Back to Journals » Psychology Research and Behavior Management » Volume 17
Exploring Stigma Experience and Coping Strategies Among Women Living with HIV/AIDS in China: A Phenomenological Study
Authors Yang Z, Yang H, Gong B, Zhang L, Fu Y ![]() , Hu Y
, Hu Y ![]()
Received 29 December 2023
Accepted for publication 30 March 2024
Published 6 April 2024 Volume 2024:17 Pages 1487—1498
DOI https://doi.org/10.2147/PRBM.S456850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gabriela Topa
Zhongfang Yang,1– 4 Hongli Yang,5 Beibei Gong,6 Lin Zhang,7 Yanfen Fu,8 Yan Hu1– 3
1Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, Shanghai, People’s Republic of China; 2School of Nursing, Fudan University, Shanghai, People’s Republic of China; 3Fudan University Centre for Evidence-Based Nursing: A Joanna Briggs Institute Centre of Excellence Department, Fudan University, Shanghai, People’s Republic of China; 4NYU Rory Meyers College of Nursing, New York University, New York, NY, USA; 5Department of Nursing, Yunnan Provincial Hospital of Infectious Disease/Yunnan AIDS Care Center/Yunnan Mental Health Center, Kunming, People’s Republic of China; 6Department of Nursing, The Fourth People’s Hospital of Nanning, Nanning, People’s Republic of China; 7Department of Nursing, Shanghai Public Health Clinical Center, Shanghai, People’s Republic of China; 8School of Nursing, Dali University, Dali, People’s Republic of China
Correspondence: Yan Hu, Shanghai Institute of Infectious Disease and Biosecurity, Fudan University, No. 305 Fenglin Road, Xuhui District, Shanghai, 200032, People’s Republic of China, Email [email protected]
Purpose: As of the end of 2022, over 20 million women worldwide, aged 15 and above, are living with HIV. Stigma remains a formidable barrier for women living with HIV/AIDS, hindering their access to healthcare and exacerbating health disparities. Indeed, some women living with HIV/AIDS can successfully confront and overcome stigma. There remains a paucity of qualitative research exploring the stigma coping strategies of women living with HIV/AIDS in China. This study was aimed to gain the deeper understanding of stigma experienced by women living with HIV/AIDS and coping strategies.
Patients and Methods: We recruited diverse participants using snowball sampling and purposive sampling. Semi-structured personal in-depth interviews were conducted with 30 women living with HIV/AIDS from December 2022 to June 2023. The samples were from four HIV/AIDS designated hospitals. The data were analyzed using the Colaizzi seven-step model.
Results: The experiences of stigma among women living with HIV/AIDS included family role (wife/mother/grandmother) collapse and disgusted by family, resignation in being shunned by others, helplessness due to social exclusion, grief at being devaluated, and resentment for experiencing injustice. The coping strategies used to deal with stigma included concealing their conditions, avoiding socialization, and attempting to retaliate against society.
Conclusion: Healthcare professionals are recommended to offer women living with HIV/AIDS effective emotional support and guidance to cope with stigma. The study highlights the stigma they face, providing valuable evidence for policymakers. Recommendations emphasize the importance of developing services addressing both physical and psychological needs of women living with HIV/AIDS.
Keywords: female, acquired immunodeficiency syndrome, social stigma, Asian, qualitative research
Introduction
Since the first cases of AIDS were detected in the 1980s, it has posed a significant global public health threat.1 This threat is particularly pronounced among women due to the confluence of factors, including biological vulnerability, low economic status, the predominance of male sexual behavior, and various epidemiological factors.2 As of the end of 2022, there has been approximately 39 million people globally infected with HIV, with 20.67 million (53%) being women and girl.3
Most women living with HIV/AIDS (WLWHA) contracted HIV from their husbands.4 It is not easy for WLWHA to accept the fact that they were infected with HIV, especially from their husbands, even WLWHA’s husbands did not intentionally infect them with HIV. WLWHA’s husbands often realized that they were infected with HIV only after they have experienced opportunistic infections or even died, but it was too late. WLWHA may pass HIV to their children. On one hand, WLWHA may become pregnant without knowing they were infected with HIV and passed HIV to their children through mother-to-child transmission (MTCT).5 On the other hand, it is also possible to transmit HIV to their child through blood transmission or other means in everyday life.6 HIV infection can lead to challenges in the ability of WLWHA to care for their children, potentially resulting in custody loss.7 WLWHA will not be able to continue their maternal responsibilities. All of the above are sources of self-stigma experienced by WLWHA. Although women may be infected with HIV from their husbands or through MTCT, there is a public misconception that attributes their infection to perceived immoral behaviors like promiscuity or drug use.8 This reinforces public stigma against WLWHA.
Many WLWHA have experienced high level of stigmatization.9 HIV-related stigma has severe consequences for people living with HIV/AIDS (PLWHA), including income and livelihood loss, marital problems, inadequate healthcare, reduced home-based care, feelings of hopelessness, worthlessness, and damaged reputations.10 Additionally, among WLWHA, this stigma is linked to reproductive choices, depression, violence, disengagement from medical care, poor treatment adherence, higher viral loads, and an increased risk of mother-to-child HIV transmission.11 Stigma is preventing health equity.
