")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Extended-Spectrum β-Lactamase-Producing Escherichia coli and Klebsiella pneumoniae: Risk Factors and Economic Burden Among Patients with Bloodstream Infections
Authors Chen J, Allel K, Zhuo C, Luo W, He N, Yang X, Guo Y, Wang J, Yao L, Li J, Lin Y, Tu R, Yakob L, Zhuo C
Received 6 December 2023
Accepted for publication 20 February 2024
Published 28 February 2024 Volume 2024:17 Pages 375—385
DOI https://doi.org/10.2147/RMHP.S453686
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Jiakang Chen,1,* Kasim Allel,2– 4,* Chuyue Zhuo,1,* Wenwei Luo,5 Nanhao He,1 Xu Yang,1 Yingyi Guo,1 Jiong Wang,1 Likang Yao,1 Jiahui Li,1 Yexin Lin,1 Ruiyang Tu,6 Laith Yakob,2,3 Chao Zhuo1
1State Key Laboratory of Respiratory Disease, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Disease Control, Faculty of Infectious & Tropical Diseases, London School of Hygiene & Tropical Medicine, London, UK; 3Antimicrobial Resistance Centre, London School of Hygiene & Tropical Medicine, London, UK; 4Institute for Global Health, University College London, London, UK; 5Department of Clinical Laboratory, the First Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, People’s Republic of China; 6Department of Science and Technology Studies, University College London, London, UK
*These authors contributed equally to this work
Correspondence: Chao Zhuo, State Key Laboratory of Respiratory Disease, the First Affiliated Hospital of Guangzhou Medical University, 151 Yanjiang Road, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Introduction: Although Extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae (ESBL-EK) significantly contribute to bloodstream infections, their economic repercussions remain largely unquantified.
Data Source and Methods: We performed a retrospective analysis of inpatients diagnosed with Escherichia coli or Klebsiella pneumoniae bacteremia in a tertiary hospital from January 2020 to December 2022 in Guangzhou, China. We employed the chi-square test to examine ESBL risk factors and utilized propensity score matching (PSM) to negate baseline confounding factors, assessing economic burden through disability-adjusted life years (DALYs), hospital costs and productivity losses. We employed mediation analysis to eliminate confounding factors and better identify ESBL sources of burden related.
Results: We found 166 ESBL-EC/KP BSI patients (52.2% of the total examined 318 patients). Post-PSM analysis revealed that ESBL-producing EC/KP will reduce the effectiveness of empirical medication by 19.8%, extend the total length of hospitalization by an average of 3 days, and increase the patient’s financial burden by US$2047. No significant disparity was found in overall mortality and mean DALYs between the groups. Mediation analysis showed that the link between ESBL and hospital costs is predominantly, if not entirely, influenced by the appropriateness of empirical antibiotic treatment and length of hospital stay.
Conclusion: Patients with BSI due to ESBL-producing ESBL-EK incur higher costs compared to those with non-ESBL-EK BSI. This cost disparity is rooted in varying rates of effective empirical antimicrobial therapy and differences in hospital stay durations. A nuanced approach, incorporating a thorough understanding of regional epidemiological trends and judicious antibiotic use, is crucial for mitigating the financial impact on patients.
Keywords: Escherichia coli, Klebsiella pneumoniae, bacteremia, ESBL, risk factors, medical costs
Introduction
Bloodstream infections (BSI) rank among the most prevalent and severe bacterial challenges in clinical medicine, significantly contributing to global disease burden.1–3 A European study estimated over 160,000 healthcare-associated (HA) primary BSIs in the European Union and the European Economic Area (EU/EEA) per year, leading to more than 24,000 fatalities.4,5 This burden is surpassed only by hospital-acquired pneumonia (HAP) among HA infections, presenting a formidable public health crisis. Furthermore, in 2019, antimicrobial resistance (AMR) was a complicating factor in approximately 1,500,000 BSI-related deaths worldwide, severely limiting treatment options and escalating the healthcare challenge.2
Klebsiella pneumoniae (KP) and Escherichia coli (EC) stand out as leading pathogens in bloodstream infections (BSI), with their global prevalence escalating notably in the past decade.3,5 In China, EC and KP are found in 35% of blood samples, with elevated presence of resistance mechanisms, including ESBL carrying rates (surpassing 40% among isolates).6 A Guangdong Province study highlighted that over 40% of pediatric EC and KP isolates are ESBL-producers, hinting at possibly higher current rates.7 ESBL genes, predominantly housed on mobile genetic elements (MGE) like plasmids, facilitate widespread transfer between EC and KP.8,9 These genes not only confer resistance to β-lactam antibiotics like cephalosporins but often coexist with multiple drug-resistance genes,10,11 complicating clinical treatment decisions and potentially escalating patient care costs.12
Literature has suggested differing attempts to quantify the economic and burden impact of ESBL on EC/KP-induced bacteremia, including the importance of study designs.13 Recent figures from the World Health Organization (WHO) Global Antimicrobial Resistance and Surveillance System (GLASS) showed that the proportion of BSIs caused by third-generation cephalosporins-resistant EC was 3-times higher in low- and middle-income countries (LMICs) compared to high-income countries, (58.3% and 17.53%, respectively).14 A meta-analysis showed that patients with antibiotic-resistant Gram-negative BSI in China had higher excess mortality, length of hospital stay (LOS) and intensive care unit (ICU) admissions compared with other LMICs.1 However, the study did not differentiate regions across China, which largely failed to account for differences in epidemiology and clinical impacts across China.15
Here, we explore the epidemiological status and disease burden, including economic impacts, of local carriers of ESBL bacteria through a single-center retrospective study.
