Back to Journals » Cancer Management and Research » Volume 12
Expression Pattern and Prognostic Utility of PME-1 in Patients with Hepatocellular Carcinoma
Received 7 March 2020
Accepted for publication 2 April 2020
Published 29 April 2020 Volume 2020:12 Pages 2937—2945
DOI https://doi.org/10.2147/CMAR.S252873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Baoying Du,1 Hongfeng Liao,2 Sheng Zhang3
1Department of Hepatopancreatobiliary Surgery, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Pathology, Zhongshan Hospital of Xiamen University, Xiamen, People’s Republic of China; 3Department of Pathology, Hubei Cancer Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Sheng Zhang
Department of Pathology, Hubei Cancer Hospital, No. 116, Zhuodaoquan South Road, Wuhan, Hubei Province, People’s Republic of China
Tel/Fax +86-27-87670411
Email [email protected]
Purpose: Hepatocellular carcinoma (HCC) remains one of the most common malignancies. While there is lack of markers capable of predicting which patients are at risk of aggressive course of the disease. Although a few protein phosphatase methyl-esterase-1 (PME-1) tumor-promoting mechanisms have been reported, the role of PME-1 in cancer including HCC occurrence and progression remains to be elucidated. The aim of this study was to explore the expression pattern and relationship between PME-1 with the pathological parameters in patients with HCC.
Methods: PME-1 expression was assessed from HCC tissue chips via immunohistochemistry. Chi-square test was used to identify the association between PME-1 staining and clinicopathological variables of HCC patients. Kaplan–Meier analysis and Cox regression analysis were performed to draw survival curves and verify the independent prognostic factors of HCC patients, respectively.
Results: We found that PME-1 expression was significantly higher in HCC tumor tissues compared with non-tumor tissues (P < 0.001). Furthermore, high expression level of PME-1 was significantly associated with differentiation (P = 0.047), tumor number (P = 0.001), intrahepatic or extrahepatic metastasis (P = 0.018), and recurrence (P = 0.001). Kaplan–Meier analysis revealed that high expression level of PME-1 was associated with shorter survival (P < 0.001). Univariate analysis with Log-rank test revealed that PME-1 expression status was significantly correlated with overall survival (P < 0.001). Furthermore, multivariate models with Cox proportional hazards analysis showed that high expression of PME-1 was a statistically independent predictive factor of poor prognosis in HCC patients (hazard ratio, 3.429; 95% confidence interval, 1.369– 8.589; P = 0.009).
Conclusion: In conclusion, these findings indicated that PME-1 expression was associated with aggressive pathological features and worse oncological outcomes, suggesting its potential therapeutic value for patients with HCC.
Keywords: hepatocellular carcinoma, PME-1, survival, immunohistochemistry
Introduction
Hepatocellular carcinoma (HCC) remains one of the most common malignancies and becomes the third leading cause of cancer-associated deaths worldwide.1,2 Its prognosis has gradually improved due to advancements in surgery and adjuvant chemotherapy. However, a portion of the patients still die of this disease. Hence, there is a need for biomarkers to predict which patients are at risk of disease recurrence. This would help to direct adjuvant treatments to those patients that gain benefit from them and protect the low-risk patients from the side effects of therapy.
Protein Phosphatase Methyl-Esterase-1 (PME-1) is a protein phosphatase 2A (PP2A) specific methylesterase that binds to the active site of PP2A and resulting in both the demethylation and inactivation of PP2A.3,4 PME-1 impairs poly-ubiquitination of PP2Ac and prolongs the half-life of PP2Ac protein resulting in increased PP2Ac levels.5 The latest reports suggest that PME-1 level is up-regulated in both progressive supranuclear palsy and Alzheimer's disease brains compared to controls.6 Some researches also reveal that PME-1 is critical for regulating mitotic spindle size and thereby promotes cell division,7 glucose uptake in skeletal muscle cells,8 as well as differentiation of neuroblastoma cells.9 What is more, PME-1 expression has been studied in a limited number of human neoplasms, such as astrocytic gliomas, endometrial, lung, gastric and colorectal cancer. PME-1 mediated inhibition of the PP2A increases the basal extracellular signal-regulated kinase (ERK) pathway activity and promotes malignant cell growth of human glioblastoma cells.10 Puustinen P et al also find that PME-1 expression significantly correlates with disease progression in human astrocytic gliomas. Moreover, PME-1 immuno-positivity has been strongly correlated with an increased Ki-67 proliferation index in tumor samples.11 PME-1 expression forces progression of low-grade astrocytic gliomas to malignant glioblastomas.9 Elevated amounts of PME-1 have been found in clinical specimens of endometrial adenocarcinoma, which are linked to the increased cell proliferation ability and invasive phenotypes in endometrial adenocarcinoma cells.12 Additionally, a small fraction of the gastric and lung cancer patients shows PME-1 gene amplification (3.8% and 3.1%, respectively), which also corresponds to activation of ERK, AKT signaling and a significant promotion of cell proliferation and inhibition of cell apoptosis.13 Furthermore, the depletion of PME-1 decreased the migration and invasion of choriocarcinoma cells.14 Contrary to the above cancer types, PME-1 expression predicts a favorable outcome of colorectal cancer patients.15
These previous studies have highlighted the potential oncogenic role of PME-1 in these malignant neoplasms. However, whether the oncogenic function of PME-1 can be generalized to various human cancer types is as yet unclear. Also, these studies so far have failed to identify any correlation between PME-1 expression and the patients’ survival in HCC. Since approximately 841,000 new cases of liver cancer and 782,000 mortalities worldwide, among which 50% of the total number of new cases and deaths in China,16–18 we urgently asked whether PME-1 plays a role in HCC progression.
