Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 14
Exploring Spiritual and Religious Coping Among PLHIV in a Malaysian Muslim Community: A Qualitative Study
Authors Zainal-Abidin ANI ![]() , Ariffin F, Badlishah-Sham SF
, Ariffin F, Badlishah-Sham SF ![]() , Razali S
, Razali S
Received 20 April 2022
Accepted for publication 20 August 2022
Published 31 August 2022 Volume 2022:14 Pages 409—422
DOI https://doi.org/10.2147/HIV.S371554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Aiza Nur Izdihar Zainal-Abidin,1 Farnaza Ariffin,1,2 Siti Fatimah Badlishah-Sham,1 Salmi Razali2,3
1Department of Primary Care Medicine, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh, Selangor, Malaysia; 2Maternofoetal and Embryology Research Group (MatE), Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh, Selangor, Malaysia; 3Department of Psychiatry, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh, Selangor, Malaysia
Correspondence: Aiza Nur Izdihar Zainal-Abidin, Department of Primary Care Medicine, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh, Selangor, Malaysia, Tel +6019 3308095, Fax +603 61268888, Email [email protected]
Purpose: Increase in life expectancy of PLHIV has brought new challenges especially for young Malay Muslim men who have sex with men (MSM) in Malaysia. This country has strong religious and cultural roots that may pose as additional stigma and discrimination in the lives of PLHIV. Therefore, coping skills among PLHIV is important. Theories on coping strategies has shown that spiritual and religion are one aspect of emotional focused coping. The aim of this study is to explore the views on spiritual and religious (S/R) coping among Malay Muslim MSMs.
Patients and Methods: This was a qualitative study using in-depth interview. Eligible participants were recruited using purposive and snowballing sampling techniques via NGOs and online flyers. The narrative inquiry approach was used to understand the lived experiences of PLHIV and their coping strategies, particularly using S/R coping. The interviews were transcribed verbatim and analysed using Qualitative Data Analysis (QDA) Miner. The data was analysed using thematic analysis.
Results: Interviews with seven participants yielded four themes. Ambivalence towards religion was experienced by participants at some point following their diagnosis. Using S/R as a form of self-reflection was identified. Having positive religious support from family or NGOs helped some participants to embrace religious coping rather than to avoid it, and relationship with God was an important aspect of religious coping.
Conclusion: Spirituality and religiosity can be a form of positive coping for PLHIV. This study suggests the need for S/R guidance as well as positive support from healthcare professionals and religious-based organizations for PLHIV. This can have positive effects towards handling of the condition, adherence to treatment and health outcomes.
Keywords: spiritual, religious, coping, PLHIV, MSM
Introduction
Coping is the process of executing the response towards stress. The conceptual analysis of stress and coping introduced by Lazarus in 1966, explained that stress involves three processes starting with a perceived threat to oneself, followed by the thought process of a response to the threat and finally, coping is the process of executing that response.1 Previous scholarly works1,2 have divided coping strategies into problem-focused coping, emotion-focused coping, adaptive coping and dysfunctional coping. Most stresses will elicit a mixture of all types of coping, problem-focused coping tend to predominate when a person feels that a direct action can be taken to solve the problem. However, when the problem is enduring, emotion-focused coping is necessary to handle the problem.1,3
People living with HIV (PLHIV) have unique stressors that require good coping skills. Coping is fundamental to lessen the impacts and difficulties faced by PLHIV.1,4,5 In Malaysia, the landscape of HIV transmission has changed over the years. Before 2011, HIV transmission was mainly via intravenous drug use (IVDU). From 2011 onwards, HIV transmission is via sexual intercourse and specifically, among men who have sex with men (MSM),6 malay and are young adults aged between 20 to 39 years old. It was estimated that in 2018, more than 70% of HIV new infections were within this group and are projected to be the front-runner of the HIV epidemic in the year 2030.7 These young populations have higher vulnerability to transmission of HIV attributed by numerous factors such as substance abuse, low rates of condom use, low rates of testing and promiscuity. Survey has also observed prominent stigma, discrimination and violence among them probably due to lack of knowledge about HIV causing them to remain hidden from health and support services.7
Coping is even more challenging when they are at their most productive age, and MSM living in Malaysia, a country with strong religious and traditional roots. The Malaysian population consist of two-thirds Malay Muslim8 and the society are heavily influenced by cultural, religious backgrounds and expectations from family and society.9 On top of that, both criminal law and Syariah law (Islam legal system) criminalize homosexuality and other perceived indecent sexual behavior.10,11
Life expectancy for PLHIV has improved greatly since the introduction of antiretroviral therapy in 1995. Consequently, PLHIV live longer, are asymptomatic, and can contribute towards society in terms of education, social interaction, and work.12,13 Young adults PLHIV may face typical challenges for example they maybe in education or early stages of their career. In addition, they have further stressors in the form of stigma and discrimination.14 The stigma and discrimination may arise from family members, the workplace, healthcare professionals, religious and cultural perceptions, and the judiciary system. Studies have shown that bias and prejudice attitudes towards PLHIV are still present among healthcare professionals and can create a barrier for optimum HIV prevention, treatment, and care.14–17 There is also an interrelation between stigma, disease disclosure, coping, and treatment adherence.18
The Lazarus model1 that was improvised by Carver2 shows that PLHIV often employ a more emotion-focused coping strategy such as by avoidance, positive reappraisal or via social support.4,5,19 However, living within a society with strong religious and traditional values, can spirituality and religion be a form of coping mechanism rather than an additional stressor? Spirituality can be defined as an aspect of humanity that refers to the way individuals seek and express meaning and purpose, and the way they experience their connectedness to the moment, to self, to others, to nature, and to the significant or sacred.20 The power of spirituality has been found to help patients with chronic illness or during end-of-life care.21 Health care providers have acknowledged the role of spirituality as a significant influence on an individual’s ability to cope.21 Religion on the other hand is a spirituality that is shared by a group of people, often with a common set of beliefs and practices. Religious coping is defined as religiously framed cognitive, emotional or behavioral responses to stress, encompassing multiple methods and purpose as well as positive and negative dimensions.22 Koenig23 explained that “spiritual-religious coping is the use of religious beliefs, attitudes or practices to reduce the emotional distress caused by stressful events of life, such as loss or change, which gives suffering meaning and makes it more bearable”. In exploring use of Islamic religious approach, studies have explored Muslim transgender issues and the use of spirituality and religion, in this case Islam, as a method of coping.24,25 From the positive side, religion helps with acceptance, improving health outcomes and overall quality of life.18,26,27 On the contrary, those who adopt negative religious coping such as believing HIV is a punishment from God related to certain high-risk sexual behaviors, can interfere with their health status.18,28,29 Practicing religion and spirituality have been accepted by experts as parts of coping strategies.1,2
There is scarce information about the lived experiences of Muslim PLHIV in Malaysia and with regard to the role of spiritual or religious (S/R) coping. Nevertheless, understanding how they “turn to religion” is still under-researched. PLHIV have little opportunities to voice out their feelings especially with regard to their views on religion and spirituality and whether it can be a positive coping strategy for them. It is important to explore and gather information from PLHIV themselves. This will aid healthcare providers to understand them better and to identify appropriate interventions that may include S/R coping skills to deal with stressors. The aim of this study is to explore the role of S/R coping among Malay Muslim MSMs.
