Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Extent and Factors Associated with Adherence to Antidepressant Treatment During Acute and Continuation Phase Depression Treatment Among Older Adults with Dementia and Major Depressive Disorder
Authors Bhattacharjee S ![]() , Lee JK
, Lee JK ![]() , Vadiei N
, Vadiei N ![]() , Patanwala AE, Malone DC, Knapp SM, Lo-Ciganic WH
, Patanwala AE, Malone DC, Knapp SM, Lo-Ciganic WH ![]() , Burke WJ
, Burke WJ
Received 10 December 2019
Accepted for publication 12 May 2020
Published 8 June 2020 Volume 2020:16 Pages 1433—1450
DOI https://doi.org/10.2147/NDT.S241749
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Sandipan Bhattacharjee,1 Jeannie K Lee,1 Nina Vadiei,1 Asad E Patanwala,2 Daniel C Malone,3 Shannon M Knapp,4 Wei-Hsuan Lo-Ciganic,5 William J Burke6
1Department of Pharmacy Practice and Science, College of Pharmacy, The University of Arizona, Tucson, AZ, USA; 2Sydney Pharmacy School, University of Sydney, Sydney, Australia; 3Department of Pharmacotherapy, Skaggs College of Pharmacy, University of Utah, Salt Lake City, UT, USA; 4Statistics Consulting Laboratory, Bio5 Institute, The University of Arizona, Tucson, AZ, USA; 5Department of Pharmaceutical Outcomes & Policy, College of Pharmacy, University of Florida, Gainesville, FL, USA; 6Banner Alzheimer’s Institute, Phoenix, AZ, USA
Correspondence: Sandipan Bhattacharjee
Department of Pharmacy Practice and Science, The University of Arizona College of Pharmacy, Tucson, AZ, USA
Tel +1 520 626-4124
Fax +1 520-626-7355
Email [email protected]
Purpose: Little is known about adherence to antidepressant treatment during acute and continuation phase of depression among older adults with dementia and newly diagnosed major depressive disorders (MDD). This study estimated the extent of and factors associated with adherence to acute and continuation phase antidepressant treatment among older adults with dementia and newly diagnosed MDD.
Methods: We conducted a retrospective cohort study using the Medicare 5% sample claims data (2012– 2013) among older adults (age≥ 65 years) with dementia who were newly diagnosed with MDD. Intake period of our study was from 01-May-2012 through 30-April-2013. The dependent variables of this study were acute and continuation phase depression treatment adherence. Factors associated with acute and continuation phase antidepressant treatment adherence were identified using multiple logistic regression analyses.
Results: The final study sample consisted of 6239 [adherent: N=4644 (74.44%)] and 5617 [adherent: N=3584 (63.81%)] older adults with dementia and MDD during the acute and continuation phase treatment, respectively. During the acute phase, only race/ethnicity was significantly associated with adherence to depression treatment, whereas race/ethnicity and baseline antipsychotic use were significantly associated with adherence to depression treatment during the continuation phase.
Conclusion: Approximately, 74% and 64% older adults with dementia and MDD were adherent to acute and continuation phase antidepressant treatment in this nationally representative sample of Medicare beneficiaries, and we identified several modifiable and non-modifiable factors associated with adherence.
Keywords: dementia, depression, antidepressants, adherence, acute phase depression, continuation phase depression
Introduction
It is estimated that the global proportion of individuals over 60 years will approximately double from 12% (2015 figure) to 22% in 2050.1 With this aging population, dementia (currently 50 million diagnosed cases globally) and depression (7% of general older adults globally) pose major public health issues.2 This is particularly relevant in the context of the aging population of United States (US). According to a recent estimate, the number of older adults (age ≥65 years) with dementia is expected to increase approximately two-and-half times from 5.8 million in 2020 to 13.8 million in 2050.3 Co-occurring physical and mental chronic conditions burden is high among older adults with dementia, with depression being one of the most prevalent chronic psychiatric conditions in this population.4 It is well documented that presence of depression among older adults with dementia not only decreases the quality of life (QoL), but is also associated with several negative outcomes such as faster cognitive decline, poor adherence to medications, high functional disability, increased rates of institutionalization, and mortality.5–8
Existing studies examining the efficacy/effectiveness of antidepressants to treat depression have shown conflicting findings. Some studies have shown positive effects9–15 while some have shown no beneficial effects16–18 of antidepressants to treat depression among older adults with dementia and depression. A multicenter, randomized, double-blind, placebo-controlled pragmatic trial examining the clinical effectiveness of sertraline and mirtazapine among individuals with Alzheimer’s disease and co-occurring depression failed to demonstrate the clinical effectiveness of sertraline and mirtazapine compared to placebo (all three groups had normal care) in terms of reducing depression.19 However, trend towards the beneficial effect of antidepressants was noted in a recent meta-analysis.20 Moreover, a population-based retrospective cohort study utilizing the National Health Insurance medical claims data demonstrated the protective effects of antidepressants in all-cause mortality among older adults with dementia and depression.21 Thus, there is evidence of potential clinical benefits of antidepressants to treat depression among older adults with dementia and depression.
Currently, there are no depression treatment guidelines for older adults with dementia and MDD. In one of our previous studies,22 we quantified the extent of potentially inappropriate antidepressants among older adults with dementia and newly diagnosed MDD using the National Committee for Quality Assurance’s (NCQA’s) Healthcare Effectiveness Data and Information Set (HEDIS) guidelines for antidepressant medication management (AMM).23 A list of potentially inappropriate antidepressants for older adults with dementia in our recently published study22 was developed using the Beers criteria and Screening Tool of Older Persons’ potentially inappropriate Prescriptions (STOPP) criteria.24,25 Given the evidence supporting the potential benefits of depression treatment and the serious lack of studies examining adherence to depression treatment among older adults with dementia and newly diagnosed MDD, there is a need to examine the status of depression treatment adherence in this vulnerable population. Hence, excluding the potentially inappropriate antidepressants, we sought to estimate the extent of and identify factors associated with adherence to acute and continuation phase antidepressant treatment among older adults with dementia and newly diagnosed MDD using a nationally representative sample of Medicare beneficiaries.
Methods
Study Design
Using Medicare 5% sample claims data (2012–2013), we conducted a retrospective cohort study.
Data Source
We used several data files of the Medicare 5% sample claims data (2012–2013) for the purpose of this study. Data files included in this study were: (i) inpatient; (ii) outpatient; (iii) skilled nursing facility; (iv) carrier; (v) hospice care; (vi) home health agency; (vii) Part D event (PDE); and (viii) durable medical equipment files. Longitudinal follow-up of the Medicare beneficiaries and linking different data files are achieved by a unique de-identified Medicare beneficiary identifier assigned to each beneficiary. Information available in the claims data include: dates of service provided; charge and payment amounts; medication utilization; clinical diagnosis codes; and procedure codes. Demographic (e.g. age, gender, race/ethnicity) and eligibility information are available in the Medicare Beneficiary Summary File (MBSF).
