Back to Journals » Clinical Interventions in Aging » Volume 18
Exploring Whether Weight-Related Cues Affect Food Intake in Older Adults with Dementia
Authors Kimura A ![]() , Yamaguchi K
, Yamaguchi K ![]() , Tohara H, Sato Y, Sawada N, Nakagawa Y, Matsuda Y, Inoue M, Wada Y, Tamaki K
, Tohara H, Sato Y, Sawada N, Nakagawa Y, Matsuda Y, Inoue M, Wada Y, Tamaki K
Received 8 May 2023
Accepted for publication 21 August 2023
Published 1 September 2023 Volume 2023:18 Pages 1453—1461
DOI https://doi.org/10.2147/CIA.S417254
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Atsushi Kimura,1 Kohei Yamaguchi,2 Haruka Tohara,2 Yusuke Sato,3 Naoko Sawada,3 Yasuhide Nakagawa,3 Yukako Matsuda,4,5 Motoharu Inoue,5 Yuji Wada,6 Kazuhiro Tamaki3,4
1College of Risk Management, Nihon University, Tokyo, Japan; 2Department of Dysphagia Rehabilitation, Tokyo Medical and Dental University, Tokyo, Japan; 3Geriatric Health Services Facility Nanohana, Medical Corporation Kanjinkai, Tokyo, Japan; 4Nanohana Dentistry Clinic, Medical Corporation Kanjinkai, Tokyo, Japan; 5Department of Dysphagia Rehabilitation, Nihon University of Dentistry, Tokyo, Japan; 6College of Gastronomy Management, Ritsumeikan University, Shiga, Japan
Correspondence: Atsushi Kimura, College of Risk Management, Nihon University, Setagaya-ku, Tokyo, 1548513, Japan, Tel +81 3 6453 1600, Fax +81 3 6453 1630, Email [email protected] Kazuhiro Tamaki, Geriatric Health Services Facility Nanohana, Medical Corporation Kanjinkai, Nishitama-Gun, Tokyo, 1901212, Japan, Tel +81 42 568 5111, Fax +81 42 568 5127, Email [email protected]
Purpose: Past research has shown that exposure to the image of a slim person reduces food consumption among young adults. However, it remains unknown whether this paradigm could be adapted and applied to increase food intake among older adults with dementia by exposing them to the image of a higher-weight person to mitigate weight loss and malnutrition. The present study explored whether weight-related visual cues affect the amount of food consumed by older adults with dementia.
Participants and Methods: In the experiment, twenty-one elderly people with dementia living in a nursing home were visually exposed to one of four conditions (a cartoon image of a normal-weight chef, a higher-weight chef, a flower or no image) during real-life daily lunch situations over the course of four weeks, during which each condition was presented for one week.
Results: Results demonstrate that participants finished their meals more frequently when they were exposed to the image of the higher-weight chef than when they were not exposed to any images.
Conclusion: These results suggest that exposure to a cartoon chef character representing a stereotyped social group related to body weight activates the stereotype and increases stereotype-consistent behavior in older adults with dementia. The present findings will contribute to understanding the effect of visual information on eating behavior and to designing eating environments which facilitate sufficient nutrition intake among older adults with dementia.
Keywords: nudge, body weight, dementia, food consumption, dining environment
Introduction
Dementia is any disorder where significant decline from one’s previous level of cognition causes interference in occupational, domestic or social functioning. It is characterized by global cognitive impairment with a decline in memory and at least in one other cognitive domain, such as language, visuospatial function or executive function.1–3 Dementia is one of the most serious diseases of aging, and it is estimated that more than 46 million people are currently living with dementia worldwide; without a way to stop or slow its progression, there is predicted to be a tripling of this number to more than 131 million by 2050.4 Most dementia in the older people is caused by some degree of neurodegeneration. Some common degenerative forms of dementia found in the older people are Alzheimer’s disease, dementia with Lewy bodies, vascular dementia, frontotemporal lobe degeneration and Parkinson’s disease.1,3,4
The risk of weight loss and malnutrition is high in people with dementia.5 As dementia leads to both cognitive and physical decline, nutritional intake is frequently impaired in elderly people with dementia.6–8 These risks also lead to sarcopenia and falls.9,10 Thus, the malnutrition of elderly people with dementia can lead to deterioration of independent activity and can accompany the risk of an increasing number of burdens in their day-to-day lives. Malnutrition in elderly people with dementia may be derived from conditions such as dysphagia; indeed, pre-oral stage disorders are among the major factors.11 Pre-oral stage disorders, which is to say non-eating, unlike oral cavity and pharyngeal disorders, may be difficult to improve with exercises, so it is necessary to adjust the eating environments of elderly patients with such disorders.6,8,12–14 However, there are still few fully effective solutions for pre-oral disorders, and the accompanying malnutrition, in older people with dementia.
