Back to Journals » Advances in Medical Education and Practice » Volume 16
Exploring the Multidimensional Advantages of Productive Failure in Cultivating Clinical Thinking, Collaboration, Stress Management, and Learning Retention in Resident Physicians
Authors Ding Y ![]() , Wang H
, Wang H ![]() , Wang X, Angula LN, Fang N
, Wang X, Angula LN, Fang N
Received 13 June 2025
Accepted for publication 21 December 2025
Published 31 December 2025 Volume 2025:16 Pages 2491—2505
DOI https://doi.org/10.2147/AMEP.S546816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Yingjie Ding, Heng Wang, Xin Wang, Laina Ndapewa Angula, Ning Fang
Department of Otorhinolaryngology, First Hospital of Jilin University, Changchun, Jilin, People’s Republic of China
Correspondence: Ning Fang, Department of Otorhinolaryngology, the First Hospital of Jilin University, Changchun, Jilin, 130021, People’s Republic of China, Email [email protected]
Abstract: The Productive Failure (PF) technique is an educational strategy that uses collaborative problem-solving to facilitate resident physicians’ understanding of new concepts. A novel implementation of this approach is PF simulation, in which they engage in simulation before receiving comprehensive teaching on the involved aspects. PF commences with the generation and consolidation phases, where resident physicians develop and analyze the advantages and constraints of various Representations and Solution Methods. These are followed by the knowledge assembly phases, respectively. Wherein physicians gain essential concepts by organizing their representations and thoughts in alignment with established responses. PF is deliberately designed to induce failure in problem-solving; however, in the following review, this process of failure can help resident physicians better acquire target ideas. The crucial aspect of PF design is that throughout the problem-solving phase, physicians receive no instructional support or scaffolding. Explicit failure-driven scaffolding is an alternative method for enhancing the efficacy of preparatory problem-solving. This narrative review examines the theoretical foundation of PF and its role in collaboration, clinical reasoning development, stress management, and knowledge retention among resident physicians. Using cognitive psychology, clinical reasoning theories, and reflective practice, we examined how PF helps people learn from failure, shift from traditional teaching to retain knowledge long-term, and develop flexible skills in complex clinical settings. Highlighting these components underscores the significance of practical simulations, varied information sources, and systematic feedback in cultivating these competencies. The role of PF in medical education policy suggests ways to integrate it into future training models to address current curriculum gaps. Future directions for PF in medical education include individualized learning, interdisciplinary collaboration, and the integration of future technologies such as virtual reality (VR). PF constitutes a viable educational approach for augmenting the clinical and cognitive competencies of resident physicians, equipping them with the intricacies of contemporary medical practices.
Keywords: stress management, productive failure, clinical reasoning, resident physicians, collaborative learning
Introduction
Clinical medical science is a rigorous and demanding field that requires a high level of scientific thinking. Cultivation of clinical thinking is an essential manifestation of medical science in clinical teaching. Clinical thinking involves combining basic theoretical knowledge with clinical experience, critically evaluating and reflecting on specific clinical phenomena, and ultimately drawing conclusions that align with reality.1 Upon commencing their practice, physicians encounter an unforeseen fusion of challenges: those they have academically prepared for and those they have not previously faced. The new paradigm in clinical thinking and cognition suggests that it is social and dialogical, rather than monological and individual.2 By presenting critical thinking as a broad umbrella for various thinking modes, resident physicians might misinterpret the distinct logics and purposes of these modes. Both resident physicians and scientists require a set of cognitive strategies, including critical thinking, clinical judgment, diagnostic reasoning, cautious rationality, scientific reasoning, effective communication, argumentation, and creative thinking.3 The ability to handle ambiguous situations, manage stress, and maintain effective collaboration is crucial for clinical reasoning in a multidisciplinary environment. But when things are unclear, clinical reasoning becomes more complex because nurses must cope with missing information, unexpected patient reactions, and rapidly changing clinical settings. Psychological and social aspects, including stress management and collaboration, are essential for making educated therapeutic decisions, particularly in emergency or high-pressure contexts.4
The cognitive apprenticeship model effectively integrates theoretical knowledge with clinical practice through observation, participation, clinical reasoning, and independent practice, thereby promoting skill development.5 Cognitive apprenticeship is a teaching method that helps resident doctors learn essential thinking skills, such as analysis, interpretation, and decision-making. Developing these skills involves a complex learning process because much of it occurs internally and is not directly observable.6 Resident physicians begin medical training with a comparatively strong capacity for reflection, indicating they already possess a basic ability for growth in this skill. Nonetheless, it highlights the need to include structured self-reflection exercises consistently throughout the medical education program.7 Over the past two decades, reflection and reflective practices have been widely adopted across various healthcare fields, likely because practitioners have recognized the importance of integrating experiential learning. This includes professions such as occupational therapy, physical therapy, nursing, therapy, and medicine.8 The role of educators in fostering collaboration and emotional resilience has not been extensively studied. Educators must create a learning environment that nurtures adaptable expertise, autonomous learning, and stress resilience. These components are essential for future medical professionals who will encounter increasingly complex and unpredictable medical environments.9
Physicians face an unexpected mixture of challenges: those they have studied academically and those they have not encountered before. Consequently, education should not only expose trainees to familiar, everyday difficulties but also equip them to devise solutions for novel and anticipated challenges in practice.10 Traditional teaching methods often struggle to fully engage resident physicians or replicate the complexities of real-world medical decision-making.11 The present training mainly concentrates on theoretical knowledge and procedural abilities, although it insufficiently highlights adaptive competence and the ability to manage unpredictable, high-pressure clinical scenarios. Research has shown that student nurses often feel anxious and fearful during clinical placements, which, in turn, affects their responses to the clinical learning environment. This widening gap in clinical training may impair residents’ capacity to think critically, make well-informed decisions, and modify strategies when encountering new situations and problems.12 Productive failure (PF) is an educational method that requires physicians to grapple with problem-solving before receiving direct instruction on a specific idea. PF emphasizes stimulating deep learning and understanding by allowing resident physicians to experience failure while solving problems or completing tasks. Compared to traditional teaching methods, PF emphasizes the beneficial experiences that resident physicians gain from failures rather than focusing solely on obtaining the correct answers (Figure 1).13 This ability is a fundamental requirement for physicians to solve practical clinical problems independently. However, traditional medical education tends to focus more on imparting knowledge, leading to a lack of enthusiasm among resident physicians to actively apply theoretical knowledge to clinical practice, thereby hindering the cultivation of clinical thinking.14
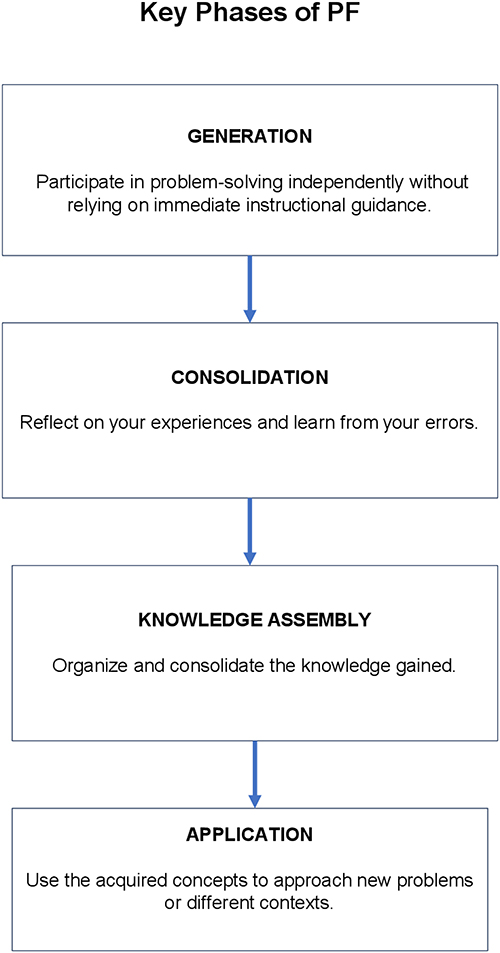 |