The international community has shown increasing concern for the stigma faced by WLWHA and has implemented numerous intervention programs to address this issue, yielding some positive results.12–16 However, current research remained the notably scarce of exploring mechanism that delved into assessment and interventions. To address these gaps, it is necessary to explore HIV-related stigma experienced by WLWHA and how they cope with these experiences. This study aimed to provide an in-depth understanding of WLWHA’s experiences with stigma and their coping mechanisms from their perspective. This research will serve as a foundational basis for developing stigma assessment tools and formulating effective intervention strategies.
Methods
Research Ethics
Every participant signed an Informed Consent Form. The participants informed consent specifically included publication of their anonymized responses. It is essential to emphasize that the information garnered from these participants was rigorously upheld as confidential throughout the entire research process. Furthermore, it is noteworthy that the present study diligently adhered to the ethical principles set forth in the Declaration of Helsinki. This study was approved by the Institutional Review Board of the School of Nursing, Fudan University (IRB#2023-4-1). In accordance with these ethical considerations and research ethics guidelines, the identities of all individuals who participated in this study were safeguarded by maintaining strict confidentiality. The paramount concern throughout this research endeavor was to ensure and respect the privacy of all participants.
Participants
The participants in this study comprised WLWHA who sought care at outpatient clinics or were hospitalized in the following healthcare facilities: Shanghai Public Health Clinical Center (SPHCC), Yunnan Provincial Hospital of Infectious Disease (also known as Yunnan AIDS Care Center), The Fourth People’s Hospital of Nanning, and The People’s Hospital of Dali Bai Autonomous Prefecture. Data collection took place from December 2022 to June 2023. Inclusion Criteria were proposed for selecting candidates: (1) Women diagnosed as HIV-positive through laboratory tests, confirmed by confirmatory experiments. This encompassed both women living with HIV and those diagnosed with AIDS. The AIDS patient was defined as an HIV-infected individual with a CD4+ T-lymphocyte count of less than 200/microliter or the presence of HIV-related symptoms, opportunistic infections, or tumors;17 (2) WLWHA were required to have normal memory and comprehension skills, as assessed through Chinese version of the Mini-Mental State Examination (MMSE).18 They were also expected to express their inner experiences and actively participate in the study after (3) providing informed consent. The informed consent process itself is an opportunity to gauge the participant’s capacity to express themselves. We exclude participants with mental disabilities.
The intentional sampling method was utilized to recruit participants who represented a diverse range of characteristics, including age, marital status, sexual orientation, social support, education level, place of residence, and duration of the disease. Furthermore, we employed a snowballing approach to participant recruitment. The sample size was determined based on data saturation, where no new themes emerged from the data analysis.