With respect to eating environment, it is well known that health- and weight-related cues, such as co-eaters,15–20 advertising,21,22 human-like figures23–28 and cartoon characters29,30 have been shown to affect an individual’s food intake in studies which mainly recruited healthy young adults. For instance, van Kleef et al22 examined the influence of exposure to exercise commercials (eg, running shoes, fitness program) on food intake among college students. They found that exercise commercials could reduce participants’ caloric intake relative to the control condition in which participants were exposed to neutral (no reference to food or exercise) commercials. Bruner and Siegrist23 exposed their participants to an image of a thin, human-like sculpture by Alberto Giacometti during a tasting-chocolate task. These participants consumed less chocolate than participants who were exposed to an image of another piece of artwork. Furthermore, more than 70% of the participants in both conditions reported that they believed their eating behaviors were not at all influenced by the respective pieces of artwork. Thus, the authors concluded that the image of Giacometti’s thin sculpture provided dieting cues despite the participants not being aware of such influences. This “Giacometti effect” has also found in different situations related to food choice and eating behavior.25,27,28 These cues can be considered a “nudge” for orienting healthy eating:26 the effect of cue exposure may occur at a subconscious level and the cognitive activation may occur without awareness.31
However, previous studies in this field are mainly focused on whether the exposure to thin or slim images reduce the amount of food intake among young adults for the purpose of preventing obesity,31 and pay little attention to the reverse: whether the exposure to the image of a higher-weight or plump individual would increase food intake among, for example, older adults with dementia, in order to prevent malnutrition. To explore the influence of images of higher-weight individuals on food choice, Campbell et al29 exposed children from 6 to 14 years old to overweight or normal weight cartoon characters as prime stimuli and found that overweight primes could lead to relatively high levels of snack consumption. These findings led us to postulate that weight-related cues that suggest eating a large amount could promote food intake in general. However, it remains unknown whether exposure to weight-related cues causes a similar effect on older people with dementia. Employing older samples, Nakata and Kawai32 explored whether static visual information of someone else eating would facilitate food consumption. They compared the amount of snack intake among older adults without dementia in front of stimuli that mimicked the presence of others (ie, a mirror image or static self-image) as opposed to eating in a front of a monitor simply displaying a wall. The results demonstrated that their participants ate more snacks in the social condition than in other conditions. Navarro et al33 assessed the effect of an orange-colored napkin, a color which is associated with appetite, placed on the meal tray on food intake among hospitalized elderly adults. They found that patients in the orange napkin condition consumed more food than those in the control (white napkin) condition. Nolan and Mathews34 reported that they were able to reduce agitation in residents with dementia by adding a big clock with a large-print sign below it indicating the times for meals. These results imply that successive exposure of visual stimuli may be effective for older people with dementia.
In this study, we examined the influence of weight-related visual cues on the amount of food consumed by older adults with dementia in the real-world settings of a nursing home. We hypothesized that the number of finished meals per week would be higher when participants were exposed to higher-weight images than to other images.
Materials and Methods
Design
This experiment was based on a within-participant factor design, with the presentation of weight-related visual cues (images of a normal-weight chef, a higher-weight chef, a flower or no image). The number of finished meals and subjective evaluations of appetite during each of four weeks were measured for each condition. The details of these measurements are explained in the following “Measurements” section.
Participants
Twenty-one participants (16 females, 5 males; aged 74 to 104, average: 90.0±6.1 years) who had been diagnosed with dementia, including Alzheimer’s disease (6), dementia with Lewy bodies (2) and mixed-type dementia (13), were recruited for this study. They were all recruited in a nursing home in Tokyo, Japan. We did not measure the degree of cognitive ability of the participants directly because we aimed to explore the overall tendencies of the effect of weight-related visual cues on food consumed by older adults with dementia with a limited sample from a nursing home. For this purpose, it was sufficient to confirm that all participants had some level of dementia. All participants had normal or corrected-to-normal visual acuity, which presented no hindrance to everyday life, including eating meals, as assessed by the nursing home. Their swallowing functions were evaluated by dentists and there were no significant concerns regarding chewing and swallowing abilities. They were not allergic or intolerant to any of the foods provided in this study. The body mass index (BMI) of participants ranged from 15.1 kg/m2 to 25.4 kg/m2 with a mean BMI of 20.6 kg/m2 (SD = 2.8). One male participant had a high BMI (25.4 kg/m2), which is higher than the acceptable BMI range within 24.9 kg/m2. However, the amount of food prepared for each participant was determined based on their health condition and BMI by the clinical nutrition manager under the supervision of the nursing home’s doctor. The clinical nutrition manager and doctor judged him fit to participate in this study, which aimed to explore ways to encourage participants to finish their meals. This study was performed in accordance with the Helsinki Declaration guidelines. Family consent was obtained for each participant prior to the experiments. The study was approved by the institutional ethics committee of the nursing home Nanohana, Tokyo, Japan (reference number 79, February 15, 2019).
