Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Exploring the Current Tools for Fall Risk Assessment in Older Adults Across Southeast Asia and the Need for Culturally Adapted Models: A Scoping Review
Authors Dharmansyah D ![]() , Rahayuwati L
, Rahayuwati L ![]() , Pramukti I
, Pramukti I ![]() , Mutyara K
, Mutyara K ![]()
Received 22 March 2026
Accepted for publication 12 May 2026
Published 21 May 2026 Volume 2026:22 611180
DOI https://doi.org/10.2147/TCRM.S611180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Fall Risk Assessment in Older Adults Across Southeast Asia – Video abstract [611180]
Views: 25
Dhika Dharmansyah,1,2 Laili Rahayuwati,3 Iqbal Pramukti,3 Kuswandewi Mutyara4
1Doctoral Program in Medicine, Faculty of Medicine, Universitas Padjadjaran, Jatinangor, Sumedang, West Java, 45363, Indonesia; 2Department of Nursing, Faculty of Sport and Health Education, Universitas Pendidikan Indonesia, Bandung, West Java, 40154, Indonesia; 3Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Jatinangor, Sumedang, West Java, 45363, Indonesia; 4Department of Public Health, Faculty of Medicine, Universitas Padjadjaran, Jatinangor, Sumedang, West Java, 45363, Indonesia
Correspondence: Laili Rahayuwati, Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang KM 21, Jatinangor, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Background: Falls are a leading cause of unintentional injury, functional disability, and premature mortality among older adults worldwide, ranking second among causes of unintentional injury-related death globally according to the World Health Organization (WHO), with the burden disproportionately concentrated in low- and middle-income countries, including those across Southeast Asia (SEA). Assessing fall risk is central to primary prevention; however, it remains unclear which tools are recommended or validated for clinical practice across the 11 nations of the Association of Southeast Asian Nations (ASEAN) and whether existing Western-developed instruments adequately account for culturally specific risk determinants in this region.
Aim: This scoping review aimed to identify, review, and map the available literature on fall risk assessment tools used in older adults across SEA countries and to explore the extent to which cultural practices and local wisdom influence their applicability and the need for culturally adapted models.
Methods: This scoping review followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) and the Joanna Briggs Institute (JBI) methodology. Searches were conducted in March 2026 in the Scopus, PubMed/MEDLINE, and Web of Science (WoS) databases. English-language, full-text articles published between 2015 and 2025 from the 11 ASEAN countries were eligible; open-access status was preferred but non-open-access records were also obtained via institutional subscription and author contact. The protocol was pre-registered on the Open Science Framework (OSF; https://doi.org/10.17605/OSF.IO/5DHXK).
Results: Thirty-two primary-data studies from Thailand (n=12), Malaysia (n=10), Indonesia (n=5), Vietnam (n=3), and Singapore (n=2) met the inclusion criteria; three additional regional secondary reviews informed cut-off triangulation. Twelve fall risk tool categories were identified. Western tools dominated (84.4% of primary-data studies) with minimal cultural adaptation. The Timed Up and Go (TUG) test was the most frequently used instrument (25/32 studies), but it showed variable cut-off values (8– 14.3 s). Six ASEAN countries had no eligible primary studies. The weighted mean proportion of female participants was 63.4%; community-dwelling samples predominated (65.6%).
Conclusion: Current fall risk assessment research in SEA is geographically concentrated and dominated by unadapted Western tools. Cultural practices central to SEA — floor-level mobility, barefoot ambulation, and domestic environmental hazards — are systematically unaddressed. Urgent investment in culturally adapted tool development, multicentre validation, and digital scaling is required across ASEAN. We propose an integrative framework, Southeast Asian Fall Assessment for Living and Locality (SEA-FALL), to guide future validation and policy translation.
Keywords: fall risk assessment, older adults, Southeast Asia, ASEAN, culturally adapted tools, scoping review, PRISMA-ScR, timed up and go, frailty, geriatric syndromes
Introduction
Falls are a leading cause of unintentional injury, functional disability, and reduced quality of life among older adults globally, ranking second among causes of unintentional injury-related deaths after road-traffic injuries according to the WHO.1 Approximately 684,000 fatal falls are estimated to occur annually worldwide, with low- and middle-income countries bearing more than 80% of this burden.1 Southeast Asia is undergoing an unprecedented demographic transition: the proportion of adults aged 65 years and above across ASEAN nations is projected to triple from approximately 7% in 2020 to over 21% by 2050, creating an urgent clinical need for effective fall prevention strategies.2
A fall risk assessment is the cornerstone of primary fall prevention. Numerous tools have been developed to predict fall incidence and identify at-risk individuals across clinical and community settings.3 These instruments are intended to assist healthcare professionals in clinical decision-making, targeting preventive interventions including exercise prescription, environmental modification, and medication review.3 Systematic use of validated fall risk tools has been associated with better balance confidence, improved physical performance monitoring, and reduced fall-related hospital admissions.3
Various fall risk assessment tools have been developed, most of which were primarily created for use in Western populations — such as the Stopping Elderly Accidents, Deaths and Injuries (STEADI) algorithm,4 the Morse Fall Scale, and the Physiological Profile Assessment (PPA).5 Because most prediction models were developed in Caucasian populations with distinct body habitus, indoor floor-level habituation, and culturally specific mobility behaviours, they require validation before application in new populations to avoid systematic underestimation or overestimation of fall risk.6 A growing body of literature has focused on validating these tools in diverse populations, with mixed and inconsistent results.7–9
Interplay with Frailty and Other Geriatric Syndromes
Falls in older adults rarely occur in isolation; they cluster with the wider geriatric syndromes of frailty, sarcopenia, cognitive impairment, polypharmacy, and orthostatic dysregulation.10–14 Frailty as defined by the Fried phenotype10 and operationalised by the FRAIL Scale11 independently predicts incident falls, hip fracture, and post-fall mortality. Sarcopenia, codified by the European Working Group on Sarcopenia in Older People 2 (EWGSOP2) consensus,12 reduces lower-limb power and reactive postural control, mechanisms central to most fall-risk performance tests. Comprehensive Geriatric Assessment (CGA) reduces functional decline and institutionalisation in hospitalised older adults13 and is increasingly proposed as the appropriate scaffold within which fall-risk screening should sit.14 Any culturally adapted SEA fall-risk model must therefore be interpretable alongside, not in isolation from, these geriatric-syndrome constructs.
Existing Reviews and the Present Gap
Three previous SEA-focused syntheses have informed our work but each was narrower in scope. Choo et al9 performed a meta-analysis of TUG performance in SEA older adults and proposed a regional cut-off of 13.5 s, but addressed only a single tool. Vo et al15 conducted a SEA systematic review of fear of falling using the Falls Efficacy Scale-International (FES-I), again limited to one construct. Romli et al6 mapped occupational-therapy-based community fall-prevention interventions in SEA but did not synthesise assessment tools. The recent Therapeutics and Clinical Risk Management (TCRM) scoping review by Al-ezzi et al16 on cardiovascular disease (CVD) risk tools in the Middle East provides a structurally analogous methodological precedent in a different clinical-risk domain.
The present scoping review extends this prior work in four ways: (i) it is the first comprehensive mapping of fall risk assessment tools across all 11 ASEAN nations rather than a single tool or construct; (ii) it systematically appraises the cultural adaptation status of each identified tool against the WHO 10-step cross-cultural adaptation protocol and the COSMIN (COnsensus-based Standards for the selection of health Measurement INstruments) framework; (iii) it identifies geographic and methodological gaps in absolute terms, weighting them against national older-adult population sizes; and (iv) it proposes an integrative culturally adapted framework, SEA-FALL, to guide future tool development and validation. Therefore, this scoping review comprehensively synthesised the literature on fall risk assessment tools used for older adults across SEA over the past decade and identified cultural determinants and literature gaps in the region.
