Back to Journals » Journal of Healthcare Leadership » Volume 17
Exploring Trust and Engagement: A Qualitative Evaluation of the Relationship Between Clinicians and Healthcare Leaders at Academic Medical Centers
Authors Keller EJ, Sehgal N, Ryu RK, Chrisman H, Vogelzang RK, Shanafelt TD
Received 8 November 2024
Accepted for publication 12 February 2025
Published 27 February 2025 Volume 2025:17 Pages 75—83
DOI https://doi.org/10.2147/JHL.S503086
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Zhanming Liang
Eric J Keller,1 Niraj Sehgal,2 Robert K Ryu,3 Howard Chrisman,4 Robert K Vogelzang,4 Tait D Shanafelt2
1Department of Radiology, Stanford Health Care, Stanford, CA, USA; 2Department of Medicine, Stanford Health Care, Stanford, CA, USA; 3Department of Radiology, University of Colorado, Aurora, CO, USA; 4Department of Radiology, Northwestern Medicine, Chicago, IL, USA
Correspondence: Eric J Keller, Email [email protected]
Background: Dynamics between clinicians and healthcare leaders are critical in determining the culture and success of Academic Medical Centers (AMCs). These dynamics are complex, making it challenging to develop effective means of improving these relationships. This study sought to characterize and compare relationships between clinicians and healthcare leaders at three AMCs to develop more effective means of improving healthcare organization cultures.
Materials and Methods: The authors interviewed clinicians, clinician leaders, and operational leaders at three AMCs about their role, perceived dynamics between clinicians and healthcare leaders, and ideal leadership. Interviews continued until additional interviews stopped revealing new information at each organization, requiring a total of 92 participants (49% male, 54% clinicians, 22% clinician-leaders, 24% operational leaders). Interview transcripts were systematically analyzed based on constructivist grounded theory and content analysis for key themes.
Results and discussion: The perceived most pressing issues at each AMC varied across three key cultural levels: organization, department, and practice. When interventions targeted levels distinct from the level perceived most pressing, they tended to exacerbate existing issues and further undermine trust and engagement between clinicians and healthcare leaders. Clinicians and healthcare leaders across AMCs described similar traits of ideal leadership but exhibited different understandings of what those traits meant in application. Cultural dynamics were also challenged by professional cultural differences between the three groups and barriers such as differences in status, location, and background. Limitations of this study included its cross-sectional nature and potential sampling bias.
Conclusion: The level of organizational culture where the greatest tension exists between clinicians and healthcare leaders varies by three key levels. Discerning which level of organizational culture represents the greatest local opportunity can inform the design of more targeted interventions to improve dynamics between clinicians and healthcare leaders seeking to foster more constructive partnerships.
Keywords: organizational culture, academic medical center, cultural dynamics, cultural levels
Introduction
Academic medical centers (AMCs) have rapidly increased in size and complexity over the last few years, now likely better termed “academic medical systems”. Although this growth has many positive attributes, the paired increased organizational and social complexity has created and exacerbated challenges such as engagement, collaboration, communication, and trust across silos, as well as complicating the balance between commitments to patient care, research, and education.1,2 Analogous challenges exist in non-academic medical centers and other large, complex healthcare systems. Although these challenges are not necessarily unique to healthcare organizations/systems, the interprofessional dynamics may make it more difficult to apply some of the effective management strategies in other sectors. One critical dynamic seems to be the relationship between clinicians and organizational leadership.3–5 Negative dynamics have been associated with poor clinician engagement, work satisfaction, burnout, and turnover, which may ultimately adversely affect healthcare and organizational outcomes.6–9
Efforts to improve these dynamics and facilitate effective healthcare system cultures may be limited by a lack of clarity regarding which level of the organization has the greatest tension between clinicians and leaders.10 Although some have attempted to characterize effective clinician–leader relationships,3,11–14 we believe healthcare systems tend to rely on trials of non-targeted systemic therapies that may work in other organizations but not necessarily their own or may help to a lesser degree than if a more targeted intervention was employed. We hypothesized that there are common issues across AMCs as well as key differences in how these common issues are contextualized and perceived that may undermine less-targeted efforts to improve organizational cultures. To investigate this hypothesis, we studied and compared the dynamics between clinicians and healthcare leaders at three AMCs.