Certain important regional-level factors (such as density of psychiatrists in a zip-code area) that can influence antidepressant adherence are not available in the Medicare dataset. In order to obtain this information, we merged the Area Health Resource File (AHRF) (a publicly available county-specific data) with Medicare dataset using the Social Security Administration codes. We also merged the Medicare dataset with National Plan and Provider Enumeration System (NPPES), also referred to as the National Provider Identifier (NPI) File to obtain provider specialty information from NPIs that appear in the PDE files.
Study Sample
We used the Centers for Medicare and Medicaid Services (CMS) Chronic Conditions Data Warehouse Condition Categories algorithm to identify beneficiaries with dementia.26 Older adults (age ≥65 years) with dementia comprised our study sample. The Intake Period, based on the HEDIS AMM guideline, was from May 1, 2012, through April 30, 2013.23 The date of the first observed prescription claim of antidepressant during the Intake Period was defined as the Index Prescription Start Date (IPSD). For inclusion in the final study sample, the Medicare beneficiaries with dementia were required to have continuous Medicare Part A, B and D enrollment and no Health Maintenance Organizations (HMO) enrollment during the 105 days pre-IPSD, on the IPSD. Additionally, for inclusion in the acute and continuation phase cohort, Medicare beneficiaries with dementia were required to have continuous enrollment throughout the acute phase (114 days post-IPSD) and continuation phase (231 days post-IPSD) respectively.
Medicare beneficiaries were also required to have negative medication history defined as 105 days of no pharmacy claim for either new or refill prescriptions for an antidepressant medication prior to IPSD. Diagnosis of MDD was identified during the 121-day period from 60 days prior to IPSD, through the IPSD, and 60 days post IPSD. Based on HEDIS recommendation, MDD was defined as primary or secondary inpatient, outpatient or carrier claim of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes of 296.2 (major depressive disorder, single episode), 296.3 (major depressive disorder, recurrent episode), 309.1 (prolonged depressive reaction), 300.4 (clinically significant depression), or 311 (depression not elsewhere classified).23 These ICD-9-CM codes have been used in many existing studies to identify clinically significant or major depression.27–30 We considered 105 days before IPSD as the baseline period of our study. Exclusion criteria of our study were: (i) presence of end-stage renal disease (ESRD) at any time during the calendar year of IPSD; (ii) diagnosis of end-stage liver disease (ESLD) during baseline (iii) missing race/ethnicity information, or (iv) missing AHRF information. Additional exclusion criteria for acute phase adherence were: switch to HMO, or death or prescription claim for any inappropriate antidepressant during acute phase. For continuation phase adherence we excluded Medicare beneficiaries who switched to HMO, or died during the continuation phase or had any prescription claim of inappropriate antidepressant during continuation phase treatment. We used the MBSF to identify ESRD, while we used ICD-9-CM codes of 155.0 and 571.0–9 for ESLD identification.31
Dependent Variables
Adherence during acute and continuation phase depression treatment was the dependent variable for this study and was calculated based on the days of supply of antidepressants from prescription claims in the PDE file. Index antidepressants included in this study were those that are not deemed to be potentially inappropriate antidepressants according to the Beers and STOPP criteria.24,25 This list of potentially inappropriate antidepressants has been used in our previous study.22 Antidepressants that were included in this study based on the HEDIS guidelines are presented in Appendix 1. Antidepressants were identified using the National Drug Codes available from the PDE file.
Adherence During Acute Phase Treatment
According to HEDIS, adults with major depression, including older Medicare beneficiaries having dementia, should have ≥85 days of antidepressant use during the first 115 days to be adherent to the acute phase treatment.23
Adherence During Continuation Phase Treatment
Based on HEDIS criteria, adults with major depression, including older Medicare beneficiaries with dementia, should have ≥181 days of antidepressant use during the first 232 days to be adherent to the continuation phase treatment.23
Independent Variables
We included several variables in this study. Demographic characteristics consisted of age (65–74, and 75 years and older); gender (male/female); and race/ethnicity (white and others). Burden of co-occurring conditions during baseline was estimated using the Elixhauser comorbidity index.32 As we used all the Medicare files (excluding PDE and MBSF) to estimate Elixhauser comorbidity burden, we followed the rule-out algorithm (at least 2 diagnosis of interest that were >30 days apart) when using the Medicare physician or outpatient files to avoid overestimation of co-occurring conditions burden; whereas for all other files, only one diagnosis claim was required.32,33 Based on an existing study, we categorized Elixhauser comorbidity score into four non-ordinal groups (0, 1, 2, and ≥3) after summing all 31 individual Elixhauser conditions.33 We identified baseline use of common medications that included: angiotensin-converting-enzyme (ACE) inhibitors, angiotensin II receptor blockers (ARBs), anticoagulants, antidiabetics, antipsychotics, anxiolytics, statins, beta-blockers, calcium-channel blockers, diuretics, antiparkinsonian, and proton pump inhibitors. We identified the baseline diagnosis of Parkinson’s disease (PD) using ICD-9-CM code of 332.xx.34,35 We also examined the baseline use of psychotherapy using Current Procedural Terminology (CPT) codes from existing studies (psychotherapy CPT codes are provided in Appendix 2).36,37 Other variables that we included in this study were: physician specialty (specialty of the doctor that prescribed the index prescription such as Neurology, Psychiatry, General/Family, Other, and Unknown); census region (Northeast, South, Midwest, West); metropolitan residency status (metropolitan/non-metropolitan); and density of each of neurologists and psychiatrists available within the zip code. We categorized each of these densities into four groups (those with 0 and those with >0 divided into tertiles). We also used public assistance (indicated by Medicare premiums and deductibles that are subsidized by the state to indicate the financial status of the enrollee) as one of the individual-level variables in this study.
Statistical Analysis
We compared the adherent and non-adherent groups for each predictor variable by chi-square tests. To identify predictors of adherence during acute and continuation phase depression treatment, we conducted multiple logistic regression analysis. We used a conservative α=0.01 (to decrease Type I error rates) to establish statistical significance for all tests as our study included several variables. We conducted all analyses using SAS version 9.4 (SAS Institute, Cary, NC). When we merged the Medicare PDE files with the NPPES file, some of the NPIs did not match and we categorized them as unknown physician specialty. In order to examine the robustness of our base case analysis, we excluded the observations where the physician specialty was unknown and conducted a sensitivity analysis in that sample.
