Back to Journals » International Journal of General Medicine » Volume 14
Exploring the Application of a Multi-Targeted Nursing Group for Enhanced Recovery After Surgery Using the LEER (“Less Pain”, “Early Movement”, “Early Return to a Normal Diet” and “Reassurance”) Model
Authors Xie QY, Yang J, Lei ZH, Gao FW, Chen B, Jiang KY, Xiong H, Yang J
Received 16 July 2021
Accepted for publication 27 September 2021
Published 27 October 2021 Volume 2021:14 Pages 7187—7196
DOI https://doi.org/10.2147/IJGM.S329837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Qing-Yun Xie,1,* Jie Yang,2,* Ze-Hua Lei,1 Feng-Wei Gao,1 Bing Chen,1 Kang-Yi Jiang,1 Hui Xiong,1 Jie Yang1
1Department of Hepatobiliary Pancreatic Splenic Surgery, The People’s Hospital of Leshan, Leshan, Sichuan, 614000, People’s Republic of China; 2Diagnosis and Treatment Center of Hepatobiliary Pancreatic Splenic Systemic Disease in Leshan, The Second Batch of Hepatobiliary and Pancreatic ERAS Standard Wards of Hubei Chen Xiaoping Science and Technology Development Foundation, Leshan, Sichuan, 614000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ze-Hua Lei
Department of Hepatobiliary Pancreatic Splenic Surgery, Leshan People’s Hospital of Sichuan Province, Leshan, Sichuan, 614000, People’s Republic of China
Tel +86 833-2119894
Email [email protected]
Objective: To explore the effects and value of establishing a multi-target nursing group (MTNG) for facilitating goal-oriented enhanced recovery after surgery (ERAS) using the LEER (“less pain”, “early movement”, “early return to a normal diet” and “reassurance”) model.
Methods: The clinical data of 198 patients with hepatobiliary and pancreatic malignancies were retrospectively analyzed. The patients were divided into two groups: 91 cases were collected in a traditional group, which adopted traditional perioperative care, and 107 cases were collected in an MTNG group, which adopted MTNG measures. The differences in the clinical data including postoperative recovery, unplanned readmission rate, the implementation rate of nursing measures, the degree of a patient’s understanding of the disease, and patient compliance and satisfaction with nursing care during hospitalization were compared and analyzed between the two groups.
Results: The MTNG group reflected a lower pain degree and hospitalization expenses (P < 0.05), earlier postoperative flatulence, earlier recommencing of a normal diet, and earlier postoperative ambulation (P < 0.05), together with a shorter postoperative indwelling catheter duration and length of hospital stay (P < 0.05). There were no significant differences in the incidence of postoperative complications and unplanned postoperative readmission rates between the two groups (P > 0.05). The implementation rate of nursing measures and the degree of patients understanding the disease, and patient compliance and satisfaction with nursing care were higher in the MTNG group (P < 0.05).
Conclusion: The MTNG approach, based on ERAS with the LEER model, was conducive to the safe and rapid postoperative recovery of patients, the precise and efficient implementation of ERAS measures, the improvement of medical treatment satisfaction among patients.
