Back to Journals » Infection and Drug Resistance » Volume 19
Extended vs Intermittent Infusion of Meropenem with Colistimethate Sodium and Risk of Acute Kidney Injury in Critically Ill Patients: A Propensity Score-Matched Retrospective Cohort Study
Received 7 January 2026
Accepted for publication 6 April 2026
Published 29 May 2026 Volume 2026:19 594482
DOI https://doi.org/10.2147/IDR.S594482
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Qiaoqiao Hu,1 Huajun Wang2
1Department of Pharmacy, The Affiliated People’s Hospital of Ningbo University, Ningbo City, Zhejiang Province, 315000, People’s Republic of China; 2Department of Intensive Care Unit, The Affiliated People’s Hospital of Ningbo University, Ningbo City, Zhejiang Province, 315000, People’s Republic of China
Correspondence: Qiaoqiao Hu, Department of Pharmacy, The Affiliated People’s Hospital of Ningbo University, No. 791, Jiangning Road, Zhonggongmiao Street, Yinzhou District, Ningbo City, Zhejiang Province, 315000, People’s Republic of China, Email [email protected]
Purpose: The objective of this study was to evaluate whether an extended-infusion strategy for meropenem is associated with a reduced incidence and severity of acute kidney injury in critically ill patients receiving combination therapy with colistimethate sodium for carbapenem-resistant gram-negative infections. While extended infusion is known to optimize pharmacokinetic/pharmacodynamic targets, its potential as a kidney-sparing intervention remains to be elucidated.
Patients and methods: A single-center, retrospective cohort study was conducted in the intensive care unit between January 2021 and October 2025. Critically ill adults receiving combination therapy with colistimethate sodium and meropenem for at least 72 hours were included. Patients were stratified into prolonged infusion (at least 3 hours per dose) and intermittent infusion (less than 1 hour per dose) groups. Propensity score matching (1:1) was performed to balance baseline characteristics. To account for the variable duration of therapy and the competing risk of mortality, data were analyzed using the Fine-Gray proportional subdistribution hazards model. The primary outcome was the incidence of acute kidney injury according to the Kidney Disease: Improving Global Outcomes criteria. Secondary outcomes included severity of injury, requirement for renal replacement therapy, and in-hospital mortality.
Results: After matching, 146 pairs (292 patients) were analyzed. The prolonged infusion group exhibited a significantly lower incidence of acute kidney injury than the intermittent infusion group (24.7% versus 39.7%, p=0.006). Severe acute kidney injury (stage 2 or 3) was also less frequent in the prolonged infusion group (9.6% versus 19.2%, p=0.019). In-hospital mortality (19.2% versus 28.1%, p=0.021) and renal replacement therapy requirements (5.5% versus 12.3%, p=0.034) were significantly lower with prolonged infusion. Multivariate Fine-Gray analysis confirmed that prolonged infusion was an independent protective factor against acute kidney injury (adjusted subdistribution hazard ratio 0.55, 95% confidence interval 0.35– 0.86, p=0.009).
Conclusion: Extended infusion of meropenem is independently associated with a reduced incidence and severity of acute kidney injury in critically ill patients receiving colistimethate sodium. This dosing strategy may also lower mortality and the need for renal replacement therapy. While these observational findings require validation in prospective trials, they support the consideration of extended infusion as a potential kidney-sparing intervention in this high-risk population.
Plain Language Summary: Why was the study done? Critically ill patients in the intensive care unit often receive a combination of two powerful antibiotics, colistimethate sodium and meropenem, to treat severe infections. While effective, colistimethate sodium frequently causes acute kidney injury, which is a sudden and serious form of kidney damage. We conducted this study to determine whether changing the way doctors administer meropenem—using a slow, three-hour “extended infusion” instead of a standard quick drip—could reduce the risk of kidney damage in these patients.
What did the researchers do and find? We analyzed 292 patients who received both antibiotics for at least three days between 2021 and 2025. We compared those who received slow infusions of meropenem to those who received quick infusions, ensuring that both groups had similar health characteristics to make the comparison fair. We found that patients in the slow-infusion group had a significantly lower rate of kidney injury (24.7% compared to 39.7% in the quick-infusion group). Furthermore, patients receiving the slow infusion were less likely to die during their hospital stay or require dialysis.
What do these results mean? Administering meropenem as a slow drip appears to be a simple, no-cost change that may help improve the safety profile of this antibiotic combination for critically ill patients. Our observational data showed that this approach is associated with a significantly lower chance of severe kidney damage and potentially better overall survival. We suggest that hospitals could consider slow infusion as a potential protective strategy when treating high-risk patients with these two drugs, although further prospective research is needed to definitively confirm these benefits.
Keywords: acute kidney injury, colistimethate sodium, meropenem, extended infusion, critical care
Introduction
Infections caused by carbapenem-resistant gram-negative bacteria (CR-GNB) have emerged as a formidable challenge in critical care settings worldwide. These infections are associated with high rates of morbidity and mortality and severely limit effective therapeutic options.1 In response to this growing threat of resistance, polymyxin antibiotics, particularly colistimethate sodium (CMS), have re-entered the clinical arena as a last-line therapy for CR-GNB infections. In clinical practice, CMS is frequently used in combination with a carbapenem such as meropenem, with the goal of achieving synergistic antimicrobial activity and potentially delaying the development of further resistance.2
Acute kidney injury (AKI) is a pervasive complication in the intensive care unit; the multinational AKI-EPI study demonstrated an overall magnitude affecting over 50% of all critically ill patients, significantly contributing to adverse outcomes.3 Against this inherently high-risk baseline, the widespread use of CMS is further constrained by its profound intrinsic nephrotoxicity. Studies have reported that the incidence of AKI among patients treated with CMS can range from 25% to as high as 45%, a serious adverse event that represents a key barrier to its clinical utility.4,5 Clinicians are consequently forced to make difficult trade-offs between ensuring therapeutic efficacy and mitigating the substantial risk of renal damage. To optimize this balance, various strategies within combination therapy regimens are being explored to enhance efficacy while reducing toxic side effects.
Within these combination regimens, the administration method of meropenem has become a focus for optimizing pharmacokinetic/pharmacodynamic (PK/PD) parameters to improve treatment outcomes. As a time-dependent antibiotic, the efficacy of meropenem is determined by the duration for which the drug concentration remains above the minimum inhibitory concentration (MIC) of the pathogen (%T>MIC).6 Consequently, compared to traditional intermittent infusions, an extended-infusion strategy is recognized for its ability to more effectively optimize %T>MIC, thereby potentially improving clinical efficacy. This modification has primarily been investigated as a means to enhance the bactericidal activity of the drug.
While some studies have investigated the overall safety of combination therapy with CMS and meropenem,7,8 there is a scarcity of research focused on whether the administration method of meropenem itself, extended versus intermittent infusion, can modulate the nephrotoxicity associated with CMS. This gap in the literature limits a comprehensive understanding of how dosing strategies can be optimized to minimize the toxicity of combination regimens. Therefore, investigating the impact of different meropenem infusion methods on the incidence of CMS-associated AKI is of significant clinical and scientific importance.
This study aims to determine whether an extended-infusion strategy for meropenem is independently associated with a reduced incidence of acute kidney injury in critically ill patients receiving combination therapy with colistimethate sodium. We hypothesized that, compared to intermittent infusion, administering meropenem via extended infusion might mitigate the nephrotoxicity of CMS, thereby providing new clinical evidence to optimize combination therapy for severe CR-GNB infections.
Methods
Study Design
This single-center, retrospective cohort study was conducted in the Intensive Care Unit (ICU) of Ningbo University Affiliated People’s Hospital. The study utilized anonymized data from electronic medical records (EMR) to investigate the impact of prolonged infusion versus intermittent infusion of meropenem, in combination with CMS, on the incidence of AKI in critically ill patients. Data for all eligible patients admitted between January 1, 2021, and October 31, 2025, were reviewed. The study protocol was reviewed and approved by the Hospital’s Institutional Review Board, which granted a waiver of informed consent due to the retrospective, observational, and anonymized nature of the research. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All patient data were handled with strict confidentiality and in compliance with institutional data protection policies.
Study Population
Patients were included if they met all the following criteria: (1) age ≥ 18 years; (2) admission to the ICU; (3) receipt of combined intravenous therapy with colistimethate sodium and meropenem for a minimum duration of 72 hours for the treatment of documented or suspected severe infections caused by carbapenem-resistant gram-negative organisms;9 (4) normal or near-normal baseline renal function, defined as an estimated glomerular filtration rate (eGFR) > 60 mL/min/1.73 m2 prior to the initiation of combination therapy;10 and (5) availability of a complete electronic medical record for data extraction. The key exclusion criteria were as follows: (1) preexisting AKI at the start of combination therapy, as defined by the KDIGO 2012 criteria;11 (2) a diagnosis of end-stage renal disease (ESRD) or chronic dependence on renal replacement therapy (RRT); (3) pregnancy or lactation; (4) administration of other concomitant, potentially nephrotoxic antimicrobials (eg., vancomycin, aminoglycosides) that were not grounds for exclusion but were meticulously recorded for adjustment in the analysis; and (5) absence of key data, specifically daily serum creatinine values or precise records of meropenem infusion duration. A total of 632 patients were initially screened; after applying the inclusion and exclusion criteria, 188 patients were excluded (85 for preexisting AKI/ESRD, 48 for therapy < 72 h, 32 for missing data, and 23 for other reasons), leaving 444 patients for propensity score analysis.
