Despite the therapeutic potential of stem cell-derived EVs in preclinical studies, their clinical translation faces significant challenges. These include standardizing large-scale production, determining optimal administration routes, and assessing long-term safety. Additionally, the distinct pathological microenvironment of inhalation-induced lung injury poses multiple barriers: during the acute phase, reactive oxygen species (ROS) can degrade EVs functional components, while the dense fibrotic matrix in chronic phases severely impedes targeted EVs delivery.4,27–29 To address these challenges, this review establishes a “spatiotemporal dynamic regulation” framework, systematically exploring: 1) EVs molecular mechanisms across pathological stages; 2) recent advances in engineered modification strategies; and 3) clinical translation bottlenecks. By integrating multi-omics data and advanced nanotechnology, we emphasize smart responsive EVs carrier design principles to inform precision treatment strategies. Finally, we advocate establishing a “basic-translational-clinical” R&D continuum to streamline EVs therapy translation from bench to bedside.
Biological Characteristics of Stem Cell EVs
Stem cells possess the capability to self-renew, differentiate into multiple types, and regenerate tissues that are functional.30 Based on their differentiation potential, they are classified into totipotent, pluripotent, multipotent, oligopotent, and unipotent stem cells. Pluripotent stem cells include embryonic stem cells (ESCs) and induced pluripotent stem cells (iPSCs), while adult multipotent stem cells comprise hematopoietic stem cells (HSCs), mesenchymal stem cells (MSCs), neural stem cells (NSCs), and endothelial progenitor cells (EPCs).15 These subtypes are widely used in clinical trials for treating human diseases. This review focuses on EVs derived from MSCs for treating lung injuries caused by inhaled toxins.
MSCs are adult multipotent stem cells present in bone marrow, umbilical cord, placenta, adipose tissue, and dental pulp (Figure 2A). These non-terminally differentiated cells exhibit features of both mesenchymal cells and endothelial or epithelial cells. Their multipotent differentiation capacity enables them to stimulate growth, survival, and repair in other cells, making them a subject of significant interest.31 Nonetheless, certain trials have not demonstrated clinical advantages, possibly because of the intrinsic limitations of stem cell therapy, such as infusion toxicity, immune response, and the potential to cause tumors. Notably, MSCs-derived EVs can directly interact with target cells, acting as intercellular communication mediators, and can be engineered as drug carriers to deliver miRNAs and small-molecule drugs. Importantly, they are associated with minimal risks of immune reactions and tumor formation32(Figure 2B). Through multiple pathways, these agents modulate the biological behavior of target cells, thereby regulating physiological homeostasis and/or the progression of human diseases.33
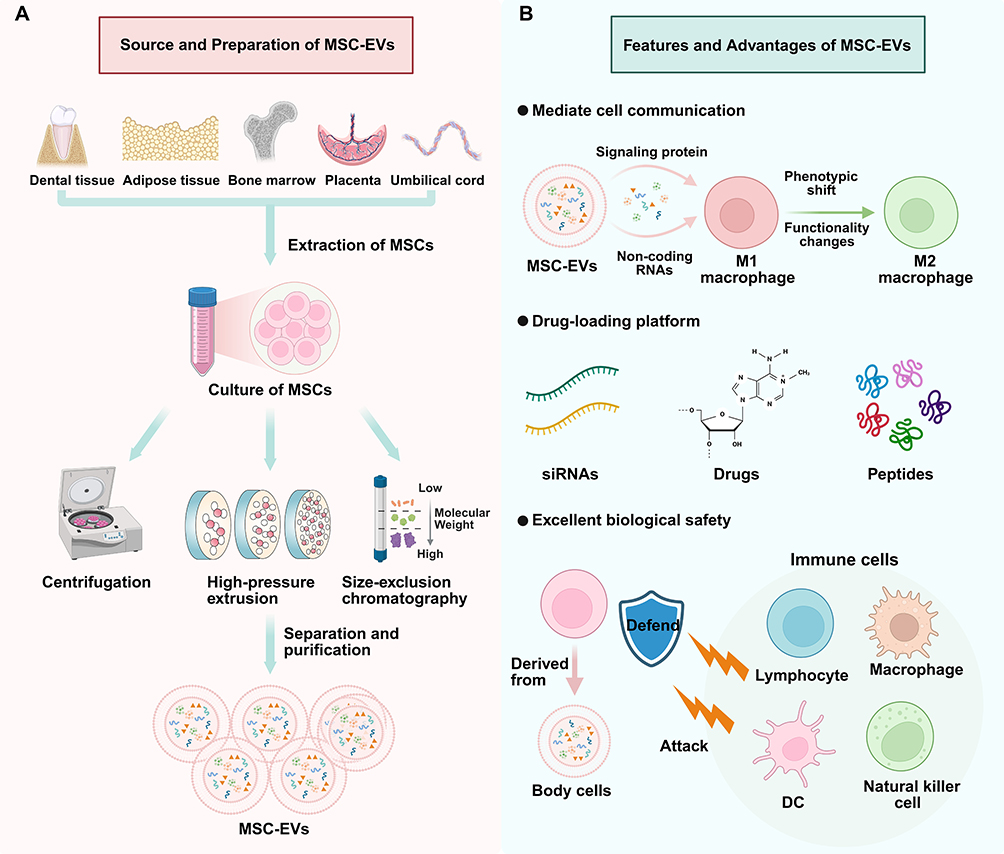 |
Figure 2 The origin and biological characteristics of extracellular vesicles. (A) The sources of EVs and their purification and separation preparation process; (B) the characteristics and advantages of EVs: extracellular vesicles have excellent biological safety and can be used as a medium for cell communication and a carrier platform for drug delivery. |
MSC-EVs, which are small vesicles with biological activity, are secreted by MSCs and have a double-layer lipid membrane structure.34 They carry numerous proteins associated with membrane transport and fusion, including adhesion proteins, ESCRT components, and Rab-GTPases. Additionally, EVs contain common membrane surface markers such as tetraspanins (CD9, CD63, CD81, CD82) and heat shock proteins (HSP70), along with various miRNAs/mRNAs, metabolites, growth factors, and cytokines.35,36 EVs are nanoscale particles actively secreted by cells. Based on their biogenesis pathways, size, contents, and functions, EVs are broadly categorized into three types: apoptotic bodies (50–2000 nm), microvesicles (50–1,000 nm), and exosomes (40–160 nm).37–39 The overlapping size ranges among these categories underscore the limitations of this classification system.40
The vesicles cited in several studies are essentially referring to the broader category of EVs.41 As stated in the 2023 Minimal information for studies of EVs (MISEV2023),39 EVs refers to particles that are released from cells, are delimited by a lipid bilayer, and cannot replicate on their own. Exosomes are a subtype of EVs that differ in their biogenesis from microvesicles and apoptotic bodies. They originate from the endosomal pathway, a process through which multivesicular bodies (MVBs) are formed and subsequently released from the cell. MVBs can either integrate with lysosomes for degradation or with the cell membrane to release EVs into the extracellular space, depending on their final outcome16,42,43 (Figure 3).
 |
Figure 3 The generation process and molecular composition of EVs. Generation process: Various extracellular components, including proteins and lipids, are internalized to form early endosomes; early endosomes differentiate into late endosomes, forming multivesicular bodies (MVBs); MVBs fuse with microtubules and the cytoskeleton and then fuse with the plasma membrane to form EVs. The remaining MVBs are transported and fuse with lysosomes to degrade their cargo. EVs enter recipient cells through various pathways, including endocytosis, uptake, phagocytosis, and fusion. |
Compared to conventional stem cell therapy, MSC-EVs exhibit superior clinical translation potential. Their nanoscale size and lipid bilayer structure enable efficient penetration of the pulmonary capillary network and blood-air barrier while avoiding the embolism and tumorigenesis risks associated with live cell infusion. Furthermore, MSC-EVs maintain biological activity during long-term storage at −80 °C, providing critical assurance for clinical emergency use.44–46
The Molecular Mechanism of Stem Cell EVs Repairing Inhalation Lung Injury
Although EVs derived from stem cells (particularly MSCs) exhibit significant advantages in treating inhalation lung injury, critical challenges remain in practical application. This progression occurs in two phases: the acute inflammation stage and the chronic fibrosis stage. The pathological microenvironments of these two stages differ significantly, necessitating MSC-EVs to exert stage-specific reparative effects by regulating molecular mechanisms across multiple dimensions (Figure 4). Elucidating the mechanisms of MSC-EVs in distinct disease stages is fundamental to optimizing therapeutic strategies and advancing clinical translation.
