Back to Journals » OncoTargets and Therapy » Volume 13
Expression of PD-1 and PD-L1 on Tumor-Infiltrating Lymphocytes Predicts Prognosis in Patients with Small-Cell Lung Cancer
Authors Sun C, Zhang L ![]() , Zhang W
, Zhang W ![]() , Liu Y, Chen B, Zhao S, Li W, Wang L, Ye L, Jia K, Wang H, Wu C, He Y
, Liu Y, Chen B, Zhao S, Li W, Wang L, Ye L, Jia K, Wang H, Wu C, He Y ![]() , Zhou C
, Zhou C
Received 1 March 2020
Accepted for publication 28 May 2020
Published 3 July 2020 Volume 2020:13 Pages 6475—6483
DOI https://doi.org/10.2147/OTT.S252031
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Takuya Aoki
Chenglong Sun,1– 3,* Liping Zhang,4,* Wei Zhang,4,* Yu Liu,3,5 Bin Chen,3 Sha Zhao,3 Wei Li,3 Lei Wang,3 Lingyun Ye,3 Keyi Jia,3,5 Hao Wang,3,5 Chunyan Wu,4 Yayi He,3 Caicun Zhou3
1Medical College of Soochow University, Suzhou 215123, Jiangsu, People’s Republic of China; 2Anhui No.2 Provincial People’s Hospital, Hefei 230041, Anhui, People’s Republic of China; 3Department of Medical Oncology, Shanghai Pulmonary Hospital, Tongji University Medical School Cancer Institute, Tongji University School of Medicine, Shanghai 200433, People’s Republic of China; 4Pathology Department, Shanghai Pulmonary Hospital, Tongji University Medical School Cancer Institute, Tongji University School of Medicine, Shanghai 200433, People’s Republic of China; 5Medical School, Tongji University, Shanghai 200433, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yayi He
Department of Medical Oncology, Shanghai Pulmonary Hospital, Tongji University Medical School Cancer Institute, Tongji University School of Medicine, No. 507 Zhengmin Road, Shanghai 200433, People’s Republic of China
Tel +13818828623
Email [email protected]
Caicun Zhou
Department of Medical Oncology, Shanghai Pulmonary Hospital, Tongji University Medical School Cancer Institute, Tongji University School of Medicine, No. 507 Zhengmin Road, Shanghai 200433, People’s Republic of China
Tel +13301825532
Email [email protected]
Introduction: Immune therapy has shown good results in small-cell lung cancer (SCLC), but the impact of immune microenvironment of the disease is unclear. In this work, we detected expression of programmed death 1 (PD-1), PD-ligand 1 (PD-L1), and other immune biomarkers of cancer. We also analyzed the correlations between these markers and survival in SCLC.
Patients and Methods: Protein expression of PD-1, PD-L1, PD-L2, CD3, CD4, CD8, and FOXP3 was analyzed in surgical tissues from 102 SCLC patients by immunohistochemistry.
Results: Positive expression of PD-1 on tumor-infiltrating lymphocytes (TILs) was found in 40.2% of patients; 37.3% of patients showed positive expression of PD-L1 on TILs; and 3.9% showed positive expression of PD-L1 on tumor cells. PD-L2 protein was not expressed on tumor cells or TILs. Survival analysis showed that positive expression of PD-L1 on TILs was correlated with longer relapse-free survival (RFS) (p=0.004). Positive expression of PD-1 combined with a high ratio of lymphocytes (CD3, p=0.004; CD4, p=0.011; CD8, p=0.009; FOXP3, p=0.009) was associated with significantly better RFS than negative expression of PD-1 combined with a lower ratio of lymphocytes. Positive expression of PD-L1 combined with a high ratio of lymphocytes (CD3, p< 0.001; CD4, p=0.001; CD8, p=0.002; FOXP3, p=0.001) was associated with significantly better RFS than negative expression of PD-L1 combined with a lower ratio of lymphocytes. All patients’ stage were between I and III.
Conclusion: PD-1 and PD-L1 expression might be good prognostic factors in SCLC.
Keywords: small-cell lung cancer, SCLC, programmed death-1, PD-1, programmed death-ligand 1, PD-L1, programmed death-ligand 2, PD-L2, tumor-infiltrating lymphocytes, TILs
Introduction
The incidence and mortality of lung cancer are increasing. Fifteen percent of lung cancer patients have small-cell lung cancer (SCLC).1 The standard treatment for advanced extensive SCLC is chemotherapy,2 which shows a high but transient response rate.3 The options for subsequent-line treatment are limited. There is thus an urgent need to develop new treatments for patients with SCLC. Research on immune therapy combined with chemotherapy for SCLC is ongoing: IMPOWER-133 showed better prognosis in patients receiving etoposide/carboplatin/atezolizumab treatment;4 and the CASPIAN study indicated that a combination of first-line programmed death ligand 1 (PD-L1) inhibitors with chemotherapy increased overall survival (OS).5 Although immunotherapy showing the antitumor activity on SCLC in some studies,6,7 but SCLC patients did not benefit greatly from ICI compared with NSCLC patients. The implications of immune microenvironment of SCLC remain uncertain.
In this study, we detected protein expression of programmed death 1 (PD-1), PD-L1, PD-L2, CD3, CD4, CD8, and FOXP3 in 102 SCLC patients using immunohistochemistry (IHC). The correlations between PD-1/PD-L1 and pathological features were analyzed. We also performed survival analysis in these patients.
Patients and Methods
Patients
A total of 102 SCLC patients who underwent surgery in Shanghai Pulmonary Hospital from January 2014 to December 2018 were retrospectively enrolled in our study. SCLC was diagnosed by two pathologists (“L.Z. and C.W.”). Patients did not receive radiation or chemotherapy before surgery. We reviewed patient data and determined TNM stage based on the International Association for the Study of Lung Cancer version 8. All patient’s stage was between I and III that was determined after the operation. All patients were provided with written informed consent. The ethics committee of Shanghai Pulmonary Hospital approved this study. The study was performed in accordance with the International Conference on Harmonisation Guidelines on Good Clinical Practice and the Declaration of Helsinki.