Patient Grouping and Sample Size Calculation
Patients who met the eligibility criteria were divided into two distinct groups based on the administration modality of meropenem. It is crucial to note that the choice between extended and intermittent infusion was not randomized but driven by specific clinical indications, introducing a potential source of treatment selection bias. In our institutional clinical practice, intermittent infusion (typically administered over 30 minutes) generally serves as the standard empirical administration method. Conversely, extended infusion is explicitly indicated and preferentially selected by intensive care physicians as an optimized PK/PD therapeutic strategy for patients presenting with higher baseline disease severity, septic shock, or severe infections highly suspected to be caused by pathogens with elevated minimum inhibitory concentrations (MICs), such as CR-GNB.12 Because patients receiving extended infusions were inherently sicker or at higher risk of treatment failure at baseline, this indication-by-treatment bias necessitated the rigorous use of propensity score matching (PSM) in our subsequent analysis to balance these baseline disparities.
The prolonged infusion group included patients for whom the EMR documented a meropenem infusion duration of three hours or more for a single dose. This duration is consistent with definitions used in previous studies to optimize the time-dependent bactericidal activity of β-lactam antibiotics, aiming to maximize the period during which drug concentrations remain above the MIC of the pathogen.13 The intermittent infusion group consisted of patients who received meropenem via a standard short-term infusion, documented in the EMR as lasting less than one hour.
The sample size was calculated a priori to ensure sufficient statistical power to detect a clinically meaningful difference in the primary outcome of AKI incidence between the two groups. Based on the available literature, the incidence of AKI in critically ill patients receiving intermittent infusions of nephrotoxic antibiotics, such as polymyxins, varies significantly. For instance, a retrospective study comparing polymyxin B infusion strategies reported an AKI incidence of 41% in the intermittent infusion arm.14 Another study involving critically ill patients receiving vancomycin combined with intermittent meropenem infusion observed an AKI rate of 23.5%.15 Given that the current study investigates a combination regimen including colistimethate sodium, a conservative baseline AKI incidence of 40% was conservatively estimated for the intermittent infusion (control) group. We hypothesized that a prolonged infusion strategy could lead to a clinically significant absolute risk reduction of 15%. To detect a reduction of this magnitude (ie., from 40% to 25%), with a statistical power (1-β) of 80% and a two-sided significance level (α) of 0.05, a minimum of 132 patients per group would be needed. To account for potential data attrition and to ensure adequate statistical power in the postmatching analysis, we aimed to enroll a larger sample.
Data Collection and Quality Control
A standardized protocol was established for the retrospective extraction of patient data from the Hospital Information System (HIS) and the EMR database. The two authors independently performed the data extraction from the electronic medical records using a predefined electronic case report form (eCRF). Any discrepancies were resolved through direct consensus between the authors to ensure data accuracy and consistency.
A comprehensive set of variables was collected to account for potential confounders. Baseline and clinical characteristics included (1) demographic information (age, sex, body weight); (2) primary diagnosis upon ICU admission and comorbidities, quantified using the Charlson Comorbidity Index;16 (3) severity of illness scores (Acute Physiology and Chronic Health Evaluation II [APACHE II] and Sequential Organ Failure Assessment [SOFA]) calculated from the most abnormal values within the first 24 hours of ICU stay;17,18 (4) infection-related data (primary site and the presence of sepsis or septic shock as defined by the Sepsis-3 criteria); (5) baseline liver function indicators; and (6) requirements for organ support (mechanical ventilation, vasopressor therapy).
Treatment-related data were recorded for the entire duration of the combination therapy. This included the daily and total cumulative doses of both colistimethate sodium (CMS, expressed in milligrams of colistin base activity [CBA]) and meropenem, the total therapy duration, and the precise infusion time for each meropenem dose. We systematically documented the concomitant use of other potential nephrotoxic agents (eg., vancomycin, aminoglycosides, intravenous contrast media, loop diuretics, and vasopressors) administered within 72 hours before or during the index therapy, recording the agent type, dose, and duration of exposure.
Laboratory data and outcome definition: Serum creatinine (SCr) was collected at baseline (the last value within 24 hours before initiating meropenem therapy for CMS) and daily thereafter. The estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation.19 The primary outcome, AKI, was defined and staged according to the 2012 KDIGO clinical practice guidelines based on changes in SCr from baseline.11
Quality control measures were rigorously implemented. To ensure interrater reliability, at least 10% of patient records were randomly selected for independent double data extraction by both researchers; a Cohen’s kappa coefficient of >0.80 was considered indicative of substantial agreement. For inclusion in the final analysis, completeness of data for the primary outcome and key exposures (daily SCr and meropenem infusion duration) was mandatory. For missing values in other, less critical baseline covariates, multiple imputation techniques were planned.
Outcome Measures
The primary outcome was the incidence of AKI during combined therapy with colistimethate sodium and meropenem, including its severity distribution according to the KDIGO stage. AKI was diagnosed and staged based on the serum creatinine criteria of the 2012 KDIGO clinical practice guideline.11 Stage 1 was defined as an increase in serum creatinine by ≥26.5 μmol/L within 48 hours or to 1.5–1.9 times the baseline value; Stage 2 as an increase to 2.0–2.9 times baseline; and Stage 3 as an increase to ≥3.0 times baseline, an absolute serum creatinine level of ≥353.6 μmol/L, or the initiation of renal replacement therapy (RRT). The baseline serum creatinine was defined as the most recent value measured within 24 hours before starting the combination therapy. The observation period for AKI onset extended from the initiation of therapy until 72 hours after discontinuation or until ICU discharge, whichever occurred first.
Secondary outcomes were evaluated to provide a comprehensive assessment of other clinical and renal endpoints. These included (1) the proportion of patients requiring RRT during the ICU stay after initiation of the study antibiotics; (2) ICU length of stay, calculated in days from admission to discharge; (3) in-hospital all-cause mortality, defined as death from any cause during the index hospital admission in which the combination therapy was administered; and (4) renal function recovery among patients who developed AKI. Recovery was defined according to the Acute Disease Quality Initiative (ADQI) consensus criteria as a return of serum creatinine to within 1.5 times the baseline value at the time of therapy cessation or ICU discharge.20
Statistical Analysis
All statistical analyses were performed using SPSS (version 26.0; IBM Corp.) for basic descriptive statistics and initial database management and R software (version 4.2.1; R Foundation for Statistical Computing) specifically for executing propensity score matching algorithms, survival analysis, and generating complex individual trajectory graphical plots. Prior to selecting the appropriate comparative tests, the normality of all continuous variables was formally evaluated using the Shapiro‒Wilk test. Consequently, normally distributed continuous variables are presented as the mean ± standard deviation and were compared using the independent Student’s t test, whereas nonnormally distributed continuous variables are presented as the median with interquartile range and were compared using the Mann‒Whitney U-test. Categorical variables are presented as numbers (percentages) and were compared using the chi-square test or Fisher’s exact test, as appropriate. To minimize confounding bias, a propensity score was estimated for each patient using a multivariable logistic regression model that included all baseline variables with a p‑value <0.1 in univariate analysis and clinically relevant covariates (eg., age, APACHE II score, concomitant nephrotoxins). A 1:1 nearest‑neighbor matching algorithm with a caliper width of 0.2 of the standard deviation of the logit of the propensity score was employed to create well‑balanced cohorts. After matching, between‑group balance was assessed using standardized mean differences (SMD), with an SMD <0.1 indicating adequate balance. Within the matched cohort, continuous variables were compared using paired t‑tests or Wilcoxon signed‑rank tests, and categorical variables were compared using McNemar’s test. To rigorously address the inherently variable durations of the combination antibiotic therapy (right-censoring) and the potential for mortality to preclude the occurrence of kidney damage, AKI was treated as a time-to-event endpoint subject to competing risks. The cumulative incidence function (CIF) was used to estimate the probability of AKI over time, accounting for the competing risk of in-hospital death, and group differences were evaluated using Gray’s test. The independent association between the meropenem infusion strategy (prolonged vs intermittent) and the risk of AKI was quantified using a Fine-Gray proportional subdistribution hazards model, with results expressed as subdistribution hazard ratios (sHR) and 95% confidence intervals (CI). To explore effect heterogeneity, prespecified subgroup analyses were conducted within the matched cohort based on disease severity (APACHE II score ≥20 vs <20), presence of sepsis/septic shock, concomitant vancomycin use, and infection status (microbiologically proven susceptible CR-GNB vs suspected infection); interaction terms were tested. A sensitivity analysis was performed by applying the identical Fine-Gray multivariable competing-risks model adjusted for all important covariates to the entire pre-matched cohort. All tests were two‑sided, and a p‑value <0.05 was considered statistically significant.