In this study, we reported the immunohistochemical analysis of PME-1 protein expression in the tumor materials of HCC patients’ cohort and its correlation to the clinicopathological parameters as well as patients’ survival. Similarly, in accordance to its previously shown oncogenic role in other malignancies, we showed that high expression of PME-1 correlated with worse clinical outcomes in HCC.
Materials and Methods
Tissue Specimens
A total of 95 cases of formalin-fixed paraffin-embedded HCC and matched non-tumor tissuses were collected in the pathology department at Hubei Cancer Hospital (Wuhan, China) from January 2013 to December 2015. Patients did not receive radiotherapy or chemotherapy at the time of original biopsy. The clinicopathological information was collected from the medical records of patients, including age, gender, histopathological classification, tumor size, recurrence status, and so on. The overall survival time was calculated from the date of the first diagnosis until the last follow up or the death of the patients, with the maximum follow-up time being 60 months. The study was carried out in line with the World Medical Association Declaration of Helsinki and approved by the Ethics Committee of the hospital. Written informed consent was provided by all the participants.
Immunohistochemistry (IHC)
The IHC staining was performed by EliVisionTMplus Kit (KIT-9902, Maixin, Fuzhou, China) on 3‐μm tissue sections. As previously described,19 tissue was fixed with 10% formalin and embedded in paraffin then cut into 3 µm sections for immunohistochemical staining. Sections were deparaffinating, rehydrated, citrate mediated high temperature and pressure antigen retrieval was performed for 5 min. 0.3% H2O2 was applied for 20 min at room temperature to block endogenous peroxidase activity. The sections were stained with anti-PME-1 (1:200, sc-25278, Santa Cruz Biotechnology, Inc.) at 4°C overnight. After incubation with secondary antibody, the visualisation signal was obtained with 3,3ʹ‐diaminobenzidine tetrachloride, followed by counterstaining with Mayer’s hematoxylin. Finally, the sections were dehydrated through graded alcohols and cleared in xylene prior to slide mounting.
IHC Evaluation
The evaluation was based on the proportion score and the intensity score of positively stained tumor cells.20 In short, immunohistochemical staining was evaluated independently by two clinical pathologists, who were blinded to the clinicopathological data at ×200 magnification light microscopy. Any inconsistencies in the immunostained section scores were re-evaluated by a third pathologist to obtain a final result. A semiquantitative evaluation of PME-1 protein expression was performed as follows: staining intensity for the protein was scored as 0 (negative), 1 (weak), 2 (moderate) and 3 (strong) (Seen in Figure 1). Then, the staining proportion was scored as 0 (0%), 1 (1–25%), 2 (26–50%), 3 (51–75%) and 4 (76–100%). Finally, the intensity and proportion scores were multiplied to obtain a total score for each sample. Based on the previously published IHC evaluation approach,21 scores for 6 or higher were considered to represent high PME-1 expression and those of 4 or lower to indicate low PME-1 expression.
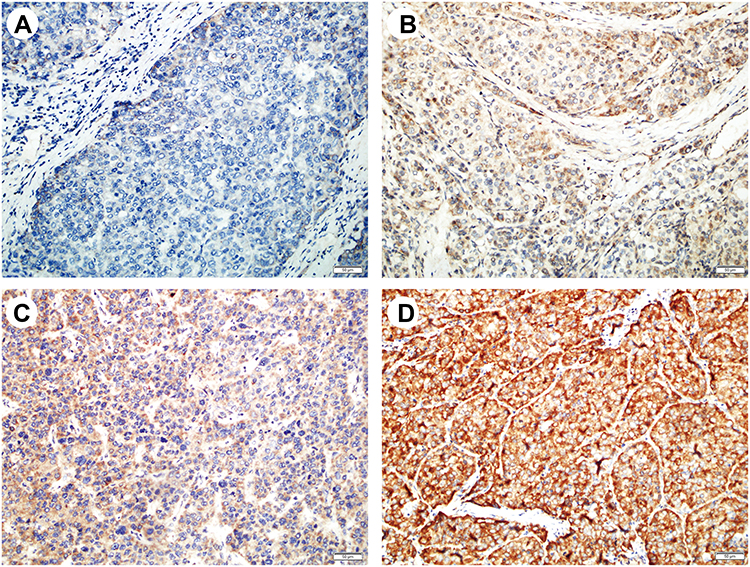 |
Figure 1 Representative IHC staining of PME-1 in HCC. Representative images of PME-1 immunohistochemical staining from HCC patient samples used for correlation analysis. (A) Negative, (B) weak, (C) moderate, (D), strong. Scale bars = 50 μm. |
Real-Time Polymerase Chain Reaction (PCR)
Total RNA was extracted from paraffin-embedded tissue using the RNeasy FFPE Kit (Qiagen, Valencia, CA, USA), according to the manufacturer’s instructions. After reverse transcription of total RNA, real-time PCR was performed to examine the expression levels of PME-1 mRNA using SYBR Green PCR Master mix (Takara Biotechnology, Ltd.) on a real-time PCR instrument (Bio-Rad, Carlsbad, CA, USA). The following primer sequences were used: PME-1, forward: 5′-GGACCTTCCTCCTCCAATTATG-3′, reverse: 5′-ATCATGCACAGACCCAAGAG-3′; GAPDH, forward: 5′-CTTTGGTATCGTGGAAGGACTC-3′, reverse: 5′-AGTAGA GGCAGGGATGATGT-3′. The expression of PME-1 was calculated using the standard curve method normalised to GAPDH. Each experiment was performed in duplicate, and the mean was adopted as the value in each experiment.