Methods
Study Design
To report the findings of this review, the PRISMA-ScR checklist17 and the JBI Manual for Evidence Synthesis (Chapter 11)18 were utilised. The protocol was pre-registered on the OSF Registries prior to data extraction (DOI: https://doi.org/10.17605/OSF.IO/5DHXK).
Eligibility Criteria
Published observational studies (cross-sectional, cohort, longitudinal) and randomised controlled trials (RCTs) reporting the use, validation, or adaptation of fall risk assessment tools for adults aged ≥ 60 years were included. Studies from the 11 ASEAN countries (Brunei Darussalam, Cambodia, Indonesia, Lao PDR, Malaysia, Myanmar, the Philippines, Singapore, Thailand, Timor-Leste, and Vietnam), published in English between 2015 and 2025 were eligible. Open-access publication was preferred, but in response to peer review, non-open-access records were also retrieved via institutional subscriptions (Universitas Padjadjaran and Universitas Pendidikan Indonesia), inter-library loan, and direct author contact. Letters, commentaries, editorials, protocol papers without results, and studies involving younger adults were excluded. Grey literature and backward and forward citation searches were not conducted, in line with the pre-registered protocol.
Information Sources
Searches were conducted in March 2025 in Scopus, PubMed/MEDLINE, and WoS. Search terms and strategies were developed and applied consistently across all databases.
Search Strategies
Two key concepts were used: (1) fall risk assessment tools and (2) Southeast Asian countries and older adults. Synonymous terms were connected using the Boolean operator “OR”; concepts were linked using “AND”. Keywords were searched in titles and abstracts because this is the indexed, comparable field across all three target databases; full-text searching is not consistently supported simultaneously across PubMed, Scopus, and WoS, and a pilot full-text query in PubMed Central alone returned more than 4,300 records dominated by irrelevant hits. To address the risk of missing eligible studies, we performed a sensitivity full-text search in PubMed Central restricted to SEA countries and the target fall-risk terms; this did not identify additional eligible studies beyond those captured by the title/abstract approach. Filters were applied for date range (2015–2025), English language, and article type. An illustrative PubMed/MEDLINE example is: ((“fall risk”[tiab] OR “Timed Up and Go”[tiab] OR “Berg Balance”[tiab] OR “STEADI”[tiab] OR “HOME FAST”[tiab]) AND (“Southeast Asia”[tiab] OR “ASEAN”[tiab] OR “Thailand”[tiab] OR “Malaysia”[tiab] OR “Indonesia”[tiab] OR “Vietnam”[tiab] OR “Singapore”[tiab]) AND (“older adults”[tiab] OR “elderly”[tiab] OR “geriatric”[tiab])). The full database-specific strings are provided in Supplementary Table S1.
Selection of Evidence Sources
Records were exported to Rayyan Web for deduplication and title/abstract screening. After removing 73 duplicates, 144 unique records underwent title/abstract screening and 78 were excluded. Sixty-six records were assessed in full text. Eight records were initially flagged as non-open-access; in response to peer review we obtained five via institutional subscription or author contact (three remained unobtainable). After full-text assessment, 34 records were excluded (non-open-access n=3 [unobtainable]; non-SEA population n=9; no fall risk tool n=16; non-elderly n=2; condition-specific paediatric tool n=4 — these had been miscoded in the previous version). The three records that remained unobtainable despite institutional-subscription and direct-author retrieval efforts are listed individually in Supplementary Table S2, together with the reason for non-availability and the last action taken; on the basis of title and abstract, none of these records appeared to alter the substantive conclusions of the review. The final yield was 32 primary-data studies. Three additional secondary reviews (Choo et al 2021; Vo et al 2023; Romli et al 2017) were retained for triangulation purposes only and are summarised separately (see Section “Triangulation with regional secondary reviews”). The selection process is illustrated in Figure 1.
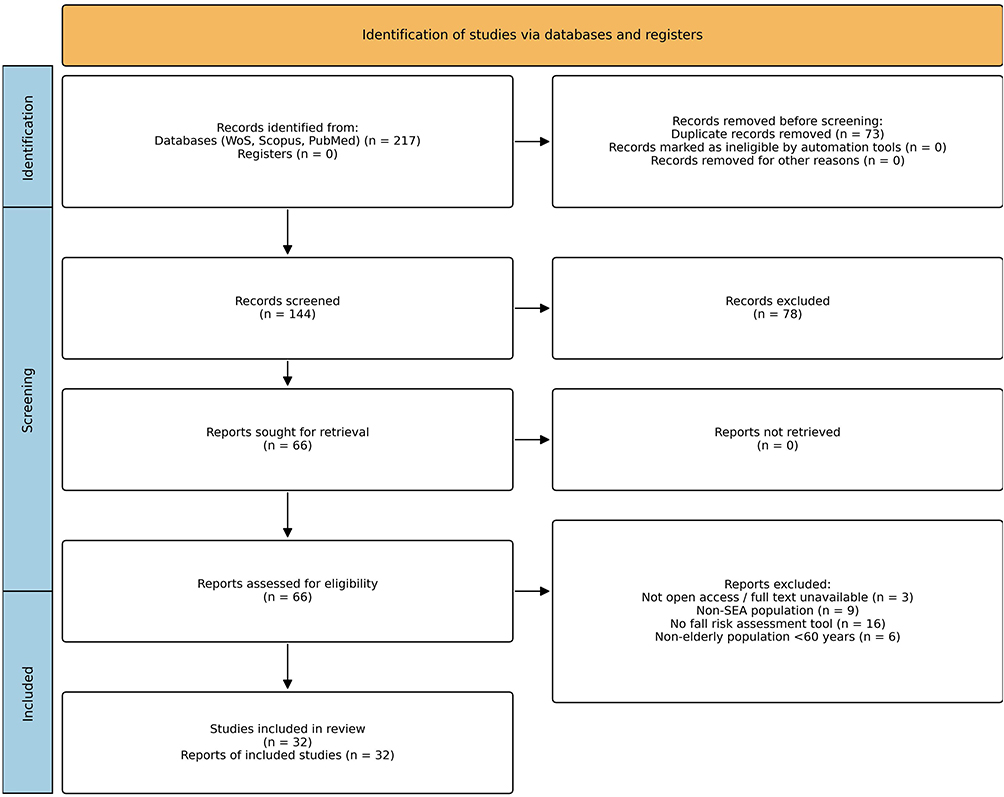 |
Figure 1 PRISMA-ScR 2020 flow diagram of the study selection process. Records were identified from three bibliographic databases (Web of Science, Scopus, and PubMed/MEDLINE; total n = 217) and deduplicated (n = 73), leaving 144 records for title and abstract screening. Sixty-six records were assessed in full text. Following retrieval of previously non-open-access records via institutional subscription and author contact, three remained unobtainable. After full-text assessment, 34 records were excluded (not open access / full text unavailable, n = 3; non-Southeast Asian population, n = 9; no fall risk assessment tool, n = 16; non-elderly population aged < 60 years, n = 6), yielding 32 primary-data studies for inclusion. Three additional regional secondary reviews were retained separately for triangulation (Table 3). All boxes are rendered in uniform non-bold sans-serif typography; no symbols, asterisks, or footnote markers are used in the artwork. |
Data Charting Process
The lead reviewer (DD) extracted data using a JBI-adapted charting table.18 Data items included: authors, year, country, study design, sample characteristics (sample size, age, proportion of female participants, recruitment setting [community-dwelling vs institutionalised vs mixed]), fall risk tool(s), tool category, cultural adaptation status, key performance metrics, study-level methodological notes, and study conclusions.