Methods
Study Setting and Recruitment
The human subject interactions were each reviewed by the institutional review board (IRB) of the center where the interview took place. Specifically, the University of Colorado IRB oversaw interviews conducted at the University of Colorado, the Northwestern Medicine IRB oversaw interviews conducted at the Northwestern, and the Stanford Medicine IRB oversaw interviews conducted at the Stanford. Because the interview questions focused on participating individuals’ perceptions of the relationship between clinicians and healthcare leaders at their center globally, rather than any personal information, the Institutional Review Boards at all three institutions (ie, the University of Colorado, Northwestern Medicine, and Stanford Medicine) deemed the study exempt from full review as the methods posed minimal risk to participants. Nevertheless, verbal consent was obtained and documented from all participants after discussing the anonymous nature of the analysis and potential use of anonymized quotes. Consent was documented in a secure spreadsheet.
We studied three geographically distinct academic medical centers (AMCs) in the United States, which was primarily a convenience sample with data collection from October 2017 through August 2020. One was in an urban setting in the Midwest (AMC 1) and two were in suburban settings in the mountain region (AMC 2) and west coast (AMC 3). The three centers were studied in series using the same approach. As previously reported, select data from AMC 1 was previously used to analyze inherent cultural difference between clinicians and healthcare leaders.2 For the current study, comparative analysis between the organizations was performed retrospectively. Participants were selected using a combination of purposeful recruitment to ensure diversity in terms of positions (CEOs to practice managers), clinical specialty, experience, and gender, as well as snowball sampling where participants were asked to recommend additional interviewees. Potential participants were initially contacted via Email with participation rates across the organizations and groups within those organizations ranging from 77% to 91%. Data collection and analysis continued until thematic saturation was achieved at each institution as is typical for the methodology used in this study.15,16 This occurred after 35, 29, and 28 interviews for AMC 1, 2, and 3, respectively, for a total of 92 participants (49% male, 54% clinicians, 22% clinician leaders, 24% operational leaders). Participant demographics by AMC are provided in Table 1.
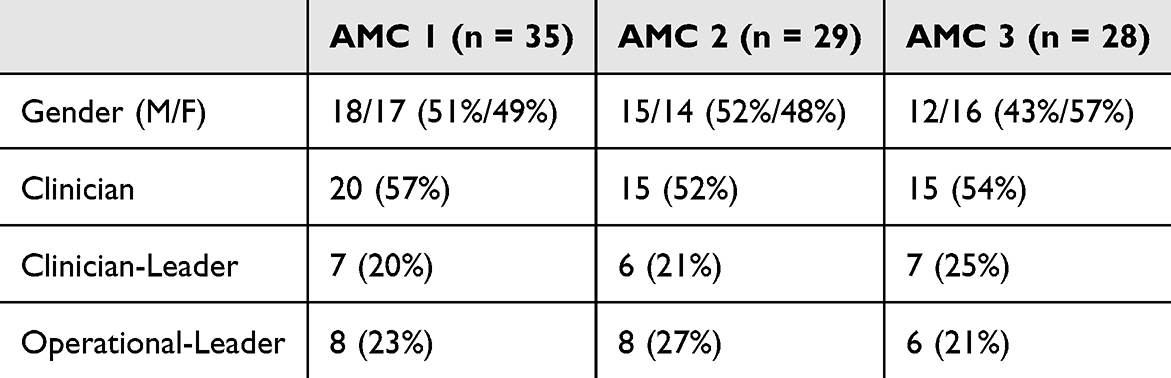 |
Table 1 Demographics |
For the purposes of this study, we defined clinicians as healthcare professionals directly involved in patient care, eg, physicians and nurses. Clinician leaders were defined as individuals with clinical training whose current role requires a substantial amount of leadership duties and would lead others to perceive them as a healthcare leader, eg, a department chair, vice president who was previously a nurse, or center director who still works as a physician on a limited basis. Operational leaders were defined as healthcare leaders not directly involved in patient care and without a clinical background.