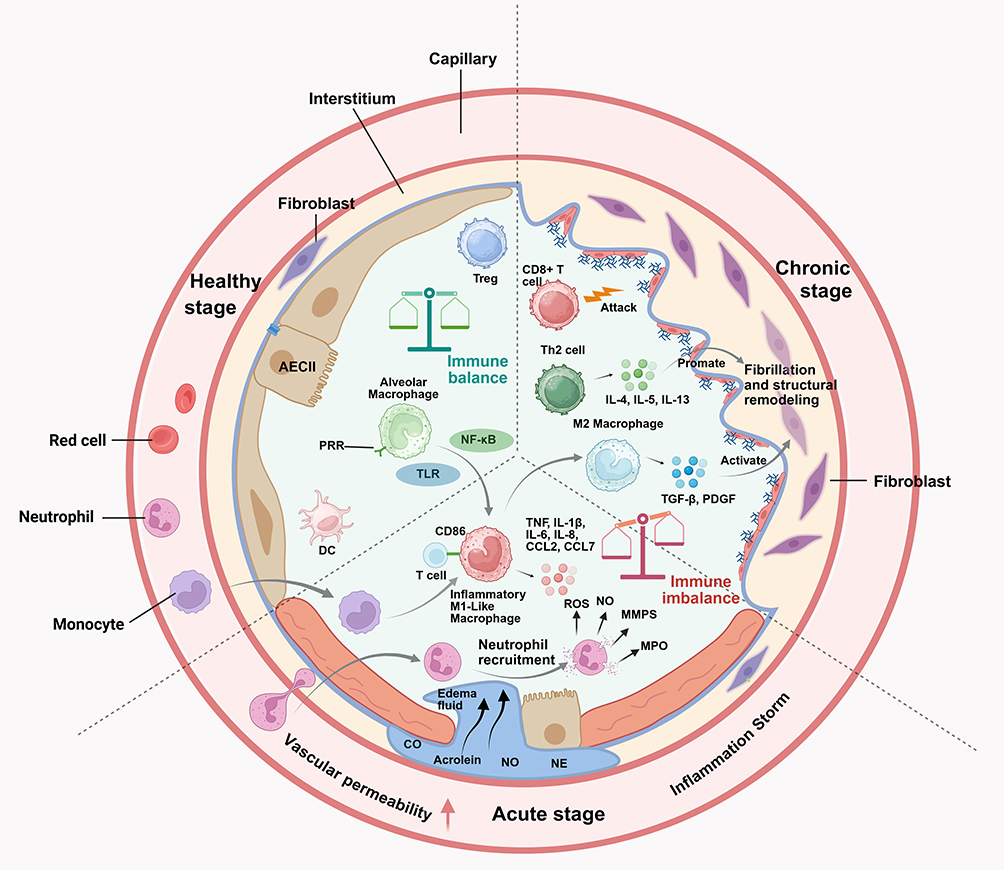 |
Figure 4 Schematic diagram of the therapeutic effects of EVs in the treatment of inhalation-induced lung injury. During the acute phase, EVs inhibit inflammatory cascades through multi-targeted interventions; during the chronic phase, they exert their effects by targeting and inhibiting signaling pathways such as TGF-β1/Smad3d; eNOS: endothelial nitric oxide synthase. |
Acute Phase of Inhalation Lung Injury
Acute lung injury (ALI) is defined as damage to the alveolar epithelium and capillary endothelium resulting from direct or indirect injury, which leads to diffuse pulmonary edema and acute hypoxic respiratory failure. Its pathological hallmarks include bronchial mucosal edema, increased permeability of the alveolar-capillary barrier, prominent neutrophil infiltration, extensive release of inflammatory mediators, and severe oxidative stress. Inhalation lung injury occurs following exposure to toxic agents, with the acute phase typically developing within days. However, the time to onset may vary depending on the type and concentration of the inhaled toxin; highly toxic agents at high concentrations can induce injury within hours.4 Toxic substances in smoke, such as carbon monoxide, can directly damage airway epithelial cells and activate Toll-like receptors (TLRs) and the nuclear factor kappa-B (NF-κB) signaling pathway. This activation leads to the massive release of pro-inflammatory factors, including IL-6 and TNF-α. These factors recruit neutrophils, triggering a “respiratory burst” that produces ROS and myeloperoxidase (MPO) proteases, thereby exacerbating tissue damage.47
At this stage, EVs inhibit inflammatory cascades through multi-targeted interventions. Bone marrow mesenchymal stem cell-derived EVs deliver miR-146a and miR-181c, which target and suppress the TLR4/NF-κB pathway. This reduces IL-8 and TNF-α expression while decreasing neutrophil chemotaxis and infiltration.48–51 Additionally, EVs transport enriched superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx), enzymes that directly scavenge ROS and thereby alleviate oxidative stress-induced damage.52,53 Zhao et al demonstrated that inhalation of MSC-EVs in LPS-stimulated RAW264.7 cells and an ALI mouse model contributes to the efficacy of MSC-EVs in treating LPS-induced ALI, macrophage polarization, and Nrf2-mediated antioxidant signaling. The study showed that MSC-EVs significantly downregulated pro-inflammatory pathways (eg, TLR4/NF-κB) and upregulated the Nrf2/HO-1 antioxidant axis, reducing oxidative damage markers including 8-OHdG. These findings suggest that MSC-EVs exert dual therapeutic effects through modulating inflammation and oxidative stress54 (Figure 5). In a mouse model of silica-induced lung injury, EVs promote macrophage polarization toward the M1 phenotype via miR-223-3p delivery, inhibit IL-1β and TNF-α secretion, and reduce inflammation and pulmonary fibrosis severity.55
 |
Figure 5 The influence of MSC-EVs on macrophage polarization in LPS-stimulated cell and animal models. ns: no significance. ns P > 0.05, ⁎P < 0.05, ⁎⁎P < 0.01, ⁎⁎⁎P < 0.001, ⁎⁎⁎⁎P < 0.0001. (A) Regulation of Key Proteins by MSC-EVs. (B–G): Inflammatory Factors Suppressed, Antioxidant Proteins Activated. (H) MSC-EVs Reduce Oxidative Stress. Representative images display double immuno-staining with ED1 (macrophage marker, green) and 8-OHdG (oxidative stress marker, red) in each group. Left image of each group, bar = 100 μm; right image of each group, bar = 25 μm. (I): Dynamic Changes in Proteins In Vivo. (J–N): MSC-EVs Inhibit TLR4/NF-κB and Activate Nrf2 Pathway. (O): MSC-EVs mitigate oxidative damage in vivo, Bottom image of each group, bar = 50 μm; top image of each group, bar = 20 μm. (A–O). Come from Ruijing Zhao, Lina Wang, Tian Wanget al, Inhalation of MSC-EVs is a noninvasive strategy for ameliorating acute lung injury. J Control Release. 2022; 345: 214–30. © 2022 The Authors. Published by Elsevier B.V. Creative Commons CC-BY-NC-ND.54 |
Chronic Phase of Inhalation Lung Injury
Long-term exposure to harmful substances can induce persistent lung tissue inflammation. Repeated inflammatory stimulation and aberrant repair processes drive continuous fibrous tissue proliferation, advancing to the chronic phase. The fibrotic stage is characterized by fibroblast activation, excessive extracellular matrix (ECM) deposition, and substantial alveolar structural damage.4,56 Pulmonary fibrosis is primarily driven by persistent activation of the TGF-β1/Smad signaling pathway, which induces fibroblast-to-myofibroblast transformation and enhances collagen and fibronectin synthesis.56 The TGF-β/Smad pathway exerts bidirectional effects in EV-mediated fibrosis regulation: low TGF-β1 concentrations promote tissue repair, whereas high concentrations exacerbate fibrosis, warranting further validation of EV dose-dependency.57–59
EVs counteract this vicious cycle through the delivery of anti-fibrotic molecules. Studies demonstrate that EVs derived from bone marrow mesenchymal stem cells (BMSCs-EVs) significantly suppress fibroblast activation and proliferation, mitigating pathological changes associated with pulmonary fibrosis. Zhou and his team discovered that BMSC-EVs are loaded with miR-186, which is markedly lower in the lung tissues of patients diagnosed with idiopathic pulmonary fibrosis (IPF). EV-delivered miR-186 is internalized by pulmonary fibroblasts and acts by directly targeting and suppressing the transcription factor SOX4. This effectively blocks fibroblast activation, migration, and invasion while promoting apoptosis, ultimately attenuating histological damage and collagen deposition in a mouse model of pulmonary fibrosis60 (Figure 6). In another study, three-dimensionally cultured human umbilical cord mesenchymal stem cell exosomes (UCMSC-EVs) were shown to effectively inhibit pulmonary fibrosis progression in a silicosis model. Xu et al showed that UCMSC-EVs target lung tissue and internalize into fibroblasts, significantly reducing collagen I (COL1A1) and fibronectin (FN) expression at both gene and protein levels, and improving lung function. The mechanism likely involves exosome-carried active components regulating downstream fibrotic signaling in the TGF-β/Smad pathway, providing experimental evidence for EV-based anti-fibrotic therapy.61
 |
Figure 6 EV-delivered miR-186 decreases the expression of DKK1 through targeting SOX4 to impair fibroblast activation. *p < 0.05 vs the fibroblasts co-transfected with scramble and oe-NC; #p < 0.05 vs the fibroblasts co-transfected with sh-SOX4 and oe-NC. (A) DKK1 expression positively correlates with SOX4 expression. (B-E) Validates the regulatory axis of SOX4-DKK1. (F–K) Reveals its functional role in fibroblast activation. (L–M) Exosome-delivered miR-186 mediates this axis. (A–M) come from Zhou J, Lin Y, Kang X, Liu Zet al, Microrna-186 in extracellular vesicles from bone marrow mesenchymal stem cells alleviates idiopathic pulmonary fibrosis via interaction with sox4 and dkk1. Stem Cell Res Ther. 2021; 12: 96. © 2023 The Authors. This work is published and licensed by Springer Nature limited. Minor adjustments have been made to the order of the content. The full terms of this license are available at http://creativecommons.org/licenses/by/4.0/.60 |
Dynamic Regulation: Integrated Effects from Acute to Chronic Conditions
The therapeutic benefit of EVs stems from their capacity to modify target sites in response to the changing microenvironment of injured tissues.62,63 During the acute phase of high oxidative stress, CD44 and integrins on EVs surfaces selectively bind to injured endothelial cells, rapidly releasing antioxidant enzymes;62,64 while in the chronic phase, EVs target fibrotic regions and regulate fibroblast metabolism by delivering miRNAs.65 This spatiotemporal specificity arises from the heterogeneous nature of EVs cargo and their microenvironment-responsive release. Recent studies also indicate that engineering EVs surface ligands (eg, CXCR4) can enhance their targeting efficiency to injured lung tissue, improving therapeutic outcomes.66 Table 1 summarizes studies on the application of stem cell-derived EVs for treating inhalation lung injuries.
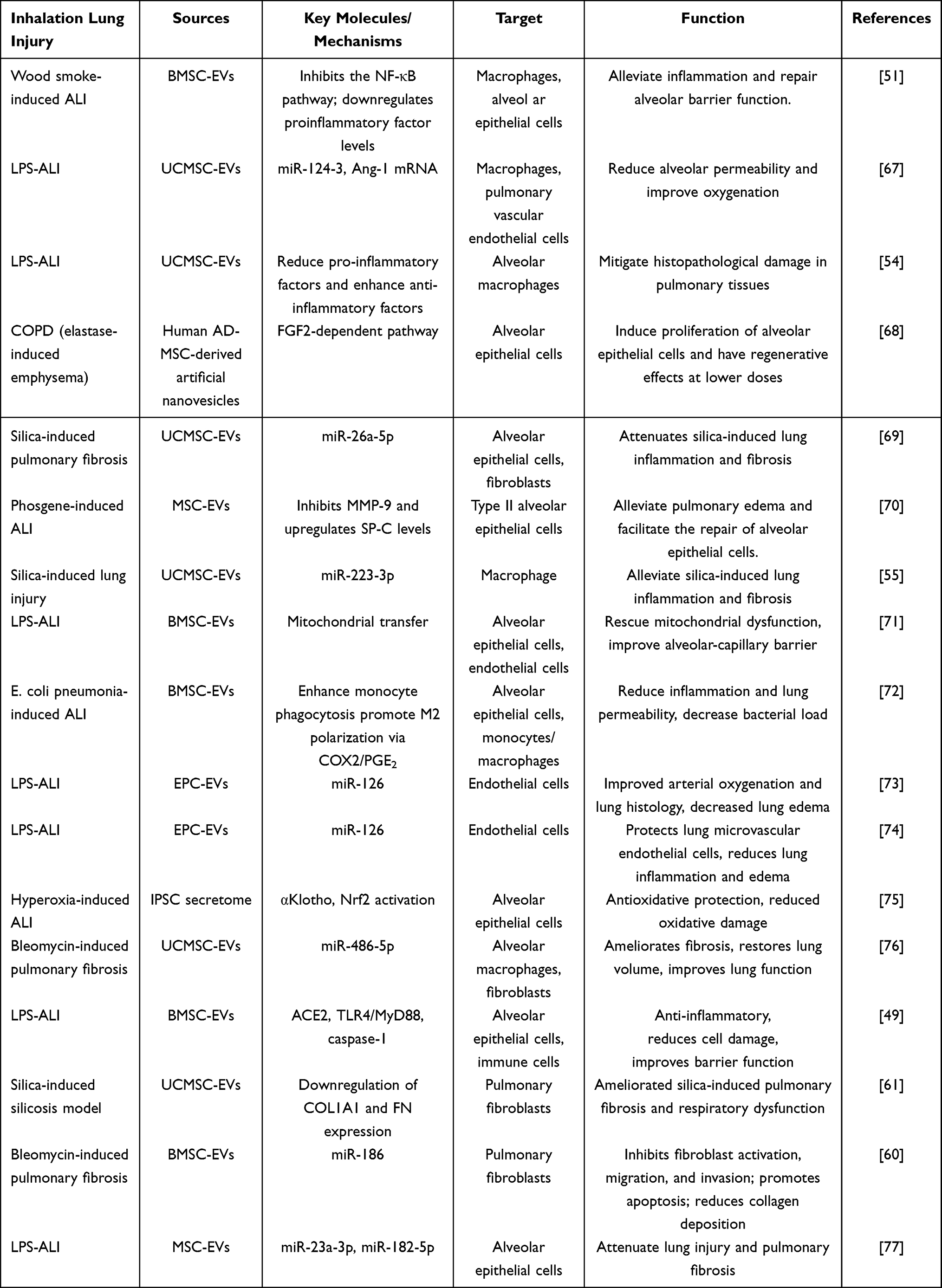 |
Table 1 Research on EVs Derived from Stem Cells in the Treatment of Inhalation Lung Injury |
EVs exhibit broad repair capabilities across pathological stages through the synergistic action of multiple components. Inhalation-induced lung injury is characterized by pathological changes, including a thickened mucous layer and heightened oxidative stress. This unique pathological microenvironment can impair the targeting efficiency and functional stability of EVs.78,79 Elevated ROS concentrations degrade EVs surface proteins, compromising their stability; increased collagen components in the fibrotic matrix may impede EVs diffusion,80 limiting bioavailability. Thus, optimizing EVs targeting efficiency and functional stability through engineering strategies is essential for refining therapeutic approaches and enabling clinical translation.