We used G*Power (v.3.1.9.7) to estimate sample size (within-participant factor: the number of groups = 4). With a small effect size of 0.15,31 power set at 0.80 and an alpha of 0.05, we determined that we would need at least 20 participants to detect significant effects at 95% power. Thus, the number of participants in the present study (21) is reasonable. However, it should be mentioned that our study design prevented us from testing the interactive effects of the weight-related visual cues with the degree of cognitive impairment of participants.
Stimuli
We used color prints of a normal-weight chef, a higher-weight chef and a flower as weight-related visual cues (Figure 1). The designs of normal- and higher-weight chefs’ bodies were created with reference to the stimuli used by Campbell et al.29 An illustration of a flower was used as a control because it was familiar to people, unrelated to weight stereotypes, and consistent with similar visual components, including color and lines, in the chef images. The words “Enjoy Your Meal” were written below each illustration. These illustrations were printed on white paper and set in a 150×100 mm menu card holder.
 |
Figure 1 Visual stimuli used in this study. Left: normal-weight chef, center: higher-weight chef and right: flower. |
Measurements
We assessed the amount of food consumed based on the number of finished meals per week in the nursing home. As the adequate volume and nutrition of meals depend on the needs of each individual, especially among older people, rather than assessing the amount of food consumed, we assessed whether the participants finished meals that were determined by the clinical nutrition manager in the nursing home. Furthermore, we hoped that this index would be easy for the staff to measure and, therefore, reduce the extra tasks asked of staff in order to conduct this intervention. We defined a finished meal as a clean dish or a dish with few leftovers that care staff judged as being less than one bite of food. In the case of noodles, soup was not considered a leftover. Also, beverages such as tea and water were not included as leftovers.
We also measured participants’ self-reported general appetites by using the Simplified Nutritional Appetite Questionnaire – Japanese version (SNAQ-J)35,36 in order to assess whether the successive exposure to weight-related cues affected the psychological states of participants with regard to general appetite. This questionnaire comprises four subscales: appetite, feeling full, food taste and meal frequency per day. Responses were given on a 5-point scale.
Procedure
Study sessions were conducted in a nursing home during lunch time, from 11:30 to 12:30, for 20 mealtimes over a four-week period (Monday to Friday). Saturdays and Sundays were excluded in order to avoid family visiting and any events in the nursing home. Based on the originally planned meal schedule at the nursing home, the lunch menu was varied as normal during the period of this experiment. There were no special meals, such as event-related meals, during the experimental period. All participants were served the same food, but each meal varied in form and in the amount of food based on each individual’s swallowing ability and health condition.
The study comprised one visual presentation condition per week: no-image (first week), normal-weight chef (second week), higher-weight chef (third week) and flower (last week). We adopted a one-week duration for each visual presentation condition because we required some differences, both within each condition and among the four conditions, in meals and in the amount of food provided. The order of presentation of the visual stimuli was constant among participants because a randomized presentation of illustrations in a nursing home dining room could cause anxiety or confusion among patients. Regarding the order of the presentation of the visual stimuli, we implemented the no-image condition for the first week in order to create a baseline. We implemented the normal-weight chef condition for the second week because we needed to determine the effect of visual exposure to the neutral chef image itself, not a weight-related cue. In order to determine whether the measurements changed during the higher-weight chef condition, which was the main intervention of this study, we implemented the higher-weight chef condition for the third week and the flower condition for the last week.
During each session, an illustration was placed on the lunchtime dining tray of each participant. The care staff gave the participants the following instructions on the first day of the study: “To explore the best way to use a menu card holder, we will add this holder on the dining tray at lunchtime for several weeks”. To avoid any experimenter effects, the care staff was blind to the experimental design and hypothesis. After lunchtime, the care staff were asked to record whether or not each participant had finished their meal completely.