Data Collection
We conducted interviews either in person or over the phone based on interviewee preference. Interviews were performed in a semi-structured manner to establish rapport and allow interviewees to discuss what they viewed as important while ensuring similar topics were discussed across interviews for comparison.17 The interview script was constructed to establish rapport and assess participants’ perceptions of their professional role/identity prior to asking more sensitive questions about dynamics between different groups. All interviews were conducted by the same researcher, with experience conducting qualitative interviews in healthcare. The interview script is provided in Supplementary Table 1. Interviews were performed once without further follow-up interviews.
Data Analysis
Interviews were recorded and professionally transcribed verbatim. Transcripts were systematically analyzed using a constructivist grounded theory approach,15 where transcripts are coded for key concepts based on emphasis and context and used to inform additional data collection. Concepts are iteratively refined and compared with additional interviews, allowing central themes to emerge that are tested against additional interviews until additional interviews stop revealing new information (thematic saturation). The final coding structure is summarized in Supplementary Table 2. Transcripts were also analyzed retrospectively using content analysis where the frequencies of coded concepts were quantified and compared across groups.16 Chi-squared tests were used for these comparisons, with statistical significance defined as p ≤0.05. All data analyses were performed by a single researcher experienced with the qualitative and quantitative methodologies employed. However, emerging themes were discussed with the research team for consensus during the data analysis process to help reduce bias.
Results
Common Cultural Divides
Common organizational-level issues involved compensation plans and funds flow between entities, which were reduced with less organizational complexity, eg, if the same leadership team oversaw the hospital staff and medical school faculty. These dynamics tended to be exacerbated by tighter financial margins, stressing an inherent balance between commitments to healthcare system growth, faculty/staff support, and education/research.
Common department-level issues involved inter-division and inter-specialty tension, eg, operating room start times between anesthesiology and surgical fields. These tended to rely heavily on dynamics between department chairs as well as individual chairs’ relationships with higher-level leaders to secure support and funding. These dynamics tended to be exacerbated by cultural differences between specialties as well as clinicians and healthcare leaders described previously, which can undermine efforts to collaborate.2,18 These differences were widened by common barriers including differences in power/status, physical location, and education/backgrounds.
Practice-level issues were more variable and practice-specific but often related to an inherent cultural divide between clinicians and healthcare leaders or a specific problematic “boss”. This issue also occurred at the department level, eg, with certain department chairs at AMC 2. Clinician leaders tended to be better able to bridge the cultural divide between clinicians and healthcare leaders but also shared a common feeling of isolation from both groups. Example quotes of key themes are provided in Table 2.
 |
Table 2 Example Quotes |
Cultural Levels and Mental Saturation
Both shared and distinct themes relative to clinician–leader relationships emerged across the AMCs studied. General perceptions of good leadership and ideal dynamics between clinicians and healthcare leaders tended to be similar across AMCs as did perceived cultural differences between clinicians, clinician leaders, and operational leaders (code prevalence p > 0.05 for comparisons between roles and AMCs). However, specific issues varied and tended to manifest at three key cultural levels: practice, department, or organization. Although perceived issues at all three levels occurred at all AMCs, one level tended to dominate and be inversely correlated with the others. For example, at AMC 1, there were more perceived organizational-level issues but relatively less department and practice-level issues such as turf wars. Conversely, at AMC 3, there were more practice-level issues but relatively less organizational-level issues. When asked about interactions with healthcare leaders at AMC 1, clinicians universally understood this to mean the organizational leadership, eg, the CEO and executive team, whereas clinicians at AMC 3 tended to ask for clarification with less of a shared perception of what was meant by “administrator” due to less of a higher-level administrative presence.