Optimization Strategies for EVs in Inhalation Injury Scenarios
The repair efficacy of EVs is closely linked to their intrinsic biological characteristics and targeting efficiency. Targeting the pathological features of inhalation-induced lung injury – such as oxidative stress, inflammatory cascade reactions, and disruption of the air-blood barrier – a systematic treatment system can be constructed through three approaches: stem cell pretreatment, engineered modification of EVs, and optimization of drug delivery routes.
Stem Cell Pretreatment
Pre-treatment strategies for stem cells represent a key approach for enhancing EVs secretion and modulating their functions.81,82 Exposing progenitor cells to hypoxia, inflammatory factors (such as TNF-α or IL-1β), or ROS significantly upregulates the expression of antioxidant enzymes (SOD3 and GPX4) and anti-inflammatory factors (TSG-6 and IL-10) within EVs.83,84 Studies have demonstrated that hypoxia pretreatment significantly elevates the content of HIF-1α-mediated pro-repair proteins in EVs derived from MSCs.85 Furthermore, advances in gene editing technology have enabled precise regulation of EVs contents. Introducing miRNA overexpression vectors into stem cells via lentiviral transfection yields EVs whose miRNAs effectively inhibit NF-κB pathway activation in alveolar epithelial cells.86,87
Modification of EVs
EVs can enhance disease treatment outcomes through two strategies: internal modification (eg, drug loading) and external modification (eg, surface modification).88 For instance, genetic engineering to overexpress the CXCR4 receptor on EV surfaces enables homing to lung injury sites with elevated SDF-1α levels, thereby mitigating lung damage.66 Similarly, CD38 antigen receptor-modified MSCs-EVs improved targeting efficiency toward type II alveolar epithelial cells, alleviating pulmonary fibrosis.89 However, these strategies present a critical trade-off: the introduction of exogenous proteins can fundamentally alter the natural EVs membrane composition and topology. This may disrupt the function of endogenous targeting ligands (eg, integrins) that mediate natural tissue tropism, potentially compromising the inherent homing capabilities of EVs even as new ones are introduced.90,91
Biomaterial integration techniques, such as liposome fusion or surface ligand anchoring, can endow EVs with targeting capabilities for damaged sites. Conjugating peptides and nanobodies to EVs via enzymatic reactions can mitigate non-specific phagocytosis and increase in vivo circulation.92–94 A pivotal consideration here is the application of “stealth” coatings like polyethylene glycol (PEG) to evade immune clearance.95 While PEGylation effectively prolongs circulation half-life by reducing opsonization and mononuclear phagocyte system uptake, it acts as a double-edged sword.96,97 The polymer chains create a steric barrier that can physically mask not only immunogenic epitopes but also the very surface proteins and glycans responsible for the EV’s innate targeting specificity.96 This trade-off between enhanced bioavailability and diminished natural targeting efficiency necessitates a delicate balance in carrier design.98 Furthermore, the chemical crosslinkers or synthetic lipid components used in these processes introduce novel immunogenic risks, such as complement activation or the generation of anti-PEG antibodies upon repeated administration.99,100
Internally, EVs can be loaded with therapeutic cargo like hyaluronic acid for sustained-release.101 Nonetheless, the intrinsic cargo capacity of EVs is physically limited. Techniques to enhance loading (eg, electroporation, sonication) often compromise EVs membrane integrity, leading to aggregation and reduced yield.102 Consequently, achieving therapeutic drug concentrations frequently requires high EVs doses, making loading efficiency a significant bottleneck that can offset the benefits of engineered delivery.103
From a translational perspective, scalability remains a paramount challenge. Techniques like lentiviral transfection, though precise, are labor-intensive and prone to batch-to-batch variability, hindering consistent, large-scale production of clinical-grade engineered EVs.104 A critical comparison of strategies reveals that while genetic engineering offers high precision, it faces scalability hurdles; chemical methods provide flexibility but carry higher immunogenic risk.103,105 Therefore, the choice of modification must be guided by a holistic view of the intended application, weighing the imperative for enhanced efficacy against the constraints of biocompatibility, manufacturing feasibility, and regulatory pathways.
Optimizing the Route of Administration
Currently, EVs are primarily administered intravenously. However, intravenous delivery faces multiple biological barriers, including adsorption of EVs’ surface-targeted molecules by serum proteins in the bloodstream and mechanical entrapment in the pulmonary capillary bed.106,107 In patients with inhalation-induced lung injury, enhanced mucociliary clearance and airway mucosal edema result in shorter retention times for EVs and reduced targeting efficiency.54,68,108–110 Conversely, nebulized inhalation allows for direct delivery to the airways, accessing damaged tissue.111 It significantly enhances EVs’ penetration through the mucus layer, increasing their deposition rate in the bronchi and lungs.112–114
While unmodified EVs possess inherent therapeutic potential, their efficacy can be significantly enhanced through engineering for specific cell targeting. Research demonstrates that in chronic obstructive pulmonary disease models, unmodified EVs exhibit substantially shorter airway retention times compared to modified counterparts.90,115
In summary, while engineering modifications have greatly enhanced the therapeutic potential of EVs, their clinical translation still faces three major challenges. Safety concerns involve the potential impact of exogenous components on biocompatibility, as well as the need for systematic evaluation of immunogenicity and in vivo metabolic behavior. Technologically, scaling up from laboratory to GMP-grade production poses challenges in reproducibility, purity, and cost control. Strategically, the absence of head-to-head comparisons among different modification approaches in terms of targeting, drug loading, stability, and efficacy impedes the selection of optimal solutions for specific applications.116,117 Moving forward, AI-driven design and high-throughput screening using organ-on-a-chip technologies could help balance functionality and safety, while also facilitating the development of scalable and standardized protocols.118
Preclinical Research and Challenges
In preclinical studies of EVs for inhalation-induced lung injuries, selecting relevant animal models and understanding the biological properties of EVs from different sources are crucial for clinical translation. However, current research challenges are primarily manifested in two key aspects: First, insufficient standardization of model systems creates a “species gap” in efficacy assessment, hindering the direct translation of findings from different species models to human clinical settings. Second, heterogeneity in cellular sources causes “batch variability” in therapeutic effects, compromising the consistency and reliability of EV treatment outcomes.
Diversity Analysis and Translational Applicability of Animal Models
In preclinical studies of inhalation lung injury, the choice of animal model directly influences the clinical translational value of experimental outcomes. The pathological mechanisms of smoke inhalation injury are complex, involving airway thermal injury, toxic gas-induced inflammatory cascades, oxidative stress, and tissue repair dysfunction. Consequently, selecting animal models with anatomical structures and physiological responses closely resembling humans’ is crucial for addressing specific research questions.
Rodents, particularly mice and rats, are widely employed in mechanistic studies and gene-targeted therapy research owing to their highly editable genomes.119,120 Mouse models offer particular value for elucidating regulatory mechanisms of inflammatory signaling pathways such as NF-κB and MAPK. However, they lack bronchial mucous glands and respiratory bronchioles, limiting their applicability in studies of mucus hypersecretion or airway remodeling.121–123 Conversely, guinea pigs exhibit a respiratory tract branching pattern closer to humans, with tracheal epithelium rich in goblet and ciliated cells, making them well-suited for modeling chronic airway disease pathology.124,125
The anatomical similarity of sheep and pig lungs to human lungs makes them ideal models for assessing the clinical feasibility of treatment methods.126,127 Sheep bronchial mucus secretion characteristics, alveolar-capillary barrier function, and inflammatory response patterns closely resemble the pathological features observed in human burn patients with inhalation injuries. These similarities make sheep commonly used to assess airway obstruction, pulmonary edema, and the efficacy of mechanical ventilation interventions.128 Pigs are commonly used to test drug delivery systems or biomaterial scaffolds because their thoracic cavity volume and cardiopulmonary parameters closely resemble those of humans.129,130 Non-human primates (eg, monkeys) exhibit tissue structures, physiological functions, and immune systems most similar to humans, making them ideal models for studying respiratory diseases and evaluating inhaled drugs or toxins (Table 2). However, large animal studies entail high costs and scarcity of targeted immunological reagents, limiting their utility in high-throughput screening.131 Ethical concerns and technical complexities further constrain their application in preclinical research.2,132–134
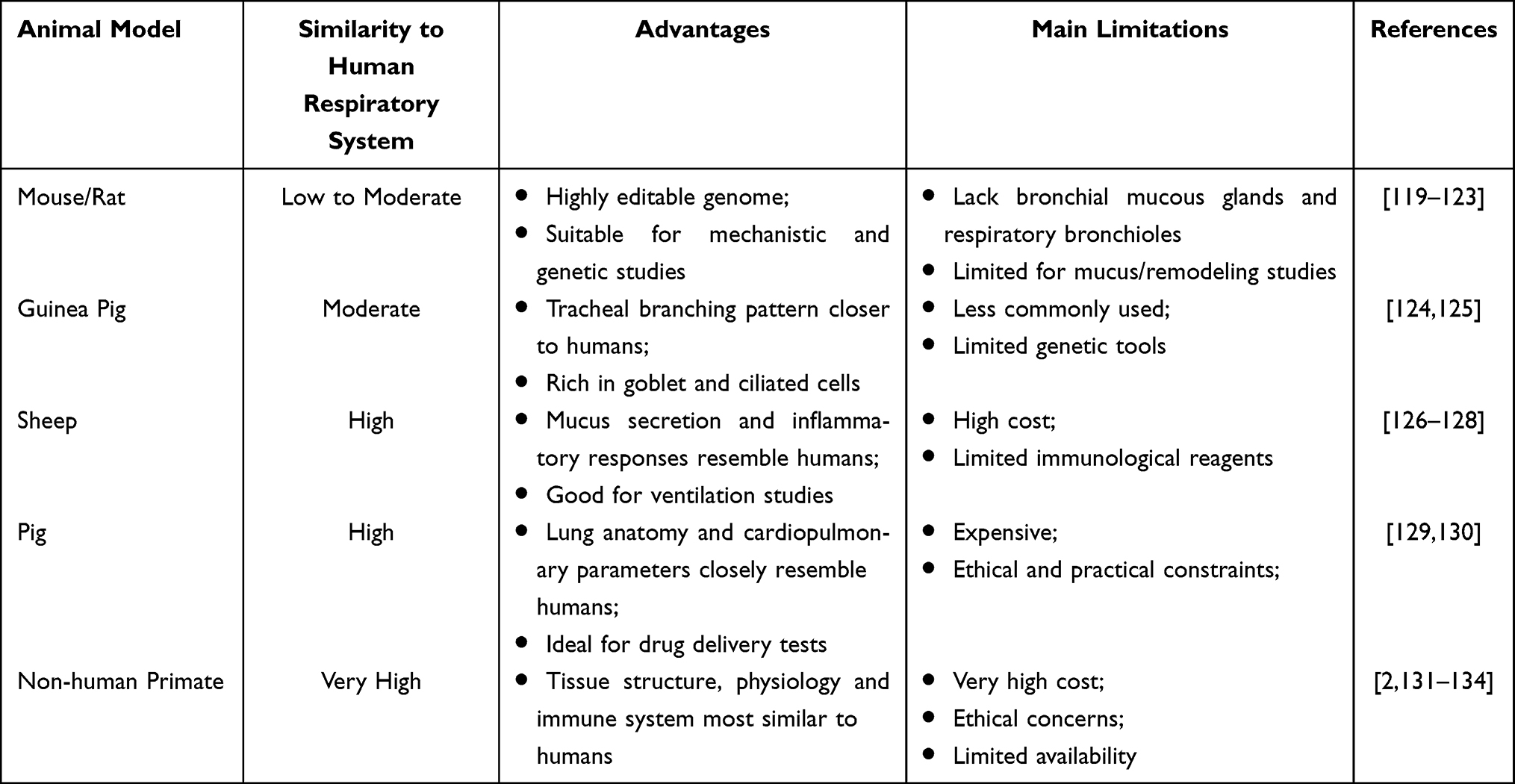 |
Table 2 Comparison of Respiratory System Compatibility Between Different Animal Models and Humans |
Beyond species selection, model diversity is also evident in the methods used for model construction. Simple smoke exposure models enable control over the concentration of toxic components, such as acrolein and carbon monoxide, by adjusting combustion materials.135 Composite injury models combining smoke inhalation with skin burns or bacterial infections better simulate the systemic inflammatory response observed in critically ill patients.136 Model diversity necessitates clear experimental objectives: mechanistic exploration requires standardized, controllable models, while translational research demands pathologically complex models and comprehensive therapeutic interventions.