There were no noteworthy environmental changes which might have affected participants’ appetites and eating behaviors, including daily activity programs, care staff organization and interior layout, through the experimental period.
On each weekend, participants were asked to answer questions about their general appetite for the week using the SNAQ-J with the assistance of nursing staff.
Data Analyses
In order to clarify whether or not the total amount of food prepared differed between weeks, we calculated the total amount of food prepared for each participant by subtracting the weight of the tray alone from the weight of the tray with food prepared and compared the results among conditions using the repeated measures analysis of variance (ANOVA).
We calculated the number of finished meals for each participant based on how many times they finished their meal completely each week (range: zero to five times). In order to determine whether the weight-related cue affected food intake, repeated measures ANOVAs with weight-related cue as a within-participant factor on the number of finished meals were performed.
To analyze self-reported appetite, the combined total of the four SNAQ-J subscale scores is generally used because this scale is considered a one-factor structure.36 However, our participants were not always be able to answer every subscale of the SNAQ-J each weekend because they had cognitive impairments related to dementia. Thus, we used the responses for the subscales that the participant was able to complete all four weekends and aggregated them for each subscale. As a result, we used n = 14 for feelings of appetite and n =10 for feeling full, food taste and meal frequency per day, respectively. In order to determine whether weight-related cues affected participants’ subjective feelings of appetite, repeated measures ANOVAs with weight-related cue as a within-participant factor on each score of each SNAQ-J subscale including appetite, feeling full, food taste and meal frequency per day, were performed respectively.
Statistical analyses were performed using IBM SPSS Statistics for Windows version 24 (IBM Corp., Armonk, NY, USA).
Results
Total Amount of Food Prepared
Table 1 shows the total amount of food prepared for each condition. A repeated measures single-factor ANOVA with the weight-related cue as a within-participant factor was performed on the total amount of food prepared. The main effect of the weight-related cue was not significant, F (3, 60) = 1.175, p = 0.327, ηp2 = 0.055.
 |
Table 1 Mean (Standard Deviation) Amount of Food Prepared (g) and Number of Finished Meals (Ranging from Zero to Five) for Each Weight-Related Cue Condition (n = 21) |
Number of Finished Meals
Table 1 also shows the number of finished meals for each condition. A repeated measures single-factor ANOVA with the weight-related cue as a within-participant factor was performed on the number of finished meals. The main effect of the weight-related cue was significant, F (3, 60) = 3.158, p = 0.031, ηp2 = 0.136. Further post-hoc statistical analysis using Tukey’s honestly significant difference (HSD) tests indicated that the number of finished meals was greater in the higher-weight chef condition than in the no-image condition (p < 0.05).
Subjective Evaluation of Appetite
Table 2 shows participants’ subjective ratings for each SNAQ-J subscale. A repeated measures single-factor ANOVA with visual cue as a within-participant factor was performed on each score for the four subscales, respectively. The results showed that the main effect of the visual cue was significant in the score for food taste, F (3, 30) = 3.676, p = 0.024, ηp2 = 0.290. Tukey’s HSD tests indicated that the score for food taste was higher in the higher-weight chef, flower and normal-weight chef conditions than in the no-image condition (ps < 0.05). We did not find significant effects of visual cue on appetite, feeling full and meal frequency per day.
