Back to Journals » Infection and Drug Resistance » Volume 10
Extended-spectrum beta-lactamase- and carbapenemase-producing Enterobacteriaceae among Ethiopian children
Authors Legese MH ![]() , Weldearegay GM, Asrat D
, Weldearegay GM, Asrat D ![]()
Received 9 November 2016
Accepted for publication 20 December 2016
Published 25 January 2017 Volume 2017:10 Pages 27—34
DOI https://doi.org/10.2147/IDR.S127177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Melese Hailu Legese,1 Gebru Mulugeta Weldearegay,1 Daniel Asrat,2
1Department of Clinical Laboratory Sciences, School of Allied Health Sciences, 2Department of Microbiology, Immunology and Parasitology, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Background: Infections by extended-spectrum beta-lactamase- (ESBL) and carbapenem-resistant Enterobacteriaceae (CRE) are an emerging problem in children nowadays. Hence, the aim of this study was to determine the prevalence of ESBL- and carbapenemase-producing Enterobacteriaceae among children suspected of septicemia and urinary tract infections (UTIs).
Methods: A cross-sectional study was conducted from January to March 2014. A total of 322 study participants suspected of septicemia and UTIs were recruited. All blood and urine samples were cultured on blood and MacConkey agar. All positive cultures were characterized by colony morphology, Gram stain, and standard biochemical tests. Antimicrobial susceptibility test was performed on Muller-Hinton agar using disk diffusion. ESBL was detected using combination disk and double-disk synergy methods, and the results were compared. Carbapenemase was detected by modified Hodge method using meropenem. Data were analyzed using SPSS version 20.
Results: The overall prevalence of ESBL- and carbapenemase-producing Enterobacteriaceae was 78.57% (n=22/28) and 12.12%, respectively. Among the Enterobacteriaceae tested, Klebsiella pneumoniae (84.2%, n=16/19), Escherichia coli (100%, n=5/5), and Klebsiella oxytoca (100%, n=1/1) were positive for ESBL. Double-disk synergy method showed 90.9% sensitivity, 66.7% specificity, 95.2% positive predictive value, and 50% negative predictive value. Carbapenemase-producing Enterobacteriaceae were K. pneumoniae (9.09%, n=3/33) and Morganella morganii (3.03%, n=1/33).
Conclusion: Screening Enterobacteriaceae for ESBL production is essential for better antibiotics selection and preventing its further emergence and spread. In resource-limited settings, double-disk synergy method can be implemented for screening and confirming ESBL production. Moreover, occurrence of CRE in countries where no carbapenems are sold is worrying microbiologists as well as clinicians. Hence, identifying factors that induce carbapenemase production in the absence of carbapenems prescription is essential for control of CRE dissemination within the community.
Keywords: ESBL, carbapenem resistance, Enterobacteriaceae, Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia
Introduction
Resistance of Gram-negative bacteria to antibiotics has increased at an alarming pace over the last two decades, particularly the emergence of Enterobacteriaceae resistant to third-generation cephalosporins and aztreonam1 which is commonly associated with the expression of extended-spectrum beta-lactamases (ESBLs).2 These enzymes confer resistance to nearly all beta-lactam antibiotics such as ceftazidime, cefotaxime, ceftriaxone, monobactam – aztreonam, and related oxyimino beta-lactams.2,3 If Enterobacteriaceae are resistant to one of the extended-spectrum cephalosporins, it means they are therapeutically resistant to all the cephalosporins even though antimicrobial sensitivity is indicated in the laboratory test results.4 Moreover, many ESBL-producing Enterobacteriaceae are also resistant to other antimicrobial agents such as aminoglycosides, trimethoprim, and the quinolones which poses a serious antibiotic management problem as the genes for ESBL production are easily transferred through plasmids.5,6
ESBL-producing Enterobacteriaceae have worldwide distributions with varying degree of prevalence in community as well as hospitals.4–7 Nowadays, infections due to ESBL-producing Enterobacteriaceae are concerning for many reasons including increased hospital costs, length of stay, and mortality rates.4,6,7 For the pediatric population, blood stream infections and urinary tract infections (UTIs) due to Enterobacteriaceae resistant to ESBL are an emerging problem.1 This alerts clinical microbiologists to identify these ESBL-producing organisms parallel to antimicrobial susceptibility testing even in resource-limited settings by applying simple screening and confirmatory methods. Data obtained from such methods are so valuable to develop appropriate institutional-based drug therapy guideline.7,8 Though various phenotypic ESBL detection methods have been described, implementation of highly sensitive and specific methods in resource-limited areas is challenging yet.8
