Back to Journals » International Medical Case Reports Journal » Volume 15
Extensive Lower Limb Deep Vein Thrombosis Provoked by Gastroenteritis-Induced Dehydration: A Case Report for Unusual Precipitating Factor
Authors Shbeer A ![]()
Received 12 October 2022
Accepted for publication 26 November 2022
Published 6 December 2022 Volume 2022:15 Pages 713—718
DOI https://doi.org/10.2147/IMCRJ.S392338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Abdullah Shbeer
College of Medicine, Jazan University, Jazan, 45142, Saudi Arabia
Correspondence: Abdullah Shbeer, College of Medicine, Jazan University, Jazan, 45142, Saudi Arabia, Tel +966505769570, Email [email protected]
Abstract: The incidence of deep vein thrombosis (DVT) has been related to a number of risk factors, including genetic and acquired prothrombotic conditions, infections, inflammatory diseases, hematologic disorders, trauma, and drug use. Dehydration is a known independent risk factor for the development of thrombosis; however possibly insufficient evidence to form a strong association. The purpose of this case report is to present a 30-year-old male with DVT provoked by acute gastroenteritis-induced dehydration. The patient presented to the emergency department (ED) with a recent history of watery diarrhea for four days, for which he was diagnosed with gastroenteritis and managed at an outpatient care facility. The patient visited the ED again with a complaint of a one-day history of progressively worsening continuous pain in his left lower calf associated with swelling. The ultrasound-Doppler/duplex scan for the left lower limb venous system showed negative augmentation signs and non-compressibility of the deep venous system with partial occlusion/echogenic thrombosis extending from the external iliac vein, saphenofemoral junction, superficial femoral vein, popliteal vein, anterior tibial vein, and posterior tibial artery vena comitans. The patient was diagnosed with acute extensive DVT (multiple emboli). Patient care (medical treatment plan/therapeutic anticoagulation) was started in the ED and continued in the Critical Care Unit for close monitoring and care for a couple of days, after which he was transferred to the ward and then discharged in stable condition. He was prescribed a three-month course of appropriate medication regimen. This rare case presentation is a reminder to emergency physicians that dehydration might induce DVT and all patients, regardless of age, diagnosis or comorbidities, should always be risk assessed upon presentation and discharge, and prophylaxis should be provided according to their risk profile.
Keywords: deep vein thrombosis, dehydration, gastroenteritis, pulmonary embolism, thromboembolism
Introduction
Deep vein thrombosis (DVT) occurs when a blood clot (thrombus) forms in one or more of the deep veins in the body. DVTs can occur in the upper and lower extremities. In the lower extremity, they are typically classified as either proximal, affecting the popliteal, femoral, or iliac veins, or distal, affecting the calves and lower leg veins.1 While all DVTs are dangerous, proximal DVTs are more likely to result in a pulmonary embolism (PE), which is responsible for 10% of all hospital deaths.2 The importance of monitoring for and diagnosing DVTs in hospitalized patients is well understood, but DVTs discovered during outpatient care, particularly in the younger population, are less frequently discussed.3 The incidence of DVT varies in different parts of the world for reasons that are not yet completely understood. The DVT incidence in the general population has been estimated to be 53.1 per 100,000 in Korea4 and 162 per 100,000 population in Sweden.5 In the United States, DVT-associated massive PE causes as many as 300,000 deaths annually.6
Making an accurate diagnosis of DVT can be difficult; in fact, research has indicated that clinical signs and symptoms alone are not sufficient for obtaining a diagnosis of DVT.7,8 Moreover, about 80% of DVTs are clinically asymptomatic.9 For the 20% symptomatic patients, the reported signs and symptoms are easily confused with those of other prevalent musculoskeletal illnesses.10
Various studies have been conducted to identify DVT risk factors, as demonstrated in the literature.11,12 Although it is widely assumed that dehydration predisposes to venous thromboembolism (VTE), there are no clinical studies to support this.13 However, expert advisory committees and international guidelines have highlighted dehydration as a risk factor.14,15 Moreover, in adult and pediatric cerebral thrombosis, dehydration has been reported as a direct cause of cerebral venous thrombosis (CVT).16 Notably, there is no published case report that the authors are aware of that presents the findings of a DVT provoked by gastroenteritis-induced dehydration in a young, healthy male, in which dehydration was suggested as a possible cause. Therefore, the goal of this case report is to describe the diagnosis of a DVT in a young, healthy male who reported to the emergency department (ED) following gastroenteritis.