Figure 1 The use of PF in medical training follows a cyclical process. It starts with a requirement assessment (pre-test) to identify challenges faced by resident physicians. Next is the design phase, where scenarios are created to evaluate physicians in virtual or real clinical settings. These scenarios are then integrated into ward rounds or daily teaching sessions. The procedure ends with a post-test to evaluate efficacy. Emotional support is continually provided to aid physicians in cultivating resilience and coping strategies. The process culminates in continuous feedback and enhancement. |
As resident physicians move from theoretical knowledge to practical application, cultivating adaptive expertise becomes crucial.15 Adaptive expertise provides a framework for understanding and cultivating professionals who can effectively balance the two dimensions of work. As in most domains of expertise, the acquisition of specialized knowledge is fundamental to adaptive expertise.16 This guarantees that resident physicians attain procedural fluency, that is, the ability to reproduce effective solutions with conceptual understanding, which entails comprehending the logic and mechanics behind an action or decision. Adaptive experts can utilize both procedural and conceptual knowledge as required for problem-solving. This enables professionals to rely on a single answer in new or complex situations, while preserving the reasoning and adjusting the action as necessary.17,18
Adaptive expertise encompasses integrating efficient problem-solving in clinical situations with established solutions, while also having the capacity to adapt and innovate when confronted with unfamiliar challenges.19 Educational methods demonstrated for developing adaptive expertise include the implementation of PF.20 The expertise above is characterized as “preparation for future learning” (PFL) and is central to pedagogical methods that prioritize the development of adaptive expertise.21 Educational methodologies that facilitate the development of PFL aim to provide trainees with instructional and evaluative cycles that enable the gathering and use of knowledge, as well as the application of pre-existing knowledge to comprehend new concepts or address innovative challenges.22
The Correlation Between PF and Medical Education
PF suggests that resident physicians are more likely to understand the essence of problems by experiencing failure during the problem-solving process.23 The role of teachers in the face of PF is to guide resident physicians to think and explore, rather than just imparting the correct answers. Resident physicians encounter various difficulties in problem-solving, and teachers’ roles are to help them overcome them. PF is typically applied to problems with specific challenges and complexities. This fosters resident physicians’ interest, motivates them to explore other options, and facilitates learning from failures.24 Following the failure, the resident physicians are urged to participate in a meta-cognitive evaluation, focusing on the knowledge acquired, practical methodologies, and potential areas for improvement. This cultivates residents’ critical thinking and problem-solving skills. PF may also be associated with social learning. PF emphasizes the learning process and encourages medical residents to think profoundly and explore knowledge through trial and error. This concept has been applied to various disciplines and educational fields.13
The application of PF in the cultivation of clinical thinking among resident physicians can be based on multiple theoretical foundations, including cognitive psychology, medical education, and clinical teaching theory.25 For example:
Clinical reasoning and problem-solving: PF can help cultivate these abilities among resident physicians. Cognitive psychology theory suggests that facing failure prompts individuals to engage in deeper thinking, leading them to analyze and solve problems more systematically.26 Two significant learning theories have influenced contemporary research on improving knowledge acquisition: constructivism and cognitive load theory. Constructivism highlights the autonomous advancement of mathematical concepts by resident physicians. The fundamental premise is that resident physicians actively construct their mathematical comprehension rather than only passively receiving it from external sources. Cognitive load theory states that unrestricted exploration of a highly intricate environment can exhaust working memory, resulting in poor learning outcomes. Advocates of this view further argue that constructivist strategies provide resident physicians with information beyond their working memory capacity and therefore do not effectively support their acquisition of mathematical knowledge.27
Rumination, along with inherent inclinations toward negative emotions triggered by the acknowledgment of objective failures, results in heightened negative affect throughout a five-minute duration. In accordance with our predictions, individuals exhibiting elevated levels of dejection in the promotion failure condition demonstrated the most pronounced correlation between post-meditation dejection and rumination. Similarly, individuals exhibiting minimal quiescence in the preventive failure condition demonstrated the most pronounced correlation between post meditation quiescence and rumination. These findings align with prior research indicating a reciprocal relationship in which negative affect prospectively forecasts heightened state rumination, and higher state rumination subsequently predicts elevated negative affect.28
Reflective Practice Theory
PF provides opportunities for reflection and helps resident physicians examine their clinical practice. Through reflection, doctors can gain a deeper understanding of their decision-making process, the reasons for diagnostic errors, and make adjustments and improvements in practice.29 The influence of reflection on medical trainees and its optimal application in graduate medical education remains ambiguous. Resident physicians established the objectives and recorded written reflections on the online portfolio. The results indicated an enhancement in the reflective capacity over time. Research shows that reflection positively influences empathy, augments comfort in navigating complicated learning scenarios, and boosts involvement in the educational process. Reflection enhances the comprehension of complex subjects, deepens professional values, and improves attitudes and comfort when resident physicians engage in challenging topics.30
Research examining the impact of reflection on residents’ learning has indicated that graduates who are taught reflective practices continued to engage in them after training. This aligns with Schön’s reflective practice and Moon’s notion that reflection facilitates a transition from superficial to profound learning.31
Introduce Diverse Sources of Information
Enable access to a wide range of information sources, including patient medical records, examination reports, and test results. This helps simulate the real clinical decision-making process and cultivates residents’ ability to obtain information from multiple perspectives and conduct comprehensive analysis.26 These cognitive processes allow physicians to connect new information with existing knowledge and intuitive concepts. Methods that draw upon prior knowledge and intuitive concepts while explicitly highlighting the constraints of the current knowledge framework and its relationship to new materials may be particularly effective in enhancing conceptual understanding. One method of eliciting prior knowledge and intuitive concepts is to have medical residents investigate problems before instruction. Recent research indicates that engaging in problem-solving before instruction may enhance the acquisition of conceptual information. Physicians who initially addressed difficulties with an unfamiliar subject before receiving training surpassed those who received direct teaching (instruction without prior problem-solving) in conceptual knowledge, but this did not detract from procedural skill development. It is generally contended that problem-solving before lectures encourages medical residents to engage their existing expertise and intuitive concepts related to the subject matter.32
Cognitive dissonance theory: Faced with failure, resident physicians may encounter cognitive dissonance where their existing cognitive structures do not align with their actual experiences. This cognitive dissonance inspires doctors to actively seek solutions, prompting them to adjust and optimize their clinical thinking.33 When two beliefs are contradictory, physicians may experience an unfavorable cognitive conflict known as cognitive dissonance. To mitigate the discomfort induced by cognitive dissonance, individuals will attempt to modify one of their beliefs. For instance, when confronted with a challenging option, individuals will alter their perspective to rationalize their choice.