Basic research on inhalation injuries requires selecting appropriate animal models based on causative factors. Pathological characteristics of smoke inhalation models primarily involve alveolar epithelial cell apoptosis and persistent neutrophil infiltration. Thermal injury models center on protein denaturation and increased vascular permeability induced by high-temperature gases, necessitating the use of Evans blue dye for enhanced vascular barrier assessment.47 It is noteworthy that the dose-response relationship of EVs is nonlinear across different models: in smoke-induced injury models, low doses reduce inflammatory factors, whereas chemical injury models require doses 2–3 times higher than low doses to inhibit collagen deposition.137 This discrepancy underscores the need for model-specific dose optimization criteria in preclinical studies.
The Influence of Cell Origin
Variations in EVs production, leading to heterogeneity and diverse therapeutic outcomes, are attributable to multiple factors. These include differences in gene expression between cell sources, fluctuations in gene expression and transcription due to culture conditions, the genomic integrity of the cells, changes in cytoplasmic and membrane protein concentrations, and the limited cargo capacity of EVs.42,138 Bone marrow mesenchymal stem cells (BMSCs) release EVs enriched with immune-regulating factors such as TSG-6 and IL-10, which significantly reduce inflammation; however, their ability to target lung tissue is limited.139–141 In contrast, EVs secreted by lung-resident stem cells, such as lung spheroid cells (LSCs), preferentially home to damaged alveolar cells and directly target alveolar type II epithelial cells. Additionally, LSC-EVs transport lung-specific markers, including AQP5, and anti-fibrotic miRNAs. These miRNAs activate the miR-30a/WISP1 axis, inhibiting TGF-β-mediated myofibroblast activation and upregulating MMP-2 to promote extracellular matrix remodeling. This process collectively reduces the severity of pulmonary fibrosis.142
Moreover, the composition of EVs from different tissues also differs. BMSCs-EVs contain a wealth of bioactive molecules that oversee cellular processes such as proliferation, differentiation, apoptosis, and inflammatory responses. EVs derived from adipose tissue mesenchymal stem cells (ADMSC-EVs) play an important role in regulating the immune system. EVs from umbilical cord-derived mesenchymal stem cells (UCMSC-EVs) demonstrate particular efficacy in repairing tissue damage.143–145 However, ethical concerns and potential cancer risks restrict their clinical research. Therefore, selecting the appropriate stem cell source and tailoring EVs for specific inhalation injuries is crucial to enhance therapeutic effectiveness. To facilitate a clear comparison of the therapeutic potential of EVs derived from different MSC sources, their key characteristics, limitations, and current translation status are summarized in Table 3.
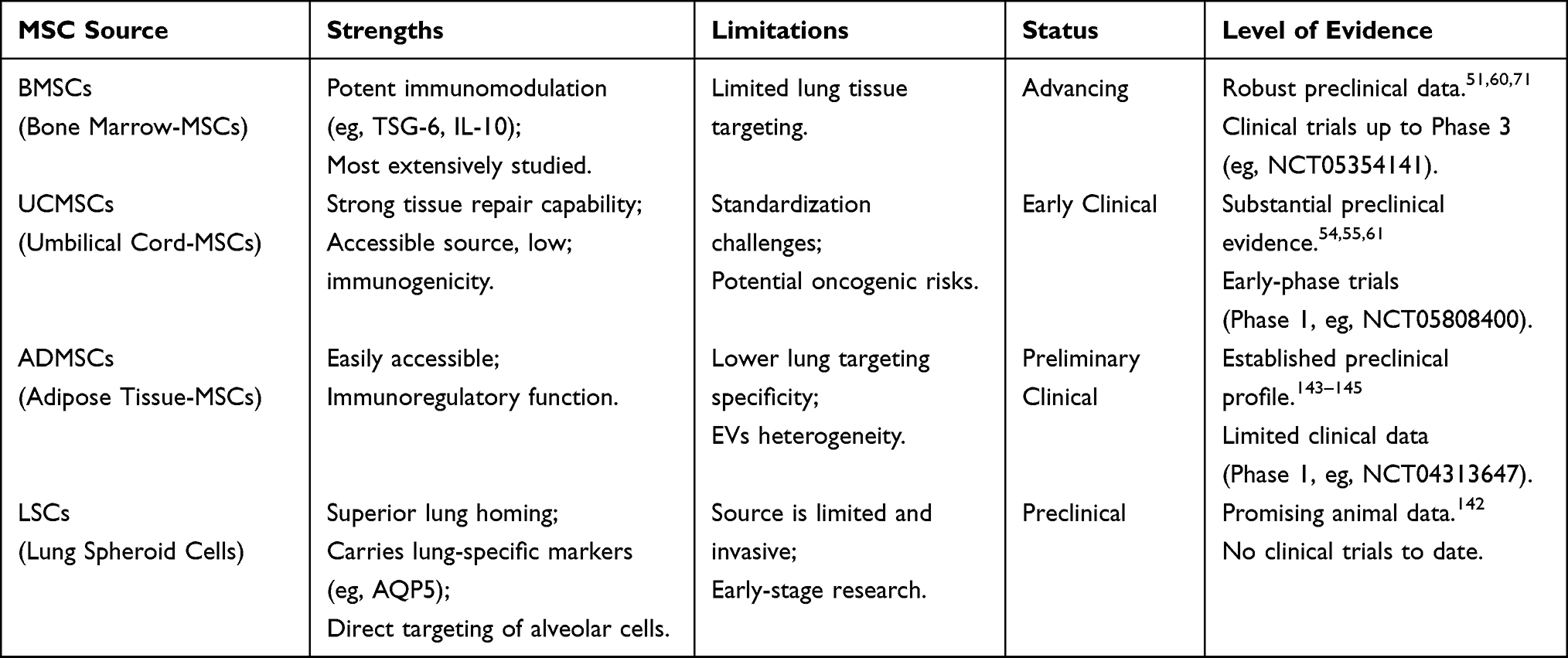 |
Table 3 Summary of Comparison of Different MSC Sources for EVs Therapy in Inhalation Lung Injury |
Investigating the similarities and differences in the molecular mechanisms underlying EVs derived from different species and stem cell sources could provide a more accurate scientific basis for clinical translation in repairing inhalation-induced lung injuries. Additionally, developing AI-based functional prediction models for EVs through deep learning and analysis of large-scale experimental data could enable precise prediction and optimized design of EVs therapeutic effects. This would represent a significant step in advancing clinical translation and holds potential for improving EV-based therapies for inhalation-induced lung injury.
Bottlenecks in Clinical Translation and Paths to Breakthroughs
Stem cell-derived EVs have been widely investigated, but clinical trials remain scarce, with many studies still in the preclinical phase. This indicates persistent bottlenecks in clinical translation, including production standardization, long-term safety assessment, and clinical trial design. Addressing these challenges would require collaboration across multiple disciplines, including enhancing production processes, conducting biosafety checks, and innovating intelligent drug delivery mechanisms. Table 4 summarizes clinical trials involving EVs for treating inhalation lung injury.
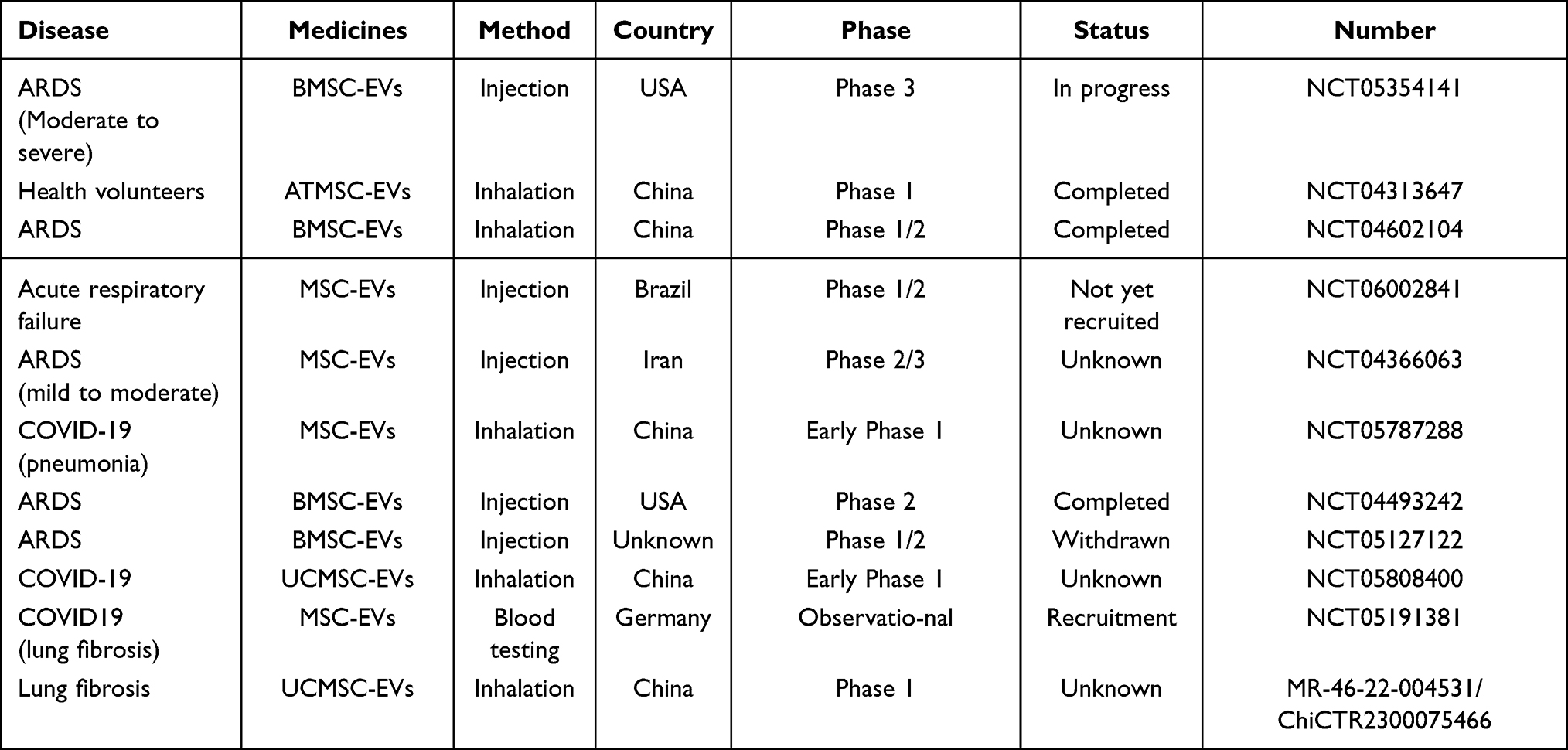 |
Table 4 Clinical Trials of EVs for the Treatment of Inhalation Lung Injury |
Standardization and Quality Control in EVs Production
Production standardization and quality control form the foundation for clinical translation of EVs, yet heterogeneity-induced efficacy variability remains a major obstacle. While engineering modifications can enhance functionality, they may introduce biosafety risks. Thus, establishing a tripartite assessment system—encompassing quality control, safety verification, and clinical adaptation—is essential for advancing EVs from laboratory to clinical application.