Immunohistochemistry
Experimental Antibodies and Configuration Conditions
Rabbit anti-human PD-1 (1:100, Golden Bridge Zhongshan, Beijing ZM-0381), PD-L1 (E1L3N 1: 300, CST # 13684S), PD-L2 (1: 200, CST # 82723S), CD3 (1:100, Dako A0452), CD4 (1:80, Dako M7310), CD8 (1:100, Dako M7103), and FOXP3 (1:100, BioLegend 320,101) antibodies were used.
The IHC route was as follows. Formalin-fixed paraffin-embedded tissue slides were dewaxed with xylene followed by alcohol, and rinsed with distilled water. Antigens were recovered with a target retrieval solution kit (DM828 or DM829, Dako) under heat and high pressure for 10 min. After cooling to room temperature, slides were immersed in 0.3% H2O2 to reduce background staining. The slides were then incubated with primary antibody for 1 h at room temperature. After rinsing with phosphate-buffered saline (PBS), they were incubated with horseradish peroxidase-conjugated goat anti-Mouse/Rabbit IgG detection antibody for a further 30 min at room temperature. After rinsing again with PBS, antigens were visualized with DAB, following standard procedures for counterstaining cell nuclei with hematoxylin and mounting cover slides. IHC was performed by Wei Zhang and Chenglong Sun.
PD-1, PD-L1, PD-L2, CD3, CD4, CD8, and FOXP3 IHC Cutoff Values
IHC scores were independently determined by two experienced pathologists (Liping Zhang and Chunyan Wu). A positive result was defined as staining on tumor-infiltrating lymphocytes (TILs) of more than 1% for PD-1 or more than 5% for PD-L1, or staining on tumor cells of more than 40% for CD3, more than 30% for CD4, more than 30% for CD8, or more than 10% for FOXP3. We used survival analysis to determine the best cutoff points by maximizing statistical differences in relapse-free survival (RFS).8,9
Statistical Analyses
We performed statistical analyses using SPSS 25.0 (IBM) and GraphPad Prism version 8.0 (GraphPad Software, Inc) for Mac OS. A chi-square test was used to assess correlations between immune-marker expression and clinical characteristics. The Kaplan–Meier method was used to construct patient survival curves. Survival analysis was performed by Log-rank test. Univariate and multivariate Cox proportionate hazard models were used to identify factors significantly related to RFS. Logistic regression was used to estimate the correlations between immune marker expression levels. p<0.05 was considered to indicate statistical significance. All statistical tests were double-sided.
Results
Patient Characteristics
A total of 102 patients were enrolled. There were 17.6% female and 82.4% male patients, and 23 were over the age of 70 years. The median age was 62 years. Fifty-eight (56.9%) patients had never smoked. All patients were stage I–III: 60 (58.8%) were stage I or II, and 42 (47.1%) were stage III. Fifty-four patients received postoperative adjuvant chemotherapy (Table 1).
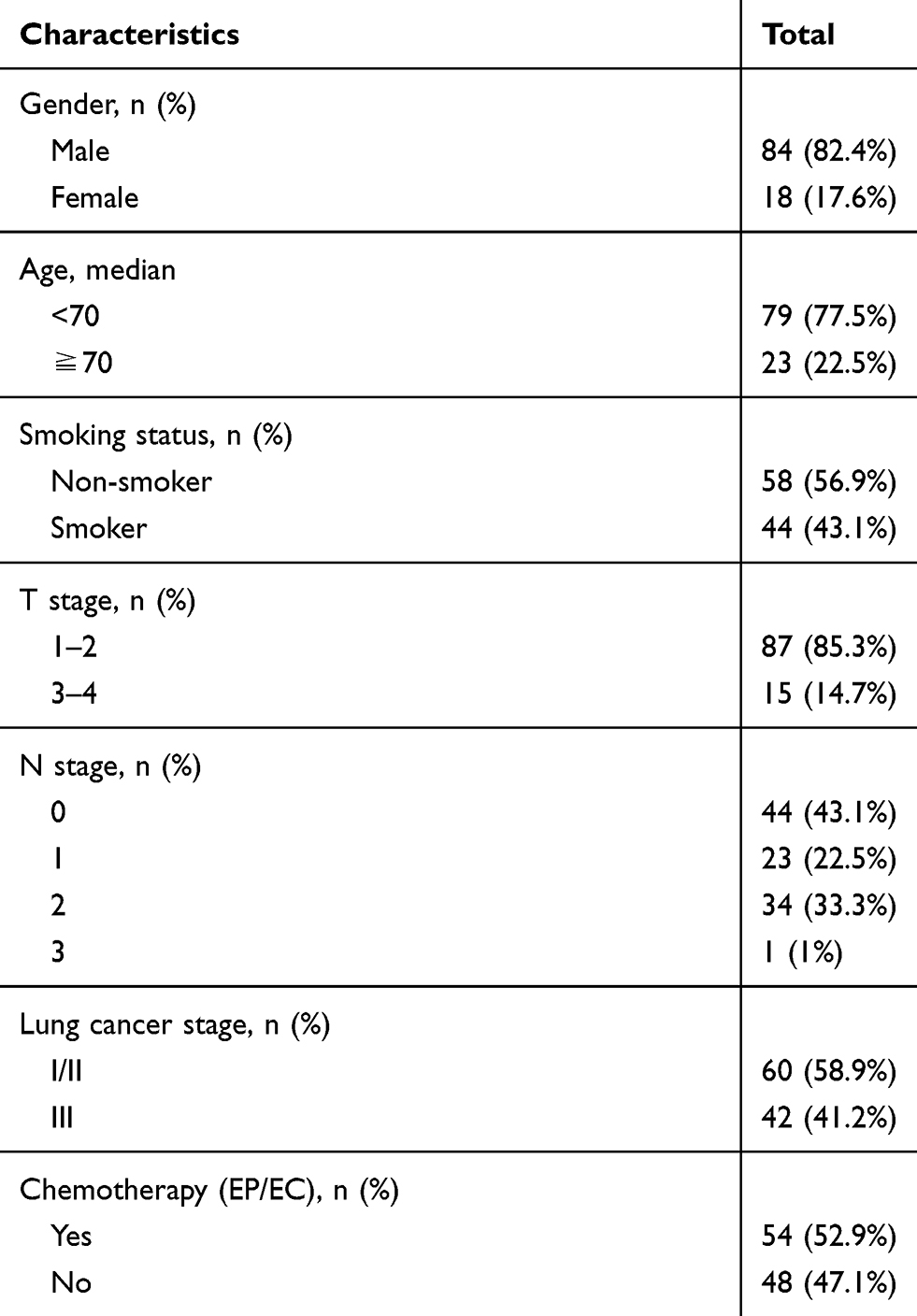 |
Table 1 Patient Characteristics (n=102) |
CD3, CD4, CD8, FOXP3, PD-1, PD-L1, and PD-L2 Expression and Correlations with Clinicopathological Data
CD3+ TILs were observed in 54/102 (52.9%) SCLC specimens, CD4+ TILs in 38/102 (37.3%), CD8+ TILs in 33/102 (32.4%), and FOXP3+ TILs in 35/102 (34.3%) (Figure 1).