Thus, a common key observation across the AMCs was that the perceived “key issue” at the organization tended to be influenced by which of the three cultural levels was perceived as most problematic, and although issues at other levels may co-exist, they were deprioritized as though participants only had a finite amount of mental/emotional energy to expend toward these issues. Once saturated at one cultural level, other issues seem trivial or non-existent. For example, at AMC 1, the senior organizational leadership seemed to exist as a “common enemy” resulting in relatively less inter-specialty and practice-level conflict. Likewise, initiatives and programs at the organizations to correct issues at other levels were perceived as disconnected and not addressing the “main issue”. Interestingly, there was no relationship between the cultural level of the perceived main issues and participants’ roles (p = 0.56), ie, department chairs were not more likely to primarily discuss department-level issues controlling for organizational differences. A comparison of the levels of perceived main issues between AMCs is provided in Figure 1 and description of cultural dynamics at each AMC is provided in Table 3.
 |
Table 3 Summary of Cultural Dynamics at Each AMC with Example Quotes |
 |
Figure 1 Cultural level of the predominant-perceived issues/challenges related to clinician–administrator relationships by organization. |
Perceptions of Ideal Leadership/Relationships
Participants across roles and organizations described similar traits of ideal leadership or administrator-clinician relationships. Common themes included transparency, intellectual honesty/humility, engaging people in decision making/giving people a voice or seat at the table, mutual respect, understanding needs, and being invested, that actions speak louder than words. The most frequently described traits are listed in decreasing frequency in Table 4.
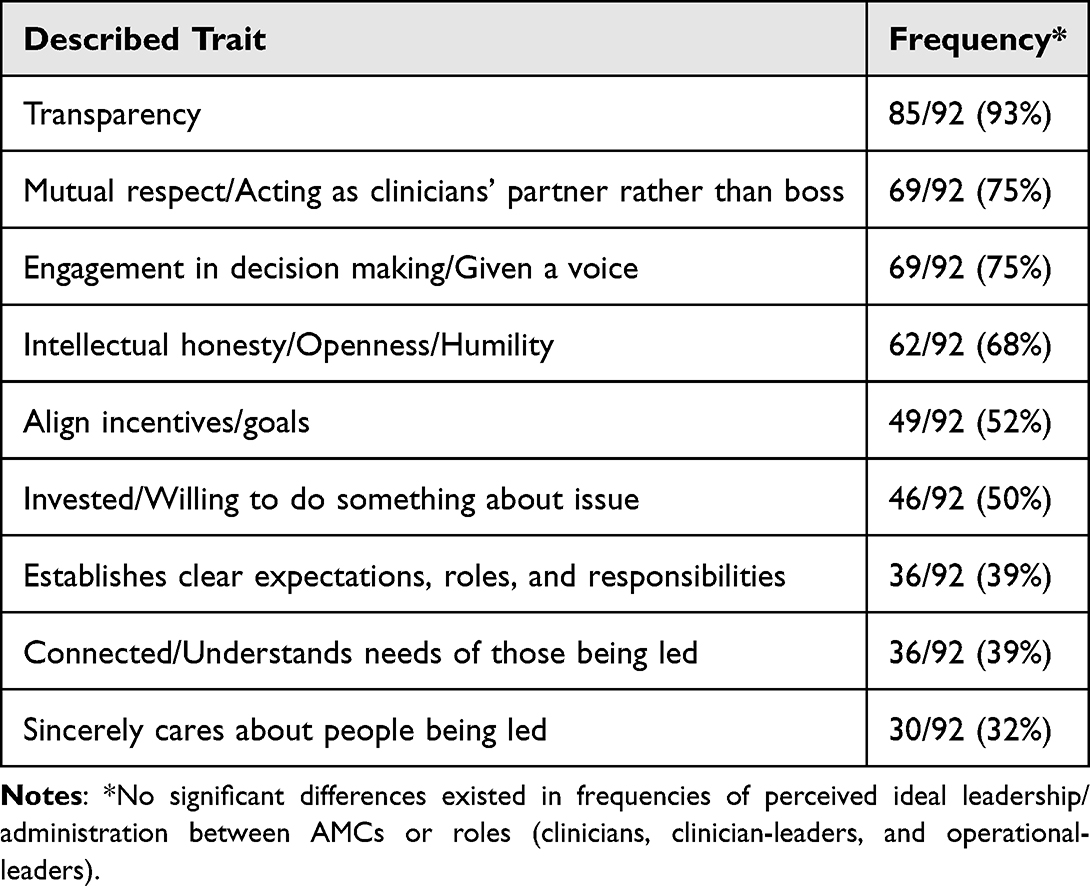 |
Table 4 Commonly Valued Traits of Ideal Leadership in Healthcare |
However, despite these common descriptions of ideal clinician–administrator relationships, two common barriers across AMCs tended to undermine these relationships, which occurred at all three cultural levels. One barrier was when the described traits are referred to so frequently that participants assume a common understanding of what these traits look like in practice despite having distinct understandings (ie, they use common language but do not have a common meaning). For example, what “transparency” meant and looked like in practice varied among participants when asked for examples. When other people acted differently than someone’s assumed shared understanding, that person tended to assume the other person must have been disingenuous (ie, they say the right things but do not act in congruent manner).
Another related barrier that occurred across AMCs involved differences in how clinicians and healthcare leaders oriented themselves to clinician–administrator relationships. Some healthcare leaders tended to view themselves as clinicians’ “partners”, whereas others viewed themselves as “bosses”. Some clinicians viewed themselves as “leaders” of a team, whereas others oriented themselves as “islands”, expecting the organization to work around them and their needs. Partners and leaders tended to described concepts such as “aligning incentives” in terms of understanding others’ perceptions and needs, whereas bosses and islands described this in terms of control and getting others to do what they needed them to do.