Data Source and Methods
Patients and Sample Selection
We extracted EC and KP blood specimen data from the laboratory’s electronic system, adhering to specific criteria: (1) Positive blood cultures for EC or KP, (2) Clinical signs of BSI, and (3) Comprehensive clinical, microbiological, and cost data. Only the first bacteremia episode was considered for patients with multiple EC BSI cases during readmission or within six months post-discharge. Exclusions applied to individuals under 18, those with incomplete records, or patients discharged, deceased, or under palliative care on the day of blood collection. Patients were categorized into two groups: those with ESBL-positive EC or KP infections (ESBL group) and those with ESBL-negative infections (non-ESBL group)
Microbiological Tests
Clinical isolates were identified using the matrix-assisted laser desorption ionization time-of-flight microbial identification system (MALDI-TOF) (biomacimrieux, France). VITEK-2 COMPACT automatic microbial identification system (biomacimrieux, France) was used to perform drug susceptibility testing. The ESBL production of EC/KP was determined by Gram Negative Susceptibility Card VITEK 2 AST-334 (biomacimrieux, France). Drug susceptibility card implemented CLSI M100.16
Clinical and Sociodemographic Characteristics
We collated clinical characteristics and sociodemographics. We included hospital-acquired BSI, defined as positive blood cultures 48 hours after admission, whereas community-acquired referred within 48 hours of admission. BSI’s severity was assessed utilizing the APACHEII score;17 the SOFA score was used to describe organ dysfunction/failure in patients with sepsis;18 the overall systemic health status of patients was determined by the age adjusted Charlson Comorbidity Index (aCCI).19 Initial antibiotic therapy, considered as empiric treatment pending susceptibility outcomes, was deemed appropriate if it included at least one in-vitro sensitive antibiotic.20 Conversely, it was classified as inappropriate empirical antibiotic treatment (IEAT) if it failed to deliver any effective in-vitro active antimicrobial within 48 hours of diagnosing the infection. For ESBL-EK BSIs, oxyimino-β-lactams (eg, cefuroxime, cefotaxime, ceftriaxone, ceftazidime, cefepime, and aztreonam) were defined as inappropriate, regardless of in vitro susceptibility.21 Records of transfers in and out of the ICU and discharge records containing a summary of the patient’s condition at discharge were included. Patient’s age and sex were also included.
The clinical outcome of this study was in-hospital and 28-day post-discharge mortality in the ESBL and non-ESBL groups calculated as the total number of deaths/total number of cases.
Cost Analysis
Treatment costs were retrieved from the hospital information system. Direct and indirect costs (ie, lost productivity due to hospitalization and death) were analyzed. All costs were converted to USD (on average from 2020–2022, 1 USD = 6.69 RMB). The total direct expenses included medical care (treatment and nursing in the ward), treatment (surgical anesthesia, laboratory tests), rehabilitation, drugs (including antibacterial drugs), traditional Chinese medicine, diagnosis (pathology, microbiology, laboratory, imaging), disposable consumables, blood transfusion, and other expenses.
The indirect economic burden of EC bacteremia was analyzed through DALYs and human capital approaches. These methods impose an indirect economic burden equal to DALYs times gross-domestic product (GDP) per capita times productivity weights.22 Different age groups have different productivity weights, children aged 0–14 were assigned a weight of 0.15; 15–44 and 45–59 years old were assigned a weight of 0.75 and 0.80, respectively; and over 60 years old were assigned a weight of 0.1.23
BSI-associated DALYs were calculated by summing all years of life lost (YLLs) and years living with disabilities (YLDs).24 Other characteristics, such as life expectancy, age (standardized), time discount rate, and disability weights were included in the calculation of YLLs and YLDs.24 We followed Murray and Lopez et al to calculate DALYs.25,26 We used Brecht Devleesschauwer’s calculator27 to compute economic costs following WHO’s recommendations.27–29 Disability weights (D) were assigned in line with the acute infection’s severity, categorizing them into mild, moderate, and severe. These categories corresponded to disability weights of 0.006, 0.051, and 0.133, respectively. To calculate “L” (years lost due to death and years discounted due to disability), we used the Standard Expected Years of Life Lost (SEYLL) as a good approximation for life expectancy.30
Statistical Analyses
We investigated the link between various clinical factors and ESBL EC/KP, employing propensity score matching to balance baseline characteristics associated with ESBL. Subsequently, we analyzed the ESBL’s influence on health outcomes and burdens, adjusted for PSM. First we divided clinical and sociodemographic variables into three categories.①Variables preceding the BSI onset (such as hospitalization time before bacteremia or the aCCI) were analyzed utilizing the chi-square (χ²) test to confirm the risk factors of ESBL infection, and at the same time, the difference between groups was excluded when calculating the economic cost.② Variables following the BSI onset, but its impact on clinical outcome of patient was independent of ESBL (such as SOFA score). These variables were not included in the risk factor analysis of ESBL in the study, but they were used as confounding factors to analyze the impact of ESBL on economic burden; excluding differences between groups due to the use of propensity score matching (PSM). ③Factors influenced by ESBL, like initial antimicrobial susceptibility, are not adjusted for economic assessments using PSM, and their mediating impact was verified.31
We computed descriptive statistics across all variables, and reported the mean, standard deviation or median (interquartile range [IQR]) for continuous variables, and proportions (%) for categorical variables. We used t-test (variables with normal distribution) and Mann–Whitney U-test (variables with non-normal distribution) to assess difference in means across ESBL and non-ESBL groups. Chi-square (χ2) test was used for categorical variables. We computed a PSM-corrected logistic regression using a backward stepwise method. We matched individuals from the ESBL and non-ESBL groups utilizing a caliper with a match tolerance equal to 0.02. Mediating effects were confirmed by Baron and Kenny’s steps for mediation analysis between ESBL and hospitalization costs via the mediating impact of LOS and ineffective empirical antimicrobial therapy.32,33 We employed a holistic and comprehensive approach considering LOS and IEAT as simultaneous mediators of the association between ESBL infections and hospitalization costs. We utilized structural equation modeling (SEM) through the “lavaan” package (in the R software) to account for the correlations and interactions between mediators and ESBL and economic costs using linear regressions. Bootstrapped standard errors with 1000 replications. P-value of less than 0.05 was considered statistically significant. Statistical analyses were performed in R version 4.3.1 and SPSS version 26.0 (SPSS, Chicago, IL, USA).