Methods
Study Design
In this qualitative study, participants were recruited via two non-governmental organization (NGO) based in Klang Valley which provided community service and support for PLHIVs as well as those at high risk of developing HIV/AIDS. The initial study design was to recruit from infectious disease centers with HIV clinics. This would have provided a wider range of coping skills from PLHIV at different stages of their condition and treatment. Unfortunately, due to the Covid-19 pandemic, the recruitment had to be adapted to include only those who were stable and healthy on treatment. Therefore, the NGOs were approached and willing to cooperate with the study.
Study Participants
The study participants were PLHIV. The inclusion criteria were men aged 20 to 39 years old, Muslim, contacted HIV through sexual intercourse with men (MSM) and has been diagnosed with HIV for at least the last three months. The 20 to 39 years old group was selected because HIV transmission via sexual intercourse is largely from this age group.7 The choice of participants who have been diagnosed for at least 3 months was made because one would then have gone through enough time to try out several coping strategies.
Participant Recruitment
Method of recruitment were via purposive and snowballing technique. Purposive refers to a selection of participants based on their capacity to provide richly textured information relevant to the subject to be explored.30 This method is typical for qualitative studies. Snowballing refers to identification of participants through suggestions made by initial contacts. The NGOs were given an online flyer to distribute among their members. Three of the participants contacted the researcher via WhatsApp after receiving the flyers. Another four participants were suggested by the NGO with their permission. The researcher presented herself as a postgraduate student doing research on HIV and in each case, the researcher screened the potential participants for their eligibility through WhatsApp chats. All of the contacted participants were eligible and chose to participate in the study. An agreed date, time and venue for the interviews were arranged.
Data Collection
The in-depth interviews were conducted from July 2020 until May 2021. The in-depth interview was conducted because a one-to-one interview allows a more comfortable atmosphere for the participants. It is also deemed more appropriate compared to a focus group considering the sensitivity of the subjects, the differences in their experiences and coping mechanisms.31,32
Those who agreed to participate signed a consent form and proceeded to arrange for a face-to-face interview with strict Covid-19 standard operating procedure (SOP). The researcher informed that their participation is voluntary, and they were then briefed individually on the purpose and benefits of the research and the assurance of confidentiality of their participation and information shared. The participants provided informed consent for their quotes to be published with their personal details to be anonymous. They were also told that the interview will be audio recorded and that they can withdraw from participating at any point of time during the interview. They were then given consent form to be signed as proof of willingness to participate.
The in-depth interview using semi-structured question guide was conducted in a private discussion or consultation room, either at the researcher’s university or at one of the NGOs offices. One researcher who was trained in qualitative interview conducted all the interviews to ensure standardization. The semi-structured questions were conceptualized, formulated and finalized by the research team and approved by the ethics committee. Interviews were conducted with the presence of a note-taker, whose role is to observe and note the actions, emotional responses, facial expressions of both participant and researcher, and to give feed back to the researcher on any possible bias, positive or negative reactions from the researcher or participant. The interviews were audio-recorded and were transcribed verbatim. Each interview session took approximately 90 minutes.
At the beginning of the session, the researcher collected basic socio-demographic data of the participant. As an icebreaker and to build rapport, the participant was asked to start the opening plot by asking them to relate the story that signify them. Subsequently, the researcher guided the participant to disclose more in terms of their coping strategies. The interview protocol was based on the S/R coping strategies developed by Carver et al.2 The coping mechanism maybe problem-focused (such as active coping, planning, suppression of competing activities, restraint coping and instrumental social support), emotion-focused (includes emotional social support, positive reinforcement, acceptance, turning to religion, and humour) or dysfunctional coping (venting of emotions, behavioural or mental disengagement, alcohol-drug use and denial).2
In eliciting their coping strategies, the questions are designed as open-ended to allow the participants to freely share on whatever strategies that they use. The questions consist of four primary open-ended questions with multiple probing questions under each primary question. The interviewer started the interview with open-ended questions, such as “Could you please share with me your story of how you experience HIV?” and “Could you share with me, how do you cope with any events in your life? Before and after being diagnosed”. Probes were used as needed and occasionally participants were asked to elaborate more. Since religious practice among PLHIV can be a sensitive issue, it was probed only when they mentioned anything related to S/R coping cues. If they did not mention anything related to this, the interviewer will probe with direct questions regarding their views on S/R coping. If the participants gave cues on matters related to religion or spirituality, the interviewer will then focus on S/R coping with questions such as, “What is your opinion on the religious way of coping with events in your life?”. To encourage the participants to provide more explanation, questions such as “Is there anything that you want to say?” were asked at the end of the interview.