Results
Patient Screening and Baseline Characteristics
A total of 292 well-matched critically ill patients (146 pairs) were included in the final analysis. The study population had a mean age of 64.3 ± 12.3 years, with a male predominance (66.1%) (Figure 1). The overall cohort exhibited high disease severity, as reflected by a mean APACHE II score of 22.7 ± 6.6 and a SOFA score of 8.8 ± 3.4. Septic shock was present in 56.2% of the patients at baseline, and a substantial majority required mechanical ventilation (81.8%) and vasopressor support (67.1%). Following propensity score matching, there were no significant differences between the prolonged infusion and intermittent infusion groups across all sociodemographic and clinical baseline characteristics (all SMD < 0.10, as detailed in Table 1), providing a balanced cohort to evaluate the impact of the meropenem infusion strategy on renal outcomes.
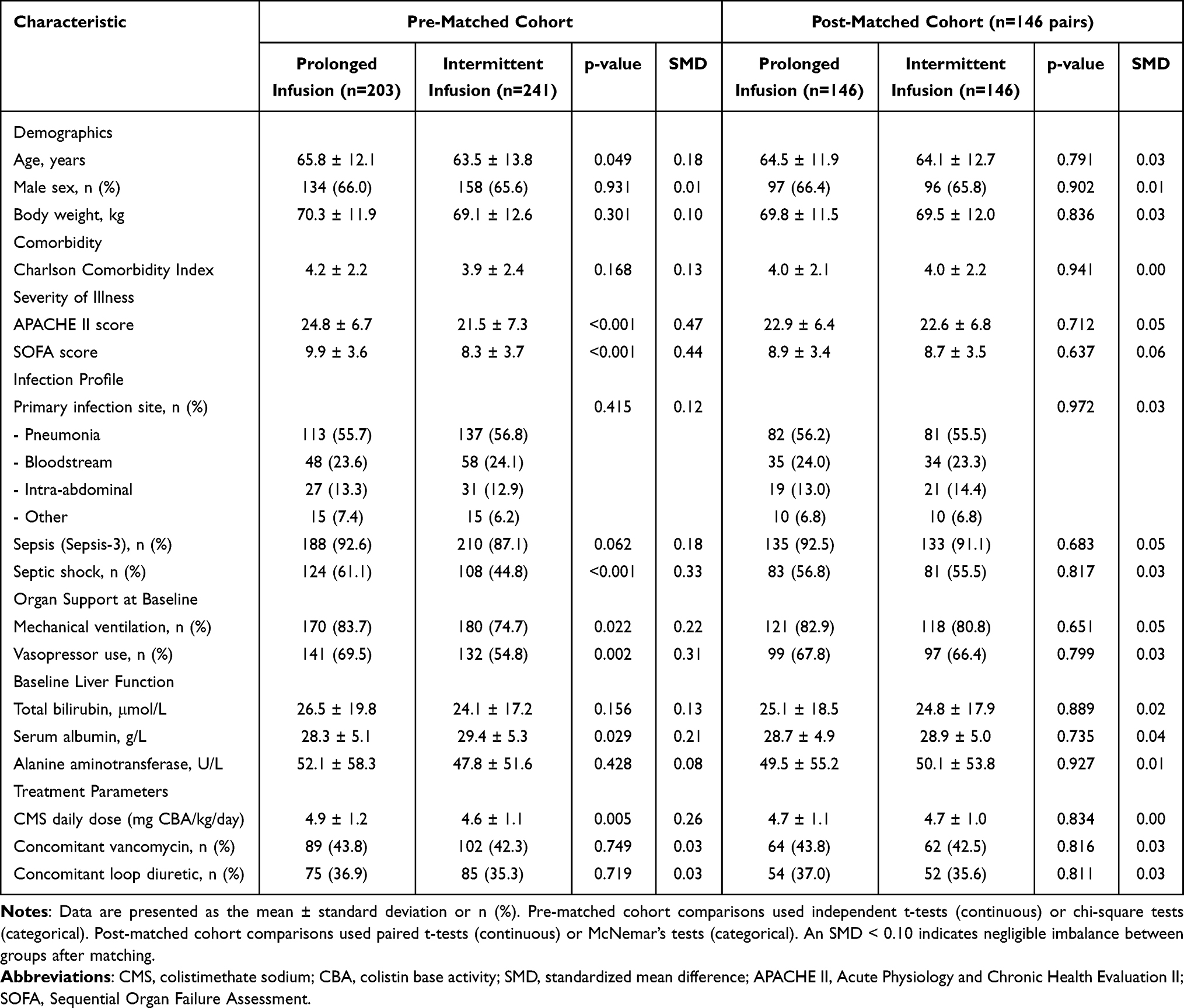 |
Table 1 Baseline and Clinical Characteristics of Patients Before and After Propensity Score Matching |
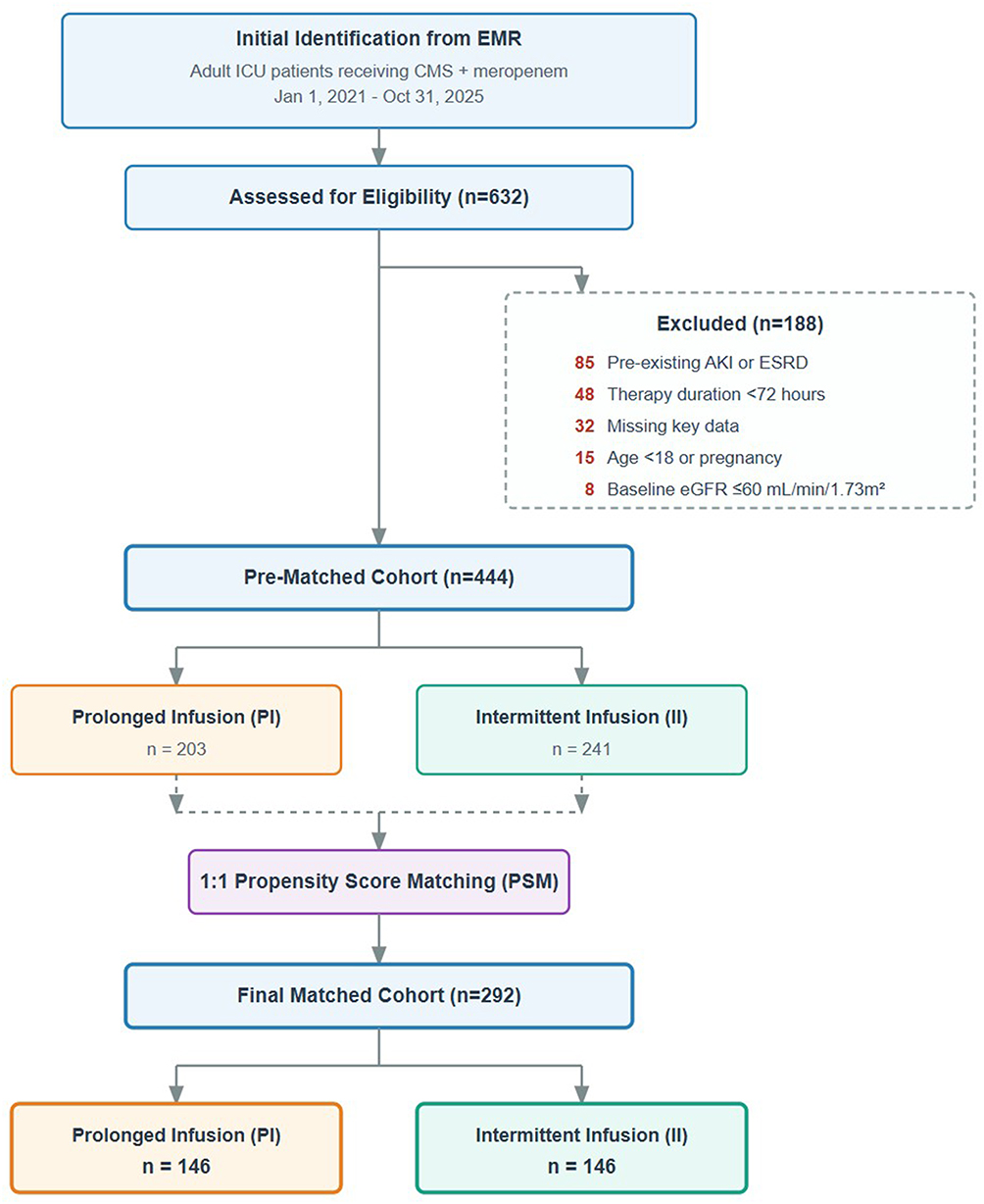 |
Figure 1 Flowchart of patient screening, eligibility assessment, and final cohort formation. Abbreviations: EMR, electronic medical record; ICU, intensive care unit; CMS, colistimethate sodium; AKI, acute kidney injury; ESRD, end-stage renal disease; eGFR, estimated glomerular filtration rate; PI, prolonged infusion; II, intermittent infusion; PSM, propensity score matching. |
Primary Outcome: Incidence of Acute Kidney Injury
In the PSM cohort of 292 patients, the overall incidence of AKI during the observation period was 32.2% (94/292). The time-to-event analysis, depicted by the CIF curves in Figure 2, revealed a significant divergence in AKI risk between the groups, accounting for the competing risk of death (Gray’s test p = 0.002). The median time to AKI onset was 4.7 days (IQR 3–8) in the intermittent infusion group and 6.1 days (IQR 4–10) in the prolonged infusion group among patients who developed AKI.