Results
We present the baseline characteristics of our study sample and the comparisons between adherent and non-adherent groups during acute and continuation phase depression treatment in Tables 1 and 2, respectively. The final study sample consisted of 6239 [adherent: N=4644 (74.44%)] and 5617 [adherent: N=3584 (63.81%)] older adults with dementia and MDD during acute and continuation phase treatment, respectively. Differences in baseline characteristics between adherent and non-adherent groups during the acute phase were observed for race/ethnicity and public assistance, whereas during the continuation phase we observed differences in race/ethnicity, region and baseline antipsychotic use. For example, whites were more adherent during both acute (75.2% vs 68.0%, chi-square test: χ2 = 17.16, df=1, p-value<0.001) and continuation (65.0% vs 54.5%, chi-square test: χ2 = 26.74, df=1, p-value<0.001) phase depression treatment compared to other race/ethnic category.
 |
Table 1 Baseline Characteristics of Antidepressant Adherent and Non-Adherent Groups During Acute Phase Medicare 5% Sample Claims Data (2012–2013) |
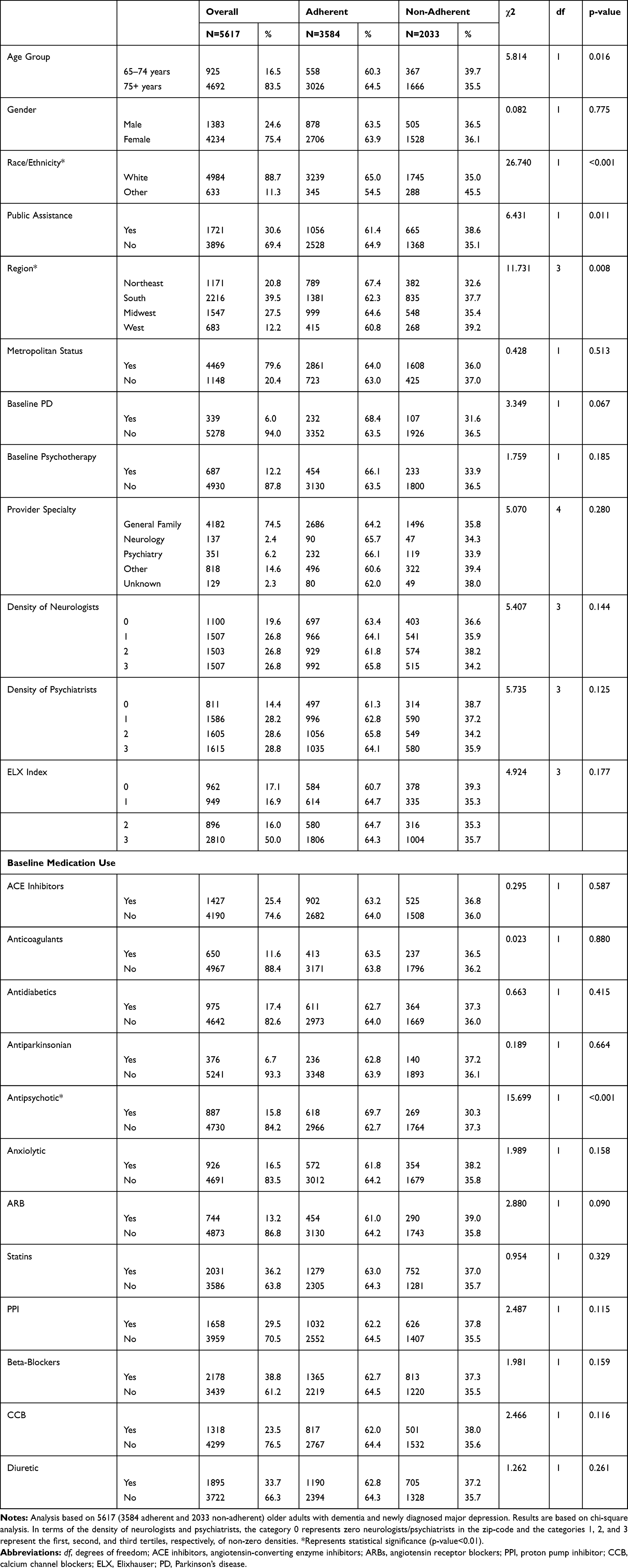 |
Table 2 Baseline Characteristics of Antidepressant Adherent and Non-Adherent Groups During Continuation Phase Medicare 5% Sample Claims Data (2012–2013) |
In Table 3, we present the class-based as well as individual antidepressant utilization distributions for adherent and non-adherent groups during acute and continuation phase depression treatment. We observed statistically significant differences with respect to adherence among index antidepressant classes during both acute (chi-square test: χ2 = 20.7, df=4, p-value<0.001) and continuation phase (chi-square test: χ2 = 15.2, df=4, p-value=0.004) depression treatment with the antidepressant category “Other” exhibiting the highest adherence among the classes. While we did not conduct chi-square tests among the individual antidepressants to compare adherent and non-adherent groups, of the Medicare beneficiaries included in the analysis of continuation phase adherence, the most common index antidepressants were sertraline (N=1386) and citalopram (N=1381) whereas it were citalopram (N=1260) and sertraline (N=1245) for continuation phase.