The research encompassed 30 semi-structured individual interviews, and the participants’ ages ranged from 19 to 67 years, with an average age of 46 years. Marital status of participants: 19 married, 4 single, 3 widowed, 4 divorced. Sexual orientation: 25 heterosexual, 5 homosexual; Social Support: 11 cases living alone, 19 cases living with family. Education level: 5 cases in primary school, 10 cases in middle school, 15 cases in college or above. Occupation: 5 cases in cadres, 3 cases in workers, 2 cases in students, 8 cases in retirement, 9 cases in unemployment, 3 cases in farmers. Place of residence: 6 cases in rural areas and 10 cases in urban areas. The total duration of the disease among the participants ranged from 1 to 25 years, with an average of 5.67 years and a median of 9 years (See Table 1).
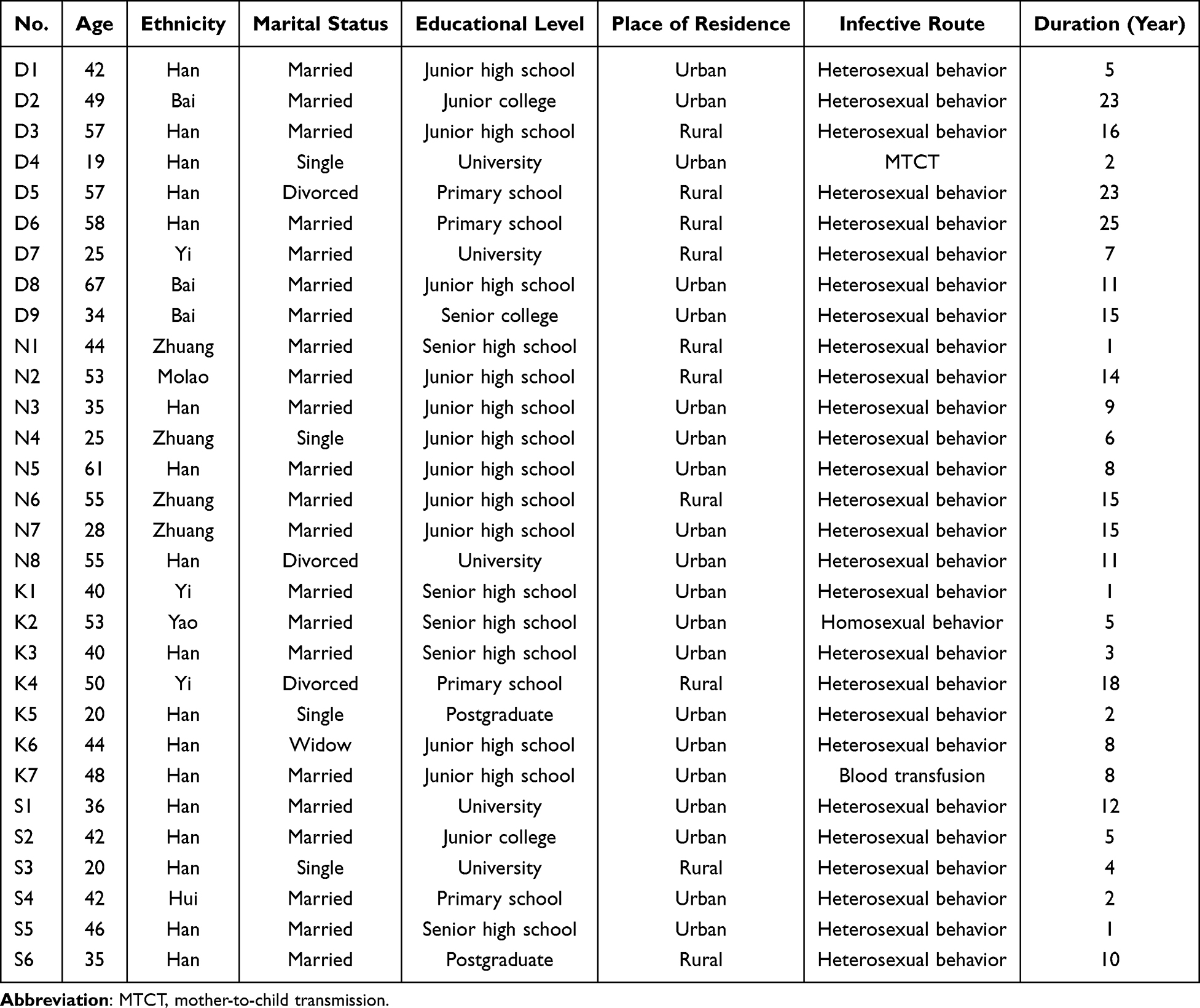 |
Table 1 General Information of Participants (n=30) |
Data Collection
Foster Connections with Participants
Data were obtained through face-to-face, personal in-depth interviews. The interviews took place in private, undisturbed independent rooms with a relaxed atmosphere and ample time allocated. Before the interviews, the researcher introduced himself. And then, participants received a detailed explanation of the study’s purpose, significance, content, and methodology. They were also informed about the necessity of audio recording. To safeguard their privacy and address any concerns, participants were assured that codes, rather than their names, would be used to identify their responses. Establish an environment that encouraged participate to provide honest and thorough answers by informing them about measures in place to ensure data security. Informed consent forms were signed to formalize the agreement.
In-Depth Interview
To operationalize the methodological approach aimed at achieving data saturation, the depth of each individual interview was outlined by employing circular questions that delve into the examined phenomenon.19 A total of 10 interview questions were employed, as outlined in Figure 1. This study adhered to a flexible approach, allowing for the adjustment of the interview outline’s content and order. The interviews commenced with the question, “Would you please share with me your experience of how HIV got to you?” This introductory question aimed to establish a relaxed conversational atmosphere. Subsequently, the scope of questions was gradually focus on their stigma experience. The interviews were conducted without providing guidance or cues to participants. Open-ended questions were utilized when interviewees shared their experiences of stigma. In cases where interviewees wished to provide detailed descriptions of impactful experiences, the researcher could accommodate by allocating additional time for elaboration and subsequently guiding the interviewee to address other questions based on the context.
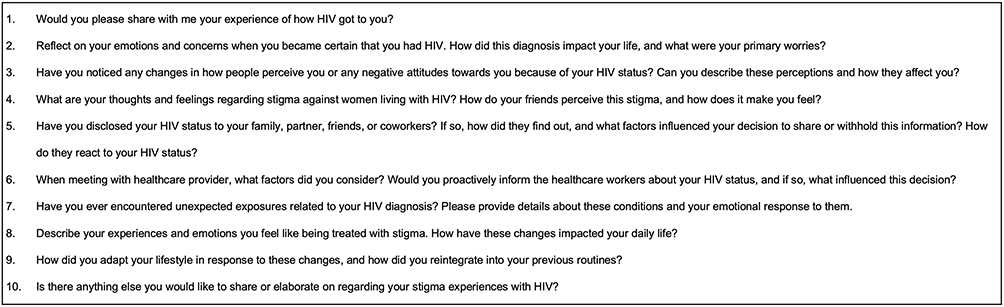 |
Figure 1 Outline of Qualitative Interview Questions. |
Supplemented by Observations and Textual Records
Throughout the interviews, the researcher attentively observed and recorded various aspects, including the participant’s speech tempo, tone, and subtle changes in facial expressions. The researcher also took steps to promptly record information and, when needed, sought clarification or confirmation of interviewee feelings or opinions. Observation and text recording was to aid in the subsequent data analysis and reflection process. Each interview lasted approximately 45–60 minutes.
