")
Back to Journals » Clinical Ophthalmology » Volume 13
Extended depth of focus lens implantation after radial keratotomy
Authors Baartman BJ, Karpuk K, Eichhorn B, Ferguson TJ , Sudhagoni RG, Berdahl JP , Thompson VM
Received 13 March 2019
Accepted for publication 14 June 2019
Published 30 July 2019 Volume 2019:13 Pages 1401—1408
DOI https://doi.org/10.2147/OPTH.S208550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Brandon J Baartman,1 Kayla Karpuk,1 Bradley Eichhorn,2 Tanner J Ferguson,2 Ramu G Sudhagoni,3 John P Berdahl,1 Vance M Thompson1
1Vance Thompson Vision, Sioux Falls, SD, USA; 2University of South Dakota School of Medicine, Vermillion, SD, USA; 3Public Health Department, School of Health Sciences, University of South Dakota, Vermillion, SD, USA
Purpose: To identify the visual performance of radial keratotomy (RK) patients that have undergone cataract surgery with implantation of an extended depth of focus (EDOF) intraocular lens (IOL).
Design: Retrospective chart review with questionnaire.
Methods: Medical charts of patients with a history of RK that had undergone phacoemulsification with implantation of the Tecnis Symfony IOL (J&J Vision) were reviewed. Data collected included preoperative demographics, number of RK incisions, pupil size, and preoperative visual acuity and manifest refraction. Primary outcome measures of the study included postoperative uncorrected distance visual acuity (UCVA) and manifest refraction spherical equivalent (SE) at each follow-up visit. Secondary outcomes included results from a telephone questionnaire assessing visual performance and satisfaction.
Results: Twenty-four eyes of 12 patients were included. UCVA improved from an average Snellen equivalent 20/73 preoperatively to 20/33 at an average final follow-up of 6 months (P=0.0011), while average manifest SE improved from +1.68 D to −0.18 D (P<0.0001). At final follow-up, 15 of 24 eyes (62.5%) were at or within 0.5 D of target refraction, while 20 of 24 eyes (83.3%) were at or within 1.0 D. In total, 79% of eyes (19 of 24) had UCVA of 20/40 or better at distance. In the survey, 78% of patients reported satisfaction with their vision after surgery and 44% of patients reported being spectacle free for all tasks.
Conclusions: An EDOF lens implant can produce good visual outcomes and satisfaction in patients with a history of RK.
Keywords: radial keratotomy, cataract, intraocular lens
A Letter to the Editor has been published for this article.
Introduction
Radial keratotomy (RK) was once the most common corneal refractive surgery performed in the United States. While it has been largely abandoned due to the induction of irregular astigmatism and fluctuation in the cornea’s refractive power, many patients that have undergone RK are beginning to age into the cataract surgery population.
Patients with prior RK present unique challenges to the cataract surgeon. These include preoperative challenges such as accurate biometry for intraocular lens (IOL) implantation,1 intraoperative challenges with wound placement and possibility of incision dehiscence,2,3 and postoperative fluctuation in refractive error.4 Much as with prior keratoablative refractive surgeries, errors in IOL calculation may occur with current-day formulas which make incorrect assumptions about anterior and posterior corneal curvature.5 Due to the cornea’s acquired instability in refractive power, the refractive error of the post-RK eye may fluctuate significantly after cataract surgery despite careful preoperative planning and IOL selection and consequently produce considerable patient dissatisfaction.
Many surgeons view post-RK cataracts as challenging and avoid the use of any sort of advanced optics IOL options (toric or multifocal). Moreover, the literature studying advanced IOL options in this population is scarce. However, post-refractive patients may carry higher expectations and be motivated to reduce spectacle dependence after cataract surgery. To date, only 5 patient cases have been described regarding use of multifocal lenses in patients with prior RK (3 patients with refractive multifocal optic, 2 patients with diffractive multifocal optic),6–8 and no summative objective or subjective data are available. The intent of the current study is to report visual performance and subjective satisfaction in patients with prior RK that have undergone cataract surgery with implantation of an extended depth of focus (EDOF) IOL.
Methods
This study was a retrospective chart review of patients having undergone cataract surgery at Vance Thompson Vision, Sioux Falls, SD, from December 2016 to December 2017. The study was approved by the Institutional Review Board (IRB) of the University of South Dakota (Vermillion, SD). All preoperative IOL planning was performed using the Holladay IOL Consultant Professional software, utilizing keratometry powers obtained from Lenstar (Haag-Streit, Switzerland) measurements. Intraoperative aberrometry was used in all cases, and spherical lens power was adjusted when indicated at surgeon discretion. Surgeries were performed by one of the 3 surgeons (BJB, JPB, VMT), and all patients received the following standard postoperative medication regimen: intraoperative injection of antibiotic, steroid, and non-steroidal anti-inflammatory medication (dexamethasone, moxifloxacin, ketorolac) and daily use of a combination drop (eg, prednisolone, gatifloxacin, nepafenac).