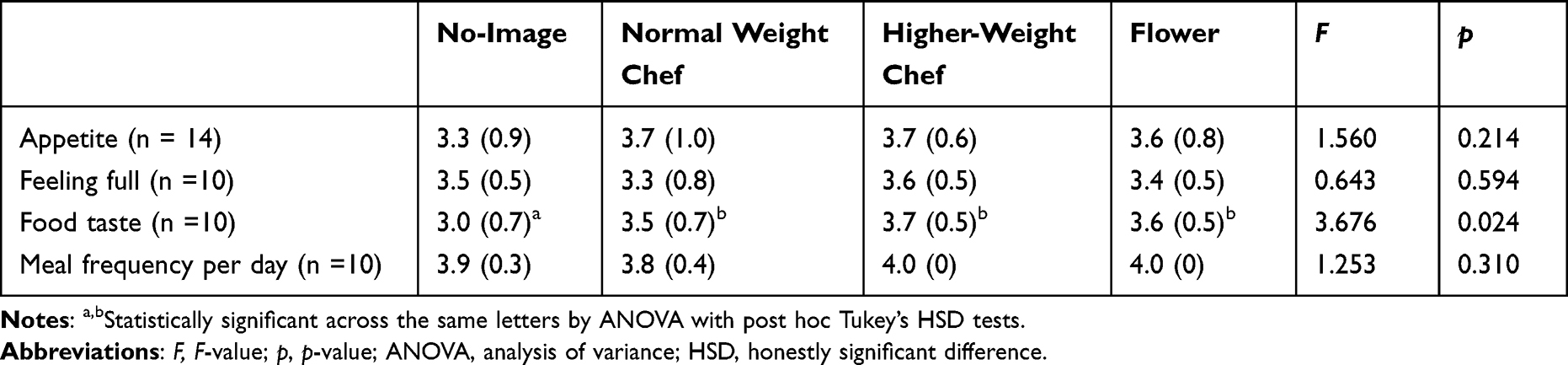 |
Table 2 Mean Scores (Standard Deviation) of Participants’ Subjective Ratings of Appetite |
Discussion
The main objective of the current study was to examine whether a weight-related cue affects the food intake of older adults with dementia. To the best of our knowledge, this is the first study which explores the possibilities of a weight-control-cue paradigm31 to prevent weight loss and malnutrition among older adults with dementia. The results demonstrate that the participants had more finished meals in the higher weight-chef condition than in the no-image condition, while the total amount of food prepared did not differ between conditions. One may argue that there is a possibility that the intervention of visual exposure to a dining-related cue at mealtimes using a menu stand in and of itself affects the participant’s food intake. For instance, Campbell et al29 discussed that presenting a mug image as a control stimulus during their food-choice task would not be ideal in their study because it could be associated with food. The images of the normal-weight chef and the flower may be as congruent with dining as is the image of a higher-weight chef. However, we did not find any significant difference between the number of finished meals in the no-image condition and those in the normal-weight condition nor those in the flower condition. Thus, the higher number of finished meals in the higher-weight chef condition cannot be explained only by general effects of experimental intervention and any dining-related cues. Rather, our results suggest that a weight-related cue might affect the amount of food consumed by older adults with dementia.
The present results suggest that successive exposure to a cartoon chef character representing a stereotyped social group related to body weight activates the stereotype and increases stereotype-consistent behavior in older adults with dementia. The effect of weight-related cues on food intake has previously been studied with the motivation of weight loss.15,21–23,25–29,31 The current study is the first to shed light on the possibility that this paradigm could also be applied to gaining weight and mitigating malnutrition in older adults with dementia.
While the current results are consistent with previous studies that have shown that an individual’s food intake is influenced by weight-related cues such as an image of a human-like figure,23–30 the impact of weight-related cues in the current study seemed to be weak compared to previous studies: whereas the mean number of finished meals was the highest in the higher-weight chef condition, a significant difference was observed only when compared with the no-image condition, not when compared with the normal-weight chef or flower conditions. Indeed, Buckland et al31 mentioned that some studies reported no effects of weight-control cues on food intake. Such discrepancies in findings might be due to the methodologies used across studies, including the level of cue engagement (attended, incidental or subliminal). With respect to the level of cue engagement, we presented the images using a postcard-sized image in a menu stand placed on each participant’s food tray. This method may be classified as incidental based on the level criteria proposed by Buckland et al31 because it was not clear whether the participant’s attention was explicitly directed to the image. While it has been reported that the level of cue engagement does not have an impact on the food intake in healthy participants,30 there might be different results for older adults with dementia because they often have some impairments of attentional function. However, we could not test for differences based on the degree of cognitive ability of the participants in this study because of a limited sample size recruited from a single nursing home. To clarify the influences of the level of cue engagement in the presentation of weight-related cues on food consumption among older adults with dementia, further studies that control both cue engagement and the degree of cognitive impairment of participants are necessary.
The results of subjective evaluations of appetite showed that the participants’ appetites, as measured using the SNAQ-J, were not influenced by exposure to the weight-related cue. The scores for feelings of appetite did not appear to correspond with the respective experimental conditions. Because the influence of the weight-related cue on food intake is subconscious,23 it is possible that the weight-related cue influenced food intake without affecting appetite. On the other hand, the scores for food taste were higher when the participants were exposed to any visual images compared to the no-image condition, not only the higher-weight chef image. These results suggest that the exposure to any visual cues, including the chef and flower images, enhance the overall taste of meals even if these cues do not relate to bodyweight. One possible explanation for the present result lies in the effect of environmental cues on food evaluation. Several studies have demonstrated that food-related items or locations enhance food acceptance and evaluation.33,37,38 It could be that the image of a chef as well as that of a flower was congruent with eating location. Thus, the presentation of food-related visual stimuli might positively impact overall taste evaluations of meals. It would also be worthwhile to explore the influence of food-related stimuli on food evaluations among older adults with dementia.