Results
Analytical Sample
From January 2020 to December 2022, we identified a total of 372 EC and KP isolates from 367 patients with BSIs. After removing duplicates and missing data, we included 318 EC and KP unique isolates. We found 152 non-ESBL-EC/KP BSI patients (47.8%) and 166 (52.2%) ESBL-EC/KP BSI patients.
Descriptive Statistics Before Matching and by ESBL Group
Of the 318 patients, 179 were male, and the mean ages for ESBL-BSI and non-ESBL-BSI were 56.5 and 63 years, respectively (p=0.064). There was no statistically significant difference in strain distribution between the two groups in this study (p=0.407). The ESBL detection rates of EC and KP were 54.0% and 49.1%, respectively. The organ transplant rate (non-ESBL=1.3% versus ESBL=6%, p=0.028) and ICU admission rate (non-ESBL=7.2% versus ESBL=19.9%, p=0.001) were higher in the ESBL group before onset than in the non-ESBL group, but nosocomial infection rates were not significantly different between the two groups (non-ESBL=40.1% versus ESBL=35.5%, p=0.399).
The most common comorbidities in ESBL group and non-ESBL group were malignant tumor (non-ESBL=36.2% versus ESBL=26.5%), hepatobiliary disease (non-ESBL=14.5% versus ESBL=22.9%) and diabetes (non-ESBL=14.5% versus ESBL=16.9%). Among comorbidities, only moderate to severe nephropathy had a statistically significant difference between groups (6.6% for non-ESBL versus 15.7% for ESBL, p=0.011). Notably, while there were partial differences in comorbidity distribution between the two groups of patients, there was no statistically significant differences in quantified aCCI (non-ESBL=4(2,6) versus ESBL=4(3,6), p=0.232). Correspondingly, the APACHEII (non-ESBL=10(7,13) versus ESBL=12(7,19), p=0.001) score and SOFA score (non-ESBL=1(0,4) versus ESBL=3(0,7), p=0.004) reflecting the patient’s basic condition and the severity of sepsis in the ESBL group were higher than those in the non-ESBL group.
Although more carbapenems were used in the ESBL group (non-ESBL=41.4% versus ESBL=53%, p=0.039), the effective rate of empiric antibacterial therapy was lower than that of the non-ESBL group (non-ESBL=80.3% versus ESBL=58.4%, p<0.001), and the total mortality rate (non-ESBL=17.8% versus ESBL=27.1%, p=0.047) was higher than that of the non-ESBL group (Table 1).