During the data collection period, the study was challenged by the increasing numbers of COVID-19 cases and lockdowns. The researcher observed the data saturation throughout data collection and transcription, and it was discovered that data saturation occurred at participant six (P6). We proceeded with another participant however, the study had to be halted due to the second wave of COVID-19 infections that brought stricter lockdowns, and we were not able to obtain ethical approval to conduct the interviews online. COVID-19 posed serious challenges in this study especially since PLHIV were a vulnerable group and were susceptible in contracting serious complications if exposed to COVID-19 infection. Hence, repeated interviews were not carried out, but the researcher maintained in touch with the participants for further clarification or to obtain missing information from them.
Data Analysis
The interview was transcribed verbatim after each interview. The transcription was in the language used by the participants, a mix between the Malay language and the English language. The transcribed interviews were analyzed using the Qualitative Data Analysis (QDA) Miner Lite software. Content analysis was conducted for the coding of the data. The first few interviews guided the researcher through the open coding process to determine the codes and this also allowed further refinement of the interview questions. Codes were determined based on what was mentioned verbally and directly or something that was inferred from phrases mentioned by the participants.
Data from each interview was fragmented and labelled to enable the researcher to continuously compare similar events in the data, a process referred to as constant comparative analysis. In other words, information that has been obtained in completed interviews was coded and refined simultaneously as new data from the subsequent interviews were gathered. Similar experiences shared were labelled with a specific code. This open coding process avoids preconceived notions and minimize biases regarding the research. The co-researchers were briefed on the codes developed for their opinions and agreement.
The next stage in the analysis requires axial coding in which the codes were revised and grouped into categories. Categories were created based on an existing code, or a new more abstract category was developed that encompasses a few different codes. Some codes were found to be redundant, thus a new code was formed. Some codes were merged and renamed. The coded data was further explored to identify recurring themes, formed through narrative thematic analysis.33 The data analysis was shared with the co-researchers who checked the plausibility of the data interpretation and ensured that the data analysis was systematic and verifiable. The research team had several face-to-face and online meetings to discuss the data interpretations and the finalized thematic analysis. Disagreements and discrepancies between code labels or identification of phrases according to codes were deliberated and resolved via group discussions. The thematic analysis was conducted together and verified by the research team. The researchers checked the final data interpretation. Figure 1 portrays the entire research process.
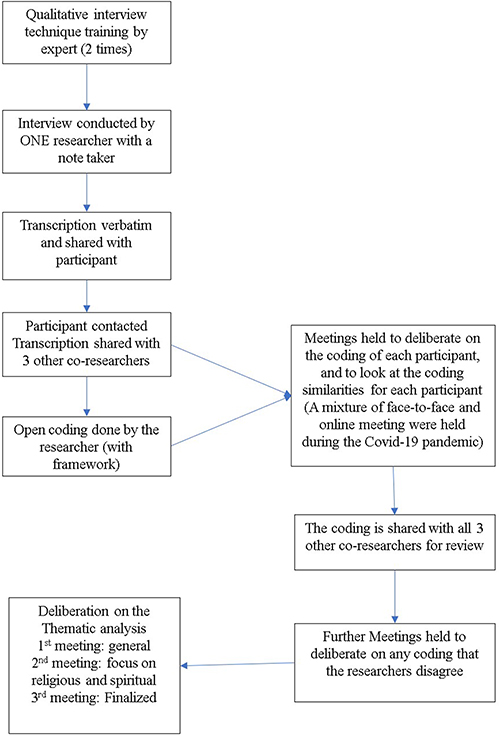 |
Figure 1 Flow chart of the interview process, transcription, data analysis (coding and thematic analysis). |
To ensure validity of the interview and data analysis, the process must be credible.34 In this study, credibility was employed using investigator triangulation and member checking to ensure the validity of the interview process. There are four types of triangulations;35,36 method, investigator, theory and data source triangulation. In this study, investigator triangulation was done which involves seeking feedbacks from the co-researchers on each process of data collection and analysis. Member checking, or referred to as participant or respondent validation, is a method for exploring the credibility and validation of results. It requires returning the data or results to research participants to check for accuracy and resonance with their experiences and is an important step to ensure how accurate the respondent’s realities were represented in the final account.34 The full transcription was sent to the participants through WhatsApp messaging immediately after the transcriptions were done. All the participants acknowledged and agreed with the transcriptions without giving further comments. In the context of this research, member checking was only done to get confirmation by participants on the preciseness of what was transcribed. The codes and themes that were developed during the analysis stage were not shared with them. Several researchers had raised that it may be an attractive idea to do so but it is arguably not a verification strategy. Methodologists including Hammersley37 and Morse38 indicated that if verification is for participants to judge that the analysis is correct, it can actually be more often a threat to validity.
Results
A total of seven participants (P1-P7) with a mean age of 30.57 years were interviewed. They all belonged to the Malay ethnicity, and were all Muslims. Table 1 describes the background sociodemographic characteristics of the participants.