Data Analysis
The audio recording of the interview was carefully reviewed. All statements made by the research subjects, as well as the researcher’s field notes, were meticulously transcribed into text format and printed separately. Data analysis commenced after the transcription of the first interview. It is noteworthy that by the time the 30th interview was analyzed, no new themes or information emerged from the data.
The data analysis procedure adhered to Colaizzi’s seven-step content analysis method, which encompasses the following steps.20
I. Comprehensive Understanding: Thoroughly read and immerse in the interview data to establish a comprehensive understanding of the descriptions provided by the interviewees. In cases of ambiguity, meticulous verification against the video recording was conducted.
II. Extraction of Significant Statements: Extract statements from the data that are relevant to the research phenomenon under investigation.
III. Bracketing and Coding: Extract the meanings embedded within the significant statements and assign codes to facilitate categorization. Throughout this process, the researcher immersed into data, bracketed the phenomena, and strived to capture the essence of the interviewee’s experiences.
IV. Formation of Themes: Summarize the coded meanings, seeking common concepts or characteristics that can be grouped into themes, thematic groups, and categories.
V. Integration and Comprehensive Description: Integrate the findings of the investigation into the phenomenon and present them in a manner that provides a rich description of the phenomenon. This step serves to provide an in-depth understanding of the research theme.
VI. Establishment of Basic Structure: Through the exhaustive description, establish the fundamental structure that characterizes the nature of the phenomenon under investigation.
VII. Comparison with Interviewee’s Experience: Present the results of the analysis to the interviewees and engage in a comparative assessment to ascertain whether the findings accurately reflect the real experiences of the interviewees.
Quality Control
In this study, the rigor and trustworthiness of the research are addressed by considering four key aspects: credibility, transferability, dependability, and confirmability, as recommended by Lincoln and Guba.21
Credibility
To specifically address the issue of credibility, the peer review process was conducted. Prior to data analysis, the researcher discussed the phenomenon under investigation with peers. Pre-interviews (five in total) were reviewed, and the meaningful statements and extracted meanings from the original data were thoroughly discussed with research team and peers. To further increase the credibility of the study, participants were purposively selected to ensure the characteristics of the participants covering various nature of WLWHA such as age, marital status, sexual orientation, social support, education level, place of residence, and duration of the disease. Additionally, the researcher had prior experience in clinical nursing practice and was skilled in communication with WLWHA. Interviews were facilitated through referrals from attending physicians and follow-up nurses/case managers, establishing a trusting and natural context for interviewees to express their true feelings.
During the interviews, full consent was obtained, and the entire interview was videotaped. Transcription of the video interviews was completed promptly within 24–72 hours after each interview. If any content was found to be missing or questionable during transcription, interviewees were contacted for clarification, and follow-up interviews were conducted as needed. Moreover, discussions were held with mentors and subject team members experienced in qualitative interviewing during the pre-interview phase to ensure that interviewing techniques were effectively employed and that comprehensive information was collected. Regular discussions with the mentor and clinical experts with caregiving experience and qualitative research training were conducted to validate the data collection and analysis process, ensuring alignment with the true essence of the phenomenon and research results.
Transferability
Open-ended questions were utilized to allow respondents the freedom to express themselves comprehensively. Furthermore, when responses were vague or required further elaboration, respondents were encouraged to provide more detailed and clear descriptions. To bolster the transferability of the study’s findings, a diverse group of WLWHA was selected from various regions, including East, Southwest, and South China. The selection criteria were clearly defined, allowing for a comprehensive exploration of the phenomenon of stigma and its underlying socio-cultural significance.
Dependability
To further bolster dependability, the researcher maintained meticulous records, including backup copies of interview outlines, videotaped interviews, transcribed transcripts, and detailed documentation of the analysis and coding process.
Confirmability
To enhance confirmability, the researcher diligently maintained primary sources of information, including interviews, memos, and relevant literature. To mitigate the impact of researcher bias on data collection and analysis, which could potentially compromise research reliability and validity, the study employed the triangulation method. This method was utilized in cross-referencing and analyzing data from multiple sources, applying diverse research methods and tools. The researcher engaged in open and transparent communication with the interviewees to clarify any ambiguities or uncertainties.
Results
The total duration of the interview recordings was 800.22 minutes. The length of individual interviews varied, with durations ranging from 20 to 56 minutes, averaging 26 minutes. The interview data underwent qualitative analysis using the NVivo software. Two overarching clusters related to stigma emerged, encompassing seven distinct themes. From these themes, a total of 304 meaningful statements were extracted to provide deeper insights into the participants’ experiences.
Theme Cluster 1: Experiences with Stigma Among WLWHA
Theme 1: Family Role (Wife/Mother/Grandmother) Collapse and Disgusted by Family
HIV infection does not diminish women’s desire to embody the ideal of the “perfect woman”. However, within traditional Chinese culture, the ideal of the “perfect woman” is often associated with being a wife and mother. The inability to maintain a normal sex life with their husbands, meet their childcare responsibilities, and fulfill their roles as wives, mothers, and grandmothers due to HIV infection has disrupted their fundamental societal roles. This disruption has had adverse effects on their self-esteem and coping self-efficacy. Even though it was not their fault, they still experienced a sense of incompleteness, as if a part of their lives is missing.
Participants S1 stated that
“After the discovery (of HIV infection), my husband became too fearful to touch me. As a result, we started sleeping in separate rooms (with a wry smile)”.