Statistical Analysis
Statistical analyses were performed by Chi-square test, Mann–Whitney test, multivariate Cox regression analysis and Kaplan–Meier analysis using SPSS version 21.0 for Windows (Chicago, IL, USA) and GraphPad Prism 5 (La Jolla, CA, USA). Chi-square test was adopted to find out the correlation of PME-1 protein expressions with clinicopathological parameters. The Mann–Whitney test was used to compare the difference of PME-1 protein and mRNA expression between HCC cancer and noncancer tissues. Cox logistic regression analysis was applied to evaluate the independent influence of various clinicopathological factors on survival. Kaplan–Meier survival analysis was used to analyze the effect of the marker on survival with the Log-rank test. All statistical tests were two-tailed. Differences at P < 0.05 were considered to be significant.
Results
Patient Characteristics
A total of ninety-five HCC patients were included in our present study. All of the patient’s characteristics are summarized in Table 1: seventy-five (78.9%) males and twenty (21.1%) females with the mean age of forty-nine years (range, 20–79 years). There were fifty-three (55.8%) patients whose tumor size was more than 5 centimeter; fifty-five (57.9%) patients were poor differentiation depend on the pathologist diagnosis, and forty-four (46.3%) of the patients presented with multifocal tumors. A total of fifty-seven (60.0%) patients were with intra or extra-hepatic metastasis and thirty-seven (38.9%) patients with liver cirrhosis. Thirty-eight (40.0%) and fifty-two (54.7%) patient serum α-fetoprotein (AFP) and Hepatitis B virus (HBV) level was more than 200 ng/mL and 1000 IU/mL, respectively. In addition, forty-one (43.2%) patients died and forty-seven (49.5%) developed recurrence.
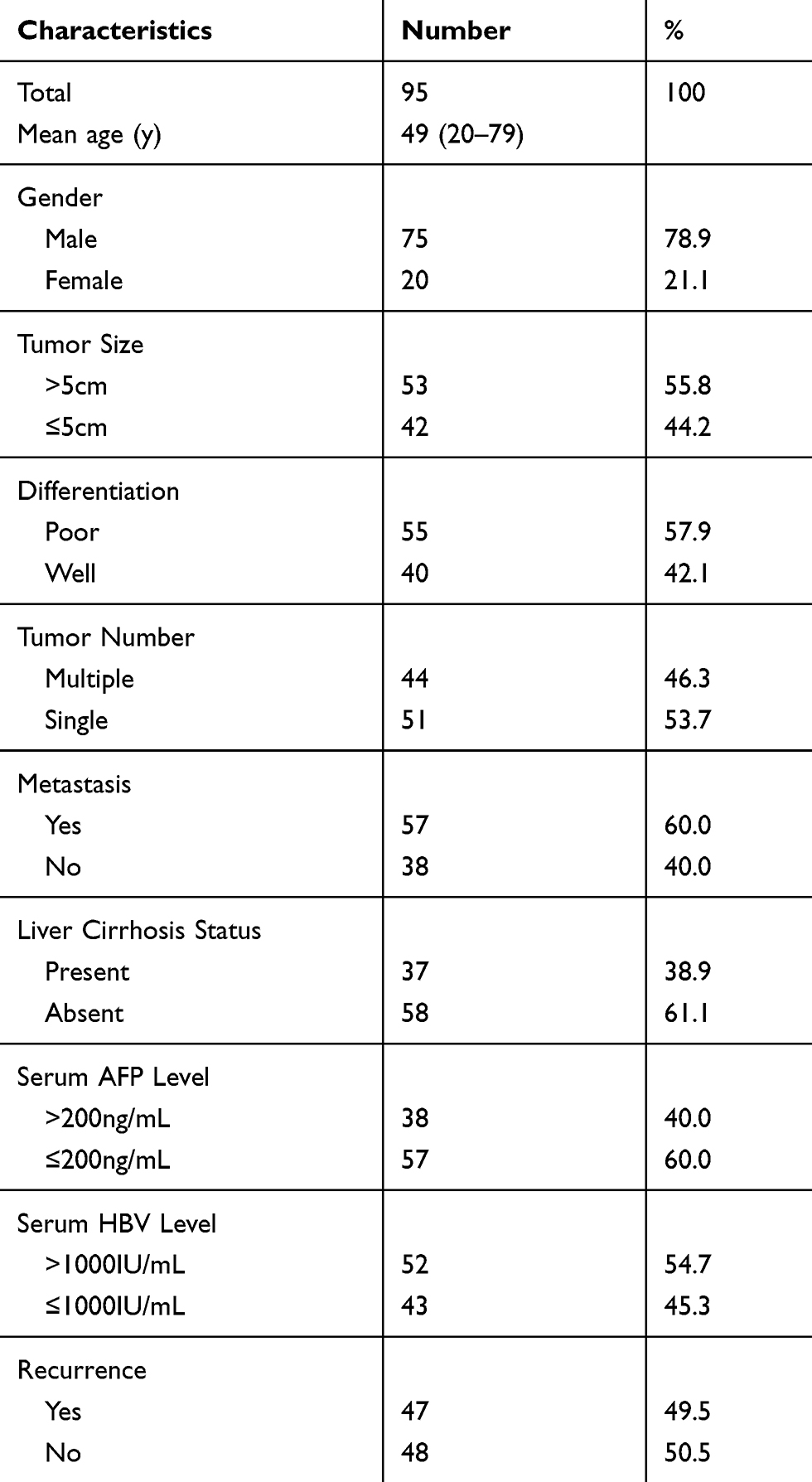 |
Table 1 Patient Characteristics |
Elevated Expression of PME-1 in HCC Tissues
Former studies revealed that PME-1 might have different roles and expression patterns in some cancers. However, the biological function and expression pattern of PME-1 in HCC was still unknown. Thus, IHC assay was carried out in paraffin-embedded HCC cancer tissues and paired adjacent noncancerous tissues. As shown in Figure 2A, the staining of PME-1 protein was predominantly identified in the cell cytoplasm of HCC cancer cells 84.2% (80 of 95). In contrast, PME-1 staining was found in only a few cases of the corresponding normal tissues 30.5% (29 of 95) (P < 0.001, Table 2). Moreover, the immunohistochemical score of PME-1 in tumor tissues was 5.93 ± 3.87, which was significantly higher than that in the corresponding normal tissues (0.94 ± 1.81, P < 0.001, seen in Figure 2B). In addition, Real-time PCR also got a similar result that PME-1 mRNA expression level was higher in HCC tissues compared with normal tissues (Figure 2C).