Discussion
The results highlight the cultural complexity of healthcare organizations as well as the need for tailored interventions to improve critical aspects of organizational cultural dynamics such as relationships between clinicians and healthcare leaders. The authors believe that healthcare systems are going to keep increasing in complexity to better meet the complex needs of their communities, making the implications of this study ever more important and potentially a key difference in how successful systems will be in their pursuits. Although common cultural divides and issues were observed across three AMCs, the cultural level and nature of the primary issues tended to vary. Leadership efforts targeting issues at other levels are not only less likely to be effective but tended to exacerbate the existing dynamics by fostering perceptions among clinicians that leadership was disconnected, ultimately undermining trust and engagement. This is likely due to a degree of mental/emotional saturation where people have limited mental energy on top of their other responsibilities to worry about multiple issues co-existing at multiple levels within their organization. Thus, issues at a single cultural level tend to be perceived as most pressing to a degree that issues at other levels may not even be perceived as issues until the most pressing issues are addressed.
Some of the findings in this study have been observed previously. For example, Edmondson and Harvey described similar barriers that can undermine inter-professional teams, including boundaries related to professional status, physical distance, and knowledge.19 The frequently described traits of ideal leadership are similar to Gittell’s description of high-quality relationships based on shared goals, shared knowledge, and mutual respect.13 The disconnect between assumed common values and individuals’ actual understandings of what these entail has been previously observed among clinicians and healthcare leaders called “the hazard of the common”.2 Schein and Schein also made a similar observation, noting that cultural issues can be identified by observing where an organizational culture’s “espoused values” (what they say they value) seems incongruent with its “artifacts” (their behaviors).20 It has also been previously suggested that perceptions of value misalignment within an organization may be particularly dependent upon perceptions of local leaders as the lens through which people view the overall organization.4 This was observed at both AMC 2 and 3 where the primary issues tended to exist at the department and practice levels, respectfully. However, the generally positively viewed local leadership at AMC 1 did not compensate for the perceived organization-level issues. In other words, ineffective local leadership (ie, a clouded lens) may degrade perceptions of the organization as a whole but good local leadership (ie, a clear lens) may not improve perceptions of the organization if significant organization-level issues exist.