Case Presentation
A 30-year-old male patient, who is not known to have any medical illness, presented with a recent history of watery diarrhea for four days, for which he sought medical care. He was diagnosed with gastroenteritis and managed at an outpatient care facility. He presented again to the ED with a one-day history of progressively worsening continuous pain in his left lower calf associated with swelling. The patient has no history of trauma, recent surgery, travel, prolonged inactivity, or similar complaints. He has never smoked, and he does not drink alcohol. The patient denied any history of chest pain, dyspnea, or shortness of breath. He also denied any family history of thromboembolism, bleeding, or clotting disorders.
His initial vital signs upon arrival to the ED were as follows: blood pressure of 150/90 mmHg, heart rate of 110 beats per minute (bpm), respiratory rate of 15 breaths per minute, and temperature of 37° Celsius, with oxygen saturation of 99% on room air. The patient showed signs of dehydration, including dry mouth and tongue, tiredness, sunken eyes, and dry skin.
For the physical exam, the results of the neurological, cardiovascular, and respiratory system examinations were within normal limits. Regarding the lower extremities, his left calf was tender to palpation, with mild to moderate swelling on the left leg in comparison with the right lower limb. Extremity pulses (femoral, popliteal, posterior tibial, and dorsalis pedis arteries) were all intact and normal in both lower extremities.
Diagnostic laboratory studies, including hematology, autoimmune disease, immunochemistry, chemistry and urinalysis, were conducted (Table 1). His protein C and protein S levels were tested to help investigate the cause of DVT and to determine whether the patient may have a protein C or protein S deficiency. The results were in the normal range. Autoimmune disease and immunochemistry tests were obtained for antibodies associated with thrombosis, which is necessary for differential diagnosis and disease classification of autoimmune diseases. Negative results were concluded based on the laboratory tests. The result of the urine specific gravity test was slightly above the normal range (1.034). Blood urea nitrogen (BUN) and hematocrit (HCT) were found within the normal range, although the BUN was geared toward the high normal limit (19 mg/dL).