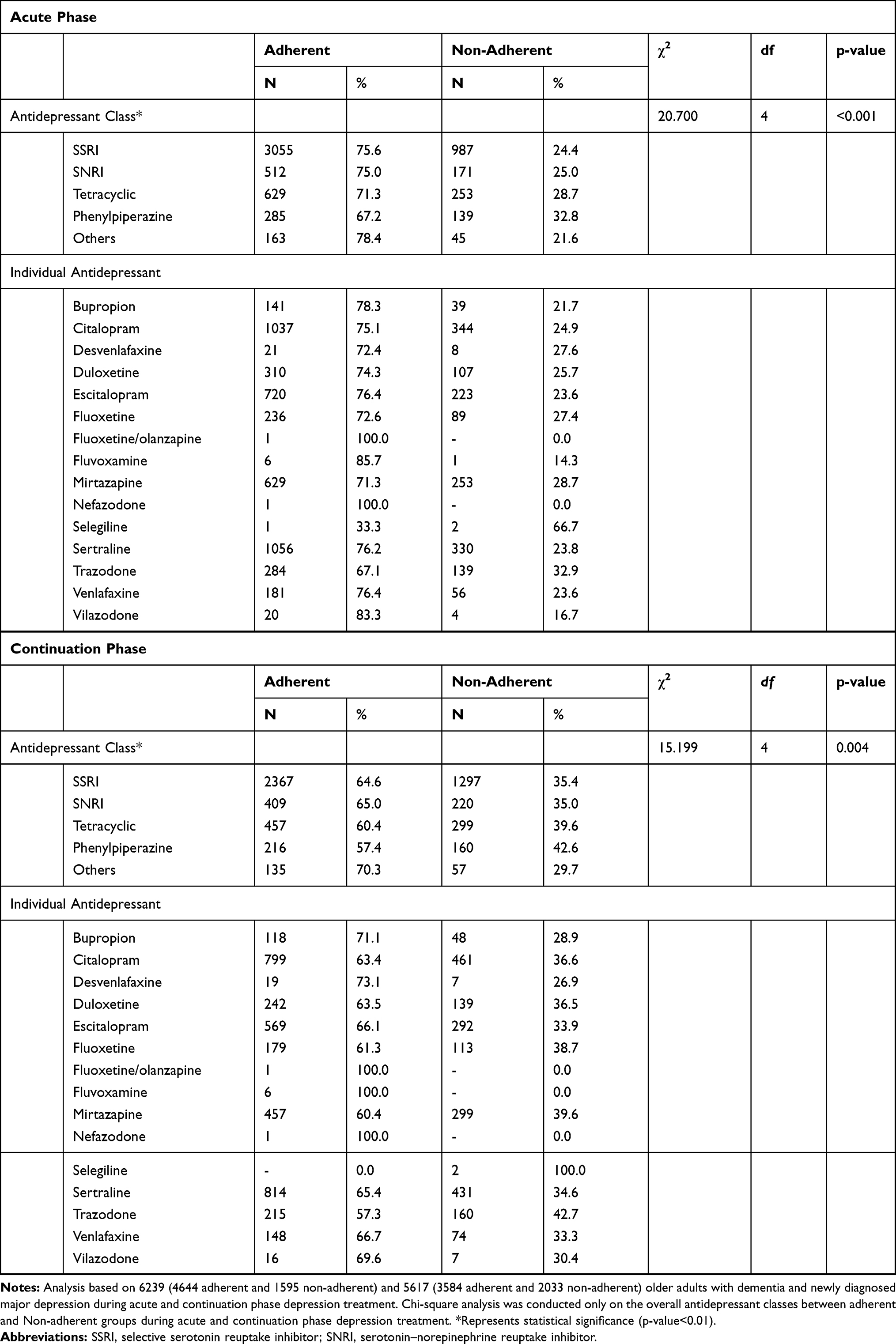 |
Table 3 Description of Antidepressant Medication Initiation by Class-Level and Individuals-Level in Acute and Continuation Phase Medicare 5% Sample Claims Data (2012–2013) |
We present the findings from multiple logistic regression analysis during acute and continuation phase depression treatment in Tables 4 and 5, respectively. During the acute phase, only race/ethnicity was significantly associated with adherence to depression treatment, with whites having 30% [Adjusted Odds Ratio (AOR): 1.30, 99% CI: 1.02–1.66, multiple logistic regression analysis Wald χ2 = 7.99, p =0.005] higher odds of being adherent compared to non-whites. We observed similar findings in terms of race/ethnicity during continuation phase treatment, with whites having a 49% (AOR: 1.49, 99% CI: 1.18–1.89, multiple logistic regression analysis Wald χ2 = 18.79, p<0.001) higher chance of depression treatment adherence than non-whites. In addition, during continuation phase depression treatment, baseline antipsychotic use was associated with 43% (AOR: 1.43, 99% CI: 1.16–1.76, multiple logistic regression analysis Wald χ2 = 18.80, p<0.001) higher odds of depression treatment adherence among older adults with dementia and newly diagnosed MDD.
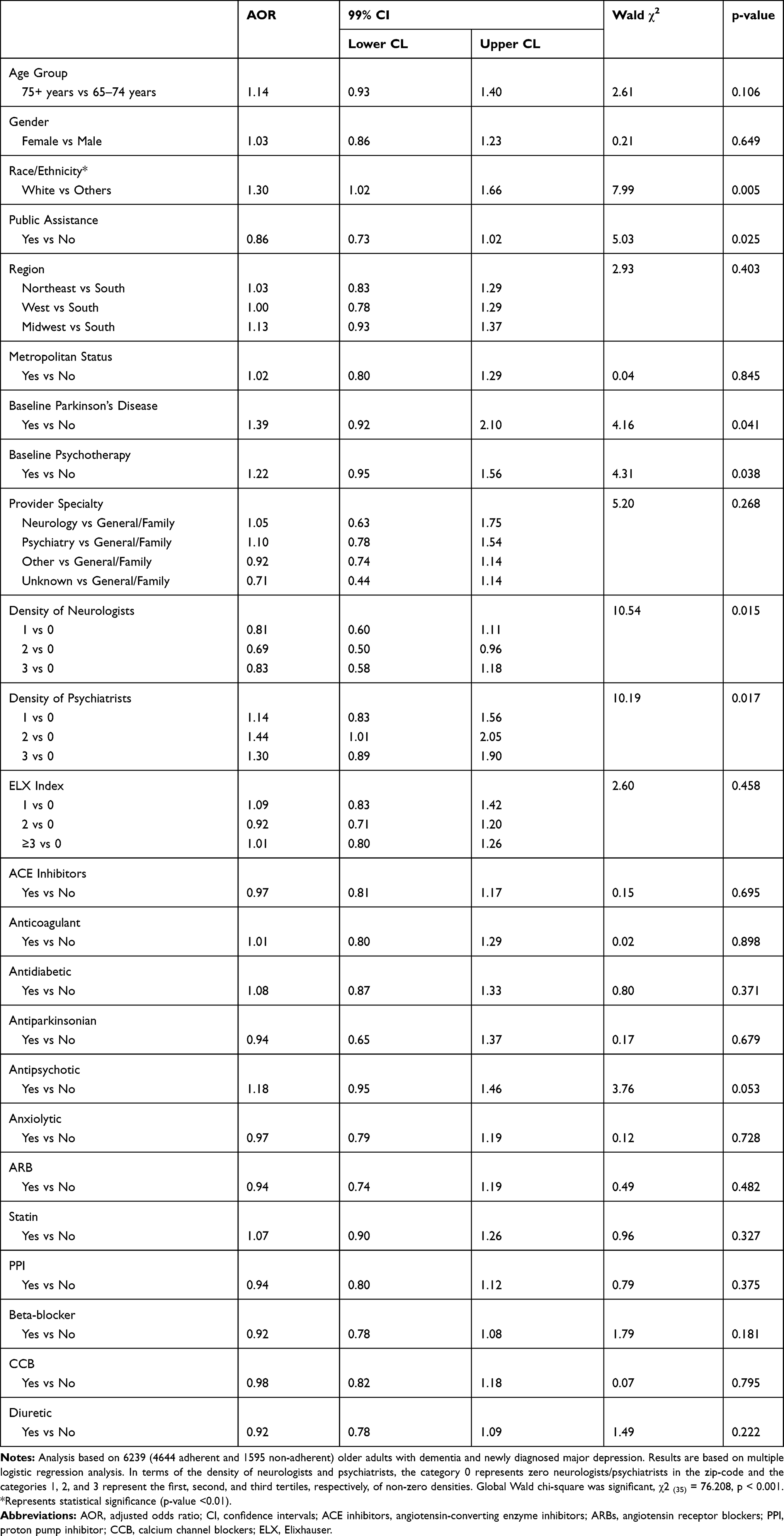 |
Table 4 Predictors of Adherence During Acute Phase Depression Treatment |
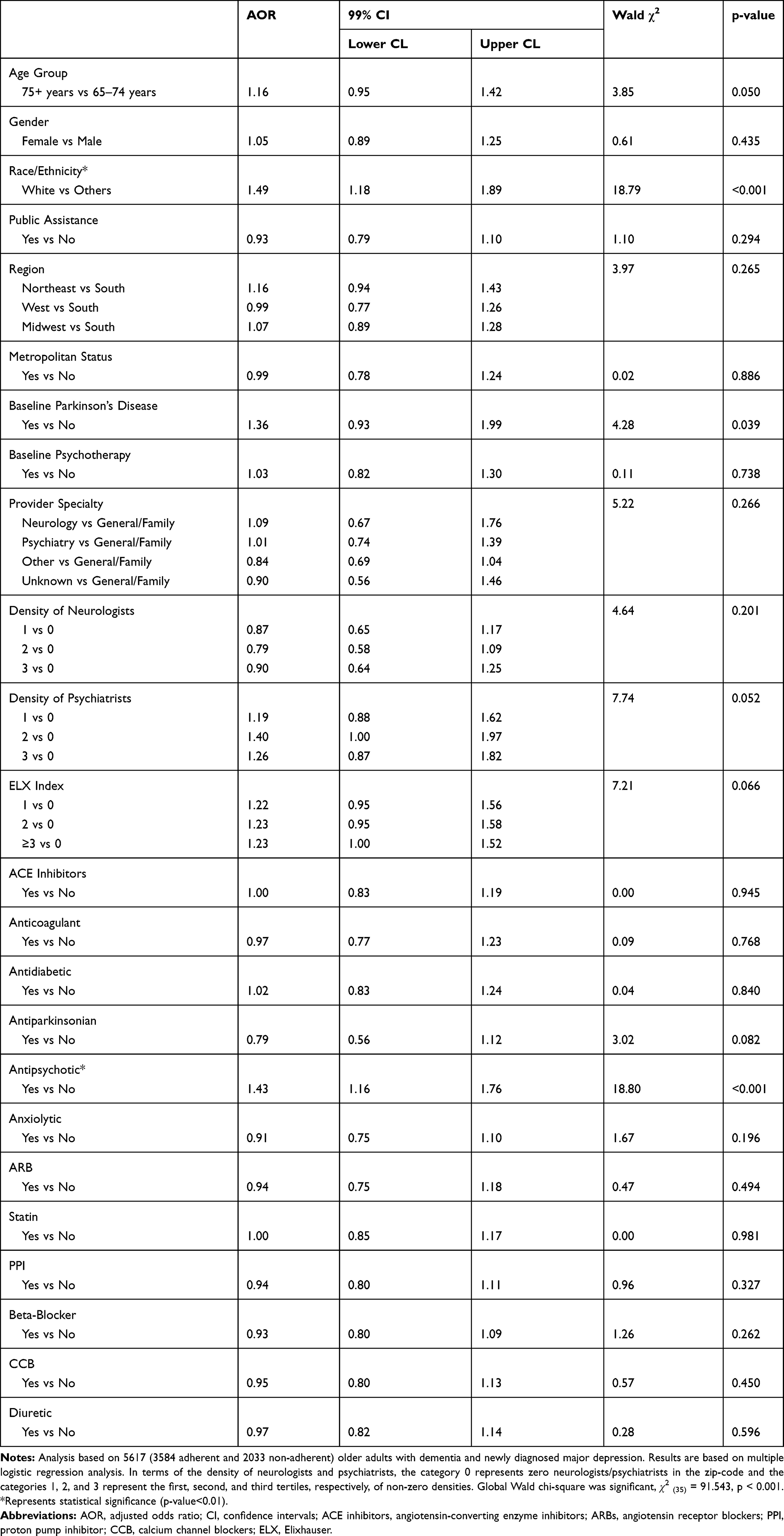 |
Table 5 Predictors of Adherence During Continuation Phase Depression Treatment |
We conducted a sensitivity analysis by removing the observations where the physician specialty was unknown (NAcute=141 and NContinuation=129). Findings from these sensitivity analyses are presented in Supplemental Tables 1–5. Overall, the findings from sensitivity analyses were similar to our primary analysis except that the density of neurologists and psychiatrists was also significantly associated with antidepressant adherence during acute phase treatment.
Discussion