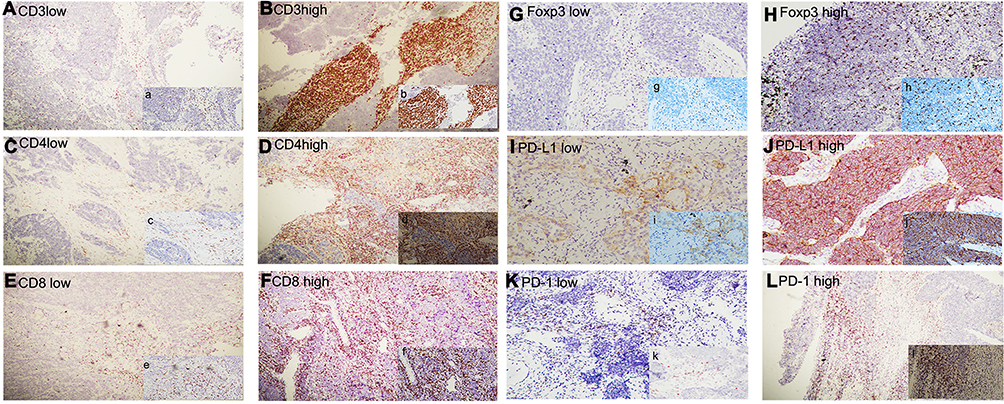 |
Figure 1 CD3, CD4, CD8, FOXP3, PD-1 were expressed on TILS, (A) low expression of CD3*4, (a) low expression of CD3*10; (B) high expression of CD3*4, (b) high expression of CD3*10; (C) low expression of CD4*4, (c) low expression of CD4*10; (D) high expression of CD4*4, (d) high expression of CD4*10; (E) low expression of CD8*4, (e) low expression of CD8*10; (F) high expression of CD8*4, (f) high expression of CD8*10; (G) low expression of FOXP3*10, (g) low expression of FOXP3*20; (H) high expression of FOXP3*10, (h) high expression of FOXP3*20; (K) low expression of PD-1*10, (k) low expression of PD-1*20; (L) high expression of PD-1*10, (l) high expression of PD-1*20; PD-L1 was expressed on Tumors; (I) low expression of PD-L1*10, (i) low expression of PD-L1*20; (J) high expression of PD-L1*10, (j) high expression of PD-L1*20. Abbreviations: PD-1, programed death-1; PD-L1, programed death-ligand 1; TILs, tumor-infiltrating lymphocytes. |
Positive expression of PD-1 on TILs was observed in 40.2% of patients; 37.3% showed positive expression of PD-L1 on TILs, and 3.9% showed positive expression of PD-L1 on tumor cells. PD-1 was not expressed on tumor cells, PD-L2 was not expressed on tumor cells or TILs in SCLC (Figure 2).
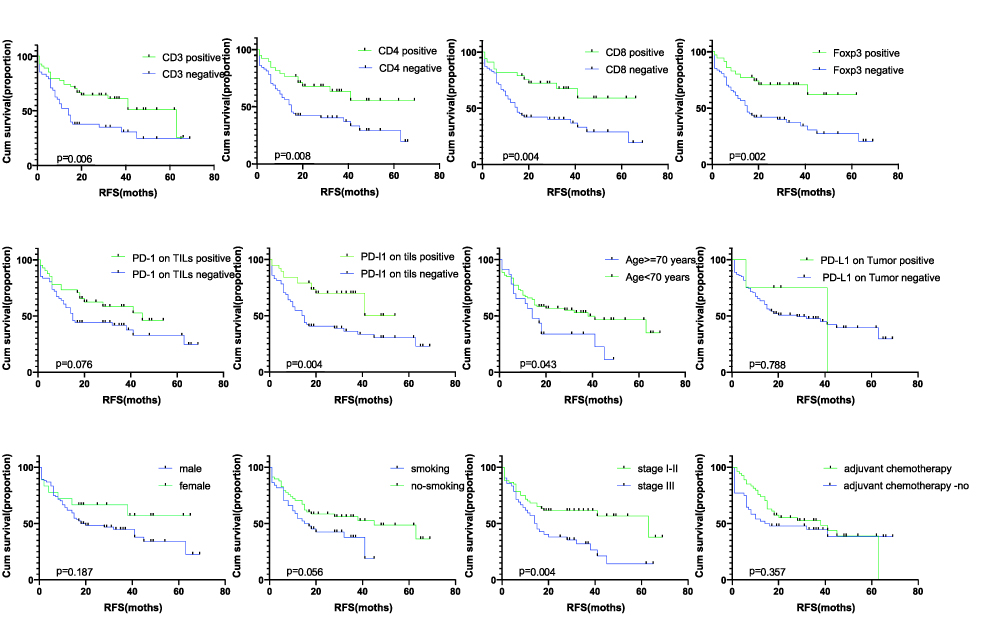 |
Figure 2 Kaplan–Meier analysis for RFS of SCLC patients based on expression of the CD3 on TILs, CD8 on TILs, FOXP3 on TILs, PD-1 on TILs, PD-L1 on TILs, PD-L1 on tumor cells, age, gender, smoking status, stage, adjuvant chemotherapy. The respective Log rank P values are indicated in the chart. Abbreviations: RFS, relapse-free survival; PD-1, programed death-1; PD-L1, programed death-ligand 1; TILs, tumor-infiltrating lymphocytes; SCLC, small-cell lung cancer. |
PD-1 expression on TILs was extensively correlated with stage (p=0.045). The expression of PD-1 on TILs showed significant correlation with CD3 (p<0.001), CD4 (p<0.001), CD8 (p<0.001), and FOXP3 (p<0.001). PD-L1 expression on TILs had significant correlation with CD3 (p<0.001), CD4 (p<0.001), CD8 (p<0.001), FOXP3 (p<0.001), and PD-1 (p<0.001). PD-1 and PD-L1 expression on TILs were not related to age, gender, or smoking status (Figure 3, Table 2). Bivariate logistic regression of TIL PD-L1 and PD-1 expression.