The core challenge in exosome isolation lies in source selection—certain biological fluids or tissues are rich in EVs, while others are not. The primary methods for separating and purifying EVs include ultracentrifugation, ultrafiltration, size-exclusion chromatography, tangential flow filtration, and polymer precipitation (Figure 2A).146,147 Among these, ultracentrifugation is most commonly used due to its low reagent consumption and ease of operation. However, its limitations include time-consuming procedures, high costs, and the risk of vesicle loss during phase separation, thereby restricting its large-scale application. Consequently, exploring alternative methods that combine high yield with good reproducibility is essential for the large-scale production of EVs.148,149 Polymer precipitation yields high quantities but is prone to contamination by protein aggregates.150 Size-based separation methods, such as ultrafiltration and size-exclusion chromatography, are rapid and ideal for large-scale applications. However, their widespread adoption is limited by pore blockage, extracellular vesicle loss, and low purity.151–153 Kekoolani S Visan and co-researchers assessed a protocol for extracting small EVs from different cancer cell lines using tangential flow filtration (TFF) and compared it with ultracentrifugation methods. Their study demonstrated TFF’s superiority over ultracentrifugation regarding yield, reproducibility, processing time, and cost.154 While each technology has limitations, combining this approach with others, such as microfluidic technology, may enhance the results.
In standardized production, strict quality control is essential. According to the MISEV guidelines published by the International Society for EVs, the combined use of transmission and scanning electron microscopy is recommended for the precise identification and quantification of EVs. Additionally, nanoparticle tracking analysis (NTA) is recommended for assessing vesicle size. Compared to electron microscopy, NTA offers cost advantages and requires no specialized expertise. Such integrated strategies are essential for achieving standardized production and quality control.39,43
Long-Term Safety Assessment of EVs
For clinical translation, assessing the long-term safety of EVs is essential. Animal studies indicate that high intravenous doses of MSC-EVs can activate the complement system and cause acute lung injury.155 The inhalation route may reduce systemic exposure, but repeated nebulization can result in heightened phagocytosis of EVs by alveolar macrophages, causing damage due to lysosomal accumulation.54 Additionally, engineering modifications of EVs can enhance targeting, though residual agents—such as chemical crosslinkers used during modification—may pose a risk of local inflammation.21 Current studies indicate that oncogenic miRNAs transported by EVs promote epithelial-mesenchymal transition in fibrotic microenvironments, enhancing tumor cell metastasis and invasion.156 Thus, longitudinal monitoring models should be established, alongside single-cell sequencing, to track the metabolic fate and potential genetic toxicity of EVs in lung tissue.
Critical Appraisal of Ongoing Clinical Trials
As shown in Table 4, numerous clinical trials have been initiated to assess the therapeutic potential of stem cell-derived exosomes in inhalation lung injury and related diseases,50 representing a pivotal transition from laboratory research to clinical practice. However, a critical evaluation of these trials reveals both the current state of research and notable challenges. Most studies are still in early stages (Phase I or I/II), involve limited sample sizes, and primarily focus on safety and feasibility—making it too early to draw definitive conclusions regarding efficacy. Moreover, considerable heterogeneity exists in trial designs, including differences in EVs sources, isolation techniques, and routes of administration. This lack of standardization hinders the comparability of results across studies.157
Notably, various delivery routes are being explored. Nebulization, as a direct and non-invasive approach, aligns with advantages observed in preclinical studies, yet requires further validation of its safety, dosage accuracy, and compatibility with delivery devices in clinical settings. Another prominent concern is the substantial number of trials listed as “Unknown” or “Not Recruiting,” which may reflect challenges in patient enrollment, manufacturing consistency, or regulatory approval processes. Despite these limitations, the completion of several early-phase trials marks an important milestone, as their outcomes will offer the first evidence regarding the safety and preliminary efficacy of EV-based therapies in humans.
To advance the field, future efforts should prioritize large-scale, randomized, placebo-controlled Phase III trials that employ standardized EVs products and well-defined patient populations, thereby establishing a solid foundation for clinical approval.
Conclusions and Perspectives
EVs represent a promising therapeutic platform for inhalation lung injury, demonstrating an inherent ability to regulate multiple pathological targets. However, their clinical translation faces significant hurdles. Current research relies heavily on simplified animal models that fail to recapitulate the complex and dynamic microenvironment of human disease, where factors such as oxidative stress and inflammatory cascades may alter EVs bioactivity.158,159 Furthermore, while engineering strategies can enhance targeting specificity, such modifications risk disrupting native vesicle structures and incurring unforeseen immunological consequences.72,160 Thus, a central challenge is to balance functional enhancement with the preservation of biocompatibility.
To address these bottlenecks, future work should prioritize two fronts. First, in EVs engineering, focus must be on optimizing targeting ligands for lesion-specific accumulation and developing “smart” EVs with microenvironment-responsive (eg, ROS/pH) release mechanisms.161 Parallel development of standardized protocols—covering isolation, potency assays, and storage stability—is critical for reproducibility. Second, bridging the preclinical-clinical gap requires establishing collaborative multicentre frameworks. This includes defining universal core outcome sets, creating centralized EVs biorepositories, and employing human organ-on-a-chip platforms for predictive validation.
Looking further ahead, next-generation EVs therapeutics should progress toward enhanced intelligence and integrated functionality. This entails engineering responsive nanocarriers for targeted release and constructing EV-eluting biomaterial scaffolds to reduce dosing frequency.162–164 Mechanistically, single-cell spatial transcriptomics and dynamic metabolomics can delineate EV-mediated recovery processes and metabolic reprogramming.165 Leveraging AI to decode EVs composition and predict functional molecules will further accelerate rational design.
In conclusion, the pathological complexity of inhalation injury demands strategies that synergize multi-target regulation with spatiotemporal precision. A concerted effort integrating multi-omics technologies, intelligent material design, and standardized collaborative frameworks is essential to propel EV-based treatments from empirical management into a new era of precision medicine.
Abbreviations
CAT, catalase; EVs, extracellular vesicles; ECM, extracellular matrix; ESCs, embryonic stem cells; EPCs, endothelial progenitor cells/stem cells; EMT, epithelial-mesenchymal transition; GPx, glutathione peroxidase; HSCs, hematopoietic stem cells; IL, interleukin; iPSCs, induced pluripotent stem cells; PDGF, platelet-derived growth factor; ROS, reactive oxygen species; TGF-β, transforming growth factor β; TNF, tumor necrosis factor; TIMP, tissue inhibitor of metalloproteinase; TLRs, activate Toll-like receptors; MSCs, mesenchymal stem cells; MVBs: multivesicular bodies; MPO, myeloperoxidase; MIP-2, macrophage inflammatory protein-2; NSCs, neural stem cells; ARDS, acute respiratory distress syndrome; LPS-ALI, lps-induced acute lung injury; COPD, Chronic obstructive pulmonary disease; ACE2, Angiotensin converting enzyme 2; TLR4, Toll like receptors 4; MyD88, Myeloid Differentiation Primary Response Gene 88; MMP-9, matrix metalloprotein-9; SPC, surfactant protein C; COL1A1, collagen 1; FN, fibronectin.
Disclosure
We declare that we have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Enkhbaatar P, Pruitt BA Jr, Suman O, et al. Pathophysiology, research challenges, and clinical management of smoke inhalation injury. Lancet. 2016;388:1437–22. doi:10.1016/S0140-6736(16)31458-1
2. Reczyńska K, Tharkar P, Kim SY, et al. Animal models of smoke inhalation injury and related acute and chronic lung diseases. Adv Drug Deliv Rev. 2018;123:107–134.
3. Inhalation injury: no mere puff of smoke. Lancet. 1984;2:849–850.
4. Sheridan RL. Fire-related inhalation injury. N Engl J Med. 2016;375:464–469. doi:10.1056/NEJMra1601128
5. Veeravagu A, Yoon BC, Jiang B, et al. National trends in burn and inhalation injury in burn patients: results of analysis of the nationwide inpatient sample database. J Burn Care Res. 2015;36:258–265. doi:10.1097/BCR.0000000000000064
6. Shirani KZ, Pruitt BA Jr, Mason AD Jr. The influence of inhalation injury and pneumonia on burn mortality. Ann Surg. 1987;205:82–87. doi:10.1097/00000658-198701000-00015
7. Liaqat A, Mason M, Foster BJ, et al. Evidence-based mechanical ventilatory strategies in ARDS. J Clin Med. 2022;12:11. doi:10.3390/jcm12010011
8. Walker PF, Buehner MF, Wood LA, et al. Diagnosis and management of inhalation injury: an updated review. Crit Care. 2015;19:351. doi:10.1186/s13054-015-1077-4
9. Lu H, Li J, Quan G, et al. Prophylactic systemic antibiotic and systemic glucocorticoid therapy after burn inhalation injury: a report of two cases and review of literature. Cureus. 2024;
10. Rehman A, Nigam A, Laino L, et al. Mesenchymal stem cells in soft tissue regenerative medicine: a comprehensive review. Medicina. 2023;59.
11. Yuan D, Bao Y, El-Hashash A. Mesenchymal stromal cell-based therapy in lung diseases; from research to clinic. Am J Stem Cells. 2024;13:37–58. doi:10.62347/JAWM2040
12. Kawamura T, Miyagawa S, Fukushima S, et al. Cardiomyocytes derived from mhc-homozygous induced pluripotent stem cells exhibit reduced allogeneic immunogenicity in mhc-matched non-human primates. Stem Cell Reports. 2016;6:312–320. doi:10.1016/j.stemcr.2016.01.012
13. Nii T, Marumoto T, Kawano H, et al. Efficient hematopoietic differentiation of common marmoset embryonic stem cells by the inhibition of their self-renewal pathway. Blood. 2012;120. doi:10.1182/blood.V120.21.2311.2311
14. Furlani D, Ugurlucan M, Ong L, et al. Is the intravascular administration of mesenchymal stem cells safe? Mesenchymal stem cells and intravital microscopy. Microvasc Res. 2009;77:370–376. doi:10.1016/j.mvr.2009.02.001
15. Tan F, Li X, Wang Z, et al. Clinical applications of stem cell-derived exosomes. Signal Transduct Target Ther. 2024;9:17. doi:10.1038/s41392-023-01704-0
16. Yang B, Chen Y, Shi J. Exosome biochemistry and advanced nanotechnology for next-generation theranostic platforms. Adv Mater. 2019;31:e1802896.
17. Clua-Ferré L, Suau R, Vañó-Segarra I, et al. Therapeutic potential of mesenchymal stem cell-derived extracellular vesicles: a focus on inflammatory bowel disease. Clin Transl Med. 2024;14:e70075. doi:10.1002/ctm2.70075
18. Chen Y, Li M, Yang J, et al. Engineerable mesenchymal stem cell-derived extracellular vesicles as promising therapeutic strategies for pulmonary fibrosis. Stem Cell Res Ther. 2025;16:367.