Previously proposed interventions have focused on creating shared identities/goals,21,22 communication styles such as sensemaking23 or appreciative inquiry,24 and the importance of leadership support.3 Others stress the importance of diverse leadership backgrounds with the involvement of clinicians25,26 as well as leadership training to ensure clinicians are successful in these roles.27 Ultimately, we believe many of these issues and proposed solutions underscore the importance of trust building, but how one most effectively does so seems to be at least partially organization- and team-specific. All these approaches are likely helpful, but our results illustrate the importance of first identifying the most pressing level and mechanism of dysfunction to most effectively and efficiently apply those interventions or develop new ones. As an analogy, steroids may help many ailments to a degree but are often less effective than therapies targeting the underlying pathophysiology and may even exacerbate other issues. In healthcare leadership, if the main perceived issue involves a lack of transparency and engagement from senior organizational leadership, focusing on communication styles among practice managers is less likely to be helpful than creating regular and timely forums where clinicians can engage with organizational leadership who foster psychological safety. Conversely, that same strategy would not be as effective for an organization like AMC 3 where issues primarily existed at the practice level.
Figure 2 proposes a potential approach with potential targeted interventions. If there is a suspected disconnect or cultural issue within a healthcare organization, we propose first identifying the primary cultural level of dysfunction. This can be accomplished through the methodology employed in this study, if necessary, but even a handful of individual conversations with some clinicians and organizational leaders by a neutral or trusted member of the organization may be sufficient. We would suggest this approach over more formal focus groups, meetings, or town halls where important but more controversial opinions are unlikely to be shared publicly. For example, AMC 3 where practice-level issues predominate would likely benefit from leadership coaching and better aligning the incentives of clinicians and organizational leaders. If organizational-level issues predominate, such as in AMC 1, then it would be more helpful to focus on leadership spending time in clinical microsystems and better engaging clinical leaders in organizational decision-making. See Figure 2 for additional strategies.
 |
Figure 2 Proposed approach to healthcare organizational culture diagnostics with potential interventions. |
A final important consideration is the unique leader/staff and clinician cultural divide that exists in healthcare organizations that may undermine effective leadership strategies in other organizations.2 Clinicians, particularly physicians and nurses, are distinct in that their professional identity tends to be less tied to a specific role within an organization than their membership in a profession that extends beyond that organization, ie, a cardiologist primarily views themselves as a cardiologist regardless of whether they are at AMC 1 or 2, even when they take on a clinician-leader role. As such, perceptions of success are more often tied to one’s personal reputation within that professional community rather than climbing an organizational hierarchy. This contrasts with healthcare leaders without clinical backgrounds whose professional identities tend to be closely tied to their role/level in the specific organization. As such, clinicians are particularly sensitive to organizational structures that are perceived to undermine their sense of autonomy and mastery.28 This is likely why the “partner” approach to leadership seems particularly important for healthcare organization leaders as well as understanding that clinicians’ perceptions of success may be more reliant on their identities as exceptional patient advocates, researchers, or educators than their clinical productivity metrics or organizational growth.2 This is also likely why clinician leaders seem to more easily bridge the cultural divide between clinicians and operational leaders, though this comes with the price of feeling isolated from both groups. Understanding this cultural divide is critical not only for facilitating better collaboration but also for more thoughtfully addressing clinician burnout.
This study had important limitations. Although three geographically distinct AMCs were studied, the themes identified may not apply to other medical centers/systems such as those in rural communities or other settings not included in this study. The qualitative methodologies employed also have inherent limitations. Although semi-structured interviewing can produce richer data, it also has more opportunities for variability and bias introduced from the researcher serving as the data collection and analysis tool. This was reduced by using an experienced researcher and systematic approach but remains an important limitation. There is also bias introduced by having a single researcher perform the analysis. We attempted to mitigate this by discussing emerging themes with the research team for consensus, but this also remains an important limitation.