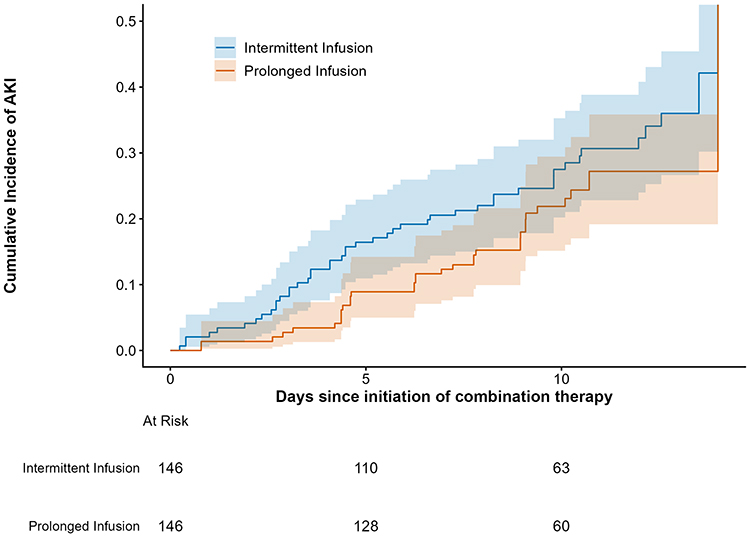 |
Figure 2 Cumulative incidence function (CIF) curves for time to acute kidney injury onset in the matched prolonged infusion and intermittent infusion groups. The curves demonstrate sustained separation throughout the observation period, with the prolonged infusion group maintaining a consistently lower cumulative incidence of AKI, accounting for the competing risk of death (Gray’s test p = 0.002). Shaded areas represent 95% confidence intervals. Abbreviation: AKI, acute kidney injury. |
Table 2 details the comparison of AKI incidence and severity between the matched groups. The incidence of AKI was significantly lower in the prolonged infusion group (24.7%, 36/146) than in the intermittent infusion group (39.7%, 58/146), representing an absolute risk reduction of 15.0% (p = 0.006). This protective effect was consistent across the spectrum of AKI severity. The proportion of patients developing stage 2 or 3 AKI was 9.6% (14/146) in the prolonged infusion group versus 19.2% (28/146) in the intermittent infusion group (p = 0.019).
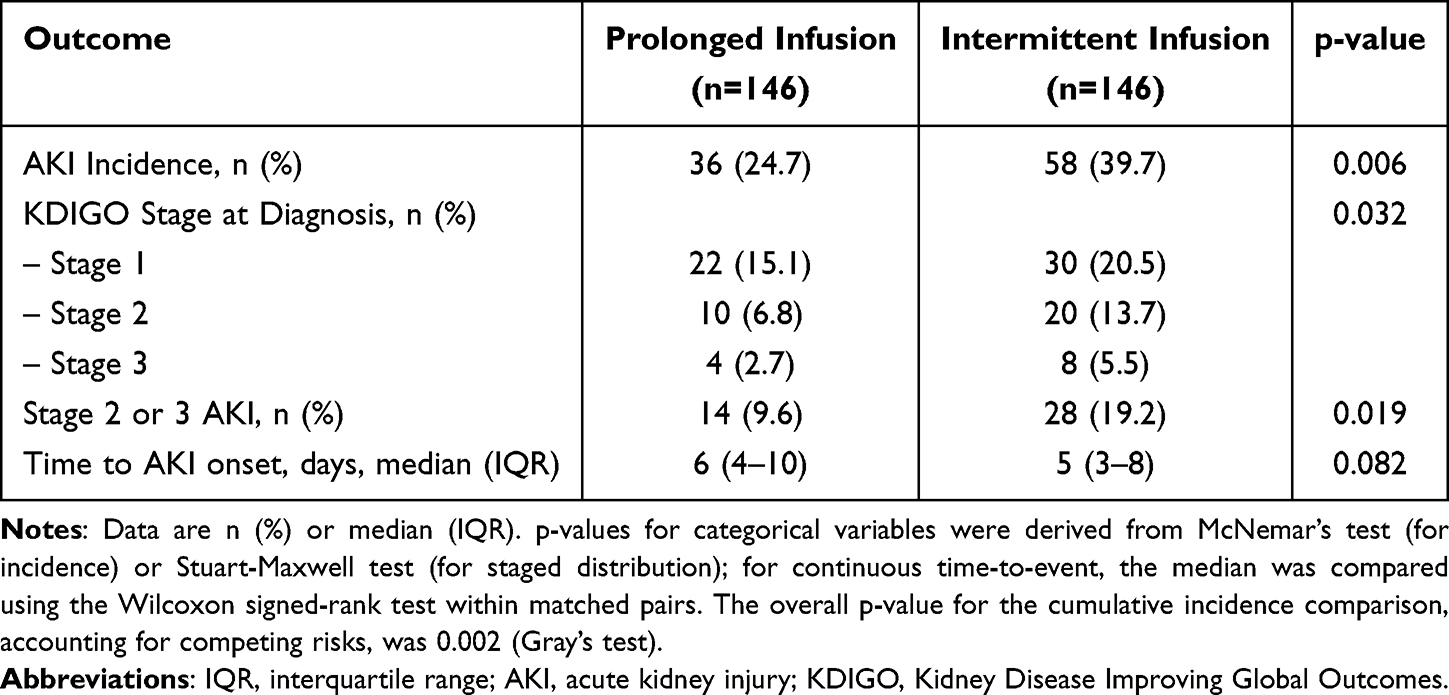 |
Table 2 Incidence and Severity of Acute Kidney Injury in the Matched Cohort |
The Fine-Gray competing-risks regression analysis confirmed that prolonged infusion of meropenem was an independent protective factor against AKI, even when accounting for the competing risk of death. Compared to intermittent infusion, prolonged infusion was associated with a significantly reduced subdistribution hazard of developing AKI (unadjusted sHR 0.58, 95% CI: 0.38–0.88; p = 0.010). After further adjusting for residual imbalances and clinically important covariates within the matched pairs (specifically, baseline serum albumin and concomitant vancomycin use), the association remained robust and significant, with an adjusted sHR of 0.55 (95% CI: 0.35–0.86; p = 0.009).
Secondary Outcomes
Clinical Outcomes
Analysis of clinical outcomes in the matched cohort (n=292) demonstrated differences consistent with the observed reduction in AKI incidence. The in-hospital all-cause mortality was 19.2% (28/146) in the prolonged infusion group and 28.1% (41/146) in the intermittent infusion group (p=0.021). Similarly, the proportion of patients requiring RRT during the ICU stay was significantly lower in the prolonged infusion group (5.5%, 8/146) than in the intermittent infusion group (12.3%, 18/146) (p=0.034). The comparative results are detailed in Table 3.
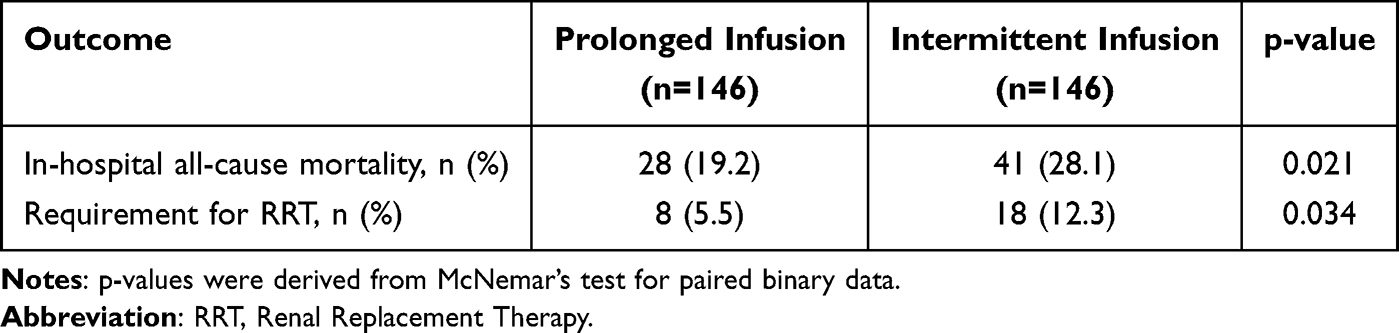 |
Table 3 Comparison of Clinical Outcomes in the Matched Cohort |
Resource Utilization and Renal Recovery
The analysis of resource utilization and renal recovery in the matched cohort yielded the following results. The median ICU length of stay was 15.0 days (interquartile range [IQR]: 9.0–22.0) in the prolonged infusion group and 16.0 days (IQR: 10.0–24.0) in the intermittent infusion group. This difference was not statistically significant (p=0.152). Among the 94 patients who developed AKI (as per Table 2), renal recovery at the end of observation (therapy cessation or ICU discharge) was observed in 23 of 36 patients (63.9%) in the prolonged infusion group and in 35 of 58 patients (60.3%) in the intermittent infusion group. The difference in recovery rates was not statistically significant (p=0.707). These findings are summarized in Table 4.