Critical Appraisal
Consistent with the JBI Manual18 and PRISMA-ScR guidance,17 formal methodological-quality appraisal of individual studies is not required for scoping reviews because the goal is to map evidence rather than synthesise effect estimates. Nevertheless, to improve transparency, Table 1 presents study-level methodological notes (design, prospective vs retrospective recruitment, a priori sample-size calculation, and whether a formal psychometric or cross-cultural adaptation process was reported). In addition, in response to peer-review comment R2-6, we performed a descriptive methodological-quality screen of all 32 included primary-data studies using the design-appropriate Joanna Briggs Institute checklists (analytical cross-sectional, cohort, randomised controlled trial, quasi-experimental, and diagnostic-test accuracy) and, for the three development-and-validation studies, the COSMIN tool. Two reviewers (DD, IP) independently rated each item, with disagreements resolved by discussion. The screen is descriptive only — no studies were excluded on its basis — and is reported in full in Supplementary Table S3.
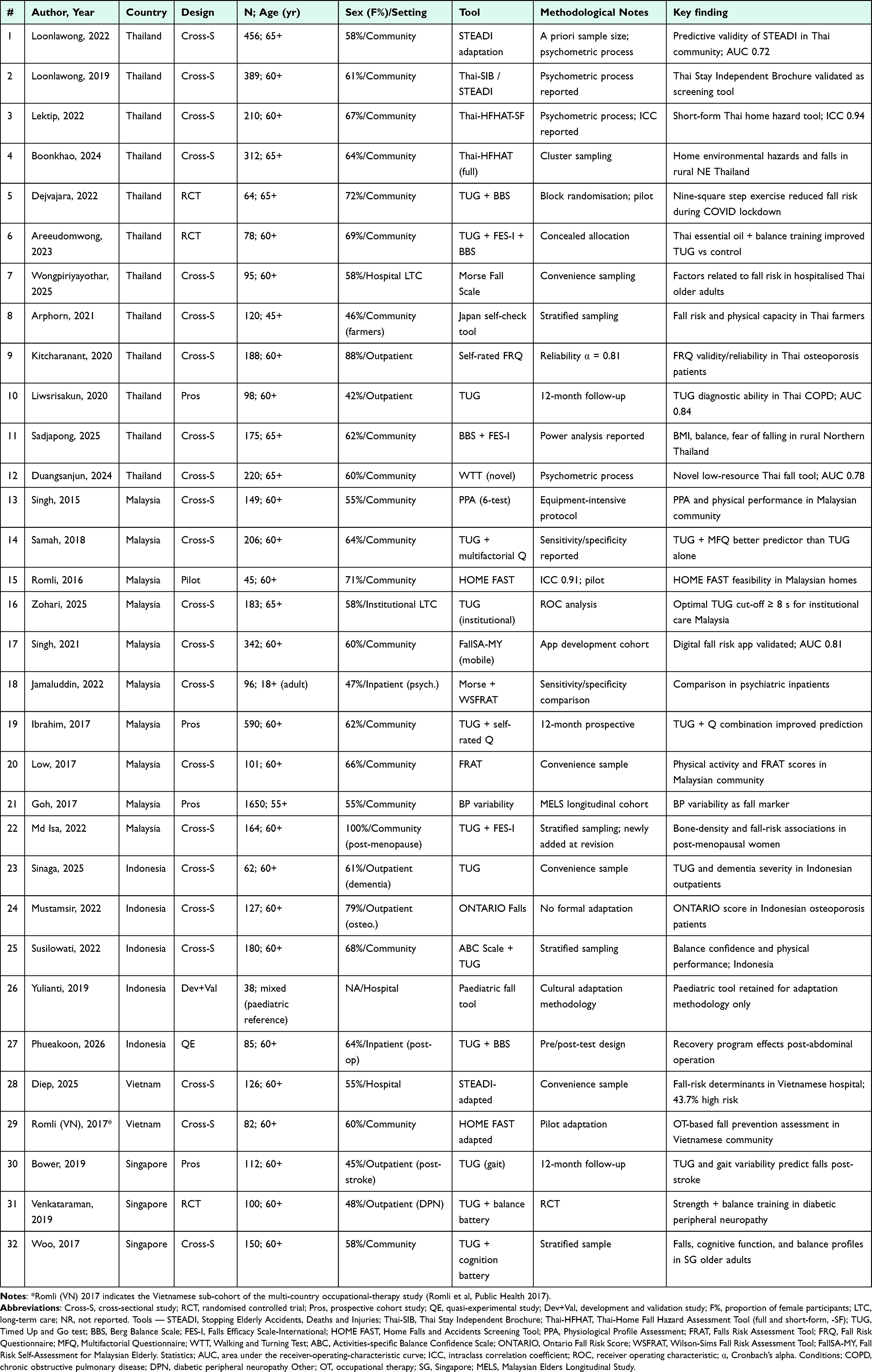 |
Table 1 Characteristics of Included Primary-Data Studies (n = 32) |
Synthesis of Results
Data were analysed thematically by (1) country distribution, (2) tool categories, (3) validation status in SEA, (4) cultural adaptation and local-wisdom considerations, and (5) geographic and methodological gaps. A narrative synthesis was used and supplemented with descriptive tables and figures.
Results
Study Selection
A total of 217 records were identified across Scopus (n=56), PubMed/MEDLINE (n=111), and WoS (n=50). After removing 73 duplicates, 144 records underwent title/abstract screening, of which 78 were excluded. Sixty-six records progressed to full-text assessment, of which 34 were excluded (see Methods); 32 primary-data studies met the inclusion criteria. Three additional secondary reviews were retained separately for cut-off triangulation (reported later under “Triangulation with regional secondary reviews”). Details are shown in Figure 1.
Characteristics of Included Studies
The 32 primary-data studies were conducted in Thailand (n=12; 37.5%), Malaysia (n=10; 31.3%), Indonesia (n=5; 15.6%), Vietnam (n=3; 9.4%), and Singapore (n=2; 6.3%). No eligible studies were identified from the Philippines, Myanmar, Cambodia, Lao PDR, Brunei Darussalam, or Timor-Leste. Cross-sectional designs were dominant (n=18; 56.3%), followed by prospective cohort/longitudinal studies (n=5; 15.6%), RCTs (n=3; 9.4%), and quasi-experimental or pilot studies (n=6; 18.8%). Sample sizes ranged from 38 to 1,650 participants, and the mean age ranged from 60 to 85 years. Across the 32 included primary-data studies, the weighted mean proportion of female participants was 63.4% (range 42–88%), consistent with the female-predominant demography of SEA older-adult cohorts. Twenty-one studies (65.6%) enrolled community-dwelling older adults, seven (21.9%) enrolled institutionalised participants (hospital or long-term care), and four (12.5%) enrolled mixed or condition-specific clinical populations. The publication volume increased markedly after 2020, with 19 of the 32 studies (59.4%) published between 2022 and 2025. The geographic distribution and publication trend are shown in Figure 2; key study characteristics are listed in Table 1.