19. Gnecchi M, Danieli P, Malpasso G, et al. Paracrine mechanisms of mesenchymal stem cells in tissue repair. Methods Mol Biol. 2016;1416:123–146.
20. Riazifar M, Pone EJ, Lötvall J, et al. Stem cell extracellular vesicles: extended messages of regeneration. Annu Rev Pharmacol Toxicol. 2017;57:125–154. doi:10.1146/annurev-pharmtox-061616-030146
21. Cruz FF, Rocco PRM. Stem-cell extracellular vesicles and lung repair. Stem Cell Investig. 2017;4:78. doi:10.21037/sci.2017.09.02
22. Kang WY, Jung S, Jeong H, et al. Effect of mechanical environment alterations in 3d stem cell culture on the therapeutic potential of extracellular vesicles. Biomater Res. 2025;29:0189. doi:10.34133/bmr.0189
23. Hu S, Park J, Liu A, et al. Mesenchymal stem cell microvesicles restore protein permeability across primary cultures of injured human lung microvascular endothelial cells. Stem Cells Transl Med. 2018;7:615–624. doi:10.1002/sctm.17-0278
24. Shi J, Li Y, Zhao H, et al. Single-cell transcriptomics reveals stem cell-derived exosomes attenuate inflammatory gene expression in pulmonary oxygen toxicity. Int J Mol Sci. 2025;26.
25. Harrell CR, Djonov V, Volarevic A, et al. Molecular mechanisms responsible for the therapeutic potential of mesenchymal stem cell-derived exosomes in the treatment of lung fibrosis. Int J Mol Sci. 2024;26:25. doi:10.3390/ijms26010025
26. Mortati L, de Girolamo L, Perucca Orfei C, et al. In vitro study of extracellular vesicles migration in cartilage-derived osteoarthritis samples using real-time quantitative multimodal nonlinear optics imaging. Pharmaceutics. 2020;13:12. doi:10.3390/pharmaceutics13010012
27. Morales-Nebreda L, Misharin AV, Perlman H, et al. The heterogeneity of lung macrophages in the susceptibility to disease. Eur Respir Rev. 2015;24:505–509. doi:10.1183/16000617.0031-2015
28. Yang Y, Lv M, Xu Q, et al. Extracellular vesicles in idiopathic pulmonary fibrosis: pathogenesis, biomarkers and innovative therapeutic strategies. Int J Nanomed. 2024;19:12593–12614. doi:10.2147/IJN.S491335
29. Gurunathan S, Kang M-H, Qasim M, et al. Biogenesis, membrane trafficking, functions, and next generation nanotherapeutics medicine of extracellular vesicles. Int J Nanomed. 2021;16:3357–3383. doi:10.2147/IJN.S310357
30. Hade MD, Suire CN, Suo Z. Mesenchymal stem cell-derived exosomes: applications in regenerative medicine. Cells. 2021;11:10. doi:10.3390/cells11010010
31. Salem HK, Thiemermann C. Mesenchymal stromal cells: current understanding and clinical status. Stem Cells. 2010;28:585–596. doi:10.1002/stem.269
32. Ding L, Guo Q, Ren Y, et al. Construction of [(89)zr]zr-labeled human umbilical cord mesenchymal stem cell-derived extracellular vesicles for noninvasive detection of tumors. ACS Appl Mater Interfaces. 2025;17:30589–30599. doi:10.1021/acsami.5c03280
33. Xunian Z, Kalluri R. Biology and therapeutic potential of mesenchymal stem cell-derived exosomes. Cancer Sci. 2020;111:3100–3110. doi:10.1111/cas.14563
34. Jia Y, Yu L, Ma T, et al. Small extracellular vesicles isolation and separation: current techniques, pending questions and clinical applications. Theranostics. 2022;12:6548–6575. doi:10.7150/thno.74305
35. Yáñez-Mó M, Siljander PR, Andreu Z, et al. Biological properties of extracellular vesicles and their physiological functions. J Extracell Vesicles. 2015;4:27066. doi:10.3402/jev.v4.27066
36. Lee JH, Park J, Lee JW. Therapeutic use of mesenchymal stem cell-derived extracellular vesicles in acute lung injury. Transfusion. 2019;59:876–883. doi:10.1111/trf.14838
37. Walsh SA, Hoyt BW, Rowe CJ, et al. Alarming cargo: the role of exosomes in trauma-induced inflammation. Biomolecules. 2021;12:11. doi:10.3390/biom12010011
38. Nederveen JP, Warnier G, Di Carlo A, et al. Extracellular vesicles and exosomes: insights from exercise science. Front Physiol. 2020;11:604274. doi:10.3389/fphys.2020.604274
39. Welsh JA, Goberdhan DCI, O’Driscoll L, et al. Minimal information for studies of extracellular vesicles (misev2023): from basic to advanced approaches. J Extracell Vesicles. 2024;13:e12404.
40. Juan T, Fürthauer M. Biogenesis and function of escrt-dependent extracellular vesicles. Semin Cell Dev Biol. 2018;74:66–77. doi:10.1016/j.semcdb.2017.08.022
41. Hade MD, Suire CN, Mossell J, et al. Extracellular vesicles: emerging frontiers in wound healing. Med Res Rev. 2022;42:2102–2125. doi:10.1002/med.21918
42. Han QF, Li WJ, Hu KS, et al. Exosome biogenesis: machinery, regulation, and therapeutic implications in cancer. Mol Cancer. 2022;21:207. doi:10.1186/s12943-022-01671-0
43. Meng W, He C, Hao Y, et al. Prospects and challenges of extracellular vesicle-based drug delivery system: considering cell source. Drug Deliv. 2020;27:585–598. doi:10.1080/10717544.2020.1748758
44. Görgens A, Corso G, Hagey DW, et al. Identification of storage conditions stabilizing extracellular vesicles preparations. J Extracell Vesicles. 2022;11:e12238. doi:10.1002/jev2.12238
45. Park KS, Lässer C, Lötvall J. Extracellular vesicles and the lung: from disease pathogenesis to biomarkers and treatments. Physiol Rev. 2025;105:1733–1821. doi:10.1152/physrev.00032.2024
46. Watanabe Y, Tsuchiya A, Terai S. The development of mesenchymal stem cell therapy in the present, and the perspective of cell-free therapy in the future. Clin Mol Hepatol. 2021;27:70–80. doi:10.3350/cmh.2020.0194
47. Erickson MJ, Enkhbaatar P, Lee JO. Inhalation injury. Seminars Plastic Surg. 2024;38:093–096. doi:10.1055/s-0044-1782646
48. Taganov KD, Boldin MP, Chang KJ, et al. Nf-kappab-dependent induction of microrna mir-146, an inhibitor targeted to signaling proteins of innate immune responses. Proc Natl Acad Sci U S A. 2006;103:12481–12486. doi:10.1073/pnas.0605298103
49. Cloer C, Roudsari L, Rochelle L, et al. Mesenchymal stromal cell-derived extracellular vesicles reduce lung inflammation and damage in nonclinical acute lung injury: implications for covid-19. PLoS One. 2021;16:e0259732.
50. Krishnan A, Muthusamy S, Fernandez FB, et al. Mesenchymal stem cell-derived extracellular vesicles in the management of covid19-associated lung injury: a review on publications, clinical trials and patent landscape. Tissue Eng Regen Med. 2022;19:659–673. doi:10.1007/s13770-022-00441-9
51. Xu B, Gan CX, Chen SS, et al. Bmsc-derived exosomes alleviate smoke inhalation lung injury through blockade of the hmgb1/nf-κb pathway. Life Sci. 2020;257:118042. doi:10.1016/j.lfs.2020.118042
52. Qi H, Wang Y, Fa S, et al. Extracellular vesicles as natural delivery carriers regulate oxidative stress under pathological conditions. Front Bioeng Biotechnol. 2021;9:752019. doi:10.3389/fbioe.2021.752019
53. Martin PJ, Héliot A, Trémolet G, et al. Cellular response and extracellular vesicles characterization of human macrophages exposed to fine atmospheric particulate matter. Environ Pollut. 2019;254:112933. doi:10.1016/j.envpol.2019.07.101
54. Zhao R, Wang L, Wang T, et al. Inhalation of msc-evs is a noninvasive strategy for ameliorating acute lung injury. J Control Release. 2022;345:214–230. doi:10.1016/j.jconrel.2022.03.025
55. Hou L, Zhu Z, Jiang F, et al. Human umbilical cord mesenchymal stem cell-derived extracellular vesicles alleviated silica induced lung inflammation and fibrosis in mice via circpwwp2a/mir-223-3p/nlrp3 axis. Ecotoxicol Environ Saf. 2023;251:114537. doi:10.1016/j.ecoenv.2023.114537
56. Budi EH, Schaub JR, Decaris M, et al. TGF -β as a driver of fibrosis: physiological roles and therapeutic opportunities. J Pathol. 2021;254:358–373. doi:10.1002/path.5680
57. Yuan R, Dai X, Li Y, et al. Exosomes from mir-29a-modified adipose-derived mesenchymal stem cells reduce excessive scar formation by inhibiting tgf-β2/smad3 signaling. Mol Med Rep. 2021;24.
58. Gangoda L, Boukouris S, Liem M, et al. Extracellular vesicles including exosomes are mediators of signal transduction: are they protective or pathogenic? Proteomics. 2015;15:260–271. doi:10.1002/pmic.201400234
59. Kadota T, Fujita Y, Araya J, et al. Human bronchial epithelial cell-derived extracellular vesicle therapy for pulmonary fibrosis via inhibition of tgf-β-wnt crosstalk. J Extracell Vesicles. 2021;10:e12124.
60. Zhou J, Lin Y, Kang X, et al. Microrna-186 in extracellular vesicles from bone marrow mesenchymal stem cells alleviates idiopathic pulmonary fibrosis via interaction with sox4 and dkk1. Stem Cell Res Ther. 2021;12:96. doi:10.1186/s13287-020-02083-x
61. Xu C, Zhao J, Li Q, et al. Exosomes derived from three-dimensional cultured human umbilical cord mesenchymal stem cells ameliorate pulmonary fibrosis in a mouse silicosis model. Stem Cell Res Ther. 2020;11:503. doi:10.1186/s13287-020-02023-9
62. Hu Q, Zhang S, Yang Y, et al. Extracellular vesicles in the pathogenesis and treatment of acute lung injury. Mil Med Res. 2022;9:61. doi:10.1186/s40779-022-00417-9
63. Zhang X, Cheng Z, Zeng M, et al. The efficacy of extracellular vesicles for acute lung injury in preclinical animal models: a meta-analysis. BMC Pulm Med. 2024;24:128. doi:10.1186/s12890-024-02910-4
64. Ouhtit A, Thouta R, Zayed H, et al. Cd44 mediates stem cell mobilization to damaged lung via its novel transcriptional targets, cortactin and survivin. Int J Med Sci. 2020;17:103–111. doi:10.7150/ijms.33125
65. Li S, Zhang J, Feng G, et al. The emerging role of extracellular vesicles from mesenchymal stem cells and macrophages in pulmonary fibrosis: insights into miRNA delivery. Pharmaceuticals. 2022;16:15. doi:10.3390/ph16010015
66. Yang JX, Zhang N, Wang HW, et al. Cxcr4 receptor overexpression in mesenchymal stem cells facilitates treatment of acute lung injury in rats. J Biol Chem. 2015;290:1994–2006. doi:10.1074/jbc.M114.605063
67. Tang XD, Shi L, Monsel A, et al. Mesenchymal stem cell microvesicles attenuate acute lung injury in mice partly mediated by ang-1 mrna. Stem Cells. 2017;35:1849–1859. doi:10.1002/stem.2619
68. Lin KC, Lin HY, Yang CY, et al. Inhalable mucociliary-on-chip system revealing pulmonary clearance dynamics in nanodrug delivery. ACS Nano. 2025;19:2228–2244. doi:10.1021/acsnano.4c11693
69. Zhao J, Jiang Q, Xu C, et al. Mir-26a-5p from hucmsc-derived extracellular vesicles inhibits epithelial mesenchymal transition by targeting adam17 in silica-induced lung fibrosis. Ecotoxicol Environ Saf. 2023;257:114950. doi:10.1016/j.ecoenv.2023.114950
70. Xu N, Shao Y, Ye K, et al. Mesenchymal stem cell-derived exosomes attenuate phosgene-induced acute lung injury in rats. Inhal Toxicol. 2019;31:52–60. doi:10.1080/08958378.2019.1597220
71. Dutra Silva J, Su Y, Calfee CS, et al. Mesenchymal stromal cell extracellular vesicles rescue mitochondrial dysfunction and improve barrier integrity in clinically relevant models of ARDS. Eur Respir J. 2021;58.