- Resident physicians confronting this issue experience internal struggles because their values conflict with the choice at hand. For instance, people may hold views that support the dismissed alternatives. Thus, they are compelled to mitigate conflicts by rationalizing their decisions. Justification is generally accomplished by altering attitudes and beliefs to ensure that new perspectives align with and rationalize the chosen decision. The resultant alteration in the mindset can be enduring.34
- Ambiguity problem-solving: Clinical practice often involves vague and complex issues. PF can be designed as a fuzzy problem, enabling doctors to develop better problem-solving skills when facing uncertainty and complexity. When implementing PF, the key is to ensure that failure is constructive and has learning value. By providing timely feedback, guidance, and support, resident physicians can learn from failures and improve their clinical thinking and practical skills.35
Highlighting the Unique Contribution of PF to the Cultivation of Clinical Thinking
PF makes a unique contribution to cultivating clinical thinking with the following key points highlighted:
- Simulation of authentic clinical scenarios: PF is performed by creating genuine clinical events that provide resident physicians with experience handling challenging medical circumstances. This authenticity enhances resident physicians’ clinical reasoning abilities and capacity to adapt to real-world clinical issues.36
- Emphasizing the problem-solving process: Unlike traditional teaching, which focuses on results, PF places more emphasis on the problem-solving process. Through the experience of failure, resident physicians can not only obtain the correct answer but also understand the principles, logic, and complexity of the problem, thus better cultivating the depth and breadth of clinical thinking.37
- Promoting team collaboration and communication: PF often manifests as group cooperation, emphasizing the collaboration of medical teams. Facing failure together, resident physicians have learned to collaborate, share knowledge, and communicate effectively, which is crucial for cultivating clinical thinking.38
- Strengthening self-directed learning and reflection: PF encourages resident physicians to pursue knowledge actively and continuously improve their learning outcomes through failure and reflection. This habit of self-directed learning enables resident physicians to take greater initiative and think more independently, fostering a deep learning mindset.39
- Cultivating the ability to resist stress and uncertainty: Clinical work is full of uncertainty and pressure, and PF can cultivate resident physicians’ ability to remain calm and thoughtful in the face of difficulties and pressure in a relatively safe teaching environment. This ability is crucial to the maturity of clinical thinking.40
- Stimulating long-term memory and knowledge transfer: PF makes knowledge more concrete and practical through contextualized learning. This helps strengthen long-term memory and enables resident physicians to transfer learned knowledge to practical clinical practice more effectively.
By highlighting these characteristics, PF can not only improve resident physicians’ practical operational ability but also play a unique and positive role in the development of clinical thinking.41
Design and Implementation of PF
When designing a failure, one should choose cases that are close to actual clinical situations or use real cases as the basis for failure, covering different departments, diseases, and conditions. Ensure that the situation is representative and can simulate the complex medical problems that resident physicians face in their actual work (Table 1). Effectively evaluating resident physicians and offering upward feedback requires a design that adheres to three key principles: (1) implementing a well-structured evaluation system grounded in a validated quality assessment tool, (2) delivering feedback that supports learning, and (3) ensuring the evaluation system is acceptable to users.42 Feedback on their teaching performance related to this role should be delivered thoughtfully and constructively. Outcomes include increased awareness of clinical teaching, residents developing feedback skills, reduced hierarchy, and an improved learning environment.43 Beyond theoretical design principles, future uses of the PF method should include statistical data and specific case studies. The Objective Structured Clinical Examination (OSCE) offers a more dependable approach for assessing trainee proficiency than conventional clinical assessments. It operates in concert with other conventional approaches, including multiple-choice questions and performance evaluations at the conclusion of rotations. To ensure reliable and valid results, it’s essential to sample the relevant competencies adequately, have enough stations, and sufficiently train examiners and standardized patients.44 Furthermore, including a variety of case studies from different specialties and at various stages of residency can demonstrate the real-world benefits of PF and its adaptability across clinical settings.
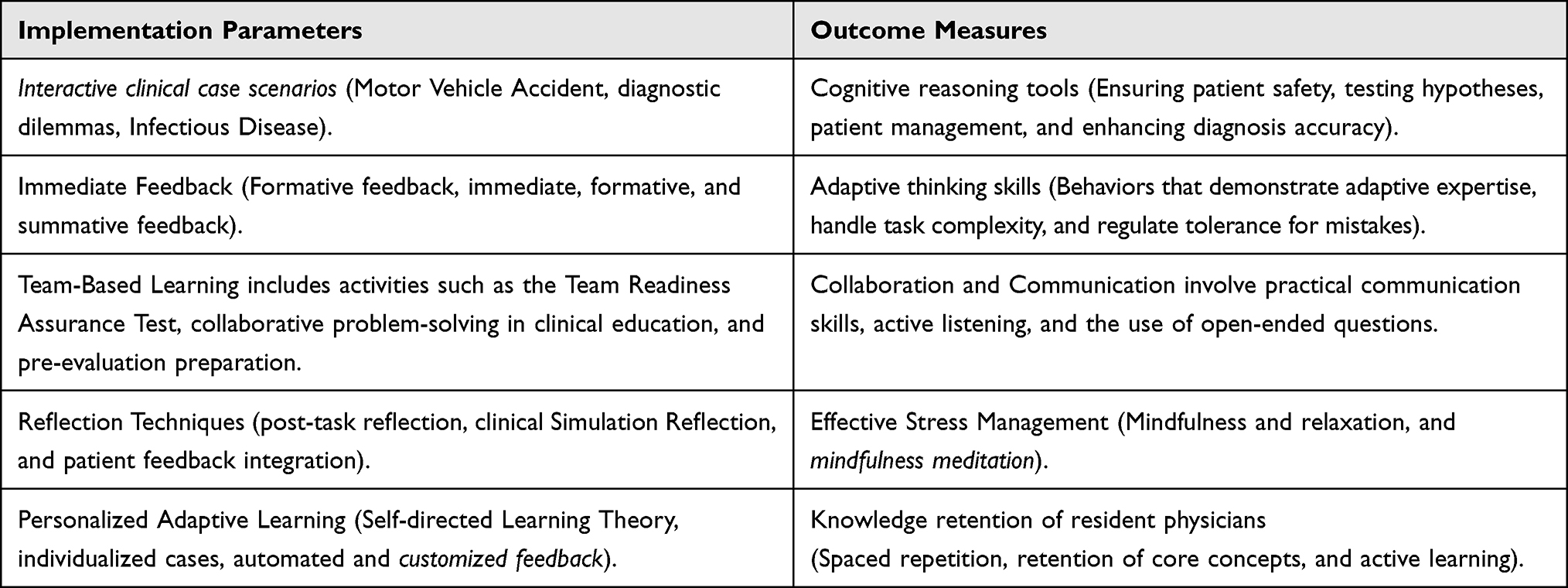 |
Table 1 Implementation Parameters and Outcome Measures for Using PF in Clinical Education |
Clarify the learning goals for failure and ensure that tasks are specific and clear. Resident physicians need to develop a level of clinical problem-solving to maximize PF. The clinical learning environment has a significant influence on resident physicians’ perceptions of stress from teachers. The nature and intensity of stressful events during clinical practice differ across various years of study.45 While the supervision experience impacts how resident physicians perceive the clinical environment overall, it does not affect their physio-psychosocial well-being, the types of stressors they encounter, or their coping strategies. There is increasing awareness of how the psychosocial work environment impacts the quality of care. Stressed physicians tend to treat patients less effectively, both medically and psychologically, and are more susceptible to making judgment errors.46
Although the benefits of PF are well acknowledged in the literature, its implementation can be made more innovative by investigating how its effectiveness varies across different contexts.41 Sinha and Kapur (2021) conducted a meta-analysis of more than 12,000 participants across 166 experimental comparisons to assess the efficacy of PF over the last 20 years. The findings indicated that resident physicians in problem-focused courses greatly surpassed their counterparts in traditional instruction-first settings regarding conceptual understanding and transfer, with a Cohen’s d of 0.36. Importantly, this improvement did not come at the expense of procedural knowledge. Additionally, higher adherence to PF design principles correlated with more potent effects, reaching a Cohen’s d of up to 0.58, which is approximately three times the influence of a skilled teacher on student learning over a year. These results underscore the significance of PF as an established technique for enhancing both conceptual understanding and problem-solving skills.47
Provide rich sources of information, including patient medical records, examination reports, and laboratory results. This helps simulate the real clinical decision-making process and cultivates residents’ ability to obtain information from multiple perspectives and conduct comprehensive analysis. Resident physicians are encouraged to utilize all available data sources, including peer evaluations, to evaluate their ability to synthesize this information effectively. Peer feedback is crucial and provides unique insights for medical residents, especially in enhancing professionalism, collaboration, and interpersonal skills. Different approaches to peer assessment and feedback are used in residency training, although there is no consensus on the most effective method.48 Additionally, deidentified survey and focus group data prevented analysis at the individual response level. A significant strength of this study is the application of focus groups, which facilitated a more profound comprehension of resident views and preferences about peer feedback systems.49 Future implementations must fully disclose statistical results, including effect sizes, p-values, and confidence intervals, to support assertions of PF’s influence. Using tables or figures to structure this data provides clearer insights into the impact of PF on residents’ clinical development over time.