Participant N3 shared her distressing experience,
After falling ill, my family prohibited me from checking my children’s homework or signing their school documents. I was also excluded from attending parent-teacher conferences. As a mother, this exclusion deeply hurts (Cover her heart with right hand). I’m incomplete.
Participant N5 shared a heart-wrenching account of her experience,
Initially, my son, daughter-in-law, and my beloved grandson lived together with me…It was there that she discovered my HIV-positive status. Upon returning home, she divorced my son and allowed her father to physically assault me. Now, she forbids me from seeing my precious grandson. (Her voice trembled as she wiped tears from her eyes)
Theme 2: Resignation in Being Shunned by Others
When WLWHA discloses her diagnosis, it often triggers intentional or unintentional avoidance by various individuals, including friends and coworkers. This avoidance is typically rooted in the fear of HIV transmission, which has been identified as the central factor contributing to stigma in numerous existing studies.
Participant S2 shared,
Some of my coworkers and I were very close, and then when they were told that I had the disease, they would intentionally or unintentionally stay away from me. I remember one chat, after I told them about the disease. One person was surprised and then unintentionally moved his chair back, and then we never talked again (sign).
This avoidance behavior can take various forms, ranging from unintentional distancing to intentional reduction of contact, refusal to share meals, or even complete severance of relationships. Such actions contribute to WLWHA’s feelings of social isolation and helplessness within society.
Theme 3: Helplessness Due to Social Exclusion
Exclusion, in this context, refers to the process of deliberately distancing oneself from individuals or groups, hindering their sense of belonging and relational needs. It often creates a psychological gap that impedes social connections. Exclusion emerges as a consequence of perceived group differences, perpetuated through social reproduction and influenced by socio-cultural ideologies. This phenomenon imposes significant social anxiety and psychological pressure on those who experience it, leading to increased feelings of isolation and helplessness.
Public perceptions of WLWHA patients often adhere to stereotypical beliefs, including notions of diminished capabilities, job rejection upon HIV detection in medical examinations. These stereotypes persist, whether or not individuals have witnessed the symptoms of WLWHA. The moment individuals learn about HIV infection or hospitalization for infectious diseases, they tend to ostracize and create psychological distance. They left WLWHA with a sense of being isolated on an island devoid of support.
Participant K3 shared her initial diagnosis experience,
I discovered this disease when I was hospitalized for appendicitis in our county hospital. I distinctly recall that once the doctors and nurses learned of my condition, they ceased their physical examinations of my stomach and subsequently transferred me to another hospital without providing any explanation.
Theme 4: Grief at Being Devalued
In the eyes of the public, HIV infection among women is often associated with judgmental labels such as “promiscuous” and “indiscreet”. This prevailing perception persists, even when the majority of WLWHA contract the virus from their husbands or through mother-to-child transmission. Consequently, WLWHA find themselves in a disheartening social position. Despite their clear status as innocent victims, they continue to face moral scrutiny from society, along with a lack of understanding and acceptance from relatives, friends, and the community. This unwarranted moral judgment deepens the emotional anguish experienced by WLWHA.
Participant N1 recounted her unfortunate situation,
I contracted HIV from my ex-boyfriend. At the time, my father was unwell, so I returned home to care for him. During my absence, my boyfriend engaged in risky behavior and contracted the disease. I began experiencing frequent illnesses, prompting a hospital visit that led to my diagnosis. Who could I confide in about this? In my pursuit of treatment, I left my job and returned to my hometown to receive medical care while attempting to conceal my condition, fearing that acquaintances might discover it. It felt like an unfortunate twist of fate.
Theme 5: Resentment for Experiencing Injustice
HIV/AIDS often carries a profound societal “label” rather than being seen as a medical condition with physical implications. This stigmatization, especially as experienced by WLWHA, is frequently accompanied by instances of unjust and discriminatory treatment, evoking deep-seated resentment among those affected. During the interviews, this issue emerged as a recurring source of distress.
Participant D3 recounted a distressing incident at a hospital,
The hospital exhibited discriminatory behavior. Upon discovering my HIV status, a doctor entered my room and interrogated me with a confrontational tone, asking, ‘What are you doing here with this disease?’ In their haste to leave, they instructed the nurse to remove all items from my bedside, casting a deep psychological shadow over me.
Theme Cluster 2: Coping Strategies for Stigma Among WLWHA
Theme 1: Concealing the Condition
To shield themselves from social stigma and the associated shame, WLWHA concealed their illness from the public. They subconsciously refrain from disclosing their condition, striving to evade the stigmatizing label that threatens their sense of self-worth.
Participant D9 shared her inner turmoil,
In the hope of securing future employment or forming meaningful relationships, I kept my condition hidden from the world, even from my closest friends. Yet, I would rather endure this isolation alone than acknowledge my status as an AIDS patient, risking hospitalization in an infectious disease ward due to the dread of social stigma.
Theme 2: Social Avoidance
WLWHA patients are frequently burdened with the label of “immorality”, dreading the revelation of their HIV-positive status during social interactions. This fear stems from the anticipation of encountering stereotypes and discriminatory attitudes from their social circles. Simultaneously, they are apprehensive about their compromised immune systems, rendering them more susceptible to infections during social gatherings than the general population. The expected psychological and physical toll often compels them to withdraw from social life, even in the absence of visible symptoms.