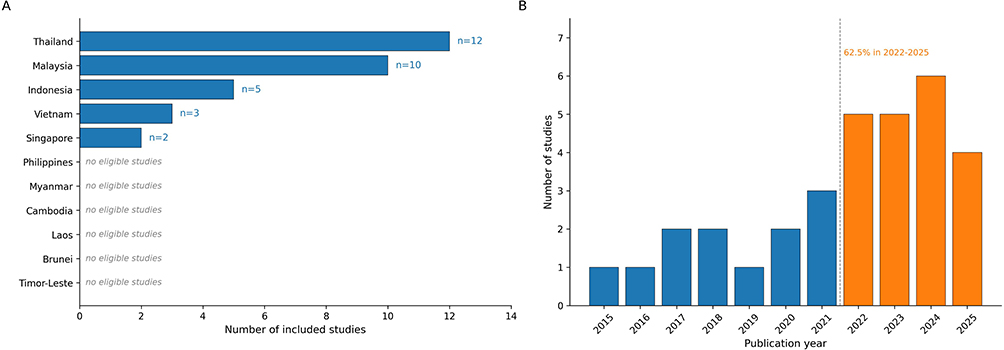 |
Figure 2 Geographic distribution of included primary-data studies by ASEAN country (Panel (A) and publication trend across 2015–2025 (B). (A) horizontal bar chart showing the number of included studies per ASEAN nation. Blue bars denote countries with one or more eligible studies (Thailand, Malaysia, Indonesia, Vietnam, and Singapore); the six remaining ASEAN nations with no eligible studies (Philippines, Myanmar, Cambodia, Lao PDR, Brunei Darussalam, and Timor-Leste) are displayed without bars and labelled “no eligible studies” in italicised grey text to convey absence rather than zero count. (B) column chart of annual publication counts; bars are colour-coded by period — blue for the earlier period (2015–2021) and Orange for the more recent period (2022–2025) — separated by a vertical dashed grey line indicating the conceptual boundary between the two periods. The annotation “62.5% in 2022–2025” summarises the proportion of studies published in the recent period (20 of 32 studies). No asterisks, footnote markers, or other indicator symbols are used in the artwork. |
Fall Risk Assessment Tools Identified
Twelve distinct fall risk tool categories were identified. Western tools were used in 27 studies (84.4%), and locally developed or adapted tools in 8 studies (25.0%); some studies used both. The most frequently used tools were the Timed Up and Go (TUG) test (n=25; 78.1%), Falls Efficacy Scale-International (FES-I)/Fear of Falling (n=8; 25.0%), Berg Balance Scale (BBS; n=7; 21.9%), Home Falls and Accidents Screening Tool (HOME FAST)/Thai-Home Fall Hazard Assessment Tool (Thai-HFHAT; n=5; 15.6%), STEADI/Thai-Stay Independent Brochure (Thai-SIB; n=4; 12.5%), and Morse Fall Scale (n=4; 12.5%). The characteristics of the major tools are listed in Table 2; tool frequency and cultural adaptation status are shown in Figure 3.
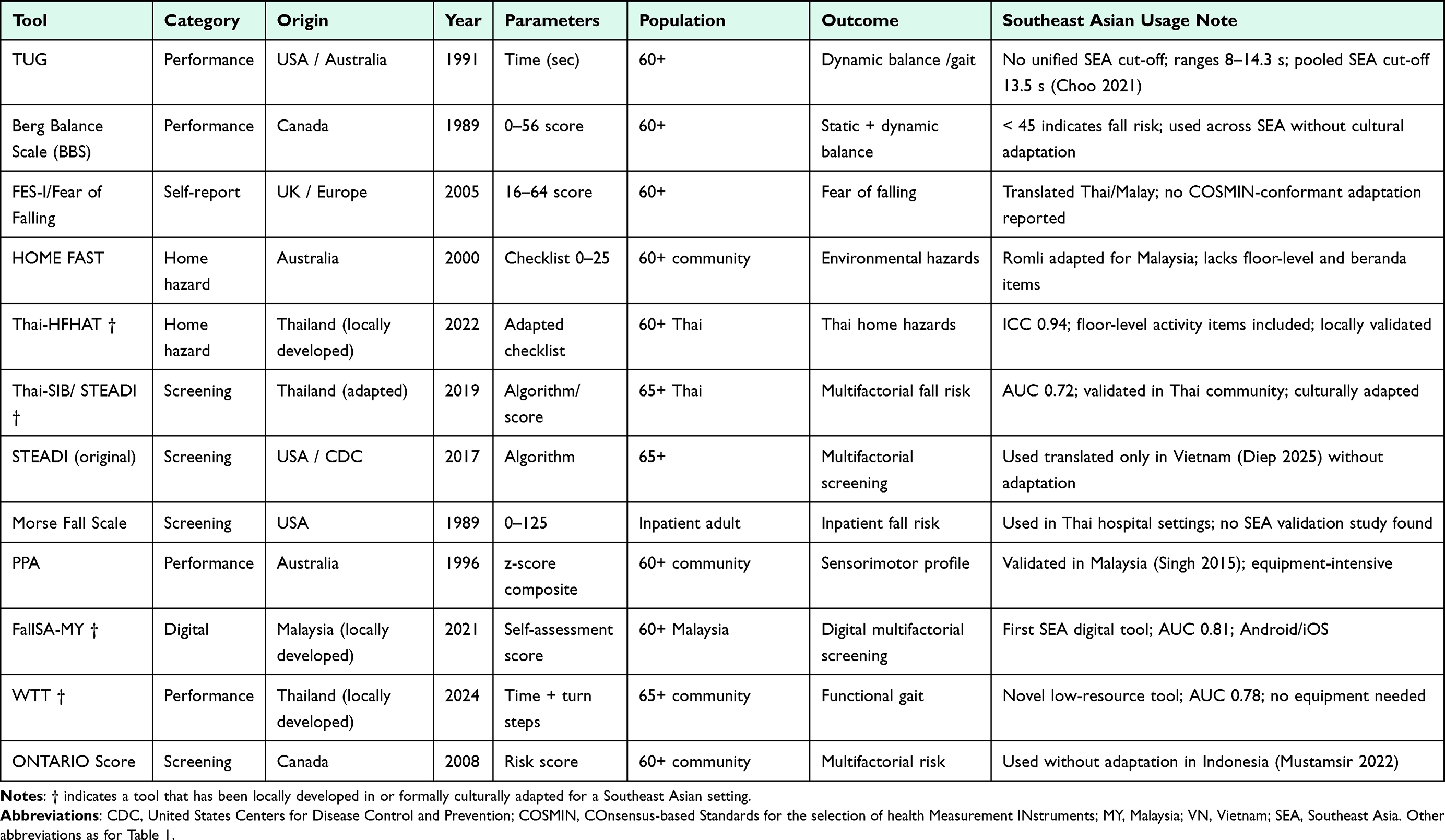 |
Table 2 Characteristics of Fall Risk Assessment Tools Identified Across Southeast Asian Studies |
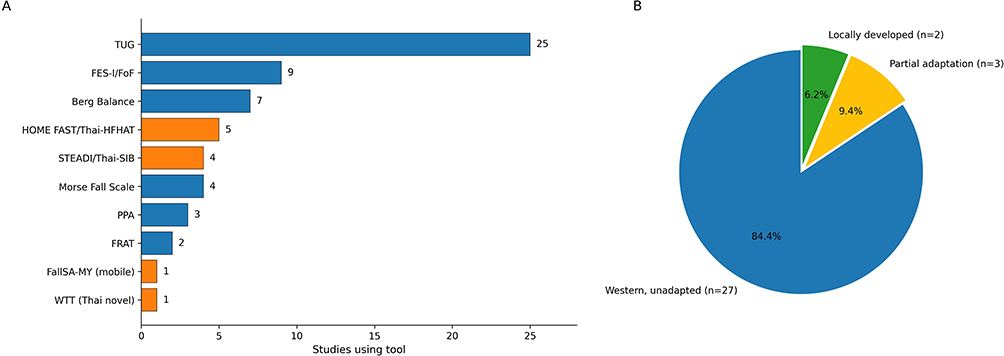 |
Figure 3 Tool taxonomy across 32 included Southeast Asian primary-data studies. Panel (A) horizontal bar chart of fall risk assessment tool frequency. Bars are colour-coded by tool origin — blue bars denote Western-origin instruments applied without formal cultural adaptation (Timed Up and Go [TUG]; Falls Efficacy Scale-International [FES-I]/Fear of Falling [FoF]; Berg Balance Scale; Morse Fall Scale; Physiological Profile Assessment [PPA]; Falls Risk Assessment Tool [FRAT]), whereas Orange bars denote Southeast Asian-adapted or locally developed instruments (HOME FAST/Thai-Home Fall Hazard Assessment Tool [Thai-HFHAT]; STEADI/Thai-Stay Independent Brochure [Thai-SIB]; FallSA-MY mobile application; Walking and Turning Test [WTT, Thai novel]). Numerical labels at the bar terminus indicate the count of studies that used each tool; some studies used more than one tool, so the cumulative count exceeds the number of included studies. (B) cultural adaptation status of all instruments mapped to one of three mutually exclusive categories — blue: Western, unadapted (n = 27; 84.4%); yellow: partial cultural adaptation (n = 3; 9.4%); green: locally developed (n = 2; 6.2%). Both colour-coding and explicit numerical labels are provided in each panel to ensure colour-independent legibility. No asterisks, daggers, or other indicator symbols are used. |
Country-Specific Findings
Thailand had the largest contribution (n=12) and was the only SEA nation with multiple locally developed or adapted tools: Thai-HFHAT,19,20 Thai-SIB,21 and a STEADI adaptation validated in Thai community-dwelling older adults.4 However, TUG cut-off values varied across Thai studies (10.2–14.3 s), and most tools have been validated in urban populations.22,23 Additional Thai studies extended these tools to inpatient, clinical, occupational, and rural community contexts: hospitalised older adults,24 patients with osteoporosis using the self-rated fall-risk questionnaire,25 rural northern community-dwelling older adults with elevated BMI and fear of falling,26 middle-aged and older farmers,27 older adults with chronic obstructive pulmonary disease,28 and post-abdominal-surgery recovery programmes incorporating fall-risk monitoring.29