PF is designed as a form of group collaboration that simulates the collaboration of a medical team. Clinical work often requires multidisciplinary collaboration, and group cooperation can cultivate residents’ communication and collaboration skills within the team. Along with the group collaboration aspect, residents’ teamwork was evaluated through rubrics that assessed their interaction during tasks. The TeamUP rubric is valuable for defining, teaching, and assessing teamwork skills among resident physicians.50 The TeamUp rubric was chosen as the initial standardized measure of teamwork and was tested in a second-year undergraduate course (Phase One). While the tool demonstrated acceptable psychometric properties, concerns arose that it was too lengthy, which could potentially hinder student completion. This led to refinements and modifications, resulting in the development of the Team-Q, which was subsequently tested again in the same undergraduate course (Phase Two). This Interdisciplinary collaboration estimates fell within an acceptable range, but logistical challenges made external evaluations less feasible.51
Provide timely and specific feedback to help resident physicians understand the causes of errors, solutions, and directions for improvement. Feedback should be personalized, focusing on the particular performance of individual physicians in the problem-solving process. Feedback is provided immediately after each task, offering formative assessments that highlight specific areas for subsequent improvement. One reason feedback often does not help resident physicians improve or develop into self-regulating, critical thinkers is that they are rarely involved in assessment discussions, especially regarding feedback.52 It is argued that feedback should not be viewed merely as an artifact provided by educators to resident physicians in a one-way communication. Instead, it should be regarded as a resident-physician-centered process in which residents interpret performance information and use it to enhance their future performance. According to this view, feedback should not be seen solely as something that happens after submission, but rather as an ongoing process that occurs during or connects performances.53
The design of PF should guide resident physicians to engage in deep learning rather than simply memorizing them to cope with challenges. They should be encouraged to pursue more background knowledge and gain a more comprehensive understanding of the problem through independent exploration.54 Resident physicians are compelled to engage in independent learning by exploring supplementary resources and reflecting on their problem-solving approaches. Autonomous learning is a fundamental aspect of education that fosters crucial skills such as critical thinking, problem-solving, and adaptation. These characteristics are essential for success in an evolving professional environment. Encouraging individual study fosters lifelong education, continuous self-improvement, and expands knowledge beyond conventional academic environments.55
Introduce reflection and discussion during the failure process and encourage resident physicians to share their thinking processes, experiences, and solutions. This helps deepen learning and promotes knowledge sharing and exchange.38 To enhance the effectiveness of the failure process, it is crucial to incorporate structured reflection and guided discussion. Deliberate reflection is a method that helps physicians improve their diagnostic reasoning by directing them to analyze a clinical case in a structured way.56 Deliberate reflection is a method that has been empirically examined for its impact on diagnostic reasoning and learning over the last 15 years.29 Deliberate reflection centers on the connection between a specific disease and its signs and symptoms. It first aims to verify a hypothesis by finding evidence that supports the underlying illness script. Next, it looks for findings that disprove the script, and finally, it searches for any omissions if the script were accurate. The process closely resembles how a scientist gathers empirical evidence to test their hypothesis.29
Given the disciplinary backgrounds and individual differences of resident physicians, PF design should offer some flexibility and personalization to meet the learning needs of different medical residents. The PF process should include adaptable scenarios that cater to each resident physician’s distinct learning styles, cognitive strengths, and clinical interests. Customized learning plans, bolstered by formative assessments, can identify case studies or simulation challenges that address individual learning gaps, ensuring that each resident encounters both familiar and novel clinical settings.36
Establish a regular evaluation mechanism that includes qualitative and quantitative assessments of student performance. This helps monitor the effectiveness of failure, adjust teaching strategies promptly, and ensure that training objectives are achieved (Figure 2).57 Creating a robust assessment framework is essential for measuring the PF method’s impact on resident physicians’ learning outcomes. OSCE is widely recognized as the “gold standard” for evaluating clinical skills and remains a key part of undergraduate medical assessments. Its reliability supports its potential application in both formative and summative settings.58 Formative assessments, in conjunction with pre- and post-simulation evaluations, provide critical insights into residents’ clinical reasoning and problem-solving abilities. These evaluations should examine the precision of therapeutic judgments and scrutinize the failure process, including its effects on long-term learning and skill development. Feedback should be an ongoing process wherein resident physicians consistently reevaluate their goals and analyze their progress. This ongoing discourse fosters profound contemplation, allowing them to adjust their learning methodologies and progressively enhance their abilities. This strategy also equips resident physicians for future roles in medical practice, underscoring the importance of seeking, accepting, and implementing feedback for continuous professional development.59
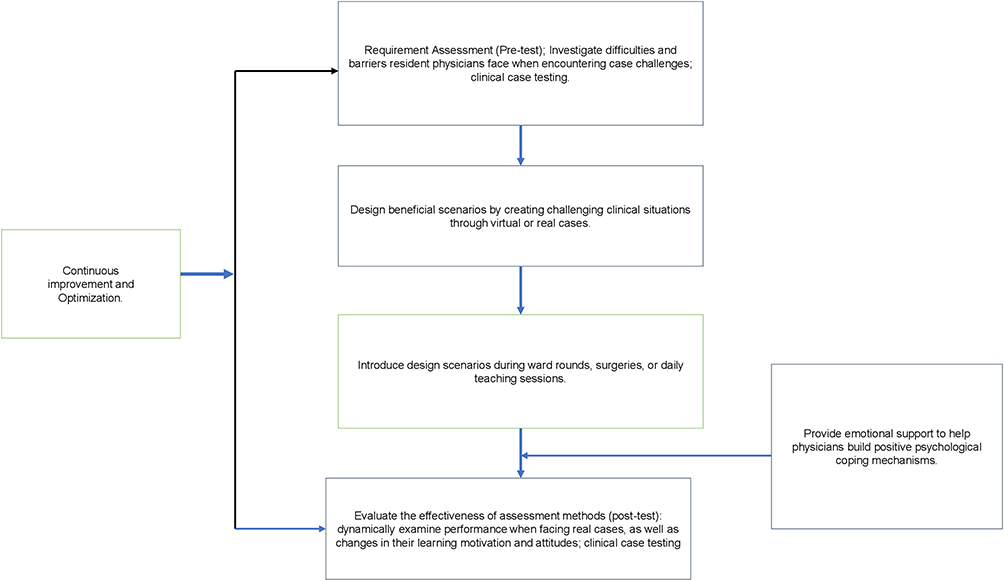 |
Figure 2 The development of clinical reasoning involves the four main stages of PF. |
Specific Examples of Implementing PF
Case
Cardiac Emergency Resuscitation. Background: An elderly patient was urgently referred to the emergency room with complaints of chest pain, shortness of breath, signs of decreased blood pressure, and a rapid heart rate. Preliminary medical history suggested that the patient had a history of hypertension and high cholesterol levels. The medical team should quickly and accurately assess and intervene with patients during emergency treatment.