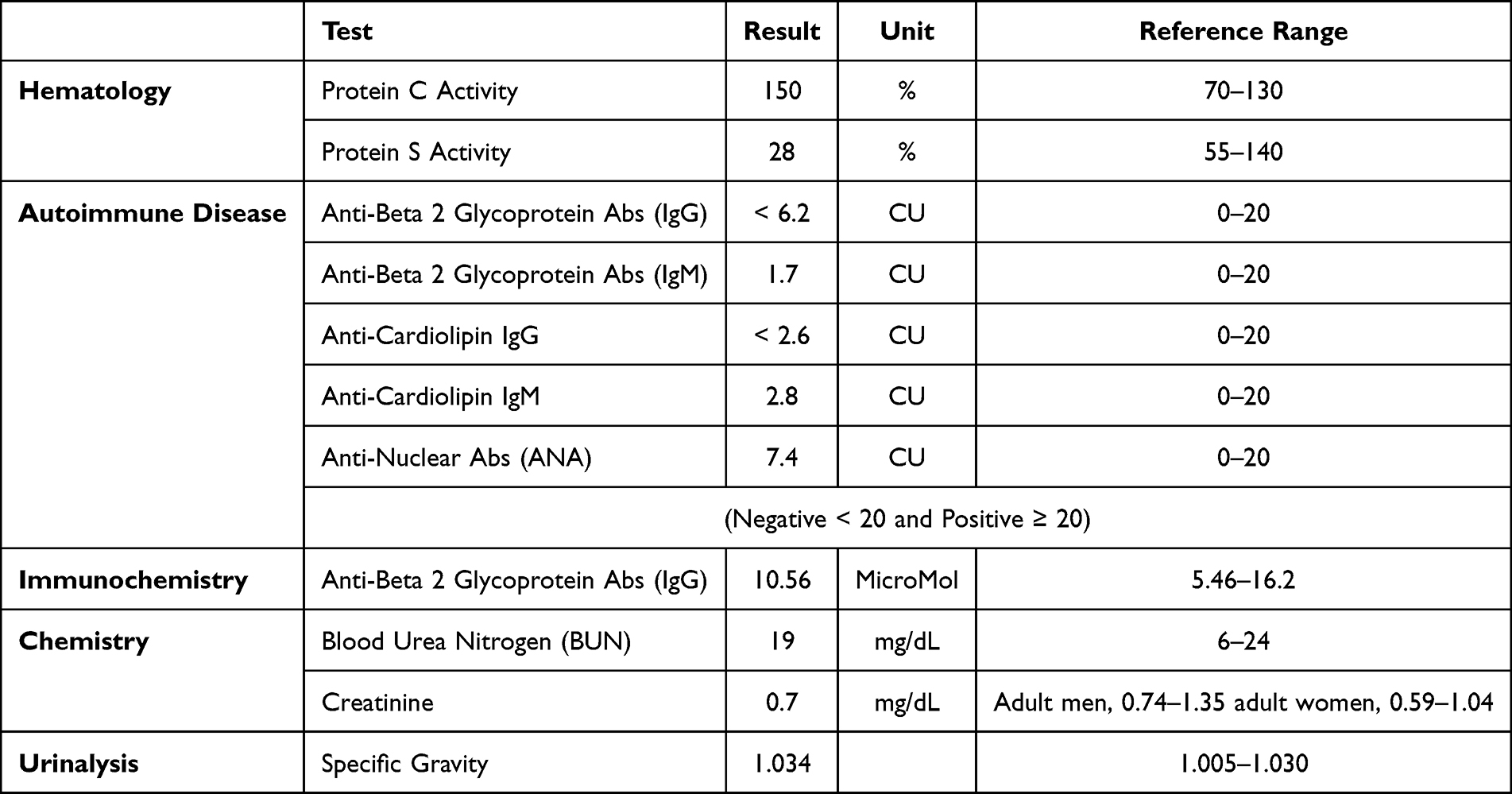 |
Table 1 Laboratory Results of Hematology, Autoimmune Disease, and Immunochemistry |
Radiological and imaging studies, including ultrasound-Doppler/duplex scan, computed tomography angiography (CTA), and echocardiography, were conducted. The ultrasound-Doppler/duplex scan for the left lower limb venous system showed negative augmentation signs and non-compressibility of the deep venous system with partial occlusion/echogenic thrombosis extending from the external iliac vein (EIV), saphenofemoral junction (SFJ), superficial femoral vein (SFV), popliteal vein (PV), anterior tibial vein (ATV), and posterior tibial artery (PTA) vena comitans (Figures 1–3). Tender probing of the left calf was observed, a finding consistent with acute extensive DVT. The right lower limb venous system showed a normal flow pattern of the superficial venous system with no echogenic thrombi. The chest CTA was negative for pulmonary emboli. Likewise, echocardiography showed normal right and left atrial and ventricular findings, with no wall motion abnormality or sign of pulmonary hypertension, indicating no evidence of left ventricular thrombus.
 |
Figure 1 Ultrasound on presentation demonstrating acute deep venous thrombosis (DVT) of the left external iliac vein. |
 |
Figure 2 Ultrasound on presentation demonstrating acute deep venous thrombosis (DVT) of the saphenofemoral junction. |
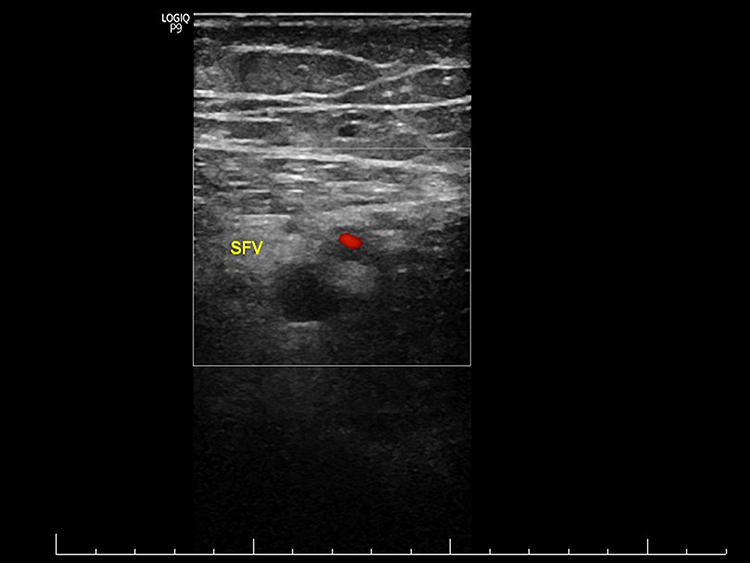 |
Figure 3 Ultrasound on presentation demonstrating acute deep venous thrombosis (DVT) of the superficial femoral vein. |
After administering the initial and appropriate standard of care for such cases, including, but not limited to, history, physical examination, and obtainment of the necessary laboratory and radiology tests, the findings from the examination revealed significant left lower extremity pain, weakness, and swelling with temperature changes. These findings jointly indicated acute DVT. Patient care (medical treatment plan/therapeutic anticoagulation) was started in the ED and continued in the Critical Care Unit for close monitoring and care for a couple of days, after which he was transferred to the ward and then discharged in stable condition. He was prescribed a three-month course of appropriate medication regimen. Patient was treated with injectable anticoagulants Enoxaparine 1 mg/ kg twice a day as suggested standard therapeutic dose.