Keywords: LEER model, enhanced recovery after surgery, multi-target nursing
Introduction
The enhanced recovery after surgery (ERAS) program is a complete perioperative care implementation process that encompasses a series of multidisciplinary collaborative and multimodal approaches, which are derived from evidence-based guidelines in the areas of surgery, nursing, anesthesia, nutrition, and other research fields.1–,3 Both domestic and international studies have shown that nurses play a critical role in the entire process of preoperative education, perioperative care, and follow-up after discharge.4,5 The nursing staff members form a critical component in overcoming barriers to the implementation of and patient compliance in the ERAS process, and successful implementation of ERAS relies to a large extent on the daily care of patients by nurses throughout consultations.6,7
The present center began the creation of ERAS standardized wards at the start of 2018 and, concurrently, initiated systematic ERAS-related theoretical and practical training for nursing staff. However, during the early stage of the operation of the ERAS ward, ERAS theory was found to be generalized while concurrently including complicated terms and conditions, as well as a lengthy process that required a high learning cost from the single nursing conductor to ensure the standardization of the process. Additionally, it was difficult for the patients to understand the ERAS concept and cooperate with its implementation.8 These issues greatly affected the quality and efficiency of the ERAS program. During the process of continuous exploration and improvement, the present center innovated the LEER (“less pain”, “early movement”, “early return to a normal diet” and “reassurance”) model and combined it with the ERAS (LEER-ERAS) program, in which relevant expert consensus, clinical pathway guidelines, and high-level evidence-based recommendations in the field of ERAS were collected and integrated. Subsequently, and based on the actual situation, the ultimate goal was the recovery of patients using the four modules (noted above) of the LEER model to simplify the work thinking and the methods for efficient clinical implementation,9 which subsequently achieved good results in clinical practice.
To highlight the central role of nursing in the LEER-ERAS model, and to enable the implementation of this innovative model of nursing care, a multi-target nursing group (MTNG) was created. The MTNG included a pain management nursing team, an organ function, movement and rehabilitation management nursing team, a feeding and nutrition management nursing team, and a psychological management nursing team, which were precisely aligned with the four ultimate goals of patient rehabilitation as proposed by the LEER-ERAS model (less pain, early movement, early return to a normal diet, and reassurance). In the present study, the clinical results of the MTNG workflow, which had been implemented precisely in the perioperative period among patients with hepatobiliary and pancreatic malignancies, are reported as follows.
Materials and Methods
General Materials
The clinical data of 198 patients with hepatobiliary and pancreatic malignancies in the present center were retrospectively analyzed from April 2018 to March 2021. The patients were divided into two groups, based on the different nursing measures adopted during the perioperative period. Accordingly, 91 cases were included in the traditional group with the adoption of traditional perioperative care, and 107 cases were included in the MTNG group with the adoption of the MTNG measures. There were no statistically significant differences in terms of age, gender ratio, body mass index, type of disease, combined underlying diseases, or other baseline characteristics between the two groups (P > 0.05), and the data were comparable (see Table 1). The present study was approved by the ethics committee of the hospital, and the patients and their families signed the relevant informed consent forms for inclusion in the research.