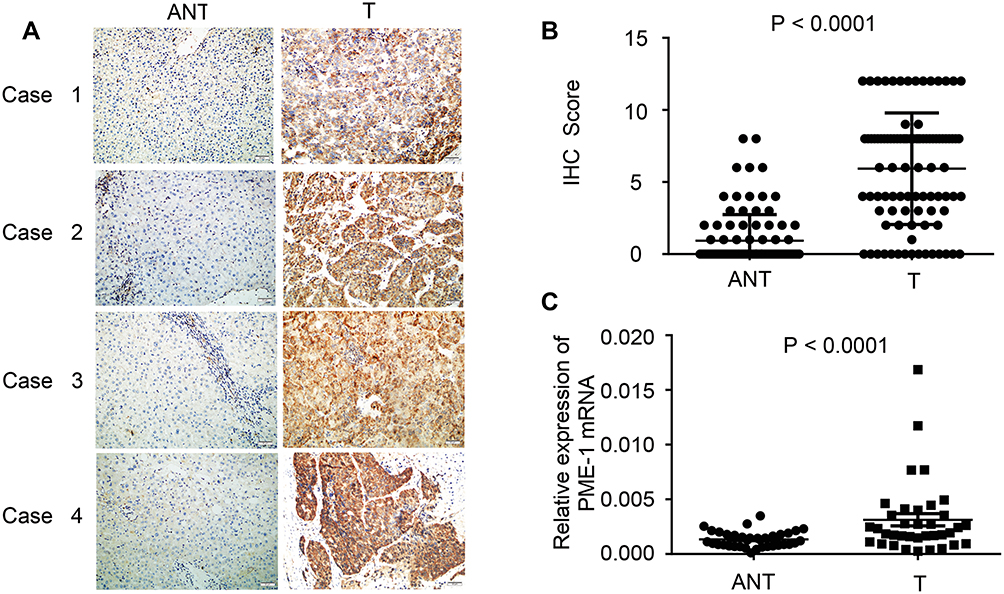 |
Figure 2 Comparison of PME-1 expression between HCC tissues and paired adjacent noncancerous liver tissue. (A) The representative expression patterns of PME-1 in four cases. Scale bars = 50μm. (B) PME-1 protein expression in HCC was significantly higher than that in normal liver tissues (P < 0.0001). (C) PME-1 mRNA expression level was relatively higher in HCC compared with that in normal liver tissues (P < 0.0001). Data were analyzed with 2-related samples Wilcoxon test. Abbreviations: ANT, adjacent noncancerous tissue; T, cancer tissues. |
 |
Table 2 Positive Rate of PME-1 Expression among HCC Cancer Tissues and Paired Adjacent Noncancerous Tissues |
Correlations Between PME-1 Expression and Clinicopathological Parameters of HCC
To investigate the clinicopathological significance of PME-1 in HCC, we analyzed the potential correlations between PME-1 expression and the clinicopathological characteristics of patients with HCC. As shown in Table 3, the rate of high PME-1 expression was higher in patients with poor differentiation (36/55; 65.5%) than those with well-differentiated tumors (18/40; 45.0%) (P = 0.047). The rate of high PME-1 expression was higher in patients with multiple tumors (33/44; 75.0%) compared with that with a single tumor (21/51; 41.2%) (P = 0.001). In addition, the patients with intrahepatic or extrahepatic metastasis (38/57; 66.7%) have significantly higher expression levels of PME-1 than patients without metastasis (16/38; 42.1%) (P = 0.018). Moreover, analysis of the association between PME-1 expression in cancer tissues and patients’ recurrence, we found that PME-1 expression was significantly associated with recurrence (P = 0.001). However, the expression level of PME-1 had no statistically significant association with other parameters, including gender, age, tumor size, liver cirrhosis status, serum AFP and HBV level (P > 0.05 for each). These results identified that PME-1 expression may play a critical role in the progression of HCC.