Tasks
- Teamwork: Assign various tasks within a group to simulate collaborative work within the medical team. Doctors, nurses, emergency personnel, and others each play different roles and work together to provide emergency care to patients.
- Information integration: Provide relevant information about patients, including clinical history, vital signs, and laboratory results. Requires resident physicians to integrate information and develop preliminary diagnoses and emergency plans quickly.
- Decision-making and emergency handling: Challenging factors introduced in the simulation, such as fluctuations in electrocardiogram readings and variations in laboratory results. Resident physicians should be required to make decisions and provide emergency treatment in urgent situations, while considering possible complications and drug reactions.
- Self-directed learning and reflection: After the simulation, a discussion session was organized for resident physicians to share their experiences in emergency rescue, learn independently, and reflect. Emphasize lessons learned from failures and encourage them to propose improvement plans.
- Real-time feedback: Provides real-time guidance and feedback with a special focus on the adaptability, teamwork, and decision-making abilities of resident physicians in emergencies. Feedback should be specific, helping resident physicians correct errors promptly and improve their performance.
This case design combines real-life emergency rescue situations, emphasizing teamwork skills, information integration, self-learning, and decision-making. By simulating actual emergency scenarios, PF can provide strong support for cultivating resident physicians’ clinical thinking and practical skills.60
Analyzing Residents’ Learning Process and Reflection
Through practical simulations of failures, residents have accumulated practical experience in emergencies. This practical experience not only enhances their proficiency in practical operations but also strengthens their confidence in similar scenarios in the future.61 In addition, when solving cases, residents need to consider multiple perspectives and the overall situation. This helps cultivate their ability to think comprehensively and better understand the patient’s overall situation, rather than just local symptoms. Through these learning processes and reflections, residents can not only improve their clinical thinking skills in the face of failure but also cultivate comprehensive abilities to cope with challenges, work effectively as a team, make ethical decisions, and address other aspects, laying a solid foundation for future medical practice.2
Future Directions for Research and Practice
The future of clinical education, particularly fostering clinical reasoning among resident physicians, is closely linked to the enhancement of the PF method. Considering the favorable results observed in clinical reasoning and problem-solving skills through the implementation of PF, various directions for future research and practice warrant exploration to guarantee its ongoing success and advancement.41 A key topic for investigation is the enduring influence of PF on clinical practice. Future studies should investigate the extent to which the clinical skills and reasoning abilities developed by PF apply to real-world medical practice. Research may examine how learning from failure in controlled settings enhances diagnostic precision, decision-making under pressure, and the capacity to manage complex, confusing clinical scenarios with greater confidence.62 Furthermore, long-term studies could monitor the retention of knowledge acquired by PF and its implementation in prolonged patient care contexts. Another promising direction is integrating PF through interdisciplinary collaboration. While PF often emphasizes individual problem-solving and clinical decision-making, future research could investigate the efficacy of applying PF in multidisciplinary teams.63 Simulating complex, multi-faceted clinical situations involving various medical specialties could potentially help future physicians work more collaboratively, improving communication and teamwork in real-world medical settings. Investigating how PF can foster better interdisciplinary approaches in medical education could be vital, particularly as healthcare becomes increasingly team-oriented.64 The design of personalized learning experiences through PF presents another key avenue for growth. Individual differences in learning styles, cognitive strength, and educational background significantly affect the effectiveness of academic methods. Educators can create more inclusive and engaging learning environments by developing tailored PF experiences that cater to the diverse needs of resident physicians. Research could investigate how PF can be personalized based on cognitive assessments, resident physicians’ preferences, and disciplinary focus, ensuring it can accommodate a broad spectrum of learning styles.65 Additionally, the exploration of emotional intelligence and resilience in the context of PF offers valuable insights.
Clinical environments are inherently stressful, and PF can serve as an effective mechanism to help physicians develop emotional resilience, stress management, and self-reflection skills. Future studies could examine how PF can be designed to cultivate these competencies, enabling residents to manage high-stress situations more effectively, reduce burnout, and approach challenging cases with greater emotional intelligence.66 The function of VR and augmented reality (AR) technology in improving PF represents a new domain for investigation. These technologies can replicate increasingly complex and authentic clinical scenarios, allowing resident physicians to hone their decision-making and problem-solving skills in a virtual environment before encountering them in real life. Examining the influence of VR and AR on PF could enhance the authenticity and efficacy of this instructional approach, thereby providing a more secure environment for learning and experimentation.67
Ultimately, broadening the parameters of ethical decision-making within the PF framework is essential. As medical education increasingly prioritizes ethical considerations, PF could immerse resident physicians in moral issues and intricate patient scenarios where failure and reflection foster profound ethical comprehension. Future studies may explore the design of PF to address its intricate dimensions, fostering a culture of ethical awareness and decision-making within healthcare.