To the best of our knowledge, this is the first study examining the adherence to antidepressants during both acute and continuation phases of depression treatment among older adults with dementia and MDD in a nationally representative sample of Medicare beneficiaries. This study uniquely contributes to the existing knowledge by informing us about the current state of antidepressant adherence as well as identifying the modifiable and non-modifiable factors associated with antidepressant adherence in this vulnerable population in the US. It is critical to identify the factors associated with antidepressant adherence in order to develop appropriate interventions to improve adherence that can lead to better health outcomes (e.g. antidepressant use showed protective effect against all-cause mortality in a similar population in Taiwan21).
Though our study categorized race/ethnicity into only 2 groups – White (Non-Hispanic Whites) and Other (non-White race and Hispanics), minority older adults with dementia were at higher risk of non-adherence with depression treatment compared with white older adults. This data provides additional evidence about health disparities among older people with dementia and depression, supplementing our previous research that showed minority older patients received significantly less depression treatment (antidepressants alone or antidepressant + psychotherapy) compared with white older patients.38 Such treatment disparity has been a consistent finding across several studies.39–43 In fact, the research that has found evidence of treatment disparities of minority patients with depression has accumulated over more than 20 years.44 Examples of reasons for depression treatment disparities include access issues (affordability, transportation), health literacy, cultural factors, patient beliefs about disease and medications, and patient–provider relationship.44 Furthermore, a recent study by our research team that evaluated the appropriateness of antidepressant selection for the older population having dementia and depression found almost equivalent rates of inappropriate antidepressant initiation between White subjects (7.6%) and their non-White counterparts (7.5%).22 Although race/ethnicity did not differ between inappropriate and appropriate antidepressants initiated by the study sample in our previous study,22 we know that not as many minority older patients are initiated on an antidepressant; thus, the similar rate of inappropriate prescribing was an unfortunate finding.