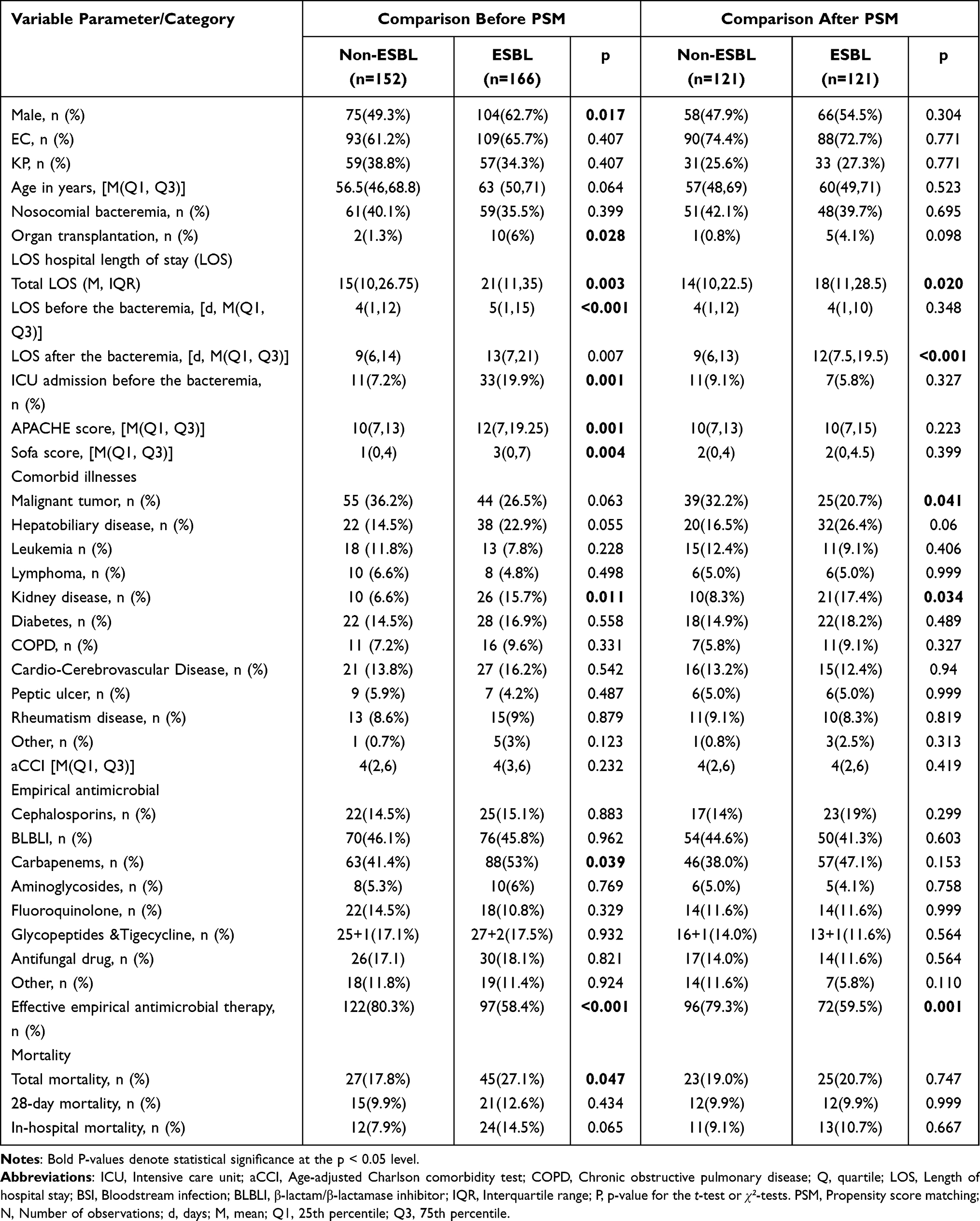 |
Table 1 Characteristics of Patients with EC/KP BSIs, Stratified by ESBL Production |
Estimation of the Propensity Score
The raw and PSM-adjusted ESBL+ and non-ESBL proportions are depicted in Table 1. We observed no significant difference in clinical characteristics considered as confounding factors between the two groups (all p>0.05), including gender, age, bacterial species, hospital infection rate, hospitalization time before infection, organ transplantation during hospitalization, empirical drug category, APACHE II score, SOFA score, and aCCI. We found similar distributions across ESBL proportions after correcting the estimates utilizing the PSM (Table 1).
Association between ESBL+ and outcome variables related to clinical burden
We noticed that after removing the interference of confounding factors, the ESBL group still had a lower rate of effective empirical antimicrobial therapy than the non-ESBL group (non-ESBL=79.3% versus ESBL=59.5%, p=0.001), longer total hospitalization time (ESBL=18(11, 28.5) versus non-ESBL=14(10, 22.5), p=0.02) and longer post-infection hospitalization time (non-ESBL=9(6, 13) versus ESBL=12(7.5, 19.5), p<0.001), but there was no significant difference in the overall mortality rate between non-ESBL group and ESBL group (non-ESBL=19.0% versus ESBL=20.7%, p=0.747) (Table 1).
Economic Costs
After PSM, the median total hospitalization cost was $5638 for non-ESBL patients and $7685 for ESBL patients (p=0.014) (Table 2). In the two groups, the cost of antibiotics accounted for 27.3% and 39.0% of the drug, respectively (p=0.002). The median cost of antibiotics during hospitalization was $400 for non-ESBL-EC BSI patients and $834 for ESBL-EC BSI patients, p<0.001) (Table 2 and Figure 1). In the non-ESBL-EC group after PSM matching, patients lost an average of 1.84 DALYs, whereas it was 2.12 among ESBL-EC group (mean test p=0.098). There was no significant difference in mean indirect loss in the ESBL-EC group compared to the non-ESBL-EC group.