Discussion
The results of this study emphasize the significance of PF in developing clinical reasoning and problem-solving abilities among resident physicians. PF provides an opportunity for deeper introspection and learning by allowing physicians to encounter failure within a regulated, supportive context, which is often absent in conventional teaching methodologies.68 This method challenges residents to address intricate clinical scenarios, fostering not only information acquisition but also the enhancement of critical thinking, adaptability, and resilience. A significant discovery was the failure to enhance the comprehension of clinical concepts. This study demonstrated that addressing clinical issues, experiencing failures, and subsequently receiving specific feedback enables physicians to understand the fundamental mechanics of their mistakes. This thus cultivates a profound and enduring understanding of therapeutic thinking.69 The occurrence of failure fosters self-directed learning, prompting residents to contemplate their decision-making, refine their techniques, and implement new knowledge in subsequent cases. Furthermore, the PF technique seems to enhance teamwork and communication skills, as it is often implemented through group-oriented projects. This collaborative element reflects actual clinical practice, where teamwork and effective communication are essential for optimal patient care. Collaborative problem-solving among resident physicians enhances their clinical competencies while fostering essential interpersonal and teamwork skills vital for their professional growth.70 The implementation of PF in clinical education poses obstacles. A primary consideration is to ensure that failure is constructive and that physicians receive sufficient assistance throughout the process. In the absence of adequate scaffolding and prompt feedback, the potential for physicians’ demotivation or dissatisfaction may surpass its advantages.71
Moreover, although PF offers substantial learning opportunities, it also presents distinct risks in clinical environments. Not disclosing mistakes and unexpected results restricts the ability to assess systems and share knowledge through safety alerts, educational sessions, changing practices, and providing chances for better performance. Disclosure also plays a key role in fostering a safety culture. It should be regarded as proa strategy for healthcare institutions aiming to become high-reliability organizations, where errors are rare even in risky settings.72 Furthermore, trainees may become frustrated, particularly if failure is seen as incompetence and not addressed promptly. The clinical environment, often constrained by limited time, may lack the space for reflection and feedback, which are essential to PF’s success.69
Consequently, meticulous design of the PF process, emphasizing explicit learning objectives and suitable coaching, is crucial for optimizing its efficacy. This research posits that PF fosters the cultivation of adaptive expertise, which is essential for managing novel and complex clinical scenarios.73 The capacity to adapt and innovate in response to novel challenges is fundamental to effective therapeutic practice. By cultivating adaptive knowledge, PF equips resident physicians to respond flexibly to the dynamic and unpredictable aspects of clinical practice. In conclusion, although PF offers a promising educational strategy for improving clinical reasoning and problem-solving skills, further research is needed to examine its long-term effects on clinical practice.74 Future research should investigate the impact of PF on knowledge retention and transfer in practical clinical environments, as well as its capacity to develop other critical competencies, including ethical decision-making, emotional intelligence, and stress management.
Conclusion
PF emphasizes the process of problem-solving rather than the result alone. Confronting failure enables resident physicians to develop accurate solutions while understanding the substance, logic, and intricacies of the issues, thereby enhancing their analytical and problem-solving skills. When confronting problems and emergencies, resident physicians develop the capacity to respond calmly and make rapid decisions under pressure, which is essential for prompt decision-making in clinical practice. Current evidence is limited, notably due to the absence of large-scale empirical studies in medical education. Additionally, implementing PF in clinical settings may pose challenges, including resource constraints and the need for adequate faculty training.75 Key barriers comprised resistance to change, limited resources, insufficient organisational backing, and a lack of locally produced research.76
Despite these challenges, PF has excellent potential to enhance resident education. Helping resident physicians recognize their knowledge gaps or failures is considered a vital part of failure-based learning methods.77 Future research should focus on longitudinal studies that monitor PF’s effects on diagnostic accuracy, decision-making, and interprofessional teamwork over time. This approach will help clarify how PF can shape long-term clinical skills and adaptability in actual medical practice. The key take-home message is that PF is an innovative approach that fosters critical thinking, self-directed learning, and collaboration, all of which are crucial for the development of competent, adaptive, and resilient physicians in the modern healthcare environment. These opportunities encourage the development of executive functioning skills, which are crucial for 21st-century abilities such as collaboration, problem-solving, and creativity, as well as for handling ambiguity.78
Furthermore, PF underscores the importance of holistic thinking and a global outlook, helping resident physicians develop a thorough, methodical approach, enabling them to evaluate patients’ illnesses more fully and enhancing the quality of diagnostic and treatment strategies. Simultaneously, ethical considerations in failure design can foster resident physicians’ awareness of moral dilemmas, improve their comprehension of and commitment to medical ethical standards, and improve their professional proficiency. Promoting a culture of continuous improvement motivates resident physicians to see failures and challenges as opportunities for growth, fosters an environment of perpetual learning and advancement, and empowers them to refine their skills consistently. Finally, the design of PF can help improve resident physicians’ stress resistance and emotional management skills, enabling them to gradually adapt to high-pressure medical environments in the face of failure. Failure emphasizes that learning is a lifelong process that helps cultivate resident physicians’ awareness of lifelong learning and enables them to adapt to developments and changes in the medical field.
Overall, PF plays a crucial role in several aspects of the comprehensive development of resident physicians’ literacy and clinical thinking. The concept of exploring personalized methods in medical education—such as learning styles and individual cognitive strengths—frequently appears in the literature, marking it as a key future focus for research and application, particularly in remediation and adaptive learning. However, the term “personalized failure design” is not widely recognized or formally studied, though the advantages of learning from failure are commonly accepted in the field. Strategies aimed at enhancing collaboration between health and social care professionals might modestly boost patient functional outcomes, increase professionals’ adherence to recommended practices, and optimize healthcare resource utilization. However, due to limited clear evidence, it remains uncertain whether these strategies actually improve patient-perceived quality of care, ensure better continuity of care, or foster more effective collaborative working.
The research and practical directions for future PF include: first, personalized failure experience design should consider individual differences among resident physicians and achieve targeted failure design by understanding their disciplinary background, learning style, and interests to stimulate maximum learning potential. Second, integrating virtual and AR technologies can create more realistic clinical scenarios, allowing resident physicians to perform practical procedures in virtual environments and enhance their clinical experience while avoiding potential risks.
Third, the interdisciplinary integration of failure design introduces additional elements that simulate collaboration between medical and other majors, helping cultivate resident physicians’ ability to collaborate across disciplines, and fourth, integrating emotional intelligence theory to examine resident physicians’ emotional experiences and coping mechanisms in the face of failure, to cultivate healthier, more positive emotional attitudes. Fifth, the development of cross-level assessment methods helps provide a more comprehensive and multidimensional understanding of the learning process and outcomes of resident physicians in the face of PF, including assessments of knowledge levels, skill mastery, teamwork, communication skills, and other aspects. Finally, by incorporating PF, more content should be developed for doctor-patient communication and ethical education, and resident physicians’ decision-making and communication skills should be cultivated in complex ethical contexts through simulated real-life scenarios. These directions will help continuously promote innovation and optimize PF in medical education, improve comprehensive literacy among resident physicians, and better meet the training needs of future medical professionals.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Jilin Province Postgraduate Education and Teaching Reform Research Project (20241994G99005B, 202419925EH001P). Jilin Provincial Higher Education Teaching Reform Research Project (2024L5LJO6C000X).
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Jensen RD, Ellaway RH, et al. No cow on the ice: a tail of word games. Adv Health Sci Educ. 2024;29(1):1–19. doi:10.1007/s10459-024-10320-8
2. Benner P, Hughes RG, Sutphen M. Clinical reasoning, decisionmaking, and action: thinking critically and clinically. Patient Safety Quality. 2008.
3. Zayapragassarazan Z, Menon V, Kar SS, Batmanabane G. Understanding critical thinking to create better doctors. Online Submission. 2016;1(3):9–13.
4. Cunha LDM, Han PKJ, Ventura F, Pestana-Santos M, Lomba L, Santos MR. Uncertainty management strategies in clinical reasoning: perceptions of nurses in post-anesthesia care units. BMC Nurs. 2025;24(1):605. doi:10.1186/s12912-025-03193-8
5. Salajegheh M. Application of cognitive apprenticeship model in clinical education: a scoping review. J Med Educ Develop. 2023;16(49):78.
6. Dennen VP. Cognitive apprenticeship in educational practice: research on scaffolding, modeling, mentoring, and coaching as instructional strategies. In: J.M. Spector, M.D. Merrill, J. van Merrienboer, and MP. Driscoll, editors. Handbook of Research on Educational Communications and Technology. Routledge; 2013:804–819.