Infections caused by ESBL- or plasmid-mediated AmpC-producing Enterobacteriaceae are often treated by carbapenems (e.g., ertapenem, imipenem, meropenem, and doripenem) which are antimicrobials of last resort and crucial for the management of life-threatening health care-associated infections.9 However, due to recent emergence and spread of imipenem/meropenem-resistant Enterobacteriaceae throughout the world, clinical utility of this group of antibiotics is under threat.10 Production of carbapenemases that are capable of hydrolyzing the carbapenems and loss of outer membrane proteins are major mechanisms through which Enterobacteriaceae develop resistance against this group of drugs.9,10 The growing incidence of carbapenemase-producing strains is therefore another major concern especially among countries where carbapenems are not prescribed at all like Ethiopia.10
Materials and methods
A cross-sectional study was conducted from January to March 2014 at Tikur Anbessa Specialized Hospital, located in the capital city Addis Ababa. It is the largest referral hospital of Ethiopia. A total of 322 study participants (children <15 years) who were suspected of septicemia and UTIs were recruited using convenient sampling technique. The sample size was calculated based on single-population proportion using a previous study done in Ethiopia.11 Both inpatients and outpatients were included; however, patients who took antibiotics within the last 2 weeks and nonvolunteers were excluded. Demographic characteristics of the patients were recorded using predesigned sheets after obtaining informed consent. From septicemia-suspected children, 3–5 mL of blood was collected aseptically using antiseptics (70% alcohol and 2% tincture iodine) and transferred to blood culture bottle containing sterile brain heart infusion (Thermo Fisher Scientific, Waltham, MA, USA). A minimum blood-to-broth ratio of 1:10 was maintained. From the UTIs-suspected children, first morning mid-stream urine samples were collected using sterile wide-mouth container. The study participants’ parents/guardians were given appropriate instructions before providing urine samples. Blood specimens within 30 minutes and urine specimens immediately after collection were brought to microbiology laboratory for bacterial analysis.
Culture and identification
Blood culture bottles were incubated at 37°C and inspected daily for the signs of bacterial growth for 7 days. Turbid blood samples before the seventh day and nonturbid blood samples on the seventh day were subcultured on blood agar (Oxoid) and MacConkey agar (BD, Franklin Lakes, NJ, USA), and incubated at 37°C for 24 hours aerobically. All urine samples were inoculated on blood agar (Oxoid) and MacConkey agar (BD), and incubated at 37°C for 24 hours. Significant bacteriuria was determined on MacConkey agar. All positive cultures were characterized by colony characteristics, Gram stain, and standard biochemical tests. Enterobacteriaceae were classified to species levels using triple sugar iron, indole, citrate, urea, lysine decarboxylase, and motility. After identification, each Enterobacteriaceae was subjected to ESBL and carbapenemase detections as per Clinical and Laboratory Standards Institute (CLSI) and European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines.11,12
Drug susceptibility patterns
The disk diffusion was performed, and after 16–18 hours of incubation at 37°C, zone of inhibition was measured and interpreted as recommended by the CLSI.11 Using a sterile wire loop, three to five pure colonies were picked from MacConkey agar and emulsified in nutrient broth. Standard inoculums adjusted to 0.5 McFarland using McFarland Densitometer were swabbed onto Muller-Hinton agar (dispensed on 100 mm plate). Drug susceptibility testing of all Enterobacteriaceae was performed using disk diffusion method against amoxicillin (30 µg, BD), amoxicillin-clavulanic acid (30 µg, BD), chloramphenicol (30 µg, BD), gentamicin (10 µg, BD), sulfamethoxazole-trimethoprim (1.25 µg, BD), cefotaxime (30 µg, BD), cefoxitin (30 µg, Oxoid), tetracycline (30 µg, BD), nitrofurantoin (300 µg, BD), norfloxacin (5 µg, BD), imipenem (10 µg, Oxoid), and meropenem (10 µg, Oxoid). In this study, multidrug resistance was defined as simultaneous resistance to two or more drugs of different classes of antimicrobial agents.