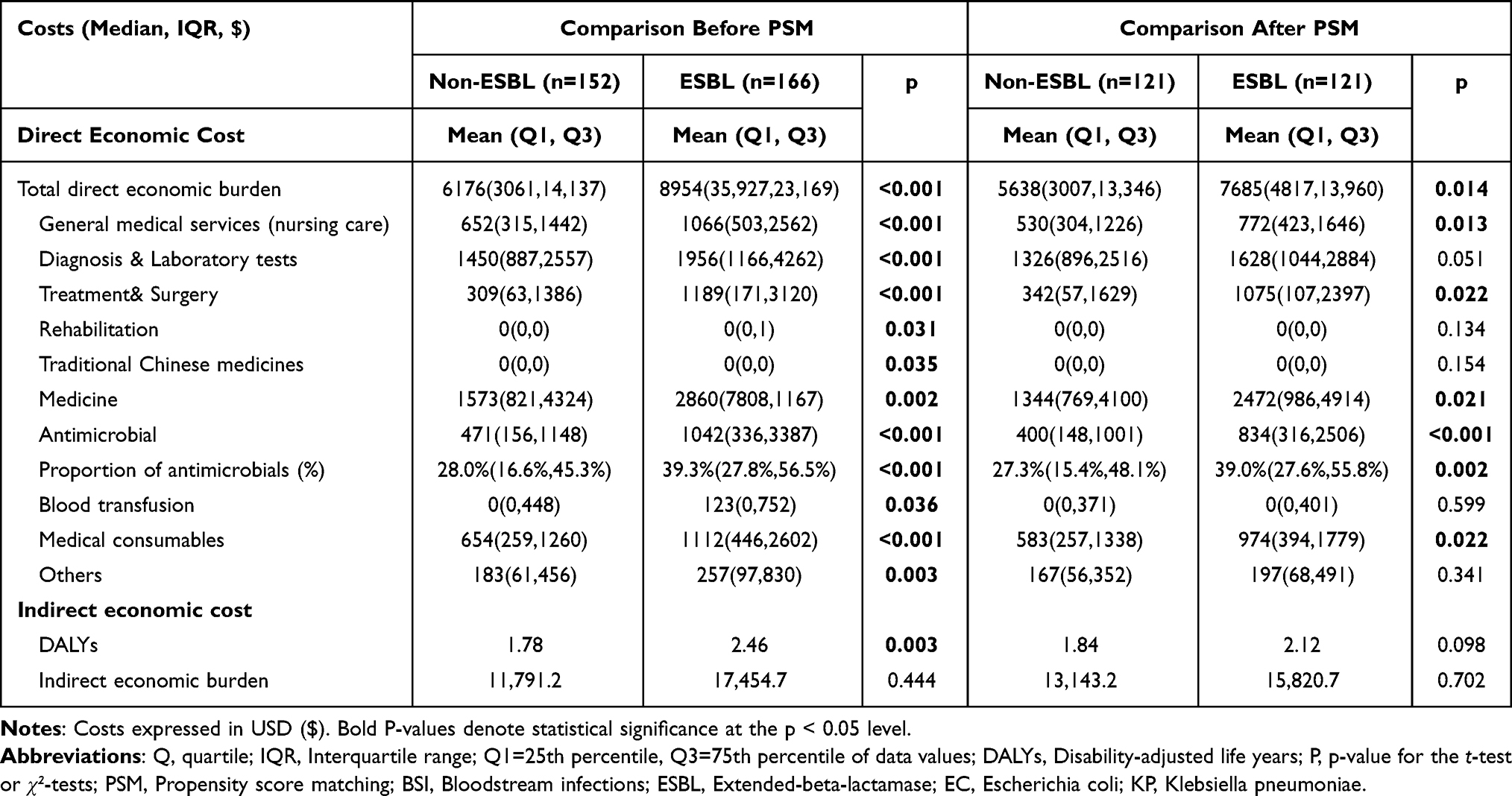 |
Table 2 Costs of Patients with EC/KP BSIs, Stratified by ESBL Production |
 |
Figure 1 Economic costs by ESBL group before (A) and after (B) adjusting for PSM results. Abbreviations: ESBL, Extended Spectrum Beta-lactamase producing; PSM, Propensity score matching. |
Mediation Analyses
ESBL was positively associated with IEAT (Estimate = 0.215, SE=, p<0.05) and LOS (Estimate = 0.151, SE=0.05, p<0.05) (Table 3). However, ESBL did not show a direct impact on economic costs (−0.03, SE=, p>0.05), whereby IEAT and LOS were significantly and directly associated with economic costs (Estimate= 0.13, SE=0.06, p-value=0.037, Estimate= 0.62, SE=0.14, p-value<0.001, respectively). All estimated variances for the residuals (errors) of the three models (a, b, and c) are significant, indicating variability around the predicted values of these variables (Table 3, variance). The total indirect impact of ESBL on cost was significant (Estimate= 0.12, SE=0.06, p-value<0.027), with marginal indirect impacts from IEAT and more significant impacts via LOS (Table 3 and Figure 2, impacts of indirect effects). The total indirect effect impact was significant suggesting that the relationship between ESBL and cost is largely or fully mediated by IEAT and LOS.