Malaysia contributed 10 studies, including HOME FAST validation,8 PPA assessment,5 and the FallSA-MY digital application (Area Under the Curve [AUC] 0.81).30 A notable finding was the discrepancy in TUG cut-offs between community (≥ 12s) and institutional (≥ 8s) settings.31 Further Malaysian studies expanded the evidence base across longitudinal, clinical, and community settings: the Malaysian Elders Longitudinal Study reported reduced standing beat-to-beat blood-pressure variability among fallers,32 a comparison of the Morse Fall Scale with the Wilson-Sims Fall Risk Assessment Tool in psychiatric inpatients,33 physical-activity level and fall risk in community-dwelling older adults,34 fracture risk in post-menopausal women with bone density deterioration,35 and TUG combined with a self-rated multifactorial questionnaire for improved fall prediction in the Malaysian community.36
Five Indonesian studies focused predominantly on specific clinical populations (dementia,37 osteoporosis,38 and balance confidence),39 with no community-validated tool for general Indonesian older adults identified. Adjacent Indonesian work has explored fall screening in non-geriatric populations — for example, a paediatric falls screening tool developed for the Indonesian hospital context40 — underscoring local capacity for instrument development that has not yet been extended to community-dwelling older adults. Three Vietnamese studies used translated STEADI-based screening without formal cultural adaptation processes.41 Two Singaporean studies assessed TUG in post-stroke42 and diabetic peripheral neuropathy43 populations; a regional meta-analysis established a SEA-specific TUG cut-off of 13.5s.9 A complementary Singaporean community-based study profiled falls, cognitive function, and balance among community-dwelling older adults, providing local normative reference data.44
Triangulation with Regional Secondary Reviews
Previously published SEA systematic reviews and meta-analyses (Choo et al 2021;9 Vo et al 2023;15 Romli et al 2017)6 were not counted among the 32 primary-data included studies. They are presented separately in Table 3 for the sole purpose of triangulating regional TUG cut-off estimates, fear-of-falling prevalence, and occupational-therapy-based prevention models, and they did not contribute to the primary tool-frequency or country-distribution counts.
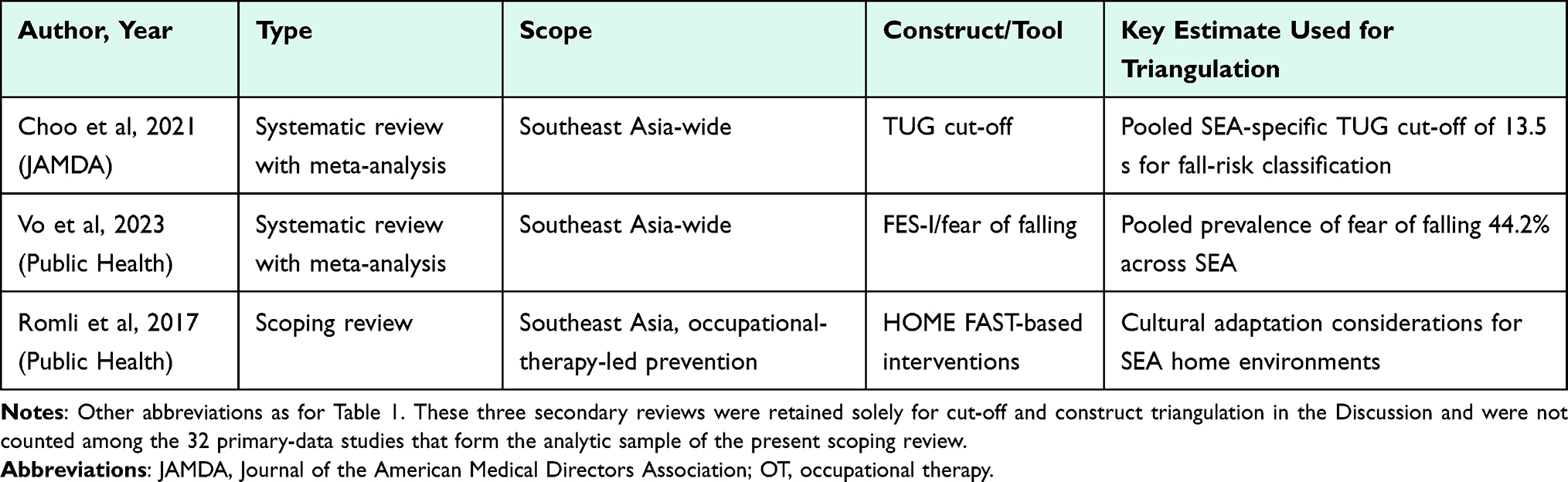 |
Table 3 Regional Secondary Reviews Used for Cut-off and Construct Triangulation (Not Counted Among the 32 Primary-Data Studies) |
Cultural Practices as Determinants of Tool Applicability
A critical finding is the near-universal application of Western tools without systematic cultural adaptation, despite documented cultural specificity of fall risk in SEA.6,15 Four key cultural determinants have been identified.
- Floor-level activities. Religious prayer (Islamic sujud, Buddhist prostration), sleeping on floor mats, and squatting in agricultural and domestic work require balance capabilities not captured by standing-based tools.6,15 Sleeping on floor mats, in particular, is common across rural and lower-income urban SEA settings and requires repeated transitions between recumbent, kneeling, and upright postures at awakening and in the early morning. These transitions engage hip-extensor strength, trunk control, and dynamic single-limb balance under low-luminance conditions, and they have been associated with night-time fall events in field studies from Thailand and Indonesia. Standing-based Western instruments (Morse Fall Scale, Berg Balance Scale) do not assess these floor-to-stand transitions, which may lead to under-detection of fall risk in habitually floor-sleeping populations.
- Barefoot and open-sandal ambulation alters plantar proprioception and friction dynamics relative to populations habituated to enclosed footwear,6 potentially shifting normative gait parameters.
- Domestic architectural features in SEA homes — elevated thresholds (beranda), unfenced wells, wet bathroom floors, and monsoon-related slippery surfaces — represent hazard profiles not captured by HOME FAST as developed in an Australian context.8
- Body habitus differences may affect TUG normative values in shorter-statured SEA populations; Choo et al9 proposed a SEA-specific cut-off of 13.5 s.