At the same time, there is a lack of research examining depression treatment adherence among older adults with dementia. A wide range of adherence (20–80%) has been reported for depression medications, while poorer adherence rates, along with lower social support, greater limitations with daily living activities and higher baseline depression scores, have been associated with higher 12-month depression scores among older adults.45 In the current study, non-Whites exhibited a higher risk of depression medication non-adherence than Whites among older adults with dementia and MDD. Because multiple factors contribute to depression medication non-adherence,46 there likely are several reasons for racial/ethnic differences in adherence, particularly among older patients with dementia. A study showed that African Americans and Latino patients accepted treatment for depression less often than White patients.47 Another study found that African Americans reported greater concerns about depression treatment.48 In the same study, White women had significantly higher antidepressant adherence compared to African-American women, and the belief about the importance of antidepressants and fewer concerns regarding antidepressants were associated with higher adherence. This study suggested that interventions targeting improved patient-provider communication, and culturally sensitive education and motivational enhancement may improve depression medication adherence.48
Above mentioned gaps and disparities exist in the presence of no clear clinical guideline on treating depression among older adults with dementia. Therefore, a treatment guideline tailored to older patients with dementia and MDD is critically needed. Such clinical guidelines should emphasize appropriate antidepressant prescribing for older adults with dementia and emphasize treating minority patients as well as the importance of adherence. One perspective recommended research into help-seeking behaviors by individuals that may uncover cultural and contextual factors that influence treatment decisions.44 This seems to be a valuable research direction since beliefs about health and medications, social support, and environmental barriers can determine depression treatment and adherence as described in the above sections. To reduce racial and ethnic disparities in antidepressant adherence among older people with dementia and MDD, an innovative and effective intervention is warranted that addresses barriers specific to minority populations, including cultural beliefs. In addition, though our study subjects were community-dwelling, because there are patients with dementia of varying degrees in the communities across the US, it is important to involve care partners in interventions to enhance adherence.
A surprising finding from the present study is that older adults with dementia and MDD who used antipsychotics had higher antidepressant adherence compared with those who did not use antipsychotics. The difficulty of interpreting this result is that claims for antipsychotics in the data cannot be linked to a particular diagnosis, and antipsychotics may be used as an adjunctive treatment of depression or for behavioral symptoms related to dementia, in addition to psychiatric illnesses such as schizophrenia and bipolar disorder. Also, we do not have severity information related to depression or dementia in Medicare claims data. Thus, we can only guess what might be the reason for the difference. A presumption is that if study subjects’ depression was better controlled due to the use of adjunct antipsychotics, their improved condition may have led to better medication adherence of antidepressants. Similarly, if the study patients’ dementia-related behavioral symptoms, such as hyperactivity or agitation, were improved due to their antipsychotic use, medication adherence may have improved as a consequence. Therefore, future studies should further explore the relationship between antipsychotic use and antidepressant adherence among older adults with dementia and MDD to confirm our findings. Moreover, factors driving the relationship may be investigated and included in building an optimal adherence intervention for older adults with dementia and depression.
A higher percentage of older adults with dementia and newly diagnosed MDD were adherent to depression treatment during the acute phase compared to the continuation phase, which is unsurprising because the acute phase is a subset of the continuation phase. This finding is reflective of previous studies demonstrating many patients do not continue treatment for the recommended length of time in the continuation phase of treatment.49–53 For example, a study by Akincigil et al found that 51% of privately insured patients diagnosed with depression were adherent to depression treatment during the acute phase, but this dropped to 42% being adherent in the continuation phase.49 The goal of acute-phase treatment is to relieve symptoms of depression, while the continuation phase is meant to prevent relapse.54 Since symptoms tend to resolve during the acute treatment phase, it makes sense that some patients choose to discontinue treatment during the continuation phase. This can occur if patients no longer understand the need to continue treatment when they are feeling better. In fact, lack of patient education regarding the duration of therapy has been found to be one of the most important causes of early treatment discontinuation.55 Patients may also wish to be on fewer medications and see the resolution in their depressive symptoms as an opportunity to reduce the number of medications they are taking.
In our study, Medicare beneficiaries who initiated on antidepressants in the “Others” category were more likely to be adherent compared to Selective Serotonin Reuptake Inhibitors (SSRIs), Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs), tetracyclic and phenylpiperazine antidepressants. This may be due to differences in the side-effect profiles of the different antidepressant classes. For example, bupropion is often prescribed for patients who are more distressed by having low energy, which is a common symptom in both dementia and depression.56 This is an example of how medication side-effects can be used to help target specific symptoms that are common in this patient population. SSRIs and SNRIs tend to have milder side-effects,57 meaning it may be more difficult for patients to notice acute changes when starting these medication classes. As antidepressants often take weeks to become efficacious,57 it can be discouraging for patients/caregivers to not notice any changes during the first few weeks of treatment, which may consequently lead to early treatment discontinuation. However, medications like bupropion may lead to certain symptoms improving more quickly58 (e.g. fatigue), resulting in patients/caregivers feeling more hopeful.
Findings from our main analysis were similar to the sensitivity analysis except that both the density of neurologist and density of psychiatrist showed a significant negative and positive association with antidepressant adherence during the acute phase of depression treatment. While it is challenging to explain these findings based on our data, we can speculate that early and close access to psychiatrists during the acute phase of depression treatment may help in improving antidepressant adherence among older adults with dementia and depression. Future research should investigate the effect of the density of specialists on antidepressant adherence in more detail.
Some of the strengths of the current study are the possibility of generalizability of our study findings due to the use of a large nationally representative sample of Medicare beneficiaries, absence of recall bias and utilization of a strong depression treatment framework. A few limitations such as possibility of coding error (as with any secondary database), use of prescription claims to measure adherence and lack of severity measure if dementia and depression in claims data. Moreover, the independent variables examined for being the predictors of adherence to antidepressants in our study were limited to the availability of these variables in the datasets; there could be other factors (such as caregiver effect) that influence the antidepressant adherence in our study sample. Furthermore, it should be noted that antidepressants can be used to treat other conditions such as sedation, agitation, sleep and appetite stimulation but the exact reason for antidepressant use cannot be determined from the Medicare claims data. And finally, given the range of years of data (2012–2013) used in this study, it may not represent the current status of depression treatment among Medicare beneficiaries with dementia and MDD.
Conclusion
Approximately 74% and 64% of older adults with dementia and MDD were adherent to acute and continuation phase antidepressant treatment in this nationally representative sample of Medicare beneficiaries. Race/ethnicity was significantly associated with adherence during both acute and continuation phases.
Data Sharing Statement
The data used in this study (Medicare 5% sample claims data) can be procured from the Centers for Medicare & Medicaid Services (CMS) via a Data Use Agreement (DUA). While we will not be able to share the data used in this study based on our DUA, but we will be happy to share our DUA files with researchers upon reasonable request so that they can obtain the Medicare 5% sample claims data from CMS.
Ethical Approval
The Human Subjects Protection Program Institutional Review Board (IRB) of The University of Arizona approved this study and determined that human subjects review is not required for this study.