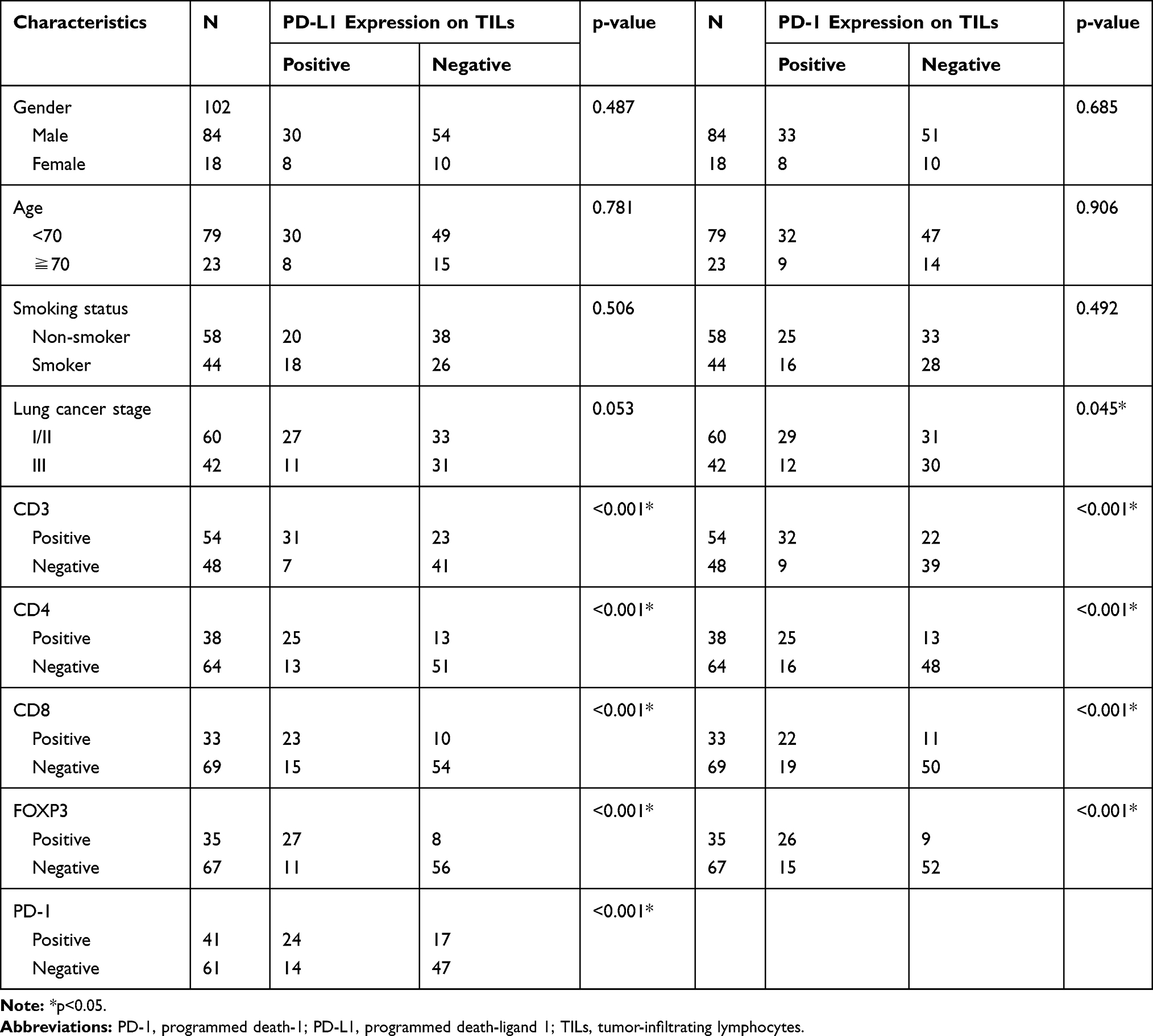 |
Table 2 Relationship Between PD-L1 and PD-1 Expression on TILs and Various Patient Characteristics |
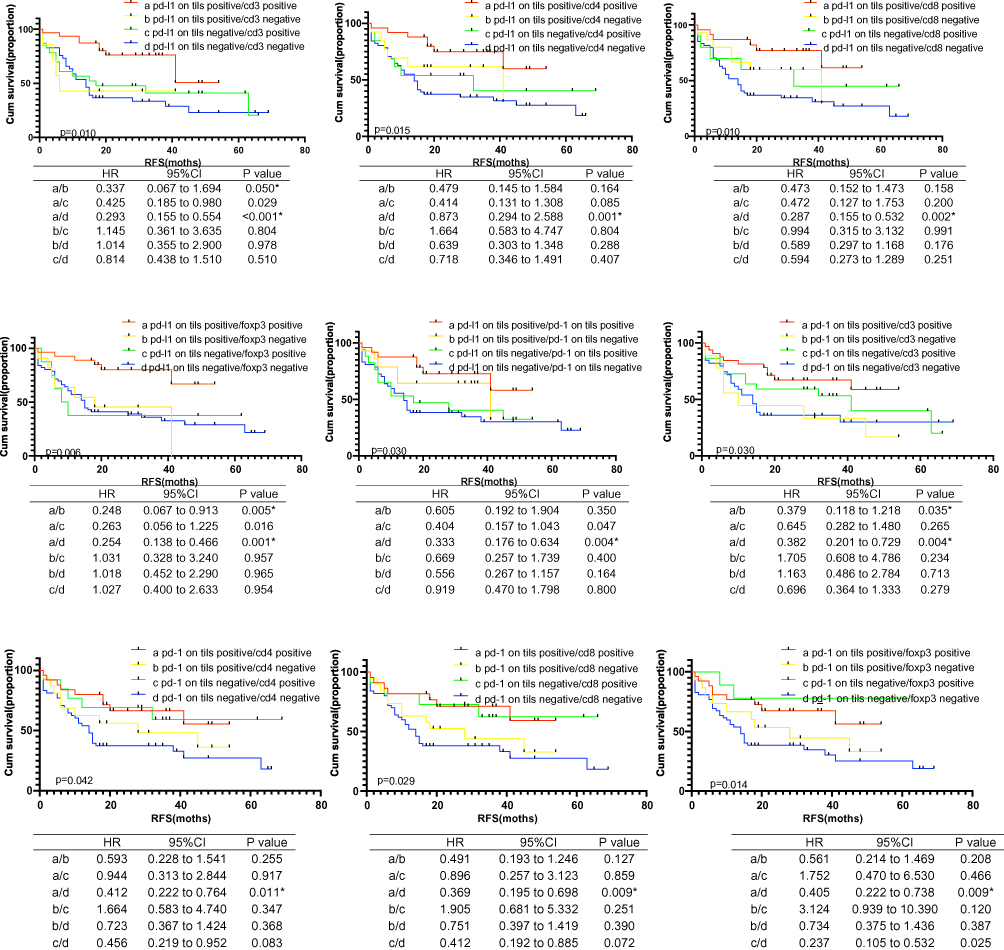 |
Figure 3 Kaplan–Meier analysis for RFS of SCLC patients based on the two by two combination of the following markers: PD-1 on TILs, PD-L1 on TILs, CD3 on TILs, CD4 on TILs, CD8 on TILs, FOXP3 on TILs and PD-L1 on tumor cells. The respective Log Rank P values are shown in the chart. Abbreviations: RFS, relapse-free survival; PD-1, programed death-1; PD-L1, programed death-ligand 1; TILs, tumor-infiltrating lymphocytes; SCLC, small-cell lung cancer. |
The expression of PD-L1 on TILs was correlated with CD3 (p=0.001; R2=0.25), CD4 (p=0.001; R2=0.257), CD8 (p=0.001; R2=0.271), FOXP3 (p=0.001; R2=0.423), and PD-1 (p=0.001; R2=0.166). The