ESBL detection
Initial screening of Enterobacteriaceae for ESBL was done based on diameters of zone of inhibitions produced by ceftazidime (30 µg, BD), ceftriaxone (30 µg, BD), and cefotaxime (30 µg, BD) according to the CLSI screening criteria. The breakpoints indicative of suspicion for ESBL production were ≤22 mm for ceftazidime, ≤25 mm for ceftriaxone, and ≤27 mm for cefotaxime. A combined disk method was used as a confirmatory phenotypic method for ESBLs detection according to CLSI. Ceftazidime (30 µg, BD) and cefotaxime (30 µg, BD) disks alone and their combinations with clavulanic acid (30 µg/10 µg) were used for phenotypic confirmations of ESBLs presence. A ≥5 mm increase in zone diameters for either of the cephalosporin disks or their respective cephalosporin/clavulanate disks was interpreted as ESBL producer.
Double-disk synergy method was compared against combination disk method for detection of ESBL to know if it was the best suitable phenotypic method in resource-limited routine bacteriology laboratory. Hence, all ESBL-positive Enterobacteriaceae detected by combination disk method were tested again by double-disk synergy method for ESBL production. The antibiotic disks used were ceftriaxone (30 µg, BD), cefotaxime (30 µg, BD), ceftazidime (30 µg, BD), aztreonam (30 µg, BD), and amoxicillin/clavulanic acid (20/10 µg, BD) according to EUCAST.12 The four antibiotics were placed at distances of 20 mm edge to edge from the amoxicillin/clavulanic acid disk that was placed in the middle of the plate. After 24 hours of incubation, if an enhanced zone of inhibition between either of the cephalosporin antibiotics and the amoxicillin/clavulanic acid disk occurred, the test was considered as ESBL positive. Finally, sensitivity, specificity, and positive and negative predictive values of double-disk synergy method were calculated against combination disk method.
Carbapenemase detection
All carbapenem (imipenem and/or meropenem)-resistant or carbapenem-intermediate Enterobacteriaceae were checked for the production of carbapenemase using modified Hodge test (MHT; cloverleaf test) according to CLSI. When Escherichia coli American Type Culture Collection (ATCC) 25922 grew around the streak organism and showed indentation, the isolate was recorded as a carbapenemase producer, while no growth of the ATCC E. coli 25922 along the streak organism indicated a negative test and the isolate was not a carbapenemase producer.
Quality control and data quality assurance
Standard operating procedures (SOPs) were strictly followed verifying that media meet expiration date and quality control parameters per CLSI. Visual inspections of cracks in media or plastic petridishes, unequal fill, hemolysis, evidence of freezing, bubbles, and contaminations were done. Quality control was performed to check the quality of medium. Each new lot was quality-controlled before use by testing the E. coli ATCC 25922 and/or Staphylococcus aureus ATCC 25923 standard control strains. During ESBLs detection, ESBL-positive Klebsiella pneumoniae ATCC 700603 and ESBL-negative E. coli ATCC 25922 control strains were used in this study. For carbapenemase detection, E. coli ATCC 25922 strain was used as a negative control. Blood and urine specimens were collected in accordance with SOPs and brought to bacteriology laboratory immediately for bacteriological analysis. Culture results were recorded carefully before data entry, and the data were double-checked by a different person before analysis.
Statistical analysis and interpretation
The data were analyzed using SPSS version 20 (IBM Corporation, Armonk, NY, USA), and descriptive statistics (mean, percentages, or frequency) was calculated. Sensitivity, specificity, and positive and negative predictive values were calculated for comparing double-disk synergy method against combination disk method.
Ethical clearance
The study was approved by Department Research and Ethical Review Committee (DRERC) of the Department of Medical Laboratory Science, School of Allied Health Sciences, College of Health Sciences, Addis Ababa University. After explaining the purpose and procedures of the study to the study participants’ parents or guardians, a written informed consent was obtained. Permission letter was also obtained from the study site. Those children whose parents or guardians gave written informed consent were selected and enrolled as study participants in this study.