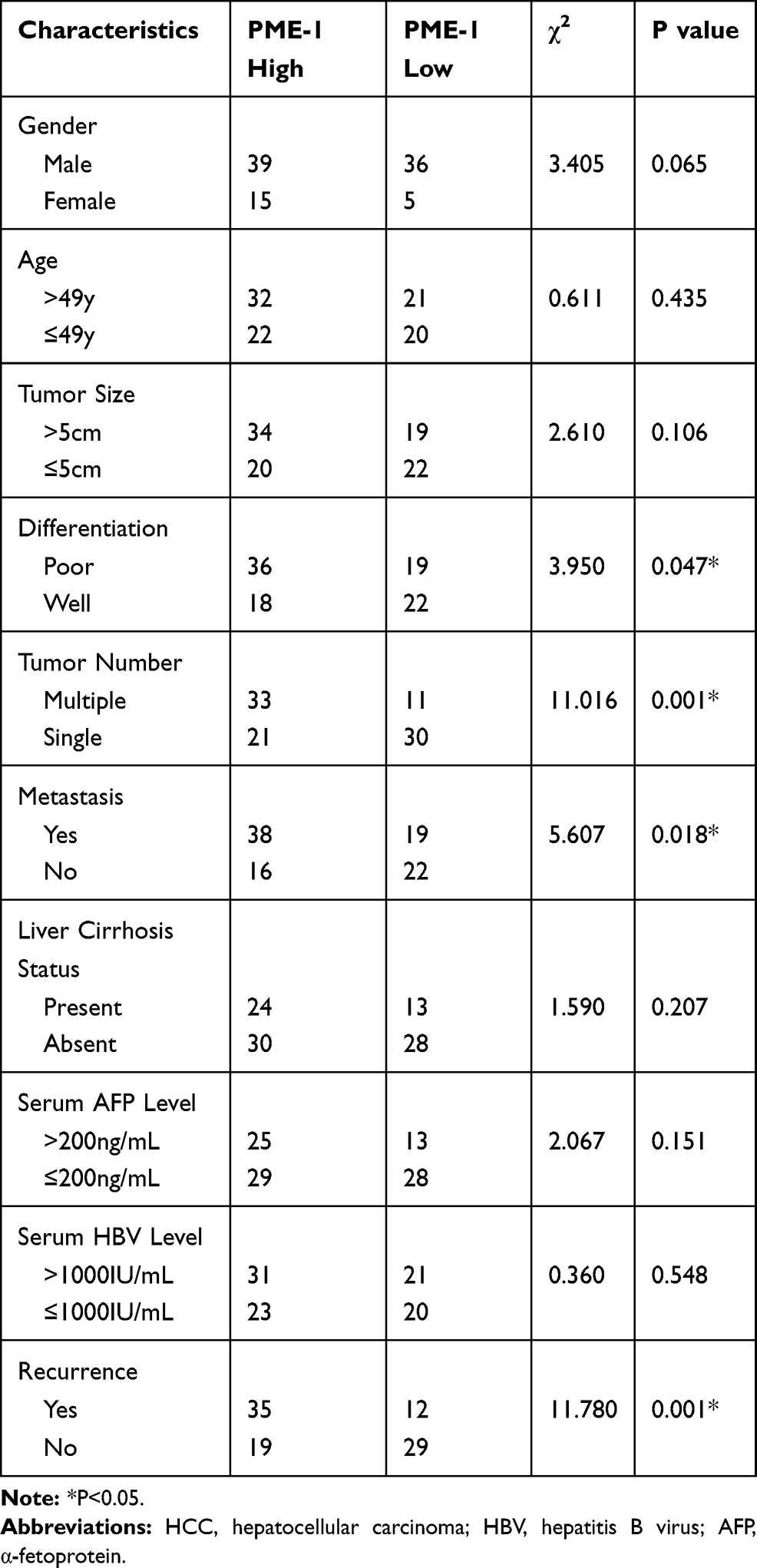 |
Table 3 Correlations Between PME-1 Expression and the Clinicopathological Characteristics of Patients with HCC |
PME-1 Overexpression Was Associated with Poor Survival in HCC
To further evaluate the relationship between PME-1 expression and prognosis of HCC patients, we used Kaplan–Meier curves and Log-rank test to analyze the survival data based on follow-up. HCC patients with complete follow-up information (n = 95) were classified into the PME-1 low (n = 41) and PME-1 high groups (n = 54) according to the IHC score of PME-1 expression. As shown in Figure 3, we discovered that the survival curve was significantly better for patients with PME-1 lower than those with PME-1 higher expression by Kaplan–Meier method with the Log rank test (P < 0.001). Univariate analysis with Log-rank tests revealed that PME-1 expression status, recurrence, serum HBV level, metastasis, tumor number, tumor size and differentiation were significantly correlated with overall survival (Table 4). Furthermore, multivariate models with Cox proportional hazards analysis showed that high PME-1 expression was a statistically independent predictive factor of worse prognosis in HCC patients (Hazard ratio, 3.429; 95% confidence interval, 1.369–8.589; P = 0.009; Table 5).