The present findings may provide some important insight into designing the eating environment for older adults with dementia. If the amount of food intake is inhibited by surrounding cues of, for example, a low bodyweight figure,23 co-eating among elderly people with malnutrition might lead to reduced food intake because the already thin fellow diners could represent a weight-related cue that promotes less food intake. Thus, the successive exposure of images of higher-weight bodies in the eating environments of nursing homes would be efficacious in avoiding such weight-loss and malnutrition spirals. Our findings may provide a convenient yet effective means of enhancing the eating behavior of older adults with dementia. Furthermore, the intervention using visual images would be widely acceptable in nursing homes and hospitals because it is a contactless intervention and, therefore, will contribute to keeping the eating environment hygienic. In addition, our findings offer easy care prospects for pre-oral disorders and deserve further research to validate and confirm their beneficial effects.
The present results are subject to some limitations. First, this is a pilot experiment without a randomized control design that recruited participants from a single nursing home. Therefore, the order in which we presented each image stimulus was constant among participants, meaning that an order effect cannot be ruled out for the present results because the presentation of the higher-weight chef image was neither first nor last. Future studies should control for order effects by using a randomized controlled trial design and by recruiting participants from several nursing homes, which would also allow for generalization of the present findings. Secondly, we assessed the amount of food intake for each condition by the number of finished meals per week for the following reasons: (1) There are large individual differences and intrapersonal variabilities in what constitutes an adequate amount of food for each participant. Thus, we assessed whether the participants reached the goal of eating entire meals which were determined by the clinical nutrition manager in the nursing home. (2) This finished-meal index may be easy for care staff to measure, and, therefore, contribute to reducing any extra work burden the staff may experience in conducting the intervention. However, there is little information about the ingested calories and nutrition in this index. Thus, convenient methods to assess caloric and nutritional information are needed. One possible solution is a photographic method.33,39,40 For instance, Navarro et al used the Modified Comstock Plate Waste Scale with digitally captured images of plate waste of patients in hospital.33,39 With this method, raters were asked to indicate the proportion of the food items remaining on the plate, 0%, 25%, 50%, 75%, 90% or 100%, for each meal component such as vegetable, starch and main course. This method may be reasonable for measuring the amount of food intake for residents of nursing homes both in the aspect of accuracy and convenience. Furthermore, most previous studies tested the effects of weight-related cues on the amount of food consumption with a single trial using a between-participant experiment design. We designed our experimental intervention to be longer than most previous studies (four conditions with five trials each), and our results produced evidence that weight-related cues influenced participants’ food consumption. Thus, the next step would be to combine a randomized controlled trial design with a longer intervention to investigate whether weight-related visual cues affect the amount of food consumed by older adults with dementia over a relatively long duration.
Conclusion
The main interest of the present study is whether the exposure to weight-related visual cues affect the amount of food consumed by older adults with dementia. The results show that the participants finished their meals more frequently when they were exposed to the higher-weight image than when they were not exposed to any images. However, these results should be considered with caution due to some methodological limitations of this pilot study. Further research using tightly controlled experimental designs is necessary in order to clarify to what extent and in what way weight-related cues affect food consumption and evaluation among older people with dementia.
Acknowledgments
We are grateful to all participants and staff at the nursing home involved. We would like to thank ELCS (English Language Consultation Services) for examination of the manuscript. This work is supported in part by Grant-in-Aid for Scientific Research (C) from the Japan Society for the Promotion of Science 21K02115.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gale SA, Acar D, Daffner KR. Dementia. Am J Med. 2018;131(10):1161–1169. doi:10.1016/j.amjmed.2018.01.022
2. Volkert D, Chourdakis M, Faxen-Irving G, et al. ESPEN guidelines on nutrition in dementia. Clin Nutr. 2015;34(6):1052–1073. doi:10.1016/j.clnu.2015.09.004
3. Kimura A, Yamaguchi K, Tohara H, et al. Addition of sauce enhances finger-snack intake among Japanese elderly people with dementia. Clin Interv Aging. 2019;14:2031–2040. doi:10.2147/CIA.S225815
4. Prince MJ, Wimo A, Guerchet MM, Ali GC, Wu Y-T, Prina M. World Alzheimer Report 2015: The Global Impact of Dementia. An Analysis of Prevalence, Incidence, Cost and Trends. London: Alzheimer’s Disease International; 2015.