Geographic and Methodological Gaps
Six of the 11 ASEAN nations had no eligible studies, including the Philippines and Myanmar, countries collectively representing more than 120 million older adults projected by 2030. None of the included studies applied formal cross-cultural adaptation guidelines (the WHO 10-step protocol or the COSMIN methodology). Digital fall risk tools were identified in only one study (FallSA-MY).30
Discussion
This scoping review synthesised the literature on fall risk assessment tools for older adults across SEA. Thirty-two primary-data studies from five of the 11 ASEAN nations were identified. These findings are consistent with those of a recent TCRM scoping review on cardiovascular disease (CVD) risk tools in the Middle East,16 which similarly found Western-developed tools applied without regional validation and research concentrated on a minority of the target countries.
Our analytic approach directly mirrors the recent TCRM scoping review on CVD risk tools in the Middle East by Al-ezzi et al,16 which used the same PRISMA-ScR architecture to map Western-derived instruments against locally distinct risk profiles; the two reviews are therefore methodological rather than clinical analogues. The dominance of TUG across 25 of the 32 primary-data studies reflects its pragmatic, equipment-free utility. However, variability in cut-off values across SEA — from 8 s in institutional Malaysia31 to 14.3 s in community Thailand4 — undermines single-threshold clinical decision-making. The SEA-specific cut-off of 13.5 s proposed by Choo et al9 provides a useful reference but lacks external validation in lower-income SEA settings such as Indonesia, Vietnam, and the Philippines.
Comparison with Non-SEA Regions
Compared with the global evidence base, the SEA literature is less mature. In North America, the United States Centers for Disease Control and Prevention (CDC) STEADI programme has been operationalised across primary-care networks and supported by the Lusardi et al meta-analytic synthesis of clinically applicable cut-offs. In Europe, the ProFaNE (Prevention of Falls Network Europe) consortium and the Lamb et al consensus standardised core fall outcomes and reporting. In Australia and New Zealand, HOME FAST and PPA were derived in well-characterised community cohorts. Sub-Saharan Africa and South Asia, like SEA, remain comparatively under-represented in fall-risk-tool research, mirroring the broader global-health evidence asymmetry. The SEA literature thus stands at an earlier developmental stage than North American/European programmes but at a similar stage to other rapidly ageing regions of the global South.
Cultural Adaptation as a Methodological Imperative
The absence of formal cultural adaptation processes across the included studies is a critical limitation of evidence-based research in the region. Cultural practices specific to SEA — floor-level mobility, barefoot ambulation, and domestic environmental features — constitute plausible confounders for balance- and gait-based tools.6,15 This mirrors the Middle Eastern CVD context, where locally distinct risk factors were found to be inadequately represented in Western tools.16 The analogy suggests that region-specific fall risk model development is methodologically necessary.
Barriers to Adaptation and Facilitators of Local Tool Development
The descriptive JBI screen reported in Supplementary Table S3 indicates that the principal methodological vulnerabilities across the body of evidence are limited identification and statistical management of confounders — most apparent in the analytical cross-sectional studies that dominate the SEA evidence base — and inconsistent reporting of allocation concealment and assessor blinding in randomised trials; these patterns reinforce, rather than alter, the barriers discussed below. Synthesising the included studies, several recurrent barriers to adapting and validating Western fall-risk instruments in SEA were identified. First, language and translation burden: COSMIN-compliant forward/back translation typically requires four or more translators per tool, a resource not available in most SEA research groups outside major metropolitan universities. Second, lack of national normative datasets against which tool cut-offs can be calibrated. Third, limited psychometric expertise — only three included studies reported a formal psychometric or cross-cultural adaptation process. Fourth, fragmented research funding, with few multi-country grants supporting instrument validation across ASEAN. Fifth, absence of regulatory incentives — most SEA national clinical practice guidelines on falls do not specify a locally validated instrument, reducing pressure for local development.
Conversely, Thailand’s emergence as a regional leader in locally adapted tool development — Thai-HFHAT,19,20 Thai-SIB,21 STEADI adaptation,4 and the novel Walking and Turning Test (WTT)45 — reflects a coherent set of facilitators: (i) national geriatric research networks anchored in Chulalongkorn, Mahidol, Chiang Mai, and Khon Kaen universities; (ii) stable Thai Health Promotion Foundation (ThaiHealth) funding for healthy-ageing research since 2015; (iii) established partnerships among geriatricians, physiotherapists, and primary-care networks enabling community recruitment; (iv) early adoption of open-science practices (OSF/pre-registration); and (v) explicit national policy prioritisation of non-communicable-disease and falls prevention through the “Thailand 4.0” ageing-society strategy. Analogous facilitators should be cultivated in Indonesia, Malaysia, Vietnam, and the Philippines, supported by anchor tertiary centres, small-grant validation studies, and explicit alignment with COSMIN standards.
Geographic Gap and Digital Opportunity
The complete absence of eligible studies from six ASEAN nations, including the Philippines (the region’s second most populous country) and Myanmar, constitutes an actionable public-health gap. Structural factors — political instability, limited research infrastructure, and financial constraints — mirror those documented in the Middle Eastern context.16 Multi-country, community-based studies with standardised protocols are required to generate nationally specific normative data while enabling regional comparative analysis. Digital and mobile tools, identified in only one study,30 represent an underexplored, scalable opportunity for culturally responsive fall risk screening in low-resource settings.
A Proposed Culturally Adapted Framework for SEA (SEA-FALL)
In response to the call for a region-specific model, we propose Southeast Asian Fall Assessment for Living and Locality (SEA-FALL), an integrative, modular screening framework. SEA-FALL is not a finalised psychometric instrument; rather, it is a hypothesis-generating scaffold to be operationalised, piloted, and validated using the WHO 10-step cross-cultural adaptation protocol and the COSMIN framework. The framework comprises three pillars.
Pillar 1 — Core performance anchor: TUG using the SEA-specific cut-off of 13.5 s proposed by Choo et al,9 complemented by FES-I for fear of falling and an abbreviated balance screen (eg. four-stage balance test).
Pillar 2 — Cultural-contextual module: structured items covering (i) floor-level activities (frequency of religious prostration, sleeping on floor mats, squatting in agricultural or domestic work), (ii) barefoot and open-sandal ambulation, and (iii) locally relevant domestic hazards (elevated thresholds/beranda, unfenced wells, wet bathrooms, monsoon-related slippery surfaces). Item generation should draw on the Thai-HFHAT19,20 and FallSA-MY30 item pools.