72. Monsel A, Zhu YG, Gudapati V, et al. Mesenchymal stem cell derived secretome and extracellular vesicles for acute lung injury and other inflammatory lung diseases. Expert Opin Biol Ther. 2016;16:859–871. doi:10.1517/14712598.2016.1170804
73. Zhou Y, Li P, Goodwin AJ, et al. Exosomes from endothelial progenitor cells improve outcomes of the lipopolysaccharide-induced acute lung injury. Crit Care. 2019;23:44. doi:10.1186/s13054-019-2339-3
74. Wu X, Liu Z, Hu L, et al. Exosomes derived from endothelial progenitor cells ameliorate acute lung injury by transferring mir-126. Exp Cell Res. 2018;370:13–23. doi:10.1016/j.yexcr.2018.06.003
75. Gazdhar A, Ravikumar P, Pastor J, et al. Alpha-klotho enrichment in induced pluripotent stem cell secretome contributes to antioxidative protection in acute lung injury. Stem Cells. 2018;36:616–625. doi:10.1002/stem.2752
76. Li M, Huang H, Wei X, et al. Clinical investigation on nebulized human umbilical cord msc-derived extracellular vesicles for pulmonary fibrosis treatment. Signal Transduct Target Ther. 2025;10:179. doi:10.1038/s41392-025-02262-3
77. Xiao K, He W, Guan W, et al. Mesenchymal stem cells reverse emt process through blocking the activation of nf-κb and hedgehog pathways in lps-induced acute lung injury. Cell Death Dis. 2020;11:863. doi:10.1038/s41419-020-03034-3
78. Jurgielewicz B, Stice S, Yao Y. Therapeutic potential of nucleic acids when combined with extracellular vesicles. Aging Dis. 2021;12:1476–1493. doi:10.14336/AD.2021.0708
79. Wang L, Tang Y, Tang J, et al. Endothelial cell-derived extracellular vesicles expressing surface vcam1 promote sepsis-related acute lung injury by targeting and reprogramming monocytes. J Extracell Vesicles. 2024;13:e12423.
80. Charoenviriyakul C, Takahashi Y, Morishita M, et al. Role of extracellular vesicle surface proteins in the pharmacokinetics of extracellular vesicles. Mol Pharm. 2018;15:1073–1080. doi:10.1021/acs.molpharmaceut.7b00950
81. Chen S, Sun F, Qian H, et al. Preconditioning and engineering strategies for improving the efficacy of mesenchymal stem cell-derived exosomes in cell-free therapy. Stem Cells Int. 2022;2022:1779346. doi:10.1155/2022/1779346
82. Kou M, Huang L, Yang J, et al. Mesenchymal stem cell-derived extracellular vesicles for immunomodulation and regeneration: a next generation therapeutic tool? Cell Death Dis. 2022;13:580. doi:10.1038/s41419-022-05034-x
83. Saleh NA, Gagea MA, Vitija X, et al. Harnessing extracellular vesicles for stabilized and functional il-10 delivery in macrophage immunomodulation. bioRxiv. 2025. doi:10.1101/2025.01.14.633016
84. Zeng B, Li Y, Khan N, et al. Yin-yang: two sides of extracellular vesicles in inflammatory diseases. J Nanobiotechnology. 2024;22:514. doi:10.1186/s12951-024-02779-9
85. Forkan CP, Shrestha A, Yu A, et al. Could hypoxic conditioning augment the potential of mesenchymal stromal cell-derived extracellular vesicles as a treatment for type 1 diabetes? Stem Cell Res Ther. 2025;16:37. doi:10.1186/s13287-025-04153-4
86. Cecchin R, Troyer Z, Witwer K, et al. Extracellular vesicles: the next generation in gene therapy delivery. Mol Ther. 2023;31:1225–1230. doi:10.1016/j.ymthe.2023.01.021
87. Zhang W, Uyemura R, Zhong K, et al. Current advances and future perspectives on mesenchymal stem cell-derived extracellular vesicles in Alzheimer’s disease. Aging Dis. 2024;15:2015–2027. doi:10.14336/AD.2023.1206
88. Pan Z, Sun W, Chen Y, et al. Extracellular vesicles in tissue engineering: biology and engineered strategy. Adv Healthc Mater. 2022;11:e2201384. doi:10.1002/adhm.202201384
89. Long Y, Yang B, Lei Q, et al. Targeting senescent alveolar epithelial cells using engineered mesenchymal stem cell-derived extracellular vesicles to treat pulmonary fibrosis. ACS Nano. 2024;18:7046–7063. doi:10.1021/acsnano.3c10547
90. Murphy DE, de Jong OG, Brouwer M, et al. Extracellular vesicle-based therapeutics: natural versus engineered targeting and trafficking. Exp Mol Med. 2019;51:1–12. doi:10.1038/s12276-019-0223-5
91. Whitley JA, Cai H. Engineering extracellular vesicles to deliver CRISPR ribonucleoprotein for gene editing. J Extracell Vesicles. 2023;12:e12343.
92. Zhang K, Li R, Chen X, et al. Renal endothelial cell-targeted extracellular vesicles protect the kidney from ischemic injury. Adv Sci. 2023;10:e2204626. doi:10.1002/advs.202204626
93. Piffoux M, Silva AKA, Wilhelm C, et al. Modification of extracellular vesicles by fusion with liposomes for the design of personalized biogenic drug delivery systems. ACS Nano. 2018;12:6830–6842. doi:10.1021/acsnano.8b02053
94. Zhao S, Di Y, Fan H, et al. Targeted delivery of extracellular vesicles: the mechanisms, techniques and therapeutic applications. Mol Biomed. 2024;5:60. doi:10.1186/s43556-024-00230-x
95. Richter M, Vader P, Fuhrmann G. Approaches to surface engineering of extracellular vesicles. Adv Drug Deliv Rev. 2021;173:416–426. doi:10.1016/j.addr.2021.03.020
96. Kooijmans SAA, Fliervoet LAL, van der Meel R, et al. Pegylated and targeted extracellular vesicles display enhanced cell specificity and circulation time. J Control Release. 2016;224:77–85. doi:10.1016/j.jconrel.2016.01.009
97. Zhang Y, Dou Y, Liu Y, et al. Advances in therapeutic applications of extracellular vesicles. Int J Nanomed. 2023;18:3285–3307. doi:10.2147/IJN.S409588
98. Xu P, He J, Xu T, et al. Synergistic integration of extracellular vesicles and metal-organic frameworks: unlocking new opportunities in disease diagnosis and therapy. Theranostics. 2025;15:8609–8638. doi:10.7150/thno.113474
99. Ju Y, Hu Y, Yang P, et al. Extracellular vesicle-loaded hydrogels for tissue repair and regeneration. Mater Today Bio. 2023;18:100522. doi:10.1016/j.mtbio.2022.100522
100. Simon L, Lapinte V, Morille M. Exploring the role of polymers to overcome ongoing challenges in the field of extracellular vesicles. J Extracell Vesicles. 2023;12:e12386. doi:10.1002/jev2.12386
101. Della Sala F, Longobardo G, Di Gennaro M, et al. The interplay between hyaluronic acid and stem cell secretome boosts pulmonary differentiation in 3d biomimetic microenvironments. Int J Biol Macromol. 2024;276:133793. doi:10.1016/j.ijbiomac.2024.133793
102. Hettich BF, Bader JJ, Leroux JC. Encapsulation of hydrophilic compounds in small extracellular vesicles: loading capacity and impact on vesicle functions. Adv Healthc Mater. 2022;11:e2100047. doi:10.1002/adhm.202100047
103. Xu G, Jin J, Fu Z, et al. Extracellular vesicle-based drug overview: research landscape, quality control and nonclinical evaluation strategies. Signal Transduct Target Ther. 2025;10:255. doi:10.1038/s41392-025-02312-w
104. Piffoux M, Volatron J, Cherukula K, et al. Engineering and loading therapeutic extracellular vesicles for clinical translation: a data reporting frame for comparability. Adv Drug Deliv Rev. 2021;178:113972. doi:10.1016/j.addr.2021.113972
105. Mohammadi AH, Ghazvinian Z, Bagheri F, et al. Modification of extracellular vesicle surfaces: an approach for targeted drug delivery. BioDrugs. 2023;37:353–374. doi:10.1007/s40259-023-00595-5
106. Lazarovits J, Chen YY, Sykes EA, et al. Nanoparticle-blood interactions: the implications on solid tumour targeting. Chem Commun. 2015;51:2756–2767. doi:10.1039/C4CC07644C
107. Belenkovich M, Sznitman J, Korin N. Micro-particle entrapment dynamics in microfluidic pulmonary capillary networks. J Biomech. 2022;137:111082. doi:10.1016/j.jbiomech.2022.111082
108. Tilley AE, Walters MS, Shaykhiev R, et al. Cilia dysfunction in lung disease. Annu Rev Physiol. 2015;77:379–406. doi:10.1146/annurev-physiol-021014-071931
109. Carpenter J, Wang Y, Gupta R, et al. Assembly and organization of the n-terminal region of mucin muc5ac: indications for structural and functional distinction from muc5b. Proc Natl Acad Sci U S A. 2021;118.