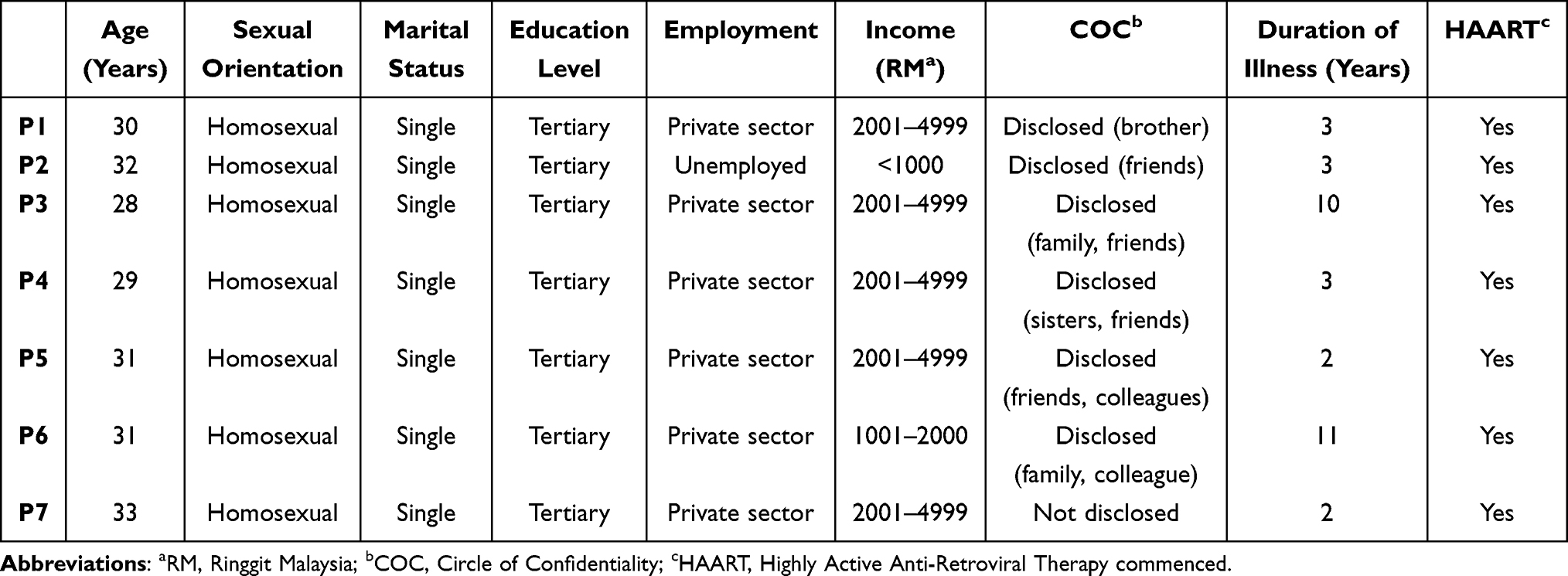 |
Table 1 Sociodemographic Data of Participants (n=7) |
The participants, when invited to share about themselves or their stories, narrated different opening plots based on what signifies them. We extracted three codes in the opening plots which are job background, the plot of their diagnosis of HIV, and acknowledging that HIV is their turning point. Table 2 describes the narrative summary of the lived experiences shared by the participants.
 |
Table 2 The Narrative Summary of the Lived Experiences |
The Themes
Four main themes emerged from the analysis, and they were ambivalence towards the religion, breaking stigma through self-reflection, the need of support for positive guidance and religion and relationship with God as part of coping. Table 3 shows the themes and sub-themes that emerged from the in-depth interviews.
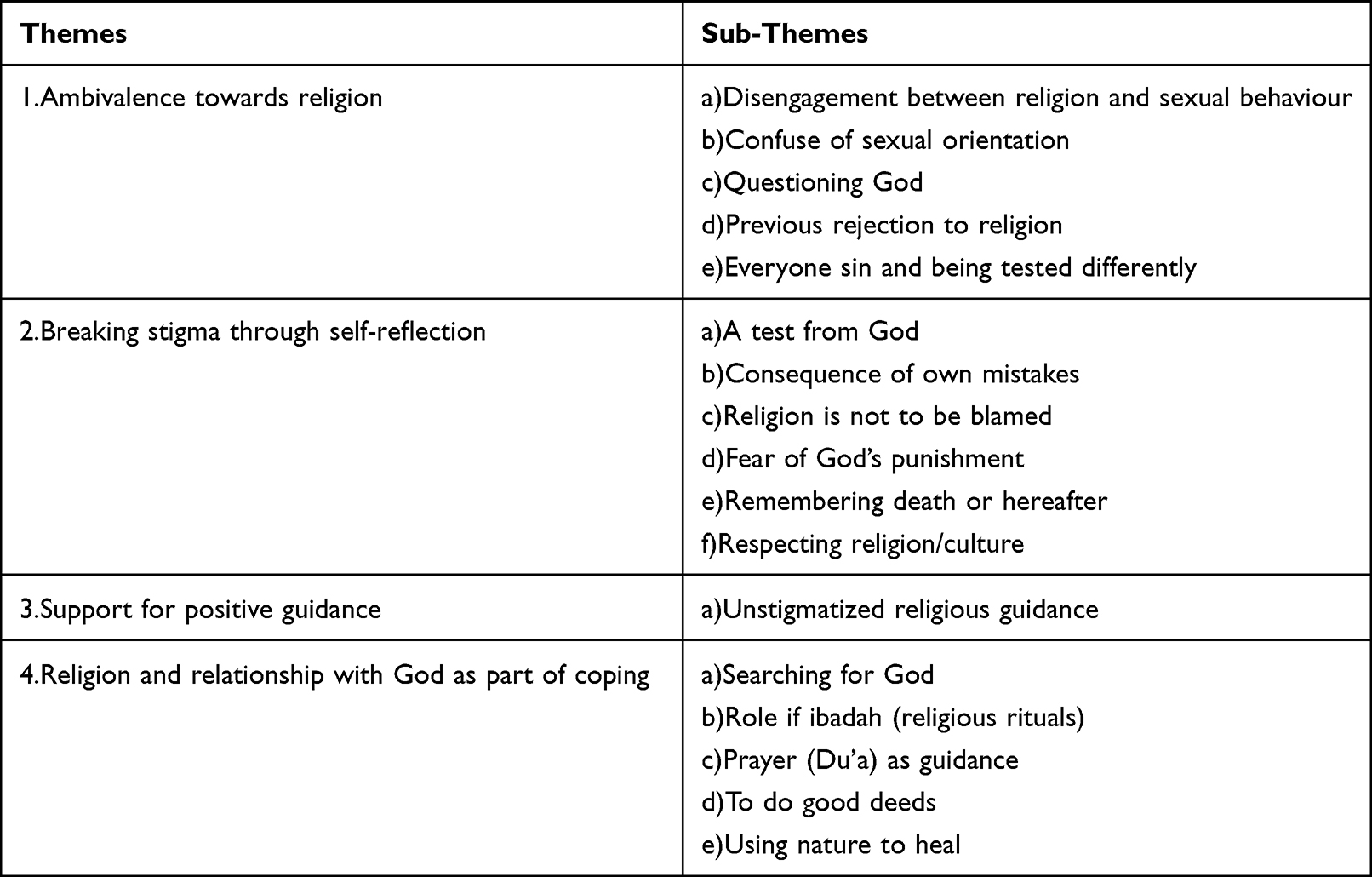 |
Table 3 Themes and Sub-Themes of R/S Coping of Participants |
Ambivalence Towards Religion
All participants described their uncertainties and feelings of ambivalence towards religion at some point following their HIV diagnosis. Although some of the participants have faith that religion plays a role in self-restraint and sexual abstinence, most agreed that they felt a disengagement between religion and sexual behavior. This is a common perception for MSMs and is supported by five of the participants, including Mr. P5,
If you see it roughly, actually it (the religion) aids to improve, meaning self-improvement in the sense of spirituality, for a better soul. But to be straight, it’s unlikely. [P5]
During the stages of grief of the participants, some of them portrayed uncertainty and feeling doubt towards the religion. Questioning God, for example, can be part of the cycle before reaching acceptance. Mr. P3 who was doubtful and denied treatment for three years after being diagnosed stated that,
When we relate to (life) before being diagnosed, we will question why … why me? Why that moment? And many other things. Because, first, I am disputing why I was born and suddenly been flicked the instinct to like men. Second, to be diagnosed. These two factors. Once in a while, why aren’t we born as normal human beings?. [P3]
Being ambivalent towards religion also made a participant to reminisce his previous rejection of the religion and it was a decision that he regretted, Mr. P1 said he would have responded to the “call of religion” earlier if he knew he will become like this,
My mom has gone for Hajj, to umrah. She asked me to come along, to go together, saying it’s okay, I am paying for everything. But at that time, I was not ready yet. Now that I have gotten this, I regret not going afore. [P1]
However, another participant has a dissimilar opinion about religious practice. Mr. P2 for instance, who has support from the LGBT community has some doubts toward religious rituals, believing that worshipping is not the only part of the conduct of the religion.
I don’t go, like, let’s go for prayer, do sunnah prayer or anything. I’m not that level yet … at the moment Allah has provided that realization, is also, a sustenance. [P2]
He feels that conforming with others who were more liberal in gender expression and sexual practice became the medium to reduce the anxiety of having done a great sin.
Mr. P2 has a strong opinion that everyone is a sinner and being a PLHIV did not make him any different or a worse sinner, he is just being tested differently.
We are all tested with our difficulties. If you look at the list of major sins, right, it’s not just homosexuality. For instance, you take orphans’ properties. So, like we are all sinner. [P2]
Breaking Stigma Through Self-Reflection
Most participants believed that being aware of themselves and looking back at their life can be a form of self-reflection to alleviate internal stigma. As with other participants, Mr. P2 who faced various difficulties during his childhood and has many uncertainties about religion however, reflected that getting HIV is a form of test from God. “First, Allah does not charge a soul except within its capacity, and second, everything happens for a reason” (P2).