Results
Enterobacteriaceae from blood and urine culture
Three hundred and twenty-two study participants (children <15 years) who were suspected of septicemia and UTIs were included in this study. Of these patients, 53.4% (n=172/322) were males, while 46.6% (n=150/322) were females with a mean (standard deviation) age of 3.22 (1.229) years, and 61.5% (n=198/322) of them were inpatients. Thirty-three Enterobacteriaceae were isolated from 322 blood and urine specimens (Table 1). Majority of Enterobacteriaceae (72.7%, n=24/33) were isolated from urine cultures, and 63.6% (n=21/33) of them were identified from male patients. The most frequent isolates were K. pneumoniae (57.57%, n=19/33) and E. coli (18.2%, n=6/33). Other Enterobacteriaceae isolates were Morganella morganii (6.1%, n=2/33), Enterobacter aerogenes (3.0%, n=1/33), Enterobacter cloacae (3.0%, n=1/33), Citrobacter spp. (3.0%, n=1/33), Salmonella spp. (3.0%, n=1/33), Klebsiella oxytoca (3.0%, n=1/33), and Proteus mirabilis (3.0%, n=1/33). Most of these Enterobacteriaceae were isolated from patients who attended outpatient department.
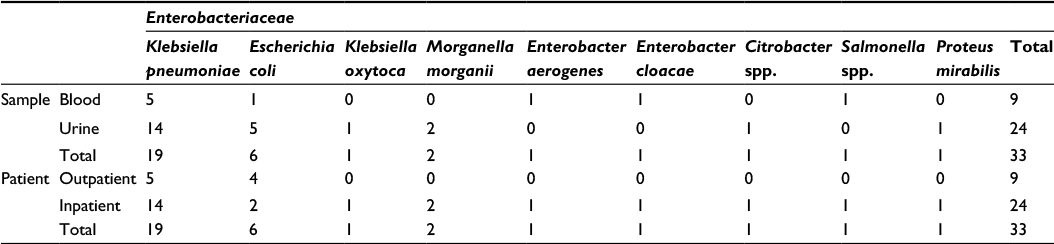 | Table 1 Frequency of Enterobacteriaceae isolated from blood and urine cultures |
Antibiotic resistance patterns of isolated Enterobacteriaceae
All Enterobacteriaceae showed the highest resistance to amoxicillin (89.1%), sulfamethoxazole-trimethoprim (83.6%), and cefotaxime (85.5%), and least resistance to nitrofurantoin (36.9%), imipenem (12.2%), and meropenem (14.6%). The frequent isolates K. pneumoniae (57.57%, n=19/33) showed the highest resistance to cefotaxime (100%), amoxicillin (94.7%), amoxicillin-clavulanic acid (89.5%), sulfamethoxazole-trimethoprim (89.5%), and gentamicin (89.5%). They showed the lowest resistance to imipenem (10.5%), meropenem (15.8%), and norfloxacin (15.8%) compared to the other tested drugs (Table 2). In our study, cefotaxime was least effective (100% resistance) against K. pneumoniae (57.57%, n=19/33), M. morganii (6.1%, n=2/33), Citrobacter spp. (3%, n=1/33), E. aerogenes (3%, n=1/33), and E. cloacae (3%, n=1/33) (Table 2).
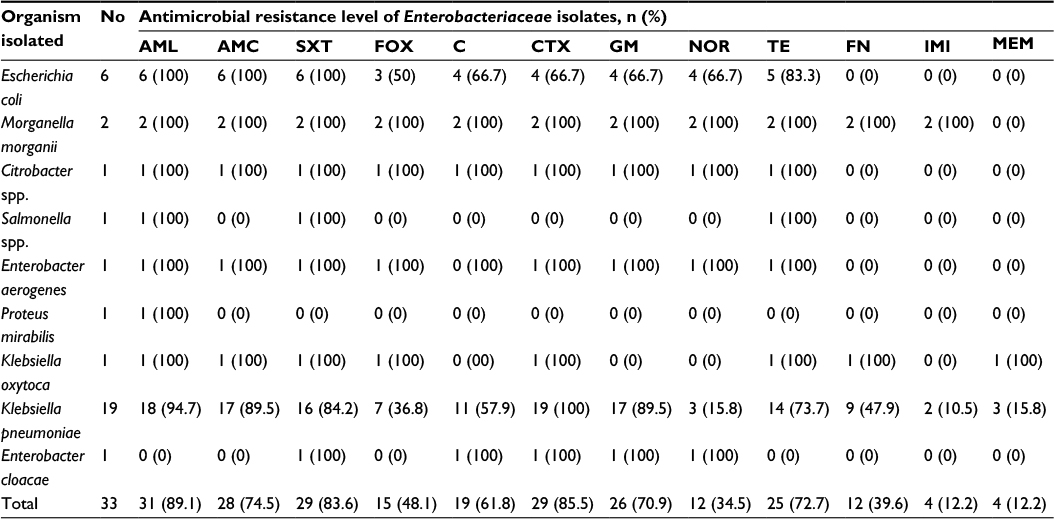 | Table 2 Antimicrobial resistance levels of Enterobacteriaceae Abbreviations: AML, amoxicillin; AMC, amoxicillin-clavulanic acid; SXT, sulfamethoxazole-trimethoprim; FOX, cefoxitin; C, chloramphenicol; CTX, cefotaxime; GM, gentamicin; NOR, norfloxacin; TE, tetracycline; FN, nitrofurantoin; IMI, imipenem; MEM, meropenem. |
Prevalence of ESBL-positive Enterobacteriaceae
From the 33 Enterobacteriaceae, 28 of them were tested for ESBLs production, while M. morganii (6.1%, n=2/33), E. aerogenes (3.0%, n=1/33), E. cloacae (3.0%, n=1/33), and Citrobacter (3.0%, n=1/33) were excluded from ESBL testing because cefepime alone and with clavulanic acid combination was not available. The overall prevalence of ESBL-producing Enterobacteriaceae was 78.6% (n=22/28). Among Enterobacteriaceae tested for ESBL, K. pneumoniae (84.2%, n=16/19), E. coli (100%, n=5/5), and K. oxytoca (100%, n=1/1) were positive.
Comparison of double-disk synergy method against combination disk method