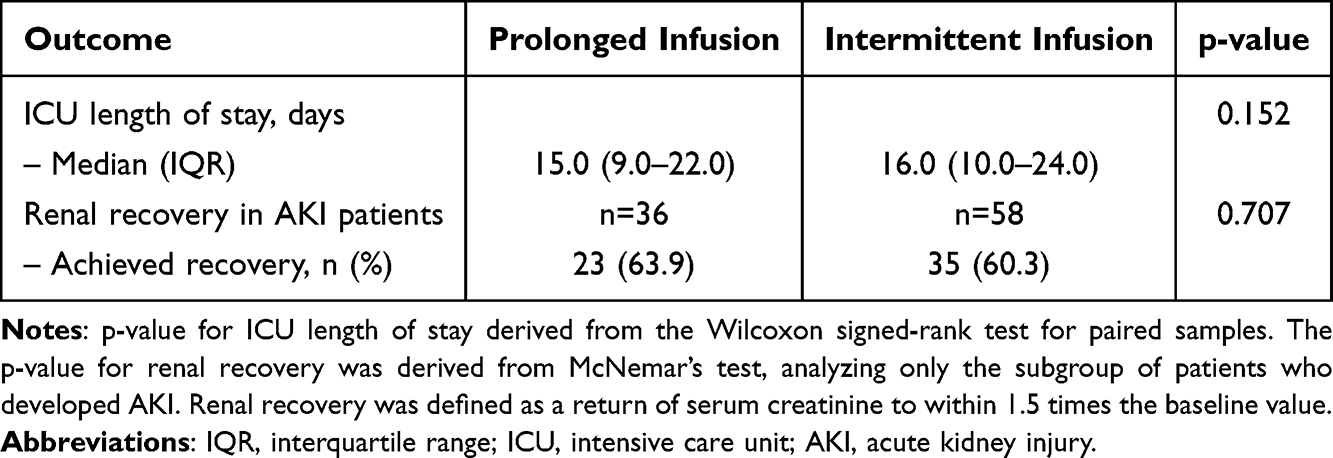 |
Table 4 Resource Utilization and Renal Recovery in the Matched Cohort |
Individual Trajectories of Renal Function
To visualize the dynamic process of renal injury and recovery at the individual level, spaghetti plots of SCr trajectories were constructed for all patients in the matched cohort (n=292). Figure 3 presents the individual SCr values (plotted as a percentage change from baseline) over the 14-day period following the initiation of combination therapy, with separate panels for the prolonged infusion (Figure 3A) and intermittent infusion (Figure 3B) groups. Substantial heterogeneity in individual responses was evident within both groups. However, the aggregated patterns align with the primary findings. In the intermittent infusion group (Figure 3B), a greater number of individual trajectories exhibited sharp, upward deflections exceeding a 50% increase from baseline, indicative of AKI onset. Consequently, the group’s mean trend line, generated using locally estimated scatterplot smoothing (LOESS), remained elevated above that of the prolonged infusion group throughout the observation period. In contrast, the prolonged infusion group (Panel A) demonstrated a cluster of trajectories with less pronounced fluctuation and a more stable overall mean trend, visually corroborating the lower incidence and mitigated severity of AKI observed in the aggregate analysis.
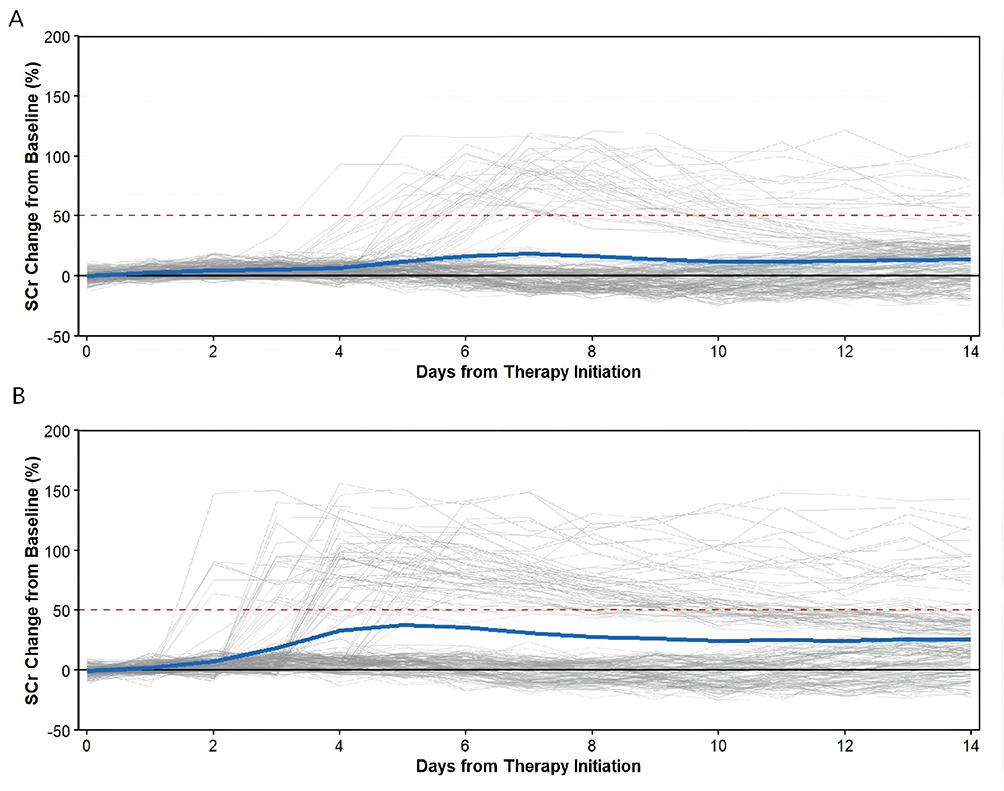 |
Figure 3 Trajectories of renal function according to meropenem infusion strategy. Shown are individual patient trajectories of serum creatinine levels (expressed as percentage change from baseline at therapy initiation) over a 14-day period in the propensity score–matched cohort. (A) shows the prolonged infusion group (n=146), and (B) shows the intermittent infusion group (n=146). Gray lines represent individual patients; the blue line indicates the smoothed group mean (LOESS). The dashed red line marks the threshold for stage 1 acute kidney injury (+50% increase from baseline). The intermittent infusion group had a higher incidence of trajectories exceeding the injury threshold (39.7% vs 24.7%), greater peak elevations (mean, 99.3% vs 86.8%), and earlier injury onset (mean, day 5.5 vs day 7.6). Among patients with acute kidney injury, recovery (defined as a decline to <70% of peak by day 14) occurred in 60.3% of the intermittent infusion group and 63.9% of the prolonged infusion group. Abbreviations: SCr, serum creatinine; LOESS, locally estimated scatterplot smoothing. |
Subgroup Analyses
To investigate the consistency of the treatment effect across clinically relevant patient subsets and to explore potential effect modifiers while accounting for competing risks, prespecified exploratory subgroup analyses were performed within the propensity score-matched cohort (n=292). It is important to note that these analyses were not primarily powered to detect definitive differences and should be interpreted cautiously. Figure 4 presents a forest plot of the subdistribution hazard ratios (sHRs) for AKI associated with prolonged meropenem infusion.