expression of PD-1 on TILs was correlated with CD3 (p=0.001; R2=0.217), CD4 (p=0.001; R2=0.205), CD8 (p=0.001; R2=0.182), and FOXP3 (p=0.001; R2=0.314) (Table 3).
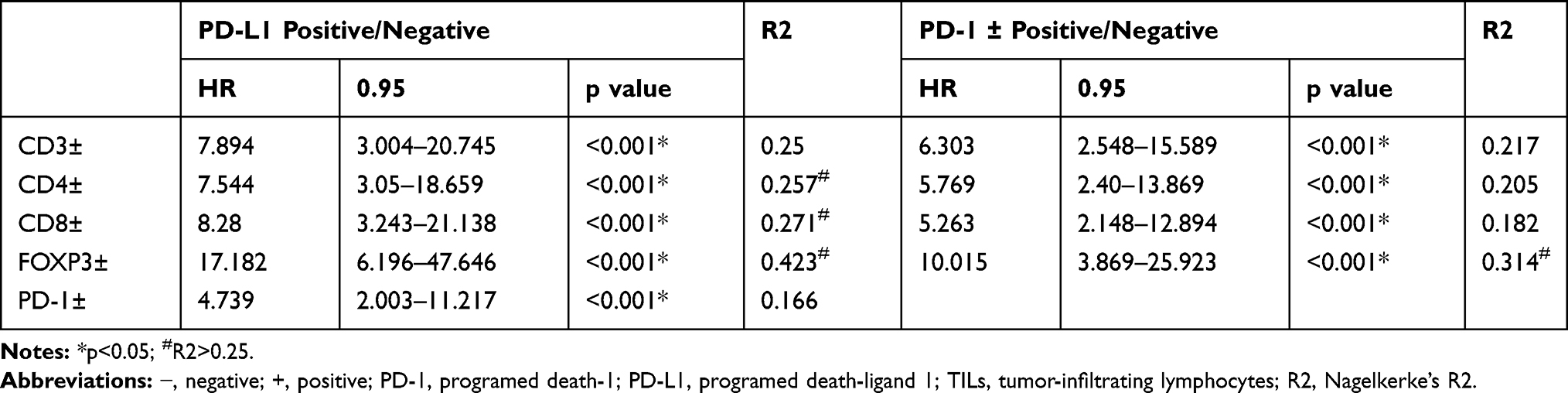 |
Table 3 Bivariate Logistic Regression of TILs PD-L1 and PD-1 Expression |
Survival Analysis
We used univariate and multivariate regression to analyze clinical factors and expression of immune biomarkers. Stage (I/II vs III) could predict RFS (univariate analysis: hazard ratio (HR) 2.111, 95% CI 1.243–3.586, p=0.006; multivariate analysis: HR 1.890, 95% CI 1.100–3.220, p=0.021). The expression of CD3, CD4, CD8, FOXP3, and PD-L1 on TILs was significant in univariate Cox regression (CD3 p=0.007; CD4 p=0.010; CD8 p=0.007; FOXP3 p=0.004; PD-L1 p=0.006) but not in multivariate Cox regression (Table 4).