Patient charts were selected by querying the medical record database for CPT codes for cataract surgery or complex cataract surgery and had documentation of prior RK. These charts were then reviewed for type of lens implanted at time of surgery. All patients having undergone cataract surgery with a history of prior RK with Tecnis Symfony lens (Johnson & Johnson Vision, Santa Ana, CA, USA) implanted in at least one eye were included in the study. Any patient having had lens implantation of other lenses (monofocal, toric, or other multifocal) was excluded. Other exclusions were patients with concomitant clinically significant corneal scarring, macular disease (eg, age-related macular degeneration), glaucoma, or diabetic retinopathy.
Data collected from qualifying patient charts included demographics and ocular history (age, gender, date of prior RK, number of RK incisions, ocular dominance, prior excimer ablation procedure), as well as scotopic pupil size, preoperative best spectacle-corrected visual acuity (BSCVA), and manifest refraction with spherical equivalent (SE). All patients underwent corneal wavefront analysis as part of the cataract preoperative workup using the NIDEK OPD-III scanner (NIDEK CO., Gamagori, Japan). Data obtained included mesopic pupil size and corneal aberrometry such as spherical aberration, coma, and total higher-order aberrations (HOA).
Preoperative planning such as IOL power selection, targeted postoperative refraction with corresponding IOL formula and intraoperative lens power selection based on intraoperative aberrometry were recorded. Primary outcomes included uncorrected distance visual acuity (UCVA), manifest refraction and SE, and near visual acuity when recorded in the medical record. Visual acuity data were recorded in Snellen notation and converted to logMAR notation for statistical analysis. Near vision was recorded as documented in the medical chart in Jaeger notation.9 Data were organized by time to follow-up after surgery, including day 1, week 1, month 1, month 3, and final follow-up.
Secondary outcomes included results from a questionnaire administered at the time of chart review to assess patient visual performance and satisfaction after surgery. The questionnaire was adapted from Maurino et al,10 and included elements of visual functioning, spectacle independence, and dysphotopsia screening. All questionnaires were administered via telephone by a single author (BE) using a standardized telephone script approved by the IRB. All patients were made aware of the medical chart review and consented for involvement in the questionnaire, and given the chance to decline or postpone the questionnaire to a later date. Numerical values were assigned to responses, with highest values assigned to best possible result for simplicity. For the section assessing visual function, patients were asked to rate how much difficulty they had performing a variety of tasks, with a score of 0 being “very great difficulty,” 1 being “great difficulty,” 2 being “some difficulty,” and a score of 3 being “no difficulty.” For the spectacle dependence section of the questionnaire, patients were asked to assign a numerical value to how often they required spectacles for various tasks, with 0 being “always,” 1 being “sometimes,” and 3 being “never.” Dysphotopsia ratings were assessed on a scale from 0 being “debilitating,” 1 being “annoying,” 2 being “barely noticeable,” and 3 being “none.” Lastly, overall satisfaction was assessed, with a score of 1 being “very dissatisfied,” 2 being “fairly dissatisfied,” 3 being “fairly satisfied,” and 4 being “very satisfied” with vision after surgery.
Statistical analysis
Mean baseline and final follow-up UCVA and SE were compared using a paired T-test procedure. A one-way repeated measures of ANOVA procedure was used to compare the mean simultaneously at several visits within the group. A chi-square test used to test equality of proportions. Significant level considered at 0.05. All data analyses were carried out using SAS 9.14 (Cary, NC, USA).
Results
Twenty-four eyes of 12 patients were included in the chart review after exclusions. Patient demographic and preoperative refractive data are listed in Table 1. Refractive target was set at plano in 15 eyes (62%) and myopic in 9 eyes (38%; range −0.25 to −1.00 D). All cases had the Tecnis Symfony lens implanted after cataract extraction by phacoemulsification. The average-implanted IOL power was 23.5 D (range 20.5–28.0 D; ZXR00 in 23 cases, ZXT300 in 1 case). The IOL power was changed based on intraoperative aberrometry in 10 cases (42%). No cases of intraoperative wound dehiscence or other complication occurred.