Participant K2 told her experience,
I used to enjoy playing mahjong with my neighbors before falling ill. However, after my diagnosis, I became too fearful to participate. I worry that if my neighbors spot me taking my medication, which is for AIDS (revealing the pill case), they will engage in gossip and stigma, even though we previously shared a cordial relationship.
Theme 3: Attempting to Retaliate Against Society
Some WLWHA patients contemplate seeking vengeance against society following their devaluation and unjust treatment due to their illness. The disease has resulted in the decline in their economic and social status, despite their personal efforts. Several interviewees in this study candidly expressed their resentment after facing stigma and experiencing injustice, leading them to entertain thoughts of rebellion.
Participant N6 revealed the financial toll the illness had taken,
“Frequent hospitalizations due to this disease have left me financially destitute. I’ve grown to loathe society, leading me to contemplate revenge”.
Discussion
In summary, this study utilized a phenomenological research approach to conduct in-depth interviews with WLWHA. It provided a distinctive perspective on their encounters with stigma, their responses to stigma, and the coping strategies they employ.
Gender-Based HIV-Related Stigma Interventions are Vital in Addressing the Gender-Specific Consequences of the AIDS Epidemic and Mitigating “Moral” Barriers to Women’s Well-Being
This study identified five facets of stigma experienced by WLWHA, including family role (wife/mother/grandmother) collapse and disgusted by family, feelings of resignation in being shunned by others, helplessness due to social exclusion, grief at being devaluated, and resentment for experiencing injustice. The mentioned themes in results section occurred closely intertwined with traditional Chinese culture and the roles of women within the family in China.
Firstly, Chinese society places a strong emphasis on family, and personal experiences are often closely connected to the family unit. As a result, HIV-related stigma, such as being labeled as “infectious”, “incurable”, or “immoral”, impacts not only WLWHA but also their entire families.22 Moral judgments made by the Chinese public regarding WLWHA might reduce the public willingness to provide support to those affected and their families.23 Furthermore, the stoicism and introversion commonly found in Chinese women may act as barriers to seeking assistance from sources beyond their family, like friends and colleagues.24 This reluctance is often motivated by the desire to shield themselves and their families from heightened stigmatization, which ultimately diminishes the social support accessible to them.
Secondly, women traditionally bear the primary caregiving responsibilities within Chinese families. Upon contracting HIV, women face a challenging conflict between their declining health and their gender-based caregiving duties. They may be willing to continue fulfilling their caregiving “responsibilities”, but family members may prevent them from doing so due to concerns about infection. This role collapse might compound their perceived stigma.25 Moreover, the illness can reduce their ability to provide care to family members, placing dependent children and/or the elderly in a vulnerable situation. This, in turn, exacerbates the moral burden on WLWHA.22 The increased household expenses due to their own illnesses further complicate their self-perception.22
To prevent further exacerbation of the perceived stigma experienced by WLWHA, it is imperative to address socioeconomic conditions at a macrostructural level. This can be achieved through the equitable distribution of care resources and the development of gender-sensitive welfare policies. These measures provide the foundation for challenging and transforming the gender-based inequities impacting “womanhood”. Much of the existing intervention research on HIV-related stigma has been conducted outside of China. However, the concept of HIV-related stigma is closely intertwined with culture. WLWHA in different countries may have distinct experiences of perceived stigma due to varying cultural attributes. Therefore, it is imperative to continue developing localized interventions in China. Misir observed that many interventions tend to overlook the resilience and active capacity of PLWHA to respond positively to stigma.26 They are often unfairly perceived as passive and unable to influence their circumstances. Similar to the women in our study, they aspire to have a voice, seek recognition from the state, access social support, and enhance their adaptive coping skills (Participant D5). In the long term, by positively impacting stigma, we believe that this intervention has the potential to enhance medication adherence, promote safer sexual behaviors, and improve the physical and psychosocial well-being of HIV-infected women affected by stigma.
Assist WLWHA in Evaluating Ineffective Coping Mechanisms for Stigma and Offer Guidance on Adopting More Appropriate Strategies
This study also revealed that WLWHA patients employed various strategies when facing stigma, including concealing their condition, social avoidance, and even attempting to retaliate against society. Healthcare professionals should play the crucial role in assisting WLWHA in evaluating the appropriateness of these responses.
Concealing one’s condition, while it may temporarily shield WLWHA from prejudice and discrimination, can also lead to heightened psychological pressure, loneliness, social anxiety, and delayed treatment.27 Healthcare professionals should guide patients to make informed decisions about disclosing their condition to trusted individuals to access emotional and social support. Simultaneously, WLWHA should be educated on seeking timely and appropriate medical care at infectious disease healthcare institutions.