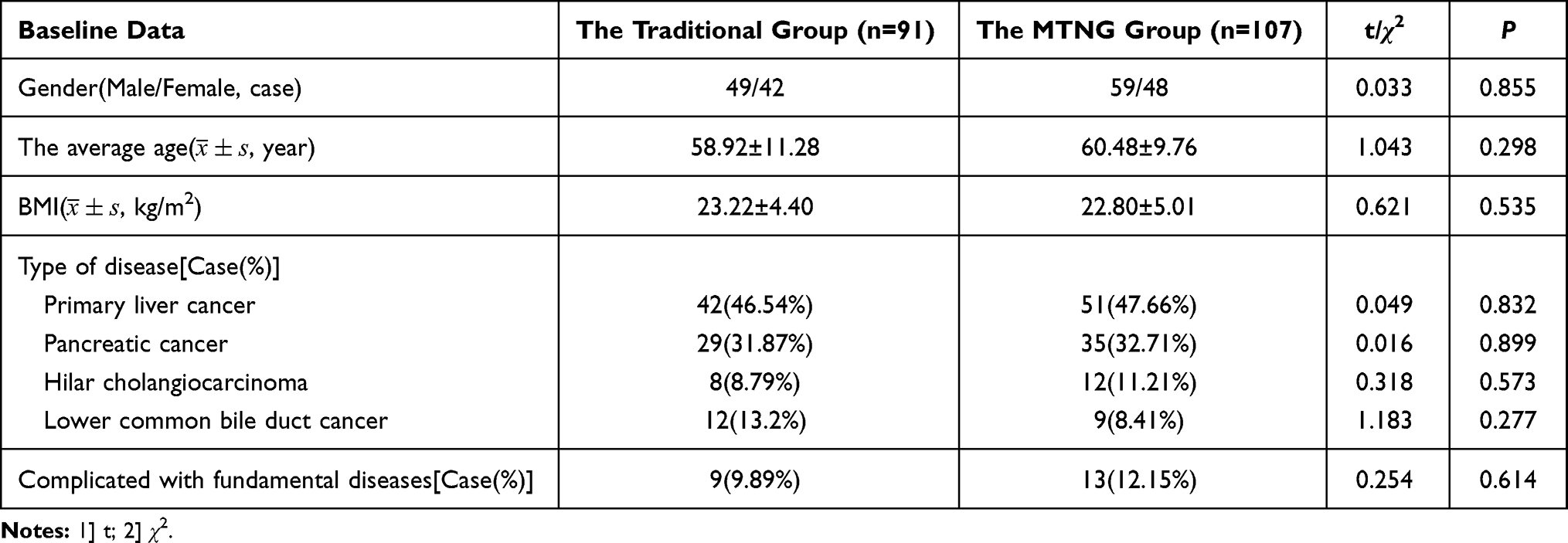 |
Table 1 Comparison of the General Characteristics Between Patients in the Traditional Group and the MTGN Group |
The Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) patients aged 18 or older but ≤75 years with a preoperative pathological or clinical diagnosis of hepatobiliary and pancreatic malignancies; (2) patients who had not received any preoperative local intervention and systemic treatments including radiotherapy, targeted therapy, and bioimmunotherapy; (3) patients with normal cardiac and pulmonary function and with grade I or II American Society of Anesthesiologist (ASA) scores; (4) patients who met the recommended surgical indications for hepatobiliary and pancreatic malignancies, had no contraindications to surgery, and who were to be treated with radical surgery; (5) patients who provided informed consent for their voluntary participation and cooperation in the study. The exclusion criteria were as follows: (1) patients with severe cardiovascular, cerebrovascular, respiratory, and psychiatric diseases; (2) patients with severe diabetes mellitus or coagulation abnormalities; (3) patients with metastatic cancers who were to be treated by palliative resection, or those with unresectable cancers; (4) patients with severe hepatic and renal dysfunction.
Method
The Traditional Group
(1) Pre-operative procedures: on admission, routine admission information and education, routine pain composite assessment, and routine mood index score were conducted by the charge nurse. The preoperative physical exercise training and respiratory function exercise, special nutritional support treatment, and special preoperative psychological guidance intervention processes were not conducted by the daily bedside nurse. The patients routinely underwent food and drink fasting for 10 hours before surgery, and preoperative total bowel preparation was routinely performed.
(2) Intra-operative and post-operative procedures. Gastric and urinary catheters were routinely placed by the surgical traveling nurses without the practice of intraoperative warming care. Psychological reassurance measures were not conducted by the anesthesia preparation nurses in the anesthesia waiting room. Infusions for pain management were postoperatively routinely administered by the bedside nurses without pain scoring using the visual analog scale (VAS). The opioid medication for pain was dispensed randomly according to the patients’ needs. No systematic motor rehabilitation training was conducted. The family members of patients were advised to help the patient move appropriately. The gastric tube was removed, and the patients were allowed to eat and drink as per the recovery of gastrointestinal function (after flatulence). The urinary catheter was clamped following the surgery and was removed until the patient felt like holding urine. The infusion volume and rate were empirically adjusted by the bedside nurses, and there was no uniform discharge standard.
The multi-target nursing group. The MTNG was a care management team that had been developed based on the LEER-ERAS model. According to this approach, the nursing staff of the department was divided into four groups, based on the four core objectives of the LEER-ERAS model. The nursing staff members were trained in the four different professional areas (pain, rehabilitation, nutrition, and psychiatry) through studies completed abroad and domestic training. The nursing cadres were selected as the team leaders of the pain management nursing team, the organ function, movement and rehabilitation management nursing team, the feeding and nutrition management nursing team, and the psychological management nursing team, with priority given to specialist nurses during the selection.