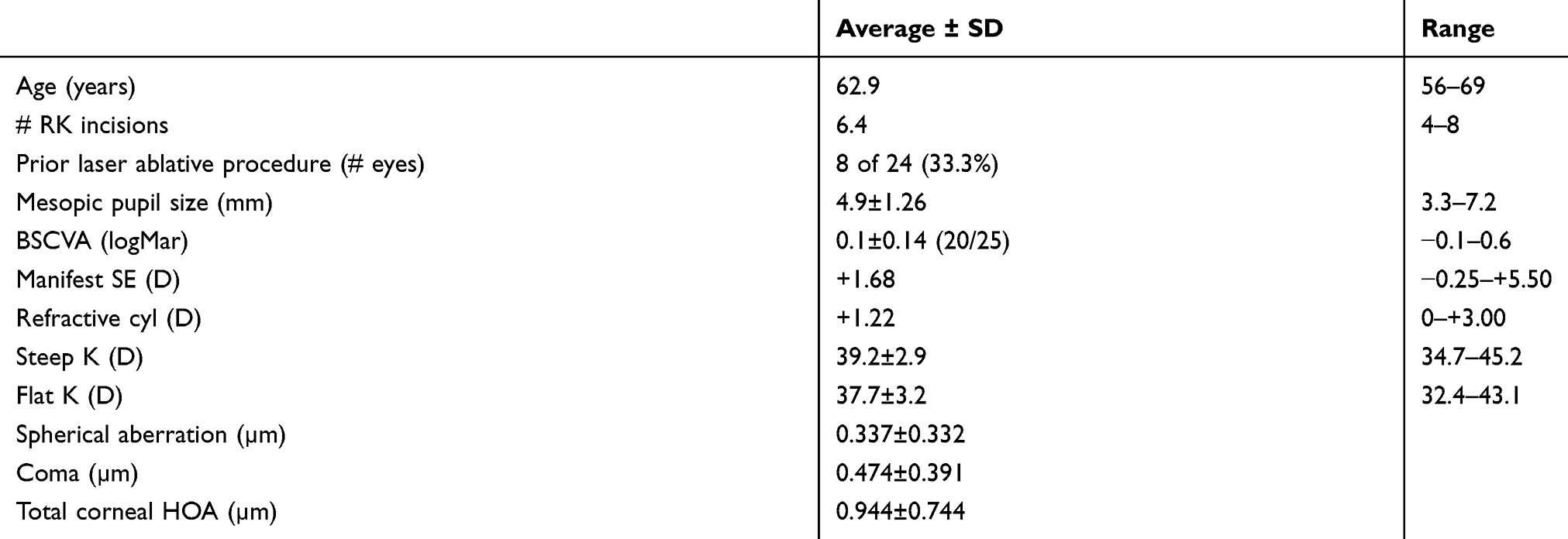 |
Table 1 Preoperative patient demographics and characteristics |
The primary outcome measures of the study were UCVA and SE at follow-up after surgery. At baseline, the mean UCVA was 0.56±0.35 (20/70). At final collected follow-up, the mean UCVA had significantly improved to 0.22±0.17 (20/33; P=0.0011) as seen in Figure 1. Average SE on manifest refraction improved from +1.68 D preoperatively to −0.18 D at time of final follow-up (P<0.0001). The percentage of patients with UCVA at or better than 20/40 at preoperative evaluation was 35% (7 of 20); this value at postoperative day 1, week 1, month 1, and month 3 was 50% (9 of 18), 78% (18 of 23), 71% (17 of 24) and 75% (12 of 16), respectively. By final follow-up (average 5 months; range 1–11 months), the percentage of patients with UCVA 20/40 or better had improved to 79% (19 of 24), which was statistically significant (P=0.0083). A summary of the visual outcomes and refractive data observed over the course of follow-up period can be seen in Table 2.
 |
Table 2 Illustrates uncorrected visual acuity, SE, and proportions of patients 20/40 or better at various time points pre- and postoperatively. *Indicates level of significance |
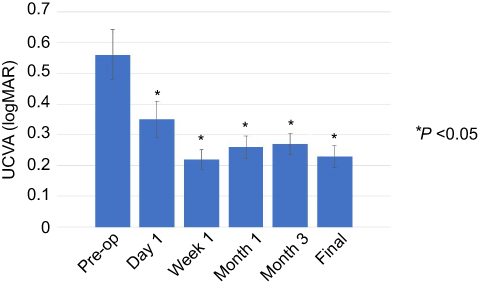 |
Figure 1 Mean pre- and postoperative uncorrected visual acuity (UCVA) presented in logMAR form with error bars representing standard error. Asterisk (*) denotes statistically significant difference compared to preoperative UCVA. |
At the time of final follow-up, 62.5% of patients (15 of 24) were at or within 0.5 D of target, while 83.3% (20 of 24) were at or within 1.0 D. Of the 24 eyes, 4 eyes (16.7%) were hyperopic at time of final follow-up. Near visual acuity was recorded at J3 or better in 11 of 16 eyes (68.8%) and J4–J6 in 5 of 16 eyes (31.3%) at the time of final follow=up. At the time of final follow=up, 10 patients (41.7%) had undergone YAG capsulotomy.