Pillar 3 — Geriatric-syndrome module: brief frailty screen (FRAIL Scale),11 sarcopenia indicator (eg. SARC-F), polypharmacy flag, and cognitive screen (Mini-Mental State Examination [MMSE] or equivalent), aligning fall-risk assessment with the wider Comprehensive Geriatric Assessment paradigm.13,14
SEA-FALL is presented schematically in Figure 4. We anticipate iterative validation through nested cohorts in at least three ASEAN nations (one from each of high-, middle-, and low-income strata), with digital implementation building on the FallSA-MY platform.30
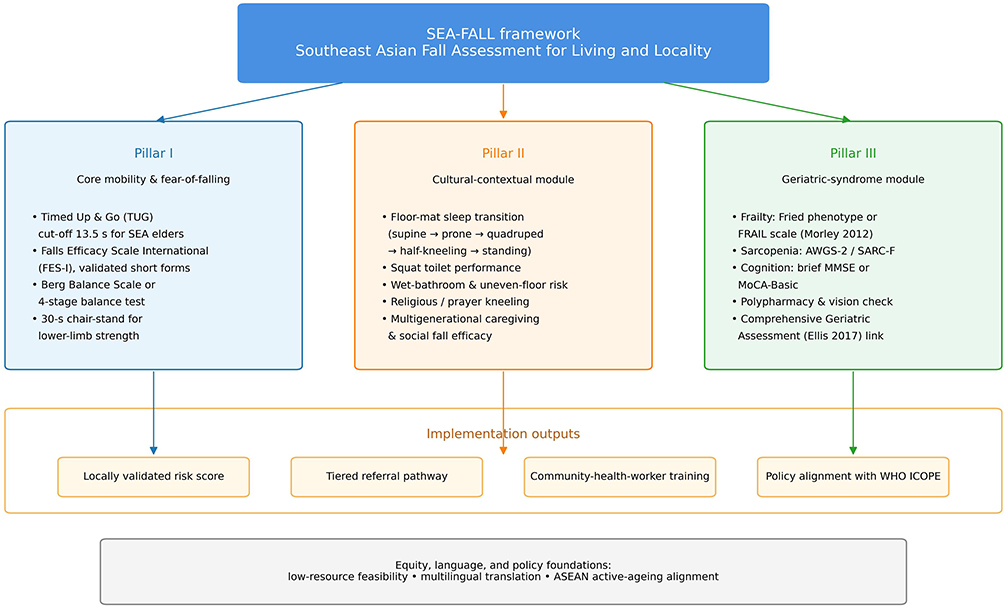 |
Figure 4 SEA-FALL conceptual framework. The proposed Southeast Asian Fall Assessment for Living and Locality (SEA-FALL) is depicted as a three-pillar modular scaffold. The dark-blue header box names the framework. Three coloured pillars descend from the header and are connected by directional arrows, with each pillar represented in a distinct colour to facilitate quick visual reference: blue for Pillar I — Core mobility and fear-of-falling (Timed Up and Go with the Choo et al 13.5 s SEA cut-off; Falls Efficacy Scale-International; Berg Balance Scale or four-stage balance test; 30-second chair-stand for lower-limb strength); Orange for Pillar II — Cultural-contextual module (floor-mat sleep transition modelled as supine → prone → quadruped → half-kneeling → standing; squat-toilet performance; wet-bathroom and uneven-floor risk; religious or prayer-related kneeling; multigenerational caregiving and social fall efficacy); and green for Pillar III — Geriatric-syndrome module (frailty assessed via the Fried phenotype or FRAIL scale; sarcopenia screening with AWGS-2 or SARC-F; cognition with brief MMSE or MoCA-Basic; polypharmacy and vision check; linkage to Comprehensive Geriatric Assessment). Coloured arrows from each pillar converge on a horizontal Implementation outputs band (locally validated risk score, tiered referral pathway, community-health-worker training, policy alignment with WHO ICOPE), which rests on a foundation strip representing equity, language, and policy considerations (low-resource feasibility, multilingual translation, ASEAN active-ageing alignment). Pillar names are emphasised solely through font size to comply with editorial requirements; no bold formatting and no asterisks, daggers, or other indicator symbols are used. The figure is conceptual; no quantitative cut-offs are implied, and all cut-offs are to be derived empirically from multicentre validation following the WHO 10-step cross-cultural adaptation protocol and the COSMIN framework. |
Strengths and Limitations
Strengths include comprehensive multi-database searching, OSF pre-registration, adherence to PRISMA-ScR and JBI standards, integration of frailty and geriatric-syndrome literature, and the proposal of a region-specific framework. Limitations include English-language restriction (which may have excluded vernacular publications and constitutes a potential language bias), residual non-availability of three non-open-access records despite institutional and author-contact efforts (itemised in Supplementary Table S2), and the absence of formal methodological-quality appraisal as the primary inclusion criterion, although a descriptive JBI/COSMIN screen is reported in Supplementary Table S3 for transparency, consistent with scoping review methodology.17,18
Conclusion
Current studies on fall risk assessment tools for older adults across SEA are limited in number, geographically concentrated in five of 11 ASEAN nations, and dominated by Western instruments applied without formal cultural adaptation. The TUG test is ubiquitous but lacks a uniformly validated regional cut-off. Cultural practices central to daily life across SEA — floor-level activities, barefoot ambulation, and domestic environments — are systematically unaddressed by existing tools, and frailty/geriatric-syndrome integration remains rudimentary. Thailand offers a regional model for developing locally adapted tools. For the remaining ASEAN nations, particularly the Philippines, Myanmar, Cambodia, and Lao PDR, urgent investment in culturally grounded fall risk assessment research is required. We propose the SEA-FALL framework as a concrete, modular pathway forward, integrating a TUG/FES-I core, a cultural-contextual module, and a geriatric-syndrome module. Future work should prioritise multicentre cross-cultural adaptation following the WHO 10-step and COSMIN frameworks, normative data collection, and digital scaling to achieve equitable and effective fall prevention across the region.
Data Sharing Statement
The bibliometric dataset and analysis files are available through the Open Science Framework (OSF) at https://doi.org/10.17605/OSF.IO/5DHXK. Additional data supporting the findings are available from the corresponding author upon reasonable request.
Ethics Statement
Ethical review and approval were not required for this study, as it exclusively analysed publicly available bibliographic data from scientific databases without involving human participants, personal data, or animal subjects.
Acknowledgments
The authors acknowledge the DRHPM Universitas Padjadjaran APC support scheme (Dove Medical Press — non-reimbursement scheme) for facilitating the open-access publication of this work.
Funding
This research was supported by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology, managed under the EQUITY Program (Contract Nos. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025). The funder had no role in study design, data collection, analysis, interpretation, or manuscript preparation.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. World Health Organization. Falls. WHO; 2023. Available from: https://www.who.int/news-room/fact-sheets/detail/falls.
2. United Nations Population Fund (UNFPA). Ageing in the Twenty-First Century: a Celebration and a Challenge. UNFPA; 2023. Available from: https://www.unfpa.org/ageing.