 |
Table 3 Mediation Effect Analysis Results |
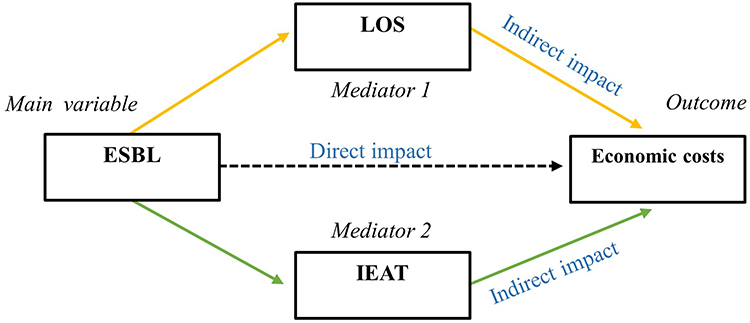 |
Figure 2 Diagram of the mediation effects (LOS and IEAT) between ESBL and economic costs. Abbreviations: IEAT, Ineffective empirical antibiotic treatment; LOS, Length of hospital stay; ESBL, Extended Spectrum Beta-Lactamase. |
Discussion
Our findings align with the China Antimicrobial Surveillance Network (CHINET)34 regarding ESBL positivity in EC. However, the ESBL rate in Klebsiella pneumoniae (KP) among adults exceeded our previous provincial study (49.1% versus 28.7%).7 Compared to the non-ESBL group, patients with ESBL-related BSI faced higher empirical treatment failure, mortality rates, extended hospital stays, and increased medical expenses. Significant disparities were noted in effective empirical therapy, hospitalization duration, and costs between the ESBL and non-ESBL groups if cofounding factors were excluded.
We included DALYs to calculate the overall burden on patients and society, which indicated reduced productivity due to disease.35 Similar to most studies included in a recent systematic literature review written by Zhen X et al,13 we found that patients with ESBL BSIs had longer hospital stays and higher financial burdens. We found a 33.3% increase in median post-bacteremia LOS (from 9 days to 12 days), a 28.6% increase in total LOS (from 14 days to 18 days), and a 36.3% increase in hospital costs (an additional $2047 per patient) in the post-PSM ESBL group.
The impact of initial treatment efficacy and antibiotic costs on the total direct burden remains debated, potentially due to regional variations in medical services and drug pricing.13 Our study revealed that ESBL significantly affected IEAT and LOS, which in turn significantly impacted hospitalization expenses. This suggests that targeting ESBL could indirectly reduce costs by altering IEAT and LOS. Investigating these mediating factors could further elucidate how ESBL influences hospitalization costs. In our analysis, the median difference in antimicrobial expenditure represented 21.2% (434/2037) of the total median hospitalization cost difference. Notably, the ESBL group incurred higher antimicrobial costs, contributing substantially to overall Western medicine expenses (27.3% versus 39%, p = 0.002), indicating that the elevated drug costs associated with ESBL-BSI also escalated overall hospitalization expenses.
In our study, we noted that the average disability years (1.84–2.12 years) and the average hospitalization duration (14–18 days) contributed to less than 1% of the YLDs within the DALYs after disease weighting. This is expected due to the brief duration of bloodstream infections and their high mortality rate. We propose that for researchers lacking comprehensive data, relying solely on YLDs, in the absence of long-term sequelae associated with bacteremia, can adequately represent the disease burden in adults with acute bloodstream infections.
Our analysis revealed that carbapenem use by clinicians was influenced by factors other than ESBL presence alone (non-ESBL=45.4% versus ESBL=53%, p=0.039). However, this difference became statistically insignificant (p=0.153) after adjusting for SOFA and APACHE II scores. This suggests clinicians might prioritize clinical severity over ESBL-related risk factors when choosing treatments before receiving drug sensitivity reports. A notable finding was the lack of recorded antibacterial drug use information in the six months preceding admission in most electronic medical records. Given that non-β-lactam antibiotic use is also a reported risk factor for ESBL, this omission presents a significant concern.36 Therefore, we advocate for detailed documentation of all antimicrobial drugs during admission consultations to enhance the precision of antimicrobial stewardship.
In previous studies, nosocomial infection was usually a high-risk factor for ESBL-producing bacterial infection.37 In this study, despite the longer LOS in the ESBL group pre-PSM the nosocomial infection rates between the groups showed no significant difference (non-ESBL=40.1% versus ESBL= 35.5%, p=0.399). This indicates a widespread community transmission of blaESBL in the region. Given the substantial local ESBL prevalence, clinicians are advised to exercise caution in prescribing third-generation cephalosporins until definitive drug susceptibility results are obtained.7,34 Studies in China indicate that using antimicrobials effective against ESBL-producing bacteria as empirical therapy can enhance cure rates and decrease both direct and indirect societal costs.30 Clinics must, therefore, weigh individual patient needs against broader societal considerations. We advocate for a more rigorous implementation of the WHO’s ESBL detection tricycle plan and the AWaRe tool, along with the establishment of multi-dimensional molecular epidemiological surveillance and robust antimicrobial stewardship programs, to address the complex, multidisciplinary challenge posed by antimicrobial resistance.38–41
Despite controlling for various confounders, potential selection biases in our study cannot be entirely ruled out. To optimize patient inclusion in the PSM, we did not factor in individual comorbidities, given the varying weights assigned to diseases in the Charlson score. While previous research suggests a link between ESBL plasmids and certain virulence factors,42 our study focused solely on the impact of drug resistance genes. We mitigated potential biases from virulence factors by integrating metrics like the SOFA score into our PSM criteria.
In conclusion, our findings affirm that BSIs caused by ESBL-producing EC/KP diminish the effectiveness of empirical treatments, extend hospitalization, and heighten financial strain on patients. The study underscores the critical need for accurate ESBL risk assessment and precise antibiotic utilization to alleviate patient burdens. Ultimately, ongoing epidemiological monitoring and risk evaluation of antimicrobial resistance are essential for both clinical management and effective antimicrobial stewardship.