All ESBL-positive Enterobacteriaceae (n=22) were further tested by the double-disk synergy method for ESBL production. This method showed 90.9% (n=20/22) sensitivity, 66.7% specificity, 95.2% positive predictive value, and 50% negative predictive value.
Carbapenem-resistant Enterobacteriaceae
Regardless of their ESBL result, all Enterobacteriaceae were tested for carbapenemase production. Among the 33 isolated Enterobacteriaceae, 18.2% (n=6/33) showed intermediate or high resistance to imipenem and/or meropenem, and they were suspected of carbapenemase production. All carbapenemase-suspected organisms were isolated from urine cultures of inpatients. The overall prevalence of carbapenem-resistant Enterobacteriaceae (CRE) was 12.12% (n=4/33). Carbapenemase-producing organisms in this study were K. pneumoniae (10.5%, n=2/19), K. oxytoca (100%, n=1/1), and M. morganii (50%, n=1/2).
Discussion
Prevalence of ESBL-producing Enterobacteriaceae
The overall prevalence of ESBL-positive Enterobacteriaceae was 78.57% (n=22/28) which showed agreement with another study.13 Our result was better than other studies done in India where prevalence of ESBL-positive Enterobacteriaceae was 32.14% and that of carbapenemase-positive Enterobacteriaceae was 58%.14,15 K. pneumoniae (84.2%, n=16/19) were the most frequent ESBL-positive Enterobacteriaceae in line with a study done in Ahmadabad where the prevalence of ESBL-producing K. pneumoniae was 81.48%.13 However, our result was better compared to a previous study done in Ethiopia where prevalence of ESBL-producing K. pneumoniae was 33.3%.16 This indicated that ESBL-producing Enterobacteriaceae are growing rapidly overtime. K. oxytoca (100%, n=1/1) was another Klebsiella sp. positive for ESBL in this study which agreed with a study done in Sudan.17 Among all Enterobacteriaceae tested, E. coli (100%, n=5/5) were ESBL-positive in line with a study done in Saudi Arabia where all the 31 E. coli tested were positive for ESBL.18 Thus, the emergence of ESBLs-producing Enterobacteriaceae is clinically important, yet it remains relatively unappreciated by most clinicians.
Inappropriate and incorrect administration of antimicrobial agents in empirical therapies, lack of appropriate infection-control strategies which can cause a shift to increase in prevalence of resistant organisms in the community, and the selective pressure created for the use of third-generation cephalosporins have been described as most important factors in the appearance of ESBL-producing strains, though many reasons can be responsible and mentioned.15,16,19–23
All ESBL-positive Enterobacteriaceae showed the highest resistance to amoxicillin (89.1%), sulfamethoxazole-trimethoprim (83.5%), and cefotaxime (85.5%). It means that the use of these antibiotics for the treatment of infection caused by ESBL-producing strains may result in failure in significant proportion of cases. The choice of antibiotic agents effective against ESBLs-producing species is currently limited, which may cause serious therapeutic problems in the future.24,25 In our study, the organisms were only susceptible to norfloxacin (63.9%) and cefoxitin (50%) compared to other commonly tested drugs.