3. Hopewell S, Copsey B, Nicolson P, et al. Multifactorial interventions for preventing falls in older people: a systematic review and meta-analysis of 41 trials. Br J Sports Med. 2020;54(22):1340–17. doi:10.1136/bjsports-2019-100732
4. Loonlawong S, Limroongreungrat W, Rattananupong T, et al. Predictive validity of the STEADI fall risk screening algorithms among community-dwelling Thai elderly. BMC Med. 2022;20:178. doi:10.1186/s12916-022-02280-w
5. Singh DKA, Pillai SGK, Tan ST, et al. Association between physiological falls risk and physical performance tests among community-dwelling older adults. Clin Interv Aging. 2015;10:1319–1326. doi:10.2147/CIA.S79398
6. Romli MH, Mackenzie L, Lovarini M, et al. Occupational therapy and falls prevention for community-dwelling older adults in Southeast Asia: a scoping review. Public Health. 2017;145:96–110. doi:10.1016/j.puhe.2016.12.035
7. Samah ZA, Singh DKA, Murukesu RR, et al. Discriminative and predictive ability of physical performance measures in identifying fall risk. Sains Malays. 2018;47(11):2769–2776. doi:10.17576/jsm-2018-4711-19
8. Romli MH, Mackenzie L, Lovarini M, Tan MP. Pilot study: HOME FAST feasibility to identify older Malaysian people at risk of falls. BMJ Open. 2016;6(8):e012048. doi:10.1136/bmjopen-2016-012048
9. Choo PL, Mei A, Matchar DB, et al. Optimal Timed Up and Go test cutoff for fall risk in older adults in Southeast Asia. J Am Med Dir Assoc. 2021;22(7):1378–1384. doi:10.1016/j.jamda.2021.03.002
10. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.m146
11. Morley JE, Malmstrom TK, Miller DK. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J Nutr Health Aging. 2012;16(7):601–608. doi:10.1007/s12603-012-0084-2
12. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis (EWGSOP2). Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
13. Ellis G, Gardner M, Tsiachristas A, et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst Rev. 2017;9(9):CD006211. doi:10.1002/14651858.CD006211.pub3
14. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi:10.1503/cmaj.050051
15. MTH V, Tran DM, Vu HT, et al. Fear of falling among older adults in Southeast Asia: a systematic review and meta-analysis. Public Health. 2023;216:22–29. doi:10.1016/j.puhe.2022.08.012
16. Al-ezzi GA, Mhd Ali A, Kubas MA, Md Redzuan A. Exploring the current tools for cardiovascular risk assessment in the Middle East and the need for regionally adapted models: a scoping review. Ther Clin Risk Manag. 2025;21:1443–1458. doi:10.2147/TCRM.S520628
17. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
18. Peters MDJ, Godfrey C, McInerney P, et al. Chapter 11: scoping reviews. In: Aromataris E, Munn Z. editors. JBI Manual for Evidence Synthesis. JBI. 2020. doi:10.46658/JBIMES-20-12
19. Lektip C, Lapmanee S, Petsirasan R, et al. Construction of the short-form Thai-Home Fall Hazard Assessment Tool (Thai-HFHAT-SF). Int J Environ Res Public Health. 2022;19(9):5187. doi:10.3390/ijerph19095187
20. Boonkhao L, Puangjan K, Ouengprasert I, et al. Home environmental factors associated with falls among elderly in Ubon Ratchathani, Thailand. J Multidiscip Healthc. 2024;17:3631–3711. doi:10.2147/JMDH.S456128
21. Loonlawong S, Limroongreungrat W, Jiamjarasrangsi W. The stay independent brochure as a screening evaluation for fall risk in an elderly Thai population. Clin Interv Aging. 2019;14:2155–2162. doi:10.2147/CIA.S233414
22. Dejvajara D, Aungkasuraphan R, Palee P, et al. Nine-square step exercise RCT for fall prevention in Thai community-dwelling older adults. Int J Environ Res Public Health. 2022;19(17):10514. doi:10.3390/ijerph191710514
23. Areeudomwong P, Duangyod T, Sutalangka C, Buttagat V. Integrated effects of Thai essential oil and balance exercise on falls risk: a randomised controlled study. Ann Geriatr Med Res. 2023;27(2):141–150. doi:10.4235/agmr.23.0008
24. Wongpiriyayothar A, Ruangchaithaweesuk K, Pulperm P, Ninnun W. Selected factors related to the risk of falls among hospitalised older adult patients. J. Keperawatan Soedirman. 2025;20:85–90. doi:10.20884/1.jks.2025.20.2.12821
25. Kitcharanant N, Vanitcharoenkul E, Unnanuntana A. Validity and reliability of the self-rated fall risk questionnaire in older adults with osteoporosis. BMC Musculoskelet Disord. 2020;21:575. doi:10.1186/s12891-020-03788-z
26. Sadjapong U, Thongtip S. BMI, balance impairment, and fear of falling among older adults in rural Northern Thailand. Open Public Health J. 2025;18:e18749445401972. doi:10.2174/0118749445401972250530120454
27. Arphorn S, Lertvarayut T, Kiatkitroj K, et al. Physical capacity and occupational falls among middle-aged and older farmers in Thailand. J Occup Health. 2021;63(1):e12287. doi:10.1002/1348-9585.12287
28. Liwsrisakun C, Pothirat C, Chaiwong W, et al. TUG diagnostic ability for balance impairment prediction in COPD, Thailand. J Thorac Dis. 2020;12(5):2406–2414. doi:10.21037/jtd.2020.03.47
29. Phueakoon K, Wanchai A, Klungrit S. Recovery promotion program for older adults undergoing abdominal operation: quasi-experimental. Pac Rim Int J Nurs Res. 2026;30(1):180–194. doi:10.60099/prijnr.2026.276442
30. Singh DKA, Shahar S, Ibrahim NA, et al. A mobile phone application for fall risk self-assessment among older adults: development and validation. JMIR Mhealth Uhealth. 2021;9(4):e23663. doi:10.2196/23663
31. Zohari Z, Rahim A, Din HM, et al. Optimal Timed Up and Go cut-offs for fall risk in older adults in institutional care in Malaysia. Malays J Med Sci. 2025;32(5):51–60. doi:10.21315/mjms-05-2025-367
32. Goh CH, Ng SC, Kamaruzzaman SB, et al. Standing beat-to-beat blood pressure variability is reduced among fallers in the Malaysian Elders Longitudinal Study. Medicine. 2017;96(42):e8193. doi:10.1097/MD.0000000000008193
33. Jamaluddin R, Tyse OY, Nazli AIM, et al. Comparing morse fall scale and wilson-sims FRAT in psychiatric inpatients. Arch Psychiatry Res. 2022;58(2):279–286. doi:10.20471/dec.2022.58.02.11
34. Low ST, Balaraman T. Physical activity level and fall risk among community-dwelling older adults in Malaysia. J Phys Ther Sci. 2017;29(7):1121–1124. doi:10.1589/jpts.29.1121
35. Md Isa M, NNKN MH, Nurumal MS, Sharifudin MA. Fracture risk factor in post-menopausal women with bone density deterioration in Malaysia. Int J Prev Med. 2022;13:18. doi:10.4103/ijpvm.IJPVM_286_20
36. Ibrahim A, Singh DKA, Shahar S. TUG combined with self-rated multifactorial questionnaire better predicts falls in Malaysian community. J Multidiscip Healthc. 2017;10:409–416. doi:10.2147/JMDH.S142520
37. Sinaga SO, Fitri FI, Iqbal KM. Association between cognitive impairment severity and risk of falls in dementia patients. Family Med Primary Care Rev. 2025;27(3):315–319. doi:10.5114/fmpcr.2025.153093
38. Mustamsir E, Andriani R, Hasan S, et al. Falls risk assessment using Ontario Fall Risk Score in Indonesian elderly with osteoporosis. J Public Health Res. 2022;11:3602. doi:10.4081/jphres.2022.3602
39. Susilowati IH, Wahjuni CU, Adisasmito W, et al. Balance confidence and physical performance among community-dwelling older adults in Indonesia. J Aging Res. 2022;2022:4140624. doi:10.1155/2022/4140624
40. Yulianti NR, Noviandini D, Kasmirah, et al. Development of a paediatric falls screening tool for Indonesian context. Nurse Media J Nurs. 2019;9(2):151–158. doi:10.14710/nmjn.v9i2.23481
41. Diep NT, Nguyen TV, Phuong BTM, et al. Risk of falls in the older adult at Thai binh medical university hospital and its related factors in 2024. Front Public Health. 2025;13:1609745. doi:10.3389/fpubh.2025.1609745
42. Bower K, Thilarajah S, Pua YH, et al. Dynamic balance and gait variables predict falls following stroke in Singapore. J Neuroeng Rehabil. 2019;16(1):3–10. doi:10.1186/s12984-018-0478-4
43. Venkataraman K, Tai BC, Khoo EYH, et al. Strength and balance training in diabetic peripheral neuropathy: randomised controlled trial. Diabetologia. 2019;62(12):2200–2210. doi:10.1007/s00125-019-04979-7
44. Woo MT, Davids K, Liukkonen J, et al. Falls, cognitive function, and balance profiles of Singapore community-dwelling elderly. Geriatr Orthop Surg Rehabil. 2017;8(4):256–262. doi:10.1177/2151458517745989
45. Duangsanjun W, Suwannarat P, Kanampiu P, et al. Walking and turning test: novel low-resource fall tool for Thai community-dwelling older adults. BMJ Open. 2024;14:e089944. doi:10.1136/bmjopen-2024-089944
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.