Questionnaire
The response rate of the patient questionnaire was 75% (9 of 12 patients participated), and all results are listed according to category in Table 3. On average, the questionnaire was administered 6 months after the IOL was implanted (range 3–12 months). For the visual function portion of the questionnaire, where a higher point total indicates better function, the average score was 26.3 of a possible 32 points, with individual responses ranging from 19 to 31 points across all 9 patients. Regarding spectacle dependence, 7 patients (78%) reported never wearing glasses for distance vision, while 5 patients (56%) reported never wearing glasses for intermediate or near vision. Of all patients surveyed, 4 patients (44%) reported never wearing glasses for any purpose (spectacle-free). The breakdown of spectacle usage patterns by number of patients is presented in Figure 2. Glare and dazzle were the most prevalent of the dysphotopsia symptoms, with 4 patients (44%) of patients reporting glare/dazzle to be annoying, while only 1 patient (11%) reported it as debilitating. Unwanted images were reported “barely noticeable” for 7 patients (78%). No patients reported having any unwanted shadowing effect. Overall, 7 patients (78%) reported to be either fairly or very satisfied with their visual outcome.
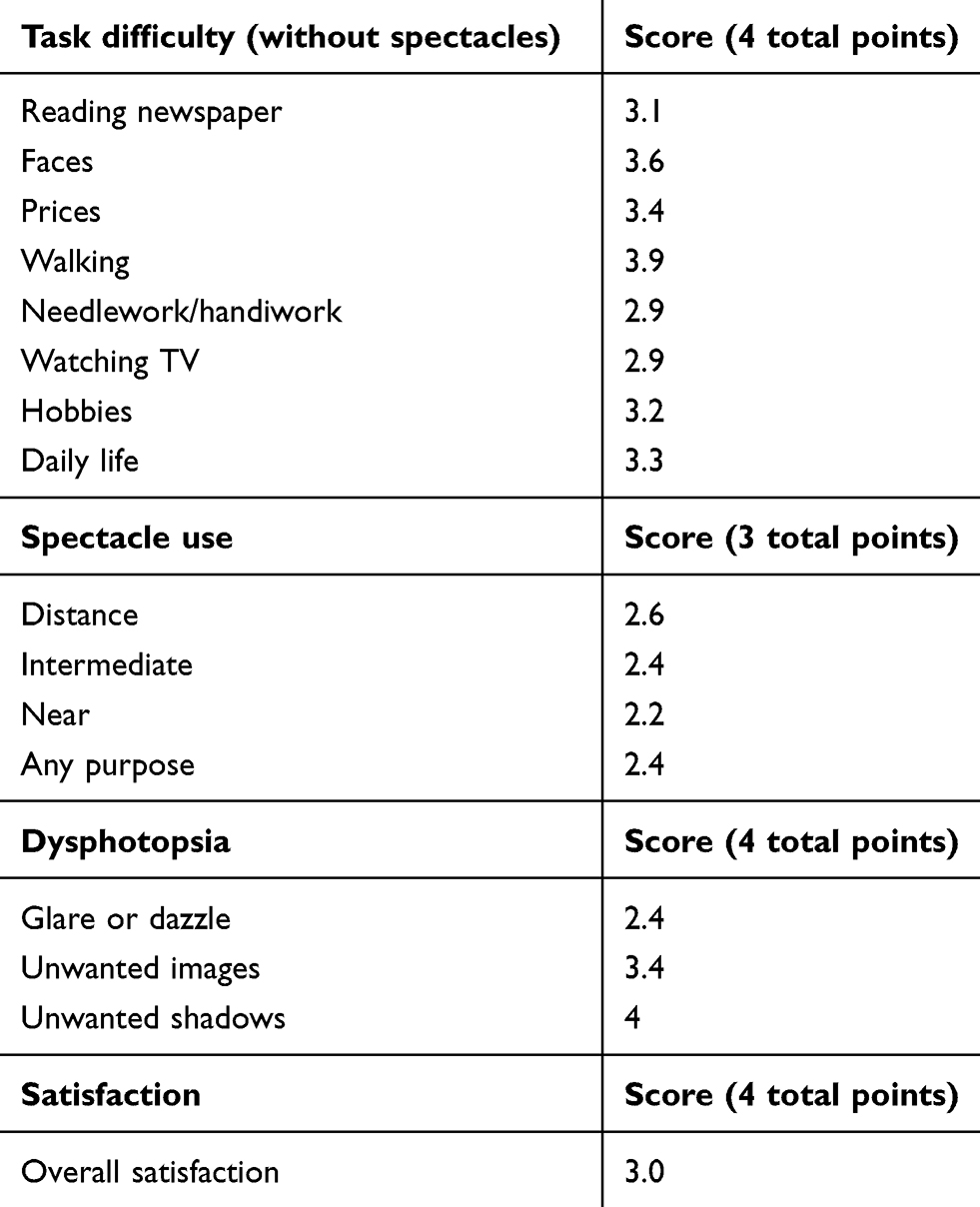 |
Table 3 Average scores (9 patients) from telephone-administered patient questionnaire after cataract surgery with implantation of the Tecnis Symfony lens. Task difficulty, spectacle use, dysphotopsia, and overall satisfaction were assessed. Higher scores indicate a better result (less difficulty, higher spectacle independence or satisfaction, etc.) |
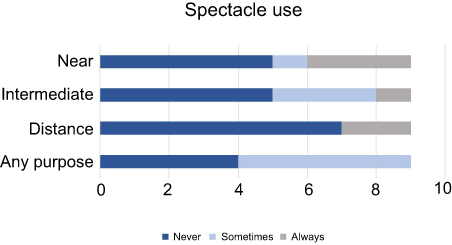 |
Figure 2 Number of patients categorizing their spectacle use as “Never” (Dark), “Sometimes” (Light), and “Never” (Grey) for various distance tasks as well as “Any Purpose.” n=9 respondents. |
Discussion
Many patients who underwent RK at its peak in the 1980s and 1990s are now entering the cataract age. These patients often present with not only reduced quality of vision in the presence of a cataract, but also a desire to achieve reduction in their dependence on glasses or contacts. These scenarios provide a challenge for surgeons because it is difficult to help these patients achieve any degree of spectacle independence, even with monofocal lenses set for distance vision despite the advancements in corneal power estimation and late generation formulae. For these patients that desire a greater level of spectacle independence, multifocal lenses are likely not a good option, as the performance of such lenses is often contingent on a true plano and stable refractive endpoint to achieve effectiveness in bifocality. However, the advent of an IOL with multifocality created through elongation of the focal point, rather than multiple distinct focal points, presents an intriguing possibility of restoring both clarity and functionality without spectacles for patients with a history of RK.