Other participants self-reflected by blaming their own mistakes. Mr. P7 has good active coping whereby he proceeded with HIV treatment without delay after he was admitted for pulmonary tuberculosis. He stated, “seriously, I don’t know who to blame. So, I blame myself because I created the problem” (P7). The participants mostly believed that no one should be responsible for what had happened to them, and they hold themselves accountable regardless of their religious beliefs. Religion is not something to be blamed and this is advocated by a participant,
I don’t want to be a fitnah to religion. So, what I did, it’s because of me. It’s not because of Islam. Islam has its framework. It was my fault, I did it because I wanted to. [P2]
Furthermore, from the perspective of some of the participants, religion can help them to avoid doing more sin and functions as self-restraint. They can do that by remembering death or hereafter and fear of God’s punishment. “This world is not a place for us to live, but a place for us to die. The eternal place for us is the akhirah” (P4). Moreover, Mr. P6 who joined an NGO as a form of charity to help other MSMs confessed that it is a challenging task when some of the homosexual men that he helps request to have sexual contact with him. However, he can reject them, “It means that it is sinful … it means homosexuality is a great sin, hence I avoid it” (P6)
Finally, Mr. P2 albeit having acquaintances from the LGBT community, he opposes the opinion of openly promoting the lifestyle. He agrees that respecting the religion is also necessary as a part of being Muslim,
well, because you are loud, so people think, the rest is like you. No. I hate that kind of people. Like if you’re fighting for human rights outside Malaysia, go ahead. This is Malaysia, you have to respect the foundation of Malaysia- we have religion, and the culture. [P2]
Support for Positive Guidance
The participants expressed having positive guidance and support as important, such as family members, friends, and religious teachers. When seeking help from another person for religious guidance, the participants highlighted that sincere help without bias, prejudice, or stigma from the religious person is more acceptable and fulfilling. For example, Mr. P3 who suffered from depression for three years confessed that positive guidance depends on the person who advocates them. He has found professional help to discuss religious and spiritual issues in the religious-based-NGO where he works,
The teachers who understand us are there too, so … any questions that we ask, they will help to answer. We feel reassured … Good because the responses are not discriminating of stigmatize us. [P3]
Other participants sought support from their family members to guide them in practicing more positive lifestyles and religious coping. For example, Mr. P1 was fully supported by his brother who encouraged him to have good health-seeking behavior and adopt positive religious coping strategies such as improving his ibadah and believing in the power of prayers. Similarly, Mr. P4 has his sister while others have friends and colleagues as their trusted confidants.
It was during fasting month, I remember I read Qur’an and all, I was looking for peace but I was not peaceful at the time. Even though I prayed. Maybe at the time, I didn’t have anyone to talk to.
For Mr P4, having someone to confide in and to receive that guidance is important.
Seeking peace and tranquility while struggling with HIV comes also from their involvement with non-governmental organizations (NGOs). For P3, the support from NGO with religious guidance is important, he said “The ustaz who understand us is there like … whatever question, so with me, when we ask, the ustaz can help give answers. So, we feel relieved.”