Acknowledgments
The authors would like to thank Ms. Zufan Yegezu for her help with the formatting of this manuscript. The abstract of this paper was presented at the International Society for Pharmacoeconomics and Outcomes Research 24th Annual International Meeting (May 18–22, 2019; New Orleans, LA, USA) as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in Value in Health journal (May 2019, Volume 22, Supplement 2, Page S287): https://doi.org/10.1016/j.jval.2019.04.1365.
Disclosure
Dr Sandipan Bhattacharjee reports grants from National Institute of Mental Health, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. World Health Organization (WHO). Ageing and health. 2018. Available from: https://www.who.int/news-room/fact-sheets/detail/ageing-and-health.
2. World Health Organization (WHO). Mental health of older adults. 2017. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-of-older-adults.
3. Alzheimer’s Association. Alzheimer’s disease facts and figures. 2020. Available from: https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf.
4. Steinberg M, Shao H, Zandi P, et al. Point and 5-year period prevalence of neuropsychiatric symptoms in dementia: the cache county study. Int J Geriatr Psychiatry. 2008;23(2):170–177. doi:10.1002/gps.1858
5. Appleby BS, Roy P, Valenti A, Lee HB. Diagnosis and treatment of depression in Alzheimer’s disease: impact on mood and cognition. Panminerva Med. 2007;49(3):139–149.
6. Netuveli G, Blane D. Quality of life in older ages. Br Med Bull. 2008;85:113–126. doi:10.1093/bmb/ldn003
7. Kales HC, Chen P, Blow FC, Welsh DE, Mellow AM. Rates of clinical depression diagnosis, functional impairment, and nursing home placement in coexisting dementia and depression. Am J Geriatr Psychiatry. 2005;13(6):441–449. doi:10.1097/00019442-200506000-00002
8. Buettner LL, Fitzsimmons S, Dudley WN. Impact of underlying depression on treatment of neuropsychiatric symptoms in older adults with dementia. Res Gerontol Nurs. 2010;3(3):221–232. doi:10.3928/19404921-20100601-02
9. Buhr GT, White HK. Difficult behaviors in long-term care patients with dementia. J Am Med Dir Assoc. 2006;7(3):180–192. doi:10.1016/j.jamda.2005.12.003
10. Herrmann N, Lanctot KL. Pharmacologic management of neuropsychiatric symptoms of alzheimer disease. Can J Psychiatry. 2007;52(10):630–646. doi:10.1177/070674370705201004
11. Sink KM, Holden KF, Yaffe K. Pharmacological treatment of neuropsychiatric symptoms of dementia: a review of the evidence. JAMA. 2005;293(5):596–608. doi:10.1001/jama.293.5.596
12. Lyketsos CG, DelCampo L, Steinberg M, et al. Treating depression in Alzheimer disease: efficacy and safety of sertraline therapy, and the benefits of depression reduction: the DIADS. Arch Gen Psychiatry. 2003;60(7):737–746. doi:10.1001/archpsyc.60.7.737
13. Caballero J, Hitchcock M, Beversdorf D, Scharre D, Nahata M. Long-term effects of antidepressants on cognition in patients with Alzheimer’s disease. J Clin Pharm Ther. 2006;31(6):593–598. doi:10.1111/j.1365-2710.2006.00778.x
14. Starkstein SE, Mizrahi R. Depression in Alzheimer’s disease. Expert Rev Neurother. 2006;6(6):887–895. doi:10.1586/14737175.6.6.887
15. Cooper JP. Buspirone for anxiety and agitation in dementia. J Psychiatry Neurosci. 2003;28(6):469.
16. Rosenberg PB, Martin BK, Frangakis C, et al. Sertraline for the treatment of depression in Alzheimer disease. Am J Geriatr Psychiatry. 2010;18(2):136–145. doi:10.1097/JGP.0b013e3181c796eb
17. Weintraub D, Rosenberg PB, Drye LT, et al. Sertraline for the treatment of depression in Alzheimer disease: week-24 outcomes. Am J Geriatr Psychiatry. 2010;18(4):332–340. doi:10.1097/JGP.0b013e3181cc0333
18. Dudas R, Malouf R, McCleery J, Dening T. Antidepressants for treating depression in dementia. Cochrane Database Syst Rev. 2018;8:CD003944.
19. Banerjee S, Hellier J, Romeo R, et al. Study of the use of antidepressants for depression in dementia: the HTA-SADD trial–a multicentre, randomised, double-blind, placebo-controlled trial of the clinical effectiveness and cost-effectiveness of sertraline and mirtazapine. Health Technol Assess. 2013;17(7):1–166. doi:10.3310/hta17070
20. Orgeta V, Tabet N, Nilforooshan R, Howard R. Efficacy of antidepressants for depression in Alzheimer’s disease: systematic review and meta-analysis. J Alzheimers Dis. 2017;58(3):725–733. doi:10.3233/JAD-161247
21. Su JA, Chang CC, Wang HM, Chen KJ, Yang YH, Lin CY. Antidepressant treatment and mortality risk in patients with dementia and depression: a nationwide population cohort study in Taiwan. Ther Adv Chronic Dis. 2019;10:2040622319853719. doi:10.1177/2040622319853719
22. Bhattacharjee S, Lee JK, Patanwala AE, et al. Extent and predictors of potentially inappropriate antidepressant use among older adults with dementia and major depressive disorder. Am J Geriatr Psychiatry. 2019;27(8):794–805. doi:10.1016/j.jagp.2019.02.002
23. Assurance NCfQ. HEDIS Technical Specifications. Vol. 2. Washington, DC: National Committee for Quality Assurance; 2016:160–163.
24. By the American Geriatrics Society Beers Criteria Update Expert P. American Geriatrics Society 2015 updated beers criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2015;63(11):2227–2246. doi:10.1111/jgs.13702
25. O’Mahony D, O’Sullivan D, Byrne S, O’Connor MN, Ryan C, Gallagher P. STOPP/START criteria for potentially inappropriate prescribing in older people: version 2. Age Ageing. 2015;44(2):213–218. doi:10.1093/ageing/afu145
26. Centers for Medicare and Medicaid Services. Chronic conditions data warehouse. Available from: https://www.ccwdata.org/web/guest/condition-categories. 2016.