Comparison of double-disk synergy test against combination disk test
Double-disk synergy method using any of the four disks with a disk spacing of 20 mm detected enhancement of zone in 90.9% (n=20/22) from the 100% (n=22) of phenotypically confirmed ESBL-producing isolates detected by combination disk method. It showed similarity with another study which showed 95.0% sensitivity.24 However, it showed a higher sensitivity as compared to a study done in Ahmadabad;13 the sensitivity of double-disk synergy test was 81.18%. This method showed significant sensitivity (90.9%) with 66.7% specificity, 95.2% positive predictive value, and 50% negative predictive value. For controlling further emergence and spread of ESBL-positive Enterobacteriaceae, this method can be applied as routine ESBL detection method in routine bacteriology laboratory for general hospitals where technical resources and expertise may not be in abundant supply.
Carbapenem-resistant Enterobacteriaceae
Resistance to carbapenems with varying prevalence has been reported in places worldwide, such as Argentina, India, Nigeria, and the Netherlands.21,23,26,27 In our study, the prevalence of carbapenemase-producing Enterobacteriaceae was 12.2% which was in line with a study done in India which showed 12.26% prevalence of CRE28 and agreed with a study done in Nigeria which showed 14.0% prevalence of CRE.29 However, our finding showed a much lowered prevalence as compared to a study done in India23 which showed 59.1% prevalence of CRE. The lower prevalence in our study might be due to the fact that carbapenem is not commonly sold in our country. Occurrence of CRE is worrying microbiologists as well as clinicians, especially in areas where no carbapenems are prescribed. These enzymes-encoding genes might be imported from abroad probably, or they emerge locally and spread by gene transfer.26 In addition, the indiscriminate use of antibiotics as empirical therapy to treat the multidrug-resistant pathogens might be responsible for the emergence of these carbapenemase-producing Enterobacteriaceae isolates in the hospital settings.9,26 However, we have to be aware of the fact that these pathogens can also be community-acquired as CREs have also been isolated from the common water sources.23
In our study, all CRE were isolated from urine samples of inpatients which was supported by other studies done in India where most of the CRE isolates were from urine sample.23,28 Carbapenemase-producing organisms in this study were K. pneumoniae (10.5%, n=2/19), K. oxytoca (100%, n=1/1), and M. morganii (50%, n=1/2). This showed disagreement in prevalence as well as type of carbapenem-resistant bacteria isolated with the study done in Nigeria, in which CRE identified were E. coli (13.5%), K. pneumoniae (16.7%), and Proteus sp. (16.0%).30 However, a study done in Italy showed that the tested K. oxytoca (1, 100%) were positive for CRE by MHT.31 And this study also indicated a lower prevalence (15%, n=3/20) of carbapenem-resistant Klebsiella spp. as compared to other study where the prevalence of carbapenem-resistant Klebsiella spp. was 28.7%.32 The prevalence of 10.5% (n=2/19) of carbapenem-resistant K. pneumoniae was a relatively lower finding as compared to a study done in Iran.9
Most of the carbapenemase-producing Enterobacteriaceae were resistant to the routinely used antimicrobial agents as seen in almost all the studies.21,26,28 The frequent coresistance to other classes of antibiotics seen in CRE isolates might be because of the simultaneous presence of other resistance determinants often carried on plasmids and insertion sequence.9,23 CRE isolates often exhibit an extensively drug-resistant phenotype, resistance to most of the currently available antibiotics rendering them ineffective, and the clinical data on the antimicrobial agents available for the treatment of these isolates remains sparse.9,21 The multiple resistance capability of these bacteria may be due to multiple factors including uncontrolled antibiotic usage, inappropriate dosing regimens, widespread counterfeit and substandard antibiotics, and local hospital practices concerning isolation of patients with multiresistant pathogens which is poorly managed.27
Conclusion
The increasing frequency of ESBL-producing Enterobacteriaceae (78.57%) among children is an important problem for both microbiologists and clinicians. In resource-limited settings, double-disk synergy method can be implemented for screening and confirming ESBL production that might give valuable information for appropriate antibiotics selection and controlling the spread of ESBL-positive Enterobacteriaceae. The increasing prevalence of CRE mainly due to carbapenemase production is alarming in clinical practice, specifically in areas where no carbapenems are sold. This study provides a clearer picture of the current CRE scenario in the hospital setup, and hence, identifying factors that induce carbapenemase production in the absence of carbapenems prescription is essential for control of CRE dissemination within the community.