Blake et al found that stigma mainly existed in the interpersonal domain, which was consistent with this study.28 Social avoidance, although an understandable reaction to stigma, can further diminish patients’ social interaction skills and self-esteem.29 Healthcare providers could equip patients with interpersonal communication skills, problem-solving strategies, and psychological guidance to encourage social integration, thereby enhancing their social adaptive functioning. In addition, healthcare providers could offer some online platforms for WLWHA. The full-time and spatial characteristics of the online platform can establish a relatively uninterrupted and secure safety ecosystem for WLWHA. By addressing the hesitation of WLWHA to disconnect from offline social constraints, WLWHA sharing the same HIV/AIDS symbol can engage in meaningful interactions, express themselves openly, and actively listen to one another within this continuous and stable ecosystem. This facilitates the effective exchange of beliefs and attitudes related to their shared status, ultimately enabling the collective reconstruction of a new sense of stigma.
Instances of retaliation against society, can lead to delinquent behavior among WLWHA patients. It has been reported that public misunderstanding, prejudice and discrimination against AIDS are one of the major causes of delinquent behavior among WLWHA patients.30 A significant portion of the incidents of delinquency by AIDS patients is due to stigma, which is consistent with the results of this study.31 Choosing to retaliate against the society will inevitably cause the occurrence of delinquent and criminal incidents among WLWHA. On the one hand, patients and their families have to bear criminal and civil liabilities. On the other hand, it is more unfavorable to improve the social public’s avoidance, rejection and discriminatory attitudes toward them. Therefore, for the patients’ psychological tendency of resentment and retaliation due to social stigma, healthcare professionals should promptly identify and address patients’ tendencies towards resentment and retaliation. Education on legal matters can help patients understand the consequences of such actions and guide them towards constructive channels for addressing stigma, defending their rights, and maintaining a positive outlook on life.
Conclusion
This study described the experience of stigma and coping strategies from the perspective of WLWHA. The local interventions are yet to be further studied in China. In the face of the tremendous psychological pressure and social life difficulties brought by social stigma to patients, it is necessary for infectious disease healthcare professionals to conduct targeted research on this issue to eliminate or alleviate social stigma. Healthcare professionals are suggested to provide WLWHA with effective emotional support and guidance on coping with stigma. The study highlighted the stigma faced by WLWHA, providing valuable evidence for policymakers. The recommendations underscore the importance of developing and enhancing services that address not only the physical but also the psychological needs of WLWHA.
Acknowledgments
We extend our heartfelt gratitude to those who generously provided research facilities and offered invaluable program guidance and human support for this project: Kou Jianqiong (Yunnan Provincial Hospital of Infectious Disease); Caiyun Wei (The Fourth People’s Hospital of Nanning). We are also appreciative of those who actively participated in the recruitment of this project: Meiyan Sun (Shanghai Public Health Clinical Center); Fang Zhang and Guotao Lu (School of Nursing Dali University); Xiaoyi Zhang (The People’s Hospital of Dali Bai Autonomous Prefecture); Meixiang Lu and Jingping Huang (The Fourth People’s Hospital of Nanning).
An unauthorized version of the Chinese MMSE was used by the study team, and this issue was rectified between the authors and PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Funding
We would like to thank the Fudan-Fosun Nursing Research Fund (FNF202303); and National Natural Science Foundation of China (71673057); and the China Scholarship Council (202306100228).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heymann DL, Prentice T, Reinders LT. The world health report 2007: a safer future: global public health security in the 21st century. World Health Organization; 2007.
2. Sari T, Jannah SR, Asniar, et al. Stigma experienced by women living with HIV/AIDS in Aceh province: a phenomenological study. Enfermería Clínica. 2022;32:S62–S65.
3. UNAIDS. Global HIV & AIDS statistics — fact sheet [Internet]. Geneva, Switzerland: The Joint United Nations Programme on HIV/AIDS; 2023. Available from: https://www.unaids.org/en/resources/fact-sheet.
4. Halimatusa’diyah I. Moral injury and the struggle for recognition of women living with HIV/AIDS in Indonesia. Sociol Int J. 2019;34(6):696–715. doi:10.1177/0268580919865099
5. Osório D, Munyangaju I, Nacarapa E, et al. Mother-to-child transmission of HIV infection and its associated factors in the district of Bilene, Gaza Province-Mozambique. PLoS One. 2021;16(12):e0260941. doi:10.1371/journal.pone.0260941
6. Bassett MT, Mhloyi M. Women and AIDS in Zimbabwe: the making of an epidemic. In: Women’s Health, Politics, and Power. Routledge; 1994.
7. Valeria J, Surilena S, Budiman Y, Djauzi S, Indah H. Family support is not a risk factor of negative self-esteem in HIV/AIDS women. Universa Med. 2016;34(1):61–67. doi:10.18051/UnivMed.2015.v34.61-67
8. Songwathana P, Manderson L. Perceptions of HIV/AIDS and caring for people with terminal AIDS in southern Thailand. AIDS Care. 1998;10(2):155–165. doi:10.1080/09540129850124262
9. Ho SS, Holloway A. The impact of HIV-related stigma on the lives of HIV-positive women: an integrated literature review. J Clin Nurs. 2016;25(1–2):8–19. doi:10.1111/jocn.12938
10. Mwabenga BK Effectiveness of HIV/AIDS social support coping skill to PLWHA in Kinondoni Municipality, Dar Es Salaam: A case study of Mwananyamala hospital. Doctoral dissertation. The Open University of Tanzania; 2019.