Extended depth of focus (EDOF) IOLs arrived at the US market with the introduction of the Tecnis Symfony lens, FDA approved in 2016, to much excitement among refractive cataract surgeons. The lens uses an achromatic, diffractive echelette design to produce a multifocal-like effect and has been reported to provide improved vision at all distances in monofocal comparisons.11 Thus far, reports evaluating the use of this lens have been favorable in patients with normal corneas, and it is now being widely adopted by surgeons to enable patients to achieve an impressive degree of spectacle independence while mitigating the unwanted side effects common to other diffractive-type optics.12
Patients with a history of RK often maintain the desire for spectacle independence that initially drove them to seek the keratorefractive surgery in the first place. Unfortunately, the presence of RK has left these patients with unstable and often highly aberrated corneas that many surgeons consider challenging cases at best even for monofocal implants. Lens power selection has been a subject of interest in these cases for many years. Because the radial incisions disrupt the anterior to posterior curvature ratio and induce discontinuities in curvature across the surface of the cornea, the presence of RK can alter prediction of effective lens position and overestimate corneal power. Consequently, studies reviewing cataract surgery in post-RK patients have reported hyperopic error in as high as 83.4% of patients.13 In the current study, we utilized one of a number of newer methods of IOL power estimation, the Holladay II formula using the Holladay IOL Consultant software, which takes into account 7 biometric variables and includes an internal modifier for post-RK keratometry. Other methods have also proven useful, including the ASCRS post-RK calculator, which utilizes the Holladay I formula and an Aramberri double-k method of determining true corneal power.14,15 There are no head-to-head studies comparing the use of these later generation calculation methods and either method may be used, but surgeons should make sure to utilize a formula that can similarly adjust for the presence of iatrogenically flattened corneas. While IOL prediction methods have continued to improve, options for spectacle independence for these patients continue to be limited.
To our knowledge, there have been few case reports and no reviews investigating the use of multifocal lenses in patients with a history of RK. Two reports describe favorable patient satisfaction in 3 patients (5 total eyes) using a refractive-type multifocal IOL (Oculentis LS313-MF30; Soleko FIL611PVT),6,7 while a third describes 2 eyes of 2 patients that received a ReSTOR diffractive multifocal optic in the nondominant eye.8 While the aforementioned reports suggested acceptable levels of patient satisfaction and spectacle independence, there remains insufficient objective evidence supporting the routine use of advanced-optics IOLs in this patient population.