7. Hafiz AM. Factors affecting the level of reflective thinking and clinical decision-making skills in medical faculty students. SiSli Etfal Hastanesi Tip Bulteni. 2023;57(4):543. doi:10.14744/SEMB.2023.52223
8. McIntyre C, Lathlean J, Esteves JE. Reflective practice enhances osteopathic clinical reasoning. Int J Osteopath Med. 2019;33-34:8–15. doi:10.1016/j.ijosm.2019.07.002
9. Chan L, Bilney EVM, Ganotice FA, et al. Unveiling how medical educators conceptualise resilience: a qualitative study. BMC Med Educ. 2025;25(1):1241. doi:10.1186/s12909-025-07834-z
10. Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–1510. doi:10.1007/s11606-013-2441-1
11. Lee C-Y, Lee C-H, Lai H-Y, Chen P-J, Chen -M-M, Yau S-Y. Emerging trends in gamification for clinical reasoning education: a scoping review. BMC Med Educ. 2025;25(1):435. doi:10.1186/s12909-025-07044-7
12. Negm LM, Mersal FA, Fawzy MS, Rajennal AT, Alanazi RS, Alanazi LO. Challenges of nursing students during clinical training: a nursing perspective. AIMS Public Health. 2024;11(2):379. doi:10.3934/publichealth.2024019
13. Steenhof N, Woods NN, Mylopoulos M. Exploring why we learn from productive failure: insights from the cognitive and learning sciences. Adv Health Sci Educ. 2020;25(5):1099–1106. doi:10.1007/s10459-020-10013-y
14. Palominos E, Levett-Jones T, Power T, Alcorn N, Martinez-Maldonado R. Measuring the impact of productive failure on nursing students’ learning in healthcare simulation: a quasi-experimental study. Nurse Education Today. 2021;101:104871. doi:10.1016/j.nedt.2021.104871
15. Gamborg ML, Mehlsen M, Paltved C, Vetter SS, Musaeus P. Clinical decision-making and adaptive expertise in residency: a think-aloud study. BMC med educ. 2023;23(1):22. doi:10.1186/s12909-022-03990-8
16. Pelgrim E, Hissink E, Bus L, et al. Professionals’ adaptive expertise and adaptive performance in educational and workplace settings: an overview of reviews. Adv Health Sci Educ. 2022;27(5):1245–1263. doi:10.1007/s10459-022-10190-y
17. Hatano G, Inagaki K. Two courses of expertise. Res Clin Center Child Develop Ann Rep. 1984;6:27–36.
18. Mylopoulos M, Kulasegaram K, Woods NN. Developing the experts we need: fostering adaptive expertise through education. J Evaluation Clin Prac. 2018;24(3):674–677. doi:10.1111/jep.12905
19. Pusic MV, Hall E, Billings H, et al. Educating for adaptive expertise: case examples along the medical education continuum. Adv Health Sci Educ. 2022;27(5):1383–1400. doi:10.1007/s10459-022-10165-z
20. Kapur M, Rummel N. Productive failure in learning from generation and invention activities. Instructional Sci. 2012;40(4):645–650. doi:10.1007/s11251-012-9235-4
21. Mylopoulos M, Brydges R, Woods NN, Manzone J, Schwartz DL. Preparation for future learning: a missing competency in health professions education? Med Educ. 2016;50(1):115–123. doi:10.1111/medu.12893
22. Woods NN, Mylopoulos M. How to improve the teaching of clinical reasoning: from processing to preparation. Med Educ. 2015;49(10):952–953. doi:10.1111/medu.12823
23. Kapur M, Bielaczyc K. Designing for productive failure. J Learn Sci. 2012;21(1):45–83. doi:10.1080/10508406.2011.591717
24. Lodge JM, Kennedy G, Lockyer L, Arguel A, Pachman M. Understanding difficulties and resulting confusion in learning: an integrative review. Paper Presented. 2018.
25. Song SL, Yu ZZ, Pavlech L, Scott IU, Greenberg PB. Theoretical frameworks in medical education: using a systematic review of ophthalmology education research to create a theory of change model. J Graduate Med Edu. 2022;14(5):568–582. doi:10.4300/JGME-D-22-00115.1
26. Steenhof N, Woods NN, Van Gerven PWM, Mylopoulos M. Productive failure as an instructional approach to promote future learning. Adv Health Sci Educ. 2019;24(4):739–749. doi:10.1007/s10459-019-09895-4
27. Upu H. Constructivism versus cognitive load theory: in search for an effective mathematics teaching. arXiv preprint arXiv:210804796 2021.
28. Moberly NJ, Watkins ER. Ruminative self-focus and negative affect: an experience sampling study. J Abnormal Psychol. 2008;117(2):314. doi:10.1037/0021-843X.117.2.314
29. Mamede S, Schmidt HG. Deliberate reflection and clinical reasoning: founding ideas and empirical findings. Med Educ. 2023;57(1):76–85. doi:10.1111/medu.14863
30. Winkel AF, Yingling S, Jones -A-A, Nicholson J. Reflection as a learning tool in graduate medical education: a systematic review. J Graduate Med Edu. 2017;9(4):430–439. doi:10.4300/JGME-D-16-00500.1
31. Mann K, Gordon J, MacLeod A. Reflection and reflective practice in health professions education: a systematic review. Adv Health Sci Educ. 2009;14(4):595–621. doi:10.1007/s10459-007-9090-2
32. Loibl K, Rummel N. Knowing what you don’t know makes failure productive. Learn Instruct. 2014;34:74–85. doi:10.1016/j.learninstruc.2014.08.004
33. Klein J, McColl G. Cognitive dissonance: how self-protective distortions can undermine clinical judgement. Med Educ. 2019;53(12):1178–1186. doi:10.1111/medu.13938
34. Kitayama S, Tompson S. A biosocial model of affective decision making: implications for dissonance, motivation, and culture. In: Advances in Experimental Social Psychology. Vol. 52. Elsevier; 2015:71–137.
35. Hall KK, Shoemaker-Hunt S, Hoffman L, et al. Diagnostic errors. In: Making Healthcare Safer III: A Critical Analysis of Existing and Emerging Patient Safety Practices [Internet]. Agency for Healthcare Research and Quality (US); 2020.
36. Elendu C, Amaechi DC, Okatta AU, et al. The impact of simulation-based training in medical education: a review. Medicine. 2024;103(27):e38813. doi:10.1097/MD.0000000000038813
37. Ramani S, Leinster S. AMEE guide no. 34: teaching in the clinical environment. Med Teach. 2008;30(4):347–364. doi:10.1080/01421590802061613
38. Rosenstein AH, O’Daniel M. Professional communication and team collaboration. Patient Safety Quality. 2008.
39. Charokar K, Dulloo P. Self-directed learning theory to practice: a footstep towards the path of being a life-long learne. J Adv Med Educ Profess. 2022;10(3):135.