5. Guérin O, Andrieu S, Schneider SM, et al. Different modes of weight loss in Alzheimer disease: a prospective study of 395 patients. Am J Clin Nutr. 2005;82(2):435–441. doi:10.1093/ajcn/82.2.435
6. Douglas JW, Lawrence JC. Environmental considerations for improving nutritional status in older adults with dementia: a narrative review. J Acad Nutr Diet. 2015;115(11):1815–1831. doi:10.1016/j.jand.2015.06.376
7. Lin LC, Watson R, Wu SC. What is associated with low food intake in older people with dementia? J Clin Nurs. 2010;19(1–2):53–59. doi:10.1111/j.1365-2702.2009.02962.x
8. Stone L. Eating/feeding issues in dementia: improving the dining experience. End Life J. 2014;4(1):1–7. doi:10.1136/eoljnl-04-01.1
9. Ligthart-Melis GC, Luiking YC, Kakourou A, Cederholm T, Maier AB, de van der Schueren MAE. Frailty, sarcopenia, and malnutrition frequently (co-)occur in hospitalized older adults: a systematic review and meta-analysis. J Am Med Dir Assoc. 2020;21(9):1216–1228. doi:10.1016/j.jamda.2020.03.006
10. Xu Q, Ou X, Li J. The risk of falls among the aging population: a systematic review and meta-analysis. Front Public Health. 2022;10:902599. doi:10.3389/fpubh.2022.902599
11. Leopold NA, Kagel MC. Dysphagia--ingestion or deglutition? A proposed paradigm. Dysphagia. 1997;12(4):202–206. doi:10.1007/PL00009537
12. Abbott RA, Whear R, Thompson-Coon J, et al. Effectiveness of mealtime interventions on nutritional outcomes for the elderly living in residential care: a systematic review and meta-analysis. Ageing Res Rev. 2013;12(4):967–981. doi:10.1016/j.arr.2013.06.002
13. Liu W, Cheon J, Thomas SA. Interventions on mealtime difficulties in older adults with dementia: a systematic review. Int J Nurs St. 2014;51(1):14–27. doi:10.1016/j.ijnurstu.2012.12.021
14. Whear R, Abbott R, Thompson-Coon J, et al. Effectiveness of mealtime interventions on behavior symptoms of people with dementia living in care homes: a systematic review. J Am Med Dir Assoc. 2014;15(3):185–193. doi:10.1016/j.jamda.2013.10.016
15. Brunner TA. How weight-related cues affect food intake in a modeling situation. Appetite. 2010;55(3):507–511. doi:10.1016/j.appet.2010.08.018
16. Cruwys T, Bevelander KE, Hermans RCJ. Social modeling of eating: a review of when and why social influence affects food intake and choice. Appetite. 2015;86:3–18. doi:10.1016/j.appet.2014.08.035
17. Nisbett R, Storms M. Cognitive and social determinants of food intake. In: London H, Nisbett R, editors. Thought and Feeling: Cognitive Alternation of Feeling States. Chicago: Aldine; 1974:190–208.