Conclusions
In summary, we studied the dynamics between clinicians and organizational leadership at three AMCs given that these dynamics are likely a key aspect of effective healthcare organization cultures. We found that although common issues and perceptions existed across all three AMCs, the cultural level and nature of the perceived main issue varied to a degree where well-meaning, non-targeted strategies to improve these dynamics could worsen them. This is a timely observation as AMCs have been rapidly increasing in complexity, raising these issues. As such, we believe more effective organizational effort to discern the cultural level of greatest opportunity can both focus efforts and determine which interventions may be most helpful to strengthen relationships between clinicians and leaders within individual organizations.
Disclosure
Dr Robert Ryu reports consultant for Philips Medical, outside the submitted work. Dr. Shanafelt is co-inventor of the Well-being Index and Mayo Leadership Impact Index; Mayo Clinic owns the copyright on these instruments, has licensed them for use and and shares a portion of royalties with Dr. Shanafelt; as an expert on the topic of clinician well-being, Dr Shanafelt gives grand rounds/keynote presentations and advises organizations on their efforts to foster clinician well-being. He receives honoraria for some of these presentations. The authors report no other conflicts of interest in this work.
References
1. State of the American workplace. Gallup, 2017 February. Report No.
2. Keller EJ, Giafaglione B, Chrisman HB, Collins JD, Vogelzang RL. The growing pains of physician-administration relationships in an academic medical center and the effects on physician engagement. PLoS One. 2019;14(2):e0212014. doi:10.1371/journal.pone.0212014 Epub 2019/02/14 PubMed PMID: 30759151; PubMed Central PMCID: PMCPMC6373942.
3. Shanafelt TD, Schein E, Minor LB, Trockel M, Schein P, Kirch D. Healing the professional culture of medicine. Mayo Clin Proc. 2019;94(8):1556–1566. doi:10.1016/j.mayocp.2019.03.026 Epub 2019/07/16 PubMed PMID: 31303431.
4. Shanafelt TD, Wang H, Leonard M, et al. Assessment of the association of leadership behaviors of supervising physicians with personal-organizational values alignment among staff physicians. JAMA Network Open. 2021;4(2):e2035622. doi:10.1001/jamanetworkopen.2020.35622
5. Berenson RA, Ginsburg PB, May JH. Hospital-physicians relations: cooperation, competition, or separation? Health Aff. 2007;26(1):w31–43. doi:10.1377/hlthaff.26.1.w31 PubMed PMID: 17148489 Epub 2006/12/07.
6. Abdulsalam Y, Gopalakrishnan M, Maltz A, Schneller E. The impact of physician-hospital integration on hospital supply management. J Oper Manage. 2018;57:11–22. doi:10.1016/j.jom.2018.01.001
7. Petriglieri JL. Under threat: responses to and the consequences of threats to individuals’ identities. Acad Manage Rev. 2011;36(4):641–662.
8. Swensen S, Kabcenell A, Shanafelt T. Physician-organization collaboration reduces physician burnout and promotes engagement: the mayo clinic experience. J Healthc Manag. 2016;61(2):105–127. Epub 2016/04/27. PubMed PMID: 27111930.
9. Braithwaite J, Herkes J, Ludlow K, Testa L, Lamprell G. Association between organisational and workplace cultures, and patient outcomes: systematic review. BMJ open. 2017;7(11):e017708. doi:10.1136/bmjopen-2017-017708
10. Mannion R, Davies H. Understanding organisational culture for healthcare quality improvement. BMJ. 2018;363:k4907. doi:10.1136/bmj.k4907 Epub 2018/11/30 PubMed PMID: 30487286; PubMed Central PMCID: PMCPMC6260242.
11. Curteanu D, Constantin I. Organizational culture diagnosis-a new model. Leadership Mentoring Coaching Motiv. 2010;11(1):14–21.