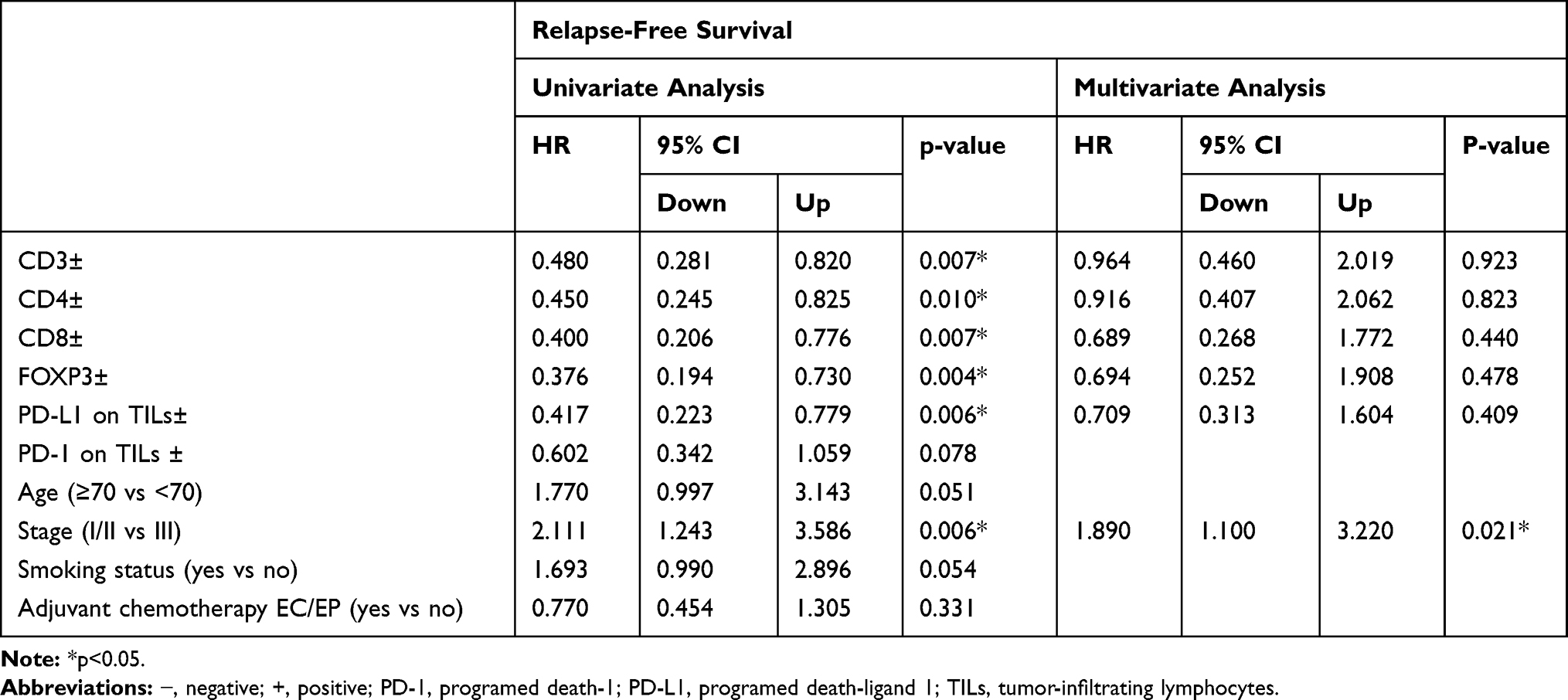 |
Table 4 Cox Regression Analysis |
Clinicopathological factors and immune biomarkers were analyzed with respect to RFS. Age (p=0.043), stage (p=0.004), CD3 (p=0.006), CD4 (p=0.008), CD8 (p=0.004), FOXP3 (p=0.002), and PD-L1 on TILs (p=0.004) were significantly correlated with RFS. Smoking status (p=0.056), gender (p=0.187), adjuvant chemotherapy (p=0.357), PD-1 on TILs (p=0.076), and PD-L1 on tumor cells (p=0.788) had no significant association with RFS (Figure 3).
We divided patients into subgroups by PD-L1 and PD-1 expression on TILs (Figure 4) combined with CD3, CD4, CD8, and FOXP3. Positive expression of PD-1 or PD-L1 combined with a higher ratio of CD3, CD4, CD8, and FOXP3 was associated with higher RFS than was negative expression of PD-1 or PD-L1 combined with a lower ratio of CD3, CD4, CD8, and FOXP3.
Positive expression of PD-1 combined with a higher ratio of lymphocytes (CD3 p=0.004; CD4 p=0.011; CD8 p=0.009; FOXP3 p=0.009) was associated with significantly better RFS than negative expression of PD-1 combined with a lower ratio of lymphocytes. Positive expression of PD-L1 combined with a higher ratio of lymphocytes (CD3 p<0.001; CD4 p=0.001; CD8 p=0.002; FOXP3 p=0.001) was associated with significantly better RFS than negative expression of PD-L1 combined with a lower ratio of lymphocytes. There was a significant difference in RFS for positive vs negative PD-L1 and PD-1 expression on TILs (p=0.004). These results indicate that PD-L1 and PD-1 expression on TILs combined with expression of CD3, CD4, CD8, and FOXP3 represent important biomarkers that could be used to predict RFS in SCLC. All patients in this study received surgical resection of their lesion in early stage. Most of the them failed to reach the end point of OS, so we did not analyze the OS data.
Discussion
In this survey, we detected the expression of PD-1, PD-L1, CD3, CD4, CD8, and FOXP3. We also analyzed the correlations between PD-1, PD-L1, CD3, CD4, CD8, and FOXP3 and survival in SCLC patients.
PD-1 and PD-L1 expression have been detected in non-small-cell lung cancer (NSCLC)10,11 and SCLC,12,13 with PD-L1 expression in SCLC varying greatly. One study of 61 samples found 0% PD-L1 protein expression,14 whereas another study of 102 patients reported a value of 71.6%.15 In this study, we detected not only the expression of PD-1 and PD-L1 but also that of PD-L2, CD3, CD4, CD8, and FOXP3 in SCLC. Furthermore, for the first time, we performed subgroup analysis of the expression of PD-1 or PD-L1 combined with the ratio of lymphocytes and analyzed the relationships with RFS.