 |
Figure 3 PME-1 expression was correlated with poor survival. Kaplan–Meier analysis and Log rank test showed that patients with high expression of PME-1 had a shorter survival time than that with low PME-1 expression (P < 0.001). |
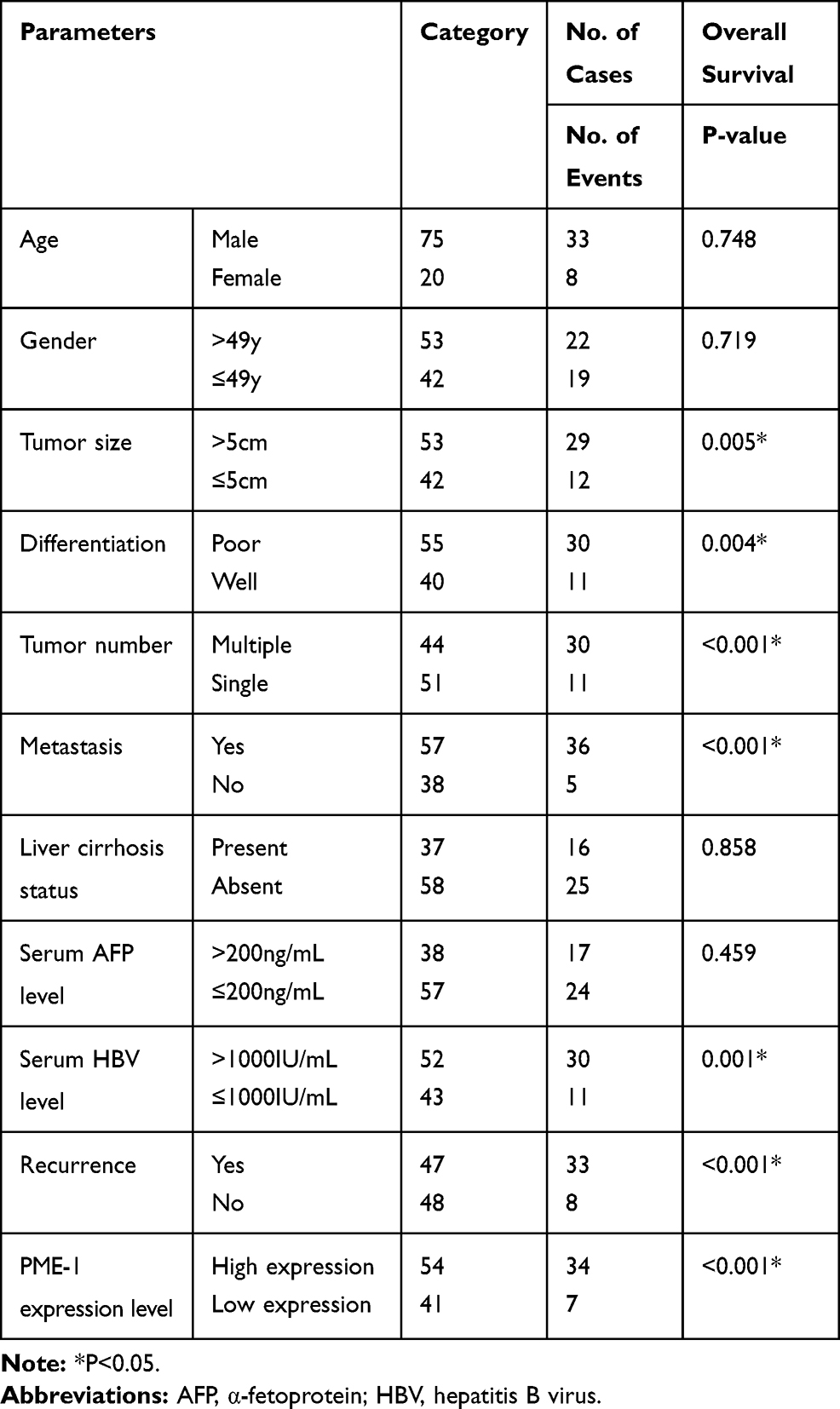 |
Table 4 Univariate Log Rank Analyses |
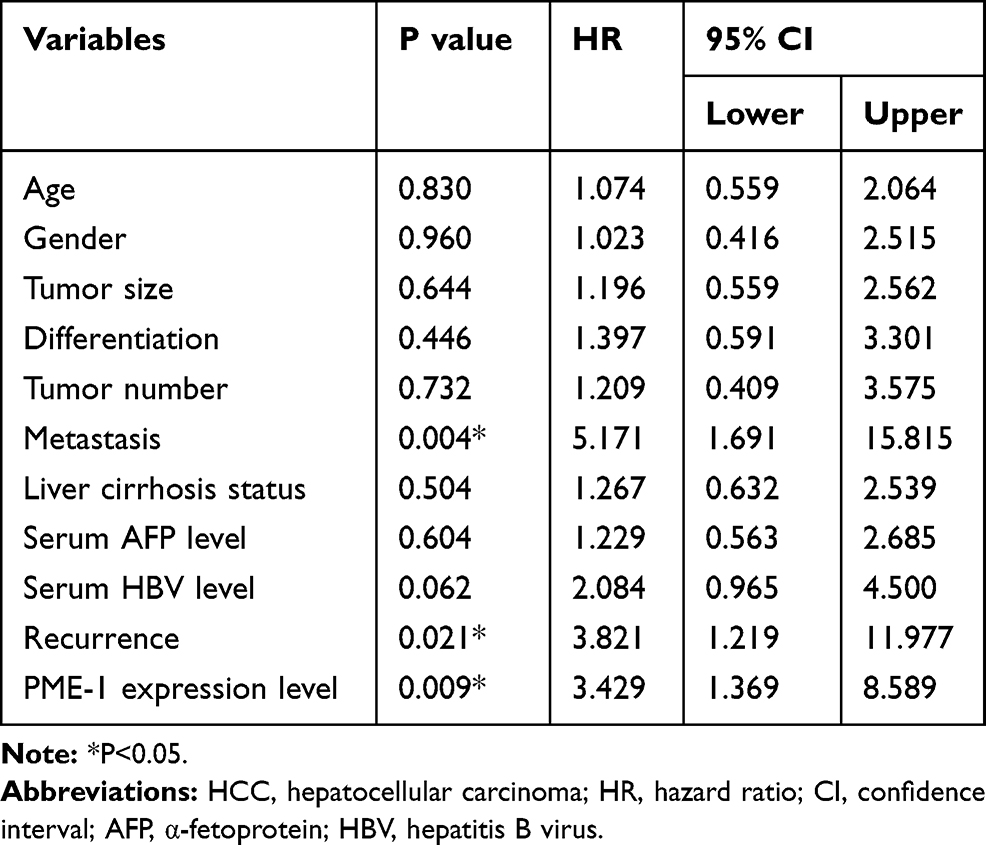 |
Table 5 Multivariate Survival Analyses |
Discussion
Although many advances in treatment strategies for HCC have been explored, the overall survival of these patients has not been dramatically improved.22 Thus, novel biomarkers that can be used to predict the prognosis of these patients remain urgently needed.