12. Kreindler SA, Dowd DA, Dana Star N, Gottschalk T. Silos and social identity: the social identity approach as a framework for understanding and overcoming divisions in health care. Milbank Q. 2012;90(2):347–374. doi:10.1111/j.1468-0009.2012.00666.x Epub 2012/06/20 PubMed PMID: 22709391; PubMed Central PMCID: PMCPMC3460209.
13. Gittell JH. Transforming Relationships for High Performance: The Power of Relational Coordination. Vol. x. Stanford, California: Stanford Business Books, an imprint of Stanford University Press; 2016:307.
14. Schein EH, Schein PA. Humble Leadership: The Power of Relationships, Openness, and Trust.
15. Charmaz K. Constructing Grounded Theory. Vol. xiii. London; Thousand Oaks, Calif: Sage Publications; 2006:208.
16. Corbin JM, Strauss AL. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory.
17. Spradley JP. The Ethnographic Interview. Vol. vii. New York: Holt, Rinehart and Winston; 1979:247.
18. Keller EJ, Vogelzang RL, Freed BH, Carr JC, Collins JD. Physicians’ professional identities: a roadmap to understanding ”value” in cardiovascular imaging. J Cardiovasc Magn Reson. 2016;18(1):52. doi:10.1186/s12968-016-0274-x Epub 2016/08/28 PubMed PMID: 27566058; PubMed Central PMCID: PMCPMC5002193.
19. Edmondson AC, Harvey J-F. Cross-boundary teaming for innovation: integrating research on teams and knowledge in organizations. Human Res Manag Rev. 2018;28(4):347–360. doi:10.1016/j.hrmr.2017.03.002
20. Schein EH, Schein PA. The Corporate Culture Survival Guide. Hoboken, New Jersey: John Wiley & Sons, Inc.; 2019.
21. Greenaway KH, Wright RG, Willingham J, Reynolds KJ, Haslam SA. Shared identity is key to effective communication. Personality Soc Psychol Bull. 2015;41(2):171–182. doi:10.1177/0146167214559709
22. Kreindler SA, Larson BK, Wu FM, et al. The rules of engagement: physician engagement strategies in intergroup contexts. J Health Organ Manag. 2014;28(1):41–61. doi:10.1108/JHOM-02-2013-0024 Epub 2014/05/03 PubMed PMID: 24783665.
23. Seshadri SB, Piderit SK, Perelli SJ, editors. Sensemaking and meaning-arbitrage in loosely-coupled healthcare organizations.
24. Stubblefield A. The Baptist Health Care Journey to Excellence: Creating a Culture That WOWs! Vol. xiv. Hoboken, N.J: John Wiley & Sons, Inc.; 2005:225.
25. Goodall AH. Physician-leaders and hospital performance: is there an association? Soc Sci Med. 2011;73(4):535–539. doi:10.1016/j.socscimed.2011.06.025 PubMed PMID: 21802184.
26. Kaissi A. Enhancing physician engagement: an international perspective. Int J Health Serv. 2014;44(3):567–592. doi:10.2190/HS.44.3.h
27. Quinn JF. First and foremost, physicians: The clinical versus managerial identities of physician leaders. Unpublished thesis proposal, Case Western Reserve University. 2010.
28. De Brantes F, Eccleston S. Improving Incentive to Free Motivation. Health Care Incentives Improv Inst. 2013;2013:1.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing Virtual vs In-Person Immersive Leadership Training for Physicians
Fernandez CSP, Hays CN, Adatsi G, Noble CC, Abel-Shoup M, Connolly A
Journal of Healthcare Leadership 2023, 15:139-152
Published Date: 11 August 2023
Physicians’ Perceptions and Experiences Regarding Leadership: A Link Between Beliefs and Identity Formation
Lüchinger R, Audétat MC, Bajwa NM, Bréchet-Bachmann AC, Richard-Lepouriel H, Dominicé Dao M, Junod Perron N
Journal of Healthcare Leadership 2024, 16:263-276
Published Date: 1 July 2024