Data Sharing Statement
The datasets used are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Our study complied with the Declaration of Helsinki. All admitted patients have signed a consent form allowing review of their medical records, and all patients’ personal information has been maintained with confidentiality. Our study was approved by the First Affiliated Hospital of Guangzhou Medical University Ethics Committee (approval number: ES-2023-057-01).
Acknowledgments
We acknowledge Prof Lixiong Yang, School of Labor and Human Resources, Renmin University of China and Xiaoyi Fang, Institute of Population research Peking University for their invaluable help and expertise. The study has been posted as a preprint on Research Square:https://www.researchsquare.com/article/rs-3432080/v1
Funding
This research was funded by the Special Foundation for National Science and Technology Basic Research Program of China 2019FY101200. The funders had no role in the design, conduct, analysis or interpretation of the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Allel K, Stone J, Undurraga EA, et al. The impact of inpatient bloodstream infections caused by antibiotic-resistant bacteria in low- and middle-income countries: a systematic review and meta-analysis. PLoS Med. 2023;20(6):e1004199. doi:10.1371/journal.pmed.1004199
2. Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Ikuta KS, Swetschinski LR, Robles Aguilar G, GBD 2019 Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2022;400(10369):2221–2248. doi:10.1016/S0140-6736(22)02185-7
4. Cassini A, Plachouras D, Eckmanns T, et al. Burden of Six Healthcare-Associated Infections on European Population Health: estimating Incidence-Based Disability-Adjusted Life Years through a Population Prevalence-Based Modelling Study. PLoS Med. 2016;13(10):e1002150. doi:10.1371/journal.pmed.1002150
5. Tabah A, Buetti N, Staiquly Q, et al. Epidemiology and outcomes of hospital-acquired bloodstream infections in intensive care unit patients: the EUROBACT-2 international cohort study. Intensive Care Med. 2023;49(2):178–190. doi:10.1007/s00134-022-06944-2
6. Chen Y, Ji J, Ying C, et al. Blood bacterial resistant investigation collaborative system (BRICS) report: a national surveillance in China from 2014 to 2019. Antimicrob Resist Infect Control. 2022;11(1):17. doi:10.1186/s13756-022-01055-5
7. Zhuo CY, Guo YY, Liu NJ, et al. 广东地区血液内科血流感染的病原菌流行病学分析 [Epidemiological analysis of pathogens causing bloodstream infections in department of hematology in Guangdong Province]. Zhonghua Xue Ye Xue Za Zhi. 2020;41(12):996–1001. Chinese. doi:10.3760/cma.j.issn.0253-2727.2020.12.005
8. Partridge SR, Kwong SM, Firth N, Jensen SO. Mobile Genetic Elements Associated with Antimicrobial Resistance. Clin Microbiol Rev. 2018;31(4):e00088–17. doi:10.1128/CMR.00088-17
9. Lerminiaux NA, Cameron ADS. Horizontal transfer of antibiotic resistance genes in clinical environments. Can J Microbiol. 2019;65(1):34–44. doi:10.1139/cjm-2018-0275
10. Schwaber MJ, Navon-Venezia S, Schwartz D, Carmeli Y. High levels of antimicrobial coresistance among extended-spectrum-beta-lactamase-producing Enterobacteriaceae. Antimicrob Agents Chemother. 2005;49(5):2137–2139. doi:10.1128/AAC.49.5.2137-2139.2005
11. Mammeri H, Van De Loo M, Poirel L, Martinez-Martinez L, Nordmann P. Emergence of plasmid-mediated quinolone resistance in Escherichia coli in Europe. Antimicrob Agents Chemother. 2005;49(1):71–76. doi:10.1128/AAC.49.1.71-76.2005
12. Gandra S, Barter DM, Laxminarayan R. Economic burden of antibiotic resistance: how much do we really know? Clin Microbiol Infect. 2014;20(10):973–980. doi:10.1111/1469-0691.12798
13. Zhen X, Lundborg CS, Sun X, Hu X, Dong H. Economic burden of antibiotic resistance in ESKAPE organisms: a systematic review. Antimicrob Resist Infect Control. 2019;8:137. doi:10.1186/s13756-019-0590-7
14. World Health Organization. Global Antimicrobial Resistance and Use Surveillance System (GLASS) Report; 2021.
15. Hu B, Ye H, Xu Y, et al. Clinical and economic outcomes associated with community-acquired intra-abdominal infections caused by extended spectrum beta-lactamase (ESBL) producing bacteria in China. Curr Med Res Opin. 2010;26(6):1443–1449. doi:10.1185/03007991003769068
16. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing.
17. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
18. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):801–10. doi:10.1001/jama.2016.0287
19. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
20. Hill PC, Birch M, Chambers S, et al. Prospective study of 424 cases of Staphylococcus aureus bacteraemia: determination of factors affecting incidence and mortality. Intern Med J. 2001;31(2):97–103. doi:10.1111/j.1444-0903.2001.00029.x
21. Apisarnthanarak A, Kiratisin P, Mundy LM. Predictors of mortality from community-onset bloodstream infections due to extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella pneumoniae. Infect Control Hosp Epidemiol. 2008;29(7):671–674. doi:10.1086/588082
22. National bureau of statistics of china. China: china’s Gross Domestic Product (GDP). Available from: http://data.stats.gov.cn/search.htm?s=GDP.