Religion as Part of Coping
Many of the participants believed that an important aspect of religious coping is the relationship with God. While describing their relationship with God, a few of the participants described that the search for God came in many ways. It was either by their effort to get near Him or by getting guidance from another person. A few who felt guilty for practicing homosexuality perceived that having been diagnosed with HIV became the main turning point to be a more religious person. For example, the early life narratives of being guilty as MSMs who was against religious teaching had turned into using religion as part of routine ways to find comfort in their lives.
This was described by Mr. P4, a nurse who described a closer relationship with God after he was first diagnosed with HIV. He described,
After I was diagnosed, I was indeed looking for God in my life. Aa … I guess, I searched for it for quite a while, I was looking for what I really want in my life. [P4]
He is currently working with a religious-based NGO and that has assisted him in his quest to get closer to God.
Well, people say the power of God is enormous. That was when I got closer to Allah, all along. Praise to Him, it’s right when people say Allah helps us a lot. If you ask me, in terms of spiritual, definitely Allah helps us a lot. In this world, there is nothing we can be proud of. Even if we have a position, or whatever it is, when we are unwell like this nothing can aid us other than Allah’s mercy. [P4]
Relationship with God is strengthened by religious practice. Religious practices were considered by all participants to be part of their spiritual needs. The rituals can be in any form, for instance in this study the participants described more towards the role of mandatory prayer itself or by reciting prayers as their guidance. Mr. P1 who found substantial emotional social support from his brother, also concluded that ibadah plays a role in his religious coping. “Prayers, you fast, recite Quran, ha all those things … to be honest when I started to do that, maybe it is one thing that makes me feel stronger” (P1). Meanwhile, Mr. P4 who acquired emotional social support from his sister, seeks enduring guidance from God through his prayers,
If we take even minimal wrong step, we can return to the previous path. That’s why, I pray Oh Allah, my lord, give me your light and your guidance, Oh Allah, please change me. [P4]
A few of the participants also suggested that doing good deeds can be part of their religious coping. Participation in active philanthropy and charity work instilled satisfaction and positive evaluation in oneself. It can help them to be closer to God or enhance their spirituality. For example, Mr. P6 who had lived a social life until he was faced with the repercussion of contracting HIV, suggested that
By doing this job (working with an NGO), I help people. It means, I feel satisfied with that I have helped and now some of my clients are already on treatment, and they get education from me. [P6]
Most of them who work with the NGOs believe that helping another person who is at risk of contracting HIV is rewarding, while others believe in charity or donation, “And now that I am like this, I like to … even if I have only one ringgit, I like to give sadaqah” (P4)
Interestingly, one of the participants, Mr. P5 he used a symbolic meaning of getting himself closer to God through nature. Right after being, he was told that he was HIV positive, he cried for a while before putting himself back together by getting inspired by the trees. He said, “I can be calm. When I cry and I think of the One who made the trees, and this is what gives me peace.” Direct preaching about religion would not go into his heart, but he will look at the trees to make sense of what has been told to him. “Hence, I interact with the trees. Trees are my source of inspiration for me to motivate myself” (P5). “To help me, Allah eases me with the greeneries” (P5).
Discussion
In this study, we extracted the perceptions related to spirituality and religion faced by Malay, Muslim MSMs as coping strategies after being diagnosed with HIV. The four themes identified gives a better understanding on how spirituality and religion can provide a positive coping mechanism among PLHIV.
The narrative of the Malay, Muslim MSMs from this study emphasized that the ambivalence of religion exists at the beginning of their lived experiences as MSMs. Hence, this reaction is normal and part of the early phase of grief and handling the diagnosis of HIV. Those who received religious support would eventually adopt religion as a coping mechanism. On the other hand, those who sought and receive support from NGOs with liberal and gender equality background would maintain ambivalence towards religion. The support system given to those MSMs and PLHIV determines the outcome of the spectrum of acceptance in adopting religious coping.
Among PLHIV, stigma can lead to denial of HIV diagnosis and poor medication adherence.18 Internalized stigma with regard to being HIV positive can make a person feel “dirty” or “worthless”.16 Therefore, breaking the stigma through self-reflection is an important aspect of coping. In this study, the participants had good self-reflection and even though some believed that HIV is a “test from God” and that “they have no one to blame but themselves”. Some even considered it a punishment from God. It is difficult to differentiate between a test from God or a divine judgement29 and is all based on the perception of the individual. However, to self-reflect is one of the spiritual foundations and an important aspect to break stigmatization.22
The majority of PLHIV in the present study received support either from family members, friends, or religious-based organizations that focus on supporting those with HIV. In Malaysia, the Malaysian AIDS Council (MAC) was established to represent and strengthen the NGOs who are directly involved with HIV/AIDS issues. Under the umbrella of MAC, there are many partner organizations from the medical industry, religious-based communities, and also legal foundations.39 Our study has shown the significant impact of religious-based NGOs on the participant’s religious coping. The participants who worked with the NGOs have positive religious coping, hence the good acceptance of the illness. This finding is supported by studies that demonstrated a better quality of life through the roles of NGOs and how religious coping positively relates to acceptance.18,40 This is because they have good ART adherence to have a near-normal life expectancy and can contribute more to society.
Positive religious coping skills identified from this study include self-reflection, support, building a strong relationship with God via contemplation and religious practices. It is demonstrated by the participants that religious coping can be a positive coping mechanism in their lives. However, in Malaysia, a question arises whether PLHIV receives the guidance for positive religious coping. Although a training manual for “HIV and Islam”41 was developed for use among religious and medical personnel, there is still a query on how much training has been conducted and implemented in medical settings. In terms of medical care, even though the first line of HIV treatment is given for free at government hospitals and clinics, only 50% of the PLHIV seek treatment. This is due to multiple factors, not only due to shame and fear of social stigma but some do not have stable jobs and frequent hospital visits can affect them financially.42,43 While only approximately half of the PLHIVs come forward for medical care and seeing healthcare professionals (HCP) regularly, many of the HCPs however are not confident to incorporate S/R coping as a more holistic patient-centered care.44 Draman24,45 has suggested a multidisciplinary approach from educational, medical and religious fields to attend to the needs of those stigmatized such as transexual in this country. From this study, we conclude that more training is needed to approach, and include marginalized communities such as MSMs and PLHIV to give them better knowledge and access to healthcare. There is a need for more support and collaboration between religious-based organizations, NGOs with our healthcare system.