Each team leader was responsible for the training and education of nurses in their respective teams, in addition to work planning, ensuring the quality control of nursing care, as well as the implementation of clinical measures for patients enrolled in the ERAS program in their area of responsibility. The professional strengths of the specialist nurses were strongly encouraged to drive the effective operation of the group. Concurrently, the team members could participate in the development of the ERAS program for the patients and in making adjustments to the plan. For this purpose, the center also developed the details related to work responsibilities, workflow, quality standards, and health information forms for each team. All patients in the LEER-ERAS group followed the four principles of less pain, early movement, early return to a normal diet, and reassurance, and the MTNG team was involved in the entire care management, hence forming a truly patient-centered and group-to-person care model. The detailed perioperative ERAS strategies aimed at patients enrolled in the MTNG full management group are shown in Table 2.
 |
Table 2 The Peri-Operative ERAS Strategies in the MTNG Group |
Observation Indicators
The postoperative recovery indicators (including the postoperative VAS pain score, time of postoperative ambulation, postoperative time to flatulence, postoperative time to resuming a normal diet, postoperative catheter indwelling duration, postoperative length of hospital stay, and hospitalization expenses), the incidence of postoperative complications, postoperative unplanned readmission rate, and the implementation rate of nursing measures were observed and compared between the two groups.
Patients’ degree of understanding of the disease, compliance, and satisfaction with nursing care were investigated and compared between the two groups. (1) Based on the actual situation in the present center, the “Questionnaire for the Patient’s Understanding of Disease” was developed, which addressed the ERAS concept, perioperative precautions, and discharge guidelines. The total score was 100 points, and a score of ≥90 points reflected that the patient had a good understanding of the disease. (2) A scale for patient compliance was developed, which included the accessibility of health services, the influence of medical personnel on patients, the psychological and behavioral factors of patients, and attitudes toward diseases. The total score was 100 points, and a score ≥90 points reflected good compliance. (3) Patient satisfaction with nursing care was investigated using a questionnaire with a score of 100 points, which was divided into “very satisfied” (80–100 points), “satisfied” (79–60 points), and “unsatisfied” (less than 60 points) scores. The total satisfaction rate equaled the number of very satisfied cases + the number of satisfied cases/the total number of cases × 100%.
Statistical Methods
The SPSS Statistics (v.25) software program was adopted to conduct statistical analysis for all of the collected data. The measurement data that satisfied the normal distribution were expressed as the mean ± the standard deviation; t-tests were also conducted. The chi-squared test was used for the comparison of countable data and the comparison of rates; P < 0.05 was considered statistically significant.
Results
The Comparison of Postoperative Recovery Indicators Between the Traditional Group and the Multi-Target Nursing Group
Compared with the traditional group, the MTNG group had lower levels of pain and hospitalization expenses, earlier postoperative flatulence, the earlier continuation of a normal diet, and earlier postoperative ambulation, together with a shorter postoperative indwelling duration and length of hospital stay (P < 0.05) as shown in Table 3.
 |
Table 3 The Postoperative Recovery Indicators Between the Traditional Group and the MTNG Group |
The Comparison of Postoperative Complication Incidence, Unplanned Readmission Rate, and the Implementation Rate of Nursing Measures Between the Traditional Group and the Multi-Target Nursing Group
Compared with the traditional group, there were no significant differences in the incidence of postoperative complications and unplanned postoperative readmission rate in the MTNG group (P > 0.05). The MTNG group had a higher implementation rate of nursing measures (P < 0.05) as shown in Table 4.