The present study is the first to report the outcomes of EDOF lens implantation in patients with a history of RK. In general, we feel the results accurately reflect our clinical experience, with most patients (78% in this study) reporting satisfaction with their visual outcome. UCVA at the final collected follow=up was an average 20/33 in Snellen equivalent and 79% of patients achieved an uncorrected visual acuity 20/40 or better, a result which approaches the values reported by Waring and colleagues in the 3-year PERK study of RK patients prior to development of cataract.16 Moreover, the strong refractive accuracy observed in this study using the Symfony lens after RK is compelling. While the mean SE fluctuated over the course of follow=up, the final mean SE was −0.18 D at an average 5 months after cataract surgery. At that time, 62.5% of patients refracted to or within 0.5 D of target, while 83.3% of patients refracted to or within 1.0 D. We feel these results compare very favorably to other studies reporting this metric with monofocal implants in post-RK eyes utilizing a variety of IOL prediction methods. In a study evaluating the ASCRS online calculator for monofocal implants in post-RK eyes, authors reported 46.67% at or within 0.5 D of target and 66.67% at or within 1.0 D of target.15 Another study by Potvin and Hill utilizing Scheimpflug data for measurement of K values in post-RK eyes reported 42% at or within 0.5 D and 76% at or within 1.0 D.4 A recent study employed IOL master K values with the Haigis formula and found 69% of patients at or within 0.5 D and 88% at or within 1 D.1
There are a few potential explanations as to why an EDOF IOL may prove beneficial in a patient with a history of RK. First, as noted above, one of the major challenges for the cataract surgeon is IOL power calculation after corneal refractive surgery. In the post-RK cornea, it is difficult to determine true corneal power and effective lens position, and an overestimation of corneal power may lead to hyperopic surprise.17,18 Many surgeons have overcome this hurdle with monofocal optics by targeting a myopic refractive error. An optic with an elongated focal point, such as the Symfony lens, may actually permit a larger “landing zone” for IOL power. In other words, the elongated focal point and resultant broadened defocus curve may produce acceptable levels of UCVA across a larger width of residual refractive error. In addition to allowing for more forgiveness in IOL power calculation, the broad defocus curve may also contribute to patient satisfaction levels by absorbing some of the refractive error fluctuations that are known to occur after RK. As seen in Figure 3, the Symfony lens produces a defocus curve that allows for maintenance of 20/40 vision or better across 3D of defocus, with the greatest range over negative defocus (simulating hyperopia relative to the focal point). This may partially explain why many of these patients did favorably in the early postoperative period, a time when RK fluctuations have been most frequently reported.18
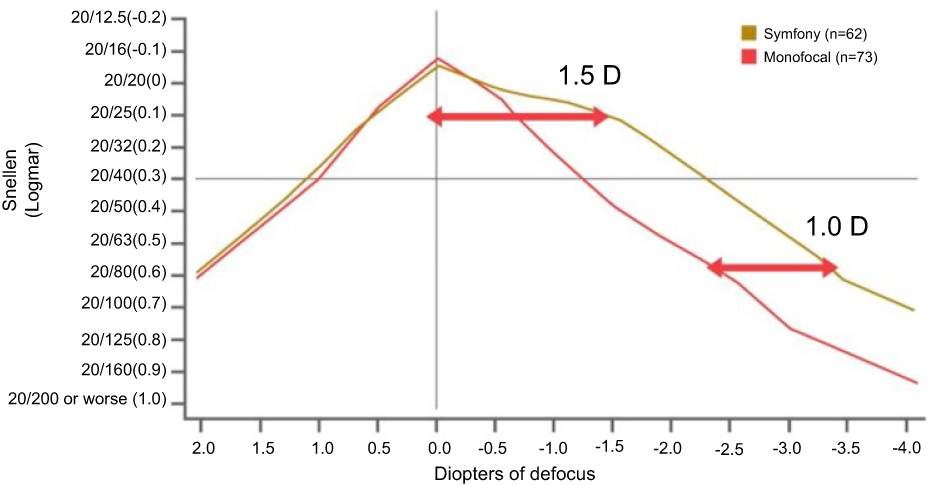 |
Figure 3 Defocus curves of Tecnis Symfony lens vs Tecnis monofocal lens. Vertical line denotes zero diopters of defocus, while horizontal line represents 20/40 visual acuity. Area under the curve remaining above horizontal line denotes amount of defocus tolerated maintaining vision at 20/40 or better.Note: Copyright © 2018. Johnson & Johnson Surgical Vision, Inc. Reproduced from TECNIS Symfony®. Extended Range of Vision IOLs DFU. Santa Ana: Johnson & Johnson Surgical Vision, Inc.; 2016. Available from: http://www.precisionlens.net/Websites/precisionlens/images/JJ%20Tecnis%20Symfony%20DFU.pdf./. Accessed July 11, 2019.19 |
In addition to postoperative fluctuations in refractive error, post-RK corneas are known to demonstrate higher levels of corneal aberrations than normal corneas and increase with magnitude of refractive correction.20 The increase in HOA, particularly spherical aberration, is thought to result in reduced visual quality and contrast sensitivity.21,22 Some concern may be raised regarding implantation of advanced optic IOLs, including multifocal or EDOF lens designs, in patients already predisposed to reduced contrast sensitivity, as traditional diffractive multifocal lenses have demonstrated significantly greater compromise in contrast sensitivity after cataract surgery when compared to monofocal lenses.23 This has not been demonstrated with the Tecnis Symfony EDOF lens, which compares favorably to monofocal lenses in this regard.11 As expected from prior reports, our patients had higher corneal spherical aberration than those reported in the literature for normal corneas utilizing the same aberrometer.24 While the exact contribution of these aberrations on the objective and subjective visual outcomes of the present study is unknown, we recognize these as preoperative characteristics that may determine outcomes of cataract surgery. Future studies regarding performance of EDOF lenses in patients with a history of RK could evaluate corneal aberrations and contrast sensitivity, which may provide clarity on the impact of aberration profiles on predicting postoperative performance.