The abnormal expression of PME-1, which has a close association with the development, progression, metastasis, and prognosis of some cancer, has been frequently reported. However, both PME-1 expression and its association with clinicopathological factors and the 5-year survival rate have not been defined in HCC. In the current study, we found that high expression of PME-1 was significantly associated with lymph node metastasis and recurrence. Previous work has demonstrated that PME-1 enhanced the migration and invasion ability of choriocarcinoma cells.14 However, invasion-related research is unavailable, although the expression of PME-1 was reported to correlate with the progression of human astrocytic glioma.11 Existing data indicate that ERK and glycogen synthase kinase-3β (GSK-3β) are possible pathways involved in PME-1.23 However, no direct evidence supports the role of PME-1 in tumor cell migration and invasion. Given the versatility of the critical role of ERK and GSK-3β pathway in HCC tumorigenesis,24,25 we speculate that the tumor promotor role of PME-1 in HCC can be ascribed to this mechanism, and more studies are necessary to clarify this speculation in the future work.
Although there has been an agreement that PME-1 functions as a tumor promoter in various cancers, including glioma,11,26 endometrial cancer,12 choriocarcinoma,14 gastric and lung cancer,13 the opposite phenomenon was also reported in colorectal cancer.15 The discrepancies may due to differences in the cancer types involved in the studies. Therefore, to unequivocally illustrate the specific role of PME-1 in HCC, we think it is more appropriate to directly investigate the prognostic value of PME-1 expression in patients with HCC. Consequently, in our study, Cox proportional hazard regression model was used to analyze predictors of HCC. Our results clearly showed that the survival rate of patients with HCC having higher PME-1 expression was significantly shorter than those with lower PME-1 expression. Overall, the unexpected role for PME-1 in colorectal cancer is intriguing and calls for a careful examination of cancer-specific function for PME-1 when considering its role as biomarkers and potential targets for future cancer therapies. To the best of our knowledge, this is the first study analyzing the prognostic value of the PME-1 expression in HCC. Together with other studies of PME-1, our study provided insight into the role of PME-1 expression in various cancer types. However, as we did not explore the underlying mechanism of the function of PME-1 in HCC, future in vitro and in vivo experiments are needed to investigate the mechanism in depth.
In this study, we also found that PME-1 protein and mRNA were up-regulated in HCC tissues compared to adjacent non-tumor tissues. A previous study demonstrates that deubiquitinating enzyme USP36 binds to and regulates PME-1 through its deubiquitinating enzyme activity.27 Analysis of USP36 protein expression in clinical specimens from the Human Protein Atlas (www.proteinatlas.org) showed that USP36 is a high expression in HCC. Hence, we speculate that the up-regulation of PME-1 in HCC may be due to USP36, which need further verified.