In our study, 40.2% of patients showed positive expression of PD-1 and 37.3% showed positive expression of PD-L1 on TILs; 3.9% of patients showed positive expression of PD-L1 on tumor cells. Our results are consistent with former findings.13,16 PD-L2 protein expression was not examined in the 102 surgical samples, in either tumor cells or TILs. Previous studies have shown 39.5% PD-L2 expression in SCLC,17 compared with 47–52.8% in NSCLC.18,19 This might be related to the heterogeneity of immune checkpoint expression in tumor tissue.
It has been reported that PD-L1 expression and clinicopathological features have no correlation in lung malignancies.20 In our study, the correlations between PD-1 or PD-L1 expression and immune cells were evaluated. In our previous research, PD-L1 expression showed no substantial effect on OS in NSCLC,11 and Carvajal-Hausdorf et al showed that PD-L1 protein had no substantial effect on 5-year OS in SCLC.12 In another study, high PD-L1 expression was shown to be associated with better OS.21 In the current study, positive expression of PD-L1 on TILs was more favorable than negative expression with respect to RFS, consistent with the results of Cooper et al.21 This might have been because our patients were mostly in the early stages of the disease.
Our results also revealed that higher expression levels of CD3, CD4, CD8, and FOXP3 were associated with better survival, suggesting that TILs could increase antitumor efficacy. TILs are important predictors of malignancy.22 High expression of CD3 has been shown to be associated with a good prognosis in SCLC.12,13 CD3, CD4, and CD8 T cell infiltration functions as an independent predictor of a favorable result in breast cancer and esophageal carcinomas.22,23 High TIL infiltration of CD8 was associated with longer OS in NSCLC patients.24,25 The transcription factor FOXP3 is a marker of regulatory T cells. Some studies have indicated an association between FOXP3 and favorable prognosis;26–28 a FOXP3-positive group had a better 5-year OS than the FOXP3-negative group in tonsillar squamous cell carcinoma.27 Tao et al showed that FOXP3 expression in tumors was related to better prognosis in NSCLC.28 In our study, FOXP3 expression was also associated with better RFS.
In the analysis of RFS subgroups, significant differences were found between groups. Positive expression of PD-1 or PD-L1 combined with a higher ratio of lymphocytes was associated with significantly better RFS than negative expression of PD-1 or PD-L1 combined with a lower ratio of lymphocytes. The combination of PD-L1- and CD8-positive TILs (PD-L1+/CD8+) has been suggested to have predictive value in patients with NSCLC, as patients with high PD-L1+/CD8+ expression have improved survival.24 A low PD-L1+/CD8+ expression group had poor progression-free survival, whereas that of the high PD-L1−/CD8+ expression group was better.25
To the best of our knowledge, this is the first study of immune cells and PD-1 or PD-L1 expression in SCLC. We found that positive expression of PD-1 or PD-L1 combined with a higher ratio of certain immune cells (CD3, CD4, CD8, and FOXP3) was associated with significantly better survival.
Our study had some limitations. Tumor tissues were all from Shanghai Pulmonary Hospital, so the results may not be representative of the wider population. The cut-off was established using the best value for RFS; OS should also be analyzed.
To conclude, PD-1 and PD-L1 were shown to be critical elements in SCLC that represent potential markers. The correlations among PD-1, PD-L1, and immune cells were evaluated, showing that the expression of PD-1 or PD-L1 on TILs was related to CD3, CD4, CD8, and FOXP3. In the survival analysis, a combination of positive expression of PD-L1 or PD-1 with a higher ratio of immune cells (CD3, CD4, CD8, and FOXP3) was associated with a better RFS than negative expression of PD-L1 or PD-1 combined with a lower ratio of immune cells.
Acknowledgments
This study was supported in part by the Key Program of Natural Science Research of Anhui Provincial Education Department (KJ2018A0813), a grant from the National Natural Science Foundation of China (81802255), the Shanghai Pujiang Program (17PJD036), a grant from the Shanghai Municipal Commission of Health and Family Planning Program (20174Y0131), the National Key Research & Development Project (2016YFC0902300), the major disease clinical skills enhancement program three year action plan for promoting clinical skills and clinical innovation in municipal hospitals, Shanghai Shen Kang Hospital Development Center Clinical Research Plan of SHDC (16CR1001A), the “Dream Tutor” Outstanding Young Talents Program (fkyq1901), Key Disciplines of Shanghai Pulmonary Hospital (2017ZZ02012), and a grant from the Shanghai Science and Technology Commission (16JC1405900). Chenglong Sun, Liping Zhang, and Wei Zhang are co-first authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Alvarado-Luna G, Morales-Espinosa D. Treatment for small cell lung cancer, where are we now?—a review. Transl Lung Cancer Res. 2016;5(1):26–38. doi:10.3978/j.issn.2218-6751.2016.01.13
2. Rossi A, Di Maio M, Chiodini P, et al. Carboplatin or cisplatin based chemotherapy in first line treatment of small cell lung cancer. J Clin Oncol. 2012;30(14):1692–1698. doi:10.1200/JCO.2011.40.4905
3. Roth BJ, Johnson DH, Einhorn LH, et al. Randomized study of cyclophosphamide, doxorubicin, and vincristine versus etoposide and cisplatin versus alternation of these two regimens in extensive small-cell lung cancer: a phase III trial of the Southeastern cancer study group. J Clin Oncol. 1992;10(2):282–291. doi:10.1200/JCO.1992.10.2.282