A limitation of the current study is the retrospective nature and selectiveness of preoperative patient characteristics. We do not offer an EDOF lens option to all patients with a history of RK in the presence of cataract. There are some patients, particularly those who rely on rigid gas permeable contact lenses or scleral lenses for functional vision at presentation due to high degrees of irregular astigmatism, who would likely not benefit from the particular optical properties of an EDOF lens. While our study included all patients in our practice with a history of RK who received an EDOF lens, the average preoperative BSCVA was 20/25 (range 20/15 to 20/80; all with cataract and decreased brightness acuity testing), likely reflective of our selectivity in lens option offerings. A thorough discussion of risks and benefits to each option was performed with each patient, including possibility of lens exchange. Various other preoperative characteristics may be contributory to our results as well. The average number of RK incisions was 6.4, and no patient had >8-cut RK or additional AK incisions. While results of prior studies have not shown an effect of number of incisions on post-cataract refractive error,4,15 the lack of inclusion of patients with more significant incisional refractive surgery (eg, 16-cut RK or additional AK) may have influenced our results. Therefore, the present study results may not be generalizable to every patient with a history of RK, but simply a representation of our particular practice patterns. It is our recommendation that practitioners be discerning in their offering of EDOF or other diffractive IOLs to patients with history of keratorefractive surgery.
The results of this study indicate that an extended-depth-of-focus lens, such as the Tecnis Symfony, is a good option in the appropriate patient with a history of RK. Patients with otherwise excellent ocular health who retain good spectacle-corrected visual acuity and subsequently develop cataract may be good candidates for an EDOF lens. The elongated focal point of the Symfony lens may be beneficial to the post-RK patient and reduce some of the defocus from fluctuating corneal power. However, it remains imperative to thoroughly discuss lens options, risk and benefits to each option in this population. Future studies aiming to validate or deepen our understanding of the use of such lenses could directly compare results to monofocal lens performance and perform evaluations of contrast sensitivity in these optically complex patients.
Acknowledgments
The authors would like to acknowledge Douglas Wallin OD and Keith Rasmussen OD for their conceptualization of the project and clinical insight in advancing care of patients with a history of radial keratotomy. Presented at: American Society of Cataract and Refractive Surgeons (ASCRS) Annual Meeting, Washington, DC, April 2018.
Disclosure
Drs Berdahl and Thompson have received consultant fees from Johnson and Johnson Vision. Dr Berdahl reports personal fees from Alcon, Allergan, Avedro, Aurea Medical, Bausch and Lomb, CorneaGen, Dakota Lions Eye Bank, Equinox, Expert Opinion, Glaukos, Gore, Imprimis/Harrow Health, Johnson and Johnson, Kala, Kedalion, MELT Pharmaceuticals, MicroOptx, New World Medical, Ocular Surgical Data, Ocular Theraputix, Omega Ophthalmic, Orasis, Oyster Point, RxSight, Surface INC, Tarsus, Tear Clear, Vittamed, Vance Thompson Vision, Verana Health, Visionary Ventures, Zeiss, during the conduct of the study. Dr Thompson reports personal fees from Alcon, Bausch & Lomb, Johnson & Johnson, Zeiss, during the conduct of the study and personal fees from Acufocus, Allergan, Allotex, Avellino, BRIM Biotechnology, Inc, Conjtac, CSO (Costruzione Strumenti Oftalmici), Equinox, Euclid Systems, eyeBrain Medical Inc, Eyedetec, EyeGate Pharma, Healthe, Imprimis, Mynosys, Novaliq, OPHTEC, ORA (Ora Inc), Oyster Point Pharma, Precision Lens, RxSight, SightSciences, Stuart Therapeutics, Tarsus Rx, TearClear, ThruFocus, Treehouse Health, Veracity, Visant, Visiometrics, Vivior AG, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Geggel HS. Intraocular lens power selection after radial keratotomy: topography, manual, and IOL master keratometry results using Haigis formulas. Ophthalmology. 2015;122(5):897–902. doi:10.1016/j.ophtha.2014.12.002
2. Freeman M, Kumar V, Ramanathan US, O’Neill E. Dehiscence of radial keratotomy incision during phacoemulsification. Eye (Lond). 2004;18(1):101–103. doi:10.1038/sj.eye.6700526
3. Day A, Seward H. Delayed radial keratotomy dehiscence following uneventful phacoemulsification cataract surgery. Eye (Lond). 2007;21(6):887. doi:10.1038/sj.eye.6702766
4. Potvin R, Hill W. New algorithm for post-radial keratotomy intraocular lens power calculations based on rotating Scheimpflug camera data. J Cataract Refract Surg. 2013;39(3):358–365. doi:10.1016/j.jcrs.2012.09.019
5. Stakheev AA. Intraocular lens calculation for cataract after previous radial keratotomy. Ophthalmic Physiol Opt. 2002;22(4):289–295.