11. Sommer SB, Barroso JV, Bass SB, et al. Barriers and facilitators to engagement in care and medication adherence for women living with HIV in the Southern United States. AIDS Care. 2023;36(1):1–9.
12. Barroso J, Relf MV, Williams MS, et al. A randomized controlled trial of the efficacy of a stigma reduction intervention for HIV-infected women in the deep south. AIDS Patient Care STDs. 2014;28(9):489–498. doi:10.1089/apc.2014.0014
13. Batson CD, Polycarpou MR, Harmon-Jones E, et al. Empathy and attitudes: can feeling for a member of a stigmatized group improve feelings toward the group? J Pers Soc Psychol. 1997;72(1):105–118. doi:10.1037/0022-3514.72.1.105
14. Rao D, Desmond M, Andrasik M, et al. Feasibility, acceptability, and preliminary efficacy of the unity workshop: an internalized stigma reduction intervention for African American women living with HIV. AIDS Patient Care STDs. 2012;26(10):614–620. doi:10.1089/apc.2012.0106
15. Echenique M, Illa L, Saint-Jean G, et al. Impact of a secondary prevention intervention among HIV-positive older women. AIDS Care. 2013;25(4):443–446. doi:10.1080/09540121.2012.712666
16. Peltzer K, Babayigit S, Rodriguez VJ, et al. Effect of a multicomponent behavioural PMTCT cluster randomised controlled trial on HIV stigma reduction among perinatal HIV positive women in Mpumalanga province, South Africa. SAHARA J. 2018;15(1):80–88. doi:10.1080/17290376.2018.1510787
17. Dewangan A, Singh J, Kumar D, et al. Disseminated cryptococcosis in Idiopathic CD4+ lymphocytopenia. Infect Disord Drug Targets. 2023;23(1):2–5.
18. Katzman R, Zhang MY, Ouang YQ, et al. A Chinese version of the mini-mental state examination: impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol. 1988;41(10):971–978. doi:10.1016/0895-4356(88)90034-0
19. Moura COD, Silva ÍR, Silva TPD, et al. Methodological path to reach the degree of saturation in qualitative research: grounded theory. Rev Bras Enferm. 2022;75(2):e20201379. doi:10.1590/0034-7167-2020-1379
20. Colaizzi P. Psychological research as a phenomenologist views it. In: Valle R, King M, editors. Existential Phenomenological Alternatives for Psychology. New York: Open University Press; 1978.
21. Lincoln YS, Guba EG Naturalistic inquiry [Internet]. sage; 1985 [cited 2023 Sep 30]. Available from: https://books.google.com/books?hl=en&lr=&id=2oA9aWlNeooC&oi=fnd&pg=PA7&dq=Lincoln+Y%EF%BC%8CGuba+E.+Naturalistic+inquiry&ots=0uszQbQcwn&sig=6iEJmotlXy_SRBK4dYRkn8gDRec.
22. Xu JF, Ming ZQ, Zhang YQ, et al. Family support, discrimination, and quality of life among ART-treated HIV-infected patients: a two-year study in China. Infect Dis Poverty. 2017;6(1):152. doi:10.1186/s40249-017-0364-5
23. Zhou YR. Endangered womanhood: women’s experiences with HIV/AIDS in China. Qual Health Res. 2008;18(8):1115–1126. doi:10.1177/1049732308319924
24. Du A, Zhang F, Chen X, et al. Analysis of psychological characteristics of aggressive behavior and its influencing factors among middle school students. Chin J Sch Doc. 2019;33(8):606–610.
25. Powell I The effects of stigma against HIV and tuberculosis on patient mental health and healthcare-seeking behavior in dharamshala [Internet]; 2023. Available from: https://digitalcollections.sit.edu/isp_collection/3655.
26. Misir P. Structuration theory: a conceptual framework for HIV/AIDS stigma. J Int Assoc Provid AIDS Care. 2015;14(4):328–334. doi:10.1177/2325957412463072
27. Tatham CD. Life and Love Under Criminalization: The Experiences of People Living with HIV in Canada. University of Toronto (Canada); 2023.
28. Blake HC, Turan JM, Atkins G, et al. Interpersonal mechanisms contributing to the association between HIV-related internalized stigma and medication adherence. AIDS Behav. 2017;21(1):238–247. doi:10.1007/s10461-016-1320-2
29. Liu XH, Zhong JD, Zhang JE, et al. Stigma and its correlates in people living with lung cancer: a cross‐sectional study from China. Psycho-Oncology. 2020;29(2):287–293. doi:10.1002/pon.5245
30. Bogart LM, Cowgill BO, Kennedy D, et al. HIV-related stigma among people with HIV and their families: a qualitative analysis. AIDS Behav. 2008;12(2):244–254. doi:10.1007/s10461-007-9231-x
31. Yan S, Lei X, Zhou L. Risk control countermeasures in HIV occupational exposure for healthcare workers and police officers. Chin Stud. 2022;11(3):185–195. doi:10.4236/chnstd.2022.113015
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Qualitative Study on the Experience of Assisted Reproductive Technology in Women with Dyspareunia
Wei Q, Wang Z, He Y, Hong X, Shen X, Zhang S
International Journal of Women's Health 2024, 16:543-553
Published Date: 26 March 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025