4. Horn L, Mansfield AS, Szczęsna A, et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. 2018;379(23):2220–2229. doi:10.1056/NEJMoa1809064
5. Paz-Ares L, Dvorkin M, Chen Y, et al. Durvalumab plus platinum–etoposide versus platinum–etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. 2019;394(10212):1929–1939. doi:10.1016/S0140-6736(19)32222-6
6. Antonia SJ, López-Martin JA, Bendell J, et al. Nivolumab alone and nivolumab plus ipilimumab in recurrent small-cell lung cancer (CheckMate 032): a multicentre, open-label, phase 1/2 trial. Lancet Oncol. 2016;17(7):883–895. doi:10.1016/S1470-2045(16)30098-5
7. Ott PA, Elez E, Hiret S, et al. Pembrolizumab in patients with extensive-stage small-cell lung cancer: results from the phase Ib KEYNOTE-028 study. J Clin Oncol. 2017;35(34):3823–3829. doi:10.1200/JCO.2017.72.5069
8. He Y, Yu H, Rozeboom L, et al. LAG-3 protein expression in non-small cell lung cancer and its relationship with PD-1/PD-L1 and tumor-infiltrating lymphocytes. J Thorac Oncol. 2017;12(5):814–823. doi:10.1016/j.jtho.2017.01.019
9. He Y, Jia K, Dziadziuszko R, et al. Galectin-9 in non-small cell lung cancer. Lung Cancer. 2019;136:80–85. doi:10.1016/j.lungcan.2019.08.014
10. Gettinger S, Herbst RS. B7-H1/PD-1 blockade therapy in non-small cell lung cancer: current status and future direction. Cancer J. 2014;20(4):281–289. doi:10.1097/PPO.0000000000000063
11. He Y, Rozeboom L, Rivard CJ, et al. PD-1, PD-L1 protein expression in non-small cell lung cancer and their relationship with tumor infiltrating lymphocytes. Med Sci Monit. 2017;23:1208–1216. doi:10.12659/MSM.899909
12. Carvajal-Hausdorf D, Altan M, Velcheti V, et al. Expression and clinical significance of PD-L1, B7-H3, B7-H4 and TILs in human small cell lung Cancer (SCLC). J Immunother Cancer. 2019;7(1):65. doi:10.1186/s40425-019-0540-1
13. Zhao X, Kallakury B, Chahine JJ, et al. Surgical resection of SCLC: prognostic factors and the tumor microenvironment. J Thorac Oncol. 2019;14(5):914–923. doi:10.1016/j.jtho.2019.01.019
14. Schultheis AM, Scheel. AH, Ozretić L, et al. PD-L1 expression in small cell neuroendocrine carcinomas. Eur J Cancer Clin Oncol. 2015;51:421–426.
15. Ishii H, Azuma K, Kawahara A, et al. Significance of programmed cell death-ligand 1 expression and its association with survival in patients with small cell lung cancer. J Thorac Oncol. 2015;10(10):426–430. doi:10.1097/JTO.0000000000000414
16. Schultheis AM, Scheel AH, Ozretić L, et al. PD-L1 expression in small cell neuroendocrine carcinomas. Eur J Cancer. 2015;51(3):421–426. doi:10.1016/j.ejca.2014.12.006
17. Takamori S, TAKADA K, AZUMA K, et al. Prognostic impact of PD-L2 expression and association with PD-L1 in patients with small-cell lung cancer. Anticancer Res. 2018;38(10):5903–5907. doi:10.21873/anticanres.12934
18. Shinchi Y, Komohara Y, Yonemitsu K, et al. Accurate expression of PD-L1/L2 in lung adenocarcinoma cells: a retrospective study by double immunohistochemistry. Cancer Sci. 2019;110(9):2711–2721. doi:10.1111/cas.14128
19. Calles A, Liao X, Sholl LM, et al. Expression of PD-1 and its ligands, PD-L1 and PD-L2, in smokers and never smokers with KRAS-mutant lung cancer. J Thorac Oncol. 2015;10(12):1726–1735. doi:10.1097/JTO.0000000000000687
20. Konishi J, Yamazaki. K, Azuma M, et al. B7-H1 expression on non-small cell lung cancer cells and its relationship with tumor-infiltrating lymphocytes and their PD-1 expression. Clin Cancer Res. 2004;10(15):5049–5100. doi:10.1158/1078-0432.CCR-04-0428
21. Cooper WA, Tran T, Vilain RE, et al. PD-L1 expression is a favorable prognostic factor in early stage non-small cell carcinoma. Lung Cancer. 2015;89(2):181–188. doi:10.1016/j.lungcan.2015.05.007
22. Rathore AS, Kumar S, Konwar R, Makker A, Negi MP, Goel MM. CD3+, CD4+ & CD8+ tumour infiltrating lymphocytes (TILs) are predictors of favourable survival outcome in infiltrating ductal carcinoma of breast. Indian J Med Res. 2014;140(3):361–369.
23. Schumacher K, Haensch W, Roefzaad C, Schlag PM. Prognostic significance of activated CD8(+) T cell infiltrations within esophageal carcinomas. Cancer Res. 2001;61(10):3932.
24. Yang H, Shi J, Lin D, et al. Prognostic value of PD-L1 expression in combination with CD 8+ TIL s density in patients with surgically resected non-small cell lung cancer. Cancer Med. 2018;7(1):32–45. doi:10.1002/cam4.1243
25. Tokito T, Azuma K, Kawahara A, et al. Predictive relevance of PD-L1 expression combined with CD8+ TIL density in stage III non-small cell lung cancer patients receiving concurrent chemoradiotherapy. Eur J Cancer. 2016;55:7–14. doi:10.1016/j.ejca.2015.11.020
26. Ladoire S, Arnould L, Mignot G, et al. Presence of Foxp3 expression in tumor cells predicts better survival in HER2-overexpressing breast cancer patients treated with neoadjuvant chemotherapy. Breast Cancer Res Treat. 2011;125(1):65–72. doi:10.1007/s10549-010-0831-1
27. Park K, Cho KJ, Lee M, Yoon DH, Kim SB. Importance of FOXP3 in prognosis and its relationship with p16 in tonsillar squamous cell carcinoma. Anticancer Res. 2013;33(12):5667–5673.
28. Tao H, Mimura Y, Aoe K, et al. Prognostic potential of FOXP3 expression in non-small cell lung cancer cells combined with tumor-infiltrating regulatory T cells. Lung Cancer. 2012;75(1):95–101. doi:10.1016/j.lungcan.2011.06.002
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.