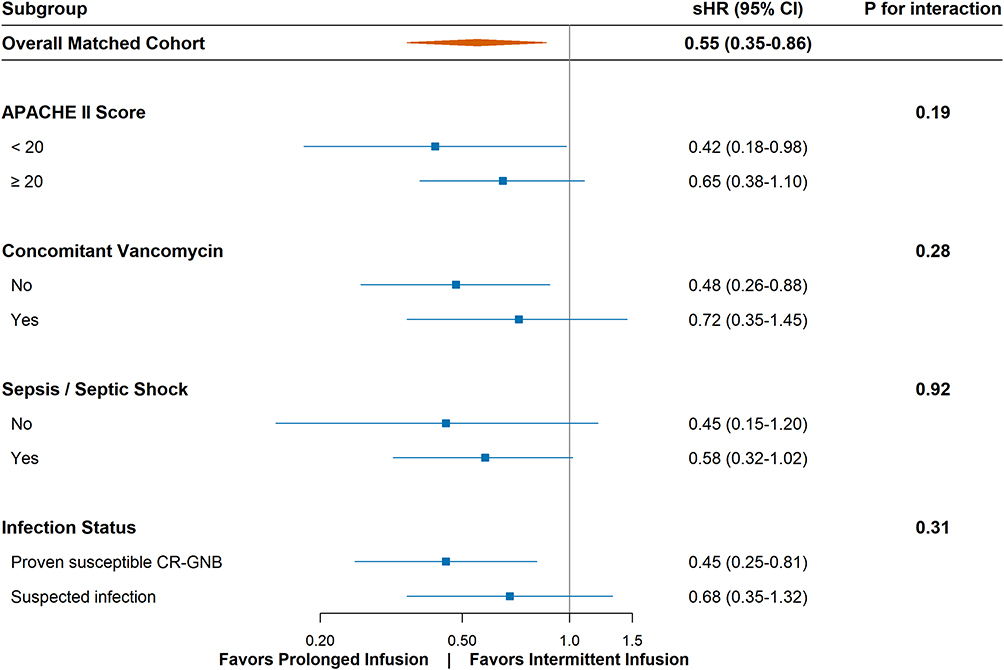 |
Figure 4 Forest plot for subgroup analyses of the association between prolonged meropenem infusion and acute kidney injury risk. Analyses were conducted within the matched cohort (n=292). Subdistribution hazard ratios (sHR) (solid squares) and 95% confidence intervals (horizontal lines) are derived from Fine-Gray competing-risks regression models within each stratum. The size of the square corresponds to the precision of the estimate (inverse of the variance). The dashed vertical line indicates the overall pooled adjusted sHR from the primary matched analysis (sHR=0.55). p-values for interaction were calculated by introducing a cross-product term (infusion strategy × subgroup variable) into the model. Abbreviations: APACHE II, Acute Physiology and Chronic Health Evaluation II; CR-GNB, carbapenem-resistant gram-negative bacteria; CI, confidence interval. |
The protective association between prolonged infusion and reduced AKI risk was consistent across all examined subgroups, with point estimates of the sHRs consistently below 1.0. Particularly noteworthy was the subgroup stratified by infection status. In patients with microbiologically proven, susceptible CR-GNB infections, the protective effect of prolonged infusion was highly pronounced and significant (sHR: 0.45, 95% CI: 0.25–0.81). A consistent, albeit slightly attenuated, trend was observed in patients with suspected infections (sHR: 0.68, 95% CI: 0.35–1.32), with no significant interaction between the strata (P for interaction = 0.31). Similarly, the effect estimates appeared nominally stronger in patients with lower disease severity (APACHE II score <20; sHR: 0.42, 95% CI: 0.18–0.98) and in those not receiving concomitant vancomycin (sHR: 0.48, 95% CI: 0.26–0.88). No significant interaction was observed for any of the prespecified subgroups (all P for interaction > 0.05). However, due to the limited sample size within individual strata, these findings suggest a consistent trend rather than definitive proof of robustness across all clinical characteristics.
Risk Factor Analysis for Acute Kidney Injury
To identify independent risk factors associated with the development of acute kidney injury while accounting for varying treatment durations and the competing risk of mortality, univariate and multivariate Fine-Gray competing-risks regression analyses were performed within the propensity score-matched cohort (n=292). The results are presented in Table 5.
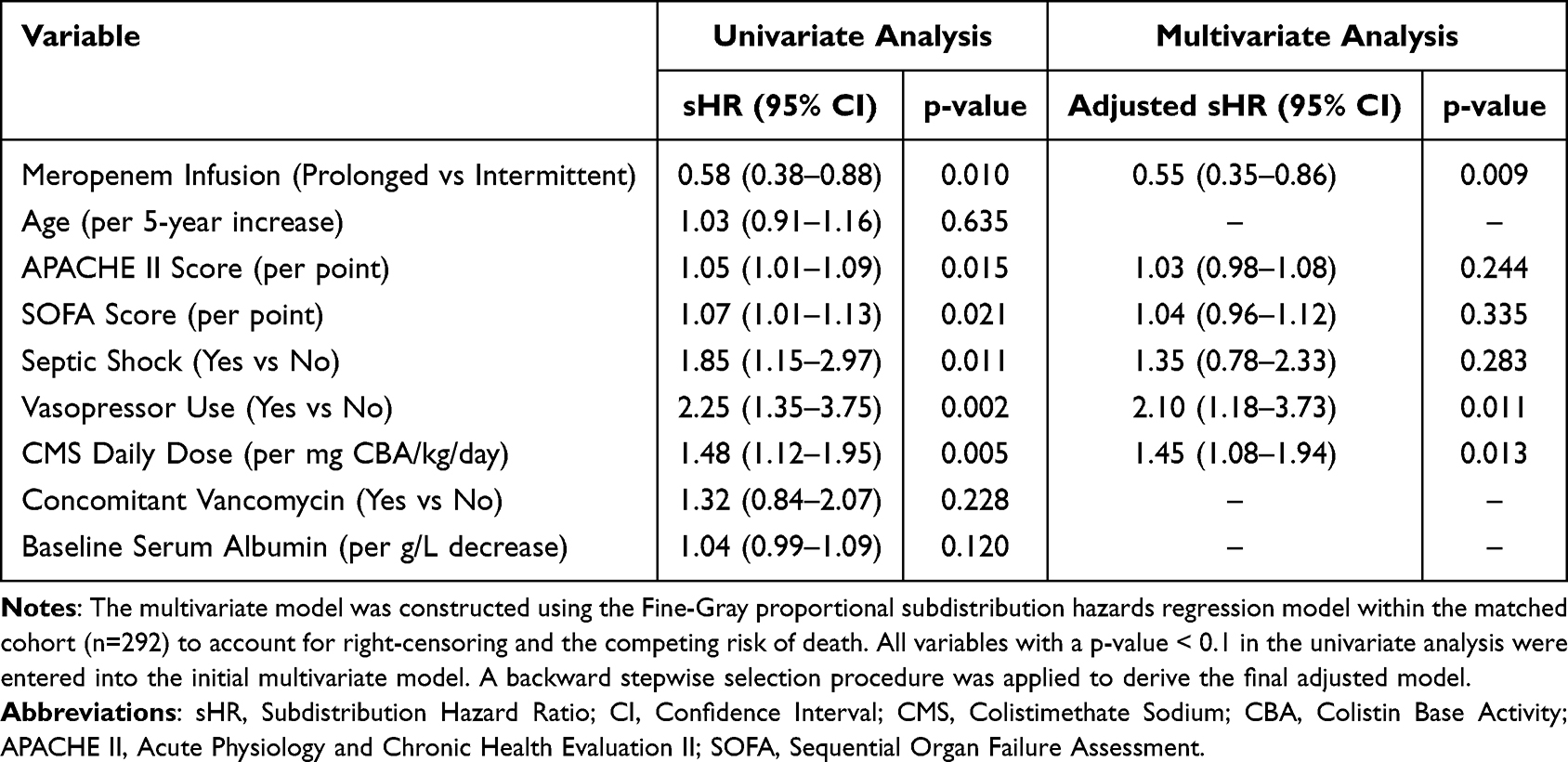 |
Table 5 Univariate and Multivariate Fine-Gray Competing-Risks Regression Analysis of Risk Factors for Acute Kidney Injury in the Matched Cohort |
In the univariate analysis, prolonged infusion of meropenem was significantly associated with a reduced risk of AKI (sHR: 0.58, 95% CI: 0.38–0.88, p=0.010). Factors associated with an increased risk of AKI included a higher APACHE II score (sHR per point: 1.05, 95% CI: 1.01–1.09, p=0.015), the presence of septic shock (sHR: 1.85, 95% CI: 1.15–2.97, p=0.011), vasopressor use (sHR: 2.25, 95% CI: 1.35–3.75, p=0.002), and a higher daily dose of colistimethate sodium (sHR per mg CBA/kg/day: 1.48, 95% CI: 1.12–1.95, p=0.005).
In the multivariate Fine-Gray model, prolonged meropenem infusion remained an independent protective factor (adjusted sHR: 0.55, 95% CI: 0.35–0.86, p=0.009). Concurrently, vasopressor use (adjusted sHR: 2.10, 95% CI: 1.18–3.73, p=0.011) and higher daily CMS dose (adjusted sHR per mg CBA/kg/day: 1.45, 95% CI: 1.08–1.94, p=0.013) were confirmed as independent risk factors driving AKI incidence.
Sensitivity Analysis
To assess the robustness of our primary findings, a sensitivity analysis was conducted using the entire pre-matched cohort (n=444) utilizing the identical competing-risks framework. A multivariable Fine-Gray regression model was constructed, adjusting for the same set of clinically relevant covariates used in the propensity score model. The results of this analysis, presented alongside the primary matched analysis in Table 6, demonstrated substantial consistency.