Discussion
The case describes a middle-aged male with an extensive left leg DVT. Notably, this case report highlights the importance of conducting a thorough differential diagnosis associated with gastroenteritis-induced dehydration. Severe or frequent diarrhea can lead to dehydration, which comes with its own health concerns. Dehydration generally causes BUN levels to rise more than the creatinine levels, which causes a high BUN-to-creatinine ratio. In the present study, a high BUN-to-creatinine ratio was observed. The urine specific gravity test indicated a substantial loss of fluid due to excessive diarrhea. Measuring blood and/or urine osmolality would have strengthened the role of dehydration as a risk factor in such cases. In addition, the patient was probably less mobile than usual due to the acute gastroenteritis, in which immobility as a risk factor for thrombosis should also be considered.
Although international guidelines have highlighted dehydration as a risk factor for the development of thrombosis,14,15 but possibly insufficient evidence to form a strong association from clinical studies to support this.13 Dehydration as a significant risk factor for the development of DVTs has been mainly studied in relation to air flights,17 bariatric surgeries,18 and ischemic strokes.13 Additionally, in pediatric cerebral thrombosis, dehydration has been found to be a major contributing factor.19 The effect of dehydration on the coagulation system was evaluated in a mouse model, showing a significant increase in the tendency to form clots in the dehydration state.20 In a single rare case report, a 32-year-old male who presented to the ED with a three-day history of persistent vomiting and watery diarrhea was diagnosed with CVT, in which dehydration secondary to gastroenteritis was considered the predisposing factor.21 In addition, in pediatric patients, gastroenteritis and dehydration have been reported as direct causes of CVT.16 Moreover, several studies have investigated the seasonal variation in the incidence of DVTs.22 A study suggested dehydration as a potential explanation for the month-related variation in the incidence of DVTs.23 The study found a significant monthly variation in the BUN-to-creatinine ratio. Patients in the provoked VTE group had higher levels of BUN and lower levels of HCT compared with the unprovoked VTE group.23
DVT is a potentially life-threatening disease, and making an accurate diagnosis of DVT is difficult; in fact, research has shown that clinical signs and symptoms alone are unreliable in making a diagnosis.7,8 Although uncommon, gastroenteritis-induced dehydration might be a risk factor for DVT in adults. Therefore, physicians must rely on prudent consideration and identification of the risk factors for DVT.
Conclusion
The implication of the case report is valuable. Most physicians only take dehydration more seriously in the pediatric population. However, this study showed that even moderate dehydration in adults could result in life-threatening conditions. We learned from the present case that dehydration secondary to acute gastroenteritis might cause DVT in adult patients. Therefore, all patients, regardless of age, diagnosis or comorbidities, should always be risk assessed upon presentation and discharge, and prophylaxis should be provided according to their risk profile. Dehydration and immobility are risk factors that should be considered as per evidence-based guidelines.
Ethical Statement
No institutional approval was required to publish the case details. The patient has provided consent to publish the case report and accompanying images.
Consent to Publish
The author affirms that patient provided informed consent for publication of the images in Figures 1–3. The patient has consented to the submission of the case report to the journal. Patients signed informed consent regarding publishing their data.
Funding
The author received no financial support for the research authorship and publication of this article.
Disclosure
The author declares that there is no conflict of interest.