110. Hill DB, Button B, Rubinstein M, et al. Physiology and pathophysiology of human airway mucus. Physiol Rev. 2022;102:1757–1836. doi:10.1152/physrev.00004.2021
111. Darquenne C, Lamm WJ, Fine JM, et al. Total and regional deposition of inhaled aerosols in supine healthy subjects and subjects with mild-to-moderate COPD. J Aerosol Sci. 2016;99:27–39. doi:10.1016/j.jaerosci.2016.01.019
112. Sunkara V, Woo HK, Cho YK. Emerging techniques in the isolation and characterization of extracellular vesicles and their roles in cancer diagnostics and prognostics. Analyst. 2016;141:371–381. doi:10.1039/C5AN01775K
113. Sivanantham A, Jin Y, Kesari KK, Kumar A. Impact of storage conditions on ev integrity/surface markers and cargos. Life. 2022;13:12. doi:10.3390/life13010012
114. He S, Li Z, Xie L, et al. Biomimetic gene delivery system coupled with extracellular vesicle-encapsulated aav for improving diabetic wound through promoting vascularization and remodeling of inflammatory microenvironment. J Nanobiotechnology. 2025;23:242. doi:10.1186/s12951-025-03261-w
115. Ziegler JN, Tian C. Engineered extracellular vesicles: emerging therapeutic strategies for translational applications. Int J Mol Sci. 2023;25:24. doi:10.3390/ijms25010024
116. de Almeida Fuzeta M, Bernardes N, Oliveira FD, et al. Scalable production of human mesenchymal stromal cell-derived extracellular vesicles under serum-/xeno-free conditions in a microcarrier-based bioreactor culture system. Front Cell Dev Biol. 2020;8:553444. doi:10.3389/fcell.2020.553444
117. Kimiz-Gebologlu I, Oncel SS. Exosomes: large-scale production, isolation, drug loading efficiency, and biodistribution and uptake. J Control Release. 2022;347:533–543. doi:10.1016/j.jconrel.2022.05.027
118. Deng S, Li C, Cao J, et al. Organ-on-a-chip meets artificial intelligence in drug evaluation. Theranostics. 2023;13:4526–4558. doi:10.7150/thno.87266
119. Mouro Pinto R, Murtha R, Azevedo A, et al. In vivo CRISPR-Cas9 genome editing in mice identifies genetic modifiers of somatic CAG repeat instability in Huntington’s disease. Nat Genet. 2025;57:314–322. doi:10.1038/s41588-024-02054-5
120. Meek S, Mashimo T, Burdon T. From engineering to editing the rat genome. Mamm Genome. 2017;28:302–314. doi:10.1007/s00335-017-9705-8
121. Tisch LJ, Bartone RD, Antoniak S, et al. Protease-activated receptor-2 (par2) mutation attenuates airway fibrosis in mice during the exacerbation of house dust mite‑induced allergic lung disease by multi‑walled carbon nanotubes. Respir Res. 2025;26:90. doi:10.1186/s12931-025-03168-y
122. Huang R, Gong S, Xiong B, et al. A classic prescription alleviates inflammation in cums model mice via modulating mydgf/map4k4/nf-κb signaling pathway, verified through uplc-hrms and proteomics analysis. Heliyon. 2024;10:34596. doi:10.1016/j.heliyon.2024.e34596
123. Wang J, Huang J, Wang L, et al. Urban particulate matter triggers lung inflammation via the ros-mapk-nf-κb signaling pathway. J Thorac Dis. 2017;9:4398–4412. doi:10.21037/jtd.2017.09.135
124. Schreider JP, Hutchens JO. Morphology of the Guinea pig respiratory tract. Anat Rec. 1980;196:313–321. doi:10.1002/ar.1091960307
125. Li Y, Wang J, He HY, et al. Immunohistochemical demonstration of airway epithelial cell markers of Guinea pig. Tissue Cell. 2011;43:283–290. doi:10.1016/j.tice.2011.05.003
126. Hsia CC, Hyde DM, Weibel ER. Lung structure and the intrinsic challenges of gas exchange. Compr Physiol. 2016;6:827–895. doi:10.1002/j.2040-4603.2016.tb00698.x
127. Judge EP, Hughes JM, Egan JJ, et al. Anatomy and bronchoscopy of the porcine lung. A model for translational respiratory medicine. Am J Respir Cell Mol Biol. 2014;51:334–343. doi:10.1165/rcmb.2013-0453TR
128. Tan W, Qi L, Tan Z. Animal models of infection-induced acute lung injury. Exp Lung Res. 2024;50:221–241. doi:10.1080/01902148.2024.2428939
129. Lunney JK, Van Goor A, Walker KE, et al. Importance of the pig as a human biomedical model. Sci Transl Med. 2021;13:eabd5758.
130. Nelson K, Bobba C, Ghadiali S, et al. Animal models of ex vivo lung perfusion as a platform for transplantation research. World J Exp Med. 2014;4:7–15. doi:10.5493/wjem.v4.i2.7
131. Swaminathan AC, Todd JL, Palmer SM. Advances in human lung transplantation. Annu Rev Med. 2021;72:135–149. doi:10.1146/annurev-med-080119-103200
132. Cryan SA, Sivadas N, Garcia-Contreras L. In vivo animal models for drug delivery across the lung mucosal barrier. Adv Drug Deliv Rev. 2007;59:1133–1151. doi:10.1016/j.addr.2007.08.023
133. Linden K, Scaravilli V, Kreyer SF, et al. Evaluation of the cytosorb™ hemoadsorptive column in a pig model of severe smoke and burn injury. Shock. 2015;44:487–495. doi:10.1097/SHK.0000000000000439
134. McLaughlin RF Jr, Tyler WS, Canada RO. Subgross pulmonary anatomy of the rabbit, rat, and Guinea pig, with additional notes on the human lung. Am Rev Respir Dis. 1966;94:380–387. doi:10.1164/arrd.1966.94.3.380
135. Tian L, Jin J, Lai F, et al. Nebulized m2 macrophage-derived nanovesicles for the treatment of explosion-induced acute lung injury. J Colloid Interface Sci. 2025;691:137381. doi:10.1016/j.jcis.2025.137381
136. Bang Y, Hwang S, Kim YE, et al. Therapeutic efficacy of thrombin-preconditioned mesenchymal stromal cell-derived extracellular vesicles on escherichia coli-induced acute lung injury in mice. Respir Res. 2024;25:303. doi:10.1186/s12931-024-02908-w
137. Ai D, Shen J, Sun J, et al. Mesenchymal stem cell-derived extracellular vesicles suppress hyperoxia-induced transdifferentiation of rat alveolar type 2 epithelial cells. Stem Cells Dev. 2022;31:53–66. doi:10.1089/scd.2021.0256
138. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367. doi:10.1126/science.aau6977
139. Bulut Ö, Gürsel İ. Mesenchymal stem cell derived extracellular vesicles: promising immunomodulators against autoimmune, autoinflammatory disorders and sars-cov-2 infection. Turk J Biol. 2020;44:273–282. doi:10.3906/biy-2002-79
140. Cai J, Wu J, Wang J, et al. Extracellular vesicles derived from different sources of mesenchymal stem cells: therapeutic effects and translational potential. Cell Biosci. 2020;10:69.
141. Sharma D, Zhao F. Updates on clinical trials evaluating the regenerative potential of allogenic mesenchymal stem cells in covid-19. NPJ Regen Med. 2021;6:37.
142. Dinh PC, Paudel D, Brochu H, et al. Inhalation of lung spheroid cell secretome and exosomes promotes lung repair in pulmonary fibrosis. Nat Commun. 2020;11:1064. doi:10.1038/s41467-020-14344-7
143. Wang ZG, He ZY, Liang S, et al. Comprehensive proteomic analysis of exosomes derived from human bone marrow, adipose tissue, and umbilical cord mesenchymal stem cells. Stem Cell Res Ther. 2020;11:511. doi:10.1186/s13287-020-02032-8
144. Kim H, Zhao Q, Barreda H, et al. Identification of molecules responsible for therapeutic effects of extracellular vesicles produced from iPSC-derived MSCs on sjo¨gren’s syndrome. Aging Dis. 2021;12:1409–1422. doi:10.14336/AD.2021.0621
145. Yang S, Sun Y, Yan C. Recent advances in the use of extracellular vesicles from adipose-derived stem cells for regenerative medical therapeutics. J Nanobiotechnology. 2024;22:316. doi:10.1186/s12951-024-02603-4
146. Khalaj K, Figueira RL, Antounians L, et al. Systematic review of extracellular vesicle-based treatments for lung injury: are evs a potential therapy for covid-19? J Extracell Vesicles. 2020;9:1795365.
147. Li P, Kaslan M, Lee SH, et al. Progress in exosome isolation techniques. Theranostics. 2017;7:789–804.
148. Livshits MA, Khomyakova E, Evtushenko EG, et al. Isolation of exosomes by differential centrifugation: theoretical analysis of a commonly used protocol. Sci Rep. 2015;5:17319. doi:10.1038/srep17319
149. Van Deun J, Mestdagh P, Sormunen R, et al. The impact of disparate isolation methods for extracellular vesicles on downstream rna profiling. J Extracell Vesicles. 2014;3.
150. Lane RE, Korbie D, Trau M, et al. Purification protocols for extracellular vesicles. Methods Mol Biol. 2017;1660:111–130.
151. Xu R, Greening DW, Zhu HJ, et al. Extracellular vesicle isolation and characterization: toward clinical application. J Clin Invest. 2016;126:1152–1162. doi:10.1172/JCI81129
152. Linares R, Tan S, Gounou C, et al. High-speed centrifugation induces aggregation of extracellular vesicles. J Extracell Vesicles. 2015;4:29509. doi:10.3402/jev.v4.29509
153. Fujita Y, Kadota T, Araya J, et al. Clinical application of mesenchymal stem cell-derived extracellular vesicle-based therapeutics for inflammatory lung diseases. J Clin Med. 2018;7.
154. Visan KS, Lobb RJ, Ham S, et al. Comparative analysis of tangential flow filtration and ultracentrifugation, both combined with subsequent size exclusion chromatography, for the isolation of small extracellular vesicles. J Extracell Vesicles. 2022;11:e12266. doi:10.1002/jev2.12266
155. Yang BL, Long YY, Lei Q, et al. Lethal pulmonary thromboembolism in mice induced by intravenous human umbilical cord mesenchymal stem cell-derived large extracellular vesicles in a dose- and tissue factor-dependent manner. Acta Pharmacol Sin. 2024;45:2300–2312. doi:10.1038/s41401-024-01327-3
156. Sun H, Zhang T, Gao J. Extracellular vesicles derived from mesenchymal stem cells: a potential biodrug for acute respiratory distress syndrome treatment. BioDrugs. 2022;36:701–715. doi:10.1007/s40259-022-00555-5
157. Fröhlich E, Berchner-Pfannschmidt U, Ting SC. Therapeutic potential of mesenchymal stem cells and their products in lung diseases-intravenous administration versus inhalation. Pharmaceutics. 2021;14:13. doi:10.3390/pharmaceutics14010013
158. Andres J, Smith LC, Murray A, et al. Role of extracellular vesicles in cell-cell communication and inflammation following exposure to pulmonary toxicants. Cytokine Growth Factor Rev. 2020;51:12–18. doi:10.1016/j.cytogfr.2019.12.001
159. Nirujogi TS, Kotha SR, Chung S, et al. Lipidomic profiling of bronchoalveolar lavage fluid extracellular vesicles indicates their involvement in lipopolysaccharide-induced acute lung injury. J Innate Immun. 2022;14:555–568. doi:10.1159/000522338
160. Sun Y, Sun F, Xu W, et al. Engineered extracellular vesicles as a targeted delivery platform for precision therapy. Tissue Eng Regen Med. 2023;20:157–175. doi:10.1007/s13770-022-00503-y
161. Cao J, Zhang X, Guo J, et al. An engineering-reinforced extracellular vesicle-integrated hydrogel with an ros-responsive release pattern mitigates spinal cord injury. Sci Adv. 2025;11:eads3398.
162. Tsintou M, Dalamagkas K, Moore TL, et al. The use of hydrogel-delivered extracellular vesicles in recovery of motor function in stroke: a testable experimental hypothesis for clinical translation including behavioral and neuroimaging assessment approaches. Neural Regen Res. 2021;16:605–613. doi:10.4103/1673-5374.295269
163. Fan Z, Jiang C, Wang Y, et al. Engineered extracellular vesicles as intelligent nanosystems for next-generation nanomedicine. Nanoscale Horiz. 2022;7:682–714. doi:10.1039/d2nh00070a
164. Song H, Chen X, Hao Y, et al. Nanoengineering facilitating the target mission: targeted extracellular vesicles delivery systems design. J Nanobiotechnology. 2022;20:431. doi:10.1186/s12951-022-01638-9
165. Liang X, Niu Z, Galli V, et al. Extracellular vesicles engineered to bind albumin demonstrate extended circulation time and lymph node accumulation in mouse models. J Extracell Vesicles. 2022;11:e12248.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Plant-Derived Nanovesicles: Resolving Conceptual Confusion, Overcoming Isolation Challenges, and Advancing Translational Potential
Zhang Z, Chen G, Zheng K, Lin M, Zheng D, Lu Y, Huang L, Chen X, Gan R
International Journal of Nanomedicine 2026, 21:592968
Published Date: 29 April 2026