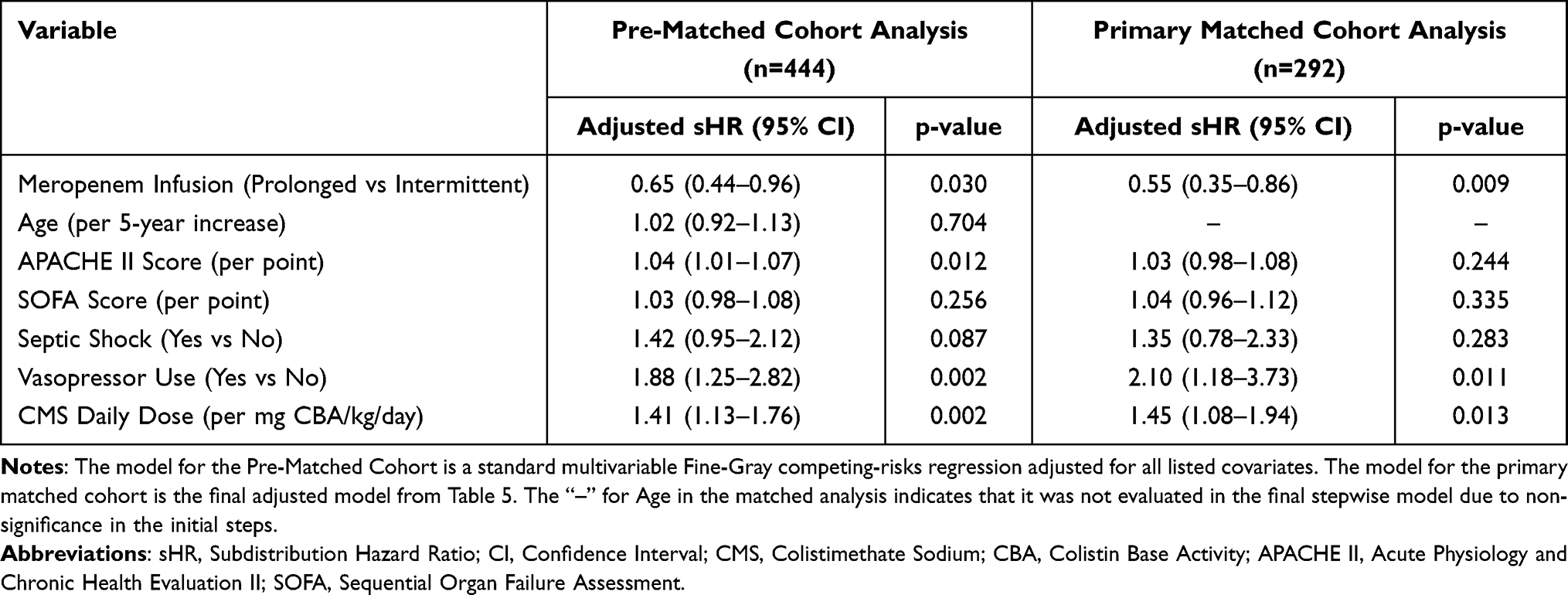 |
Table 6 Sensitivity Analysis: Comparison of Multivariable Fine-Gray Models in the Pre-Matched and Matched Cohorts |
In the pre-matched, adjusted model, prolonged meropenem infusion remained significantly associated with a reduced risk of AKI (adjusted sHR: 0.65, 95% CI: 0.44–0.96, p=0.030). While the point estimate (sHR=0.65) was slightly attenuated compared to the estimate from the matched analysis (sHR=0.55), the effect direction and statistical significance were conserved. Furthermore, the identities of the independent risk factors were consistent across both analyses. The concordance in the direction, significance, and key risk factors between the two distinct analytical approaches strongly validates the reliability of the kidney-sparing effect of the prolonged infusion strategy in the presence of competing mortality risks.
Discussion
The primary objective of this study was to evaluate whether an extended-infusion strategy for meropenem (≥3 hours) could mitigate the risk and severity of AKI in critically ill patients receiving concurrent colistimethate sodium (CMS). Our analysis demonstrated that prolonged infusion was independently associated with a significant reduction in both the incidence and severity of AKI. Additionally, we observed favorable trends toward reduced requirements for renal replacement therapy and lower in-hospital mortality.
Our findings add to the evolving evidence regarding extended-infusion beta-lactam therapy. While its impact on mortality remains debated, with some meta-analyses suggesting a survival benefit21,22 and others showing equipoise, our study innovatively shifts the focus to a critical safety outcome: nephrotoxicity. In contrast to the MERCY randomized clinical trial, which found no significant difference in 28-day mortality or clinical cure between continuous and intermittent meropenem infusions in a broad septic population,23 our cohort focused specifically on patients receiving concurrent CMS. We observed a distinct renal benefit, which aligns with a meta-analysis by Kondo et al suggesting that prolonged beta-lactam infusions may reduce AKI risk.24 While the bactericidal rationale for extending infusions of time-dependent agents is well established,25–27 our observations suggest that this administrative modification may also be associated with mitigated organ toxicity. We hypothesize that the high baseline risk of CMS-induced nephrotoxicity28,29 makes the kidney-sparing potential of this infusion strategy more discernible.
The exact mechanisms underlying the observed renal protection cannot be definitively determined from this retrospective design; however, several hypotheses can be generated. Pharmacokinetically, extended infusions avoid the high peak concentrations and fluctuations typical of intermittent boluses.27 We postulate that more stable tissue concentrations might reduce concentration-dependent toxic stress on renal tubular epithelial cells. Additionally, our risk factor analysis reaffirmed that higher CMS doses and vasopressor requirements independently predict AKI, consistent with known polymyxin nephrotoxicity and hypoperfusion effects.29,30 Despite these factors, extended meropenem infusion remained a significant protective factor.
Furthermore, our exploratory subgroup analyses generated intriguing hypotheses for future investigation, though these findings must be interpreted with extreme caution due to the limited sample sizes and wider confidence intervals within individual strata. The observed protective association appeared more pronounced in patients with lower illness severity (APACHE II <20) and those not receiving concurrent vancomycin. We hypothesize that overwhelming physiological derangements or synergistic nephrotoxic insults (eg., vancomycin combined with anti-pseudomonal beta-lactams31–33) may obscure the marginal benefit of optimizing a single drug’s infusion.34 Importantly, in the subgroup with microbiologically proven, susceptible CR-GNB infections, the kidney-sparing association was highly pronounced (sHR 0.45). While inadequately treated infection intrinsically drives AKI via systemic inflammation and microcirculatory dysfunction,35,36 isolating patients with assured antimicrobial susceptibility helps limit this confounding factor. This suggests that the observed benefit in this subgroup may be more closely related to the modified PK/PD profile rather than improved infection control alone.
Clinically, shifting from intermittent to extended infusion represents a noncost, readily implementable intervention that may optimize patient safety, pending further prospective validation. The use of PSM and multiple sensitivity analyses strengthened our evaluation of AKI and related outcomes by minimizing baseline imbalances, lending credibility to the observed associations.
Several critical limitations must be stated prominently. Most importantly, the retrospective, single-center design inherently subjects our results to potential residual, unmeasured confounding and information bias, despite rigorous PSM adjustments. Consequently, our findings establish an association, not causality. Second, reflecting a single center’s practices, the results may have limited generalizability to other healthcare settings. Third, our reliance on existing medical records limited the granularity of data regarding precise fluid balances and pathogen-specific MIC values. Furthermore, the subgroup analyses were inherently exploratory and underpowered to detect significant interactions; consequently, the point estimates within these smaller strata cannot be used to draw definitive clinical conclusions, and our institutional definition of extended infusion (≥3 hours) may not capture the full dose‒response spectrum of longer durations.
Conclusion
This PSM retrospective study demonstrated an independent association between extended infusion of meropenem and a significantly lower incidence and reduced severity of AKI in critically ill patients receiving concurrent colistimethate sodium. This simple, cost-neutral dosing adjustment represents a potential kidney-sparing strategy to improve the safety profile of this antibiotic combination. However, given the inherent limitations of our observational design, these findings are hypothesis-generating and require definitive validation through future prospective, multicenter randomized controlled trials.
Data Sharing Statement
All the reported data are available within the article.
Ethics Statement
This study was approved by the Medical Ethics Committee of The Affiliated People’s Hospital of Ningbo University (No. 2604151442172). The study protocol was reviewed and approved by the Hospital’s Institutional Review Board, which granted a waiver of informed consent due to the retrospective, observational, and anonymized nature of the research. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki. All patient data were handled with strict confidentiality and in compliance with institutional data protection policies.
Funding
This work was funded by the General Projects of the Medical Science and Technology Project of Zhejiang Province (2025KY1479).