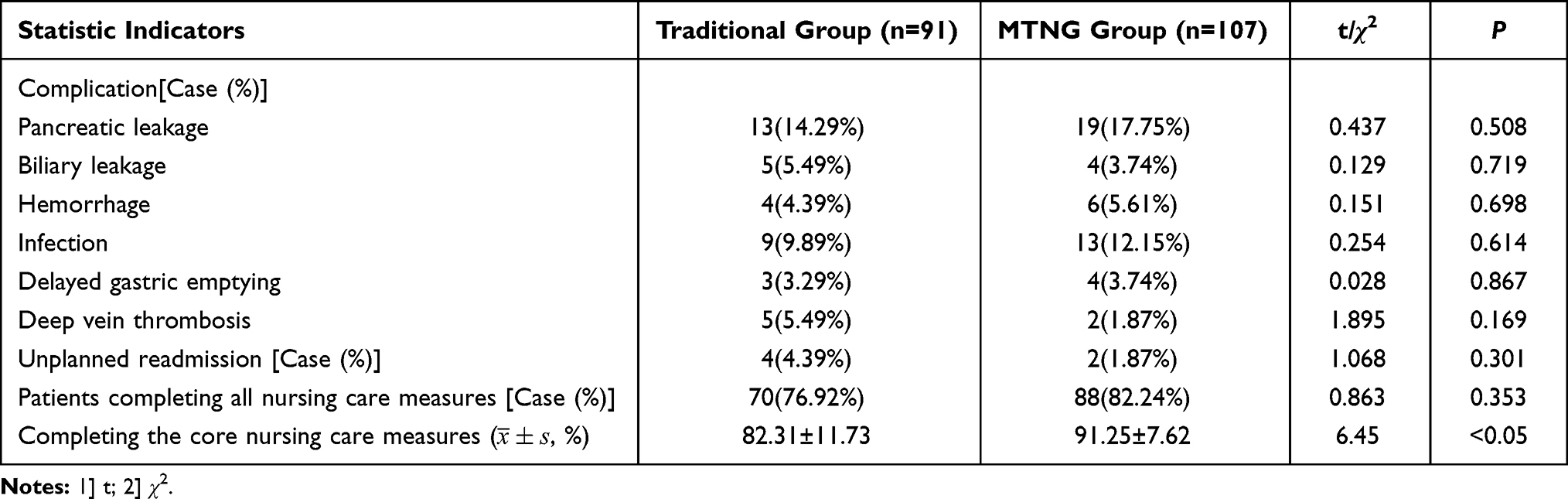 |
Table 4 Comparison of Rate of Postoperative Complications, Unplanned Readmission and Implementation of Nursing Measures |
Comparing the Level of Patient Understanding of the Disease, Compliance, and Their Satisfaction with Nursing Care During Hospitalization Between the Traditional Group and the Multi-Target Nursing Group
Compared with those in the traditional group, patients in the MTNG group reflected a higher degree of understanding of the disease, compliance with medical treatment, and satisfaction with nursing care during hospitalization; the differences were statistically significant (P < 0.05) as shown in Table 5.
 |
Table 5 Comparison of the Patients’ Understanding of the Disease, Compliance, and Satisfaction with Nursing Care |
Discussion
The Multi-Target Nursing Group Work Model Was Safe and Feasible, Could Effectively Promote Post-Operative Recovery, and Shorten the Length of Hospital Stay for Patients
In recent years, with the widespread application of ERAS procedures in perioperative care management, an increasing number of studies have demonstrated that clinical care guided by the ERAS concept can significantly relieve patients’ postoperative pain and accelerate their physical and psychological recovery,10 without increasing the perioperative risk. In the present study, the results of the MTNG group, combined with the ERAS model in terms of effectiveness, included the following: a lower degree of pain, lower hospitalization expenses, earlier postoperative flatulence, the earlier continuation of a normal diet, and earlier postoperative ambulation, together with a shorter postoperative indwelling duration and length of hospital stay (P < 0.05). Concerning safety, the results indicated no significant differences in the incidence of postoperative complications and postoperative unplanned readmission rates between the MTNG and the traditional group (P > 0.05). These results are consistent with relevant domestic and international reports,11,12 which further validates the initial results of the systematic ERAS standardization ward established in the present center.