References
1. Riddle DL, Hillner BE, Wells PS, Johnson RE, Hoffman HJ, Zuelzer WA. Diagnosis of lower-extremity deep vein thrombosis in outpatients with musculoskeletal disorders: a national survey study of physical therapists. Phys Ther. 2004;84(8):717–728. doi:10.1093/ptj/84.8.717
2. Stein PD, Matta F, Dalen JE. Is the campaign to prevent VTE in hospitalized patients working? Chest. 2011;139(6):1317–1321. doi:10.1378/chest.10-1622
3. Janku GV, Paiement GD, Green HD. Prevention of venous thromboembolism in orthopaedics in the United States. Clin Orthop Relat Res. 1996;325(325):313–321. doi:10.1097/00003086-199604000-00038
4. Jang MJ, Bang SM, Oh D. Incidence of venous thromboembolism in Korea: from the health insurance review and assessment service database. J Thromb Haemost. 2011;9(1):85–91. doi:10.1111/j.1538-7836.2010.04108.x
5. Nordström M, Lindblad B, Bergqvist D, Kjellström T. A prospective study of the incidence of deep-vein thrombosis within a defined urban population. J Intern Med. 1992;232(2):155–160. doi:10.1111/j.1365-2796.1992.tb00565.x
6. Tapson VF. Acute pulmonary embolism. N Engl J Med. 2008;358(10):1037–1052. doi:10.1056/NEJMra072753
7. Wells PS. Integrated strategies for the diagnosis of venous thromboembolism. J Thromb Haemost. 2007;5(Suppl 1):41–50. doi:10.1111/j.1538-7836.2007.02493.x
8. Akman MN, Cetin N, Bayramoglu M, Isiklar I, Kilinc S. Value of the D-dimer test in diagnosing deep vein thrombosis in rehabilitation inpatients. Arch Phys Med Rehabil. 2004;85(7):1091–1094. doi:10.1016/j.apmr.2003.10.023
9. Hannon J, Garrison C, Conway J. Residents case report: deep vein thrombosis in a high school baseball pitcher following ulnar collateral ligament (ucl) reconstruction. Int J Sports Phys Ther. 2013;8(4):472–481.
10. Horsburgh J. Case report of a deep vein thrombosis in the femoral vein, an atypical presentation. J Clin Chiropr. 2004;7(3):120–126. doi:10.1016/j.clch.2004.02.004
11. McLendon K, Goyal A, Attia M. Deep Venous Thrombosis Risk Factors. Treasure Island (FL): StatPearls Publishing; 2022.
12. Anderson FA
13. Kelly J, Hunt BJ, Lewis RR, et al. Dehydration and venous thromboembolism after acute stroke. QJM. 2004;97(5):293–296. doi:10.1093/qjmed/hch050
14. Rahman ARA, Sathar J, Chee CC, et al. Clinical Practice Guidelines Prevention and Treatment of Venous Thromboembolism. Malaysia MoH, ed. Malaysia: Ministry of Health Malaysia; 2013.
15. Watson HG, Baglin TP. Guidelines on travel-related venous thrombosis. Br J Haematol. 2011;152(1):31–34. doi:10.1111/j.1365-2141.2010.08408.x
16. Carvalho KS, Bodensteiner JB, Connolly PJ, Garg BP. Cerebral venous thrombosis in children. J Child Neurol. 2001;16(8):574–580. doi:10.1177/088307380101600807
17. Gavish I, Brenner B. Air travel and the risk of thromboembolism. Intern Emerg Med. 2011;6(2):113–116. doi:10.1007/s11739-010-0474-6
18. Gonzalez-Sánchez JA, Corujo-Vázquez O, Sahai-Hernández M. Bariatric surgery patients: reasons to visit emergency department after surgery. Bol Asoc Med P R. 2007;99(4):279–283.
19. Jackson BF, Porcher FK, Zapton DT, Losek JD. Cerebral sinovenous thrombosis in children: diagnosis and treatment. Pediatr Emerg Care. 2011;27(9):874–880; quiz 881–873. doi:10.1097/PEC.0b013e31822c9ccc
20. Tanira MO, El-Sabban FF, Fahim MA, Wasfi IA. Acetyl salicylic acid alleviates increased susceptibility to thrombosis in pial microvessels of dehydrated mice. J Vet Med Sci. 1994;56(2):245–248. doi:10.1292/jvms.56.245
21. Kuo E-Y, Chung M-H, Lin H-J, Chen K-T. Gastroenteritis followed by headache: a rare presentation of cerebral venous thrombosis. J Acute Med. 2012;2(3):92–94. doi:10.1016/j.jacme.2012.08.001
22. Dentali F, Ageno W, Rancan E, et al. Seasonal and monthly variability in the incidence of venous thromboembolism. A systematic review and a meta-analysis of the literature. Thromb Haemost. 2011;106(3):439–447. doi:10.1160/TH11-02-0116
23. Elias S, Hoffman R, Saharov G, Brenner B, Nadir Y. Dehydration as a possible cause of monthly variation in the incidence of venous thromboembolism. Clin Appl Thromb Hemost. 2016;22(6):569–574. doi:10.1177/1076029616649435
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.