27. Wei W, Sambamoorthi U, Olfson M, Walkup JT, Crystal S. Use of psychotherapy for depression in older adults. Am J Psychiatry. 2005;162(4):711–717. doi:10.1176/appi.ajp.162.4.711
28. Crystal S, Sambamoorthi U, Walkup JT, Akincigil A. Diagnosis and treatment of depression in the elderly medicare population: predictors, disparities, and trends. J Am Geriatr Soc. 2003;51(12):1718–1728. doi:10.1046/j.1532-5415.2003.51555.x
29. Sambamoorthi U, Olfson M, Walkup JT, Crystal S. Diffusion of new generation antidepressant treatment among elderly diagnosed with depression. Med Care. 2003;41(1):180–194. doi:10.1097/00005650-200301000-00019
30. Sambamoorthi U, Shen C, Findley P, Frayne S, Banerjea R. Depression treatment patterns among women veterans with cardiovascular conditions or diabetes. World Psychiatry. 2010;9(3):177–182. doi:10.1002/j.2051-5545.2010.tb00306.x
31. Perez A, Anzaldua M, McCormick J, Fisher-Hoch S. High frequency of chronic end-stage liver disease and hepatocellular carcinoma in a Hispanic population. J Gastroenterol Hepatol. 2004;19(3):289–295. doi:10.1111/j.1440-1746.2003.03277.x
32. Quan H, Sundararajan V, Halfon P, et al. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med Care. 2005;43(11):1130–1139. doi:10.1097/01.mlr.0000182534.19832.83
33. Zhu CW, Cosentino S, Ornstein KA, Gu Y, Andrews H, Stern Y. Interactive effects of dementia severity and comorbidities on medicare expenditures. J Alzheimers Dis. 2017;57(1):305–315. doi:10.3233/JAD-161077
34. Bhattacharjee S, Metzger A, Tworek C, Wei W, Pan X, Sambamoorthi U. Parkinson’s disease and home healthcare use and expenditures among elderly medicare beneficiaries. Parkinsons Dis. 2015;2015:606810.
35. Noyes K, Liu H, Holloway R, Dick AW. Accuracy of medicare claims data in identifying parkinsonism cases: comparison with the medicare current beneficiary survey. Mov Disord. 2007;22(4):509–514. doi:10.1002/mds.21299
36. Bhattacharya R, Shen C, Wachholtz AB, Dwibedi N, Sambamoorthi U. Depression treatment decreases healthcare expenditures among working age patients with comorbid conditions and type 2 diabetes mellitus along with newly-diagnosed depression. BMC Psychiatry. 2016;16:247. doi:10.1186/s12888-016-0964-9
37. Harpaz-Rotem I, Libby D, Rosenheck RA. Psychotherapy use in a privately insured population of patients diagnosed with a mental disorder. Soc Psychiatry Psychiatr Epidemiol. 2012;47(11):1837–1844. doi:10.1007/s00127-012-0486-9
38. Bhattacharjee S, Oh YM, Reiman EM, Burke WJ. Prevalence, patterns, and predictors of depression treatment among community-dwelling elderly individuals with dementia in the United States. Am J Geriatr Psychiatry. 2017;25(7):803–813. doi:10.1016/j.jagp.2017.03.003
39. Akincigil A, Olfson M, Siegel M, Zurlo KA, Walkup JT, Crystal S. Racial and ethnic disparities in depression care in community-dwelling elderly in the United States. Am J Public Health. 2012;102(2):319–328. doi:10.2105/AJPH.2011.300349
40. Alegria M, Chatterji P, Wells K, et al. Disparity in depression treatment among racial and ethnic minority populations in the United States. Psychiatr Serv. 2008;59(11):1264–1272. doi:10.1176/ps.2008.59.11.1264
41. Miranda J, Cooper LA. Disparities in care for depression among primary care patients. J Gen Intern Med. 2004;19(2):120–126. doi:10.1111/j.1525-1497.2004.30272.x
42. Health UDoHaHSM. Culture, Race, and Ethnicity a Supplement to Mental Health: A Report of the Surgeon General. Rockville, MD: US Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services; 2001:2001.
43. Gonzalez HM, Vega WA, Williams DR, Tarraf W, West BT, Neighbors HW. Depression care in the United States: too little for too few. Arch Gen Psychiatry. 2010;67(1):37–46. doi:10.1001/archgenpsychiatry.2009.168
44. Cardemil EV, Nelson T, Keefe K. Racial and ethnic disparities in depression treatment. Curr Opin Psychol. 2015;4:37–42. doi:10.1016/j.copsyc.2015.01.021
45. Bosworth HB, Voils CI, Potter GG, Steffens DC. The effects of antidepressant medication adherence as well as psychosocial and clinical factors on depression outcome among older adults. Int J Geriatr Psychiatry. 2008;23(2):129–134. doi:10.1002/gps.1852
46. Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
47. Cooper LA, Gonzales JJ, Gallo JJ, et al. The acceptability of treatment for depression among African-American, hispanic, and white primary care patients. Med Care. 2003;41(4):479–489. doi:10.1097/01.MLR.0000053228.58042.E4
48. Burnett-Zeigler I, Kim HM, Chiang C, et al. The association between race and gender, treatment attitudes, and antidepressant treatment adherence. Int J Geriatr Psychiatry. 2014;29(2):169–177. doi:10.1002/gps.3984
49. Akincigil A, Bowblis JR, Levin C, Walkup JT, Jan S, Crystal S. Adherence to antidepressant treatment among privately insured patients diagnosed with depression. Med Care. 2007;45(4):363–369. doi:10.1097/01.mlr.0000254574.23418.f6
50. Gaspar FW, Zaidel CS, Dewa CS. Rates and determinants of use of pharmacotherapy and psychotherapy by patients with major depressive disorder. Psychiatr Serv. 2019;70(4):262–270. doi:10.1176/appi.ps.201800275
51. Katon W, von Korff M, Lin E, Bush T, Ormel J. Adequacy and duration of antidepressant treatment in primary care. Med Care. 1992;30(1):67–76. doi:10.1097/00005650-199201000-00007
52. Croghan TW, Melfi CA, Dobrez DG, Kniesner TJ. Effect of mental health specialty care on antidepressant length of therapy. Med Care. 1999;37(4Suppl Lilly):AS20–AS23. doi:10.1097/00005650-199904001-00004
53. Pampallona S, Bollini P, Tibaldi G, Kupelnick B, Munizza C. Patient adherence in the treatment of depression. Br J Psychiatry. 2002;180:104–109. doi:10.1192/bjp.180.2.104
54. Work Group on Major Depressive Disorder. Practice guideline for the treatment of patients with major depressive disorder: third edition. 2010. Available from: https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/mdd.pdf.
55. Bull SA, Hu XH, Hunkeler EM, et al. Discontinuation of use and switching of antidepressants: influence of patient-physician communication. JAMA. 2002;288(11):1403–1409. doi:10.1001/jama.288.11.1403
56. Foley KF, DeSanty KP, Kast RE. Bupropion: pharmacology and therapeutic applications. Expert Rev Neurother. 2006;6(9):1249–1265. doi:10.1586/14737175.6.9.1249
57. Santarsieri D, Schwartz TL. Antidepressant efficacy and side-effect burden: a quick guide for clinicians. Drugs Context. 2015;4:212290. doi:10.7573/dic.212290
58. Quitkin FM, Taylor BP, Kremer C. Does mirtazapine have a more rapid onset than SSRIs? J Clin Psychiatry. 2001;62(5):358–361. doi:10.4088/JCP.v62n0509
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.