The Multi-Target Nursing Group Work Model Changed the Mindset of Healthcare Professionals, Improved the Implementation Rate of Nursing Measures, and Ensured the Standardization of the Enhanced Recovery After Surgery Approach
A study conducted by Brady13 showed that the implementation rate of nursing measures in an ERAS group increased from 61% to 93%, indicating that nurses were integral to the success of ERAS and that the orderly implementation of ERAS processes could also greatly improve the implementation rate of nursing measures. These results are consistent with the results in the present study presented below.
Compared to the traditional group, the MTNG group had a higher proportion of cases that completed all nursing care measures (P < 0.05), together with a higher rate of completing the core nursing care measures for a single case (P < 0.001). We believe that the MTNG team created in our center, based on the LEER model with the integrated ERAS concept, changed the inherent thinking of medical and nursing staff from doing “what I am asked to do” to considering “what I have to do”, with a focus on the four ultimate patient goals (less pain, early movement, early continuation of a normal diet, and reassurance). The procedures in the traditional and complicated ERAS measures were classified into four major areas and assigned to four nursing teams for implementation. By remembering these four ultimate goals, healthcare professionals could quickly respond to the ERAS measures and change complicated implementation procedures from being passive to proactive, which not only made the ERAS measures in terms of clauses and concepts more vivid and simple but also increased the implementation rate of ERAS measures by nurses.
The Multi-Target Nursing Group Work Model Improved the Compliance and Satisfaction of Patients and Assisted in the Implementation of Their Enhanced Recovery After Surgery
The results of a prospective cohort study by Pędziwiatr et al14 on patient compliance to improve prognosis showed that strict compliance with perioperative management of ERAS significantly reduced the incidence of postoperative complications. Accordingly, it was suggested that improving patient compliance may be a core aspect of ERAS measures. The nursing staff, as the conductors of all treatment and decision-making in the implementation of ERAS processes, are the group most capable of comprehensively and holistically observing and participating in any changes that arise in the condition and recovery process of patients. Preoperatively, as well as throughout the entire hospitalization process, education and problem-solving in various forms can help to make nurses aware of the important role they play in the program and provide them with the skills to understand patients and facilitate their cooperation, which is crucial for improving compliance and satisfaction with medical care.15 In the present study, the MTNG team aimed to achieve the four noted goals for patients, precisely formulated the standardized nursing procedures, followed the model of the surgical medical group, and adopted a “one-group-to-one-patient” approach for leading the perioperative recovery process. In doing so, the team aimed to avoid creating psychological fear among patients to the best extent possible, improve the patients’ understanding of the disease (P < 0.001) and their compliance (P < 0.01), facilitate the smooth and precise implementation of ERAS nursing measures, and improve patient satisfaction with nursing work in general (P < 0.01).
The Multi-Target Nursing Group Work Model Expanded the Development Direction and Practice Value of Specialist Nurses, Promoted the Development of a Multidisciplinary Model of Nursing Collaboration, and Ensured the Stable and Sustainable Development of Nursing Teams
Ljungqvist et al16 showed that perioperative care within ERAS measures should be multimodal and required the collaboration of nursing specialists with different medical or healthcare professional backgrounds, such as psychiatric and nutritional nurses, and physiotherapists; in some cases, multidisciplinary and multi-department collaboration will also be essential. With an emphasis on the training of specialist nurses in China in recent years, the number of specialist nurses has increased annually. However, the management of specialist nurses has not received sufficient attention; furthermore, the attitude of “training is important, but its application is not” subsists, where nurses are transferred from roles related to the certification field after obtaining a specialist nurse qualification, only to find that the content of the role is not consistent with the certification field. The lack of focus regarding the role of specialist nurses affects the stability of the specialist nurse team and the development of specialist nursing overall. In the present study, during the process of selecting and involving the personnel included in the study, the MTNG team adopted the specialty knowledge of the specialist nurses as a foundation and made an effort to involve them as it concerned their professional strengths. This ensured that their solid theoretical knowledge and highly professional skills were being fully utilized in their area of expertise and helped to guide the clinical nursing practice of the team members in the ERAS process. In turn, this helped to ensure that their learning was employed in a useful manner and that they could carry out specialist nursing work and accumulate expert nursing experience in their specific specialty areas. While improving the quality of ERAS nursing practice, this approach strengthened the training and management of specialist nurses, which was conducive to the creation of a specialist nursing talent ladder, and helped to establish the stability of the specialist nursing team.