6. Kim KH, Seok K, Kim WS. Multifocal intraocular lens results in correcting presbyopia in eyes after radial keratotomy. Eye Contact Lens. 2015;43:1–4.
7. Nuzzi R, Tridico F. Comparison of visual outcomes, spectacles dependence and patient satisfaction of multifocal and accommodative intraocular lenses: innovative perspectives for maximal refractive-oriented cataract surgery. BMC Ophthalmol. 2017;17:12. doi:10.1186/s12886-017-0411-9
8. Gupta I, Oakey Z, Ahmed F, Ambati BK. Spectacle independence after cataract extraction in post-radial keratotomy patients using hybrid monovision with ReSTOR multifocal and tecnis monofocal intraocular lenses. Case Rep Ophthalmol. 2014;5:157–161. doi:10.1159/000363372
9. Jose RT, Atcherson RM. Type-size variability for near-point acuity tests. Am J Physiol Opt. 1997;54(9):634–638.
10. Maurino V, Allan BD, Rubin GS, Bunce C, Xing W, Findl O. Quality of vision after bilateral multifocal intraocular lens implantation: a randomized trial – AT LISA 809M versus AcrySof ReSTOR SN6AD1. Ophthalmology. 2015;122(4):700–710. doi:10.1016/j.ophtha.2014.10.002
11. Pedrotti E, Bruni E, Bonacci E, Badalamenti R, Mastropasqua R, Marchini G. Comparative analysis of the clinical outcomes with a monofocal and an extended range of vision intraocular lens. J Refract Surg. 2016;32(7):436–442. doi:10.3928/1081597X-20160428-06
12. Sachdev GS, Ramamurthy S, Sharma U, Dandapani R. Visual outcomes of patients bilaterally implanted with the extended range of vision intraocular lens: a prospective study. Indian J Ophthalmol. 2018;66(3):407–410. doi:10.4103/ijo.IJO_813_17
13. Chen L, Mannis MJ, Salz JJ, Garcia-Ferrer FJ, Ge J. Analysis of intraocular lens power calculation in post-radial keratotomy eyes. J Cataract Refract Surg. 2003;29(1):65–70.
14. Aramberri J. Intraocular lens power calculation after corneal refractive surgery: double K method. J Cataract Refract Surg. 2003;29(11):2063–2068.
15. Demill DL, Hsu M, Moshirfar M. Evaluation of the American Society of Cataract and Refractive Surgery intraocular lens calculator for eyes with prior radial keratotomy. Clin Ophthalmol. 2011;5:1243–1247. doi:10.2147/OPTH.S24514
16. Waring GO
17. Lyle WA, Jin GJ. Intraocular lens power prediction in patients who undergo cataract surgery following previous radial keratotomy. Arch Ophthalmol. 1997;115(4):457–461.
18. Koch DD, Liu JF, Hyde LL, Rock RL, Emery JM. Refractive complications of cataract surgery after radial keratotomy. Am J Ophthalmol. 1989;108(6):676–682.
19. TECNIS Symfony®. Extended Range of Vision IOLs DFU. Santa Ana: Johnson & Johnson Surgical Vision, Inc.; 2016. Available from: http://www.precisionlens.net/Websites/precisionlens/images/JJ%20Tecnis%20Symfony%20DFU.pdf./. Accessed July 11, 2019.
20. Applegate RA, Hilmantel G, Howland HC. Corneal aberrations increase with the magnitude of radial keratotomy refractive correction. Optom Vis Sci. 1996;73(9):585–589.
21. Hemenger RP, Tomlinson A, Caroline PJ. Role of spherical aberrations in contrast sensitivity loss with radial keratotomy. Invest Ophthalmol Vis Sci. 1989;30(9):1997–2001.
22. Applegate RA, Howland HC, Sharp RP, Cottingham AJ, Yee RW. Corneal aberrations and visual performance after radial keratotomy. J Refract Surg. 1998;14:397–407.
23. Gil MA, Varon C, Cardona G, Vega F, Buil JA. Comparison of far and near contrast sensitivity in patients symmetrically implanted with multifocal and monofocal IOLs. Eur J Ophthalmol. 2014;24(1):44–52. doi:10.5301/ejo.5000335
24. Amirshekarizadeh N, Hasemi H, Jafarzadehpur E, Mirzanjani A, Yekta A, Khabazkhoob M. Higher-order aberrations after cyclopentolate, tropicamide, and artificial tear drops application in normal eyes. Eye Contact Lens. 2018;44:109–112.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.