Acknowledgments
The authors greatly appreciate Addis Ababa University for supporting this study. They are also grateful to the Department of Clinical Laboratory Sciences that gave them ethical clearance for this study. Their deep gratitude goes to those study participants and their parents/guardians who showed their willingness to participate in this study by giving written consent.
Disclosure
The authors report no conflicts of interest in this work.
References
Taneja N, Sharma M. ESBLs detection in clinical microbiology: why & how? Indian J Med Res. 2008;127(4):297–300. | ||
Giriyapur RS, Nandihal NW, Krishna BV, Patil AB, Chandrasekhar MR. Comparison of disc diffusion methods for the detection of extended-spectrum beta lactamase-producing Enterobacteriaceae. J Lab Physicians. 2011;3(1):33–36. | ||
Bradford PA. Extended-spectrum beta-lactamases in the 21st century: characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. 2001;14(4):933–951. | ||
Leverstein-van Hall MA, Fluit AC, Paauw A, Box AT, Brisse S, Verhoef J. Evaluation of the Etest ESBL and the BD Phoenix, VITEK 1, and VITEK 2 automated instruments for detection of extended-spectrum beta-lactamases in multiresistant Escherichia coli and Klebsiella spp. J Clin Microbiol. 2002;40(10):3703–3711. | ||
Jonathan N. Screening for extended-spectrum beta-lactamase-producing pathogenic enterobacteria in district general hospitals. J Clin Microbiol. 2005;43(3):1488–1490. | ||
Dharmishtha GT, Gandhi PJ, Patel KN. A study on antibiotic related resistance in UTI patients: a comparison between community acquired and hospital acquired Escherichia coli. Natl J Community Med. 2012;3(2):255–258. | ||
Ahmed OI, El-Hady SA, Ahmed TM, Ahmed IZ. Detection of bla SHV and bla CTX-M genes in ESBL producing Klebsiella pneumoniae isolated from Egyptian patients with suspected nosocomial infections. Egypt J Med Hum Gene. 2013;14(3):277–283. | ||
Pitout JD, Nordmann P, Laupland KB, Poirel L. Emergence of Enterobacteriaceae producing extended-spectrum beta-lactamases (ESBLs) in the community. J Antimicrob Chemother. 2005;56(1):52–59. | ||
Amjad A, Mirza IA, Abbasi S, Farwa U, Malik N, Zia F. Modified Hodge test: a simple and effective test for detection of carbapenemase production. Iran J Microbiol. 2011;3(4):189–193. | ||
Sultan BA, Khan E, Hussain F, Nasir A, Irfan S. Effectiveness of modified Hodge Test to detect NDM-1 carbapenemases: an experience from Pakistan. J Pak Med Assoc. 2013;63(8):955–960. | ||
Clinical and Laboratory Standards Institute (CLSI). Performance standards for antimicrobial disk susceptibility tests; twenty-third informational supplement. CLSI document. 2013;33(1):M100-S23. | ||
EUCAST. EUCAST guidelines for detection of resistance mechanisms and specific resistances of clinical and/or epidemiological importance. 2013. | ||
Modi D, Patel D, Patel S, Jain M, Bhatt S, Vegad MM. Comparison of various methods for the detection of extended spectrum beta lactamase in Klebsiella pneumoniae isolated from neonatal intensive care unit, Ahmadabad. Natl J Med Res. 2012;2(3):348–353. | ||
Prabhu K, Bhat S, Rao S. Bacteriologic profile and antibiogram of blood culture isolates in a pediatric care unit. J Lab Physicians. 2010;2(2):85–88. | ||
Saghir S, Faiz M, Saleem M, Younus A, Aziz H. Characterization and anti-microbial susceptibility of gram-negative bacteria isolated from bloodstream infections of cancer patients on chemotherapy in Pakistan. Indian J Med Microbiol. 2009;27(4):341–347. | ||