Strengths and Limitations
The main limitation of this study is that due to the Covid-19 pandemic, recruitment was done among PLHIV who were stable and on treatment. They were recruited from NGOs, hence, may already have good coping skills. Therefore, the views and experiences of MSMs with HIV in other community settings may differ and limits the generalization of the findings of this study. Secondly, there may be some biases in undertaking this interview as the main interviewer (ANI) is a female, Malay, and Muslim health practitioner and may have underlying preconceptions. Finally, the Covid-19 pandemic also restricted the data collection. Despite these limitations, this study provides an important insight into the S/R coping among Malay Muslim MSMs in Malaysia.
Trustworthiness
Based on four criteria: credibility, transferability, dependability, and confirmability, a few measures were taken to enhance the rigor of this study. First, to attain credibility or confidence in the research, the interviewer ensured adequate engagement with the participants. The verbatim transcripts were read and reread to vividly describe their experiences with associated quotations and data were discussed with research team. To achieve transferability and dependability, the analysis of each case was done in-depth using above-mentioned qualitative software. Audit trails were maintained, including the original recordings and questionnaires as well as verbatim transcripts. Finally, recruitment and interviews were conducted by the same investigator, who was a postgraduate family medicine student with knowledge about HIV who had undergone special training in qualitative methods and in-depth interview skills from a PhD-trained co-supervisor with expertise in qualitative studies. Regular discussions of the details of the study process were held to ensure the confirmability of the findings.
Conclusion
Positive religious and spiritual coping have beneficial effects on PLHIV among Malay Muslim MSMs. The spectrum of spiritual and religious coping is determined by the guidance and support they receive from family members, friends and religious based NGOs or the LGBT community. Those who practiced religion had both problem-focused and emotion-focused coping strategies, specifically withdrawal from previous high-risk behavior, better self-control, and positive reappraisal. Therefore, considering this study’s results, there is a need to collaborate between religious-based organizations and health care professionals to improve care towards PLHIV.
Another interesting finding from this study is the struggle that MSMs face to restrain themselves from high-risk behaviors even after they have embraced religious coping. Islamic scholars have described “Iman”, or faith as “a knowledge in the heart, a voicing with the tongue, and an activity with the limbs”. It means, submitting the heart to Islamic faith is insufficient without expressing them by tongue and activities. Further research should explore the justification and reasons behind disengagement between religion and sexual behavior.
Ethical Considerations
This study attained ethical approval from the UiTM Research Ethics Committee (REC/670/19) and Medical Research and Ethics Committee (NMRR-19-4027-51484 (IIR)).
Acknowledgments
We would like to thank all participants involved in this study and shared their precious time and experiences with us.
Author Contributions
All authors made a significant contribution to the work reported. ANI, FA, SFB, and SR were involved in the conception, study design and execution. ANI conducted the interview ie, acquisition of data. ANI, FA, SFB, and SR were involved in analysis and interpretation. ANI drafted the manuscript. FA, SFB and SR substantially revised and critically reviewed the article. ANI, FA, SFB, and SR have agreed on the journal to which the article will be submitted, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. ANI, FA, SFB, and SR agree to take responsibility and be accountable for the contents of the article.
Funding
This study was supported by grant from the Geran Penyelidikan Khas (GPK) (600-RMC/GPK 5/3 (200/2020)). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Dr Siti Fatimah Badlishah-Sham reports grants from Universiti Teknologi MARA, during the conduct of the study. The author reports no other conflicts of interest in this work.
References
1. Folkman RS, Lazarus S, Schetter CD, DeLongis A, Gruen R. Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J Pers Soc Psychol. 1986;50(5):992–1003. doi:10.1037/0022-3514.50.5.992
2. Carver C, Scheier M, Weintraub J. Assessing coping strategies: a theoretically based approach. J Pers Soc Psychol. 1989;56(2):267–283. doi:10.1037/0022-3514.56.2.267
3. Baqutayan SMS. Stress and coping mechanisms: a historical overview. Mediterr J Soc Sci. 2015;6(2):479–488.
4. Orban LA, Stein R, Koenig LJ, et al. Coping strategies of adolescents living with HIV: disease-specific stressors and responses. AIDS Care. 2010;22(4):420–430. doi:10.1080/09540120903193724
5. Silva RTS, Silva R, Rodrigues IDCV, Neto V, Silva B, Souza F. Coping strategies of people living with aids in face of the disease. Rev Latino-Am Enfermagem. 2018;26:2985. doi:10.1590/1518-8345.2284.2985
6. Ministry of Health MP. National strategic plan (NSP): ending AIDS 2016–2030; 2015: 114.
7. Ministry of Health Malaysia. (2019). Country Progress Report on HIV/AIDS
8. Malaysia DOS. Department of statistics Malaysia official portal- population projection (Revised), Malaysia 2010–2040; 2016.
9. Fadzil NA, Othman Z, Mustafa M. Stigma in Malay patients with HIV/AIDS in Malaysia. Int Med J. 2016;23(4):1–4.
10. Laws of Malaysia Act 574 Penal Code, s. 377(D) (Outrages on decency); 2006.
11. Syariah Criminal Offences (Federal Territories) Act 1997, s. 25 (Liwat), s. 26 (Musahaqah), s. 28 (Male person posing as woman); 1997.
12. Smiley CL, Rebeiro PF, Cesar C, et al. Estimated life expectancy gains among adults with HIV with Antiretroviral Therapy in Latin America and the Caribbean: a multisite retrospective cohort study. Lancet HIV. 2021;8(5):e266–e73. doi:10.1016/S2352-3018(20)30358-1
13. Ministry of Health M. Malaysian society of HIV medicine- Malaysian consensus guidelines on antiretroviral therapy; 2017.