Disclosure
The authors declare that the research was conducted in the absence of any commercial funding, and no conflict of interest exists.
References
1. Perez F, El Chakhtoura NG, Bonomo RA. Management of severe infections: multidrug-resistant and carbapenem-resistant gram-negative bacteria. Med Clin North Am. 2025;109(3):735–15. doi:10.1016/j.mcna.2025.01.003
2. Huralska M, Pogue JM, Rybak M, et al. The impact of synergistic therapy between colistin and meropenem on outcomes of patients with pneumonia or bloodstream infection due to carbapenem-resistant gram-negative pathogens. Clin Infect Dis. 2026;82(3):391–398. doi:10.1093/cid/ciaf398
3. Hoste EA, Bagshaw SM, Bellomo R, et al. Epidemiology of acute kidney injury in critically ill patients: the multinational AKI-EPI study. Intensive Care Med. 2015;41(8):1411–1423. doi:10.1007/s00134-015-3934-7
4. Mally A, Jarzina S. Mapping adverse outcome pathways for kidney injury as a basis for the development of mechanism-based animal-sparing approaches to assessment of nephrotoxicity. Front Toxicol. 2022;4:863643. doi:10.3389/ftox.2022.863643
5. Dalfino L, Puntillo F, Ondok MJ, et al. Colistin-associated acute kidney injury in severely ill patients: a step toward a better renal care? A prospective cohort study. Clin Infect Dis. 2015;61(12):1771–1777. doi:10.1093/cid/civ717
6. De Rose DU, Cairoli S, Dionisi M, et al. Therapeutic drug monitoring is a feasible tool to personalize drug administration in neonates using new techniques: an overview on the pharmacokinetics and pharmacodynamics in neonatal age. Int J Mol Sci. 2020;21(16):5898. doi:10.3390/ijms21165898
7. Sridharan K. Nephrotoxicity risks of colistin-combination therapy: a USFDA adverse event reporting system analysis using disproportionality and interaction assessment. Expert Opin Drug Saf. 2025;1–10. doi:10.1080/14740338.2025.2499672
8. Katip W, Uitrakul S, Oberdorfer P. A comparison of colistin versus colistin plus meropenem for the treatment of carbapenem-resistant Acinetobacter baumannii in critically ill patients: a propensity score-matched analysis. Antibiotics. 2020;9(10):647. doi:10.3390/antibiotics9100647
9. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious diseases Society of America 2023 guidance on the treatment of antimicrobial resistant gram-negative infections. Clin Infect Dis. 2024;ciae403. doi:10.1093/cid/ciad428
10. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–S266.
11. Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2(1):1–138.
12. Lertwattanachai T, Montakantikul P, Tangsujaritvijit V, et al. Clinical outcomes of empirical high-dose meropenem in critically ill patients with sepsis and septic shock: a randomized controlled trial. J Intensive Care. 2020;8:26. doi:10.1186/s40560-020-00442-7
13. Rolain H, Schwartz Z, Jubrail R, et al. Meta-analysis on safety of standard vs prolonged infusion of beta-lactams. Int J Antimicrob Agents. 2024;64(4):107309. doi:10.1016/j.ijantimicag.2024.107309
14. Alvarado Reyes Y, Cruz R, Gonzalez J, Perez Y, Wolowich WR. Incidence of acute kidney injury in intermittent versus continuous infusion of polymyxin B in hospitalized patients. Ann Pharmacother. 2019;53(9):886–893. doi:10.1177/1060028019841898
15. Blevins AM, Lashinsky JN, McCammon C, Kollef M, Micek S, Juang P. Incidence of acute kidney injury in critically ill patients receiving vancomycin with concomitant piperacillin-tazobactam, cefepime, or meropenem. Antimicrob Agents Chemother. 2019;63(5):e02658–18. doi:10.1128/AAC.02658-18
16. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
17. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
18. Vincent JL, Moreno R, Takala J, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on sepsis-related problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22(7):707–710. doi:10.1007/BF01709751
19. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
20. Chawla LS, Bellomo R, Bihorac A, et al. Acute kidney disease and renal recovery: consensus report of the acute disease quality initiative (ADQI) 16 Workgroup. Nat Rev Nephrol. 2017;13(4):241–257. doi:10.1038/nrneph.2017.2
21. Mu Z, Wang J, Mu E. Impact of prolonged versus intermittent infusion of meropenem on mortality and clinical outcomes in patients with severe infection: a systematic review and meta-analysis. J Infect Chemother. 2025;31(3):102634. doi:10.1016/j.jiac.2025.102634
22. Roberts JA, Croom K, Adomakoh N. Continuous infusion of beta-lactam antibiotics: narrative review of systematic reviews, and implications for outpatient parenteral antibiotic therapy. Expert Rev Anti Infect Ther. 2023;21(4):375–385. doi:10.1080/14787210.2023.2184347
23. Monti G, Bradic N, Marzaroli M, et al. Continuous vs intermittent meropenem administration in critically ill patients with sepsis: the MERCY randomized clinical trial. JAMA. 2023;330(2):141–151. doi:10.1001/jama.2023.10598
24. Kondo Y, Ota K, Imura H, Hara N, Shime N. Prolonged versus intermittent β-lactam antibiotics intravenous infusion strategy in sepsis or septic shock patients: a systematic review with meta-analysis and trial sequential analysis of randomized trials. J Intensive Care. 2020;8:77. doi:10.1186/s40560-020-00490-z
25. Gatti M, Cojutti PG, Pea F. Impact of attaining aggressive vs conservative PK/PD target on the clinical efficacy of beta-lactams for the treatment of gram-negative infections in the critically ill patients: a systematic review and meta-analysis. Crit Care. 2024;28(1):123. doi:10.1186/s13054-024-04911-5
26. Novy E, Martinière H, Roger C. The current status and future perspectives of beta-lactam therapeutic drug monitoring in critically ill patients. Antibiotics. 2023;12(4):681. doi:10.3390/antibiotics12040681
27. Zhao DW, Lohans CT. Combatting Pseudomonas aeruginosa with β-Lactam antibiotics: a revived weapon? Antibiotics. 2025;14(5):526. doi:10.3390/antibiotics14050526
28. Nation RL, Rigatto MHP, Falci DR, Zavascki AP. Polymyxin acute kidney injury: dosing and other strategies to reduce toxicity. Antibiotics. 2019;8(1):24. doi:10.3390/antibiotics8010024
29. Alotaibi FM, Alshehail BM, Al Jamea ZAH, et al. Incidence and risk factors of colistin-induced nephrotoxicity associated with the international consensus guidelines for the optimal use of the polymyxins: a retrospective study in a Tertiary Care Hospital, Saudi Arabia. Antibiotics. 2022;11(11):1569. doi:10.3390/antibiotics11111569
30. Guinot PG, Martin A, Berthoud V, et al. Vasopressor-sparing strategies in patients with shock: a scoping-review and an evidence-based strategy proposition. J Clin Med. 2021;10(14):3164. doi:10.3390/jcm10143164
31. Pan K, Li R, Li Y, Ding X, Li X, Lv Q. Vancomycin combined with piperacillin/tazobactam increases the risk of acute kidney injury compared with vancomycin plus other anti-pseudomonal beta-lactams: a systematic review and network meta-analysis. J Antimicrob Chemother. 2025;80(1):47–58. doi:10.1093/jac/dkae410
32. Alshehri AM, Al Yami MS, Aldairem A, et al. Evaluating the risk of acute kidney injury and mortality associated with concomitant use of vancomycin with piperacillin/tazobactam or meropenem in critically ill and noncritically ill patients: a systematic review and meta-analysis. BMC Infect Dis. 2025;25(1):36. doi:10.1186/s12879-024-10227-0
33. Li R, Li Y, Xu C, et al. Incidence of acute kidney injury in critically ill patients receiving vancomycin with concomitant piperacillin-tazobactam versus other beta-lactams: a systematic review and meta-analysis. J Pharm Technol. 2025;41. doi:10.1177/87551225251350894
34. Ow CPC, Trask-Marino A, Betrie AH, Evans RG, May CN, Lankadeva YR. Targeting oxidative stress in septic acute kidney injury: from theory to practice. J Clin Med. 2021;10(17):3798. doi:10.3390/jcm10173798
35. Peerapornratana S, Manrique-Caballero CL, Gómez H, Kellum JA. Acute kidney injury from sepsis: current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019;96(5):1083–1099. doi:10.1016/j.kint.2019.05.026
36. Pais T, Jorge S, Lopes JA. Acute kidney injury in sepsis. Int J Mol Sci. 2024;25(11):5924. doi:10.3390/ijms25115924
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Dexmedetomidine Exposure with Long-Term Mortality in Patients with Dialysis-Requiring Acute Kidney Injury: A Propensity Score–Matched Retrospective Cohort Study
Hung KC, Chang LC, Chang YJ, Lai YC, Lin CM, Chen IW
Drug Design, Development and Therapy 2026, 20:598443
Published Date: 27 April 2026