40. Steinauer JE, O’Sullivan P, Preskill F, Ten Cate O, Teherani A. What makes “difficult patients” difficult for medical students? Acad Med. 2018;93(9):1359–1366. doi:10.1097/ACM.0000000000002269
41. Kapur M. Productive failure. Cognition Instruct. 2008;26(3):379–424. doi:10.1080/07370000802212669
42. Fluit C. Evaluation and Feedback for Effective Clinical Teaching. Sl: sn; 2013.
43. Fluit C, Bolhuis S, Klaassen T, et al. Residents provide feedback to their clinical teachers: reflection through dialogue. Med Teach. 2013;35(9):e1485–e1492. doi:10.3109/0142159X.2013.785631
44. Hijazi M, Downing SM. Objective structured clinical examinations as an assessment method in residency training: practical considerations. Ann Saudi Med. 2008;28(3):192–199. doi:10.5144/0256-4947.2008.192
45. Sum MY, Chew QH, Sim K. Perceptions of the learning environment on the relationship between stress and burnout for residents in an ACGME-I accredited national psychiatry residency program. J Graduate Medl Educ. 2019;11(4s):85–90. doi:10.4300/JGME-D-18-00795
46. Arnetz BB. Psychosocial challenges facing physicians of today. Soc sci med. 2001;52(2):203–213. doi:10.1016/S0277-9536(00)00220-3
47. Sinha T, Kapur M. From problem-solving to sensemaking: a comparative meta-analysis of preparatory approaches for future learning. EdArXiv. 2021.
48. de la Cruz MSD, Kopec MT, Wimsatt LA. Resident perceptions of giving and receiving peer-to-peer feedback. J Graduate Med Edu. 2015;7(2):208–213. doi:10.4300/JGME-D-14-00388.1
49. Li M, Xu P, Hu J, Tang Z, Yang G. From challenges and pitfalls to recommendations and opportunities: implementing federated learning in healthcare. Med Image Anal. 2025;101:103497. doi:10.1016/j.media.2025.103497
50. Hastie C, Fahy K, Parratt J. The development of a rubric for peer assessment of individual teamwork skills in undergraduate midwifery students. Women Birth. 2014;27(3):220–226. doi:10.1016/j.wombi.2014.06.003
51. Britton E, Simper N, Leger A, Stephenson J. Assessing teamwork in undergraduate education: a measurement tool to evaluate individual teamwork skills. Assess Eval Higher Educ. 2017;42(3):378–397. doi:10.1080/02602938.2015.1116497
52. Owen L. The impact of feedback as formative assessment on student performance. Int J Teach Learn Higher Educ. 2016;28(2):168–175.
53. Henderson M, Ryan T, Boud D, et al. The usefulness of feedback. Active Learn Higher Educ. 2021;22(3):229–243. doi:10.1177/1469787419872393
54. Hayes MM, Chatterjee S, Schwartzstein RM. Critical thinking in critical care: five strategies to improve teaching and learning in the intensive care unit. Ann Am Thoracic Soc. 2017;14(4):569–575. doi:10.1513/AnnalsATS.201612-1009AS
55. Hoo FJ, Mohd Noh MA, Harun Z, Ibrahim R, Mohsin NA. Open the black box of autonomous learning: a sustainable approach to language learning. J Teach Learn. 2025;19(2):98–114. doi:10.22329/jtl.v19i2.9005
56. Kuhn J, Mamede S, van den Berg P, et al. Learning deliberate reflection in medical diagnosis: does learning-by-teaching help? Adv Health Sci Educ. 2023;28(1):13–26. doi:10.1007/s10459-022-10138-2
57. du Plooy E, Casteleijn D, Franzsen D. Personalized adaptive learning in higher education: a scoping review of key characteristics and impact on academic performance and engagement. Heliyon. 2024;10(21):e39630. doi:10.1016/j.heliyon.2024.e39630
58. Al-Hashimi K, Said UN, Khan TN. Formative objective structured clinical examinations (OSCEs) as an assessment tool in UK undergraduate medical education: a review of its utility. Cureus. 2023;15(5).
59. Lipnevich AA, Mattern K, Feddock C. Formative assessment and feedback in medical education: a practical guide: AMEE Guide No. 189. Med Teach. 2025;1–20. doi:10.1080/0142159X.2025.2569623
60. Boshnjaku A, Krasniqi E, Kamberi F. The emerging need to integrate digital health literacy as a course into health-related and care-related profession curricula. Front Public Health. 2025;13:1534139. doi:10.3389/fpubh.2025.1534139
61. Davis D, Warrington SJ. Simulation training and skill assessment in emergency medicine. 2020.
62. Sinha T, Kapur M. When productive failure fails.
63. Kapur M. Examining productive failure, productive success, unproductive failure, and unproductive success in learning. Educ Psychologist. 2016;51(2):289–299. doi:10.1080/00461520.2016.1155457
64. Weinmayr L-M, Zwierlein R, Steinhäuser J. Modifiable determinants for the success or failure of inter-physician collaboration in group practices in Germany - a qualitative study. BMC Family Practice. 2020;21(1):1–13. doi:10.1186/s12875-020-01349-w
65. Bulger M. Personalized learning: the conversations we’re not having. Data Soc. 2016;22(1):1–29.
66. Cohen C, Pignata S, Bezak E, Tie M, Childs J. Workplace interventions to improve well-being and reduce burnout for nurses, physicians and allied healthcare professionals: a systematic review. BMJ open. 2023;13(6):e071203. doi:10.1136/bmjopen-2022-071203
67. Melo M, Bentley E, McAllister KS, Cortez J. Pedagogy of productive failure: navigating the challenges of integrating VR into the classroom. J Virtual Worlds Res. 2019;12(1). doi:10.4101/jvwr.v12i1.7318
68. Kapur M. Learning from productive failure. Learning. 2015;1(1):51–65.
69. Burgess A, Mellis C. Feedback and assessment for clinical placements: achieving the right balance. Adv Med Educ Prac. 2015;373–381. doi:10.2147/AMEP.S77890
70. Brandt WC. Measuring student success skills: a review of the literature on self-directed learning. 21st century success skills. Nat Center Improve Educ Assess. 2020.
71. Loibl K, Leuders T. How to make failure productive: fostering learning from errors through elaboration prompts. Learn Instruction. 2019;62:1–10. doi:10.1016/j.learninstruc.2019.03.002
72. Wolf ZR, Hughes RG. Error reporting and disclosure. Patient Safety Quality. 2008.
73. Ng SL, Forsey J, Boyd VA, et al. Combining adaptive expertise and (critically) reflective practice to support the development of knowledge, skill, and society. Adv Health Sci Educ. 2022;27(5):1265–1281. doi:10.1007/s10459-022-10178-8
74. Lyng HB, Macrae C, Guise V, et al. Balancing adaptation and innovation for resilience in healthcare – a metasynthesis of narratives. BMC Health Serv Res. 2021;21(1):1–13. doi:10.1186/s12913-021-06592-0
75. Bonfim D, Belotti L, de Almeida LY, et al. Challenges and strategies for conducting research in primary health care practice: an integrative review. BMC Health Serv Res. 2023;23(1):1380. doi:10.1186/s12913-023-10382-1
76. Nalweyiso DI, Mbabazi J, Kabanda J, et al. Barriers and facilitators of evidence-based practice among lecturers at Makerere University College of Health Sciences, Uganda: a qualitative study. Cogent Educat. 2024;11(1):2407185. doi:10.1080/2331186X.2024.2407185
77. Nachtigall V, Serova K, Rummel N. When failure fails to be productive: probing the effectiveness of productive failure for learning beyond STEM domains. Instructional Sci. 2020;48(6):651–697. doi:10.1007/s11251-020-09525-2
78. Lawson L, Charles SC, Lake D, et al. Creating health systems citizens: enhanced professional identity formation through a para-curricular distinction track in health systems transformation and leadership. BMC Med Educ. 2025;25(1):703. doi:10.1186/s12909-025-07108-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.