14. Positive Malaysian Treatment Access & Advocacy Group (MTAAG+). PLHIV Stigma Index, Malaysia, 2012
15. Chan YC, Mawardi M, Ismail AH. Stigmatizing attitudes toward people living with HIV/AIDS (PLWHA) among primary health care providers in Kinta District, Perak. Malays Fam Phy. 2021;16(1):31–38. doi:10.51866/oa0001
16. Department of Health & Human Services. Centers for disease control and prevention-HIV Stigma Fact Sheet: U.S.; 2021. Available from: https://www.cdc.gov/hiv/basics/hiv-stigma/index.html.
17. Chambers LA, Rueda S, Baker DN, et al. Stigma, HIV and health: a qualitative synthesis. BMC Public Health. 2015;15:848. doi:10.1186/s12889-015-2197-0
18. Lyimo RA, Stutterheim SE, Hospers HJ, Glee T, Ven A, Bruin M. Stigma, disclosure, coping, and medication adherence among people living with HIV/AIDS in Northern Tanzania. AIDS Patient Care STDS. 2014;28(2):98–105. doi:10.1089/apc.2013.0306
19. Kabbash IA, El-Gueneidy M, Sharaf AY, Hassan NM, Al-Nawawy AN. Needs assessment and coping strategies of persons infected with HIV in Egypt. East Mediterr Health J. 2008;14(6):1308–1320.
20. Puchalski C, Ferrell B, Virani R. Improving the quality of spiritual care as a dimension of palliative care: the report of the Consensus Conference. J Palliat Med. 2009;12(10):885–904. doi:10.1089/jpm.2009.0142
21. Lewis M. The role of spirituality in coping with chronic illness: what health care providers need to know for advance directive decision making. J Dr Nurs Pract. 2016;9(2):194–198. doi:10.1891/2380-9418.9.2.194
22. Wortmann J. Religious coping. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York: Springer; 2013:1647–1648.
23. Koenig HG. Spirituality in Patient Care: Why, How, When, and What.
24. Draman S, Liyana A, Farhani S, Jannah R, Rus R. Psycho-social and spiritual backgrounds, experiences, and needs as a transsexual: a qualitative study within Persatuan Insaf Pahang. Int Med J Malays. 2016;15:28–36.
25. Suofeiya M, Razali ZA, Subri IM, et al. Addressing muslim transgenders’ health issues using religious approach in the Malaysian setting. Adv Sci Lett. 2017;23(5):4880–4883. doi:10.1166/asl.2017.8938
26. Ironson G, Solomon GF, Balbin EG, et al. The ironson–woods spirituality/religiousness index is associated with long survival, health behaviors, less distress, and low cortisol in people with HIV/AIDS. Ann Behav Med. 2002;24(1):34–48. doi:10.1207/S15324796ABM2401_05
27. Szaflarski M, Ritchey PN, Leonard AC, et al. Modeling the effects of spirituality/religion on patients’ perceptions of living with HIV/AIDS. J Gen Intern Med. 2006;21:S28–S38. doi:10.1111/j.1525-1497.2006.00646.x
28. Olaore IB, Olaore AY. Is HIV/AIDS a consequence or divine judgment? Implications for faith-based social services. A Nigerian faith-based university’s study. J Soc Aspects HIV/AIDS. 2014;11(1):20–25. doi:10.1080/17290376.2014.910134
29. Lyon ME, Kimmel AL, Cheng YI, Wang J. The role of religiousness/spirituality in health-related quality of life among adolescents with HIV: a latent profile analysis. J Relig Health. 2016;55(5):1688–1699. doi:10.1007/s10943-016-0238-3
30. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18(1):148. doi:10.1186/s12874-018-0594-7
31. Boyce C, Neale P. CONDUCTING IN-DEPTH INTERVIEWS: A Guide for Designing and Conducting In-Depth Interviews for Evaluation Input. Pathfinder International; 2006.
32. Milena ZR, Dainora G, Alin S. Qualitative research methods: a comparison between focus-group and in-depth interview. Ann Faculty Econ. 2008;4(1):1279–1283.
33. Butina M, Narrative A. Approach to qualitative inquiry. Clin Lab Sci. 2015;28(3):190–196. doi:10.29074/ascls.28.3.190
34. Creswell JW, Miller DL. Determining validity in qualitative inquiry. Theory Pract. 2000;39(3):124–130. doi:10.1207/s15430421tip3903_2
35. Denzin NK. Sociological Methods: A Sourcebook. Aldine Transaction; 2006.
36. Patton MQ. Enhancing the quality and credibility of qualitative analysis. Health Serv Res. 1999;34(5 Pt 2):1189–1208.
37. Hammersley M. What’s Wrong with Ethnography?: Methodological Explorations.
38. Morse JM. Validity by Committee. Qual Health Res. 1998;8(4):443–445. doi:10.1177/104973239800800401
39. Malaysian AIDS council; 2019 Available from: https://www.mac.org.my/.
40. Arevalo EAP. Redefining the perceived quality of life of PLHIV through counseling programs: a case study of pinoy plus members. J Soc Health. 2018;1(2):72–103.
41. Ministry of Health M. Manual on HIV/AIDS in Islam. Department of Islamic Development Malaysia; 2011:132.
42. Aiman A. Only 50% of people with HIV seek treatment and here’s why, says AIDS council. Free Malaysia Today; 2018.
43. Norris SA, Anuar H, Matzen P, Cheah J, Jensen,BB, Hanson M. The life and health challenges of young Malaysian couples: results from a stakeholder consensus and engagement study to support non-communicable disease prevention. BMC Public Health. 2014;14(Suppl S2):S6. doi:10.1186/1471-2458-14-S2-S6
44. Brémault-Phillips S, Olson J, Brett-MacLean P, et al. Integrating spirituality as a key component of patient care. Religions. 2015;6:476–498. doi:10.3390/rel6020476
45. Draman S, Aris M, Anuar M, et al. Knowledge and Attitude towards HIV/AIDS among transsexuals in Kuantan, Pahang. Int Med J Malays. 2016;15:45–50.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.