18. Goldman S, Herman C, Polivy J. Is the effect of a social model on eating attenuated by hunger? Appetite. 1991;17(2):129–140. doi:10.1016/0195-6663(91)90068-4
19. Herman P, Polivy J. Normative influences of food intake. Physiol Behav. 2005;86(5):762–772. doi:10.1016/j.physbeh.2005.08.064
20. Wansink B. Environmental factors that increase the food intake and consumption volume of unknowing consumers. Annu Rev Nutr. 2004;24(1):455–479. doi:10.1146/annurev.nutr.24.012003.132140
21. Papies EK, Hamstra P. Goal priming and eating behavior: enhancing self-regulation by environmental cues. Health Psychol. 2010;29(4):384–388. doi:10.1037/a0019877
22. van Kleef E, Shimizu M, Wansink B. Food compensation: do exercise ads change food intake? Int J Behav Nutr Phys Act. 2011;8(1):6. doi:10.1186/1479-5868-8-6
23. Brunner TA, Siegrist M. Reduced food intake after exposure to subtle weight-related cues. Appetite. 2012;58(3):1109–1112. doi:10.1016/j.appet.2012.03.010
24. Ohtomo S. Exposure to diet priming images as cues to reduce the influence of unhealthy eating habits. Appetite. 2017;109:83–92. doi:10.1016/j.appet.2016.11.022
25. Stämpfli AE, Brunner TA. The art of dieting: exposure to thin sculptures effortlessly reduces the intake of unhealthy food in motivated eaters. Food Qual Prefer. 2016;50:88–93. doi:10.1016/j.foodqual.2016.01.012
26. Stämpfli AE, Stöckli S, Brunner TA. A nudge in a healthier direction: how environmental cues help restrained eaters pursue their weight-control goal. Appetite. 2017;110:94–102. doi:10.1016/j.appet.2016.11.037
27. Stämpfli AE, Stöckli S, Brunner TA, Messner C. A dieting facilitator on the fridge door: can dieters deliberately apply environmental dieting cues to lose weight? Front Psychol. 2020;11:582369. doi:10.3389/fpsyg.2020.582369
28. Stöckli S, Stämpfli AE, Messner C, Brunner TA. An (un)healthy poster: when environmental cues affect consumers’ food choices at vending machines. Appetite. 2016;96:368–374. doi:10.1016/j.appet.2015.09.034
29. Campbell MC, Manning KC, Leonard B, Manning HM. Kids, cartoons, and cookies: stereotype priming effects on children’s food consumption. J Consum Psychol. 2016;26(2):257–264. doi:10.1016/j.jcps.2015.06.003
30. Gonçalves S, Ferreira R, Conceição EM, et al. The impact of exposure to cartoons promoting healthy eating on children’s food preferences and choices. J Nutr Educ Behav. 2018;50(5):451–457. doi:10.1016/j.jneb.2017.12.015
31. Buckland NJ, Er V, Redpath I, Beaulieu K. Priming food intake with weight control cues: systematic review with a meta-analysis. Int J Behav Nutr Phys Act. 2018;15(1):66. doi:10.1186/s12966-018-0698-9
32. Nakata R, Kawai N. The “social” facilitation of eating without the presence of others: self-reflection on eating makes food taste better and people eat more. Physiol Behav. 2017;179:23–29. doi:10.1016/j.physbeh.2017.05.022
33. Navarro DA, Shapiro Y, Birk R, Boaz M. Orange napkins increase food intake and satisfaction with hospital food service: a randomized intervention. Nutrition. 2019;67–68(Suppl):100008. doi:10.1016/j.nutx.2020.100008
34. Nolan BAD, Mathews RM. Facilitating resident information seeking regarding meals in a special care unit: an environmental design intervention. J Gerontol Nurs. 2004;30(10):12–16. doi:10.3928/0098-9134-20041001-07
35. Nakatsu N, Sawa R, Misu S, Ueda Y, Ono R. Reliability and validity of the Japanese version of the simplified nutritional appetite questionnaire in community-dwelling older adults. Geriatr Gerontol Int. 2015;15(12):1264–1269. doi:10.1111/ggi.12426
36. Tokudome Y, Okumura K, Kumagai Y, et al. Development of the Japanese version of the Council on Nutrition Appetite Questionnaire and its simplified versions, and evaluation of their reliability, validity, and reproducibility. J Epidemiol. 2017;27(11):524–530. doi:10.1016/j.je.2016.11.002
37. García- Segovia P, Harrington RJ, Seo HS. Influences of table setting and eating location on food acceptance and intake. Food Qual Prefer. 2015;39:1–7. doi:10.1016/j.foodqual.2014.06.004
38. Meiselman HL, Johnson JL, Reeve W, Crouch JE. Demonstrations of the influence of the eating environment on food acceptance. Appetite. 2000;35(3):231–237. doi:10.1006/appe.2000.0360
39. Navarro DA, Singer P, Leibovitz E, Krause I, Boaz M. Inter- and intra-rater reliability of digitally captured images of plate waste. Nutr Diet. 2014;71(4):284–288. doi:10.1111/1747-0080.12137
40. Pouyet V, Cuvelier G, Benattar L, Giboreau A. A photographic method to measure food item intake. Validation in geriatric institutions. Appetite. 2015;84:11–19. doi:10.1016/j.appet.2014.09.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Beliefs About Body Weight and Practices of Regulating Food and Physical Exercise Patterns of Children Among Parents in Southern Ethiopia
Zewude B, Siraw G, Melese B, Habtegiorgis T, Hizkeal A, Tadele M
Psychology Research and Behavior Management 2022, 15:1871-1883
Published Date: 27 July 2022