Seid J, Asrat D. Occurrence of extended-spectrum beta-lactamase enzymes in clinical isolates of Klebsiella species from Harar region, eastern Ethiopia. Acta Trop. 2005;95(2):143–148. | ||
Ahmed OB, Omar AO, Asghar A, El hassan MM. Increasing prevalence of ESBL-producing Enterobacteriaceae in Sudan community patients with UTIs. Egypt Acad J Biol Sci. 2013;5(1):17–24. | ||
Al-Agamy MH, Shibl AM, Hafez MM, Al-Ahdal MN, Memish ZA, Khubnani H. Molecular characteristics of extended-spectrum β-lactamase-producing Escherichia coli in Riyadh: emergence of CTX-M-15-producing E. coli ST131. Ann Clin Microbiol Antimicrob. 2014;13:4. | ||
Mohanty S, Gaind R, Ranjan R, Deb M. Use of the cefepime-clavulanate ESBL Etest for detection of extended-spectrum beta-lactamases in AmpC co-producing bacteria. J Infect Dev Ctries. 2009;4(1):24–29. | ||
Afunwa RA, Odimegwu DC, Iroha RI, Esimone CO. Antimicrobial resistance status and prevalence rates of extended spectrum beta-lactamase (ESBL) producers isolated from a mixed human population. Bosn J Basic Med Sci. 2011;11(2):91–96. | ||
Levy Hara G, Gould I, Endimiani A, et al. Detection, treatment, and prevention of carbapenemase-producing Enterobacteriaceae: recommendations from an International Working Group. J Chemother. 2013;25(3):129–140. | ||
Kumar D, Singh AK, Ali MR, Chander Y. Antimicrobial susceptibility profile of extended spectrum β-lactamase (ESBL) producing Escherichia coli from various clinical samples. Infect Dis (Auckl). 2014;7:1–8. | ||
Bhaskar MM, Anand R, Harish BN. Prevalence of blaNDM-1 producing blood isolates of Escherichia coli, Klebsiella species and Enterobacter species in a tertiary care centre in South India. J Microbiol Res Rev. 2013;1(6):61–68. | ||
Goyal A, Prasad A, Ghoshal U, Prasad KN. Comparison of disk diffusion, disk potentiation & double disk synergy methods for detection of extended spectrum beta lactamases in Enterobacteriaceae. Indian J Med Res. 2008;128(2):209–211. | ||
Singh MR, Singh HL. Comparative evaluation of six phenotypic methods for detecting extended-spectrum beta-lactamase-producing Enterobacteriaceae. J Infect Dev Ctries. 2014;8(4):408–415. | ||
Yusuf I, Magashi AM, Firdausi FS, et al. Phenotypic detection of carbapenemase in members of Enterobacteriaceae in Kano, Nigeria. Int J Sci Technol. 2012;2(11):802–806. | ||
Cohen Stuart J, Leverstein-Van Hall MA; Dutch Working Party on the Detection of Highly Resistant Microorganisms. Guideline for phenotypic screening and confirmation of carbapenemases in Enterobacteriaceae. Int J Antimicrob Agents. 2010;36(3):205–210. | ||
Nair PK, Vaz MS. Prevalence of carbapenem resistant Enterobacteriaceae from a tertiary care hospital in Mumbai, India. J Microbiol Infect Dis. 2013;3(4):207–210. | ||
Cabrera E. Effect of distance between the Clavulanate-disk and β-lactam disks in the double-disk diffusion method for the detection of extended-spectrum β-lactamase (ESBL) production. Philipp J Sci. 2004;133(1):7–16. | ||
Prakash D, Saxena R. Prevalence and distribution of Gram negative bacteria of Enterobacteriaceae causing urinary tract infections among hospitalized patients. J Acad Indus Res. 2013;1(11):650–654. | ||
Ambretti S, Gaibani P, Berlingeri A, et al. Evaluation of phenotypic and genotypic approaches for the detection of class A and class B carbapenemases in Enterobacteriaceae. Microb Drug Resist. 2013;19(3):212–215. | ||
Ramana KV, Rao R, Sharada ChV, Kareem M, Reddy LR, Mani M. Modified Hodge test: a useful and the low-cost phenotypic method for detection of carbapenemase producers in Enterobacteriaceae members. J Nat Sci Biol Med. 2013;4(2):346–348. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.