The Challenges We May Face in the Developing Countries
It’s difficult for primary hospitals to form a multi-target nursing group and perform the process precisely as the small number of nurses, especially the specialist nurses. We think one person affording some jobs at the same time is the best way to solve the problem. Though the work load in these primary hospitals were light, the nursing work was complicated and essential. We need the office nurse, logistic nurse, charge nurse, assistant nurse in a tertiary hospital, but one nurse in these primary hospitals might be enough. In other words, we should focus on the correct implements of MTNG work rather than adequate human resources. For example, one district hospital in our city has only one surgical ward, 9 nurses but 7 on duty, average patients were fewer than 20, mean surgical volume was 10–20 every month, the charge nurse could achieve all the perioperative period nursing work, including perioperative education, evaluation, health guidance, effect evaluation. The job was done perfectly although there were not enough group members.
Summary
The nursing profession must be able to adapt to new practice requirements resulting from the development of ERAS measures, revise the traditional nursing model, explore and innovate new ERAS nursing service concepts and processes, and better meet the new changes and opportunities brought about by ERAS approaches to the nursing profession. Leadership within clinical medicine is typically dictated by surgeons, who are assisted by an anesthesiologist. In contrast, for ERAS practice, the real managers are the nurses.17 As ERAS coordinators, nurses play the vital role of serving as the “engine” of the ERAS team, working on practical matters, and acting as a “bridge” between the physician-led multidisciplinary medical model and the integrated medical and nursing management model.18 With the advancement of ERAS practice, the relevant nursing concepts have received additional attention from nursing experts. In foreign countries, special training courses are provided to ERAS specialist nurses,19 while the integration of hospital and community nurses’ work is linked to extending ERAS services to post-discharge community care. The authors believe that these approaches may be among the future directions of ERAS nursing contexts. The MTNG model established in the present center, which is based on the LEER model with the ERAS concept, provides a new career direction for specialist nurses while, concurrently, implementing the ERAS approach precisely and effectively. It is hoped that in the future promotion of the LEER model in an ERAS context and the MTNG model, prospective multicenter, randomized controlled studies with more cases, and, with additional participating centers, could be jointly conducted to reduce bias and explore the clinical application value of the MTNG model, thereby providing more and higher-level evidence-based clinical pathways and guidelines for the development of ERAS measures.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Leshan People’s Hospital. A written informed consent was obtained from all participants.
Funding
Health Science Research Project of Sichuan Provincial Health Commission in 2020 (No.:20PJ296).
Disclosure
None of the authors have any financial disclosure or conflict of interest.
References
1. Sibbern T, Bull Sellevold V, Steindal SA, Dale C, Watt-Watson J, Dihle A. Patients’ experiences of enhanced recovery after surgery: a systematic review of qualitative studies. J Clin Nurs. 2017;26(9–10):1172–1188. doi:10.1111/jocn.13456
2. Melloul E, Lassen K, Roulin D, et al. Guidelines for perioperative care for pancreatoduodenectomy: Enhanced Recovery After Surgery (ERAS) recommendations 2019. World J Surg. 2020;44(7):2056–2084.