23. Barnum H. Evaluating healthy days of life gained from health projects. Soc Sci Med. 1987;24(10):833–841. doi:10.1016/0277-9536(87)90184-5
24. Murray CJ. Quantifying the burden of disease: the technical basis for disability-adjusted life years. Bull World Health Organ. 1994;72(3):429–445.
25. The Global Burden of Disease: acomprehensive Assessment of Mortality and Disability from Dis-Eases, Injuries, and Risk Factors in 1990 and Projected to 2020. Murray CJL, Lopez AD, editors. TheGlobal Burden of Disease and Injury Series. Vol. 1: Harvard University Press, for Harvard School of PublicHealth on behalf of the World Health Organisation and TheWorld Bank; Boston, MA; 1996b.
26. Lopez AD, Mathers CD, Ezzati M, et al., editors. Global Burden of Disease and Risk Factors. Washington (DC): The International Bank for Reconstruction and Development / The World Bank; 2006. Available from: https://www.ncbi.nlm.nih.gov/books/NBK11812/.
27. Center for the Evaluation of Value and Risk in Health. The Cost-Effectiveness Analysis Registry [Internet]. (Boston), Institute for Clinical Research and Health Policy Studies, Tufts Medical Center. Available from: www.cearegistry.org.
28. Devleesschauwer B, Havelaar AH, Maertens de Noordhout C, et al. Calculating disability-adjusted life years to quantify burden of disease. Int J Public Health. 2014;59(3):565–569. doi:10.1007/s00038-014-0552-z
29. Fox-Rushby JA, Hanson K. Calculating and presenting disability adjusted life years (DALYs) in cost-effectiveness analysis. Health Policy Plan. 2001;16(3):326–331. doi:10.1093/heapol/16.3.326
30. Wang Y, Xiao T, Zhu Y, et al. Economic Burden of Patients with Bloodstream Infections Caused by Extended-Spectrum β-Lactamase-Producing Escherichia coli. Infect Drug Resist. 2020;13:3583–3592. doi:10.2147/IDR.S271230
31. Caliendo M, Kopeinig S. Some Practical Guidance For The Implementation Of Propensity Score Matching. J Econ Surv. 2008;22(1):31–72. doi:10.1111/j.1467-6419.2007.00527.x
32. Bommae K. 2016. “Introduction to Mediation Analysis.” UVA Library StatLab. Available from: https://library.virginia.edu/data/articles/introduction-to-mediation-analysis/.
33. Sobel ME. D irect and indirect effects in linear structural equation mode ls. In: Long JS, editor. Common Problem s /Proper Solutions. Beverly H ills, CA: Sage; 1988:46–64.
34. China Antimicrobial Surveillance Network Available from: http://www.chinets.com/Chinet.
35. Tumbarello M, Spanu T, Di Bidino R, et al. Costs of bloodstream infections caused by Escherichia coli and influence of extended-spectrum-beta-lactamase production and inadequate initial antibiotic therapy. Antimicrob Agents Chemother. 2010;54(10):4085–4091. doi:10.1128/AAC.00143-10
36. MacVane SH, Tuttle LO, Nicolau DP. Impact of extended-spectrum β-lactamase-producing organisms on clinical and economic outcomes in patients with urinary tract infection. J Hosp Med. 2014;9(4):232–238. doi:10.1002/jhm.2157
37. Quan J, Zhao D, Liu L, et al. High prevalence of ESBL-producing Escherichia coli and Klebsiella pneumoniae in community-onset bloodstream infections in China. J Antimicrob Chemother. 2017;72(1):273–280. doi:10.1093/jac/dkw372
38. World Health Organization. (2021). WHO integrated global surveillance on ESBL-producing E. coli using a “One Health” approach: implementation and opportunities. World Health Organization. Available from: https://apps.who.int/iris/handle/10665/340079.
39. World Health Organization. (2019). AWaRe – a new WHO tool to help countries improve antibiotic treatment, increase access and reduce resistance. Available from: https://adoptaware.org.
40. Mahmoudi L, Sepasian A, Firouzabadi D, Akbari A. The Impact of an Antibiotic Stewardship Program on the Consumption of Specific Antimicrobials and Their Cost Burden: a Hospital-wide Intervention. Risk Manag Healthc Policy. 2020;13:1701–1709. doi:10.2147/RMHP.S265407
41. Nguyen-Thi HY, Nguyen DA, Huynh PT, Le NDT. Impact of Antimicrobial Stewardship Program on Vancomycin Usage: costs and Outcomes at Hospital for Tropical Diseases in Ho Chi Minh City. Vietnam Risk Manag Healthc Policy. 2021;14:2637–2646. doi:10.2147/RMHP.S307744
42. Karisik E, Ellington MJ, Pike R, Warren RE, Livermore DM, Woodford N. Molecular characterization of plasmids encoding CTX-M-15 beta-lactamases from Escherichia coli strains in the United Kingdom. J Antimicrob Chemother. 2006;58(3):665–668. doi:10.1093/jac/dkl309
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.