In conclusion, we found that PME-1 protein and mRNA were abnormal high expresses in HCC, which was associated with the differentiation, tumor number, intrahepatic or extrahepatic metastasis and recurrence. Survival analysis showed that higher expression of PME-1 was significantly associated with poor survival in patients with HCC.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 81871910), Health commission of Hubei Province Scientific Research Project (No. WJ2019M234), Nature Science Foundation of Hubei Province (No. 2019CFB642) and the Project of Wuhan Young and Middle-aged Medical Backbone Talents (No. 2019-87).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66(4):271–289. doi:10.3322/caac.21349
2. Bruix J, Gores GJ, Mazzaferro V. Hepatocellular carcinoma: clinical frontiers and perspectives. Gut. 2014;63(5):844–855. doi:10.1136/gutjnl-2013-306627
3. Yabe R, Tsuji S, Mochida S, et al. A stable association with PME-1 may be dispensable for PP2A demethylation-implications for the detection of PP2A methylation and immunoprecipitation. FEBS Open Bio. 2018;8(9):1486–1496. doi:10.1002/2211-5463.12485
4. Ortega-Gutiérrez S, Leung D, Ficarro S, Peters EC, Cravatt BF. Targeted disruption of the PME-1 gene causes loss of demethylated PP2A and perinatal lethality in mice. PLoS One. 2008;3(7):e2486. doi:10.1371/journal.pone.0002486
5. Yabe R, Miura A, Usui T, et al. Protein phosphatase methyl-esterase PME-1 protects protein phosphatase 2A from ubiquitin/proteasome degradation. PLoS One. 2015;10(12):e0145226. doi:10.1371/journal.pone.0145226
6. Park HJ, Lee KW, Oh S, et al. Protein phosphatase 2A and its methylation modulating enzymes LCMT-1 and PME-1 are dysregulated in tauopathies of progressive supranuclear palsy and Alzheimer disease. J Neuropathol Exp Neurol. 2018;77(2):139–148. doi:10.1093/jnen/nlx110
7. Xia X, Gholkar A, Senese S, Torres JZ. A LCMT1-PME-1 methylation equilibrium controls mitotic spindle size. Cell Cycle. 2015;14(12):1938–1947. doi:10.1080/15384101.2015.1026487
8. Lipina C, Hundal HS. Carnosic acid stimulates glucose uptake in skeletal muscle cells via a PME-1/PP2A/PKB signalling axis. Cell Signal. 2014;26(11):2343–2349. doi:10.1016/j.cellsig.2014.07.022
9. Sontag JM, Nunbhakdi-Craig V, Mitterhuber M, Ogris E, Sontag E. Regulation of protein phosphatase 2A methylation by LCMT1 and PME-1 plays a critical role in differentiation of neuroblastoma cells. J Neurochem. 2010;115(6):1455–1465. doi:10.1111/j.1471-4159.2010.07049.x
10. Kaur A, Westermarck J. Regulation of protein phosphatase 2A (PP2A) tumor suppressor function by PME-1. Biochem Soc Trans. 2016;44(6):1683–1693. doi:10.1042/BST20160161
11. Puustinen P, Junttila MR, Vanhatupa S, et al. PME-1 protects extracellular signal-regulated kinase pathway activity from protein phosphatase 2A-mediated inactivation in human malignant glioma. Cancer Res. 2009;69(7):2870–2877. doi:10.1158/0008-5472.CAN-08-2760
12. Wandzioch E, Pusey M, Werda A, et al. PME-1 modulates protein phosphatase 2A activity to promote the malignant phenotype of endometrial cancer cells. Cancer Res. 2014;74(16):4295–4305. doi:10.1158/0008-5472.CAN-13-3130
13. Li J, Han S, Qian Z, et al. Genetic amplification of PPME1 in gastric and lung cancer and its potential as a novel therapeutic target. Cancer Biol Ther. 2014;15(1):128–134. doi:10.4161/cbt.27146
14. Hsieh YT, Chou MM, Chen HC, Tseng JJ. IMP1 promotes choriocarcinoma cell migration and invasion through the novel effectors RSK2 and PPME1. Gynecol Oncol. 2013;131(1):182–190. doi:10.1016/j.ygyno.2013.07.106
15. Kaur A, Elzagheid A, Birkman EM, et al. Protein phosphatase methylesterase-1 (PME-1) expression predicts a favorable clinical outcome in colorectal cancer. Cancer Med. 2015;4(12):1798–1808. doi:10.1002/cam4.541
16. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
17. Llovet JM, Zucman-Rossi J, Pikarsky E, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2016;2:16018. doi:10.1038/nrdp.2016.18
18. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66(2):115–132. doi:10.3322/caac.21338
19. Zhang S, Li J, Yin ZY, et al. Expression pattern and clinicopathologic significance of NKD1 in human primary hepatocellular carcinoma. APMIS. 2015;123(4):315–320. doi:10.1111/apm.12360
20. Liu X, Chen S, Tu J, Cai W, Xu Q. HSP90 inhibits apoptosis and promotes growth by regulating HIF-1α abundance in hepatocellular carcinoma. Int J Mol Med. 2016;37(3):825–835. doi:10.3892/ijmm.2016.2482
21. Haynes HR, White P, Hares KM, et al. The transcription factor PPARα is overexpressed and is associated with a favourable prognosis in IDH-wildtype primary glioblastoma. Histopathology. 2017;70(7):1030–1043. doi:10.1111/his.13142
22. Goh GB, Chang PE, Tan CK. Changing epidemiology of hepatocellular carcinoma in Asia. Best Pract Res Clin Gastroenterol. 2015;29(6):919–928. doi:10.1016/j.bpg.2015.09.007
23. Jin N, Shi R, Jiang Y, et al. Glycogen synthase kinase-3β suppresses the expression of protein phosphatase methylesterase-1 through β-catenin. Aging (Albany NY). 2019;11(21):9672–9688. doi:10.18632/aging.102413
24. Sun J, Guo Y, Bie B, et al. Silencing of long noncoding RNA HOXD-AS1 inhibits proliferation, cell cycle progression, migration and invasion of hepatocellular carcinoma cells through MEK/ERK pathway. J Cell Biochem. 2020;121(1):443–457. doi:10.1002/jcb.29206
25. Jiang H, Zhou Z, Jin S, et al. PRMT9 promotes hepatocellular carcinoma invasion and metastasis via activating PI3K/Akt/GSK-3β/Snail signaling. Cancer Sci. 2018;109(5):1414–1427. doi:10.1111/cas.13598
26. Kaur A, Denisova OV, Qiao X, et al. PP2A inhibitor PME-1 drives kinase inhibitor resistance in glioma cells. Cancer Res. 2016;76(23):7001–7011. doi:10.1158/0008-5472.CAN-16-1134
27. Kim SY, Choi J, Lee DH, Park JH, Hwang YJ, Baek KH. PME-1 is regulated by USP36 in ERK and Akt signaling pathways. FEBS Lett. 2018;592(9):1575–1588. doi:10.1002/1873-3468.13039
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.