3. Francis NK, Walker T, Carter F, et al. Consensus on training and implementation of enhanced recovery after surgery: a Delphi Study. World J Surg. 2018;42(7):1919–1928. doi:10.1007/s00268-017-4436-2
4. Mendes DIA, de Almeida Clemente Ferrito CR, Gonçalves MIR. Nursing interventions in the enhanced recovery after surgery®: scoping review. Rev Bras Enferm. 2018;71(suppl 6):2824–2832. doi:10.1590/0034-7167-2018-0436
5. Ljungqvist O, de Boer HD, Balfour A, et al. Opportunities and challenges for the next phase of enhanced recovery after surgery: a review. JAMA Surg. 2021;156(8):775–784. doi:10.1001/jamasurg.2021.0586
6. Brown D, Xhaja A. Nursing perspectives on enhanced recovery after surgery. Surg Clin North Am. 2018;98(6):1211–1221. doi:10.1016/j.suc.2018.07.008
7. Hübner M, Addor V, Slieker J, et al. The impact of an enhanced recovery pathway on nursing workload: a retrospective cohort study. Int J Surg. 2015;24(Pt A):45–50. doi:10.1016/j.ijsu.2015.10.025
8. Visioni A, Shah R, Gabriel E, Attwood K, Kukar M, Nurkin S. Enhanced recovery after surgery for noncolorectal surgery?: a systematic review and meta-analysis of major abdominal surgery. Ann Surg. 2018;267(1):57–65. doi:10.1097/SLA.0000000000002267
9. Lei Z, Xie Q, Zhao X. Application of “LEER” mode enhanced recovery after surgery in pancreatoduodenectomy. J Hepatopancreatobiliary Surg. 2020;32(3):138–142. doi:10.11952/j.issn.1007-1954.2020.03.003
10. Hjort Jakobsen D, Rud K, Kehlet H, Egerod I. Standardising fast-track surgical nursing care in Denmark. Br J Nurs. 2014;23(9):471–476. doi:10.12968/bjon.2014.23.9.471
11. Foss M, Bernard H. Enhanced recovery after surgery: implications for nurses. Br J Nurs. 2012;21(4):221–223. doi:10.12968/bjon.2012.21.4.221
12. Zhao Y, Qin H, Wu Y, Xiang B. Enhanced recovery after surgery program reduces length of hospital stay and complications in liver resection: a PRISMA-compliant systematic review and meta-analysis of randomized controlled trials. Medicine. 2017;96(31):e7628. doi:10.1097/MD.0000000000007628
13. Brady KM, Keller DS, Delaney CP. Successful implementation of an enhanced recovery pathway: the nurse’s role. AORN J. 2015;102(5):469–481. doi:10.1016/j.aorn.2015.08.015
14. Pędziwiatr M, Kisialeuski M, Wierdak M, et al. Early implementation of Enhanced Recovery After Surgery (ERAS®) protocol - compliance improves outcomes: a prospective cohort study. Int J Surg. 2015;21:75–81. doi:10.1016/j.ijsu.2015.06.087
15. Surgery CS of, Anesthesiology CS of. Consensus on ERAS and guidelines for pathway management in China (2018). Chin J Anesthesiol. 2018;38(1):8–13. doi:10.3760/cma.j.issn.0254-1416.2018.01.003
16. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
17. Gotlib Conn L, McKenzie M, Pearsall EA, McLeod RS. Successful implementation of an enhanced recovery after surgery programme for elective colorectal surgery: a process evaluation of champions’ experiences. Implement Sci. 2015;10:99. doi:10.1186/s13012-015-0289-y
18. Galli E, Fagnani C, Laurora I, et al. Enhanced Recovery After Surgery (ERAS) multimodal programme as experienced by pancreatic surgery patients: findings from an Italian qualitative study. Int J Surg. 2015;23(Pt A):152–159. doi:10.1016/j.ijsu.2015.09.071
19. Australian Safety & Efficacy Register of New Interventional Procedures–Surgical & The Royal Australasian College of Surgeons. Brief Review: Fast-Track Surgery and Enhanced Recovery After Surgery (ERAS) Programs[R]. Melbourne, Australia: Victorian Department of Human Services; 2009:1.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.